Embed Size (px)
DESCRIPTION
Putnam Hospital Center. CODE STROKE. Putnam Hospital Center Education and Training Department. STROKE CENTER MISSION. - PowerPoint PPT Presentation
Citation preview

CODE STROKECODE STROKE
Putnam Hospital CenterPutnam Hospital CenterEducation and Training DepartmentEducation and Training Department
Putnam Hospital Putnam Hospital CenterCenter

STROKE CENTER STROKE CENTER MISSIONMISSION
The mission of the Stroke Program at Putnam Hospital Center The mission of the Stroke Program at Putnam Hospital Center is to provide state of the art, high quality medical and is to provide state of the art, high quality medical and diagnostic care to our patients who are identified as diagnostic care to our patients who are identified as possible stroke victims. All patients presenting with signs possible stroke victims. All patients presenting with signs and symptoms of Acute CVA, will be evaluated upon and symptoms of Acute CVA, will be evaluated upon arrival. They will be evaluated using established criteria for arrival. They will be evaluated using established criteria for administration of t-PA or other appropriate therapies. Each administration of t-PA or other appropriate therapies. Each patient will receive assessment, stabilization, diagnostic patient will receive assessment, stabilization, diagnostic treatment and interventions within the timeframe and treatment and interventions within the timeframe and guidelines set by the AHA/American Stroke Association.guidelines set by the AHA/American Stroke Association.
Key Elements in place to provide this care are:Key Elements in place to provide this care are: Evidence based medical and nursing care Evidence based medical and nursing care Interdepartmental approach for quality careInterdepartmental approach for quality care Education for patients and familiesEducation for patients and families Safe and appropriate discharge planningSafe and appropriate discharge planning Continuing medical and nursing educationContinuing medical and nursing education Community EducationCommunity Education

Our Commitment is Our Commitment is to…to… ……education, including hospital staff, pre-education, including hospital staff, pre-
hospital care providers, patients and the hospital care providers, patients and the community at large community at large
……quality and a continuing drive to improve the quality and a continuing drive to improve the care given to our patientscare given to our patients
……offer support services that are available 24 offer support services that are available 24 hours a day, 7 days a weekhours a day, 7 days a week
……provide timely and efficient transfers when provide timely and efficient transfers when needed. We have documented transfer needed. We have documented transfer agreements with Vassar Brothers Medical agreements with Vassar Brothers Medical Center and Westchester Medical Center for Center and Westchester Medical Center for neurosurgical services should they be neededneurosurgical services should they be needed

Designated Stroke Designated Stroke CenterCenter
These services are provided by utilizingThese services are provided by utilizing Multidisciplinary Approach Multidisciplinary Approach Designated bedsDesignated beds Performance Improvement Initiatives: Performance Improvement Initiatives:
Get With the Guidelines (GWTG)Get With the Guidelines (GWTG) Highly trained, dedicated staff which Highly trained, dedicated staff which
includes:includes: Physicians ~ Board Certified in Physicians ~ Board Certified in
Emergency Medicine, Neurology Emergency Medicine, Neurology and Interventional Radiologyand Interventional Radiology
Dedicated critical care, step-down Dedicated critical care, step-down and medical staffand medical staff
The latest monitoring and The latest monitoring and treatment technology for the care treatment technology for the care of stroke patientsof stroke patients

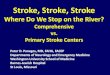
EmergencyDepartment
Registered Nurse
Registered Nurseon the Inpatient
Care Unit
EmergencyDepartmentPhysician
Stroke CenterProgram Director
EMS Paramedic
OccupationalTherapist
Attending PrimaryCare Physician
AttendingNeurologist
PhysicalTherapist
Dietician Speech Therapist
PUTNAM HOSPITAL CENTER STROKE TEAM MEMBERS

PROCEDUREPROCEDURE
Coordinated Care between the Coordinated Care between the ED and EMS ED and EMS
Patient assessed by EMS utilizing Patient assessed by EMS utilizing Cincinnati Stroke ScaleCincinnati Stroke Scale
Emergency Department contacted via Emergency Department contacted via radio or ALS phone regarding acute stroke radio or ALS phone regarding acute stroke patient en-route to facility.patient en-route to facility.
Medical control physician alerts secretary Medical control physician alerts secretary and nursing staff of incoming acute stroke and nursing staff of incoming acute stroke patientpatient
Ancillary services (radiology/lab) notified Ancillary services (radiology/lab) notified of incoming code stroke patient.of incoming code stroke patient.

Cincinnati Pre-Hospital Stroke Scale
Assess for facial droop: have the patient show their teeth or ask the patient to smile.
Assess for arm drift: have the patient close their eyes and hold both arms straight out for 10 seconds.
Assess for abnormal speech: have the patient say, “you can’t teach an old dog new tricks.”

Suspected CVA
R/o other causes of symptoms– Hypoxia– Hypoglycemia– Hypoperfusion– Post Ictal (Todd's Paralysis)
Determine Time of onset of symptoms– Less than 2 hours transport to
Stroke Center.

ASSESSMENT and ASSESSMENT and TREATMENT TIMEFRAMESTREATMENT TIMEFRAMES
Assessment and treatment times frames Assessment and treatment times frames are less than or equal to:are less than or equal to:
Door to MD assessmentDoor to MD assessment 10 minutes 10 minutes Door to Stroke Team contactDoor to Stroke Team contact 10 minutes 10 minutes Door to CT ScanDoor to CT Scan 25 minutes 25 minutes Door to CT read timeDoor to CT read time 45 minutes 45 minutes Door to Lab resultsDoor to Lab results 45 minutes45 minutes Door to t-PA administrationDoor to t-PA administration 1 hour * 1 hour *
(* from door to med – FDA is 3 (* from door to med – FDA is 3 hours from hours from
onset of witnessed symptoms) onset of witnessed symptoms)

““Code Stroke” Code Stroke” Inpatient ProtocolInpatient Protocol
Utilized for emergent treatment of patients, Utilized for emergent treatment of patients, staff or visitors currently in the hospital staff or visitors currently in the hospital building presenting with symptoms of stroke.building presenting with symptoms of stroke.
Anytime a person exhibits signs or symptoms Anytime a person exhibits signs or symptoms of stroke, and onset is less than three hours, of stroke, and onset is less than three hours, “Code Stroke” may be activated by a staff “Code Stroke” may be activated by a staff member of the hospital.member of the hospital.
Code Stroke team is activated by dialing Code Stroke team is activated by dialing “2222” and telling the operator to page “2222” and telling the operator to page “Code Stroke” overhead, adding the unit “Code Stroke” overhead, adding the unit where the event where the event
is occurring.is occurring.

PROCEDUREPROCEDURE ~ ~ TEAM ACTIVATIONTEAM ACTIVATION
Rapid Response TeamRapid Response Team responds to the responds to the call for all inpatient unitscall for all inpatient units
Emergency Dept. Code Response Emergency Dept. Code Response TeamTeam responds to all other hospital responds to all other hospital locations (outpatient, staff, or visitors)locations (outpatient, staff, or visitors)
““Code StrokeCode Stroke” alerts the Radiology dept.:” alerts the Radiology dept.: if CT scan is in use, to remove the patient from CT if CT scan is in use, to remove the patient from CT
and prepare for STAT CT scan of stroke patientand prepare for STAT CT scan of stroke patient
““Code StrokeCode Stroke” alerts lab:” alerts lab: to perform STAT lab work and turn around results to perform STAT lab work and turn around results
in 45 minutes or lessin 45 minutes or less

CODE STROKE CODE STROKE ~ POLICY, PROCEDURE ~ POLICY, PROCEDURE AND AND
DOCUMENTATION DOCUMENTATION
Code Stroke PacketCode Stroke Packet Policy & ProcedurePolicy & Procedure Code Stroke Order SheetCode Stroke Order Sheet NIH Stroke Scale Assessment SheetNIH Stroke Scale Assessment Sheet Consent Form for t-PAConsent Form for t-PA Admission or Transfer protocolsAdmission or Transfer protocols Admission Order SetsAdmission Order Sets

CODE STROKE CODE STROKE DOCUMENTATIONDOCUMENTATION Code Stroke Flow Sheets ensure Code Stroke Flow Sheets ensure
documentation compliance documentation compliance TimelineTimeline DiagnosticsDiagnostics NIHSSNIHSS Eligibility/Exclusion CriteriaEligibility/Exclusion Criteria Medications/InterventionsMedications/Interventions

CODE STROKECODE STROKE~ STROKE ~ STROKE
LOGLOG Stroke Log is the evaluation Stroke Log is the evaluation
tool used measure tool used measure
compliance withcompliance with
the evidence based the evidence based
timeframestimeframes

PUTNAM HOSPITAL CENTER PATIENT CARE SERVICES PUTNAM HOSPITAL CENTER PATIENT CARE SERVICES UNIT: DATE OF UNIT: DATE OF CODE:CODE:
PERFORMANCE IMPROVEMENTCODE STROKE EVALUATION RECORD PERFORMANCE IMPROVEMENTCODE STROKE EVALUATION RECORD TIME OF TIME OF CODE:CODE:
PATIENT NAME/DRILL:PATIENT NAME/DRILL:PRIMARY DIAGNOSIS:PRIMARY DIAGNOSIS:
1. Was Critical EMS assessment completed, if applicable, and appropriate actions taken? 1. Was Critical EMS assessment completed, if applicable, and appropriate actions taken? YES YES NO NO Support ABC’s: oxygen given if needed Support ABC’s: oxygen given if needed YES YES NO NO Perform pre-hospital stroke assessment Perform pre-hospital stroke assessment YES YES NO NO Establish time when patient last known normal Establish time when patient last known normal YES YES NO NO Transport: consider bringing a witness, family member or caregiver Transport: consider bringing a witness, family member or caregiver YES YES NO NO Alert hospital YES Alert hospital YES NO NO Check glucose if possible Check glucose if possible YES YES NO NO2. Support ABC’s: oxygen given if needed YES 2. Support ABC’s: oxygen given if needed YES NO NO Perform pre-hospital stroke assessment YESPerform pre-hospital stroke assessment YES NO NO Establish time when patient last known normal YES Establish time when patient last known normal YES NO NO Transport: consider bringing a witness, family member or caregiver YES Transport: consider bringing a witness, family member or caregiver YES NO NO Alert hospital Alert hospital YES YES NO NO Check glucose if possible Check glucose if possible YESYES NO NO3. Was there an immediate neurologic assessment by stroke team or designee 3. Was there an immediate neurologic assessment by stroke team or designee YESYES NO NO completed within completed within 25 minutes25 minutes of arrival in the ED? of arrival in the ED? YESYES NO NO Review of patient historyReview of patient history YESYES NO NO Establish symptom onsetEstablish symptom onset YESYES NO NO Perform neurologic examination using NIH Stroke Scale Perform neurologic examination using NIH Stroke Scale YESYES NO NO4. Was CT report received within 4. Was CT report received within 45 minutes 45 minutes of arrival in ED? of arrival in ED? YES YES NO NO5. Was CT consistent with no hemorrhage?5. Was CT consistent with no hemorrhage? YES YES NO NO If yes If yes Check for fibrinolytic exclusions Check for fibrinolytic exclusions YES YES NO NO Repeat the neurologic exam: are deficits rapidly improving to normal?Repeat the neurologic exam: are deficits rapidly improving to normal? YES YES NO NO 6. Was CT consistent with hemorrhage? 6. Was CT consistent with hemorrhage? YES YES NO NO If yes If yes Consult neurologist or neurosurgeon Consult neurologist or neurosurgeon YES YES NO NO Consider transfer to another facility Consider transfer to another facility YES YES NO NO 7. Is patient a candidate for fibrinolytic therapy? 7. Is patient a candidate for fibrinolytic therapy? YES YES NO NO 8. If not a candidate for fibrinolytic therapy was ASA given?8. If not a candidate for fibrinolytic therapy was ASA given? YES YES NO NO 9. If an appropriate candidate were risks and benefits explained and tPA 9. If an appropriate candidate were risks and benefits explained and tPA administered within administered within 60 minutes60 minutes of arrival in ED? of arrival in ED? YES YES NO NO
SIGNATURE AND COMMENTS OF EVALUATOR: SIGNATURE AND COMMENTS OF EVALUATOR:

DEPARTMENTAL DEPARTMENTAL RESPONSIBILITIESRESPONSIBILITIES Each department has established Each department has established
responsibilities responsibilities Each department involved in the Each department involved in the CODE STROKECODE STROKE
– Coordinates with each other Coordinates with each other – to ensure the highest quality care to ensure the highest quality care – in the most efficient amount of time ~in the most efficient amount of time ~
Time is of the essence!Time is of the essence!

CODE STROKECODE STROKE~EMERGENCY ~EMERGENCY DEPARTMENTDEPARTMENT Identification/Notification of a Identification/Notification of a
potential “potential “Code StrokeCode Stroke” patient” patient Preliminary notification of Preliminary notification of
Radiology and LaboratoryRadiology and Laboratory Patient Room Patient Room placementplacement 1 to 1 Nursing Care1 to 1 Nursing Care

CODE STROKECODE STROKE~Radiology~Radiology
All Radiologists are experienced in the All Radiologists are experienced in the interpretation of interpretation of
acute stroke CT andacute stroke CT and
MR Neuro-imagesMR Neuro-images Fellowship-trained Fellowship-trained
neuro-radiologists areneuro-radiologists are
on call 24/7 on call 24/7

CODE STROKECODE STROKE
~RADIOLOGY~RADIOLOGYGoal:Goal: Perform Rapid CT Assessment of “BRAIN Perform Rapid CT Assessment of “BRAIN
ATTACK” ATTACK” Patient with a timely, expert interpretationPatient with a timely, expert interpretation
Emergency Dept. informs CT Technologist of Emergency Dept. informs CT Technologist of Code StrokeCode Stroke CT Table is held open until patient arrivesCT Table is held open until patient arrives Radiologist is informed of Radiologist is informed of pending scanpending scan Scan performed Scan performed Results Results communicated communicated to ED physician to ED physician within designatedwithin designated timeframetimeframe

CODE STROKECODE STROKE
~LABORATORY~LABORATORY Emergency Department Emergency Department
– Calls to notify Lab of impending Code Stroke specimenCalls to notify Lab of impending Code Stroke specimen– Complete patient information is given to the Lab office Complete patient information is given to the Lab office
staff who takes the callstaff who takes the call– Lab office staff notifies the Lab technical staff of Lab office staff notifies the Lab technical staff of
impending Code Stroke so they can prepare workstations impending Code Stroke so they can prepare workstations – Lab office staff member who took the call has ownership Lab office staff member who took the call has ownership
of the specimen to log it in and deliver it to the lab of the specimen to log it in and deliver it to the lab technical staff for analysis. technical staff for analysis.
There are no handoffs! Chain of There are no handoffs! Chain of custody must be maintained by custody must be maintained by the staff member who took the call.the staff member who took the call. Lab technical staff calls the result to the ERLab technical staff calls the result to the ER

CODE STROKE CODE STROKE ~CRITICAL CARE SERVICES~CRITICAL CARE SERVICES
* ADMISSION CRITERIA * ADMISSION CRITERIA ** Acute neurologic events requiring frequent Acute neurologic events requiring frequent neurological or respiratory checks to evaluate neurological or respiratory checks to evaluate progression including:progression including:
Post IV t-PAPost IV t-PA Large hemispheric stroke, in whom impending mental Large hemispheric stroke, in whom impending mental
status decline and loss of protective airway reflexes is of status decline and loss of protective airway reflexes is of a concerna concern
Basilar thrombosis or top of the basilar syndromeBasilar thrombosis or top of the basilar syndrome Crescendo TIA’sCrescendo TIA’s Patients requiring blood pressure augmentation for a Patients requiring blood pressure augmentation for a
documented area of hypoperfusiondocumented area of hypoperfusion IV blood pressure or heart rate controlIV blood pressure or heart rate control Every1-2 h neurological evaluation depending on Every1-2 h neurological evaluation depending on
symptom fluctuation or if ongoing ischemia is suspectedsymptom fluctuation or if ongoing ischemia is suspected Worsening neurological statusWorsening neurological status

CODE STROKE CODE STROKE ~CRITICAL CARE SERVICES~CRITICAL CARE SERVICES
The “Neuro Stroke Scale Assessment Flow Sheet” The “Neuro Stroke Scale Assessment Flow Sheet” will be used to monitor will be used to monitor
All post t-PA patients with assessments done q1h x 24 hours All post t-PA patients with assessments done q1h x 24 hours All non t-PA patients with assessments done q2h x 24 hoursAll non t-PA patients with assessments done q2h x 24 hours
Stroke patients will have special attention paid to:Stroke patients will have special attention paid to: Eye careEye care Potential for seizurePotential for seizure AirwayAirway Tissue perfusionTissue perfusion Safety needsSafety needs Altered body imageAltered body image Mobility – DVT – skin breakdownMobility – DVT – skin breakdown Nutritional concernsNutritional concerns Glucose managementGlucose management Signs and symptoms of meningeal irritationSigns and symptoms of meningeal irritation

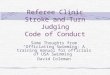
1a. Level of Consciousness:(Alert Drowsy etc.)
AlertDrowsyStuporousComa
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
1b. LOC Questions:(Month Age)
Answers both correctlyAnswers one correctlyBoth incorrect0
012
012
012
012
012
012
012
012
012
012
012
012
1c. LOC Commands:(Open, close eyes ;make fist, let go)
Obeys both correctlyObeys one correctlyBoth incorrect
012
012
012
012
012
012
012
012
012
012
012
012
2. Best Gaze:(Eyes open- patient follows finger or face)
NormalPartial gaze palsyForced deviation
012
012
012
012
012
012
012
012
012
012
012
012
3. Visual:(Introduce visual stimulus to patient’s visual field quadrants
No visual lossPartial hemianopiaComplete hemianopiaBilateral hemianopia
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
4. Facial Palsy:(Show teeth, raise eyebrows and squeeze eyes shut)
NormalMinorPartialComplete
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
5a. Motor Arm Left:(Elevate extremity to 90 degrees and score drift/movement)
No driftDriftCan’t resist gravityNo effort against gravity
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
0123
PUTNAM HOSPITAL CENTER PARTIAL FORM
NEURO STROJKE ASSESSMENT FLOW SHEET Circle times when patient care was
rendered 7 - 8 - 9 - 10 - 11 - 12 - 13 - 14 - 15 - 16 - 17 - 18 - 19 - 20 - 21 - 22 - 23 - 24 - 1 - 2 - 3 - 4 - 5 - 6
CATEGORY DESCRIPTION SCORE

CODE STROKE CODE STROKE ~MEDICAL ~MEDICAL
SERVICESSERVICES Identified Unit: Reed 2Identified Unit: Reed 2
Close to Nursing Station to facilitate safetyClose to Nursing Station to facilitate safety Easy access to equipment Easy access to equipment Modifications to the environmentModifications to the environment
All Stroke Patients onAll Stroke Patients on Yellow Dot/Falls Prevention ProgramYellow Dot/Falls Prevention Program Aspiration PrecautionsAspiration Precautions
Patient and Family Education OngoingPatient and Family Education Ongoing Begins in the Emergency DepartmentBegins in the Emergency Department Follows through discharge and outpatientFollows through discharge and outpatient

CODE STROKE ~ CODE STROKE ~ DocumentationDocumentation NIHSS needs to be completed at:NIHSS needs to be completed at:
15 minutes15 minutes 30 minutes30 minutes 60 minutes60 minutes 90 minutes90 minutes Per order for 24 hours or 48 hoursPer order for 24 hours or 48 hours DischargeDischarge

CODE STROKE ~ CODE STROKE ~ Documentation Documentation
CernerCerner Interactive ViewInteractive View
Complete Neurological AssessmentComplete Neurological Assessment Include appropriate NIHSSInclude appropriate NIHSS Include education provided to patient Include education provided to patient
and familyand family

CODE STROKE ~ CODE STROKE ~ Documentation Documentation
DischargeDischarge NIHSS must be done at dischargeNIHSS must be done at discharge Documentation of where patient is Documentation of where patient is
going after dischargegoing after discharge Documentation of discharge Documentation of discharge
medicationsmedications BOX MUST BE CHECKEDBOX MUST BE CHECKED FOR THE FOR THE
EDUCATION PORTION (page 2) OF THE EDUCATION PORTION (page 2) OF THE DISCHARGE FORMDISCHARGE FORM
Time out must be completed by two Time out must be completed by two nurses signifying that the form is nurses signifying that the form is complete and that all information has complete and that all information has been relayed to the patientbeen relayed to the patient

CODE STROKE CODE STROKE ~~REHABILITATION REHABILITATION
DEPARTMENTDEPARTMENT PHC offers comprehensive PHC offers comprehensive
Rehabilitative Services for Inpatients Rehabilitative Services for Inpatients and Outpatients and Outpatients
These services include:These services include: Physical TherapyPhysical Therapy
Range of Motion & StrengthRange of Motion & Strength Functional Mobility, Gait & BalanceFunctional Mobility, Gait & Balance
Occupational TherapyOccupational Therapy ADL’s, Safety Awareness & CognitionADL’s, Safety Awareness & Cognition
Speech and Language PathologySpeech and Language Pathology Speech, Language & Swallowing Speech, Language & Swallowing
difficultiesdifficulties

CODE STROKECODE STROKE ~CASE ~CASE MANAGEMENTMANAGEMENT Psychosocial/Continuing Care Psychosocial/Continuing Care
AssessmentAssessment 24-48 hrs. after admission24-48 hrs. after admission
Social Work Referral if indicated Social Work Referral if indicated to assist with supportive counseling to assist with supportive counseling
regarding adjustment to deficitsregarding adjustment to deficits Utilization Management Advocacy Utilization Management Advocacy
to assist patient in discharging to the to assist patient in discharging to the most appropriate post hospital care most appropriate post hospital care settingsetting

Education and TrainingEducation and Training
Annual Staff EducationAnnual Staff Education All nursing staff involved in Acute All nursing staff involved in Acute
Stroke patient care Stroke patient care Attend 4 hours of stroke education Attend 4 hours of stroke education
annuallyannually Stroke specific educational Stroke specific educational
opportunities provided by PHC opportunities provided by PHC throughout the yearthroughout the year

Educational Support of Educational Support of EMS by the Stroke EMS by the Stroke
CenterCenter EMS receives lectures bi-monthly EMS receives lectures bi-monthly
from the Assistant Director of the from the Assistant Director of the Department of Emergency Department of Emergency MedicineMedicine
Bi-annual education regarding Bi-annual education regarding acute stroke provided to EMS via acute stroke provided to EMS via didactic lectures, case didactic lectures, case presentations, and call auditspresentations, and call audits

CODE STROKECODE STROKE ~PERFORMANCE ~PERFORMANCE IMPROVEMENTIMPROVEMENT Chart reviews Chart reviews
Data is aggregated Data is aggregated Monthly P. I. meetings Monthly P. I. meetings Results forwarded to the Performance Results forwarded to the Performance
Improvement CommitteeImprovement Committee Findings reported to: Patient Care Findings reported to: Patient Care
Services, Hospital QA Committee and Services, Hospital QA Committee and to department staff members to department staff members

PROPERTIES
On passing, 'Finish' button: Close WindowOn failing, 'Finish' button: Goes to SlideAllow user to leave quiz: At any timeUser may view slides after quiz: At any timeUser may attempt quiz: 2 times