Embed Size (px)
Citation preview
Co-operation, competition and choice:
The NHS meets the market
Andrew Streetwww.york.ac.uk/inst/che/street.htm
CENTRE FOR HEALTH ECONOMICS
NHS Reforms
• Foundation Trusts• Practice Based Commissioning• Patient Choice• Payment by Results• Independent Sector• Workforce reforms
– Agenda for Change; – Revised contracts; – Changes to recruitment, retention & training
CENTRE FOR HEALTH ECONOMICS
Foundation status
• “Self-government for hospitals will encourage a stronger sense of local ownership and pride, building on the enormous fund of goodwill that exists in local communities …
• All this will ensure a better deal for the public, • improving the choice and quality of the services
offered and • the efficiency with which those services are
delivered” (p22)
CENTRE FOR HEALTH ECONOMICS

Practice based commissioning
• “The Government will enable money to flow with the patient from the GP practice itself
• The Government’s aim is to encourage a substantial number of GP practices to apply to manage their own budgets” (p50,53)
CENTRE FOR HEALTH ECONOMICS
Patient choice
• “We aim to extend patient choice … • Trusts will have an incentive to attract
patients .... • And it will be easier for patients to choose
(and change) their own GP as they wish” (p4,5)
CENTRE FOR HEALTH ECONOMICS
Payment by results
• “A Trust will earn its revenue from the services it provides …
• There will be an opportunity to finance improved and expanded services because the money will flow to where patients are going.
• Hospitals which prove more popular with GPs and patients will attract a larger share of NHS resources.” (p24)
CENTRE FOR HEALTH ECONOMICS

Independent sector
• “There is a growing partnership between the NHS and the independent health sector …
• This relieves pressure on the NHS and … • the reforms will open up further
opportunities for the two sectors to work together for their mutual benefit” (p68)
CENTRE FOR HEALTH ECONOMICS

Staff
• ‘‘A skilled and dedicated staff –
• backed by enormously increased resources
• – have coped superbly with the growing demands of modern medicine and increasing numbers of patients.’’
CENTRE FOR HEALTH ECONOMICS
CENTRE FOR HEALTH ECONOMICS
Then & Now
• Two key differences:
• Enormously increased resources
• Payment by Results: the introduction of the fixed tariffs (prices)
CENTRE FOR HEALTH ECONOMICS

Health Expenditure – cash (£bn)
CENTRE FOR HEALTH ECONOMICS
0
10
20
30
40
50
60
70
80
90
100
1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003
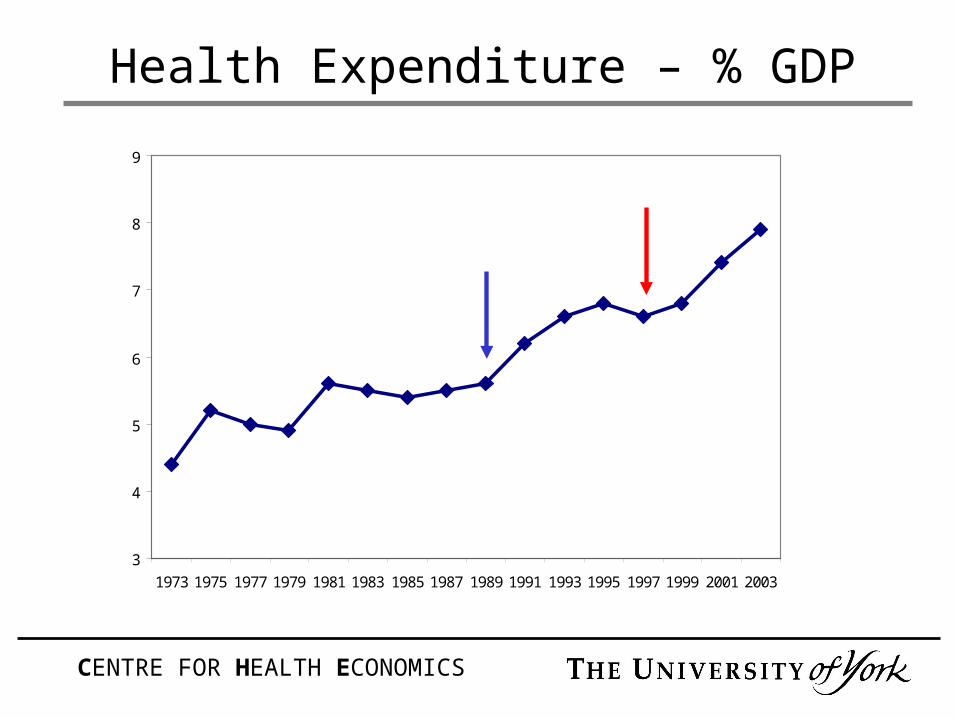
Health Expenditure – % GDP
CENTRE FOR HEALTH ECONOMICS
3
4
5
6
7
8
9
1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003

Cash Transfusion
The Economist, April 23 2005
• ‘‘The NHS budget rose in real terms by 7% a year from 1998 to 2003
• but its real output rose by only 3.7% a year
• It’s the government’s fault ...
• … cash is no good without reform’’
CENTRE FOR HEALTH ECONOMICS

What is “real” output?
• Not just finished consultant episodes and prescriptions
• What about primary and community care?
• What about reduced waiting times?
• What about declining mortality rates?
• What about a health system that treats people with dignity and respect?
CENTRE FOR HEALTH ECONOMICS

Payment by results
The Economist, April 23 2005• ‘‘The government has reintroduced the internal
market but on a more ambitious scale than in the 1990s
• The biggest change is to the payments system • The payments-by-results system will show up
inefficiencies in the system and, if carried to its logical conclusion,
• will lead to hospital closures and mergers”
CENTRE FOR HEALTH ECONOMICS
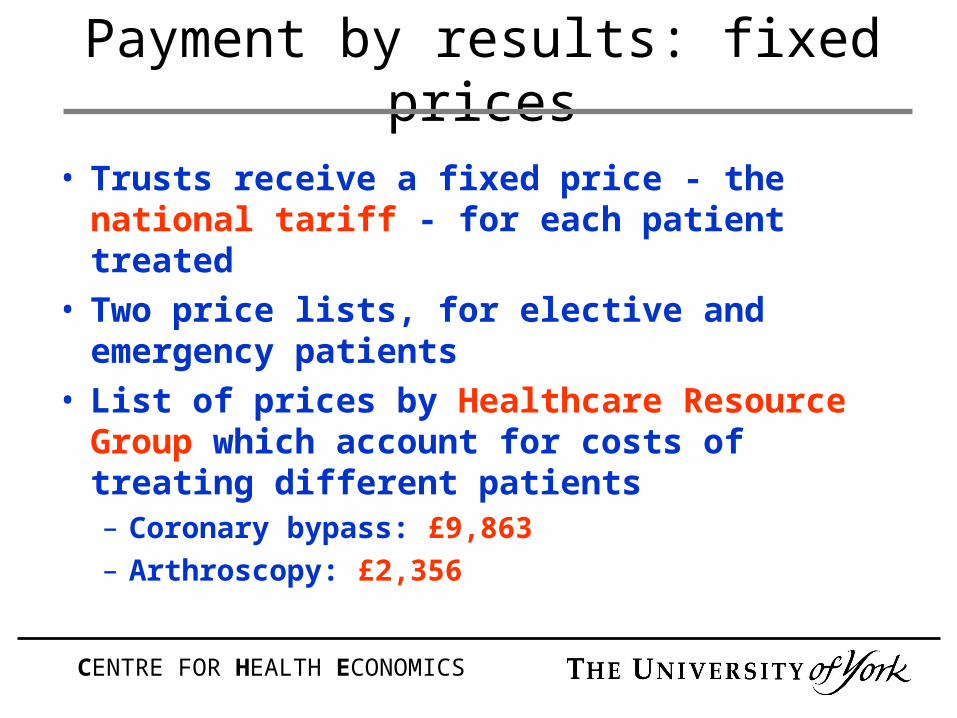
Payment by results: fixed prices
• Trusts receive a fixed price - the national tariff - for each patient treated
• Two price lists, for elective and emergency patients
• List of prices by Healthcare Resource Group which account for costs of treating different patients – Coronary bypass: £9,863
– Arthroscopy: £2,356
CENTRE FOR HEALTH ECONOMICS

Payment by results: transition
• All Foundation Trusts and Independent Sector providers
• Limited number of elective procedures in other NHS Trusts
• Aim to apply to all activity, including community and mental health, by 2007/8
CENTRE FOR HEALTH ECONOMICS

Payment by results: objectives
• Improve efficiency: payment for each patient treated
• Support choice: money follows patients
• End price competition: same price across England
CENTRE FOR HEALTH ECONOMICS
Question 1By 2007/8 Payment by Results will
apply to all NHS activity.
In how many – and which – other countries do hospitals receive all their income from PbR
type payments?
CENTRE FOR HEALTH ECONOMICS

Question 2How much of the income of an
average hospital in the US is based on PbR type payment?
< 20% 20% - 40%
40% - 60%
60% - 80% 80% - 100%
CENTRE FOR HEALTH ECONOMICS

Question 3In 301AD in Ancient Rome you could buy a turtledove in good
condition for 16 denarii.
How much would you have to pay for a wild turtledove?
CENTRE FOR HEALTH ECONOMICS

Diocletian Edict on Prices - 301AD
“Immoderate prices are so widespread that the uncurbed passion for gain is lessened neither by abundant supplies nor by fruitful years”
“It is our pleasure that the prices listed in the subjoined summary be observed in the whole of our empire in such a fashion that every man may know that permission to exceed them has been forbidden him”
CENTRE FOR HEALTH ECONOMICS
“Anyone who shall have resisted the form of this statute shall for his daring be subject to a capital penalty.” (The Edict of Diocletian)
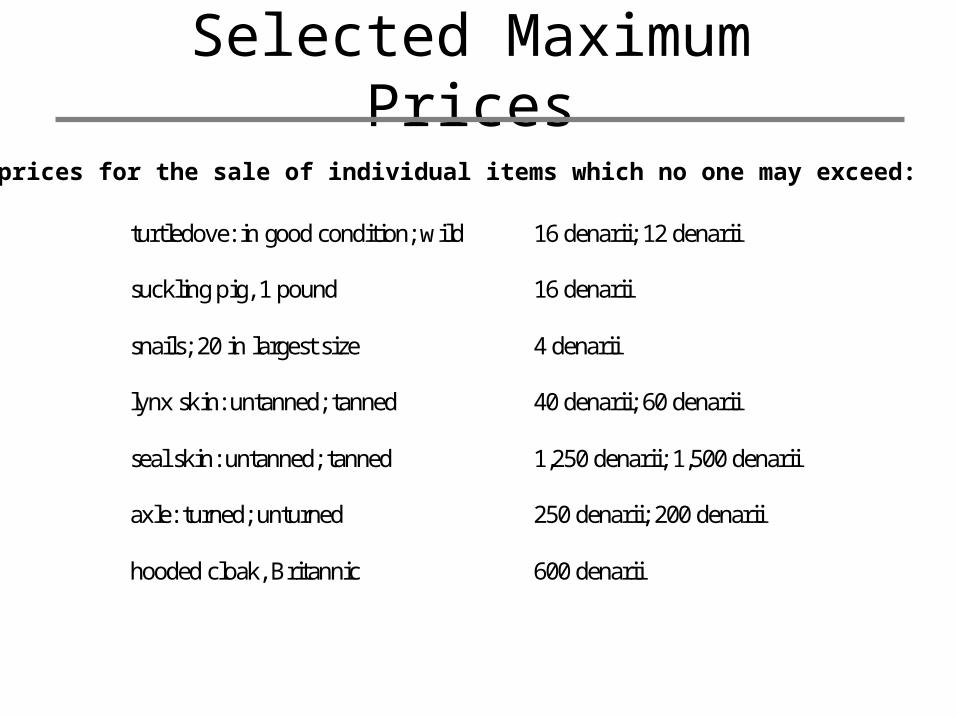
Selected Maximum Prices
turtledove: in good condition; wild 16 denarii; 12 denarii
suckling pig, 1 pound 16 denarii
snails; 20 in largest size 4 denarii
lynx skin: untanned; tanned 40 denarii; 60 denarii
seal skin: untanned; tanned 1,250 denarii; 1,500 denarii
axle: turned; unturned 250 denarii; 200 denarii
hooded cloak, Britannic 600 denarii
The prices for the sale of individual items which no one may exceed:

Benefits to the Roman Soldier
“Much blood was shed for the merest trifles; men were afraid to display anything for sale, and the scarcity became more grievous and excessive than ever” (Lactantius On the Manner in which the Persecutors Died)
A policy designed to make goods affordable failed because it made them unavailable
CENTRE FOR HEALTH ECONOMICS

The Verdict
“ The whole edict is, perhaps, the most gigantic effort of a blind though well-intentioned despotism, to control that which is, and ought to be, beyond the regulation of government” (Milman, notes on Gibbon’s Decline and Fall of the Roman Empire)
CENTRE FOR HEALTH ECONOMICS
Benefits to the English Patient
Patient Choice:
“Patients will be able to choose providers knowing that funding will not be an obstacle”
CENTRE FOR HEALTH ECONOMICS
Penalty of exceeding the price
“If you are in deficit you will get paid by the tariff or not at all. There is no borrowing or handouts if you are in trouble”
There is a “definite threat that struggling Trusts will not be bailed out by the government if they fail under the new financial regime”
CENTRE FOR HEALTH ECONOMICS

Some more questions
• Do we know which Trusts are more efficient than others?
• Do we know how much it costs to treat different patients?
• Are there good reasons why costs differ across the country?
CENTRE FOR HEALTH ECONOMICS

Is variation in the RCI due to inefficiency?Estimated efficiency and 95% confidence intervals
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Trust x mean efficiency
95% confidence interval
CENTRE FOR HEALTH ECONOMICS

Proportion of income from PbR
England• 100% by
2007/08
Elsewhere• Germany 100%• Portugal & Spain 30%• Ireland 20%• Denmark 10%• Norway 40 / 60%• Australia 50 / 70%• US < 30%
CENTRE FOR HEALTH ECONOMICS
Co-operation or Competition?
• “The market forced NHS organisations to compete against each other even when it would have been better to cooperate.
• Some were unwilling to share best practice that might benefit a wider range of patients in case they forfeited competitive advantage” (p13/14, The New NHS)
CENTRE FOR HEALTH ECONOMICS





























