Embed Size (px)
Citation preview
CNS MalformationsCNS Malformations
SCOTT KULICH, M.D., Ph.D.RAFAEL MEDINA-FLORES, M.D.
RONALD L. HAMILTON, M.D.Division of Neuropathology
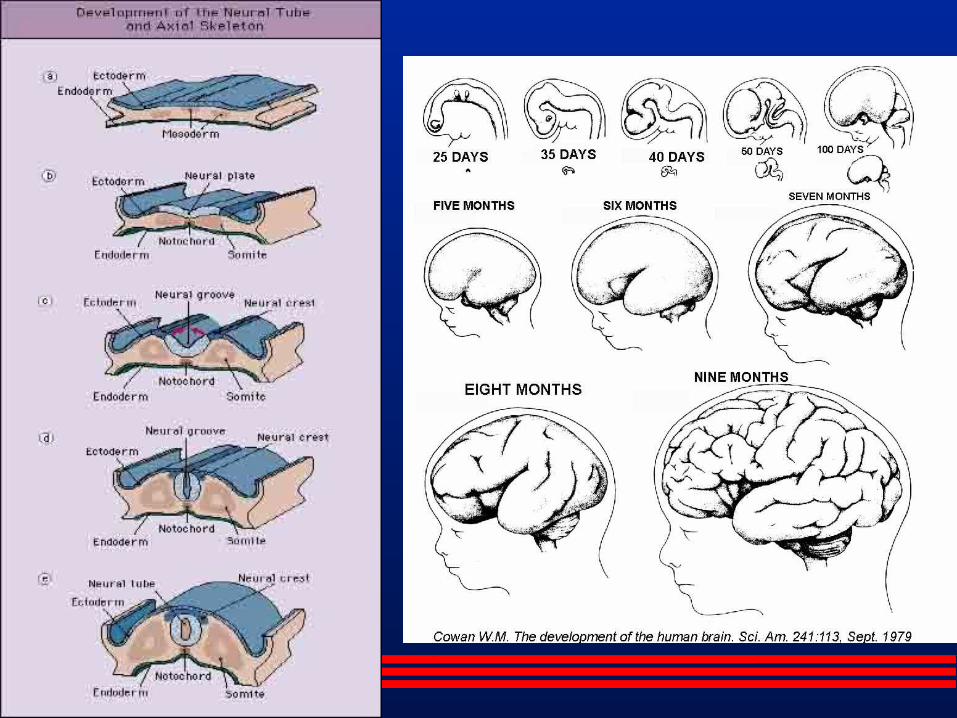
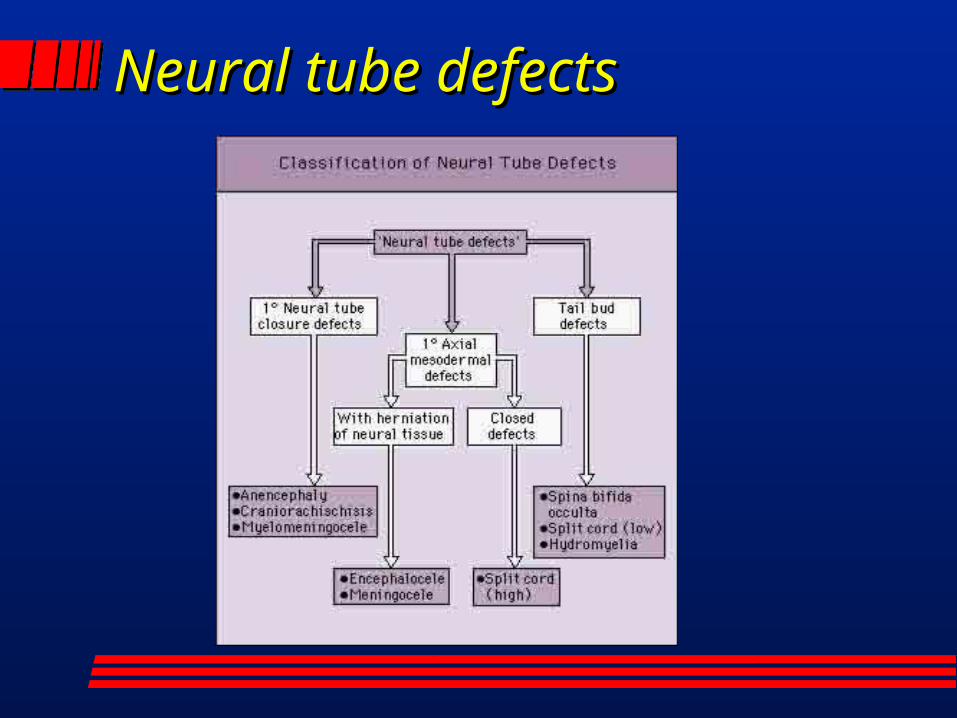
Neural tube defectsNeural tube defects
AnencephalyAnencephaly
Failure of closure of the anterior neuroporeCommon malformationFrog-like faciesArea cerebrovasculosaUnderdeveloped hypothalamusAdrenal cortical hyperplasiaMultifactorial-Folic acid supplementation

AnencephalyAnencephaly

AnencephalyAnencephaly
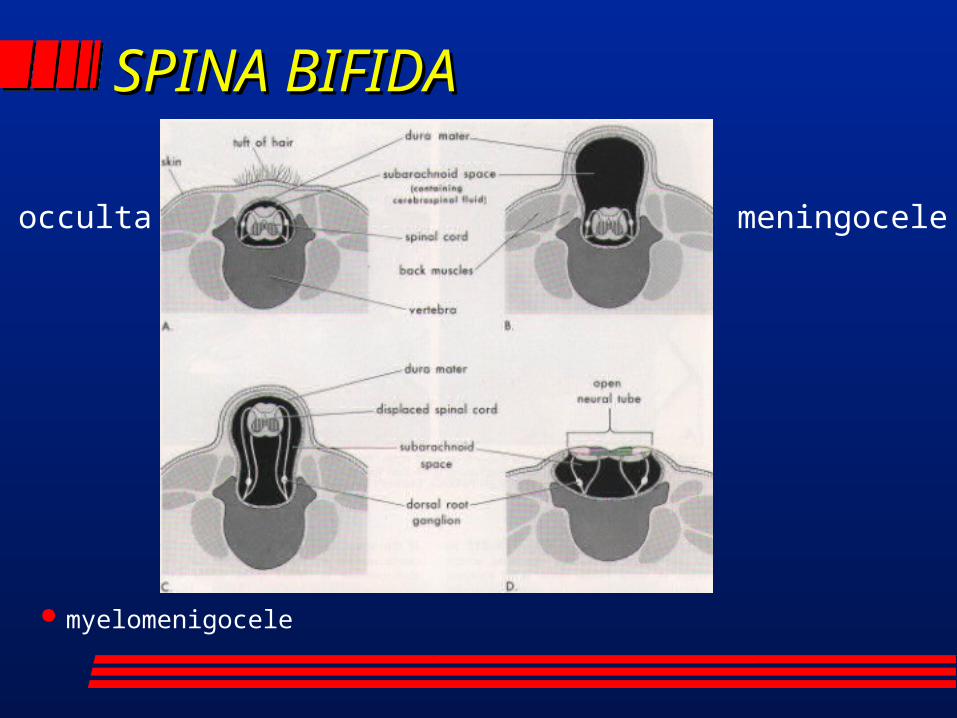
SPINA BIFIDASPINA BIFIDA
myelomenigocele
occulta meningocele
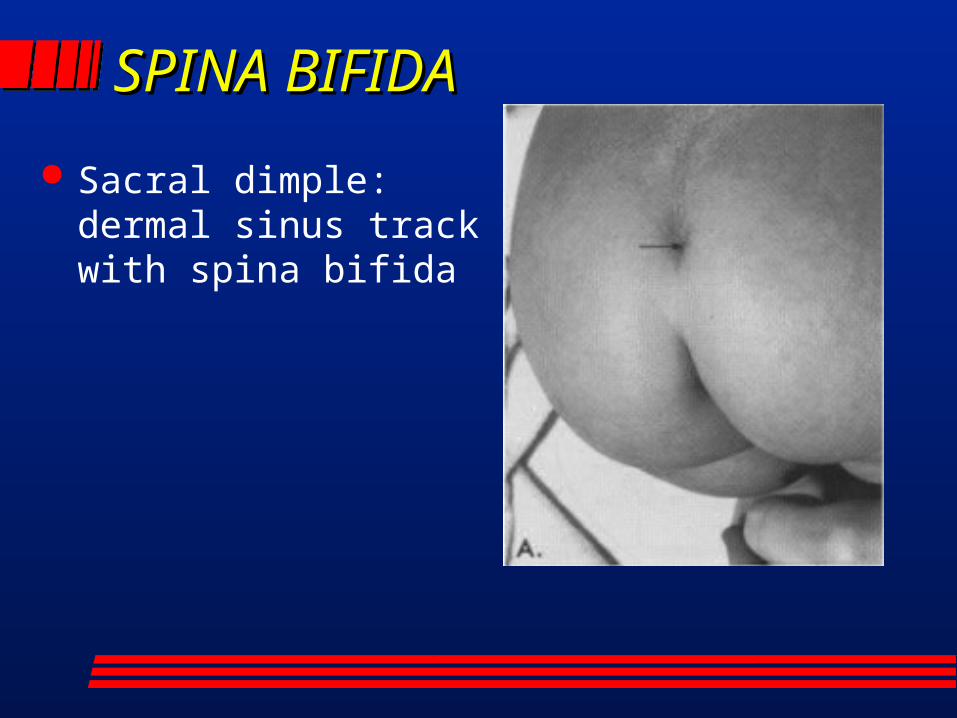
SPINA BIFIDA SPINA BIFIDA
Sacral dimple: dermal sinus track with spina bifida
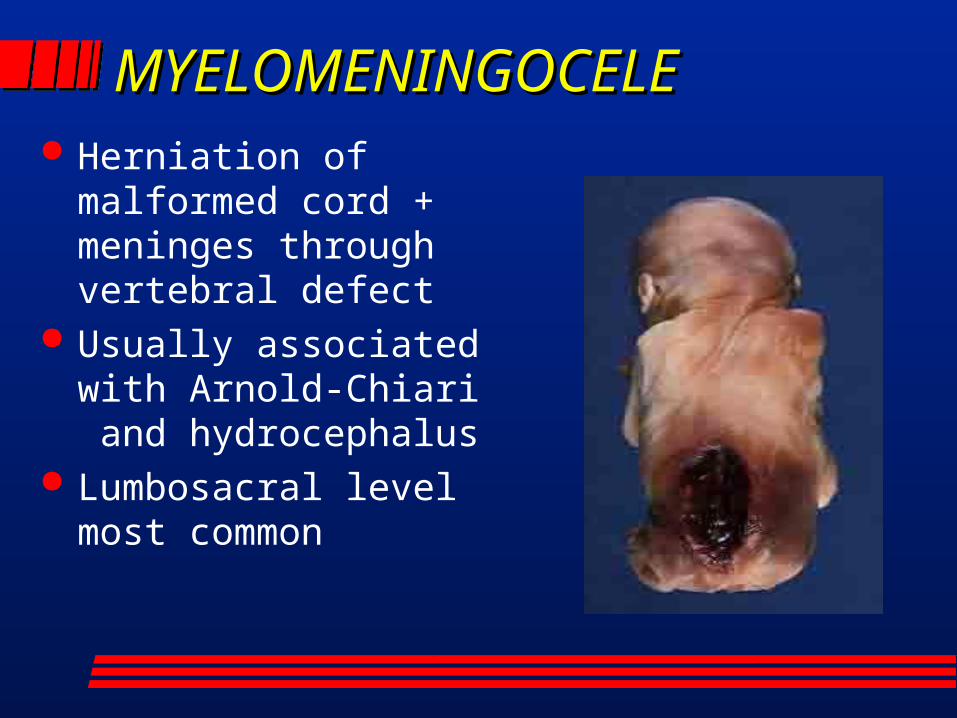
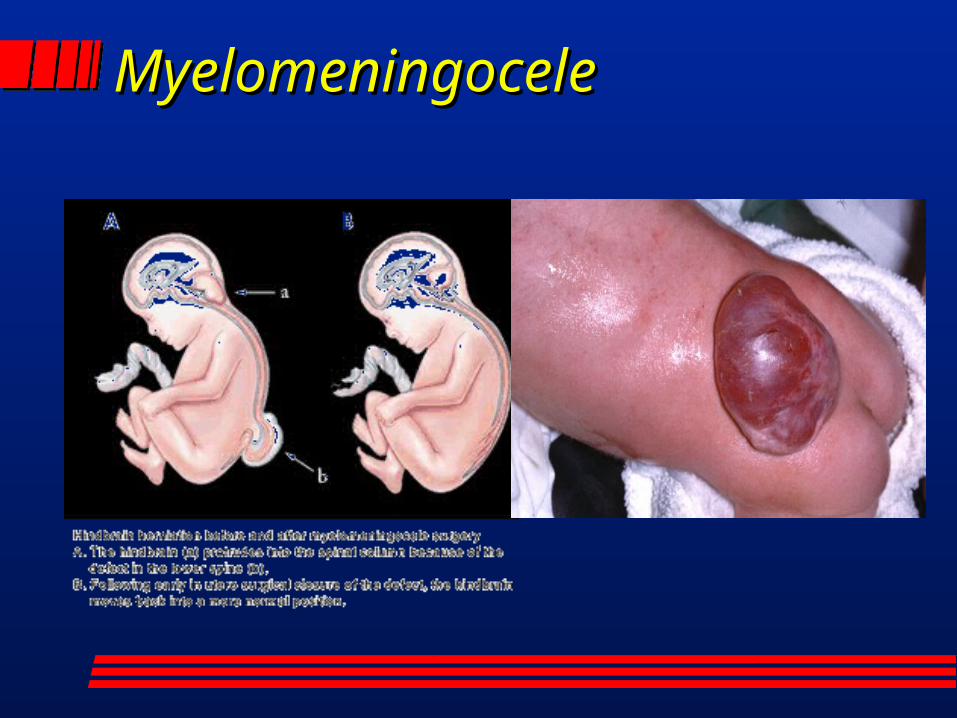
MYELOMENINGOCELEMYELOMENINGOCELE Herniation of
malformed cord + meninges through vertebral defect
Usually associated with Arnold-Chiari and hydrocephalus
Lumbosacral level most common
MyelomeningoceleMyelomeningocele
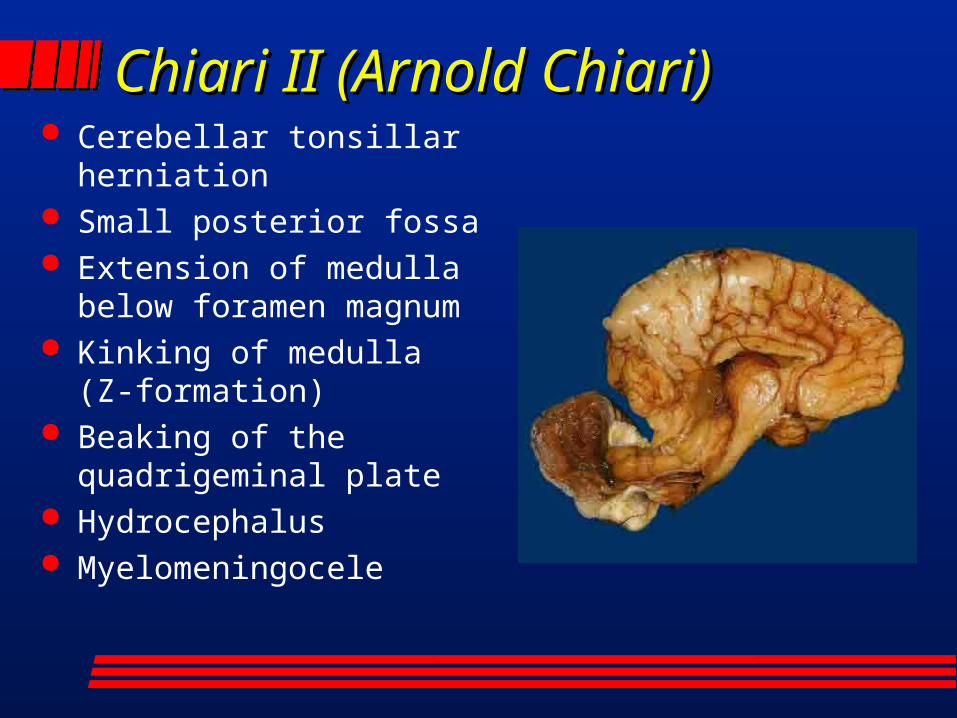
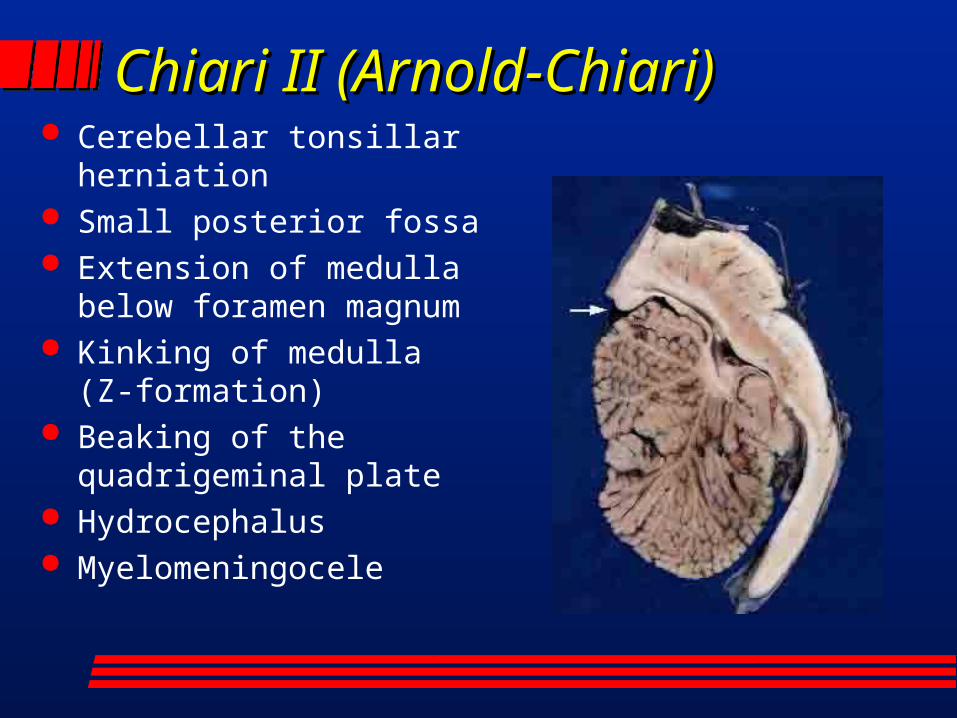
Chiari II (Arnold Chiari)Chiari II (Arnold Chiari) Cerebellar tonsillar
herniation Small posterior fossa Extension of medulla
below foramen magnum Kinking of medulla (Z-
formation) Beaking of the
quadrigeminal plate Hydrocephalus Myelomeningocele
Chiari II (Arnold-Chiari)Chiari II (Arnold-Chiari) Cerebellar tonsillar
herniation Small posterior fossa Extension of medulla
below foramen magnum Kinking of medulla (Z-
formation) Beaking of the
quadrigeminal plate Hydrocephalus Myelomeningocele
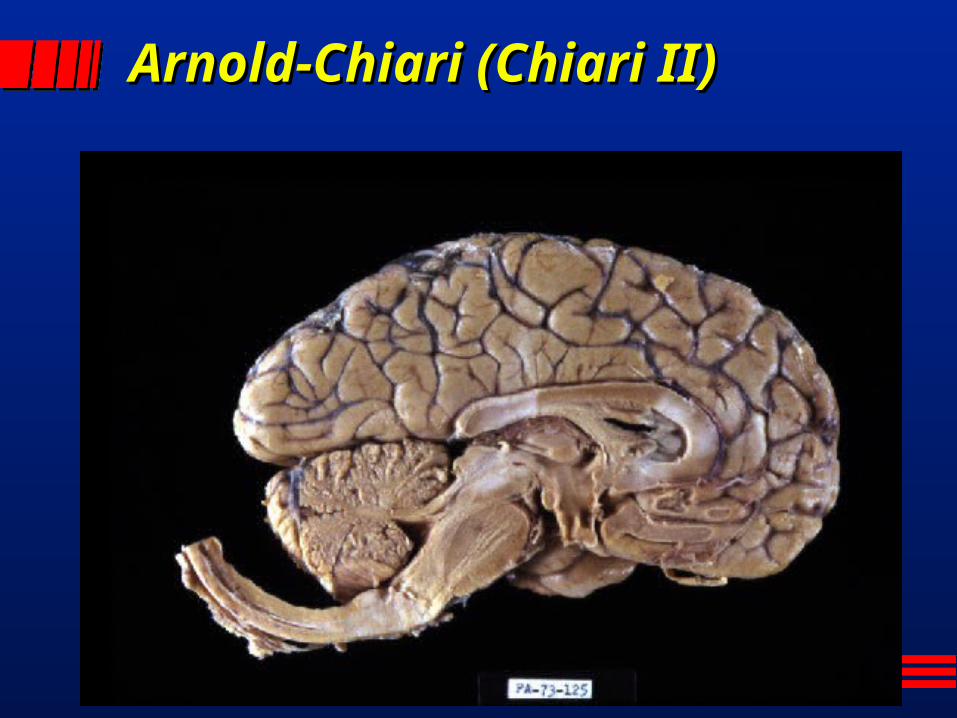
Arnold-Chiari (Chiari II)Arnold-Chiari (Chiari II)
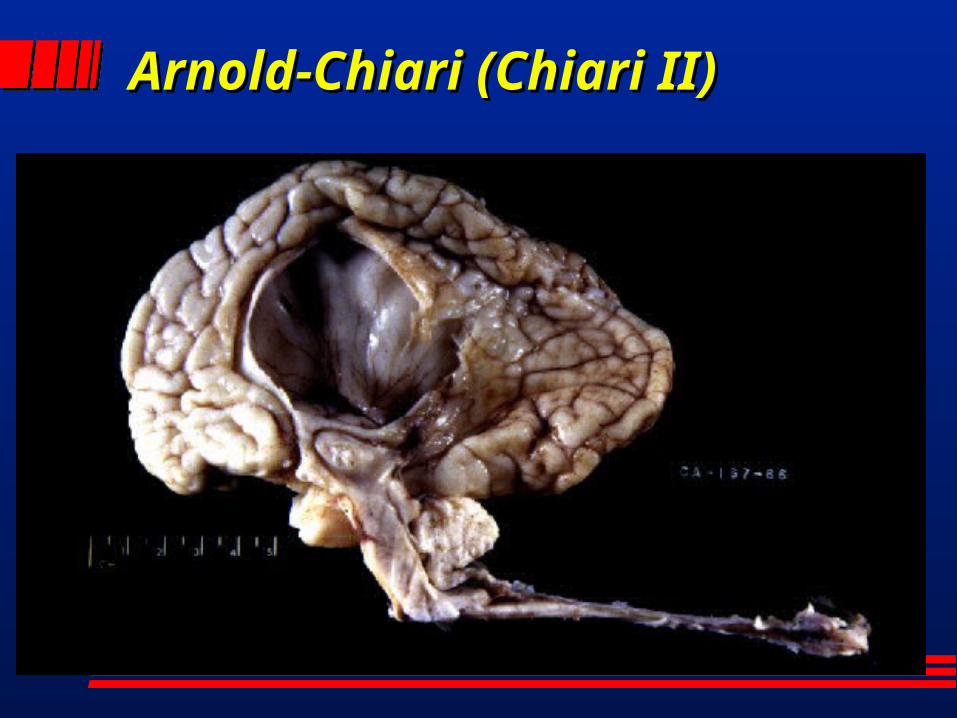
Arnold-Chiari (Chiari II)Arnold-Chiari (Chiari II)
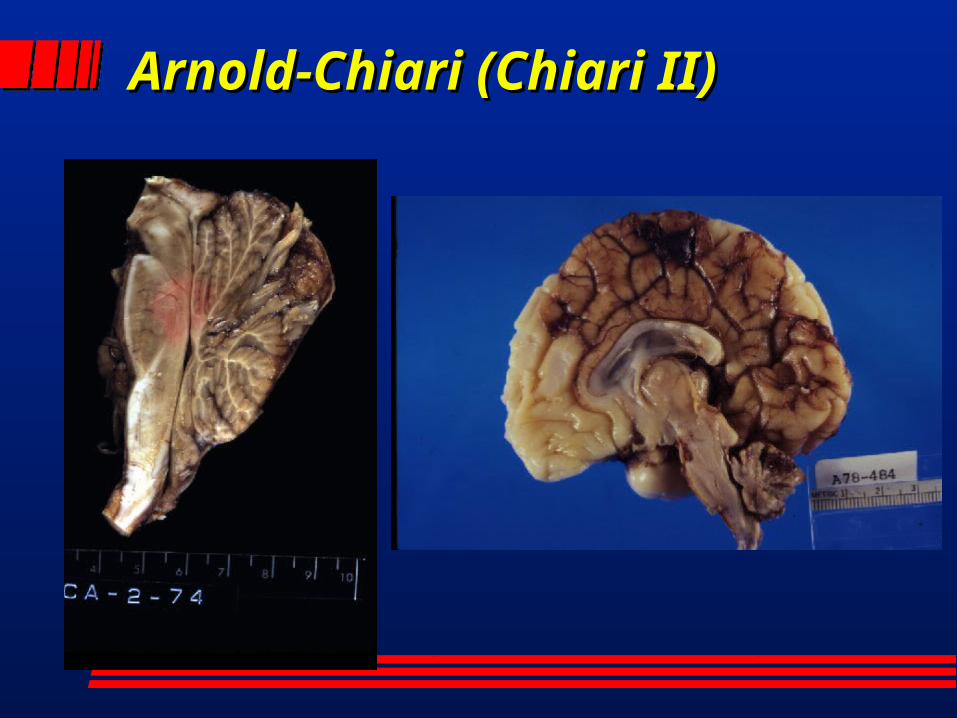
Arnold-Chiari (Chiari II)Arnold-Chiari (Chiari II)
Chiari I MalformationChiari I Malformation
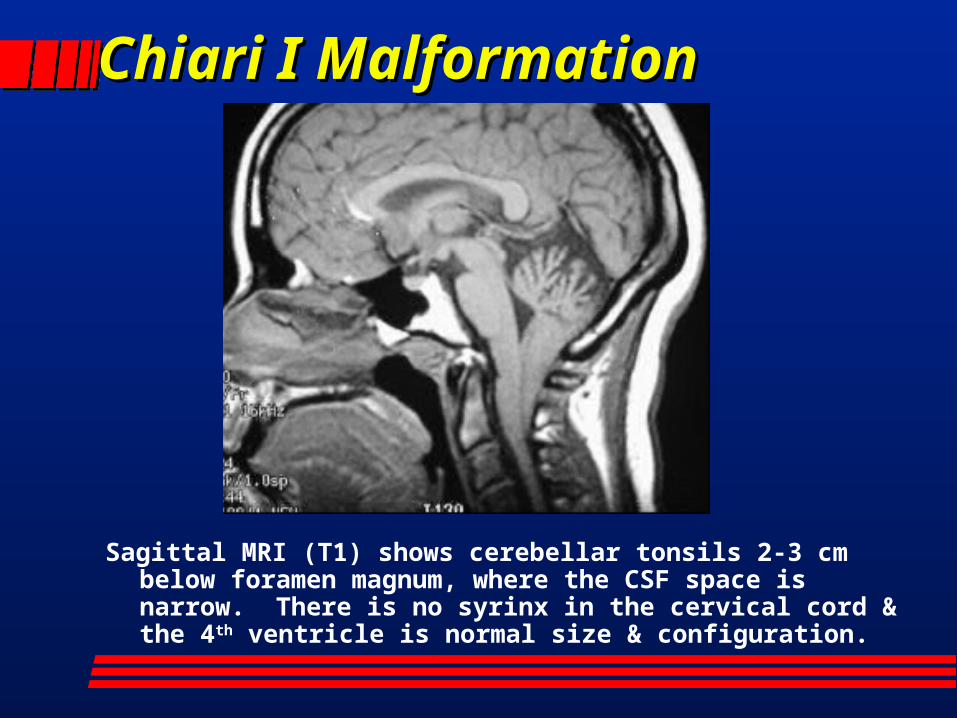
Sagittal MRI (T1) shows cerebellar tonsils 2-3 cm below foramen magnum, where the CSF space is narrow. There is no syrinx in the cervical cord & the 4th ventricle is normal size & configuration.
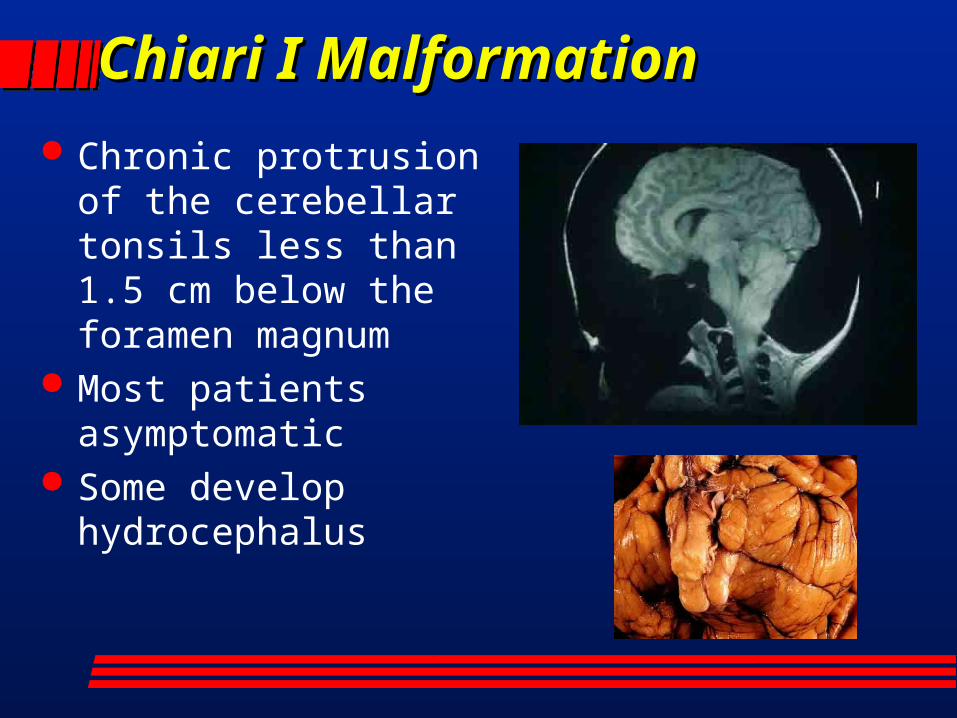
Chiari I MalformationChiari I Malformation Chronic protrusion of
the cerebellar tonsils less than 1.5 cm below the foramen magnum
Most patients asymptomatic
Some develop hydrocephalus
Dandy-Walker MalformationDandy-Walker Malformation
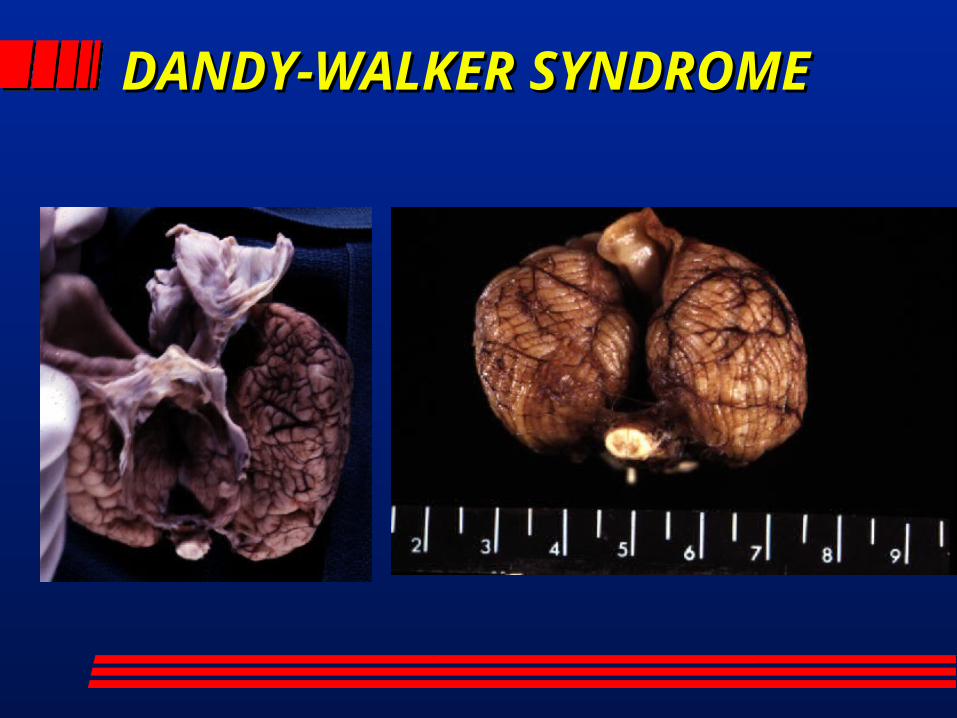
Dandy-Walker syndrome– Agenesis of cerebellar vermis– cystic dilatation of 4th venticle– enlargement of posterior fossa– Variable clinical manifestations– Hypothesized to result from arrest of
cerebellar development prior to the 3rd month
DANDY-WALKER DANDY-WALKER SYNDROMESYNDROME
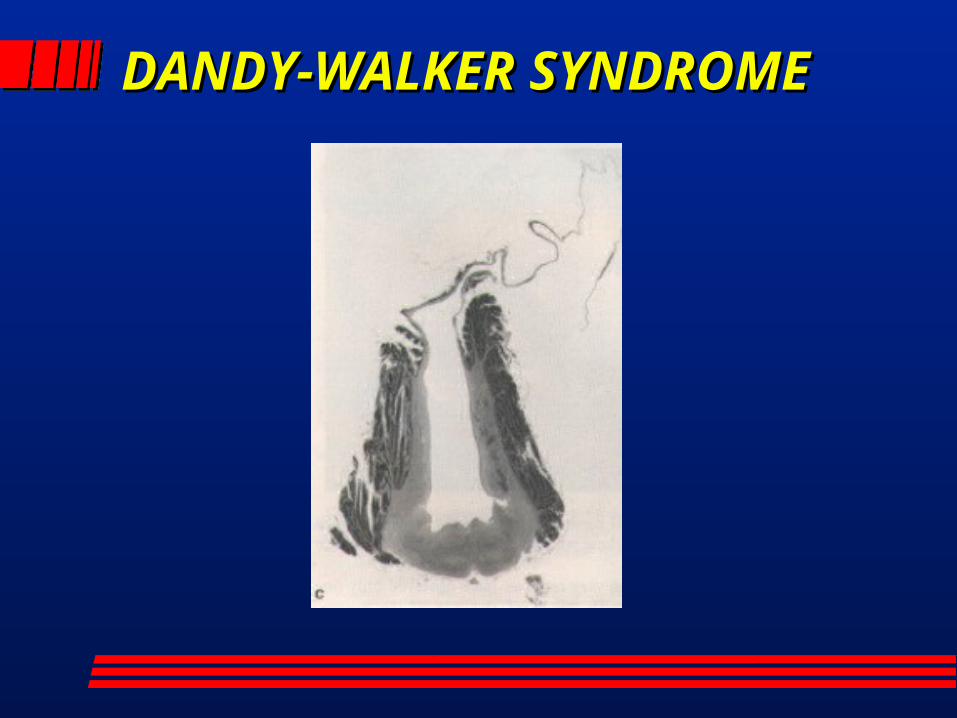
DANDY-WALKER DANDY-WALKER SYNDROMESYNDROME
CEREBELLAR MALFORMATIONS: CEREBELLAR MALFORMATIONS: VERMIAN (PALEOCEREBELLUM)VERMIAN (PALEOCEREBELLUM)
Joubert syndrome– Clinical manifestations include episodic
hyperpnea, ataxia, eye movement abnormalities, and MR
– Familial – Agenesis of vermis, cystic dilatation of 4th
venticle (but less than DWS)– Microscopically normal cerebellar cortex
with numerous subcortical heterotopias
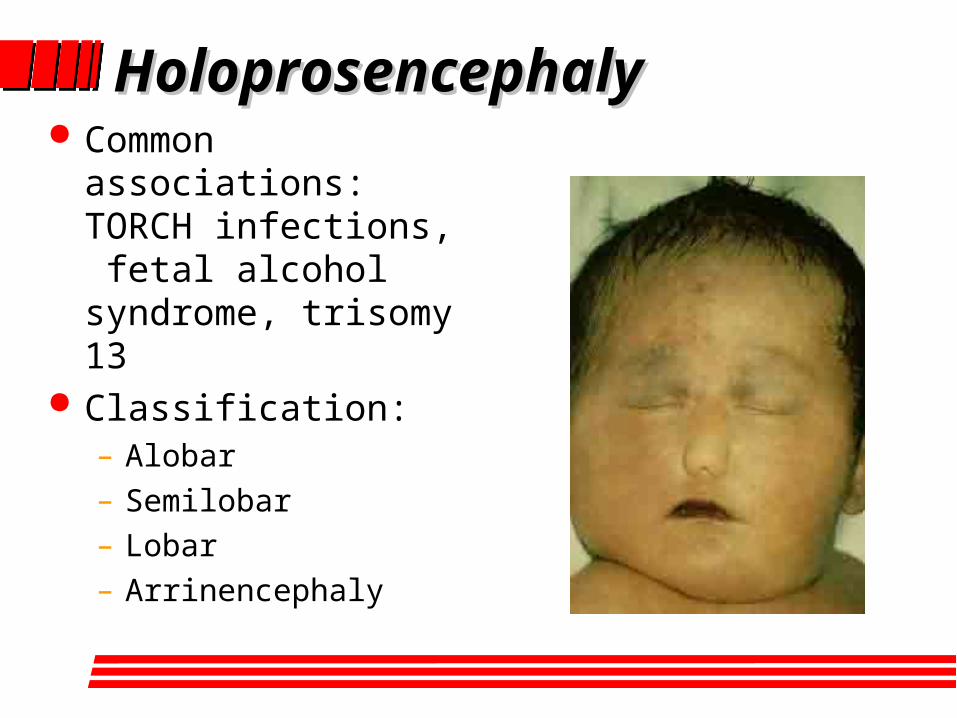
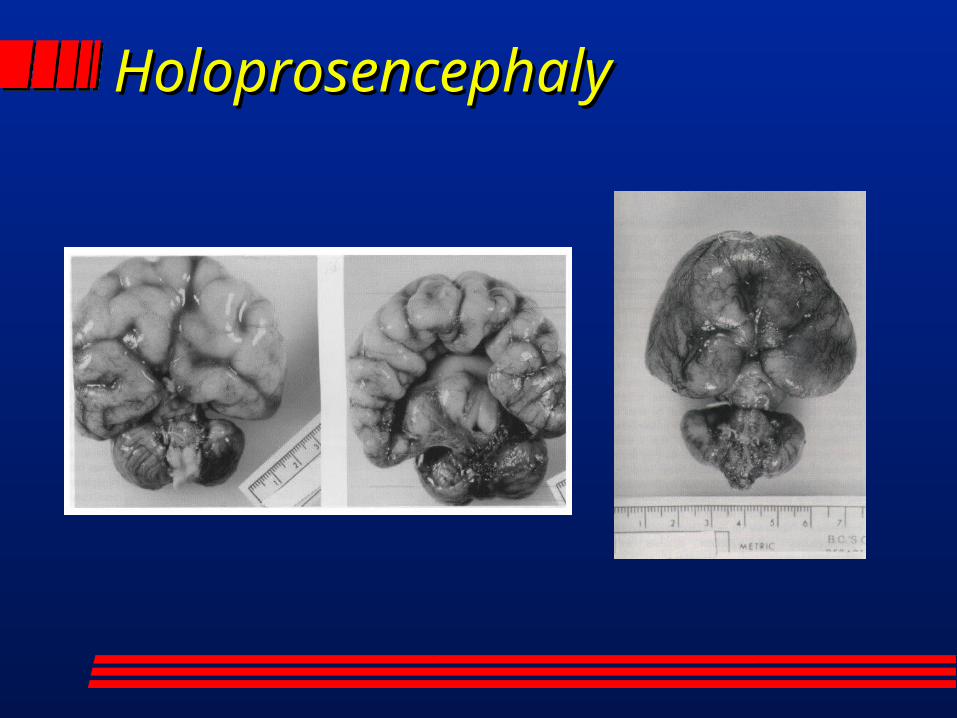
HoloprosencephalyHoloprosencephaly Common
associations: TORCH infections, fetal alcohol syndrome, trisomy 13
Classification:– Alobar– Semilobar– Lobar– Arrinencephaly
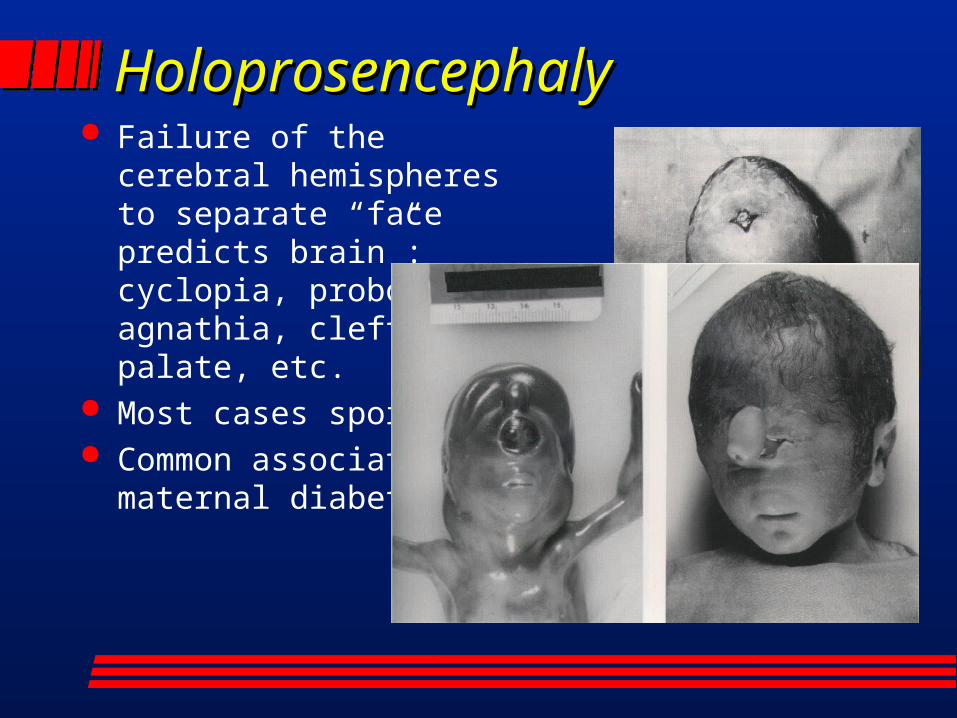
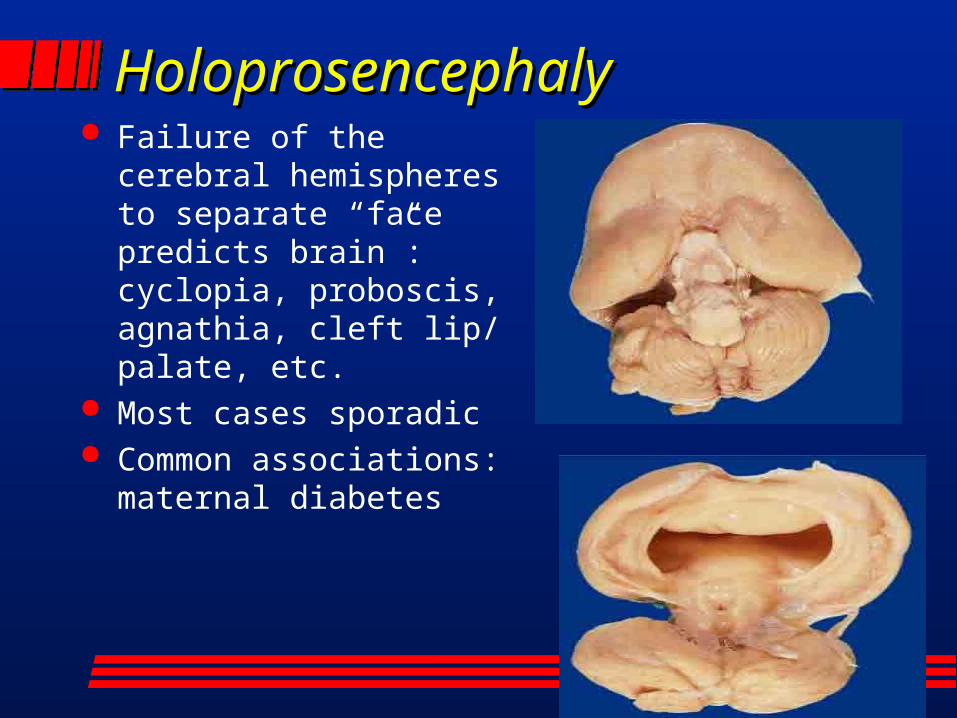
HoloprosencephalyHoloprosencephaly Failure of the cerebral
hemispheres to separate “face predicts brain”: cyclopia, proboscis, agnathia, cleft lip/ palate, etc.
Most cases sporadic Common associations:
maternal diabetes
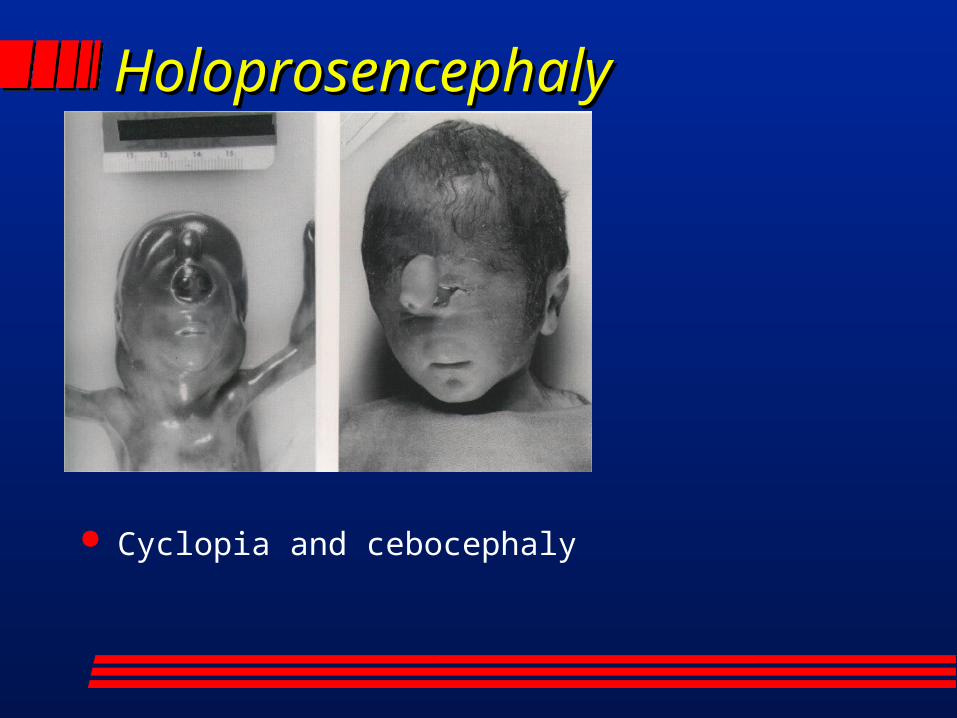
HoloprosencephalyHoloprosencephaly
Cyclopia and cebocephaly
HoloprosencephalyHoloprosencephaly Failure of the cerebral
hemispheres to separate “face predicts brain”: cyclopia, proboscis, agnathia, cleft lip/ palate, etc.
Most cases sporadic Common associations:
maternal diabetes
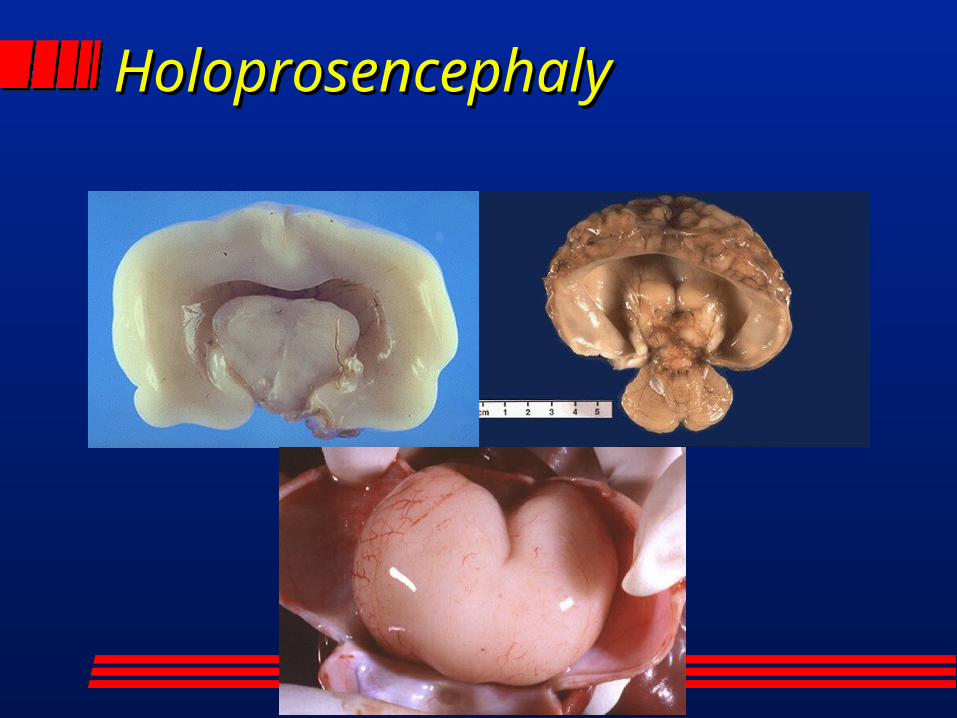
HoloprosencephalyHoloprosencephaly
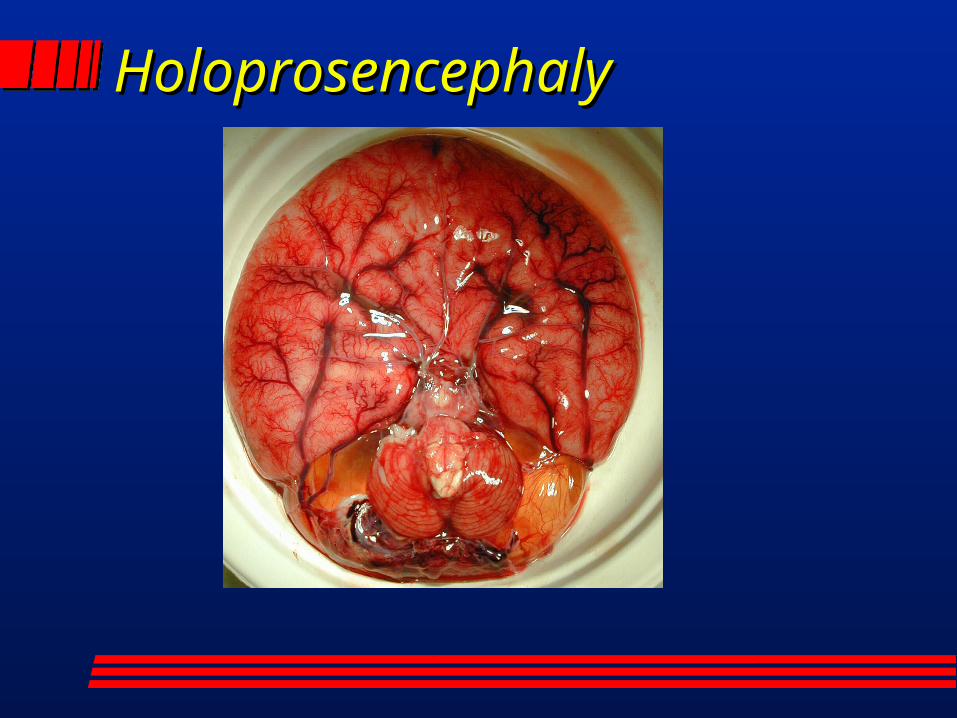
HoloprosencephalyHoloprosencephaly
HoloprosencephalyHoloprosencephaly
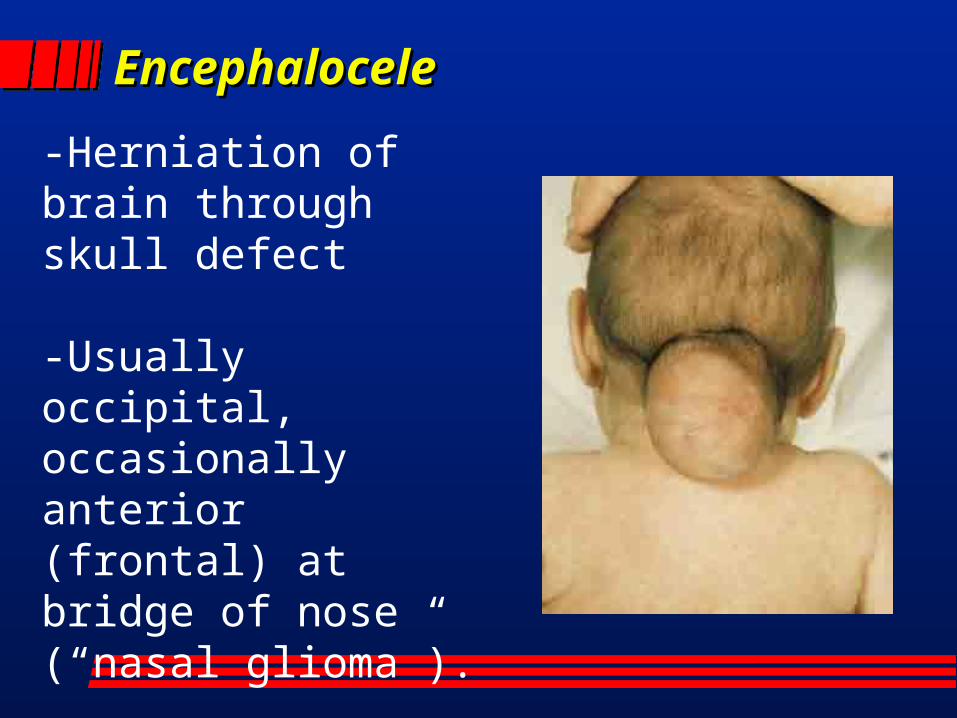
EncephaloceleEncephalocele
-Herniation of brain through skull defect
-Usually occipital, occasionally anterior (frontal) at bridge of nose (“nasal glioma”).
-Asymmetric with overlying ulceration
AGENESIS OF CORPUS AGENESIS OF CORPUS CALLOSUMCALLOSUM May be total or partial – Partial usually affects posterior
(splenium) May be sporadic or syndromic
– Acardi (infantile spasms, MR, polymicrogyria)
– Andermann (sensorimotor neuropathy, dysmorphic features)
– Meckel-Gruber (occipital encephalocele, liver/kidney abnl)
May be clinically silent
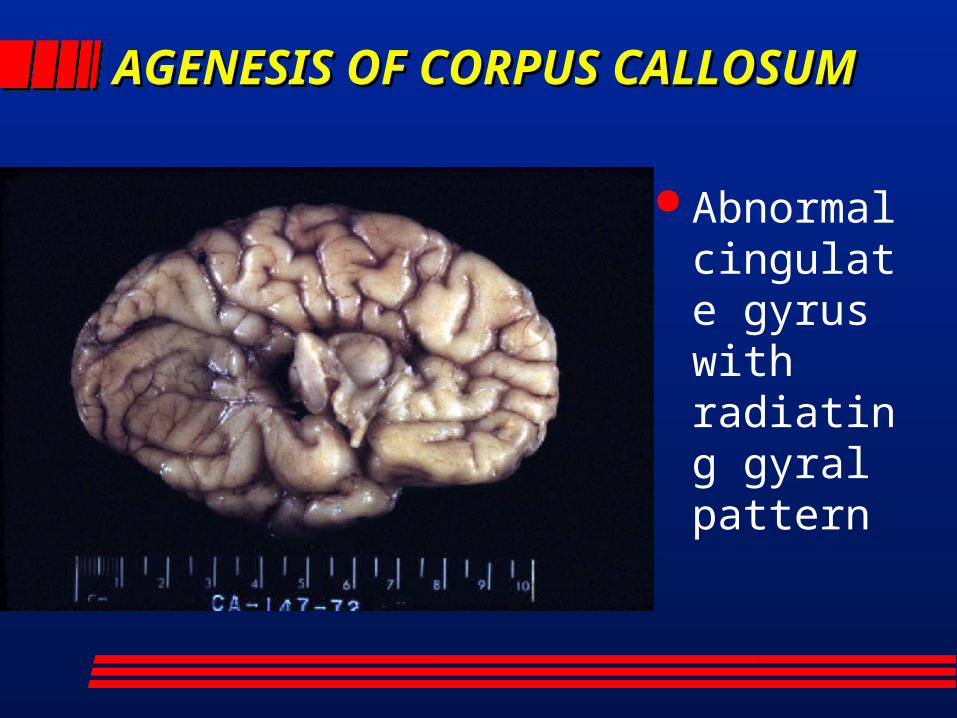
AGENESIS OF CORPUS AGENESIS OF CORPUS CALLOSUMCALLOSUM
Abnormal cingulate gyrus with radiating gyral pattern
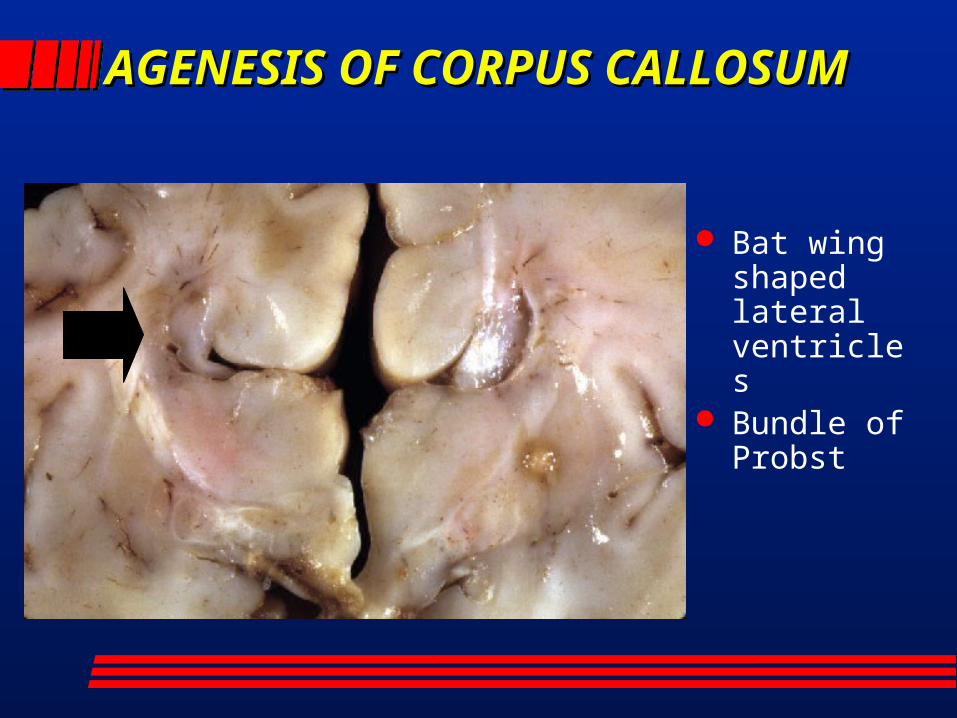
AGENESIS OF CORPUS AGENESIS OF CORPUS CALLOSUMCALLOSUM
Bat wing shaped lateral ventricles
Bundle of Probst
MICROENCEPHALMICROENCEPHALYY
MICROENCEPHALMICROENCEPHALYY
“Small brain” Primary
– with micro-cephaly (small head) Secondary
– may have normocephaly– Neurodegenerative diseases
» Ceroid lipofuscinosis (Batten’s disease)
MEGALENCEPHALYMEGALENCEPHALY Brain weight > 2.5 standard deviation
than mean Classification
– Primary: familial, achondroplasia, isolated– Secondary: leukodystrophies (Alexander’s),
neurocutaneous syndromes, errors of metabolism
May be associated with olivary heterotopia in autistic patients
1/3 with macroscopic and 1/3 with microscopic abnormalities
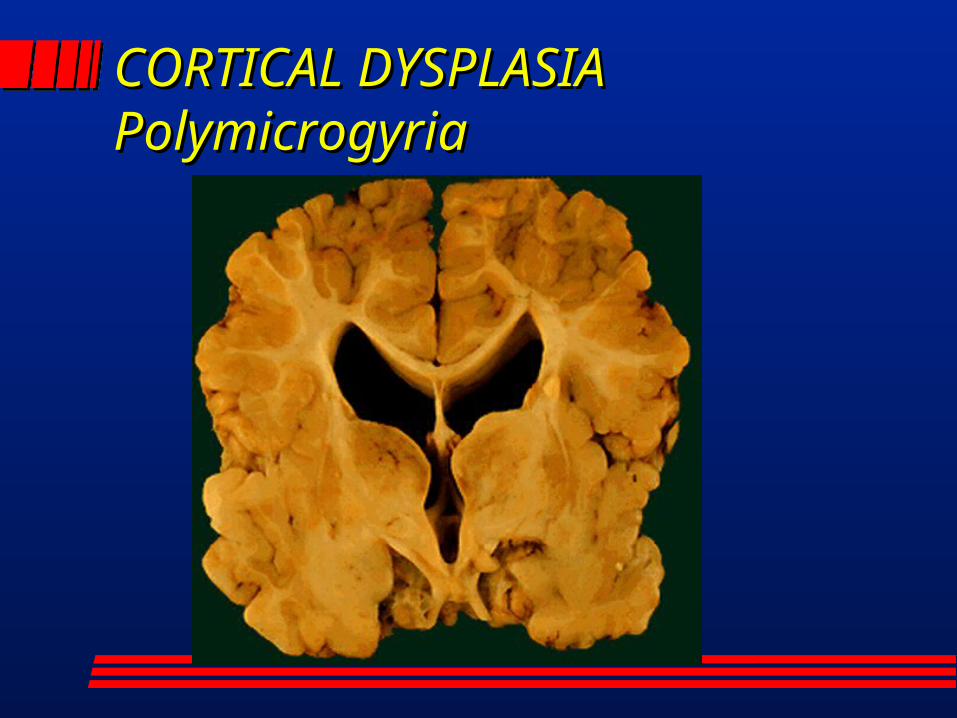
CORTICAL DYSPLASIACORTICAL DYSPLASIAPolymicrogyriaPolymicrogyria
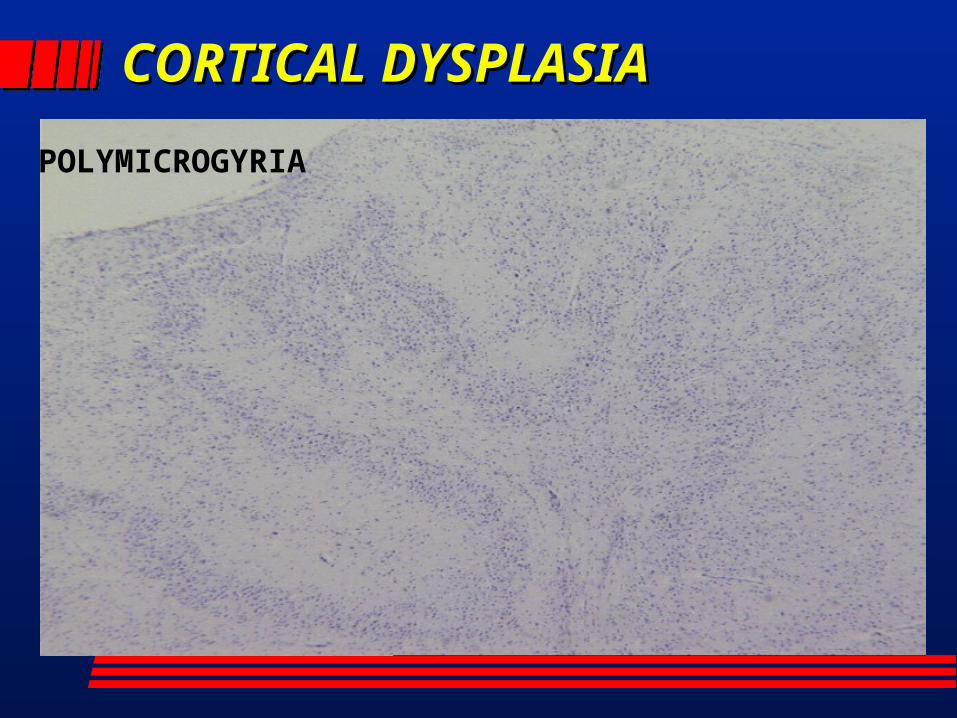
CORTICAL CORTICAL DYSPLASIADYSPLASIA
POLYMICROGYRIA
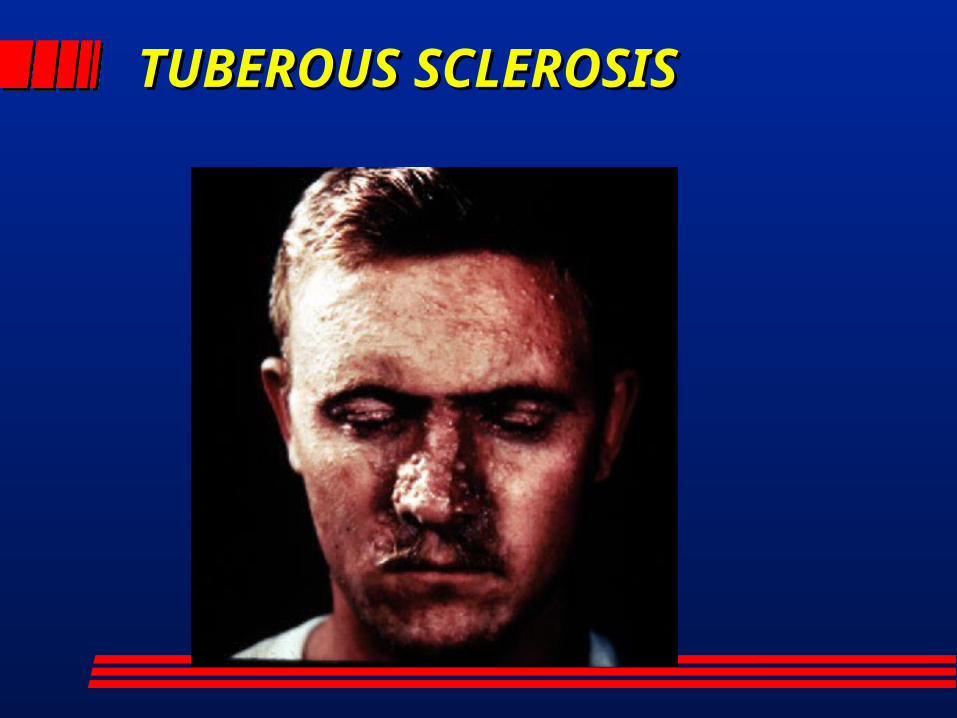
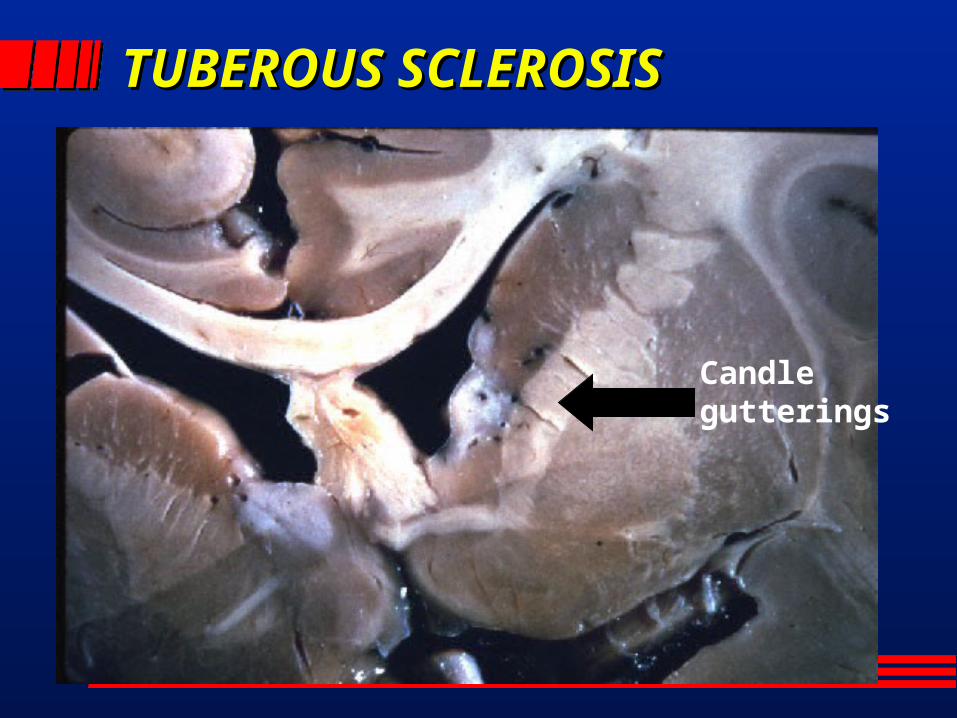
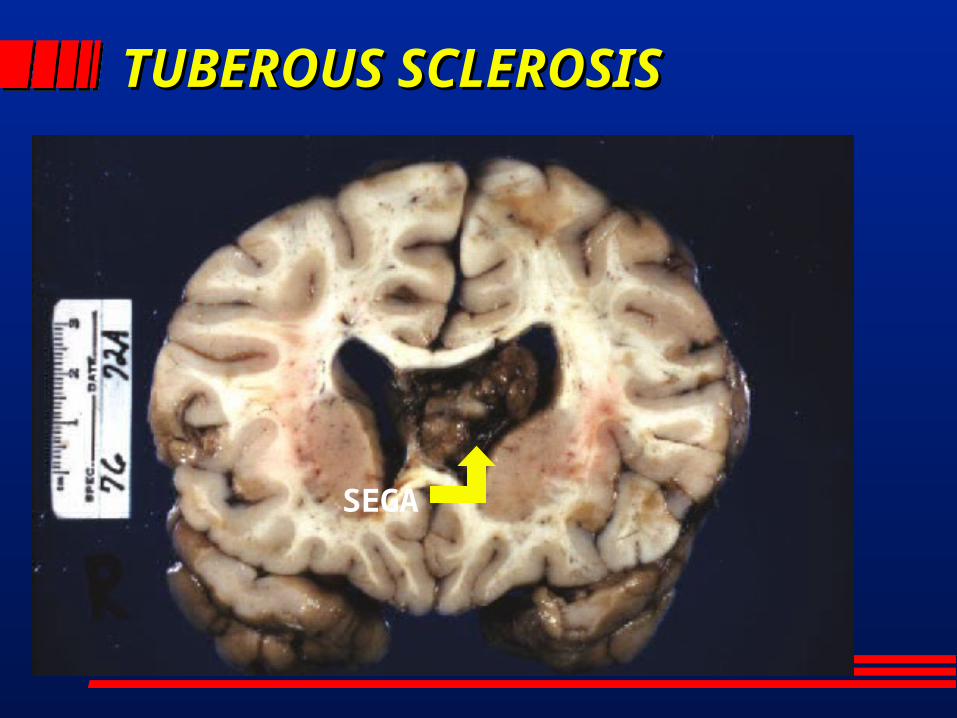
TUBEROUS TUBEROUS SCLEROSISSCLEROSIS
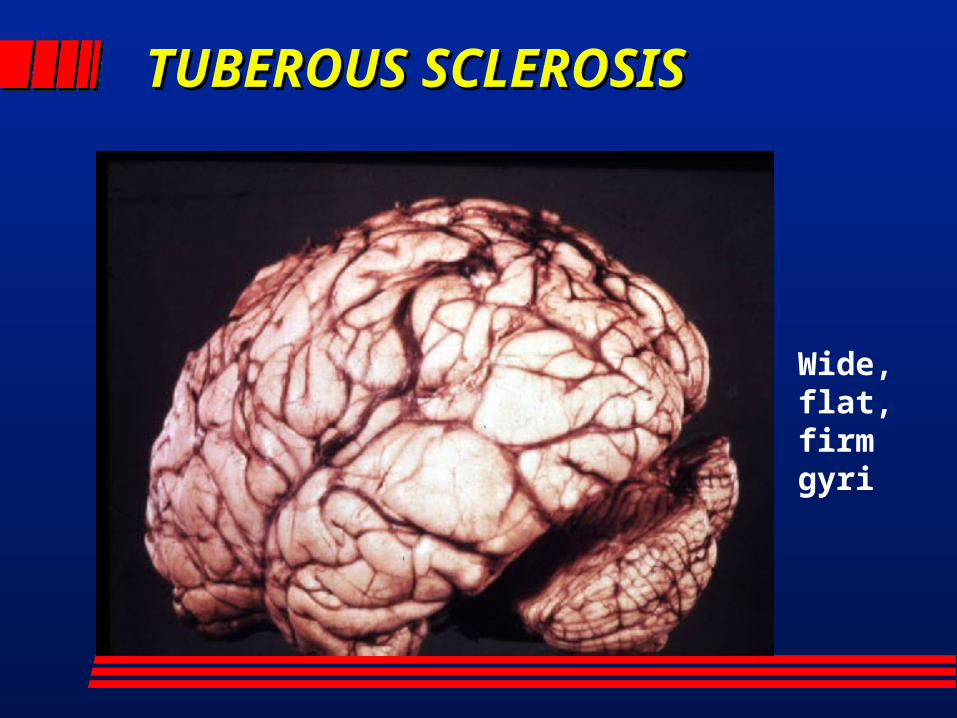
TUBEROUS TUBEROUS SCLEROSISSCLEROSIS
Wide, flat, firm gyri
TUBEROUS TUBEROUS SCLEROSISSCLEROSIS
Candle gutterings
TUBEROUS TUBEROUS SCLEROSISSCLEROSIS
SEGA
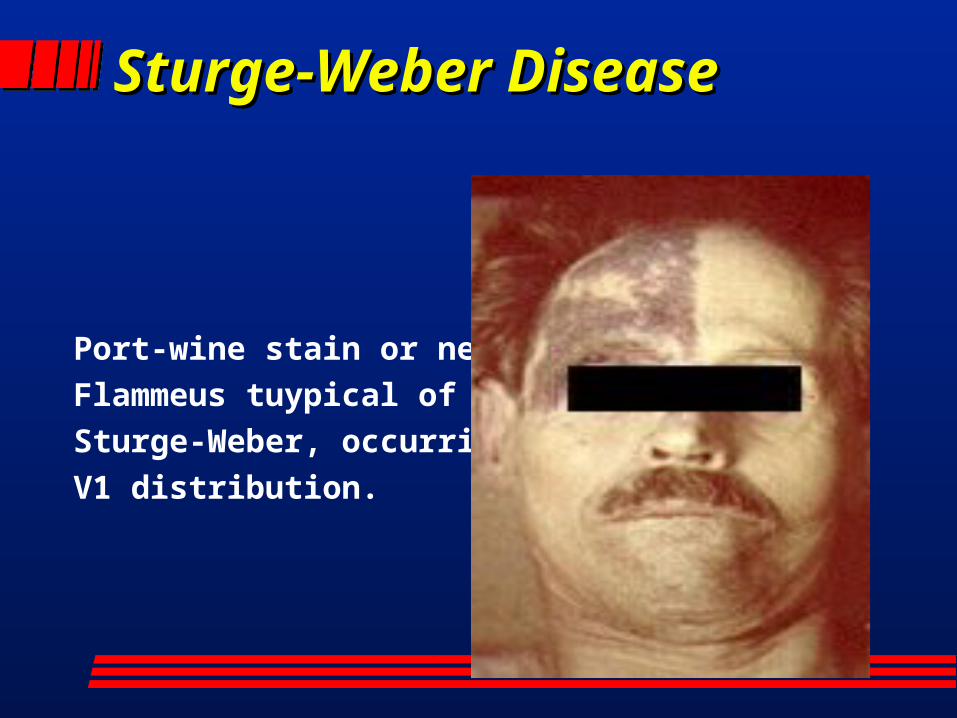
Sturge-Weber DiseaseSturge-Weber Disease
Port-wine stain or nevusFlammeus tuypical of Sturge-Weber, occurring inV1 distribution.
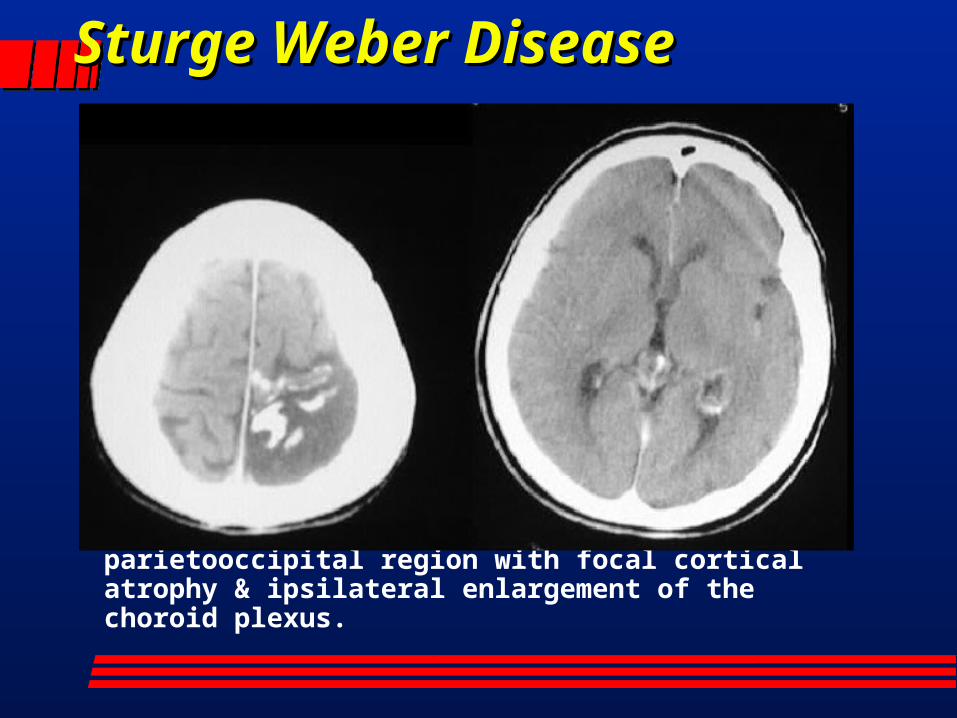
Sturge Weber DiseaseSturge Weber Disease
CT: Calcification of gyrus in the parietooccipital region with focal cortical atrophy & ipsilateral enlargement of the choroid plexus.
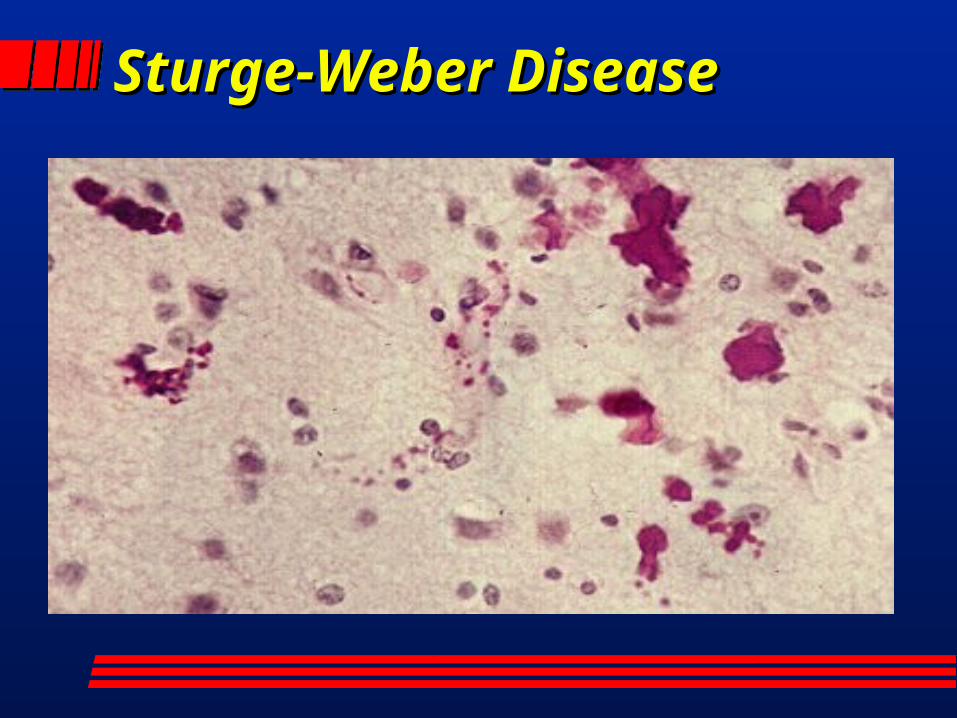
Sturge-Weber DiseaseSturge-Weber Disease