Embed Size (px)
Citation preview
Co-Existence of Cutaneous T-Cell Lymphoma and BHairy Cell Leukemia
Rossella Paolini, 1 Alessandro Poletti, 2 Emilio Ramazzina, 1 Chiara Menin, 3,4
Maria Santacatterina, 4 Marco Montagna, 4 Laura Bonaldi, 4 Annarosa Del Mistro, 5
Sergio Zamboni, 1 and Emma D’Andrea 4*1Divisione di Medicina, Ospedale di Rovigo, Rovigo, Italy
2Servizio di Anatomia Patologica I, Azienda Ospedaliera di Padova, Padova, Italy3IST, Sezione di Biotecnologie, Universita di Padova, Italy
4Dipartimento di Scienze Oncologiche e Chirurgiche, Sezione di Oncologia, CIRC, Universita di Padova, Padova, Italy5Servizio di Citologia Diagnostica, Azienda Ospedaliera di Padova, Padova, Italy
A primary cutaneous form of peripheral T-cell lymphoma (PTCL) and a low grade B-cellnon-Hodgkin’s lymphoma that was classified as a variant of hairy cell leukemia (HCL)were simultaneously diagnosed in a 79-year-old woman by both phenotypic and geno-typic analyses. The coexistence of a T- and B-cell lymphoma in the same patient is rare,and, to our knowledge, this particular association has not been previously described. Thepatient was referred to our Department for evaluation of multiple cutaneous itchy, reddishplaques; laboratory analyses disclosed a lymphocytosis, that presented 6 years earlier.A bone marrow aspirate showed a 50% B-cell interstitial infiltrate, while a skin biopsysurprisingly revealed a PTCL. Clonality of both neoplastic processes was assessed bySouthern blot analysis. The indolent clinical course of the cutaneous disease, and the lowand stable number of circulating neoplastic T cells supported the diagnosis of a mycosisfungoides (MF)-like PTCL. Possible oncogenic events and/or putative underlying viralinfections which could have played a role in the occurrence of B- and T-cell non-Hodgkin’s lymphomas in the same patient are discussed. Am. J. Hematol. 64:197–202,2000. © 2000 Wiley-Liss, Inc.
Key words: hairy cell leukemia; peripheral T-cell lymphoma; semi-nested PCR; Southernblot analysis
INTRODUCTION
Hairy cell leukemia (HCL) is a rare lymphoprolifera-tive malignancy accounting for approximately 2% of allleukemias. This chronic B-cell neoplasm is characterizedby pancytopenia, splenomegaly, immunological abnor-malities, and the presence of morphologically distinct“hairy cells” with irregular cytoplasmatic projections inthe blood, bone marrow, liver, spleen, and other tissues.Hairy cells express the usual markers of B-cell lineage,namely CD19, -20, -22, -45RO, and -79a, while they arenegative for CD5, -10, and -23. Moreover they areCD11c, -25, and -103 positive; this last molecule, usuallypresent on mucosal T lymphocytes, is an important di-agnostic marker for HCL [1] and its atypical form, as inthe present case. Before effective therapy was intro-duced, the median survival time of HCL patients wasapproximately 4 years. However, HCL occasionally hasan indolent course, and some patients have lived longer
than 25 years without systemic treatment. A small num-ber of patients, mainly those with smaller spleens, nor-mal blood counts, and few hairy cells in the blood andbone marrow, may survive untreated for long periods. Inour patient, the clinically silent HCL dated back at least6 years and was discovered during evaluation of the pa-tient for multiple cutaneous reddish and itchy plaques,later proven to be a mycosis fungoides (MF)-like periph-eral T-cell lymphoma (PTCL).
Cutaneous PTCL belongs to the group of non-Hodgkin’s lymphomas. The main representatives of
Contract grant sponsor: Italian Association for Cancer Research(AIRC).
*Correspondence to: Dr. Emma D’Andrea, Sezione di Oncologia, ViaGattamelata 64, 35128 Padova, Italy. E-mail: [email protected]
Received for publication 18 March 1999; Accepted 2 February 2000
American Journal of Hematology 64:197–202 (2000)
© 2000 Wiley-Liss, Inc.
PTCL, MF and Sezary syndrome (SS), are non-Hodgkin’s lymphomas with low malignant potential. Thecoexistence of T and B non-Hodgkin’s lymphomas(NHL) in the same patient is rare. Cutaneous T-cell lym-phomas, such as MF and SS, have occasionally beendescribed in association with myeloma [2], B-CLL [3],or other low-grade B-cell NHL [4]. Unusual cases asso-ciated with intermediate grade (centroblastic–centrocytic) lymphoma have also been reported [4]. Wedescribe a rare association between a primary cutaneousform of PTCL and a low-grade B-cell NHL diagnosed asa variant of HCL.
CASE REPORT
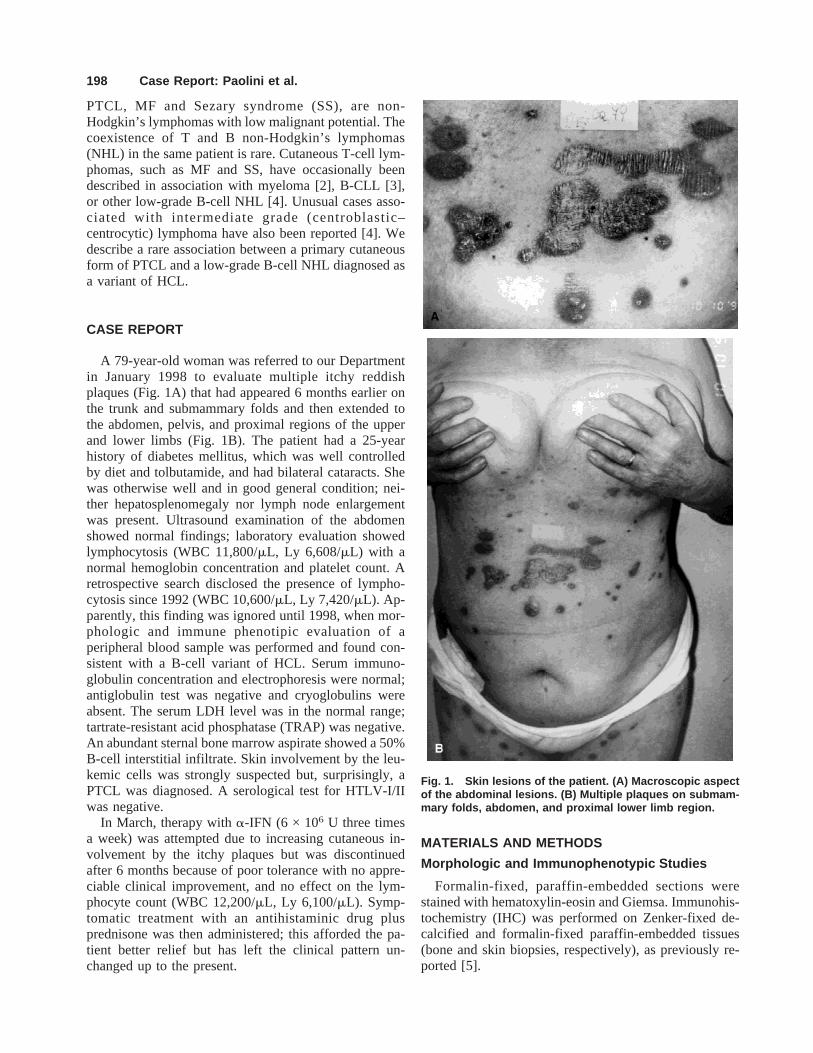
A 79-year-old woman was referred to our Departmentin January 1998 to evaluate multiple itchy reddishplaques (Fig. 1A) that had appeared 6 months earlier onthe trunk and submammary folds and then extended tothe abdomen, pelvis, and proximal regions of the upperand lower limbs (Fig. 1B). The patient had a 25-yearhistory of diabetes mellitus, which was well controlledby diet and tolbutamide, and had bilateral cataracts. Shewas otherwise well and in good general condition; nei-ther hepatosplenomegaly nor lymph node enlargementwas present. Ultrasound examination of the abdomenshowed normal findings; laboratory evaluation showedlymphocytosis (WBC 11,800/mL, Ly 6,608/mL) with anormal hemoglobin concentration and platelet count. Aretrospective search disclosed the presence of lympho-cytosis since 1992 (WBC 10,600/mL, Ly 7,420/mL). Ap-parently, this finding was ignored until 1998, when mor-phologic and immune phenotipic evaluation of aperipheral blood sample was performed and found con-sistent with a B-cell variant of HCL. Serum immuno-globulin concentration and electrophoresis were normal;antiglobulin test was negative and cryoglobulins wereabsent. The serum LDH level was in the normal range;tartrate-resistant acid phosphatase (TRAP) was negative.An abundant sternal bone marrow aspirate showed a 50%B-cell interstitial infiltrate. Skin involvement by the leu-kemic cells was strongly suspected but, surprisingly, aPTCL was diagnosed. A serological test for HTLV-I/IIwas negative.
In March, therapy witha-IFN (6 × 106 U three timesa week) was attempted due to increasing cutaneous in-volvement by the itchy plaques but was discontinuedafter 6 months because of poor tolerance with no appre-ciable clinical improvement, and no effect on the lym-phocyte count (WBC 12,200/mL, Ly 6,100/mL). Symp-tomatic treatment with an antihistaminic drug plusprednisone was then administered; this afforded the pa-tient better relief but has left the clinical pattern un-changed up to the present.
MATERIALS AND METHODS
Morphologic and Immunophenotypic Studies
Formalin-fixed, paraffin-embedded sections werestained with hematoxylin-eosin and Giemsa. Immunohis-tochemistry (IHC) was performed on Zenker-fixed de-calcified and formalin-fixed paraffin-embedded tissues(bone and skin biopsies, respectively), as previously re-ported [5].
Fig. 1. Skin lesions of the patient. (A) Macroscopic aspectof the abdominal lesions. (B) Multiple plaques on submam-mary folds, abdomen, and proximal lower limb region.
198 Case Report: Paolini et al.

Molecular Studies
Tumor tissues were also analysed by Southern blotwith human immune receptor and Epstein-Barr virus spe-cific probes, as described [6]. The semi-nested polymer-ase chain reaction (PCR) approach for the detection ofclonal VH-DH-JH junctional rearrangements was appliedto tumor sample DNA; amplified fragments were thenseparated by denaturing polyacrylamide gel electropho-resis. EBNA 2 specific PCR on tumor sample DNA wasperformed as previously described [7].
RESULTS
Immune Phenotyping and Histopathology
At the light microscope, the peripheral lymphocytesappeared as small round cells with a bean-shapednucleus, and at times an abundant cytoplasm with “hairy”projections (Fig. 2A). A few lymphocytes had a cerebri-form nucleus, similar to “atypical” monocytoid cells(Fig. 2B). Immune phenotyping of the peripheral lym-phocytes disclosed a dominant population of monoclonal(CD19+ and CD103+) B cells expressing high-densitysurface immunoglobulins restricted to thel light chain;CD5 and CD25 were negative, thus suggesting a variantof HCL. On the other hand, a T-cell phenotype for the“atypical” monocytoid cells was confirmed by immunephenotyping of the peripheral smear; these neoplasticT-cells represented less than 1% of the circulating lym-phocytes.
A bone marrow aspirate and biopsy showed a hyper-cellular pattern, with a 50% lymphoid interstitial infil-trate; a slight and focal increase in reticulin was alsoobserved. The neoplastic cells expressed CD45 andCD20, while only few cells were DBA 44 positive, atvariance with the classical form of HCL.
A skin biopsy showed the presence of a rich lymphoidinfiltrate prevalently located in the superficial and reticu-lar derma (Fig. 2C); however, at high power, small in-tradermal groups of atypical lymphocytes with convoluteor cerebroid nuclei, inconspicuous nucleoli, and pale cy-toplasm were also observed (Fig. 2D). Phenotypic char-acterization demonstrated a peripheral T-cell phenotype(CD45, CD3, CD4, CD43, CD45RO positive; CD8,TIA1, Granzyme-B, Perforin, CD20, CD30 negative). Asan example, specific staining for CD45RO is presented inFigures 2E and F.
Molecular Characterization
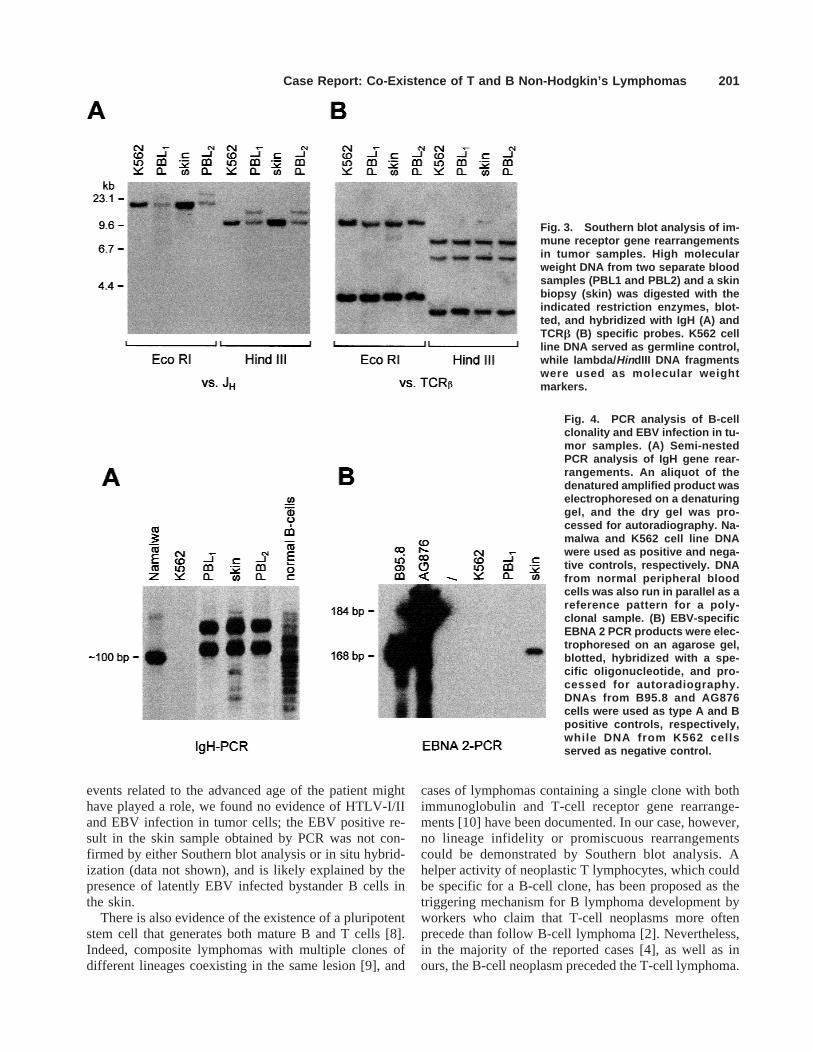
Southern blot analysis of the DNA from two bloodsamples collected at 3 month intervals (PBL-1 and PBL-2) disclosed superimposable patterns of IgH gene rear-rangement, thus suggesting the presence of the sameclonal B-cell subpopulation in both samples, while DNAfrom the skin biopsy was found in the germline configu-
ration (Fig. 3A). The opposite result was obtained usingthe TCRb specific probe because a rearranged band wasdetected only in the skin biopsy, while DNA from bothblood samples presented the same germline pattern as theDNA of control K562 cells (Fig. 3B).
To better ascertain the persistence of the same clonalB-cell population in peripheral blood, tumor sampleswere analyzed by a semi-nested PCR approach. Asshown in Fig. 4A, comigrating bands could be detectedin both blood samples. Surprisingly, identical bands wereamplified from skin DNA, suggesting the presence ofrare clonal B cells, that could not be detected by Southernblot analysis; this latter finding could be due to the veryhigh sensitivity of the PCR approach.
Finally, the presence of EBV specific sequences wasanalyzed by both Southern blot and PCR methods: usinga terminal repeat specific probe, neither linear (replica-tive), nor episomal (latent) EBV genomes could be de-tected in any of the patient’s samples (data not shown),while an amplified EBV type A EBNA 2A fragment wasobserved only in the skin (Fig. 4B).
DISCUSSION
Our patient presented with multiple, reddish, itchyplaques on an otherwise normal skin; no extracutaneousinvolvement was apparent in accordance with the diag-nosis of primary cutaneous T-cell lymphoma (PTCL).The presence of sporadic T lymphocytes in the peripheralblood smear, together with the atypical hairy cells, wasfirst suspected on morphological grounds and then con-firmed by immune phenotyping. The low number of cir-culating neoplastic T cells (less than 1%) explains theabsence of clonal TCRb gene rearrangements in the pe-ripheral blood cells. The indolent clinical behavior with-out lymph node involvement in the absence of anyimportant treatment supports the diagnosis of PTCL,MF-like, in agreement with tumor histopathology andimmune phenotype. However, a close follow-up of thecirculating T-cell neoplastic component in this patient ismandatory in order to detect a potential systemic in-volvement as early as possible. We could document thatperipheral lymphocytosis was present 6 years prior to ourobservation, thus suggesting that the B-cell neoplasmpreceded the cutaneous T-cell lymphoma. Morphologicaland immune phenotypic patterns defined the B-cell pro-liferation as a variant of HCL; the absence of splenomeg-aly, the lack of a “dry tap” and the low expression ofCD25 and DBA44 were consistent with this diagnosis.
The occurrence of both B- and T-cell lymphomas inone patient may merely be coincidental. Nevertheless,possible explanations for such a condition can be ad-vanced, such as genetic predisposition for lymphoprolif-erative diseases, underlying viral infections, and possiblemutagenic effects of cytostatic drugs. While oncogenic
Case Report: Co-Existence of T and B Non-Hodgkin’s Lymphomas 199
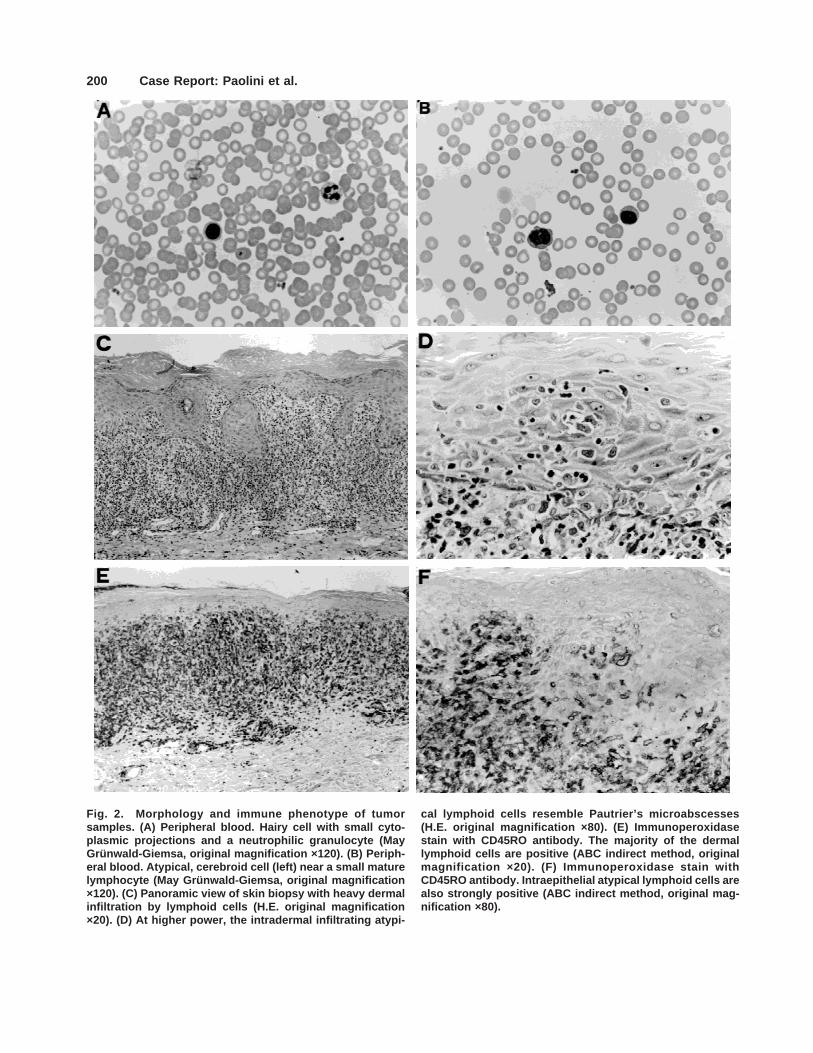
Fig. 2. Morphology and immune phenotype of tumorsamples. (A) Peripheral blood. Hairy cell with small cyto-plasmic projections and a neutrophilic granulocyte (MayGrunwald-Giemsa, original magnification ×120). (B) Periph-eral blood. Atypical, cerebroid cell (left) near a small maturelymphocyte (May Gru ¨ nwald-Giemsa, original magnification×120). (C) Panoramic view of skin biopsy with heavy dermalinfiltration by lymphoid cells (H.E. original magnification×20). (D) At higher power, the intradermal infiltrating atypi-
cal lymphoid cells resemble Pautrier’s microabscesses(H.E. original magnification ×80). (E) Immunoperoxidasestain with CD45RO antibody. The majority of the dermallymphoid cells are positive (ABC indirect method, originalmagnification ×20). (F) Immunoperoxidase stain withCD45RO antibody. Intraepithelial atypical lymphoid cells arealso strongly positive (ABC indirect method, original mag-nification ×80).
200 Case Report: Paolini et al.
events related to the advanced age of the patient mighthave played a role, we found no evidence of HTLV-I/IIand EBV infection in tumor cells; the EBV positive re-sult in the skin sample obtained by PCR was not con-firmed by either Southern blot analysis or in situ hybrid-ization (data not shown), and is likely explained by thepresence of latently EBV infected bystander B cells inthe skin.
There is also evidence of the existence of a pluripotentstem cell that generates both mature B and T cells [8].Indeed, composite lymphomas with multiple clones ofdifferent lineages coexisting in the same lesion [9], and
cases of lymphomas containing a single clone with bothimmunoglobulin and T-cell receptor gene rearrange-ments [10] have been documented. In our case, however,no lineage infidelity or promiscuous rearrangementscould be demonstrated by Southern blot analysis. Ahelper activity of neoplastic T lymphocytes, which couldbe specific for a B-cell clone, has been proposed as thetriggering mechanism for B lymphoma development byworkers who claim that T-cell neoplasms more oftenprecede than follow B-cell lymphoma [2]. Nevertheless,in the majority of the reported cases [4], as well as inours, the B-cell neoplasm preceded the T-cell lymphoma.
Fig. 3. Southern blot analysis of im-mune receptor gene rearrangementsin tumor samples. High molecularweight DNA from two separate bloodsamples (PBL1 and PBL2) and a skinbiopsy (skin) was digested with theindicated restriction enzymes, blot-ted, and hybridized with IgH (A) andTCRb (B) specific probes. K562 cellline DNA served as germline control,while lambda/ HindIII DNA fragmentswere used as molecular weightmarkers.
Fig. 4. PCR analysis of B-cellclonality and EBV infection in tu-mor samples. (A) Semi-nestedPCR analysis of IgH gene rear-rangements. An aliquot of thedenatured amplified product waselectrophoresed on a denaturinggel, and the dry gel was pro-cessed for autoradiography. Na-malwa and K562 cell line DNAwere used as positive and nega-tive controls, respectively. DNAfrom normal peripheral bloodcells was also run in parallel as areference pattern for a poly-clonal sample. (B) EBV-specificEBNA 2 PCR products were elec-trophoresed on an agarose gel,blotted, hybridized with a spe-cific oligonucleotide, and pro-cessed for autoradiography.DNAs from B95.8 and AG876cells were used as type A and Bpositive controls, respectively,while DNA from K562 cellsserved as negative control.
Case Report: Co-Existence of T and B Non-Hodgkin’s Lymphomas 201

Small T-cell clones were identified in 3 of 13 patientswith B-CLL [11]. Since the malignant B-cells of B-CLLare, as in HCL, well differentiated, they may secretecytokines or other factors that could chronically stimu-late T-cells, thus increasing the risk for the emergence ofa T-cell clone. These clonal T-cells in turn could undergoadditional genetic alterations, that might lead to malig-nant transformation with development of a T-cell lym-phoma. Similar mechanisms could explain the excep-tional development of a high grade T-cell lymphoma inpatients with B-cell CLL [12], and the development ofPTCL in this patient with HCL. An impaired T-cell func-tioning, namely a decrease number of CD4+ CD45RO+cells, can occur in the course of HCL, and it might berelated to the frequent occurrence of opportunistic infec-tions in these patients [13,14]. Since this T-cell subsetplays an important role in tumor invasion [15], its deple-tion could further explain the emergence of a secondmalignancy; interestingly, in our HCL patient, clonal T-cells express precisely this phenotype.
ACKNOWLEDGMENTS
This work was supported in part by grants from theItalian Association for Cancer Research (AIRC);MURST 40% and 60%. We thank Mrs. M. Quaggio andMrs. D. Zullato for technical assistance, Mrs. P. Segatoand Mrs. A. Tomasi for help in preparing the manuscript,and Mr. P. Gallo for artwork. MS and MM are supportedby FIRC and AIRC fellowships, respectively.
REFERENCES
1. Harris NL, Jaffe ES, Stein H, Banks PM, Chan JKC, Cleary ML,Delsol G, De Wolf-Peeters C, Falini B, Gatter KC, Grogan TM, Isaac-son PJ, Knowles DM, Mason DY, Muller-Hermelink H-K, Pileri SA,Piris MA, Ralfkiaer E, Warnke RA. A revised European-Americanclassification of lymphoid neoplasms: a proposal from the interna-tional study group. Blood 1994;84:1361–1392.
2. Bryant E, Ronan SG, Iossifedes IA. Plasma cell myeloma in a patientwith cutaneous T-cell lymphoma. Cancer 1982;50:2122–2125.
3. Sheibani K, Forman SJ, Winberg CD, Rappaport H. Coincidence ofB-cell chronic lymphocytic leukemia and cutaneous T-cell lymphoma
(mycosis fungoides): immunologic characterization by monoclonal an-tibodies. Blood 1983;62:1176–1181.
4. Grange F, Avril MF, Esteve E, Joly P, Bosq J, De Murets A, ThomineE, Ortoli J-C, Duvillard P, Vaillant L, Bagot M, Wechsler J, and theFrench Study Group on Cutaneous Lymphomas. Coexistent cutaneousT-cell lymphoma and B-cell malignancy. J Am Acad Dermatol 1994;31:724–731.
5. Poletti A, Giacon C, Pennelli N. Simultaneous visualization of immu-nodetected antigens and tissue components revealed by non-enzymatichistochemical stains. J Histochem Cytochem 1992;40:1965–1970.
6. Strazzabosco M, Corneo B, Iemmolo RM, Menin C, Gerunda G, Bon-aldi L, Merenda R, Neri D, Poletti A, Montagna M, Del Mistro A,Maffei-Faccioli A, D’Andrea E. Epstein–Barr virus-associated post-transplant lympho-proliferative disease of donor origin in liver trans-plant recipients. J Hepatol 1997;26:926–934.
7. Menin C, Ometto L, Veronesi A, Montagna M, Coppola V, VeroneseML, Indraccolo S, Bruni L, Corneo B, Amadori A, De Rossi A,Chieco-Bianchi L, D’Andrea E. Dominance of a single Epstein–Barrvirus strain in SCID-mouse tumors induced by injection of peripheralblood mononuclear cells from healthy human donors. Virus Res 1995;36:215–231.
8. Greaves MF, Chan LC, Furley AJW, Watt SM, Molgaard HV. Lineagepromiscuity in hemopoietic differentiation and leukemia. Blood 1986;67:1–11.
9. York JC, Cousar JB, Glick AD, Flexner JM, Stein R, Collins RD.Morphologic and immunologic evidence of composite B- and T-celllymphomas: a report of three cases developing in follicular center celllymphomas. Am J Clin Pathol 1985;84:35–43.
10. Biondi A, Di Celle PF, Rossi V, Casorati G, Matullo G, Giudici G, FoaR, Migone N. High prevalence of T-cell receptor Vd2-(D)-Dd3 or Dd1/2-Dd3 rearrangements in B-precursor acute lymphoblastic leuke-mias. Blood 1990;75:1834–1840.
11. Wen T, Mellstedt H, Jondal M. Presence of clonal T-cell populationsin chronic B lymphocytic leukemia and smoldering myeloma. J ExpMed 1990;171:659–666.
12. Lee A, Skelly ME, Kingma DW, Medeiros LJ. B-cell chronic lym-phocytic leukemia followed by high grade T-cell lymphoma. Am JClin Pathol 1995;103:348–352.
13. van der Host FAL, van der Marel A, den Ottolander GJ, Kluin-Nelemans HC. Decrease of memory T helper cells (CD4+ CD45RO+)in hairy cell leukemia. Leukemia 1993;7:46–50.
14. Raspadori D, Rondelli D, Birtolo S, Lenoci M, Nardi G, Scalia G,Sestigiani C, Tozzi M, Marotta G, Lauria F. Long-lasting decrease ofCD4+/CD45RA+ T cells in HCL patients after 2-chlorodeoxyadeno-sine (2-CdA) treatment. Leukemia 1999;13:1254–1257.
15. Jacob MC, Favre M, Lemarc’Hadour F, Sotto MF, Bonnefoix T, SottoJJ, Bensa JC. CD45RA expression by CD4 T lymphocytes in tumorsinvaded by B-cell non-Hodgkin’s lymphoma (NHL) or Hodgkin’s dis-ease (HD). Am J Hematol 1992;39:45–51.
202 Case Report: Paolini et al.