Embed Size (px)
Citation preview

1

Have you ever had that experience, or witnessed someone else having it, when you have lost your carkeys, or your glasses, or something really important that you need. You are absolutely convinced they were right there, you might blame someone else for moving them. A?er half an hour of increasingly irritated searching you find them in a surprising spot you’d never thought of, and realise you must have le? them there all along. But you were absolutely convinced for a while that you’d put them somewhere else. Now, carkeys and spectacles generally don’t grow legs and move by themselves. But this liDle story illustrates how someEmes we irraEonally prefer to think they do, rather than raEonally accept that our first convicEon “I le? them right here!” might be wrong. If any of you watch TED Talks watch Kathryn Shultz’s “On being wrong”. She says something interesEng – most of the Eme being wrong feels exactly the same as being right; it’s only when we REALISE we are wrong we feel bad! While we intellectually appreciate that humans are fallible and make mistakes all the Eme, we personally feel ashamed/embarrassed about being wrong because since primary school it’s been ingrained in us that being wrong is BAD. This personal feeling about being wrong is a problem – as doctors, this subconscious human tendency to feel right all the Eme can make us unsafe. .
2

Now clearly I don’t want you to doubt your decisions all the Eme – doctors have to, a?er all, make decisions based on available informaEon! – but the message of this lecture is that being convinced you’re right isn’t enough (altho we have a human tendency to think that way) – instead you need to think how you got to that conclusion, and about whether your reasoning is sound. This lecture is about cogniEve debiasing strategies – methods you can use to keep your thinking in check when you are working on a clinical problem.
3

4

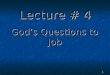
Acknowledgement: Pat Croskerry. A schemaEc applicaEon of dual process theory to diagnosEc reasoning. (Figure). In: Ch 9 of Cooper N and Frain J [Eds]. ABC of Clinical Reasoning. Wiley, 2016. As we have talked about previously, there are two principle modes of decision making, referred to as ‘dual process theory’. There’s a fast, intuiEve mode (type 1) which we use most of the Eme in everyday life, and a slow, deliberate, efforhul mode (type 2). Taking shortcuts and using abbreviated ways of thinking (what is called ‘heurisEcs’/paDern recognising or ‘rules of thumb’) works well a lot of the Eme and is parEcularly used by experts in their par7cular field (remember I told you how chess players could see pieces on a board mid-‐game like leDers in a word? – they just ‘see’ it and can recall the posiEon of every piece) – but for most situaEons it involves biases and can lead to costly errors. Last Eme we talked about the fact that errors in thinking can occur due to a mixture of knowledge gaps as well as cogniEve errors. If you don’t know what you don’t know you may apply the wrong ‘rule of thumb’ or interpret data incorrectly … this is why strategic reading is so important – for example taking 5 mins out to look up the answer to a quesEon. When clinicians are faced with a problem, if we “recognise” it we default in to fast, paDern recognising mode. [things that influence this in yellow box]. [Talk through slide]. But just because we are thinking this way does not mean we are unaware of it. We can stop to analyse our own thinking. Watch out for assumpEons!! Being able to think about your thinking is the key to good decision making in medicine. Because we are so prone to subconscious omissions and biases there are some established strategies that doctors use to prevent errors. That’s what we’re going to talk about now.
5

The most obvious guard against diagnosEc error is simple: take a history and examine the paEent. (In your clinical skills sessions you are learning I hope how to listen effec7vely for example). Sounds obvious? Many drs do not do it. Medical students get confused on MAU when they can’t get a history from the paEent and they have to get on the phone to get the history. Gesng the history is key. Here’s a story I heard only last week that illustrates how we o?en don’t pay aDenEon to the paEent’s story… Of all the diagnosEc tests that are used and abused, it is the humble d dimer. Introduced in the 1990's, it has become an important test in paEents with suspected venous thromboembolism (blood clots). D dimer is a small protein fragment present in the blood. It's levels shoot up when there is a blood clot somewhere in the body being degraded by a process known as fibrinolysis. D dimer is really useful when it is normal and the paEent is unlikely to have thromboembolism. Unfortunately, the opposite is not true. D dimer levels can be high for lots of reasons that have nothing to do with thromboembolism -‐ for example, bleeding/trauma, cancer, heart disease, infecEon/inflammaEon, pregnancy and old age. So when levels are raised it does not mean the paEent has thromboembolism ... I hope you see where I am going here. Tests rarely give a yes/no answer. Results have to be interpreted in the light of the paEent's story. That's why we have doctors. A 60-‐year-‐old man was clearing his guDer when he disturbed a wasps' nest. In the surprise and chaos that ensued, he fell off his ladder and got stung several Emes, bruising his hip in the process. He was brought to hospital by ambulance. To keep waiEng Emes down, paEents in UK Emergency Departments are usually seen by a triage nurse immediately on arrival and have bloods taken while waiEng to see a doctor. In this case, the paEent had a d dimer test and it was significantly raised. He was admiDed to the Acute Medical Unit, seen by a junior doctor and listed for a CT pulmonary angiogram (a test for a suspected blood clot on the lung). Now, even lay people will ask themselves at this point: how has falling off a ladder and being stung by wasps been interpreted as a blood clot on
6

AFTER taking a history and examining the paEent, being able to summarise what the problem is is a key skill in clinical reasoning terms. Last Eme I talked about using precise medical terms and pracEcing summary statements. Just to clarify – the presenEng complaint is in the pts own words, so is the history of presenEng complaint. But at the end of the history and examinaEon there is a really crucial moment when we synthesise all that gathered informaEon as doctors and translate it in to a summary of what we think is going on, and what could be causing it. There’s a reason you see House wriEng down problem lists and THEN the team discusses the differenEal diagnosis. This is in order to idenEfy key clinical data gathered from the history and examinaEon and iniEal test results. I encourage you to try this for yourself. PracEce “naming”/idenEfying problems of the case (history, exam, iniEal tests) using precise medical language (e.g. pleuriEc chest pain, polyuria and polydipsia, right sided hemi-‐paresis, thunderclap headache, high INR etc). Then consider the differenEal diagnosis that could be causing these problems. If you just leap to a differenEal diagnosis you can miss key problems that require acEon … example on next slide.
7

70 yr old woman “Polyuria and polydipsia in a type 2 diabeEc” is a summary statement We have also made a problem list by adding “low mood” We can work on differenEal diagnoses now – this is when the brain starts to make connecEons. Start with the most common things first – this is exercising your brain’s ability to reason probabalis7cally. Make connecEons -‐ for example, hypercalcaemia causes low mood as well as polyuria and polydipsia. This act of making connecEons is really important in knowledge organisaEon. This is when you can also read strategically – look up the causes of polyuria and polydipsia. But you have to apply this to your parEcular paEent. If the paEent does not look Cushingoid, it’s probably not Cushings. If she is not on any medicaEon, it’s not medicaEon. It’s only a?er this step you can make a proper PLAN. The job of a doctor is to decide what is going on and then make a plan. In this case we will take blood for glucose, calcium, U&Es, enquire about medicaEon. Maybe go back and double check for any Cushingoid features.
8

Another recommended read: `The checklist manifesto’ by Atul Gawande, US surgeon and author who led the introducEon of the WHO Surgical Checklist worldwide. AnaestheEsts use checklists when sesng up the anaestheEc machine e.g. SOCRATES for pain Site -‐ Onset -‐ Character -‐ RadiaEon -‐ AssociaEons -‐ Time course -‐ ExacerbaEng/Relieving factors – Severity Many scoring systems are more accurate than ‘clinical judgement’ e.g. ODawa Ankle Rules / Alvorado Score Using guidelines/o?en a flowchart e.g. assessment and management of acute severe asthma – good in emergencies. I always get the hyperkalaemia guideline/flowchart out when I am dealing with a case of that. First Q: is it haemolysed (tell story).
9

Which leads us nicely on to the topic of “human factors” The third aspect of cogniEve debiasing is understanding the science of human factors. Human factors is about human behaviour and team communicaEon. It’s about how we can make it easy for people to do the right thing through well designed equipment/work environment and how we train people to understand the limitaEons of human performance and how to communicate effecEvely in a team. The example of human factors I always use is the ATM. [read slide] The areas of the brain required for system 2 processes (more effort required) are most affected by things like stress, cogniEve overload, sleep deprivaEon and faEgue … There are specific situaEons or condiEons in which mistakes are more likely to happen. Human factors is a specific discipline in healthcare that you will be trained in at some point in the future. It covers: 1. An understanding of error/how things can go wrong 2. Understanding the limitaEons of human performance and how to miEgate this – including
how good rotas/workspace design/simplified procedures/checklists etc can make it easy for people to do the right thing (or create an accident waiEng to happen!)
3. How to communicate effec7vely in a team In the majority of serious healthcare accidents, poor communicaEon within the team played a major role. As students you learn lots about how to communicate with paEents, but in final year and house jobs you will learn about how important it is to communicate effecEvely with other team members.
10

hDps://youtu.be/L_oXvXtQlBA Human factors originated in the aviaEon industry – here’s a liDle video explaining more about it.
11

12
Let’s try this experiment. If you have done this before, please keep quiet! Look at this sentence for a few seconds -‐ how many ‘Fs’ are there?

13
How many people saw 2 Fs? 3? 4? 5? 6? (Usually there is a spread of answers across the group)

14
Here it is again.

15
There are 6 Fs – here they are highlighted. Now what is interesEng about this experiment is that everyone in the room is smart. Everyone can read English. And we were all looking at the same thing. I show this experiment to illustrate how someone can be really obvious to us, but not obvious to someone else who is looking at the same thing. And it’s absolutely nothing to do with how smart we are or how technically good we are at reading! So communicaEng in a clinical team, including staEng the obvious, or raising a concern out loud is really key in healthcare. Remember how we started this lecture by staEng that being convinced you’re right does not mean you are right at all!

16
This is a true story. Two large ships in a narrow strait in the USA crashed in to each other in the dark. The co-‐pilot saw the other ship approaching and said ‘do you see that light?’. ‘Yes’ replied the captain. However, the ships crashed before the captain realised the light was indeed another ship coming towards them. When asked why he did not state the obvious (eg the final sentence) to the captain, the co-‐pilot said it would have been ‘patronising and redundant’ to do so!

Many years ago I got some medical students to follow me and my team on the MAU WR. No-‐one knew what they were doing, they were just told the students would be observing us with clipboards and were not part of the team for that day. Their remit was to look at how the way we communicated impacted on pt safety. At the end of their study they wrote an amazing report. And they said, “Dr Cooper our eyes have been opened!”
17

This is what they found. The way we communicated on WRs was really unsafe. First, we commonly used “problemaEc pronouns” – he/she/it/they/the man in Bed 1 Second, we always interrupted eachother (unecessarily) – e.g. nurses on drug rounds Third, it was o?en so noisy we could not actually hear eachother and people did not speak up! Handovers were poor Junior drs were o?en unsure WHY they had been asked to request a test but did not aDempt to clarify with the Consultant at all … (this makes a big difference to how a test is then interpreted by the radiologist by the way). When interviewed later, EVERYONE said team communicaEon was really important. They had no idea how bad we were at it. They decided that some form of training would be helpful. So we introduced a few simple rules that are followed to this day. 1. No problemaEc pronouns 2. No unnecessary interrupEons 3. Regular board rounds with the whole team parEcipaEng, no interrupEons allowed 4. Speaking up when things are not clear 5. Using SBAR
18

The IoM published a landmark study 15 years ago “To Err is Human” which kick started massive change in healthcare quality across the world. It has just published a new report: “DiagnosEc error in healthcare”. IoM definiEon of diagnosEc error: the failure to a) establish an accurate and Emely explanaEon of the paEent’s health problem(s) or b) communicate that explanaEon to the paEent. The report is 350 pages long (!) but recommendaEons include: 1. Explicit training for healthcare professions in the diagnos7c process 2. Emphasis on mdt communica7on in the diagnos7c process and properly
involving the pa7ents and/or carers in gathering informa7on 3. Establish a work system and culture that supports the diagnosEc process (think
about your ward rounds!) 4. Develop and deploy approaches to idenEfy, learn from, and reduce diagnosEc
errors and near misses
19

20

You WILL have human factors training later in your career, for now pracEce this.
21

22