Embed Size (px)
Citation preview

IMAGE OF THE ISSUE
Cobra-head choledochocele: depiction with computed tomographyand cholangiogramAnkur Arora1, Abhay Kapoor2 & Sunil Kumar Puri2
1Department of Radiodiagnosis, Institute of Liver & Biliary Sciences, and 2Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India
Received 15 February 2012; accepted 20 February 2012
CorrespondenceAnkur Arora, Department of Radiodiagnosis, Institute of Liver & Biliary Sciences, D-1 Vasant Kunj, New Delhi-110070, India. Tel.: +91
9873030114. Fax: +91 11 23411385. E-mail: [email protected]
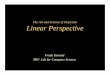
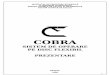
A 35-year old male with acute cholecystitis and septic cholangitisunderwent an open cholecystectomy before referral. Subsequentcontrast-enhanced CT showed a cystic intra-duodenal lesion atthe ampulla of Vater (Fig. 1a) and a T-tube cholangiogramshowed a lower common bile duct ovoid filling defect protrudinginto the duodenum giving a characteristic ‘cobra-head’ appear-ance suggestive of Type-III choledochocele. There was also anintra-luminal calculus seen as a filling defect (arrow) (Fig. 1b).
A Type-III choledochal cyst is one of the most infrequentsubtypes of choledochal cysts, constituting 1–5% of all cases.1
Type IIIa represents an intraluminal choledochocoele in theduodenum that contains the terminal pancreatic as well as the
common bile duct as a common channel; Type IIIb contains aseparate pancreatic and a common duct within an intraluminalcyst; and Type IIIc shows a completely intramural cyst within theduodenal wall.2
References
1. De Backer AI, Van den Abbeele K, De Schepper AM, Van Baarle A. (2000)
Choledochocele: diagnosis by magnetic resonance imaging. Abdom
Imaging 25:508–510.
2. Greene FL, Brown JJ, Rubinstein P, Anderson MC. (1985) Choledochocele
and recurrent pancreatitis. Diagnosis and surgical management. Am J Surg
149:306–309.
Figure 1 Contrast-enhanced CT scan reveals cystic lesion protruding into the second part of duodenum in the region of ampulla (arrow).T-tube cholangiogram displays a bulbous dilatation of the distal common bile duct (arrow), which protrudes into the duodenum giving riseto a ‘cobra-head’ appearance. Intra-luminal calculus is seen as an ovoid filling defect
DOI:10.1111/j.1477-2574.2012.00459.x HPB
HPB 2012, 14, 422 © 2012 International Hepato-Pancreato-Biliary Association