Embed Size (px)
Citation preview
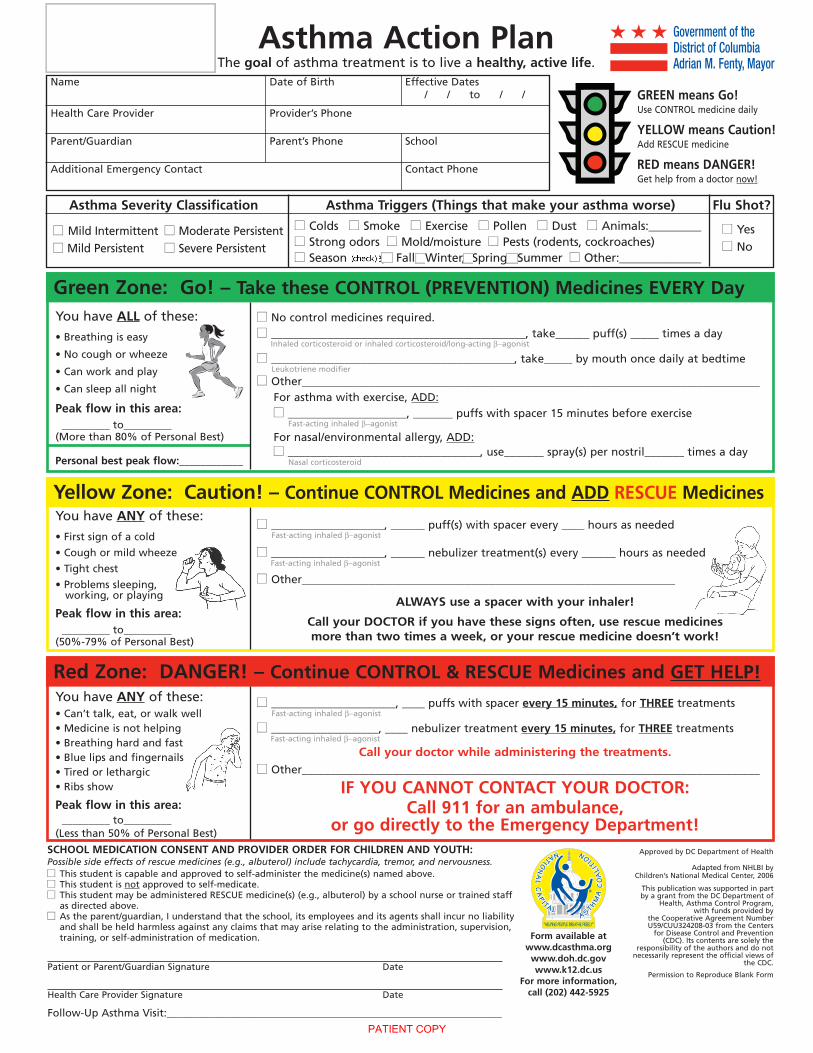
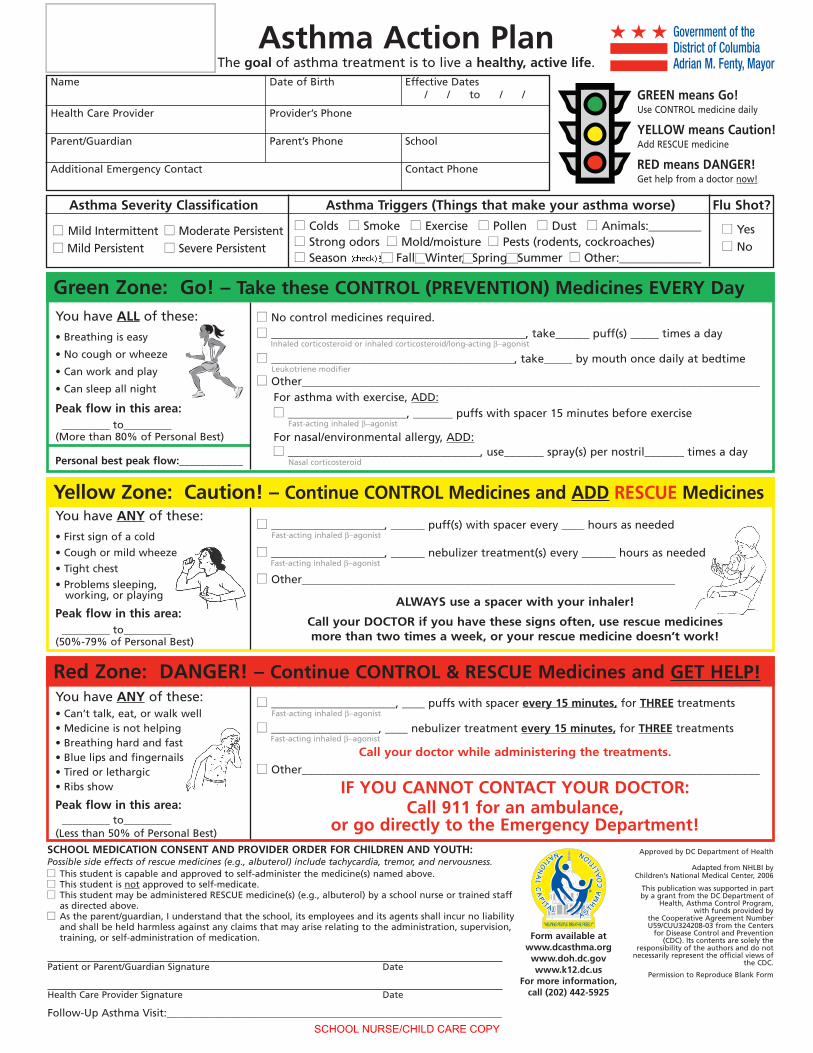
Asthma Action PlanThe goal of asthma treatment is to live a healthy, active life.
Name Date of Birth Effective Dates/ / to / /
Health Care Provider Provider’s Phone
Parent/Guardian Parent’s Phone School
Additional Emergency Contact Contact Phone
GREEN means Go!Use CONTROL medicine daily
YELLOW means Caution!Add RESCUE medicine
RED means DANGER!Get help from a doctor now!
Asthma Severity Classification Asthma Triggers (Things that make your asthma worse) Flu Shot?
■■ Mild Intermittent ■■ Moderate Persistent■■ Mild Persistent ■■ Severe Persistent
■■ Colds ■■ Smoke ■■ Exercise ■■ Pollen ■■ Dust ■■ Animals:_________■■ Strong odors ■■ Mold/moisture ■■ Pests (rodents, cockroaches)■■ Season (circle): Fall, Winter, Spring, Summer ■■ Other:______________
■■ Yes■■ No
Green Zone: Go! – Take these CONTROL (PREVENTION) Medicines EVERY DayYou have ALL of these:
• Breathing is easy
• No cough or wheeze
• Can work and play
• Can sleep all night
Peak flow in this area:_________ to_________
(More than 80% of Personal Best)
Personal best peak flow:____________
■■ No control medicines required.■■ _____________________________________________, take______ puff(s) _____ times a day
Inhaled corticosteroid or inhaled corticosteroid/long-acting β−agonist
■■ ___________________________________________, take_____ by mouth once daily at bedtimeLeukotriene modifier
■■ Other_________________________________________________________________________________For asthma with exercise, ADD:■■ _____________________, _______ puffs with spacer 15 minutes before exercise
Fast-acting inhaled β−agonist
For nasal/environmental allergy, ADD:■■ __________________________________, use_______ spray(s) per nostril_______ times a day
Nasal corticosteroid
Yellow Zone: Caution! – Continue CONTROL Medicines and ADD RESCUE MedicinesYou have ANY of these:
• First sign of a cold
• Cough or mild wheeze
• Tight chest
• Problems sleeping,working, or playing
Peak flow in this area:_________ to_________
(50%-79% of Personal Best)
You have ANY of these:• Can’t talk, eat, or walk well• Medicine is not helping• Breathing hard and fast• Blue lips and fingernails• Tired or lethargic• Ribs show
Peak flow in this area:_________ to_________
(Less than 50% of Personal Best)
■■ ____________________, ______ puff(s) with spacer every ____ hours as neededFast-acting inhaled β−agonist
■■ ____________________, ______ nebulizer treatment(s) every ______ hours as neededFast-acting inhaled β−agonist
■■ Other__________________________________________________________________
ALWAYS use a spacer with your inhaler!
Call your DOCTOR if you have these signs often, use rescue medicinesmore than two times a week, or your rescue medicine doesn’t work!
■■ ______________________, ____ puffs with spacer every 15 minutes, for THREE treatmentsFast-acting inhaled β−agonist
■■ ___________________, ____ nebulizer treatment every 15 minutes, for THREE treatmentsFast-acting inhaled β−agonist
Call your doctor while administering the treatments.■■ Other_________________________________________________________________________________
IF YOU CANNOT CONTACT YOUR DOCTOR:Call 911 for an ambulance,
or go directly to the Emergency Department!
Red Zone: DANGER! – Continue CONTROL & RESCUE Medicines and GET HELP!
Approved by DC Department of Health
Adapted from NHLBI byChildren’s National Medical Center, 2006
This publication was supported in partby a grant from the DC Department of
Health, Asthma Control Program,with funds provided by
the Cooperative Agreement NumberU59/CUU324208-03 from the Centers
for Disease Control and Prevention(CDC). Its contents are solely the
responsibility of the authors and do notnecessarily represent the official views of
the CDC.
Permission to Reproduce Blank FormPatient or Parent/Guardian Signature Date
Health Care Provider Signature Date
Follow-Up Asthma Visit:_______________________________________________________________
SCHOOL MEDICATION CONSENT AND PROVIDER ORDER FOR CHILDREN AND YOUTH:Possible side effects of rescue medicines (e.g., albuterol) include tachycardia, tremor, and nervousness.■■ This student is capable and approved to self-administer the medicine(s) named above.■■ This student is not approved to self-medicate.■■ This student may be administered RESCUE medicine(s) (e.g., albuterol) by a school nurse or trained staff
as directed above.■■ As the parent/guardian, I understand that the school, its employees and its agents shall incur no liability
and shall be held harmless against any claims that may arise relating to the administration, supervision,training, or self-administration of medication. Form available at
www.dcasthma.orgwww.doh.dc.govwww.k12.dc.us
For more information,call (202) 442-5925
Government of theDistrict of ColumbiaAdrian M. Fenty, Mayor
PATIENT COPY
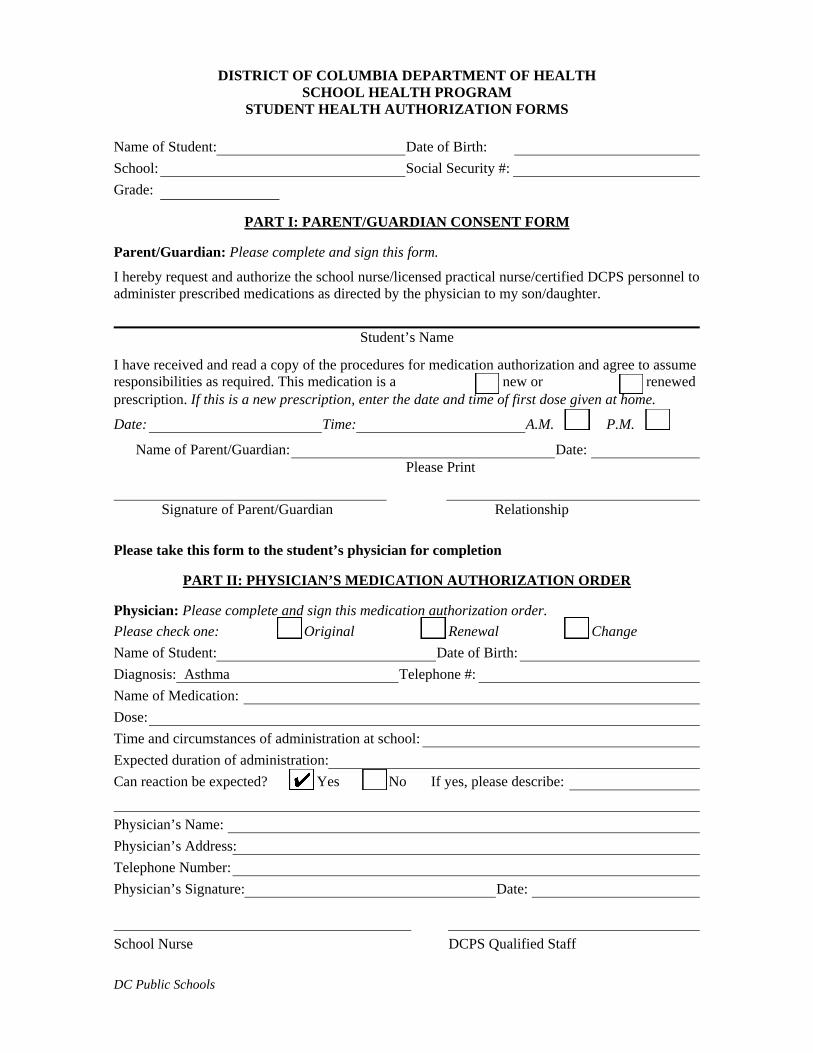
DISTRICT OF COLUMBIA DEPARTMENT OF HEALTH SCHOOL HEALTH PROGRAM
STUDENT HEALTH AUTHORIZATION FORMS
Name of Student: Date of Birth: School: Social Security #: Grade:
PART I: PARENT/GUARDIAN CONSENT FORM
Parent/Guardian: Please complete and sign this form.
I hereby request and authorize the school nurse/licensed practical nurse/certified DCPS personnel to administer prescribed medications as directed by the physician to my son/daughter.
Student’s Name
I have received and read a copy of the procedures for medication authorization and agree to assume responsibilities as required. This medication is a new or renewedprescription. If this is a new prescription, enter the date and time of first dose given at home.
Date: Time: A.M. P.M.
Name of Parent/Guardian: Date: Please Print
Signature of Parent/Guardian Relationship
Please take this form to the student’s physician for completion
PART II: PHYSICIAN’S MEDICATION AUTHORIZATION ORDER
Physician: Please complete and sign this medication authorization order. Please check one: Original Renewal Change Name of Student: Date of Birth: Diagnosis: Asthma Telephone #: Name of Medication: Dose: Time and circumstances of administration at school: Expected duration of administration: Can reaction be expected? Yes No If yes, please describe: Physician’s Name: Physician’s Address: Telephone Number: Physician’s Signature: Date:
School Nurse DCPS Qualified Staff DC Public Schools
Asthma Action PlanThe goal of asthma treatment is to live a healthy, active life.
Name Date of Birth Effective Dates/ / to / /
Health Care Provider Provider’s Phone
Parent/Guardian Parent’s Phone School
Additional Emergency Contact Contact Phone
GREEN means Go!Use CONTROL medicine daily
YELLOW means Caution!Add RESCUE medicine
RED means DANGER!Get help from a doctor now!
Asthma Severity Classification Asthma Triggers (Things that make your asthma worse) Flu Shot?
■■ Mild Intermittent ■■ Moderate Persistent■■ Mild Persistent ■■ Severe Persistent
■■ Colds ■■ Smoke ■■ Exercise ■■ Pollen ■■ Dust ■■ Animals:_________■■ Strong odors ■■ Mold/moisture ■■ Pests (rodents, cockroaches)■■ Season (circle): Fall, Winter, Spring, Summer ■■ Other:______________
■■ Yes■■ No
Green Zone: Go! – Take these CONTROL (PREVENTION) Medicines EVERY DayYou have ALL of these:
• Breathing is easy
• No cough or wheeze
• Can work and play
• Can sleep all night
Peak flow in this area:_________ to_________
(More than 80% of Personal Best)
Personal best peak flow:____________
■■ No control medicines required.■■ _____________________________________________, take______ puff(s) _____ times a day
Inhaled corticosteroid or inhaled corticosteroid/long-acting β−agonist
■■ ___________________________________________, take_____ by mouth once daily at bedtimeLeukotriene modifier
■■ Other_________________________________________________________________________________For asthma with exercise, ADD:■■ _____________________, _______ puffs with spacer 15 minutes before exercise
Fast-acting inhaled β−agonist
For nasal/environmental allergy, ADD:■■ __________________________________, use_______ spray(s) per nostril_______ times a day
Nasal corticosteroid
Yellow Zone: Caution! – Continue CONTROL Medicines and ADD RESCUE MedicinesYou have ANY of these:
• First sign of a cold
• Cough or mild wheeze
• Tight chest
• Problems sleeping,working, or playing
Peak flow in this area:_________ to_________
(50%-79% of Personal Best)
You have ANY of these:• Can’t talk, eat, or walk well• Medicine is not helping• Breathing hard and fast• Blue lips and fingernails• Tired or lethargic• Ribs show
Peak flow in this area:_________ to_________
(Less than 50% of Personal Best)
■■ ____________________, ______ puff(s) with spacer every ____ hours as neededFast-acting inhaled β−agonist
■■ ____________________, ______ nebulizer treatment(s) every ______ hours as neededFast-acting inhaled β−agonist
■■ Other__________________________________________________________________
ALWAYS use a spacer with your inhaler!
Call your DOCTOR if you have these signs often, use rescue medicinesmore than two times a week, or your rescue medicine doesn’t work!
■■ ______________________, ____ puffs with spacer every 15 minutes, for THREE treatmentsFast-acting inhaled β−agonist
■■ ___________________, ____ nebulizer treatment every 15 minutes, for THREE treatmentsFast-acting inhaled β−agonist
Call your doctor while administering the treatments.■■ Other_________________________________________________________________________________
IF YOU CANNOT CONTACT YOUR DOCTOR:Call 911 for an ambulance,
or go directly to the Emergency Department!
Red Zone: DANGER! – Continue CONTROL & RESCUE Medicines and GET HELP!
Approved by DC Department of Health
Adapted from NHLBI byChildren’s National Medical Center, 2006
This publication was supported in partby a grant from the DC Department of
Health, Asthma Control Program,with funds provided by
the Cooperative Agreement NumberU59/CUU324208-03 from the Centers
for Disease Control and Prevention(CDC). Its contents are solely the
responsibility of the authors and do notnecessarily represent the official views of
the CDC.
Permission to Reproduce Blank FormPatient or Parent/Guardian Signature Date
Health Care Provider Signature Date
Follow-Up Asthma Visit:_______________________________________________________________
SCHOOL MEDICATION CONSENT AND PROVIDER ORDER FOR CHILDREN AND YOUTH:Possible side effects of rescue medicines (e.g., albuterol) include tachycardia, tremor, and nervousness.■■ This student is capable and approved to self-administer the medicine(s) named above.■■ This student is not approved to self-medicate.■■ This student may be administered RESCUE medicine(s) (e.g., albuterol) by a school nurse or trained staff
as directed above.■■ As the parent/guardian, I understand that the school, its employees and its agents shall incur no liability
and shall be held harmless against any claims that may arise relating to the administration, supervision,training, or self-administration of medication. Form available at
www.dcasthma.orgwww.doh.dc.govwww.k12.dc.us
For more information,call (202) 442-5925
Government of theDistrict of ColumbiaAdrian M. Fenty, Mayor
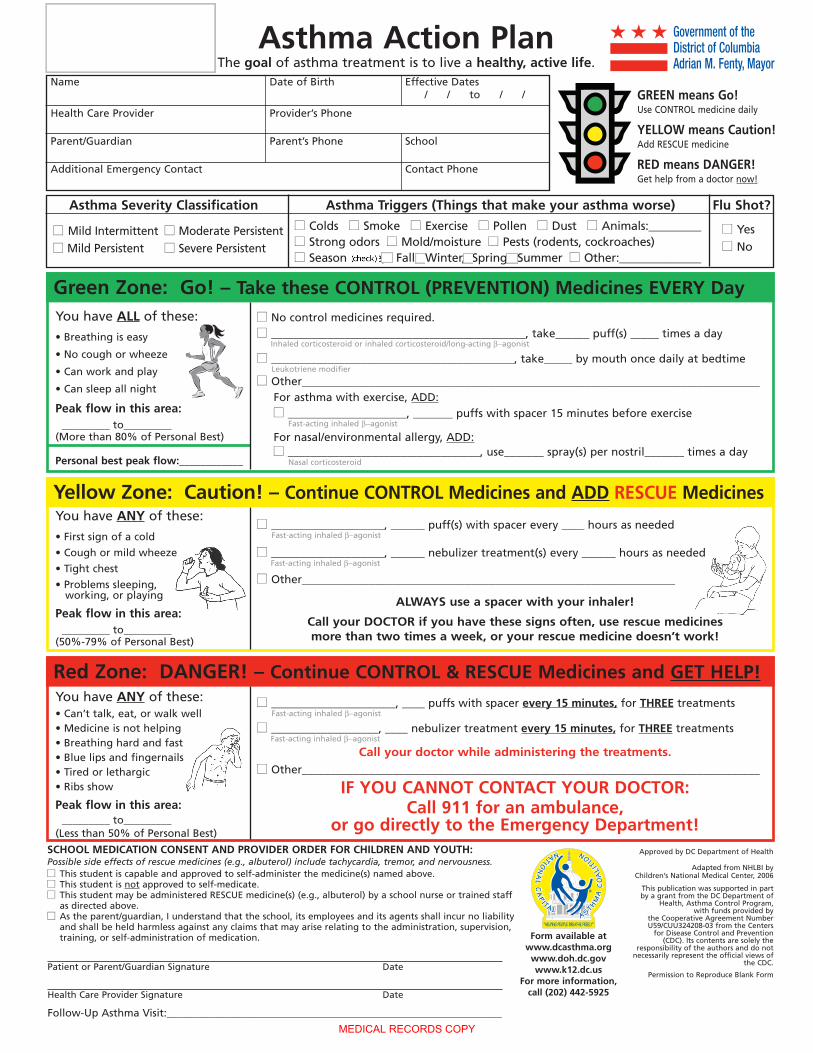
SCHOOL NURSE/CHILD CARE COPY
Asthma Action PlanThe goal of asthma treatment is to live a healthy, active life.
Name Date of Birth Effective Dates/ / to / /
Health Care Provider Provider’s Phone
Parent/Guardian Parent’s Phone School
Additional Emergency Contact Contact Phone
GREEN means Go!Use CONTROL medicine daily
YELLOW means Caution!Add RESCUE medicine
RED means DANGER!Get help from a doctor now!
Asthma Severity Classification Asthma Triggers (Things that make your asthma worse) Flu Shot?
■■ Mild Intermittent ■■ Moderate Persistent■■ Mild Persistent ■■ Severe Persistent
■■ Colds ■■ Smoke ■■ Exercise ■■ Pollen ■■ Dust ■■ Animals:_________■■ Strong odors ■■ Mold/moisture ■■ Pests (rodents, cockroaches)■■ Season (circle): Fall, Winter, Spring, Summer ■■ Other:______________
■■ Yes■■ No
Green Zone: Go! – Take these CONTROL (PREVENTION) Medicines EVERY DayYou have ALL of these:
• Breathing is easy
• No cough or wheeze
• Can work and play
• Can sleep all night
Peak flow in this area:_________ to_________
(More than 80% of Personal Best)
Personal best peak flow:____________
■■ No control medicines required.■■ _____________________________________________, take______ puff(s) _____ times a day
Inhaled corticosteroid or inhaled corticosteroid/long-acting β−agonist
■■ ___________________________________________, take_____ by mouth once daily at bedtimeLeukotriene modifier
■■ Other_________________________________________________________________________________For asthma with exercise, ADD:■■ _____________________, _______ puffs with spacer 15 minutes before exercise
Fast-acting inhaled β−agonist
For nasal/environmental allergy, ADD:■■ __________________________________, use_______ spray(s) per nostril_______ times a day
Nasal corticosteroid
Yellow Zone: Caution! – Continue CONTROL Medicines and ADD RESCUE MedicinesYou have ANY of these:
• First sign of a cold
• Cough or mild wheeze
• Tight chest
• Problems sleeping,working, or playing
Peak flow in this area:_________ to_________
(50%-79% of Personal Best)
You have ANY of these:• Can’t talk, eat, or walk well• Medicine is not helping• Breathing hard and fast• Blue lips and fingernails• Tired or lethargic• Ribs show
Peak flow in this area:_________ to_________
(Less than 50% of Personal Best)
■■ ____________________, ______ puff(s) with spacer every ____ hours as neededFast-acting inhaled β−agonist
■■ ____________________, ______ nebulizer treatment(s) every ______ hours as neededFast-acting inhaled β−agonist
■■ Other__________________________________________________________________
ALWAYS use a spacer with your inhaler!
Call your DOCTOR if you have these signs often, use rescue medicinesmore than two times a week, or your rescue medicine doesn’t work!
■■ ______________________, ____ puffs with spacer every 15 minutes, for THREE treatmentsFast-acting inhaled β−agonist
■■ ___________________, ____ nebulizer treatment every 15 minutes, for THREE treatmentsFast-acting inhaled β−agonist
Call your doctor while administering the treatments.■■ Other_________________________________________________________________________________
IF YOU CANNOT CONTACT YOUR DOCTOR:Call 911 for an ambulance,
or go directly to the Emergency Department!
Red Zone: DANGER! – Continue CONTROL & RESCUE Medicines and GET HELP!
Approved by DC Department of Health
Adapted from NHLBI byChildren’s National Medical Center, 2006
This publication was supported in partby a grant from the DC Department of
Health, Asthma Control Program,with funds provided by
the Cooperative Agreement NumberU59/CUU324208-03 from the Centers
for Disease Control and Prevention(CDC). Its contents are solely the
responsibility of the authors and do notnecessarily represent the official views of
the CDC.
Permission to Reproduce Blank FormPatient or Parent/Guardian Signature Date
Health Care Provider Signature Date
Follow-Up Asthma Visit:_______________________________________________________________
SCHOOL MEDICATION CONSENT AND PROVIDER ORDER FOR CHILDREN AND YOUTH:Possible side effects of rescue medicines (e.g., albuterol) include tachycardia, tremor, and nervousness.■■ This student is capable and approved to self-administer the medicine(s) named above.■■ This student is not approved to self-medicate.■■ This student may be administered RESCUE medicine(s) (e.g., albuterol) by a school nurse or trained staff
as directed above.■■ As the parent/guardian, I understand that the school, its employees and its agents shall incur no liability
and shall be held harmless against any claims that may arise relating to the administration, supervision,training, or self-administration of medication. Form available at
www.dcasthma.orgwww.doh.dc.govwww.k12.dc.us
For more information,call (202) 442-5925
Government of theDistrict of ColumbiaAdrian M. Fenty, Mayor
MEDICAL RECORDS COPY
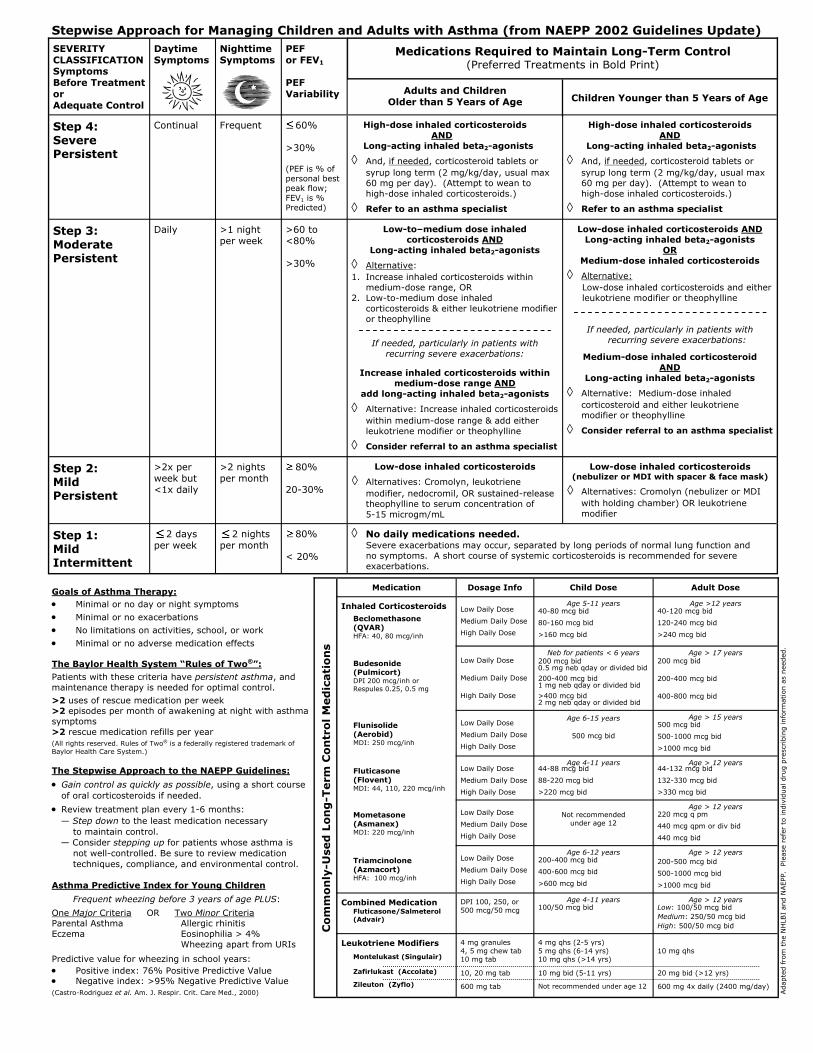
Stepwise Approach for Managing Children and Adults with Asthma (from NAEPP 2002 Guidelines Update)
SEVERITY CLASSIFICATION Symptoms Before Treatment or Adequate Control
Daytime Symptoms
Nighttime Symptoms
PEF or FEV1
PEF Variability
Children Younger than 5 Years of Age
Step 4: Severe Persistent
Continual Frequent
60% >30% (PEF is % of personal best peak flow; FEV1 is % Predicted)
High-dose inhaled corticosteroids AND
Long-acting inhaled beta2-agonists
◊ And, if needed, corticosteroid tablets or syrup long term (2 mg/kg/day, usual max 60 mg per day). (Attempt to wean to high-dose inhaled corticosteroids.)
◊ Refer to an asthma specialist
Step 3: Moderate Persistent
Daily >1 night per week
>60 to <80% >30%
Low-dose inhaled corticosteroids AND Long-acting inhaled beta2-agonists
OR Medium-dose inhaled corticosteroids
◊ Alternative: Low-dose inhaled corticosteroids and either leukotriene modifier or theophylline
If needed, particularly in patients with
recurring severe exacerbations:
Medium-dose inhaled corticosteroid AND
Long-acting inhaled beta2-agonists
◊ Alternative: Medium-dose inhaled corticosteroid and either leukotriene modifier or theophylline
◊ Consider referral to an asthma specialist
Step 2: Mild Persistent
>2x per week but <1x daily
>2 nights per month
80% 20-30%
Low-dose inhaled corticosteroids (nebulizer or MDI with spacer & face mask)
◊ Alternatives: Cromolyn (nebulizer or MDI with holding chamber) OR leukotriene modifier
Step 1: Mild Intermittent
2 days per week
2 nights per month
80% < 20%
Adults and Children Older than 5 Years of Age
High-dose inhaled corticosteroids AND Long-acting inhaled beta2-agonists
◊ And, if needed, corticosteroid tablets or syrup long term (2 mg/kg/day, usual max 60 mg per day). (Attempt to wean to high-dose inhaled corticosteroids.)
◊ Refer to an asthma specialist
Low-to–medium dose inhaled corticosteroids AND
Long-acting inhaled beta2-agonists
◊ Alternative: 1. Increase inhaled corticosteroids within
medium-dose range, OR 2. Low-to-medium dose inhaled
corticosteroids & either leukotriene modifier or theophylline
If needed, particularly in patients with recurring severe exacerbations:
Increase inhaled corticosteroids within medium-dose range AND
add long-acting inhaled beta2-agonists
◊ Alternative: Increase inhaled corticosteroids within medium-dose range & add either leukotriene modifier or theophylline
◊ Consider referral to an asthma specialist
Low-dose inhaled corticosteroids
◊ Alternatives: Cromolyn, leukotriene modifier, nedocromil, OR sustained-release theophylline to serum concentration of 5-15 microgm/mL
◊ No daily medications needed.
Medications Required to Maintain Long-Term Control (Preferred Treatments in Bold Print)
Severe exacerbations may occur, separated by long periods of normal lung function and no symptoms. A short course of systemic corticosteroids is recommended for severe exacerbations.
Goals of Asthma Therapy: • Minimal or no day or night symptoms
• Minimal or no exacerbations
• No limitations on activities, school, or work
• Minimal or no adverse medication effects The Baylor Health System “Rules of Two®”:
Patients with these criteria have persistent asthma, and maintenance therapy is needed for optimal control.
>2 uses of rescue medication per week >2 episodes per month of awakening at night with asthma symptoms >2 rescue medication refills per year
(All rights reserved. Rules of Two® is a federally registered trademark of Baylor Health Care System.) The Stepwise Approach to the NAEPP Guidelines:
• Gain control as quickly as possible, using a short course of oral corticosteroids if needed.
• Review treatment plan every 1-6 months: — Step down to the least medication necessary to maintain control. — Consider stepping up for patients whose asthma is not well-controlled. Be sure to review medication techniques, compliance, and environmental control. Asthma Predictive Index for Young Children
Frequent wheezing before 3 years of age PLUS:
One Major Criteria OR Two Minor Criteria Parental Asthma Allergic rhinitis Eczema Eosinophilia > 4% Wheezing apart from URIs
Predictive value for wheezing in school years: • Positive index: 76% Positive Predictive Value • Negative index: >95% Negative Predictive Value
(Castro-Rodriguez et al. Am. J. Respir. Crit. Care Med., 2000) Adapte
d fro
m t
he
NH
LBI
and N
AEPP.
Ple
ase
refe
r to
indiv
idual
dru
g p
resc
ribin
g info
rmation
as
nee
ded
.
Medication Dosage Info Child Dose Adult Dose
Inhaled Corticosteroids
Beclomethasone (QVAR) HFA: 40, 80 mcg/inh
Low Daily Dose Medium Daily Dose High Daily Dose
Age 5-11 years
40-80 mcg bid 80-160 mcg bid >160 mcg bid
Age >12 years
40-120 mcg bid 120-240 mcg bid >240 mcg bid
Budesonide (Pulmicort) DPI 200 mcg/inh or Respules 0.25, 0.5 mg
Low Daily Dose Medium Daily Dose High Daily Dose
Neb for patients < 6 years
200 mcg bid 0.5 mg neb qday or divided bid
200-400 mcg bid 1 mg neb qday or divided bid
>400 mcg bid 2 mg neb qday or divided bid
Age > 17 years
200 mcg bid 200-400 mcg bid 400-800 mcg bid
Flunisolide (Aerobid) MDI: 250 mcg/inh
Low Daily Dose Medium Daily Dose High Daily Dose
Age 6-15 years
500 mcg bid
Age > 15 years
500 mcg bid 500-1000 mcg bid >1000 mcg bid
Fluticasone (Flovent) MDI: 44, 110, 220 mcg/inh
Low Daily Dose Medium Daily Dose High Daily Dose
Age 4-11 years 44-88 mcg bid 88-220 mcg bid >220 mcg bid
Age > 12 years 44-132 mcg bid 132-330 mcg bid >330 mcg bid
Mometasone (Asmanex) MDI: 220 mcg/inh
Low Daily Dose Medium Daily Dose High Daily Dose
Not recommended
under age 12
Age > 12 years
220 mcg q pm 440 mcg qpm or div bid 440 mcg bid
Triamcinolone (Azmacort) HFA: 100 mcg/inh
Low Daily Dose Medium Daily Dose High Daily Dose
Age 6-12 years
200-400 mcg bid 400-600 mcg bid >600 mcg bid
Age > 12 years
200-500 mcg bid 500-1000 mcg bid >1000 mcg bid
Combined Medication Fluticasone/Salmeterol(Advair)
DPI 100, 250, or 500 mcg/50 mcg
Age 4-11 years
100/50 mcg bid
Age > 12 years
Low: 100/50 mcg bid Medium: 250/50 mcg bid High: 500/50 mcg bid
Leukotriene Modifiers
Montelukast (Singulair) Zafirlukast (Accolate) Zileuton (Zyflo)
4 mg granules 4, 5 mg chew tab 10 mg tab 10, 20 mg tab 600 mg tab
4 mg qhs (2-5 yrs) 5 mg qhs (6-14 yrs) 10 mg qhs (>14 yrs) 10 mg bid (5-11 yrs) Not recommended under age 12
10 mg qhs 20 mg bid (>12 yrs) 600 mg 4x daily (2400 mg/day)
Co
mm
on
ly-U
sed
Lo
ng
-Term
Co
ntr
ol
Med
icati
on
s