Embed Size (px)
Citation preview

MEDICAL NECESSITY IN PRIVATE HEALTH PLANS
Implications for Behavioral Health Care
CMHS8_01_Cover.qxd 5/9/2003 2:01 PM Page c1
U.S. Department of Health and
Human Services
Substance Abuse and Mental HealthServices Administration
Center for Mental Health Services
Sara RosenbaumBrian KamoieD. Richard MaueryBrian Walitt
Special Report
MEDICAL NECESSITY
IN PRIVATE HEALTH PLANS
Implications for Behavioral Health Care

Special Reportii
AcknowledgmentsThis report was prepared by the Center for Health Services Research and Policy, Departmentof Health Policy, The George Washington University School of Public Health and HealthServices under contract number 01M008689 for the Substance Abuse and Mental HealthServices Administration (SAMHSA), U.S. Department of Health and Human Services(DHHS). Jeffrey Buck, Ph.D., Associate Director for Organization and Financing, Center forMental Health Services, served as project officer for this report. William L. Wallace, Ph.D.,assisted with the preparation of this report.
Disclaimer
The views, opinions, and content of this publication are those of the authors and do notnecessarily reflect the views or policies of SAMHSA or DHHS.
Public Domain Notice
All material appearing in this report is in the public domain and may be reproduced orcopied without permission from SAMHSA. Citation of the source is appreciated. However,this publication may not be reproduced or distributed for a fee without the specific, writtenauthorization of the Office of Communications, SAMHSA, DHHS.
Electronic Access and Copies of Publication
This publication can be accessed electronically at www.samhsa.gov/. For additional freecopies of this publication, please call SAMHSA’s Mental Health Services Information Center1-800-789-2647.
Recommended Citation
Rosenbaum, S., Kamoie, B., Mauery, D. R., Walitt, B. (2003). Medical Necessity in PrivateHealth Plans: Implications for Behavioral Health Care. DHHS Pub. No. (SMA) 03-3790.Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental HealthServices Administration.
Originating Office
Office of the Associate Director for Organization and Financing, Center for Mental HealthServices, Substance Abuse and Mental Health Services Administration, U.S. Department ofHealth and Human Services (DHHS), 5600 Fishers Lane, 15-87, Rockville, MD 20857.DHHS Publication No. (SMA) 03-3790Printed 2003

Table of ContentsI. Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
II. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Research Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Structure and Organization of the Review . . . . . . . . . . . . . . . . . . . 6
III. Medical Necessity and the Published Literature . . . . . . . . . . . . . . . . . . . 7
IV. Industry Practices in the Managed Care Industry . . . . . . . . . . . . . . . . . 11
Analysis of the Structure of Medical Necessity Definitions . . . . . . 11
Interviews With Managed Care Officials on the Processes of Medical Necessity Determinations . . . . . . . . . . . . 13
Managed Care Accreditation Organizations . . . . . . . . . . . . . . . . . 16
Judicial Case Law, Official Investigations, and Legal Actions . . . . 19
Judicial Case Law . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Investigations and Official Legal Actions . . . . . . . . . . . . . . . . . 21
New York . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Maine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Connecticut . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
V. State Law Regulation of Medical Necessity . . . . . . . . . . . . . . . . . . . . . 25
Laws That Regulate the Content of Insurance Contracts . . . . . . . . 25
Independent Review Statutes . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
VI. Relevant Federal Laws Pertaining to Medical Necessity Reviews . . . . . . 29
ERISA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Office of Personnel Management Standards: FEHBP . . . . . . . . . . . 31
VII. Synthesis and Implications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
VIII. References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
IX. Endnotes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Medical Necessity in Private Health Plans iii
FiguresFigure 1: The Five Dimensions of the Medical Necessity Definition:
Industry Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figure 2: NCQA and JCAHO Utilization Management Standards . . . . . . 17
Figure 3: NCQA and JCAHO External Appeals Standards . . . . . . . . . . . . 18
Figure 4: Common Procedural Problems in Medical Necessity Determination Processes Noted in Investigations, Litigation, and Case Law . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Figure 5: Medical Necessity Utilization Review and Appeals Procedures . . . 31
TablesTable 1. Medical Necessity Definitions in Published
Literature (See Also Appendix C) . . . . . . . . . . . . . . . . . . . . . . . 45
Table 2. Medical Necessity Definitions: Managed Care Industry . . . . . . . 50
Table 3. Medical Necessity Definitions Identified in Case Law (Sorted by Case Name) . . . . . . . . . . . . . . . . . . . . . . . 51
Table 4. Medical Necessity Definitions Contained in State Statutes and Regulations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Table 5. State Independent Review Statutes and Regulations . . . . . . . . . . 64
Table 6. Medical Necessity Definitions: State InsuranceLaws and IRO Statutes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
Table 7. State Independent Review Statutes With Specific Behavioral Health Provisions . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
Table 8. Qualifications of External Reviewer in State IRO Statutes . . . . . 71
Table 9. Independent Reviews: Standard of Review for Medical Necessity Determinations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
AppendicesAppendix A. Selected Published Literature on Medical Necessity
(Sorted by Year) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
Appendix B. NCQA and JCAHO Utilization Management and External Appeals Standards . . . . . . . . . . . . . . . . . . . . . . . . 92
Appendix C. Litigation Regarding Medical Necessity Definitions and Procedures (Sorted by Case Name) . . . . . . . . . . 95
Appendix D. State Investigations and Legal Actions Regarding Medical Necessity Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
Special Reportiv

I.This report addresses how the term “medical necessity” is
defined in private health insurance coverage decisions. Itsummarizes a review of the literature, an extensive review of
legal cases that challenge insurer decisions, materials prepared by theinsurance industry, consultation with experts in the field, a review ofinvestigations conducted by State departments of insurance and attor-neys general, and interviews with health care executives regarding thedecisionmaking process itself. The report does not explore factors thatcan affect access to care that might be considered clinically necessary bytreating professionals or the effects of medical necessity decisions ontherapeutic outcomes.
Executive Summary
Sources of medical necessity definition: Fewregulations address the definition of medicalnecessity. There is no Federal definition,and only slightly more than one-third ofStates have any regulatory definition ofmedical necessity. As a result, the meaningof “medical necessity” is most commonlyfound in individual insurance contracts thatare defined by the insurer and hold primacyin most determinations.
Rather than turning simply on whether aproposed treatment meets professional med-ical standards, the prevailing definition ofmedical necessity is broadly framed, multi-dimensional, and controlled by the insurer,not the treating professional. The process ofmedical necessity determination is rarely pub-lic information. Even where a claimant canshow that a clinical recommendation is con-sistent with professional clinical standards,the insurer may reject a proposed treatmentif it is inconsistent with other definitionalelements such as relative cost and efficiency.
The multiple dimensions of the prevailingmedical necessity definition: The evidencesuggests that the medical necessity definitionspans five dimensions:1. Contractual scope—whether the contract
provides any coverage for certain proce-dures and treatments, such as preventiveand maintenance treatments that are notnecessary to restore a patient to “normalfunctioning.” This dimension preemptsany other coverage decision.
2. Standards of practice—whether the treat-ment accords with professional standardsof practice.
3. Patient safety and setting—whether thetreatment will be delivered in the safestand least intrusive manner.
4. Medical service—whether the treatmentis considered medical as opposed to socialor nonmedical.
5. Cost—whether the treatment is consideredcost-effective by the insurer.
Medical Necessity in Private Health Plans 1

Regulation of the medical necessity defini-tion and coverage determination process:Some State external review laws provideappeals procedures that permit reviewers toreject the insurer’s medical necessity defini-tion and look at the evidence with a fresh
eye. However, many State laws parallelinsurers’ multidimensional definitionalapproach. It does not appear that eitherthe State or Federal regulatory processhas moved away from the industry’sprevailing medical necessity standard.
Special Report2

II.Under basic principles that guide the American health care
system, decisions regarding which particular treatments, orthe amount of treatment, are medically necessary are made
by medical professionals in light of their patients’ condition and desires,and the state of health care knowledge. Despite all the changes that havetaken place in the health system over the past generation, medicalprofessionals remain legally and ethically obligated to make treatmentrecommendations that reflect sound professional judgment and that areappropriate in light of their individual patients’ needs.
Introduction
At the same time, however, whether apatient ultimately will receive care consid-ered necessary by a treating professional isinfluenced heavily by the availability ofhealth insurance coverage to finance the rec-ommended treatments (Hadley, 2002). Theinfluence of health insurance on access toand utilization of behavioral health servicesis well documented and is a consequence ofthe high cost of treatment that frequentlycan involve expensive and (in the case ofchronic conditions) long-term therapies(Buck, Teich, Umland, & Stein, 1999). Forthis reason, the coverage decisions made byhealth insurers and employee health benefitplans are fundamentally linked to the ques-tion of whether individuals will have accessto health services that their treating profes-sionals consider medically necessary andappropriate.
In the early years of the modernAmerican health insurance era (said to dateto the Second World War, when employer-sponsored group health insurance became
increasingly common), insurers paid forwhatever health services treating physi-cians recommended (Rosenblatt, Law, &Rosenbaum, 1997; Rosenblatt, Rosenbaum,and Frankford, 2002). As health care costsescalated, first public and then privatehealth insurers introduced utilization reviewtechniques. These techniques were designedto verify coverage and to independentlyassess the treatment recommendationsmade by health professionals. These earlyutilization review decisions, as they wereknown, were made retrospectively (afterthe fact). Subsequent analyses of theseearly cost containment efforts led to theconclusion that retrospective review wasineffective; as a result, insurers increasinglyturned to prospective and concurrentreview techniques.
Prospective and concurrent reviews soonbecame an industry standard, particularlywith the growth of managed care. Inmanaged care–style insurance, coverage iseither entirely or partially conditioned on
Medical Necessity in Private Health Plans 3

a patient’s receipt of care from a medicalprofessional who has been accepted into theplan’s treating provider network and whosecovered treatment recommendations aresubject to the standards set by the plan. Aninsurer or health plan can exercise controlin one of two ways. The intermediary mightin the first instance issue general treatmentguidelines that are supposed to guide physi-cians in their treating recommendations.Alternatively, the treating professional maysubmit specific recommendations for treat-ment to the insurer or health plan on behalfof an individual patient. Both approachestypically are present in any health plan; thatis, a treating professional may apply stan-dard guidelines to many patient treatmentdecisions (Domino et al., 1998; Institute ofMedicine, 1990; Manderscheid, Henderson,& Brown, 2001; Varble, 2001), reservingpatient-specific requests for treatment to arelatively small number of cases that do notappear to fit the parameters of such standardguidelines (e.g., patients with co-occurringconditions that place them out of standard-ized norms or particularly complex versionsof a recognized health problem).
This analysis, prepared for the SubstanceAbuse and Mental Health ServicesAdministration of the U.S. Department ofHealth and Human Services, focuses onmedical necessity in health insurance as theconcept applies to utilization managementdecisions by health insurers and employeebenefit plans in specific patient cases. Thisanalysis does not consider other factorsthat can influence access to coverage in themodern insurance system, such as the qualityof the general treatment guidelines used byinsurers or the contractual limitations oncoverage that can exclude certain treatmentsaltogether, no matter how medically neces-
sary (a phenomenon that has received enor-mous attention in the case of behavioralhealth as a result of the mental health paritydebate). Nor does this analysis considerlimitations on access to care that can resultfrom restrictions on the size and availabilityof a provider network established and usedby an insurer or health plan.
Instead, this analysis focuses on those situ-ations in which, in response to the perceivedneeds of an individual patient, a treatinghealth professional recommends treatmentthat may require specific approval of cover-age by an insurer or health plan. This analy-sis examines both the standards and proce-dures that insurers and health plans useexplicitly to determine whether recommend-ed services are necessary in specific instances;it does not address the process involved indetermining the amount of treatment deemedappropriate.
The structure of this review is based onthe assumption that, in determining whethera recommended course of treatment is med-ically necessary under the terms of the insur-ance contract, the definition of medicalnecessity and the process by which the con-tract is applied to a particular patient are ofequal importance. In assessing the processof decisionmaking, this report considers thequalifications and impartiality of the review-er as well as the extent to which the reviewerconsiders the specific condition of the indi-vidual patient, not merely what treatmentsare generally recommended in preset treat-ment guidelines. The procedural aspects ofcoverage decisionmaking are critical because,as this analysis shows, medical necessity defi-nitions are broad and ambiguous and vestinsurers with a great deal of discretion overthe treatment of individual patients. Howan insurer goes about deciding the necessity
Special Report4

of care is a particularly important questionin the case of patients whose conditionsare further complicated by the existence ofco-occurring health problems or a historyof failure under standard treatments.
This review examines a broad range ofinformation, including peer-reviewed litera-ture, judicial decisions construing contractterms, legislation, and documents developedby insurers themselves. Much of the evidenceregarding medical necessity presented in thisanalysis is found in legal documents, includ-ing judicial decisions in cases brought bypatients whose requests for treatment havebeen denied, as well as in investigations con-ducted and actions brought by State attor-neys general and insurance departments inresponse to evidence of systemic problems inobtaining access to insured coverage as aresult of ongoing medical necessity denials.
Judicial decisions and official investiga-tions frequently involve complaints regardingaccess to behavioral health coverage. This isprobably not surprising, given the cost oflong-term treatment for health conditionsrelated to mental illness and substance abusedisorders as well as evidence of major effortsby insurers over the past decade to achievesignificant reductions in behavioral healthspending (DHHS, 1999). Because of thelengthy and costly process of pursuing a caseagainst an insurer or health plan, reportedjudicial decisions are rare. (Indeed, in greatpart in response to the difficulty of pursuinglegal claims against health plans that havedenied coverage, Federal and State lawmak-ers have sought in recent years to establishsimpler, less formal, and less costly externalappeals procedures to challenge insurerdenials) (Dallek & Pollitz, 2000).1 At thesame time, it is in these official sources ofevidence that one is able to see most clearly
the terms of the contract (which outside alegal setting is a confidential and closely helddocument) as well as the process by whichan insurer or health plan administratorreached a decision. Medical necessity deter-minations that do not rise to the level ofappeal or complaint are beyond the scope ofthis analysis.
Research MethodsThe following research methods were used toconduct this review:■ Completing a literature review and syn-
thesis of findings regarding the definitionand process of delimiting medical necessityin a behavioral health context. Sourcesincluded the peer-reviewed medical andhealth services literature on medical neces-sity, as well as judicial decisions, Federaland State laws, illustrative contract terms,accreditation standards, materials gath-ered from the industry, and State-levelinvestigations and legal settlementsregarding medical necessity practices.2
■ Convening a working group of 20 expertsfor a half-day consultation (May 7, 2002)on issues related to medical necessity inbehavioral health care to provide commentand feedback on the draft literature review.Experts included professionals in clinicalpractice (e.g., psychiatry, psychology),employer purchasers of health care insur-ance, officials with managed care accredi-tation organizations, representatives ofconsumer advocacy organizations, andindividuals with expertise in insurance andhealth plan regulation at the State andFederal levels. Officials from three largemanaged care organizations who were notable to attend the May 7 meeting werelater interviewed by telephone. Officialsfrom two State attorneys general offices
Medical Necessity in Private Health Plans 5

(New York and Connecticut) and a Statebureau of insurance (Maine) were inter-viewed by telephone to provide additionalinsight for the section on legal settlementsand investigations. This report wasrefined based on the expert consultation,feedback, and assistance provided bythese advisors.
Structure and Organizationof the ReviewPart 1 summarizes peer-reviewed and pro-fessional literature on medical necessity, andconsiders the views and recommendationsof researchers and analysts regarding boththe definition of medical necessity and thestructure of the review process.
Part 2 describes industry practices asevidenced by individual insurer practicesand accreditation standards, as well as judi-cial opinions and official investigations thathave examined contract terms and decision-making procedures.
Part 3 reviews State insurance laws andexamines in detail not only the definition ofmedical necessity adopted by States as partof their insurance regulation laws, but alsothe procedural elements of their independentreview statutes.
Part 4 examines two major sources of lawrelevant to understanding the medical neces-sity review process in the private insurancecontext—the bodies of regulations that gov-ern private employee health benefit planscovered by the Employee Retirement IncomeSecurity Act (ERISA) and standards applica-ble to medical necessity determinations andappeals under the Federal Employee HealthBenefits program.
This review concludes with a synthesisof findings and a discussion of their impli-cations for coverage of behavioral healthservices.
Tables 1–9 and Appendixes A–D can befound at the end of this review.
Special Report6

III.Table 1 presents definitions of medical necessity drawn from
a search of peer-reviewed journals, trade journals, and indus-try and organization publications. A full list of these sources
appears in Appendix A. Over the past decade, authors have paid con-siderable attention to the question of medical necessity as prospectiveutilization review has come to dominate health insurance.
Medical Necessityand the PublishedLiterature
While variation exists in the opinionsexpressed, the articles summarized in Table 1display a significant level of consensus onthree basic issues. The first is that merelybecause a recommended treatment falls with-in the zone of professionally accepted med-ical practice does not mean it must be cov-ered. Only one source (the National HealthLaw Program) confines the evidence to theopinion of the treating physician. The secondis that a recommended definition of medicalnecessity should be multidimensional andshould consider factors such as cost, conven-ience, and relative effectiveness compared toother treatments based on various forms ofevidence. Third, the authors uniformly rec-ommend broadening the scope of when anintervention can be considered necessary(i.e., not merely to diagnose and treat an ill-ness but also to improve functioning, avertdeterioration, and maintain functioning).
Several authors address the issue of thequality, reliability, and relevance of the evi-dence considered when making a medicalnecessity determination; in addition, one
article examines the question of who bearsthe burden of proof in a medical necessitydetermination, an issue that has not beendirectly addressed in State or Federal law.
From the health services research commu-nity, probably the most seminal work is bySinger, Bergthold, Vorhaus, and Enthoven(1999). The definition of medical necessitythey crafted was the result of a consensusprocess among project participants (Singer,Bergthold, Vorhaus, & Enthoven, 1999):
For contractual purposes, an interven-tion will be covered if it is an otherwisecovered category of service, not specifi-cally excluded, and medically necessary.An intervention is medically necessaryif, as recommended by the treatingphysician and determined by the healthplan’s medical director or physiciandesignee, it is (all of the following):A health intervention for the purposeof treating a medical condition; themost appropriate supply or level ofservice, considering potential benefitsand harms to the patient; known to beeffective in improving health outcomes.
Medical Necessity in Private Health Plans 7

For new interventions, effectiveness isdetermined by scientific evidence. Forexisting interventions, effectiveness isdetermined first by scientific evidence,then by professional standards, then byexpert opinion; and cost-effective forthis condition compared to alternativeinterventions, including no intervention.“Cost-effective” does not necessarilymean lowest price. An intervention maybe medically indicated yet not be a cov-ered benefit or meet this contractualdefinition of medical necessity. A healthplan may choose to cover interventionsthat do not meet this contractual defi-nition of medical necessity.
This definition requires a review of thetreating clinician’s recommendation to ensurethat it is “for the purpose of treating a con-dition” and “the most appropriate” interven-tion in light of the patient’s particular condi-tion, benefits, and risks. The definition alsoassumes plan review of the provider’s treat-ment recommendations. The authors alsocontemplate that cost-effectiveness will be abasic element of the decision, but clarify thatthe question of cost-effectiveness is not oneof price alone. In addition, the authors createa hierarchy of evidence, with “scientific”evidence classified as the best evidence. Nodistinction is made by type of condition.
Of particular significance in the Singer/Bergthold analysis is its emphasis on theprimacy of coverage limitations, a majorconcern of insurers. The authors recognizethat once a particular type of treatment isexcluded for a specific condition as a con-tractual matter,3 no general finding of med-ical necessity can override the exclusion.This emphasis on the primacy of the con-tract in controlling the range of treatmentsand procedures that will be considered atall in a medical necessity determination isreinforced by the Health Insurance
Association of America (Schiffbauer, 1999),which has stated:
When the provider, rather than thehealth plan or insurer, interprets thescope of coverage under the contract,health plan fiduciaries cannot guaranteeto the insured that health care dollarsare being spent fairly and equitablyon medical treatments that are safe,proven, and effective.
The American Medical Association(AMA), representing physicians (includingpsychiatrists), has created a prototypemedical necessity definition as part of itsModel Managed Care Contract project:
Section 1.9 defines medically neces-sary/medical necessity as health careservices or products that a prudentphysician would provide to a patientfor the purpose of preventing, diag-nosing, or treating an illness, injury,disease, or its symptoms in a mannerthat is a) in accordance with generallyaccepted standards of medical practice;b) clinically appropriate in terms oftype, frequency, extent, site, and dura-tion; and c) not primarily for the con-venience of the patient, physician, orother health care provider.4
Like the others this definition is multi-dimensional but it focuses the utilizationreview on what a prudent physician wouldconclude based on the evidence rather thanwhat the insurer would determine. Whilethe definition is crafted in such a way as totransfer more medical decisionmaking powerback to the provider, the practical impact ofthis distinction is difficult to assess, since thedecision remains reviewable and the reviewis multidimensional. However, cost consider-ations as an explicit measure are removed.By using the “prudent physician” rather thanthe insurer as the standard of measurementwhere judgment is concerned, the definition
Special Report8

seeks to focus the determination on “general-ly accepted” medical opinion (and thus thephenomenon of multiple schools of thought)rather than the opinion of utilization reviewprofessionals who may or may not be physi-cians and who view their task as selectingthe single best form of treatment. Thus, inan appeal made under the AMA definition,a claimant would be able to introduce a widerange of schools-of-thought evidence from“prudent physicians” to show the variationin treatments that prudent physicians mightrecognize.
Several authors focus on definitions ofmedical necessity in the behavioral healtharena, although their proposed definitionsappear to differ more in terminology than insubstance. Paul Chodoff (1998) and WilliamFord (1998, 2000) have called for replacingthe term with “health necessity,” “treatmentnecessity,” or “clinical necessity.” In Chodoff’sview, health necessity criteria would befounded on a biopsychosocial rather than ona medical model. The former model requiresa view of health as encompassing quality-of-life factors and not just the absence ofdisease. The terms “biopsychosocial” and“psychosocial” arose from the need to differ-entiate between mental and physical health.5
The practical effects of this distinctionwould be on the “scope” element of thedefinition, that is, the range of possibleconditions for which treatment, if necessary,would be approved. Interventions wouldnot be solely for the diagnosis or treatmentof an illness, but also for the achievement ofbroader health goals. Furthermore, Chodoffproposes consideration of services for indi-viduals whose diagnoses may not easily fitinto categories defined by the Diagnosticand Statistical Manual of Mental Disorders(DSM-IV), a reference often cited as a clini-
cal standard in medical necessity definitionsfor behavioral health (APA, 1994).
Ford’s (1998, 2000) behavioral health caredefinition urges a movement away from cov-ering only acute care to covering longer-termcare designed to manage and prevent dete-rioration of chronic conditions and onsetof acute conditions. This definition wouldinclude access to psychiatric rehabilitationservices when needed for the treatment ofchronic mental conditions. (This definition ofcourse would require a dramatic expansionof the terms of coverage under conventionalinsurance, which, unlike Medicaid, tends tobe confined to relatively short-term therapiesto help an individual significantly improve orrecover in a relatively short period of time.)(Rosenbaum, forthcoming; Rosenbaum &Rousseau, 2001) Like Chodoff, Ford stressesthe importance of both the quality of day-to-day functioning as a goal of treatment, andthe need to cover treatment designed for alle-viation of symptoms in addition to “cure.”
Ireys, Wehr, and Cooke (1999) proposea specific definition of medical necessityfor persons with developmental disabilities,mental retardation, and other special healthcare needs. Their article represents a detailedand specific attempt to articulate individual-ized decisionmaking criteria that can “assistthe individual to achieve or maintain suffi-cient functional capacity to perform age-appropriate or developmentally appropriatedaily activities.”(p. 19) The authors callfor an expanded view of the informationsources an insurer should consider beyond“medical evidence” (i.e., information fromthe patient, the family, collateral providers,and support institutions). They also empha-size the effect of treatment on day-to-dayfunctioning and require that final determina-tions be made by a physician employed by
Medical Necessity in Private Health Plans 9

the insurer (rather than a claims reviewerwith lesser qualifications).
Two articles (Appendix A) deal specificallywith evidentiary matters and the use of evi-dence in decisionmaking. David Eddy (1994)posits that when determining the appropriateuse of an intervention, analysis of its poten-tial value should shift from qualitative toquantitative, with use of randomized, con-trolled clinical trials as a definitive evidencebase. Furthermore, in his view, a shift fromindividual-based decisionmaking to popula-tion-based decisionmaking is needed, basedlargely on the utility of controlled clinicaltrials that demonstrate treatment efficacyacross large numbers of people. He advo-cates for the development of explicit criteriato sort out high-value practices from thoseof little or no value and believes that theterm “medical necessity” is too vague andopen to too much variability in interpreta-tion. By contrast, Rosenbaum, Frankford,Moore, and Borzi (1999) recommend anemphasis on individualized decisions ratherthan across-the-board conclusions based onthe application of generalized guidelines andresearch results to specific cases. They callfor strict scrutiny of the reliability and rele-vance of scientific evidence, as well as forgreater emphasis on the facts of an individ-ual case and expert judgment. They also rec-ommend shifting the burden of proof to thehealth plan in any review of its decision onmedical necessity, arguing that the plan hasbest access to the evidence, and that fairnessin allocating the burden of proof wouldplace the burden on the party with the bestaccess to evidence.
Sabin and Daniels (1994) address thequestion of the utility of medical necessity
definitions for mental health services fromthe perspective of severity of diagnosis.While no question exists that severe mentalillness such as schizophrenia, clinicaldepression, and bipolar depression are cov-ered by traditional medical necessity defi-nitions, Sabin and Daniels investigate theextent to which such definitions also shouldcover conditions such as shyness, unhappi-ness, and lack of personal fulfillment. Usingsix illustrative case studies, such as “TheShy Bipolar,” “The Unhappy Husband,”“The Cranky Victim,” (pp. 5–7) and others,Sabin and Daniels illustrate the differencesof opinion between “hard-line” and“expansive” clinicians (p. 5) in decidingwhether psychiatric services are needed.Following an analysis of three models ofmedical necessity, the authors conclude thatthe most rational model is one that treatsa medically defined diagnosis, such as onedelineated in the DSM-IV, to decrease theimpact of disease or disability. A typicalmental health medical necessity definitionwould be “those mental health serviceswhich are essential for the treatment of aMember’s mental health disorder as definedby the DSM-IV in accordance with general-ly accepted mental health practice”(p. 12).Sabin and Daniels note that diagnostic cate-gories continue to change but that society“needs a publicly acceptable and adminis-terable system for defining the boundariesof health insurance coverage.” To that end,the DSM-IV (and subsequent editions) pro-vides a workable definition of those bound-aries, to the extent that it is “the result ofa highly public process open to scientificscrutiny, field testing, and repetitive criti-cism over time.”6
Special Report10

IV.Insurers have continued to customize and streamline their defini-
tion of medical necessity over time to expand their control over,and the allocation of, health plan resources. By defining medical
necessity and controlling the coverage determination process, insurerscan attempt both to stem what they perceive to be the unnecessaryexpenditure of resources and to improve the quality of health care.7
Industry Practices in the Managed Care Industry
Analysis of the Structure ofMedical Necessity DefinitionsInsurers and insuring organizations rarelymake their medical necessity definitionsand determination procedures public. Thedefinitions and procedures are typicallycontained in contracts and internal opera-tional documents such as provider manualsand operating guidelines that are consideredproprietary and confidential.8 While manymanaged care organizations (MCOs) haveWeb sites, most require registration andpasswords from contracted providers toaccess detailed information about theirmedical necessity definitions and proce-dures. Consumers and researchers usuallyare permitted Web site access only togeneral health plan information.
Table 2 presents five insurer definitionsobtained for this research. An exception tothe rule, ValueOptions allows public accessto its Web site, which contains the text of itsprovider manuals. Cigna Behavioral HealthCare provides online access to its “Levelsof Care Guidelines for Mental Health and
Substance Abuse Treatment,” which con-tains a definition of medical necessity.9 Table2 also contains definitions from HighmarkBlue Cross, an anonymous managed behav-ioral health plan, and United BehavioralHealth. The Highmark definition wasobtained from the proceedings of an Agencyfor Healthcare Research and Quality(AHRQ) User Liaison workshop on coveragedecisions by Hill, Hanson, and O’Connell(2000). The third medical necessity defini-tion in Table 2 was obtained from materialsprovided to one of this review’s authorsduring a December 2001 meeting withbehavioral health care providers to discussmedical necessity issues. The company’sname is not disclosed for purposes of confi-dentiality. The United Behavioral Health(UBH) medical necessity definition wascontained in a consent agreement that UBHentered into in 2000 with the Maine Bureauof Insurance, published on the MaineDepartment of Professional & FinancialRegulation Web site.10 The consent agreementitself is discussed in Legal Settlements below.
Medical Necessity in Private Health Plans 11

Despite the limited number of definitionsavailable directly from the industry, thoseavailable suggest that insurers and insuringorganizations use a definition of medicalnecessity far more complex than whetherthe prescribed treatment is consistent withaccepted practice in the field. The use of adefinition of medical necessity that extendswell beyond the threshold question ofwhether the care is professionally sound canbest be understood as an attempt to mitigatethe “schools of thought” doctrine. This doc-trine, a critical element of professional med-ical liability law, assumes the existence ofmultiple and equally professionally accept-able approaches to professional medicalpractice in any particular case (Rosenblatt,Law, & Rosenbaum, 1997). For this reason,insurers have adopted definitions that vestthem with the power to select among variousschools of thought for the approach that,in the insurer’s view, also best satisfies theother elements of the definition.
The first dimension of the medical neces-sity definition found in Table 2 (and the onereflected in the overall structure of agree-ments themselves) can be thought of as con-tractual scope. This dimension is concernedwith whether the contract provides any cov-erage for certain procedures and treatments,such as those that prevent the worseningof a condition or that allow an individualto maintain or promote functioning. It ispossible, in other words, for the definitionto exclude any procedures that, in the viewof the insurer, do not yield recovery orresult in what the insurer considers a sig-nificant short-term improvement. Table 2shows that Highmark, the anonymousmanaged behavioral health organization(MBHO), and UBH limit the concept ofmedical necessity to services necessary for
the diagnosis or treatment of illness. Thus,a treatment necessary to respond to a con-dition not regarded as an illness (e.g., adevelopmental disorder in a child) mightfall outside the furthest reaches of the con-tract no matter how necessary the care oreffective the treatment. Similarly, if thetreatment is designed to avert deteriorationrather than treat illness to a point ofsignificant improvement, it might also beconsidered outside the scope of coverage.11
ValueOptions, in contrast, will recognizeas covered (if medically necessary) servicesaimed at preventing illness or avoiding dete-rioration. The Cigna definition, while stillincluding a “reasonable expectation” forimprovement, does include “level of func-tioning” in addition to a patient’s conditionor illness, an important criterion for per-sons with mental and physical disabilitieswhose treatment needs extend beyond thetraditional medical model.
The second dimension of the definitionreflects whether the treatment is in accordwith professional standards of practice. Thisdimension is most directly related to profes-sional opinion and clinical judgment. In thecase of ValueOptions and Cigna, the specificframe of reference is national practice stan-dards, although the fact that Highmark doesnot specifically reference national standardsis probably not particularly important, sincethe professional standard of care has beenrecognized as a national benchmark formore than 40 years.12 The UBH definitionspecifically refers to its own internal guide-lines as the standard to measure the appro-priateness of the type, frequency, and dura-tion of treatment.13
The third dimension can be thought ofas patient safety and setting. It considerswhether the prescribed treatment will be
Special Report12

delivered in a manner that the insurer con-siders to be safe and effective.
The fourth dimension is whether, in theinsurer’s view, the treatment is medical innature and not prescribed either as a matterof convenience or as a result of social orenvironmental considerations. In all of thedefinitions, convenience is measured in termsof the patient, the family, or the provider, notin terms of the managed care organization.
The fifth dimension of the definitionis cost. Table 2 suggests that a review oftreatment should include consideration ofwhether there is an equally effective andsafe, but less costly, alternative to the rec-ommended treatment. It is unclear whetherthe UBH reference to “of demonstratedmedical value” refers to treatment effec-tiveness, cost-effectiveness, or both.
The various sources of information thatsuggest the existence of these definitionaldimensions also suggest that the terms tendto remain undefined, allowing an insurertremendous leeway to define the termswithin the context of each determination.
Consistent with the issue of contractualscope, the ValueOptions definition explicitlyconsiders whether care, no matter hownecessary, is a service that falls outside thecontractual limits of the plan. This consid-eration can be seen in that portion of thedefinition that authorizes consideration ofwhether the recommended course of treat-ment would result in “non-treatment ser-vices addressing environmental factors.” Itis unclear how this element of the definitionwould work in practice. An example mightbe refusal to cover in-home care to a patientunable to obtain transportation to an out-patient provider, while providing the sameservices in-home to a patient medicallyunable to travel. Even though the care is
technically medically necessary in bothcases, ValueOptions could refuse to coverthe in-home care to the first on the groundsthat such care results from environmental(i.e., lack of transportation) rather thanmedical need.
These dimensions of the medical necessitydefinition delineate the criteria to be fulfilledfor an individual to be eligible for coverage.By choosing a high evidentiary, or tightlylimited, standard regarding the evidence thatmust be present in order to satisfy coverageeligibility, such as the evidence-based medi-cine standard of requiring two controlled,randomized clinical trials before a medicalintervention can be proven effective, insurerscould impose limits on many types of care.
Figure 1 summarizes the five dimensions ofthe medical necessity definition derived fromthe preceding analysis of industry practice.
Interviews With Managed CareOfficials on the Processes ofMedical Necessity DeterminationsIn mid-June 2002, semistructured telephoneinterviews were conducted with three offi-cials (two medical directors and a chief exec-utive officer) of two large MBHOs and onenationally based integrated health plan.14
Medical Necessity in Private Health Plans 13
Figure 1: The Five Dimensionsof the Medical Necessity Definition:Industry Practice
• The contractual scope of coverage: whetherproposed treatment is explicitly included orexcluded in the health plan contract
• Whether the proposed treatment is consistentwith professional standards of practice
• Patient safety and setting of the treatment• Whether the treatment is medical in nature
or for the convenience of the healthprofessional or patient and family
• Treatment cost

These officials, who, due to scheduling diffi-culties, were unable to participate in the May7 meeting of the expert panel, also reviewedthe draft of this document. The interviewquestions focused on the processes used inthe managed behavioral health care industryfor making initial medical necessity determi-nations and resolving appeals of claimsdenials, as well as internal quality manage-ment procedures used to incorporate andupdate treatment guideline information intodecisionmaking processes.
One official noted that his MBHO prefersto use the term “clinical appropriateness”rather than “medical necessity.” In the offi-cial’s view, the latter term implies a restric-tive orientation relating to the question ofwhether or not a patient needs care (a clini-cal decision that can only be made by theprovider and the patient). The officialemphasized that, in his opinion, the pivotalquestion is what level of services in whichsettings are most clinically appropriate fora given patient in light of his or her clinicaland social needs. Thus, as the definition sug-gests, the MCO medical director views histask as analyzing the health professional’srecommendations in accordance with thosedimensions of the medical necessity defini-tion that focus on how the care will be fur-nished, by whom, and in what settings, notwhether the professional was justified inconcluding that some particular approachto treatment was needed. In this vein, thecoverage decision concentrates more on theform and manner of treatment than whetherany treatment at all will take place.
The interviews confirmed that managedcare executives view their jobs not as deter-mining the necessity of care from a profes-sional point of view but as determiningwhether the professional’s treatment judg-
ment is consistent with the terms of coveragein the contract. The organizations view theirtask as administering and managing a pack-age of contractual benefits to determine whatis included in the benefit package purchasedby an employer, not to determine what thebenefit package should contain. Within thatdetermination is the task of ensuring thatthe levels of care and treatments providedare appropriate for an enrollee’s needs andcovered in the benefit package.
When asked why behavioral health med-ical necessity definitions have been the sub-ject of a higher level of discussion and scruti-ny than in general medicine, the intervieweesoffered several reasons:
■ The nature of behavioral health care serv-ices compared to general physical medicalcare is such that there is less “objective”evidence available to guide decisions thatreflect a consensus as to what the appro-priate treatments should be for a givendiagnosis. While progress has been madein developing a clinical evidence base forbehavioral health care, it has not yetreached the level of precision as in, forexample, cardiology or orthopedics.Behavioral health conditions are definedby “clusters” of symptoms (e.g., as foundin the DSM-IV), and the technology avail-able to provide confirmations of diagnosesis less precise than in general medical care(e.g., X-ray, magnetic resonanace imaging,blood enzyme levels).
■ Heterogeneity of providers and varietyof treatment modalities and settings ismuch greater in behavioral health than ingeneral medical care. Behavioral healthcare providers include M.D. psychiatriststo Ph.D. psychologists, clinical nurse spe-cialists, psychiatric social workers, addic-
Special Report14

tion disorder treatment providers, andothers, all receiving different professionaleducations and with different preferencesfor how they approach and work withpatients. The range of treatment modali-ties spans psychoanalysis, problem-focused and insight-oriented psychothera-py (e.g., cognitive, behavioral),psychopharmacology, intensive inpatientcare and crisis management, and long-term treatment of severe mental illness.This heterogeneity relates to the “schoolsof thought” doctrine discussed above.
■ Compared to behavioral health, generalmedical health plans enjoy greater clarityand specificity as to the scope of coveredbenefits. The more clear and specific theterms of the contract are, the less likely itis that disputes will occur.
■ One interviewee cited greater antagonismfor managed care in behavioral healthprovider associations, which has led totheir encouraging members to file appealsin situations that they feel are questionable.
The officials from all three organizationsstated that requests for authorization of serv-ices are handled by clinical intake staff withat least a master’s degree, supplemented byongoing in-house training. The guidelinesused to “vet” a request for authorizationfocus on two criteria: a) level of care criteria(e.g., inpatient, partial hospitalization, outpa-tient therapy in individual or group settings),and b) treatment guidelines (e.g., crisis inter-vention, psychotherapy, prescription drugs).One MBHO preauthorizes 10 outpatientvisits, requiring the provider to request andjustify additional needed visits.
In all three organizations, board-certifiedor board-eligible staff psychiatrists mustreview all denied claims. The vast majority
of disputed claims arise for inpatient admis-sions. As one interviewee noted, in behav-ioral health, unlike general medicine, mostinpatient admissions are unplanned andoccur because a person (or family memberor provider on behalf of that person) seeksemergency crisis admission. Typically theinpatient facility calls for authorization.While the initial admission usually isapproved, disputes may arise over length ofstay, treatment plans, and care management.The interviewees stated that many of thesedisputes are later resolved when additionalinformation regarding the patient’s clinicalneeds is provided. If such information hadbeen provided at the outset, the claim wouldnot have been denied. Most claims disputesare resolved through internal appealsprocesses; only a few go to the externalappeals process.
Interviewees cited a variety of sourcesfor the treatment guidelines used in the caremanagement and review processes: amongthem guidelines developed by providerorganizations, such as the AmericanPsychiatric Association and the AmericanPsychological Association; guidelines prom-ulgated by accreditation organizations; andongoing feedback and advice from contract-ed providers. One MBHO reported the useof local clinical advisory committees in eachlocation, including subject matter specialists(e.g., addiction disorder providers) who pro-vide feedback and information on treatmentadvances. Guidelines are updated annuallybased on actual practice and expert opinion.
Interviewees stated that guidelines are notmandates or absolute protocols; rather, theyare considered “guideposts” to be informedby, and adapted to, individual circumstancesand psychosocial needs of patients. Ongoingaudits, performance measurement of in-house
Medical Necessity in Private Health Plans 15

care managers and contracted providers, andmember and provider satisfaction surveys areused to monitor the appropriate use of treat-ment guidelines in medical necessity decisionsand to build in quality improvements at alllevels of decisionmaking.
Managed Care AccreditationOrganizationsAccreditation organizations such as theNational Committee for Quality Assurance(NCQA) and the Joint Commission on theAccreditation of Healthcare Organizations(JCAHO) have not formulated a medicalnecessity definition. For example, NCQAofficials say they want to avoid conflicts withexisting laws governing the definition ofmedical necessity (Pawlson, 2002). Instead,the accreditation bodies focus on the medicalnecessity review process, including both uti-lization management and internal appeals.In addition, NCQA and JCAHO specify theexistence of an external appeals process as acondition of accreditation.
Figures 2 and 3 and Appendix B excerptutilization management and external appealsstandards promulgated by NCQA andJCAHO (JCAHO, 1997, 2001; NCQA,2000, 2001). NCQA’s procedural standardsfor MBHOs stress the individualization ofthe process. The entity must consider evi-dence from the individual patient’s case(as well as the characteristics of the localdelivery system) and therefore, presumablycannot rely on national treatment guidelinesfor specified conditions.15 NCQA standardsalso assume involvement of practitioners inthe development of criteria, though not nec-essarily in the evaluation of individual cases.
The JCAHO standards are written fromthe point of view of providers and providernetworks, typically the focus of JCAHO
accreditation. Standard CC 1 stipulates pro-vision of health care appropriate to the soci-ocultural needs of the provider’s patient pop-ulation and consistent with the provider’smission and contractual obligations, as wellas being based on an individual patient’sneeds. Disclosure of the review criteria usedin adverse determination decisions, timelynotice, and a review of adverse decisions bya physician, dentist, or behavioral clinicianprior to notification to the enrollee or pre-scribing provider are all required by JCAHO.
The JCAHO guidelines for MBHOs arevery similar to its general MCO guidelines.However, in some instances the MBHOguidelines are somewhat more explicit.Decisions regarding a member’s eligibilityfor entry into specific treatment programscan be interpreted as a frame of referencefor meeting medical necessity criteria.
CC 2.1: Criteria define the informationnecessary to determine a member’s eligi-bility for entry to a program or servicewithin the delivery system.
Intent of CC 2.1: The delivery system’scentral operations require care and serv-ice provider organizations to define theinformation necessary to determine amember’s eligibility for entry to a pro-gram or service. The care and serviceprovider organization defines the mini-mum essential information needed todetermine a member’s eligibility forentry to a setting or program. The cri-teria are based on the specific programor service that can meet or respond tothe member’s needs or presenting condi-tions. To add clarity, entry criteria alsoinclude exclusionary statements thatindicate the information needed to initi-ate referral to another, more appropriatecare and service provider organization.
JCAHO takes a condition/treatment-specific view for substance abuse services
Special Report16

Medical Necessity in Private Health Plans 17
NCQA Managed Behavioral HealthUtilization Management Standards
UM 2. To make utilization decisions, themanaged healthcare organization useswritten criteria based on sound clinicalevidence and specifies procedures forapplying those criteria in an appropriatemanner:
• The criteria for determining medicalnecessity are clearly documentedand include procedures for apply-ing criteria basedon the needs ofindividual patients and characteris-tics of the local delivery system.
• The managed healthcare organ-ization involves appropriate, activelypracticing practitioners in its devel-opment or adoption of criteria andin the development and review ofprocedures for applying criteria.
• The managed healthcare organi-zation reviews the criteria atspecified intervals and updatesthem, as necessary.
• The managed healthcare organi-zation states in writing howpractitioners can obtain the UM[Utilization Management] criteriaand makes the criteria availableto its practitioners upon request.
• At least annually, the managedcare organization evaluates theconsistency with which the healthcare professionals involved inutilization review apply thecriteria in decision making.
Figure 2: NCQA and JCAHO Utilization Management Standards
JCAHO Utilization Management Standards
CC 1: Health care services provided directly or by arrangement areappropriate:
• In scope to meet the health care needs of the population served;• To the health care needs, as influenced by socio-cultural
characteristics, of the population served;• To the network’s mission;• To the network’s contractual obligations.
CC 8: When the network or an external entity conducts a utilizationreview of a licensed independent practitioner’s or a network com-ponent’s care that results in denial of payment, decisions by thelicensed independent practitioner or network component regardingongoing care or discharge are based on the care required by themember’s assessed needs.CC 8.1: When utilization review results in an adverse utilization man-agement decision, the network provides the criteria for the decisionand information regarding appeal to the licensed independent prac-titioner responsible for the member’s care.JCAHO provides examples of implementation. “These examplesare simply ideas for your network to consider.”Example of implementation for CC 8: The network requests thereview criteria used by any external entity that carries out a utiliza-tion review on the network’s members. The review criteria are madeavailable to those within the network responsible for treatment anddischarge decisions. When the external utilization review organiza-tion’s recommendation conflicts with the member’s medical carerequirements, justification for the course of action taken is docu-mented. Information from the external entity is collected and incor-porated into the network’s assessment and improvement activities.RI 2: The network provides for member involvement in care andtreatment decisions.RI 2.1: The network provides an authorization process for care andtreatment that is timely, efficient, and meets member health careneeds.The network’s process for authorizing care and treatment includes:
• Providing members with a description of the treatmentauthorization process.
• Initial decisions made by an appropriately trained health careprofessional using evidence-based, network approved criteria toauthorize admission, care, and transition to another care setting.
• A review of all initial treatment authorization denials by aphysician, dentist, or behavioral clinician prior to notifying themember or their representative(s) of an adversedetermination.
• Informing members in a timely manner, in writing, when arequest to authorize treatment has been denied.
• Informing members of the basis and reason(s) for the adversedeterminations.
• Informing members of the review criteria used to make thedetermination.
• Providing members with information as to whether, and underwhat circumstances, investigational procedures are availableand are covered by the network.

Special Report18
Figure 3: NCQA and JCAHO External Appeals Standards
NCQA Managed Behavioral Health External Appeals Standards
UM 7.5 The managed behavioral healthcare organi-zation has a procedure for providing independent,external review of final determinations, including:Eligibility criteria stating that the MBHO offersenrollees the right to an independent, third party,binding review whenever:
• The enrollee is appealing an adverse deter-mination that is based on medical necessity,as defined by MBHO.
• The MBHO has completed two levels of inter-nal reviews and its decision is unfavorable tothe enrollee, or has elected to bypass one orboth levels of internal review or has exceededits time limit for internal reviews, without goodcause and without reaching a decision.
• The enrollee has not withdrawn the appealrequest, agreed to another dispute resolutionproceeding, or submitted to an external disputeresolution proceeding required by law.
• Notification to enrollees about the independ-ent appeals program and clear and timelyexplanations of denials and approvals toboth enrollees and their physicians.
Use of an independent review organization that meetsthe following criteria:
• Conducts a thorough review in which it consid-ers anew all previously determined facts,allows the introduction of new information,considers and assesses sound medicaladvice, and makes a decision or conclusionsthat are not bound by the decisions or con-clusions of the internal appeal.
• Has no material professional, familial, orfinancial conflicts of interest with the MBHO.
• MBHO non-interference with the proceedingsof the external review.
• Enrollee exemption from the cost of externalreview, including filing fees, and allowanceof designating a representative to act on thebehalf of the enrollee.
• Implementation of independent review organ-ization decision within specified timeframe.MBHO data tracking of external appeals foruse in evaluating its medical necessity deci-sion making process.
JCAHO External Appeals Standards
RI 2.2: The network provides a method for resolvingdisagreements between the network and the memberor designated decision maker(s) regarding care ortreatment authorization decisions.The network’s process includes:
• Informing members how to seek appeals ofadverse determinations.
• Defined timeframes in which the member cananticipate response to an appeal.
• Appeal timeframes that are appropriate to theurgency of the member’s health care needs.
• An appeal review panel including health careprofessionals who are appropriately trained,experienced, and competent with respect tothe care and treatment involved, and whowere not involved in the initial determination.
• Informing members about further steps avail-able when disagreements cannot be resolvedthrough the treatment authorization andappeal process, such as an internal grievanceprocess, arbitration, legal proceedings, andany other external review processes.
RI 5: The network provides for the receipt andresolution of complaints and grievances frommembers in a timely manner.The member has the right to voice complaints withoutfear of recrimination about the care received and tohave complaints reviewed and, whenever possible,resolved. This right and the way it is protected areexplained to the member. The network has a meansof providing for the following:
• Procedures for registering and managing com-plaints and grievances, including identifyingthe party receiving complaints and grievances.
• Aggregating and reporting actions taken oncomplaints and grievances.
• A timely response to the member, substantivelyaddressing the action taken on the complaintor grievance.
• Including the aggregate complaint and griev-ance information in performance improvementactivities.
• An appeal process for grievance decisions.• Member protection from any sanctions or
penalties resulting solely or primarily fromusing the complaint or grievance process.

as well. In discussing how an MBHO canprovide access to the appropriate level ofcare to meet an enrollee’s needs, it providesthe following example:
The alcohol/drug program of a commu-nity mental health center establishedseparate admission criteria for subpop-ulations. Separate criteria are in placefor alcoholism, cocaine dependence,dual diagnosis, and heroin dependence.Members are placed in levels and sitesof care in accordance with the primarysubstance(s) being abused.
In sum, neither NCQA nor JCAHO pro-vide prototypical medical necessity defini-tions but rather focus on the adequacy of thedecision processes used by the organizationsthey accredit. As is shown in the discussionof case law below, the procedures used tomake these decisions are as important as, andat times more important than, the structureand content of the definitions upon whichthey are based.
Judicial Case Law, OfficialInvestigations, and Legal ActionsSince the introduction of the concept of med-ical necessity into insurance contracts, count-less challenges have been made to insurerand health plan denials of coverage basedon medical necessity criteria. In deciding amedical necessity case, a court must construethe terms of an agreement; consequentlythese decisions offer a rich source of con-tractual medical necessity definitions, sincethe court’s opinion almost invariably setsout the relevant contract terms.
Judicial Case Law
Two types of medical necessity cases pre-dominate. The first type of case involveschallenges to the actual decision on themerits, with the claimant arguing that the
insurer’s conclusions about a treatment’smedical necessity are not supported by theevidence in the record. The second type ofchallenge goes to alleged flaws in the deci-sionmaking process, such as a decisionmak-er’s failure to follow applicable legal proce-dural standards in reviewing the case orconsidering the evidence. In all such casesthe claimant (i.e., the provider and/or thepatient) carries the burden of proving thatthe insurer’s decision was contrary to theterms of the agreement.
Other cases raise questions of medicalnecessity in a malpractice context. In suchcases, a managed care organization’s alleged-ly negligent treatment (and subsequent cover-age) decisions are claimed to be a proximatecause of death or injury. These cases typicallyappear in the case law at a threshold point(i.e., before there is any review on the meritsof the claim) and are decided on ERISA pre-emption grounds. For this reason, these casesare omitted from this review. Two of the bestknown managed care liability cases involvingbehavioral health services are Moscovitch v.Danbury State Hospital (1998) and Lazorkov. Pennsylvania Hospital (2000). Both casesinvolved suicides by individuals covered byERISA health plans. The patients wereordered to be discharged from treatment fol-lowing a determination by the MCO thatcare was not medically necessary. Both caseswere permitted to proceed as malpracticeactions after a judicial determination that theclaims in question fell outside of the scope ofERISA because they raised issues of State lawprofessional liability rather than ERISA cov-erage claims.
For this review, an online search wasconducted for all cases decided since 1992involving challenges to medical necessity cov-erage decisions. The search was confined to
Medical Necessity in Private Health Plans 19

the past decade in order to avoid examiningcontracts whose terms may be significantlyoutdated. A total of 54 medical necessitycases were identified, 21 of which involveappeals by insurers and health plans seekingreversals of treatment orders issued by lowercourts, and 33 of which are cases broughtby providers and patients that seek toreverse a claims denial. Insurers are slightlymore likely to prevail in these cases with29 of the 54 cases decided in favor of theinsurers while in only 25 of the cases theinsurers’ denials were reversed. A summaryof all of the cases reviewed can be found inAppendix C.
The fact that insurers are somewhat morelikely to prevail in medical necessity casesmay reflect the merits of their decisions. Itmay also reflect the difficulties claimantsencounter in challenging a medical necessitydenial. For example, the plaintiff carries theburden of proof and generally is barred fromintroducing new medical evidence on appeal,since review is limited to the evidentiaryrecord before the court. Thus, if the insureror plan failed to consider certain evidenceor misconstrued the evidence before it, theplaintiff typically cannot rectify the short-coming in court. Furthermore, under prin-ciples of contract and trust law (the twobodies of law that apply to decisions oncoverage in the case of employee healthplans) (Firestone Tire and Rubber v. Bruch,1989), insurers and health plan administra-tors are vested with considerable power todecide whether contract beneficiaries areentitled to the benefits they seek. A court’sscope of review is therefore limited underjudicial principles, and a court will generallyscrutinize a record closely if it considers theinsurer or plan to have a clear conflict of
interest that has colored its views (Bedrickv. Travelers Ins. Co., 1996).16
Of the 54 identified cases, 28 contain adefinition of medical necessity (Table 3).Jones v. Kodak Medical Assistance Plan(1999), not included in Table 3 but summa-rized in Appendix C, is the leading case forthe proposition that insurers have the powerto contractually limit the types of necessarytreatments they will cover by building theirguidelines directly into the structure of theplan documents. As a result, Jones, whichconcerned treatment of alcoholism, con-tained no medical necessity definition per sebut instead a provision construed by thecourt as limiting treatment to the guidelinesused by the managed behavioral healthsubcontractor.
Other cases shown in Table 3 containa more traditional definition of medicalnecessity and reflect the multidimensionalapproach seen in Table 2. This finding sug-gests that rather than being isolated events,the multidimensional definitions found inTable 2 are the prevailing industry standard.That is, the insurance industry today uses anapproach to defining medical necessity thatgoes beyond assessing whether treatmentmeets a professional standard of care andpermits the insurer to select among thetreatments that ostensibly are all appropri-ate in favor of one that is the safest, theleast costly, and not only for the conven-ience of the member or provider.
Four of the definitions drawn from thecase law contain an explicit reference to thesite of care, identifying treatment delivery inoutpatient settings as preferable to inpatientcare (Dettmer Clinic v. Associated InsuranceCompanies, Inc.; Kornman v. Blue CrossBlue Shield of Louisiana; Milone v. ExclusiveHealth Care, Inc.; Scalamandre v. Oxford
Special Report20

Health Plans, Inc.). For example, in the 1995case Kornman v. Blue Cross Blue Shield ofLouisiana, the insurer’s third criterion formedical necessity was as follows: “as toinpatient care, could not have been providedin a Physician’s office, in the Outpatientdepartment of a Hospital, or in a lesserfacility without affecting the patient’s condi-tion or quality of medical care rendered.”17
Forty-two of the 54 cases reviewed—thesingle largest subgroup—involved a challengeto a medical necessity determination basedon a treatment exclusion clause or an allegedflaw in the insurer’s decisionmaking process-es. Twenty-two cases focused on exclusionsbased on the allegedly experimental status ofthe requested treatment and thus dealt withthe proper application of an exclusionaryterm rather than a medical necessity denialon the merits. Twenty cases involved allega-tions that the insurer improperly applied thedefinition in its determination procedures.Plaintiffs most typically alleged that theinsurer acted in an arbitrary or capriciousmanner by unfairly denying claims in somecases while approving them in equivalentcases.
Four of the 54 cases involved mentalhealth and substance abuse services (Heilv. Nationwide Life, Koenig v. MetropolitanLife, Burrell v. United Health Care Insurance,and Jones v. Kodak Medical AssistancePlan). The Heil and Burrell cases involveddenials of inpatient hospitalization for amental condition, and the Koenig and Jonescases involved denial of substance abusetreatment services. All four were concernedwith alleged flaws in the insurers’ determi-nation procedures.
Investigations and Official Legal Actions
In addition to cases decided in courts of law,State attorneys general and bureaus of insur-ance have responded to complaints filed byproviders and patients regarding adversedeterminations based on MCOs’ medicalnecessity criteria. In New York, Maine, andConnecticut, official investigations werelaunched in response to alleged instances ofarbitrary and capricious decisionmaking,inconsistent application of criteria, failure tomeet disclosure requirements, and conflictsof interest on the part of MCO decisionmak-ers. In New York and Maine, MCOs enteredinto settlement agreements with the States;in Connecticut, an MCO’s alleged abusesformed the basis for remedial legislation.Figure 4 summarizes the most commonproblems identified from these investigationsof the procedures used by health plans andinsurers to make medical necessity determi-nations, followed by descriptions of each ofthese States’ legal actions.
New York
The series of October 2001 settlement agree-ments reached between the New York StateAttorney General’s Office and six largeMCOs was a significant legal developmentregarding medical necessity.18 Following a2-year investigation into how these MCOsinformed their providers and enrollees ofadverse determination decisions on thegrounds of medical necessity, the AttorneyGeneral found that these MCOs were not incompliance with New York State’s utilizationreview law (discussed in more detail in PartV below). The focus of the investigation wason the processes used by the MCOs to makedeterminations and to inform providers andenrollees, rather than the content of the med-ical necessity definitions themselves. The
Medical Necessity in Private Health Plans 21

Attorney General’s office found, for example,that MCOs were often denying authorizationor reimbursement for inpatient mental healthand substance abuse treatment and offeringnothing more than a generic explanation thatthe service was “not medically necessary.”There was often no disclosure of the under-lying reasons or clinical rationale the MCOsused in making their decisions, which isrequired in New York’s utilization reviewlaw (see Appendix D for more details).
A representative of the New YorkAttorney General’s Office indicated thatalthough their investigation did not reviewthe underlying substance of claims deniedowing to medical necessity, behavioralhealth patients appeared to be more vulnera-ble to abusive medical necessity practicesthan patients with physical conditions. Inthe representative’s view, medical necessity isharder to define and measure in behavioralhealth. The representative cited New York’sutilization review law as an effort to over-come this difficulty by ensuring that all
patients receive individualized medical neces-sity decisions based on specific clinical factsand individualized assessments. Despite thisstatute, the New York Attorney General’soffice continues to receive complaints fromproviders and patients regarding the medicalnecessity decision process used by MCOs inbehavioral and physical health cases.
The Attorney General’s Office representa-tive cited the lack of a uniform medical neces-sity definition in State insurance laws as themost significant problem in medical necessitydecisionmaking and investigation of abusivepractices. External appeal statutes, utilizationreview regulations, and other insurance lawsuse medical necessity definitions and stan-dards that are often conflicting or confusing.No uniform criteria are required. As a result,each health plan uses its own definition, andthis variation makes regulation of medicalnecessity practices difficult.
Special Report22
Figure 4: Common Procedural Problems in Medical NecessityDetermination Processes Noted in Investigations, Litigation, and Case Law
• Decision made in arbitrary or capricious manner without consideration of individual patient needs• Decision made inconsistently (i.e., some patients’ claims denied while others in equivalent circumstances
approved)• Claims reviewers unqualified or not appropriately trained• Application of arbitrary and unreasonable caps on coverage and/or dollar limits• Insufficient information provided in claims denials:
– No disclosure of clinical rationale used in making decision– No disclosure of qualifying credentials of reviewer– No disclosure of evidence or documentation used in decision– No description of the procedures, timeframes, and consumer rights for grievance and appeal
• Failure to consult with treating physician• Failure to consider medical evidence provided by patient• Failure to provide full and fair review to patient appealing claims denial• Lack of clarity and specificity in plan documents of excluded services (e.g., definitions of “experimental,”
“convenience”)• Conflict of interest of MCO decisionmaker that biased impartial judgment

Maine
In 2000, both United Behavioral Health andCigna Behavioral Health, Inc., entered intoconsent agreements with the Maine Bureau ofInsurance.19 These agreements were reachedas a result of complaints filed with the bureauby health plan enrollees concerning denials ofcoverage based on medical necessity grounds.The bureau determined that the denials werenot in conformance with Maine rules regard-ing utilization review (see Appendix D formore details).
A representative from the Maine Bureauof Insurance indicated the potential for med-ical necessity abuses is similar in the physicaland behavioral health care contexts, but thatbehavioral health medical necessity determi-nations in Maine are qualitatively differentfrom those in other jurisdictions. Both therural character of the State and generalshortage of behavioral health care providershave a significant effect on the application ofmedical necessity criteria. For example, thereis only one practicing psychiatrist inWashington County, which has a populationof over 30,000 people. Since outpatient set-tings are scarce, national MCOs that dobusiness in Maine often apply medical neces-sity and “appropriate setting” criteria toresist coverage of inpatient behavioral healthtreatment, sometimes all that is available incertain regions of the State.
The paucity of providers also affects griev-ance procedures. Maine requires MCOs tooffer an independent medical review as partof their internal grievance process (it also hasan external review statute for further appealsafter the internal process has been exhaust-ed). The shortage of providers leads MCOsto find reviewers from other jurisdictions.These reviewers often question the medicalnecessity or appropriateness of inpatient
behavioral health care even though outpatientcare is not available or not practical owingto distance. Maine consumers and providersfile complaints with the Bureau of Insuranceover these issues and the general shortage ofbehavioral health care providers and services.
Maine’s Insurance Code contains a defi-nition of “medically necessary health care,”and according to the representative, insur-ers generally appear to understand thedefinition and the statute’s process require-ments (despite the frequent struggle overinpatient behavioral health services). Therepresentative indicated that several high-profile consent agreements with insurersthat failed to follow Maine’s definition orprocess requirements have had a deterrenteffect on other insurers.
Connecticut
A recent case that dramatically highlights thepotential for misconduct in the area of med-ical necessity decisionmaking by health plansinvolves an investigation conducted by theConnecticut Attorney General into the activi-ties of the State’s largest insurer, AnthemBlue Cross/Blue Shield, and its subcontractor,Psych Management, Inc. (PMI). In a widelydisseminated report issued in February 2002,the Attorney General reported that AnthemBlue Cross/Blue Shield (which enrolls600,000 State residents), prompted bydesires for significant savings and profitmaximization, contracted with PMI toadminister the behavioral health componentof its product line following a notably lowproject bid. The investigation found thatPMI’s president had serious financial con-flicts of interest and engaged in inappropriateuse of aggressive utilization management anddenials of medically necessary care solely to
Medical Necessity in Private Health Plans 23

improve PMI’s profit margin (Blumenthal,2002) (see Appendix D for more details).
A representative of the ConnecticutAttorney General’s Office indicated that theirinvestigation showed that the potential forabuses of medical necessity is greater in thebehavioral health context than in physicalhealth cases. In the view of the office, notonly is it harder to define what is medicallynecessary in behavioral health, but thepatients involved are more vulnerable andpolitically weak. In addition, the representa-tive indicated that the behavioral healthprovider lobby in Connecticut is relativelyweak and not effectively organized.
The Connecticut Attorney General’s officereceives more complaints from providers andconsumers regarding behavioral health care
than physical health care. The complaintsinclude a failure to pay claims in a timelymanner, arbitrary coverage denials (citingmedical necessity), and difficulties in findingbehavioral health providers due to out-of-date provider lists given to consumers(commonly known as “phantom panels”).
Finally, the representative indicatedthat the arbitrary financial goals, phantompanels, and lack of regulatory oversightof subcontractors are the most pressingproblems they found during their investi-gation. The Connecticut Department ofInsurance has taken the position thatthe State’s laws regulating managed carepractices do not give the departmentjurisdiction over subcontractors.
Special Report24

V.In their capacity as insurance regulators, States have developed an
extensive body of law related to the insurance industry. State lawsfall into two basic categories: laws that regulate the actual content
of the insurance contract itself (e.g., mandated benefit laws); and lawsthat regulate other aspects of the business of insurance (e.g., consumerprotection laws, antidiscrimination law, corporate law, laws providingfor oversight of insurance practice, and administrative and judicial reviewof insurer determinations). This section examines two types of State insur-ance laws that address medical necessity: insurance contract statutes andlaws that establish independent review procedures for medical necessitydeterminations.
State Law Regulationof Medical Necessity
Laws That Regulate the Contentof Insurance ContractsIn addition to detailing specific classes ofbenefits and services that must be includedin a contract of insurance sold in the State(e.g., pediatric immunizations, in vitro fer-tilization, inpatient psychiatric care),20 anumber of States have attempted to definemedical necessity. This effort to define med-ical necessity by statute is relatively recentand tracks the growth of (and backlashagainst) managed care. It probably would beincorrect to view the evolution of medicalnecessity definitions in State law solely inthe context of consumer protection. Indeed,codifying a medical necessity definition instatute actually might favor the industry,since once a statutory definition exists, acourt cannot insert its own definition intothe contract. Today it is still relatively com-mon to find insurance contracts that author-ize an insurer to decide issues of medical
necessity without a precise definition of theterm.21 In the face of this silence, a courtcan fashion its own definition under com-mon law principles of jurisprudence.22 Inso doing, a court might be inclined to useprinciples of professional liability law toarrive at a definition and adopt a standardthat measures the recommended treatmentagainst accepted standards of professionalpractice, as established through the testimo-ny of experts.23
The absence of a medical necessity defi-nition can be as harmful to insurers as itmight be to patients. In this situation, itwould be in the interest of the industry aswell as consumers to adopt a definition,particularly if the definition adopted ismultidimensional, giving the insurer dis-cretion to select among competing schoolsof thought in accordance with criteriaother than whether the treatment meetsprofessional standards of practice.
Medical Necessity in Private Health Plans 25

Seventeen definitions of medical necessitywere found in the course of this review.Table 4 sets forth these definitions, whichvary considerably in length and scope.For example, at one end of the spectrum,Massachusetts defines medical necessity as“health care services that are consistentwith generally accepted principles of pro-fessional medical practice.”24 At the otherend, Hawaii offers:
A health intervention is medicallynecessary if it is recommended by thetreating physician or treating licensedhealth care provider, is approved bythe health plan’s medical director orphysician designee, and is: (1) For thepurpose of treating a medical condi-tion; (2) The most appropriate deliveryor level of service, considering poten-tial benefits and harms to the patient;(3) Known to be effective in improv-ing health outcomes; provided that:(A) Effectiveness is determined first byscientific evidence; (B) If no scientificevidence exists, then by professionalstandards of care; and (C) If no pro-fessional standards of care exist orif they exist but are outdated or con-tradictory, then by expert opinion;and (4) Cost-effective for the medicalcondition being treated comparedto alternative health interventions,including no intervention. For thepurposes of this paragraph, cost-effective shall not necessarily meanlowest price.25
It is evident that Hawaii’s definitionapproximates those found in modern indus-try practices, while Massachusetts’s defini-tion tracks the unidimensional standardthat limits the authority of the industry tochoose among equally appropriate typesof treatments. Of special note is the factthat Hawaii’s definition, enacted in 2000,is virtually identical to the prototype defi-
nition proposed in 1999 by Singer et al. (seePart 1 and Table 1).
Independent Review StatutesBy 2002, 40 States and the District ofColumbia had enacted external review lawsthat allow enrollees to appeal to an inde-pendent review organization (IRO) healthplan decisions to deny, reduce, or terminatecare. Nearly half of these States have draftedregulations pursuant to their IRO statutes.26
Table 5 lists the statutory and regulatorycitations of these laws.
External review laws are a recent develop-ment. Only Michigan (1978) and Florida(1985) had external review statutes prior to1990. By 1998, the number of statutes hadgrown to 13 (Dallek & Pollitz, 2000), withthe remaining 28 statutes enacted within thepast 4 years.
IRO statutes and administrative regula-tions raise, and try to answer, many ques-tions. This section focuses on questions inthree critical areas that courts consider tobe basic issues of fairness in decisionmaking:(1) whether the States are tailoring statutesspecifically to address appeals of denialsinvolving behavioral health care; (2) the keyprocedural elements of the statutes, includingwho may serve as an IRO and the qualifica-tions of IRO reviewers (including the posses-sion of expertise relevant to the case underreview); and (3) how much deference theIRO must give to the initial decision andwhether new evidence may be introducedduring the IRO review. In addition, thestatutes were reviewed to determine whetherthey specify who has the burden of proofin the appeal (i.e., whether the insurer mustpresent evidence defending its initial decisionor the claimant must present evidence tochallenge it). Only one State, Maryland,
Special Report26

addresses the specific burden of proof andplaces it on the MCO to demonstrate thatits initial adverse decision was correct.27
In States that regulate the definition ofmedical necessity under their insurance con-tent statutes, the IRO presumably would beguided by this definition. Among States thatdo not have a definition of medical necessityin their insurance laws but that have enactedIRO statutes, seven include a definition ofmedical necessity in the IRO statute itself.Table 6 lists these States and the definitionof medical necessity that they have adoptedfor IRO purposes.
Only two States, Pennsylvania andVermont, specifically mention behavioralhealth care in their IRO statutes.28 Table 7sets forth the relevant provisions from Statelaw. Pennsylvania’s statute identifies licensedpsychologists as qualified reviewers; Vermontspecifies an independent review system forappeals involving mental health services andsubstance abuse treatment. While most StateIRO statutes use broad language that couldinclude a range of providers to review behav-ioral health determinations, the Vermontstatute is unique in its explicit recognitionof behavioral health reviewers.
The independent reviewer: Who, howchosen, and what qualifications? Central tothe process of obtaining external review arequestions about who performs the review,how the reviewer is chosen, and what qualifi-cations the reviewer possesses. Table 8 setsforth information on the review process. All41 statutes provide some detail about whatentities qualify to perform IRO functions.Most States require that the IRO obtain certi-fication or a license from the State insuranceor health department, and many States useaccreditation by a national accrediting organ-ization as a proxy for State certification.
Thirty-seven of the 41 States require thatreviewers used by the IRO have appropriatelicense, board certification (if applicable),and experience in the medical condition orhealth care service under review. Of theremaining four States, three do not specifysuch a requirement, and the last makes uti-lizing relevant expertise an option “whennecessary,” but does not define when thatis or who makes that determination.
In seven States, the MCO chooses theindependent review organization to performthe review (either from an approved insur-ance/health department list or from any qual-ified IRO). The insurance or health depart-ments assign the reviewer in the remainingStates. A number of States require a rotationof the IRO so no MCO is reviewed by thesame organization for every case.
Thirty states disqualify an IRO fromserving as a reviewer if the entity has finan-cial or other conflicts of interest with theparties to the case. Nine of the 11 remainingStates do not explicitly prohibit conflicts,and one State requires only that the conflictbe disclosed.
Standard of review and permissible evi-dence: Table 9 addresses the issue of stan-dard of review, identifying those States inwhich review is de novo (i.e., brand new)and those in which additional evidence ofnecessity can be submitted. The standardof review specifies how much deference,if any, the IRO should or must give to theprior decision made by the MCO. In ade novo review, the IRO is not bound atall by an earlier decision and no deferenceis required. Six States accord this absolutereview power to their IROs. Few Statesspecify any level of review short of denovo, and the majority of State IROstatutes and regulations are silent on
Medical Necessity in Private Health Plans 27

what standard of review to apply to priordecisions by the MCO.
Twenty-seven of the States permit theenrollee requesting the review to submitadditional evidence for consideration by theIRO. The statutes range from allowing spe-cific additional medical evidence to allowingany evidence the enrollee considers relevantto the appeal. Three States allow the enrolleeto request or attend a review hearing.
Additional process questions: The statutesand regulations compiled in this reviewcontain additional process questions worthnoting. Most States require an enrollee toexhaust an MCO’s internal appeals processbefore filing a request for external review,but there are notable exceptions. SomeStates require a preliminary review by thedepartment of insurance or IRO to deter-mine whether the request is eligible forreview. Many States require the enrolleeseeking review to pay a filing fee. MostStates require the MCO to pay the cost ofeach appeal, but other States have assessed afee for each MCO operating in the State tocover the costs of the entire appeals system.Almost every statute includes detailed time-lines for filing requests for appeal andresponses, and some States require that theappeal be filed on specific forms. Whilenone of these process questions answer largequestions, taken together, they allow anexamination of the burdens that enrollees
face when attempting to invoke the right toan external review.
Viewed as a whole, State independentreview statutes suggest a desire on the partof States to afford insured persons a rightto a second opinion in the case of medicalnecessity determinations. While State insur-ance law contains minimal regulation ofinsurers’ internal utilization managementand internal appeals processes, these statutessuggest that States are willing to establishminimum standards for how insurer deci-sions are to be reviewed, including absolutereview powers, impartial reviewers, andthe authority to consider new evidence inreviewing a medical necessity determination.Few IRO statutes contain independentdefinitions of medical necessity, althoughthe State’s content definition presumablywould apply where one exists.
The power of the procedural standardsto support the overturning of a denial maybe somewhat limited, however. For exam-ple, if the definition of medical necessitygives the insurer discretion to select fromamong several professionally acceptablecourses of treatment, one would expectan independent reviewer to uphold theinsurer’s decision unless it was not sup-ported by the evidence (i.e., the insurer’schoice among selected treatments was notgrounded in sufficient evidence to justifya rejection of other choices).
Special Report28

VI.
This part considers two sources of law relevant to medicalnecessity determinations. First, two sets of Federal standardsgoverning employee health plans are examined. The first set of
standards is embodied in the regulations promulgated by the Departmentof Labor in 2000 that set forth the “full and fair review” proceduralrequirements that all ERISA health benefit plans must meet. The secondset is embodied in the standards governing medical necessity reviews thatare currently in use by the U.S. Office of Personnel Management.
Relevant FederalLaws Pertaining toMedical NecessityReviews
ERISAThe ERISA statute regulates health and wel-fare benefits for more than 140 million work-ers and their families (Rosenbaum, Frankford,Moore, & Borzi, 1999). ERISA requires everyhealth benefit plan within its scope to provideadequate notice in writing to a participantwhen a claim is denied, “setting forth the spe-cific reasons for such denial, written in a man-ner calculated to be understood by the partici-pant.”29 In addition, ERISA affords a healthplan member whose claim has been denieda “reasonable opportunity . . . for a full andfair review by the appropriate named fidu-ciary of the decision denying the claim.”
In November 2000, the Department ofLabor issued final regulations that revise thefull and fair review requirements for appealsof denials of claims for health benefits,including both retrospective and prospective
claims. These regulations became effectivefor group health plans on July 1, 2002.Although ERISA does not define medicalnecessity or provide a right to externaladministrative review,30 these regulationsestablish extensive standards for internalreviews required in the case of healthclaims.31
The November 2000 regulations requireERISA-covered plans to “establish andmaintain reasonable procedures governingthe filing of benefit claims, notificationof benefit determinations, and appeal ofadverse benefit determinations.”32 A plan’sclaims procedures must safeguard and verifythat claims are made in accordance withgoverning plan documents and that planprovisions are applied consistently forsimilarly situated claimants.
Medical Necessity in Private Health Plans 29

The full and fair review regulations wereintended to make the claims process “faster,fairer and fuller.” With respect to the speedof the process, the regulations shortened thepermissible time for initial claim decisionsand appeals. Instead of 90 days under theprior applicable regulation, the November2000 rule requires initial decisions in 72hours for urgent care claims, 15 days forpre-service claims, and 30 days for post-service claims.33 Health plans are allowedone 15-day extension for pre- and post-service claims. On appeals of denied claims,instead of 60 days under the prior applicableregulation, the new regulation requires deci-sions on appeals within 72 hours for urgentcare claims, 30 days for pre-service claims,and 60 days for post-service claims. Thereare no extensions of time for health plansin determining appeals.34
Under the “fairness” category, the regula-tion allows claimants more time to file anappeal (180 days instead of 60 under theprior regulation). The decisionmaker cannotbe the same person who denied the initialclaim or that person’s subordinate. Theclaimant also has the opportunity to submitwritten comments, documents, records, andother information related to the claim, andthe review must take into account all infor-mation submitted by the claimant (whetheror not the information was considered inthe initial benefit determination).35
If the appeal involves a decision basedon medical judgment, including whetheran item or service was medically necessary,the health plan must consult with a “healthcare professional who has appropriatetraining in the field of medicine involved inthe medical judgment.” The health careprofessional must not have been involvedwith the initial decision or be a subordinate
of the initial decisionmaker. Upon request,the health plan must disclose the identity ofthe health care expert it consulted. Healthplans cannot require more than two levelsof internal review of denied claims, and ifthere are two levels, both levels must becompleted within the time frames requiredof one level.36
The “fullness” category relates toimproved access to information by personsappealing an adverse determination. Asan initial matter, the plan must provide allplan members with a full description ofthe plan’s claims and appeals procedures.Claimants appealing an adverse determina-tion must have access to any informationrelevant to their claim upon request andfree of charge. Relevant informationincludes any information the health planrelied on in making the initial decision;any information submitted, considered, orgenerated while making the initial decision;and any statements of policy or guidanceconcerning the denied treatment or benefit,even if such documents were not reliedupon in making the decision.37 In addition,when a health plan denies a claim basedon a protocol or guidelines, the plan mustdisclose such reliance and inform theclaimant that a copy of the protocol isavailable upon request. Similarly, when thedenial is based on medical necessity, therule requires the plan either to explainthe scientific or clinical judgment used inapplying the plan’s terms or to include astatement that such an explanation willbe provided free of charge if requested.38
With disclosure of protocols and explana-tions of the application of medical necessity,the Federal full and fair review regulationsexceed the reach of State utilization andindependent review statutes and regulations.
Special Report30

Office of Personnel ManagementStandards: FEHBPAnother relevant Federal law establishesseparate standards for reviewing claimsinvolving the denial of medical necessity forFederal employees. The Federal EmployeesHealth Benefit Plan (FEHBP)39 provideshealth insurance coverage to more thannine million Federal employees and theirdependents. The U.S. Office of PersonnelManagement (OPM), which contracts withhealth plans to serve Federal employees,administers the FEHBP.
Neither the FEHBP statute nor its imple-menting regulations define “medical necessi-ty” or how health plans are to make suchdeterminations. The FEHBP regulations,however, do offer enrollees a right to appealto OPM if the health plan denies a claim asecond time after reviewing its first denial orif it fails to respond to an enrollee’s requestfor reconsideration of a claim’s denial.40 Theenrollee must exercise the right to appealwithin 90 days of the health plan’s decision,or within 120 days of the request for recon-sideration if the health plan failed torespond. In reviewing the claim denied bythe health plan, OPM may (1) request thatthe claimant submit additional information;(2) obtain an advisory opinion from anindependent physician; (3) obtain any otherinformation it believes is required to make adecision; or (4) make its determination basedsolely on the information the claimant sub-mitted with the request for OPM review.41
Neither the OPM statute nor its implement-ing regulations specify the standard OPMis to use in reviewing denied claims. If aclaimant wishes to sue, the suit must be filedin Federal court to review OPM’s final actionon the claim, but the claimant is limited toERISA remedies. The suit must be broughtagainst OPM, not the health plan or itscontractors, and a recovery in such a suitis limited to a court order directing OPM torequire the health plan to pay the amountof the benefits in dispute.42
Figure 5 presents the key elements of med-ical necessity review and compares ERISAprocedures with those established by OPM.
Although the ERISA full and fair hearingregulations and the FEHBP provide furtherprocedural safeguards to health planenrollees, both have important limitations.The ERISA regulations do not contain aright to an external appeal, despite providingimportant additional access to informationand better claims procedures not previouslyavailable. The FEHBP, limited to Federalemployees, provides a right to appeal outsidethe health plan to the OPM or to Federalcourt if necessary, but, as with ERISA plans,monetary damages are limited to paymentfor the cost of the denied benefit itself (i.e.,punitive and “pain and suffering” damagesare not available).
As a result of the modest reach of Federallaw, the definition of medical necessity isstill governed by the terms of the contractnegotiated between buyers and sellers.
Medical Necessity in Private Health Plans 31

Special Report32
Figure 5: Medical Necessity Utilization Review and Appeals Procedures
Issue ERISA FEHBP
Standards for initial utilization review process ✓
Standards for internal appeals of initial denials ✓
Timelines ✓ ✓
Qualifications of reviewer ✓
De novo review ✓
Evidentiary standards ✓
Access by claimant to health plan evidence ✓
Treatment guidelines ✓
Definition of medical necessity
External de novo administrative review of health plan decision

VII.As recently as 30 years ago, health professionals had virtual
autonomy to determine whether health care was medical-ly necessary. Today the evidence suggests that this autono-
my had a profound impact on both health care cost and quality. Aftertentative incursions on decisionmaking through retrospective utilizationreview, the health insurance industry has moved to prospective reviewand has developed increasingly tight coverage provisions and definition-al terms. Some commentators such as Eddy, Singer, and Bergthold havefocused on the importance of scientific evidence in decisionmaking.Others such as Rosenbaum and Frankford have readily acknowledgedthe need for external review of clinical judgment.
Synthesis andImplications
The evidence presented in this literaturereview suggests that the modern definitionof medical necessity is multidimensional andturns only in part on the consideration ofwhether the treating professional’s recom-mendations fall within professionally accept-ed standards. Whether in State statutes,insurance contracts, case law, or peer-reviewed literature, the modern medicalnecessity definition assumes external controlof the ultimate decision. Furthermore, rela-tively widespread consensus has beenreached that the definition of medical neces-sity should have certain specific dimensions.
The first dimension (and the one that ismost embedded in the structure of the agree-ment itself and often the most elusive) is bestthought of as contractual scope. Does theagreement cover treatments that preventworsening and maintain or promote func-tioning, or is the agreement limited to treat-ments that show recovery or at least signifi-
cant improvement in the short term?43 Thesecond dimension is the professional stan-dard. Is the treatment in accord with profes-sional standards of care in the relevant areaof practice? The third dimension can bethought of as patient safety and setting. Isthe prescribed treatment gauged to be deliv-ered in the safest and most effective setting?The fourth dimension is that the treatmentbe medical and not a convenience matter orone that emanates from social or environ-mental factors.
The fifth dimension is cost. Here, however,most of the definitions (and the literature aswell) are vague on exactly what is meant bycost. Ford (2000) attempts to grapple withwhat is meant by cost, emphasizing long-termover short-term in order to permit coverageof care and services that, while not capableof producing immediate improvements, showlong-term payoff. At this point, of course,one begins to cross over from questions
Medical Necessity in Private Health Plans 33

related to the necessity of covered services tothe underlying issue of coverage itself, sincecoverage may be structured to categoricallyexclude services of certain duration or ser-vices that do not show recovery or significantimprovement within a brief period of time.
One of the notable aspects of this reviewis that there is little to suggest that healthinsurers, State legislators, accreditationbodies, or the experts consider behavioraldisorders to be so unique that the generalmultidimensional test used to measure med-ical necessity is not appropriate. A numberof commentators call for a broadening ofcoverage to include services related to thetreatment and management of chronic condi-tions, where the goal is to attain or maintainfunctioning over the long term. Such goalscan be thought of as a form of significantimprovement: attaining the ability to func-tion better can be thought of as a significantimprovement in the case of individuals withserious and chronic behavioral health disor-ders. But the improvement in such cases isnot on a “recovery” trajectory (in the sensethat the insurer may equate “recovery”with “leading to cure”) and so may continueto fall outside the scope of coverage. Thisrepresents an inconsistency with treatmentfor many persons with severe mental illness,wherein recovery, as evidenced by improvedfunctioning, is a primary treatment goal.
The evolution of a multidimensional defi-nition of medical necessity reflects the prob-lems inherent in a standard that measuresthe proposed treatment simply against theprevailing standard of care. As the schools-of-thought doctrine in liability law under-scored, the professional standard is built oncustom, practice, clinical observation, andconsultation and may embody several possi-ble approaches to a single condition. Were
an insurer to seize on one school of thoughtto the exclusion of all others, its determina-tion would be vulnerable on appeal. Evenif the plaintiff carries the burden of proof,it is possible to introduce evidence showingthe full range of possible and professionallyappropriate approaches to a particularproblem, thereby undermining the insurer’sinsistence on one particular approach.
The modern definitions found in theindustry’s own materials, the case law, Statestatutes, and the literature all point to anemerging standard of medical necessitythat effectively permits an insurer or healthplan vested with decisionmaking discretionto select among a series of professionallyaccepted approaches to care and to choosethe approach that best satisfies other con-siderations, including cost, safety, and con-venience factors. This power to choose onespecific approach to treatment, as opposedto being obligated to recognize the fullrange of treatments that fall within theprofessional standard of care, is the essenceof what separates the modern definitionfrom its predecessors.
Furthermore, depending on how thedefinition is drafted, an insurer or healthplan can exclude all evidence from itsconsideration other than evidence gleanedfrom certain sources of information suchas randomized controlled studies (Harrisv. Mutual of Omaha Co., 1993).
This shift to a multidimensional test ofnecessity can be expected to affect any condi-tion where there are multiple professionallyrecognized approaches to the treatment ofany particular condition. Because profes-sional opinion varies to a disproportionatedegree in the area of behavioral health, theissue of medical necessity has generatedheightened attention in this area. However,
Special Report34

experts in behavioral health who write aboutmedical necessity do appear to advocate adefinition that allows a decisionmaker toselect among competing approaches inaccordance with numerous other factors.
The cost dimension of the modern med-ical necessity definition also may have anespecially strong impact in behavioral healthif treatments for such illnesses vary widely incost. A course of treatment that emphasizesprescribed medications and brief therapymay have radically different costs from onethat is long-term and emphasizes psychother-apy over medication. Similarly, a require-ment of prior failure as a precondition tothe use of more expensive prescription drugtherapies may have a greater impact inbehavioral health, depending on the cost ofemerging medication treatments comparedto existing treatments. A corollary consider-ation is that of consumer choice, which israrely, if ever, addressed in medical necessitydefinitions except in the context of exclu-sions for “convenience.”
The concept of convenience is a difficultone. For example, could a “fail first” policybe designed to limit “convenience” treat-ments for patients and thus be a basis fordenying access to emerging and professional-ly accepted treatments? There has been arapid increase in the development of a newgeneration of psychopharmaceuticals used totreat unipolar and bipolar depression, anxi-ety, schizophrenia, and alcohol and opiateaddictions. These drugs have usually beenfound in clinical development testing to havegreater effectiveness and fewer negative sideeffects than previous drugs, thus increasingthe likelihood that patients who use themwill be able to adhere to the treatment regi-men. Since these drugs are new to the marketand not yet widely prescribed, they are typi-
cally relatively expensive. A “fail first” testused as part of the convenience or costdimension of the medical necessity reviewwould result in a denial of access to certainadvanced medications. The impact of thisdecision might extend beyond the immediatedenial of certain forms of recognized treat-ment. Because the modern medical necessitydefinition turns in part on what is the accept-ed treatment, the fact that insurers andhealth plans reject use of the treatment ona widespread basis may lengthen the delaybefore the treatment becomes “accepted.”
The evidence also shows a consensus inthe law and literature for an independentreview of an insurer’s medical necessity deci-sion. More than 40 States have enacted leg-islation that, to varying degrees, establishesan independent review process and the abili-ty to introduce additional relevant and reli-able evidence. While the burden of proof isnot specifically addressed in these laws,these statutes lean toward creating an inde-pendent second opinion process, in whichthe original determination is given no bene-fit of weight or presumption. Federal regula-tions revising the full and fair review processin the case of ERISA plans also emphasize(to the extent possible given the internalnature of these reviews) independence, freshevidence, and claimant access to the plan’sevidence and information. On June 20,2002, the U.S. Supreme Court ruled thatIllinois’s independent review statute is notpreempted by ERISA. The majority opinion(five justices) stated that: “[A]n HMO isboth: it provides health care, and it does soas an insurer.... [R]egulating insurance tiedto what is medically necessary is probablyinseparable from enforcing the quintessen-tially state-law standards of reasonablemedical care.” (Rush Prudential HMO, Inc.,
Medical Necessity in Private Health Plans 35

Petitioner, v. Debra C. Moran et al., 2002)The practical effect of the decision is toleave intact the status quo regarding States’abilities to enact independent reviewstatutes, thus preserving consumers’ right topursue State-level appeals of claims denials,which occur in behavioral health care casesmore often than in general medical care.
Regardless of how the process is struc-tured, however, the importance of themodern medical necessity definition is thepower it affords an insurer or health plan toselect from among professionally acceptedtreatments the one treatment that it willelect to cover. Depending on the qualityof the evidence pointing to one treatmentas preferable to all others, this power mayrepresent an advance in the effort to stan-dardize the approach to the treatment ofcertain conditions. But to the extent that theevidence is weak, unreliable, or irrelevant,
or that little focus is given to a particularpatient’s condition (or conditions) in thecourse of evaluating possible treatments,the power to select on the basis of factorsother than the professional standard ofcare may result in the rejection of possibletreatment approaches that are beneficial inthe long run.
Finally, even the broadest definition ofmedical necessity that tolerates multipleschools of thought and that calls for exten-sive consultation with the treating physicianin arriving at the right treatment cannotovercome contractual terms that limit orexclude long-term maintenance treatmentsdesigned to avert deterioration or maintainfunctioning in the case of persons withchronic behavioral health conditions. Thisis a wholly separate issue, and one that isof increasing importance for behavioralhealth care services.
Special Report36

VIII.References
American Psychiatric Association. (1994).Diagnostic and Statistical Manual ofMental Disorders (4th ed.). Washington,DC: Author.
Bedrick v. Travelers Ins. Co., 93 F.3d 149(4th Cir. 1996).
Blumenthal, R. (2002). Report of theAttorney General’s InvestigationConcerning Psych Management, Inc.and Anthem Blue Cross and Blue Shieldof Connecticut. Available at http://www.cslib.org/attygenl/mainlinks/tabindex6.htm. Accessed April 3, 2002.
Buck, J. A., Teich, J. L., Umland, B., &Stein, M. (1999). Behavioral health bene-fits in employer-sponsored health plans,1997. Health Affairs, 18(2), 67–78.
Chodoff, P. (1998). Medical necessity andpsychotherapy. Psychiatric Services,49(11),1481-1483.
Dallek, G. & Pollitz, K. (2000). Externalreview of health plan decisions: Anupdate. Prepared for the Kaiser FamilyFoundation (Washington, DC).
Dettmer Clinic v. Associated InsuranceCompanies, Inc. U.S. Dist. LEXIS 20896(1993).
Domino, M. E., Salkever, D. S., Zarin, D. A.,& Pincus, H. A. (1998). The impact ofmanaged care on psychiatry.Administration & Policy in MentalHealth, 26(2),149–157.
Eddy, D. (1994). From theory to practice:Rationing resources while improvingquality: How to get more for less.JAMA, 272, 817–824.
Firestone Tire and Rubber v. Bruch, 489 U.S.101 (1989).
Ford, W. (1998). Medical necessity: Itsimpact in managed mental health care.Psychiatric Services 49(2), 183-184.
Ford, W. (2000). Medical necessity and psy-chiatric managed care. Psychiatric Clinicsof North America, 23(2), 309-317.
Hadley, J. (2002). Sicker and poorer: Theconsequences of being uninsured: Areview of the research on the relationshipbetween health insurance, health, work,income and education. Prepared for theKaiser Commission on Medicaid and theUninsured. Available at http://www.kff.org/content/2002/20020510/4004.pdf.Accessed May 29, 2002.
Harris v. Mutual of Omaha Co., 992 F.2d706 (7th Cir. 1993).
Hill, H., Hanson, A., & O’Connell, B.(2000). Using evidence: Coveragedecisions. Proceedings from Agencyfor Healthcare Research and Quality(AHRQ) User Liaison ProgramWorkshop for State and LocalHealthcare Policymakers. Available athttp://www.ahrq.gov/news/ulp/evidence/ulpevdnc5.htm. Accessed December 15,2001.
Medical Necessity in Private Health Plans 37

Institute of Medicine. (1990). Clinicalpractice guidelines: Directions for a newprogram. Washington, DC: NationalAcademy Press.
Ireys, H., Wehr, E., & Cooke, R.E. (1999).Defining medical necessity: Strategiesfor promoting access to quality care forpersons with developmental disabilities,mental retardation, and other specialhealth care needs. Washington, DC:National Center for Education inMaternal and Child Health Report.
JCAHO. (2001). 2001–2002 Comprehensiveaccreditation manual for health carenetworks. Oakbrook Terrace, IL: Author.
JCAHO. (1997). Comprehensive accredita-tion manual for managed behavioralhealth care. Oakbrook Terrace, IL:Author.
Jones v. Kodak Medical Assistance Plan.,169 F. 3d 1287 (10th Cir. 1999).
Kaplan, A. (1999). Medical necessity: Whatis it? Psychiatric Times, 16:12 Availableat http://www.psychiatrictimes.com/p991238.html.
Kornman v. Blue Cross Blue Shield ofLouisiana 662 So. 2nd 498 (1995).
Lazorko v. Pennsylvania Hospital., 237 F. 3d242 (3d Cir. 2000).
Manderscheid, R. W., Henderson, M. J., &Brown, D. Y. (2001). Status of nationalefforts to improve accountability forquality. In B. Dickey & L.I. Sederer(Eds.). Improving mental health care:Commitment to quality. (pp. 163-178).Washington, DC: American PsychiatricPublishing, Inc.
Milone v. Exclusive Health Care, Inc., 224F.3rd 615 (8th Cir. 2001).
Moscovitch v. Danbury State Hospital., 25 F.Supp. 2d 74 (D. Ct. 1998).
NCQA. (2001). Standards for the accredita-tion of MCOs (Effective July 1, 2001).Washington, DC: Author.
NCQA. (2000). Standards and surveyorguidelines for the accreditation ofMBHOs. Washington, DC: Author.
Pawlson, G., (April 3, 2002). NCQA,personal communication.
Rosenbaum, S. (2002). Medicaid. NEJM.346(8), 635–640.
Rosenbaum, S., & Rousseau, D. (2001).Medicaid at thirty-five. St. LouisUniversity Law Jour. 45, 1–53.
Rosenbaum, S., Frankford, D., Moore, B., &Borzi, P. (1999). Who should determinewhen health care is medically necessary?NEJM, 340, 229–232.
Rosenblatt, R., Law, S., & Rosenbaum, S.(1997). Law and the American healthcare system. New York: FoundationPress.
Rosenblatt, R., Rosenbaum, S., &Frankford, D. (2002). Law and theAmerican health care system. 2001–02Supplement. New York: FoundationPress.
Rush Prudential HMO, Inc., Petitioner,v. Debra C. Moran et al., U.S.Supreme Court. No. 00-1021. 2002U.S. LEXIS 4644. Available at http://www.supremecourtus.gov/opinions/01slipopinion.html. Accessed June 21,2002.
Special Report38

Sabin, J., & Daniels, N. (1994). Determining“medical necessity” for mental healthpractice. Hastings Center Report, 24(6),5–13.
Scalamandre v. Oxford Health Plans, Inc.823 F. Supp. 1050 (E.D. NY, 1993).
Schiffbauer, W. G. (1999). Medical necessityand health plan contracts. Washington,DC: Health Insurance Association ofAmerica.
Singer, S. J., Bergthold, L. A., Vorhaus, C.,& Enthoven, A. (1999). Decreasing varia-tion in medical necessity decision-making.Palo Alto, CA: Stanford University.
U.S. Department of Health and HumanServices (DHHS). (1999). Mental health:A report of the surgeon general.Rockville, MD: Substance Abuse andMental Health Services Administration.
Varble, D. (2001). Comments on practiceguidelines. In N. A. Cummings & W.O’Donohue (Eds.), Integrated behavioralhealthcare: Positioning mental healthpractice with medical/surgical practice.(pp. 251–255). San Diego, CA:Academic Press.
Medical Necessity in Private Health Plans 39


IX. Endnotes
1 Legislation to establish simplified review proce-
dures for all health benefit plans maintained by
private employers is currently pending in the
107th Congress. Since 1997 the Medicare pro-
gram has offered an informal administrative
review system, and courts have consistently held
that external impartial review of health plan
treatment decisions is a legal right of Medicaid
managed care enrollees (Rosenblatt, Law, &
Rosenbaum, 1997).
2 Review of the medical and health services
literature was conducted via searches on
MEDLINE, HealthSTAR, and PsycINFO.
Legal cases and decisions were retrieved using
LEXIS-NEXIS. Additional research included
retrieval of information from State attorneys
general Web sites. A unified database was
created using EndNote 5 to facilitate org-
anization and analysis of medical necessity
definitions across all sources of information.
3 It is worth noting that the Senate mental health
parity legislation would appear to allow con-
tractual treatments to vary by diagnosis, even
as it constrains insurer discretion to formulate
mental illness-specific coverage limitations for
broad classes of benefits. Thus, an insurer pre-
sumably could specify covered contractual treat-
ments in the case of mental illness while using
a broader and more flexible individualized
“medical necessity” decisionmaking approach
in the case of physical illness.
4 Available at http://www.ama-assn.org/ama1/pub/
upload/mm/368/supplement1.pdf. Accessed
December 19, 2001.
5 The plausibility of this distinction has been
most recently called into question in Fitts v.
Fannie Mae, No. 98-00617, 2002 U.S. Dist.
LEXIS 3071 (D. D.C. Feb. 26, 2002).
6 According to the American Psychiatric
Association, “the DSM-IV (Diagnostic and
Statistical Manual of Mental Disorders, Fourth
Edition), published in 1994 was the last major
revision of the DSM. It was the culmination of a
six-year effort that involved over 1,000 individu-
als and numerous professional organizations.
Much of the effort involved conducting a com-
prehensive review of the literature to establish a
firm empirical basis for making modifications.
Numerous changes were made to the classifica-
tion (i.e., disorders were added, deleted, and
reorganized), to the diagnostic criteria sets, and
to the descriptive text based on a careful consid-
eration of the available research about the vari-
ous mental disorders.” The APA has recently
begun considering “relational disorders” as a
new diagnostic code in the future DSM-V
(expected for publication in 2010). See http://
www.psych.org/clin_res/dsm/dsmintro81301.cfm.
7 The fact that the industry views the utilization
review process as linked to both health care
quality and cost is best evidenced in industry
accreditation standards, which identify an
appropriate utilization management program
as an essential feature of health care quality
and thus, of accreditation. See, e.g., JCAHO
(1997, 2001) and NCQA (2000, 2001).
8 Full and fair hearing review regulations issued
in 2000 by the U. S. Department of Labor
Medical Necessity in Private Health Plans 41

require ERISA health benefit plans to disclose
any relevant information to claimants appealing
a benefit denial through the plan’s internal
review system. See 65 Fed. Reg. 70246 (Nov.
21, 2000); 29 C.F.R. Part 2560 (2001). When a
health plan denies a claim based on a protocol
or guidelines, the plan must disclose such
reliance and inform the claimant that a copy
of the protocol or guideline is available upon
request. Similarly, when the denial is based on
medical necessity, the rule requires the plan
either to explain the scientific or clinical judg-
ment used in applying the plan’s terms to the
claimant’s medical circumstances or to include
a statement that such an explanation will be
provided free of charge if requested. These
regulations are effective for claims filed under
an ERISA health plan on or after July 1, 2002.
The regulations effectively reverse a series of
judicial decisions holding that under ERISA,
health plans’ fiduciary obligations do not
require disclosure of treatment guidelines.
See Jones v. Kodak, 169 F.3d 1287 (10th Cir.
1999); Doe v. Travelers Ins. Co., 187 F.3d 53
(1st Cir. 1999). 9 Available at https://apps.cignabehavioral.com/
web/basicsite/provider/pdf/CBHguide.pdf.
Accessed September 22, 2002.10 In RE: United Behavioral Health, Consent
Agreement with Maine Bureau of Insurance,
Docket No. 00-3005. Available at http://
www.state.me.us/pfr/ins/ins003005.htm.
Accessed April 16, 2002.11 It is typical for insurers to limit the concept of
treatment to interventions that are calculated
to yield either a full recovery or a significant
improvement. See McGraw v. Prudential Ins.
Co., 137 F.3d 1253 (10th Cir. 1998) and
Bedrick v. Travelers Ins. Co., 93 F.3d 149 (4th
Cir. 1996). Where the patient cannot improve or
show significant recovery, an insurer may deny
the coverage as unnecessary. Courts that have
considered this limitation have tended to uphold
it where it is explicit in the contract and have
rejected it when it is not an express limitation
on coverage. See McGraw v. Prudential Ins.
Co., 137 F.3d 1253 (10th Cir. 1998) and
Bedrick v. Travelers Ins. Co., 93 F.3d 149 (4th
Cir. 1996) (rejecting limitation when not explicit
in contract’s medical necessity definition).12 In Shilkret v. Annapolis Emergency Hospital,
349 A.2d 245, 249-50 (Md. 1975), Maryland’s
highest court set forth what is still viewed as the
seminal articulation of the modern standard of
care for measuring professional liability:
“...that degree of care and skill which is expected
to a reasonably competent practitioner in the
same class to which he belongs, acting in the
same or similar circumstances. Under this stan-
dard, advances in the profession, availability
of facilities, specialization or general practice,
proximity of specialists and special facilities,
together with all other relevant considerations,
are to be taken into account.”
See also Law and the American Health Care
System, op. cit., at 846.
13 Since the UBH guidelines were not available
to the authors, it is not known to what extent
they refer to professional or national stan-
dards of care.
14 For purposes of confidentiality, we do not
identify the managed care organizations or the
officials by name.
15 Of course, if the contract limits coverage for
specified conditions to certain treatments, this
limitation in coverage would take precedence.
16 It would probably seem that any insurer has
an inherent conflict of interest because it is at
risk for the cost of its decision. In fact, courts
do not perceive the dual role of insurers as risk
bearers and decision makers as a fatal flaw,
although many will more closely review a
record as a result.
Special Report42

17 Advocates note the qualitative advances inher-
ent in emphasizing outpatient over inpatient
care wherever appropriate. Chris Koyanagi,
Bazelon Center for Mental Health Law.
Personal communication. April 5, 2002. (By
the same token of course, on the outpatient
side, providers of long-term psychotherapy and
psychoanalysis have seen restrictions put on the
scope and duration of their treatments, with a
particular emphasis on short-term behavioral
and cognitive therapy as preferred.)
18 Aetna/U.S. HealthCare Inc./Prudential Health
Plan of Hartford, CT; Excellus Health Plans
of Rochester; Group Health Inc. of Manhattan;
HIP Health Plan of Greater New York, Inc.;
Oxford Health Plans of Trumbull, CT; and
Vytra Health Plans of Long Island, Inc. See:
“Landmark Agreements Give Consumers New
Protections in HMO Disputes.” NY Attorney
General’s Office Press Release. October 16,
2001. Available at http://www.oag.state.ny.us.
Accessed October 29, 2001.
19 In RE: United Behavioral Health, Consent
Agreement with Maine Bureau of Insurance,
op. cit. In RE: Cigna Behavioral Health, Inc.,
Consent Agreement with Maine Bureau of
Insurance, Docket No. 00-3003. Available at
http://www.state.me.us/pfr/ins/ins003003.htm.
Accessed April 17, 2002.
20 In Metropolitan Life Insurance v.
Massachusetts, 471 U.S. 724 (1985), the
Supreme Court affirmed the power of states to
set minimum content standards in the case of
insured ERISA plans. The case involved a
Massachusetts state law mandating inpatient
hospitalization coverage up to certain levels in
the case of mental illness.
21 A recent decision illustrating the still common
practice of insurers to leave critical terms unde-
fined is Bynum v. Cigna Healthcare of North
Carolina, Inc., 287 F.3d 305 (4th Cir., 2002) in
which an insurer denied reconstructive facial
surgery for a severely deformed infant on the
grounds that the construction was excluded
as “cosmetic” without ever defining the term.
22 See Dallis v. Aetna Life Ins. Co., 574 F.Supp.
547 (N.D. Ga. 1983), aff’d, 768 F.2d 1303 (11th
Cir. 1985) (finding “no consensus among the
courts” as to the definition of “necessary” care).
23 The prospective nature of utilization review
means that managed care affects not only cover-
age but access to the care itself. Courts therefore
might consider professional liability law as a
relevant source of law from which to derive an
insurance standard of medical necessity. In recent
years, courts have repeatedly noted the “two
hats” of managed care, affecting both coverage
and health care quality through their conduct.
See Pegram v. Herdrich, 530 U.S. 211 (2000).
24 Mass. Ann. Laws ch. 176O (1) (2001).
25 HRS § 432E-1.4 (2000).
26 We limited our review of state regulations to
those available in the LEXIS-NEXIS legal
databases.
27 Md. Ins. Code Ann. § 15-10A-03(e) (2001).
28 28 Pa. Code § 9.504 (2001) and VT. Stat. tit. 8,
§ 4089f (2001).
29 29 U.S.C. § 1133 (2001).
30 Individuals may seek judicial review of a claim’s
denial. In such a case the review is on the record
rather than de novo. Under the standard of
review set forth by the United States Supreme
Court in Firestone Tire and Rubber v. Bruch,
489 U.S. 101 (1989), the plan administrator’s
decision is upheld unless the claimant can
demonstrate that it is arbitrary and capricious
or an abuse of discretion. Courts may conduct
a more rigorous review when a claimant is able
to demonstrate a conflict of interest; however,
although the fact that the internal review was
conducted by the insurer or the health plan
Medical Necessity in Private Health Plans 43

administrator raises the potential for conflict,
the interest is not sufficient to compel a more
rigorous review in every case. See Firestone Tire
and Rubber v. Bruch, 489 U.S. 101 (1989);
Bedrick v. Travelers Ins. Co., 93 F.3d 149 (4th
Cir. 1996).
31 Pending patients’ bill of rights legislation before
Congress would establish independent review as
a basic element of ERISA for all covered plans
and health insurance arrangements. See H.R.
and S. 1052, 107th Cong., 1st sess.
32 29 C.F.R. § 2560.503-1(b) (2001).
33 See 29 C.F.R. §§ 2560.503-1(f), (i) (2001).
34 See 29 C.F.R. §§ 2560.503-1 (i) (2001).
35 29 C.F.R. §§ 2560.503-1(h) (2001).
36 See id.
37 See id.
38 See id.
39 5 U.S.C. § 8901 (2001).
40 5 C.F.R. § 890.105 (2001).
41 Id.
42 5 C.F.R. § 890.107(c) (2001).
43 Several cases have focused specifically on the
use of “significant improvement” and “recov-
ery” by insurers to narrow the scope of the
treatments that can be considered medically
necessary. See McGraw v. Prudential Ins. Co.,
137 F.3d 1253 (10th Cir. 1998) and Bedrick v.
Travelers Ins. Co., 93 F.3d 149 (4th Cir. 1996).
Where the concept is not contractual but is a
“gloss on the contract” imposed by utilization
management review, courts have tended to
overturn the insurer’s decision. But where the
contract documents actually specify recovery
or short term improvements, courts will honor
the limitation.
Special Report44

Medical Necessity in Private Health Plans 45
1994
Sabi
n, J
ames
E.
and
Nor
man
Dan
iels
Thos
e m
enta
l hea
lth s
ervi
ces
that
are
ess
entia
l for
the
treat
men
t of a
Mem
ber’s
men
tal h
ealth
dis
orde
r as
defin
ed b
y th
e DS
M-IV
in a
ccor
danc
ew
ith g
ener
ally
acc
epte
d m
enta
l hea
lth p
ract
ice.
The
auth
ors
pose
d th
e qu
estio
n, “
Shou
ldm
enta
l hea
lth in
sura
nce
cove
r onl
y di
sord
ers
foun
d in
DSM
-IV, o
r sho
uld
it be
ext
ende
d to
treat
men
t for
ord
inar
y sh
ynes
s, u
nhap
pine
ss,
and
othe
r res
pons
es to
life
’s ha
rd k
nock
s?”
Thro
ugh
the
use
of s
ix il
lust
rativ
e ca
se s
tud-
ies,
the
auth
ors
exam
ined
the
reas
onin
gbe
hind
the
dete
rmin
atio
ns o
f med
ical
nec
es-
sity
. The
arti
cle
incl
udes
a d
iscu
ssio
n of
are
curr
ent c
onfli
ct b
etw
een
“har
d-lin
e” a
nd“e
xpan
sive
” vi
ews
of m
edic
al n
eces
sity
,no
ting
that
it fr
eque
ntly
refle
cts
unre
cog-
nize
d m
oral
dis
agre
emen
t abo
ut th
e ta
rget
sof
clin
ical
inte
rven
tion
and
the
ultim
ate
goal
sof
psy
chia
tric
treat
men
t. Th
e au
thor
s pr
esen
tth
ree
mod
els
for d
efin
ing
med
ical
nec
essi
tyan
d ar
gue
a de
fens
ible
ratio
nale
for t
he“n
orm
al”
mod
el, w
hich
com
pris
es a
targ
etof
a m
edic
ally
def
ined
dev
iatio
n in
tend
ed to
decr
ease
the
impa
ct o
f dis
ease
or d
isab
ility
.Th
ree
test
s of
med
ical
nec
essi
ty a
re o
ffere
d:(1
) Doe
s it
mak
e di
stin
ctio
ns th
e pu
blic
and
clin
icia
ns re
gard
as
fair?
(2) C
an it
be
adm
in-
iste
red
in th
e re
al w
orld
? (3
) Doe
s it
lead
tore
sults
that
soc
iety
can
affo
rd?
The
auth
ors
conc
lude
that
the
DSM
-IV s
tand
ard
prov
ides
wor
kabl
e bo
unda
ries
for m
edic
al n
eces
sity
defin
ition
s.
“Det
erm
inin
g‘M
edic
alN
eces
sity
’ in
Men
tal H
ealth
Prac
tice”
Hast
ings
Cen
ter
Repo
rt24
(6):5
–13
Year
Auth
orTi
tle, S
ourc
eSu
mm
ary/
Abst
ract
Med
ical
Nec
essi
ty D
efin
ition
1
Tab
le 1
. Med
ical
Nec
essi
ty D
efin
itio
ns
in P
ub
lish
ed L
iter
atu
re (
See
Als
o A
pp
end
ix C
)
1 Defin
ition
s ha
ve b
een
take
n ve
rbat
im fr
om th
e re
leva
nt d
ocum
ent;
quot
atio
n m
arks
hav
e be
en o
mitt
ed.

Special Report46
1998
Chod
off,
Paul
“H
ealth
Nec
essi
ty”
wou
ld re
ly o
n m
edic
al c
riter
ia w
hen
they
are
rele
vant
but
wou
ld a
lso
ackn
owle
dge
that
the
heal
th o
f the
citi
zenr
y ca
n be
per
ceiv
ed in
broa
der t
erm
s. A
theo
retic
al fo
unda
tion
for t
his
conc
ept m
ay b
e fo
und
in th
ebi
opsy
chos
ocia
l mod
el. H
ealth
nec
essi
ty w
ould
be
base
d on
thre
e br
oad
fund
amen
tals
: uni
form
qua
lific
atio
ns fo
r pra
ctiti
oner
s, a
ccep
tabl
e pr
ofes
sion
alid
entit
ies,
and
com
pete
nce;
crit
eria
for t
he k
inds
of s
ervi
ces
that
wou
ld b
epr
ovid
ed a
nd c
over
ed; a
nd a
fair
mec
hani
sm fo
r res
olut
ion
of d
ispu
tes
abou
tqu
estio
ns o
f ser
vice
cov
erag
e. T
he c
riter
ia fo
r ser
vice
s w
ould
incl
ude
biot
ech-
nica
l med
ical
crit
eria
whe
n ap
prop
riate
, as
wou
ld b
e th
e ca
se in
mos
t ord
inar
ym
edic
al p
ract
ice,
but
they
wou
ld b
e ac
know
ledg
ed to
be
only
a s
ubse
t of t
hehe
alth
nec
essi
ty c
riter
ia. F
or m
enta
l hea
lth n
eeds
, a b
road
rang
e of
ser
vice
sco
uld
also
be
cons
ider
ed, i
nclu
ding
app
ropr
iate
psy
chot
hera
py fo
r ind
ivid
uals
who
may
not
fit c
omfo
rtabl
y w
ith D
SM-IV
dia
gnos
tic c
ateg
orie
s bu
t who
suf
fer
a si
gnifi
cant
deg
ree
of d
istre
ss a
nd in
terp
erso
nal i
mpa
irmen
t.
Man
aged
car
e an
d, s
peci
fical
ly, t
he n
eed
toco
nfor
m to
med
ical
nec
essi
ty re
quire
men
tsha
ve h
ad a
dra
mat
ic e
ffect
on
the
med
ical
and
psyc
hiat
ric p
ract
ice,
esp
ecia
lly o
nps
ycho
ther
apy.
The
aut
hor d
escr
ibes
the
prog
ress
ion
of th
e co
ncep
t of m
edic
alne
cess
ity fr
om a
sim
ple
acco
untin
g of
serv
ices
reim
burs
able
by
insu
ranc
e co
m-
pani
es to
an
ambi
guou
s te
rm w
ithou
tde
finiti
onal
con
sens
us. H
e de
scrib
es it
sre
latio
nshi
p to
the
med
ical
mod
el a
nddi
scus
ses
the
inco
ngru
ity b
etw
een
med
ical
nece
ssity
and
certa
in a
spec
ts o
f psy
chot
her-
apy.
He
prop
oses
a b
road
er c
once
pt—
heal
thne
cess
ity—
base
d on
an
eval
uatio
nof
the
adva
ntag
es, d
isad
vant
ages
, and
cost
sof
med
ical
and
psy
chia
tric
serv
ices
.
“Med
ical
Nec
essi
ty a
ndPs
ycho
ther
apy”
Psyc
hiat
ricSe
rvic
es49
(11)
:148
1–14
83
Year
Auth
orTi
tle, S
ourc
eSu
mm
ary/
Abst
ract
Med
ical
Nec
essi
ty D
efin
ition
1
1998
Ford
, Will
iam
“T
reat
men
t nec
essi
ty”
or “
clin
ical
nec
essi
ty”
wou
ld re
quire
that
, to
qual
ify fo
rpa
ymen
t, a
serv
ice
mus
t be:
for t
he tr
eatm
ent o
f men
tal i
llnes
s an
d su
bsta
nce
use
diso
rder
s, o
r sym
ptom
s of
thes
e di
sord
ers,
and
impa
irmen
ts in
day
-to-d
ayfu
nctio
ning
rela
ted
to th
em; f
or th
e pu
rpos
e of
pre
vent
ing
the
need
for a
mor
ein
tens
ive
leve
l of m
enta
l hea
lth a
nd s
ubst
ance
abu
se c
are;
for t
he p
urpo
se o
fpr
even
ting
rela
pse
of p
erso
ns w
ith m
enta
l illn
ess
and
subs
tanc
e ab
use
diso
r-de
rs; e
ffici
ent,
in th
e se
nse
that
a le
ss e
xpen
sive
trea
tmen
t wor
ks a
s w
ell a
s a
mor
e ex
pens
ive
treat
men
t; an
d no
t for
the
patie
nt’s
or p
rovi
der’s
con
veni
ence
.
Disc
usse
s th
e im
pact
of m
anag
ed c
are
med
ical
nec
essi
ty d
efin
ition
s on
psy
chia
tric
care
. Poi
nts
to s
ome
poss
ible
reas
ons
why
MBH
Os fo
cus
on c
uttin
g sh
ort-t
erm
cos
tsra
ther
than
man
agin
g lo
ng-te
rm c
osts
,in
clud
ing
shor
t con
tract
term
s an
d la
bor-
inte
nsiv
e re
view
s.
“Med
ical
Nec
essi
ty:
ItsIm
pact
inM
anag
ed M
enta
lHe
alth
Car
e”Ps
ychi
atric
Serv
ices
49(2
):183
–184
Tab
le 1
. Co
nti
nu
ed

Medical Necessity in Private Health Plans 47
1999
Sing
er, S
ara
J.,
Lind
a A.
Berg
thol
d,Ca
rol V
orha
us,
Alai
n En
thov
en,
et a
l.
For c
ontra
ctua
l pur
pose
s, a
n in
terv
entio
n w
ill b
e co
vere
d if
it is
an
othe
r-w
ise
cove
red
cate
gory
of s
ervi
ce, n
ot s
peci
fical
ly e
xclu
ded,
and
med
ical
lyne
cess
ary.
An
inte
rven
tion
is m
edic
ally
nec
essa
ry if
, as
reco
mm
ende
d by
the
treat
ing
phys
icia
n an
d de
term
ined
by
the
heal
th p
lan’
s m
edic
al d
irect
oror
phys
icia
n de
sign
ee, i
t is
(all
of th
e fo
llow
ing)
: a h
ealth
inte
rven
tion
for t
hepu
rpos
e of
trea
ting
a m
edic
al c
ondi
tion;
the
mos
t app
ropr
iate
sup
ply
or le
vel
of s
ervi
ce, c
onsi
derin
g po
tent
ial b
enef
its a
nd h
arm
s to
the
patie
nt; a
nd k
now
nto
be
effe
ctiv
e in
impr
ovin
g he
alth
out
com
es. F
or n
ew in
terv
entio
ns, e
ffect
ive-
ness
is d
eter
min
ed b
y sc
ient
ific
evid
ence
. For
exi
stin
g in
terv
entio
ns, e
ffect
ive-
ness
is d
eter
min
ed fi
rst b
y sc
ient
ific
evid
ence
, the
n by
pro
fess
iona
l sta
ndar
ds,
then
by
expe
rt op
inio
n; a
nd th
e co
st-e
ffect
iven
ess
for t
his
inte
rven
tion
isco
mpa
red
to a
ltern
ativ
e in
terv
entio
ns, i
nclu
ding
no
inte
rven
tion.
“Co
st-
effe
ctiv
e” d
oes
not n
eces
saril
y m
ean
low
est p
rice.
An
inte
rven
tion
may
be
med
ical
ly in
dica
ted
yet n
ot b
e a
cove
red
bene
fit o
r mee
t thi
s co
ntra
ctua
lde
finiti
on o
f med
ical
nec
essi
ty. A
hea
lth p
lan
may
cho
ose
to c
over
inte
r-ve
ntio
ns th
at d
o no
t mee
t thi
s co
ntra
ctua
l def
initi
on o
f med
ical
nec
essi
ty.
This
is a
n in
-dep
th re
port
look
ing
into
the
ques
tion
of m
edic
al n
eces
sity
. It d
eals
with
the
varia
tion
and
inco
nsis
tenc
ies
of d
efin
i-tio
ns th
at th
e va
rious
sta
keho
lder
s ha
ve.
Itno
tes
a pa
ucity
of r
esea
rch
rega
rdin
ghe
alth
pla
n de
cisi
on-m
akin
g an
d w
heth
erm
edic
al n
eces
sity
def
initi
ons
play
a re
al ro
lein
dec
isio
n-m
akin
g. It
doc
umen
ts a
num
ber
of c
onfe
renc
es a
nd o
rigin
al re
sear
ch,
even
tual
ly c
oncl
udin
g w
ith a
con
sens
usfo
ra m
odel
dec
isio
n-m
akin
g pr
oces
s an
dm
edic
alne
cess
ity d
efin
ition
s. It
con
clud
esby
revi
ewin
g th
e va
rious
sta
keho
lder
s, th
eir
conc
erns
, and
wha
t act
ions
they
cou
ld ta
keto
dec
reas
e m
edic
al n
eces
sity
var
iabi
lity.
“Dec
reas
ing
Varia
tion
inM
edic
alN
eces
sity
Deci
sion
Mak
ing”
Stan
ford
Univ
ersi
ty,
Augu
st, 1
999
Year
Auth
orTi
tle, S
ourc
eSu
mm
ary/
Abst
ract
Med
ical
Nec
essi
ty D
efin
ition
1
Tab
le 1
. Co
nti
nu
ed
1999
Ireys
, Hen
ry T
.,El
izabe
th W
ehr,
and
Robe
rt E.
Coo
ke
A co
vere
d se
rvic
e or
item
is m
edic
ally
nec
essa
ry if
it w
ill d
o, o
r is
reas
onab
lyex
pect
ed to
do,
one
or m
ore
of th
e fo
llow
ing:
arr
ive
at a
cor
rect
med
ical
dia
g-no
sis;
pre
vent
the
onse
t of a
n ill
ness
, con
ditio
n, in
jury
, or d
isab
ility
(in
the
indi
-vi
dual
or i
n co
vere
d re
lativ
es, a
s ap
prop
riate
); re
duce
, cor
rect
, or a
mel
iora
teth
e ph
ysic
al, m
enta
l, de
velo
pmen
tal,
or b
ehav
iora
l effe
cts
of a
n ill
ness
, con
di-
tion,
inju
ry, o
r dis
abili
ty; a
nd a
ssis
t the
indi
vidu
al to
ach
ieve
or m
aint
ain
suffi
-ci
ent f
unct
iona
l cap
acity
to p
erfo
rm a
ge-a
ppro
pria
te o
r dev
elop
men
tally
appr
opria
te d
aily
act
iviti
es. T
he M
CO o
r ins
urer
mus
t det
erm
ine
med
ical
nece
ssity
on
the
basi
s of
hea
lth in
form
atio
n pr
ovid
ed b
y th
e fo
llow
ing
pers
ons:
the
indi
vidu
al (a
s ap
prop
riate
to h
is o
r her
age
and
com
mun
icat
ive
abili
ties)
,th
e in
divi
dual
’s fa
mily
, the
prim
ary
care
phy
sici
an, a
nd c
onsu
ltant
s w
ith a
ppro
-pr
iate
spe
cial
ty tr
aini
ng, a
s w
ell a
s ot
her p
rovi
ders
, pro
gram
s, m
ultid
isci
plin
ary
team
s, e
duca
tiona
l ins
titut
ions
, or a
genc
ies
that
hav
e ev
alua
ted
the
indi
vidu
al.
The
dete
rmin
atio
n of
med
ical
nec
essi
ty m
ust b
e m
ade
on a
n in
divi
dual
bas
isan
d m
ust c
onsi
der t
he fu
nctio
nal c
apac
ity o
f the
per
son
and
thos
e ca
paci
ties
that
are
app
ropr
iate
for p
erso
ns o
f the
sam
e ag
e or
dev
elop
men
tal l
evel
and
avai
labl
e re
sear
ch fi
ndin
gs, h
ealth
car
e pr
actic
e gu
idel
ines
, and
sta
ndar
dsis
sued
by
prof
essi
onal
ly re
cogn
ized
orga
niza
tions
or g
over
nmen
tal a
genc
ies.
Fina
l det
erm
inat
ions
will
be
mad
e by
a p
hysi
cian
in c
once
rt w
ith th
e fo
llow
ing
pers
ons:
the
indi
vidu
al’s
prim
ary
care
phy
sici
an; a
con
sulta
nt w
ith e
xper
ienc
eap
prop
riate
to th
e in
divi
dual
’s ag
e, d
isab
ility
or c
hron
ic c
ondi
tion;
and
the
indi
vidu
al a
nd/o
r fam
ily. M
edic
ally
nec
essa
ry s
ervi
ces
mus
t be
deliv
ered
ina
setti
ng th
at is
app
ropr
iate
to th
e sp
ecifi
c he
alth
nee
ds o
f the
indi
vidu
al.
Disc
usse
s m
edic
al n
eces
sity
det
erm
inat
ions
in re
gard
s to
per
sons
with
dev
elop
men
tal
disa
bilit
ies.
The
repo
rt ha
s a
flow
cha
rtsh
owin
g th
e dy
nam
ics
of m
edic
al n
eces
sity
deci
sion
s w
ithin
cur
rent
ser
vice
sys
tem
s.It
also
pro
vide
s its
ow
n sp
ecifi
catio
ns fo
rde
term
inin
g m
edic
al n
eces
sity
.
“Def
inin
gM
edic
alN
eces
sity
:St
rate
gies
for
Prom
otin
gAc
cess
toQu
ality
Care
for
Pers
ons
with
Deve
lopm
enta
lDi
sabi
litie
s,M
enta
lRe
tard
atio
n,an
dOt
her S
peci
alHe
alth
Car
eN
eeds
”
Nat
iona
l Cen
ter
for E
duca
tion
inM
ater
nal a
ndCh
ild H
ealth
,Ge
orge
tow
nUn
iver
sity
1 Defin
ition
s ha
ve b
een
take
n ve
rbat
im fr
om th
e re
leva
nt d
ocum
ent;
quot
atio
n m
arks
hav
e be
en o
mitt
ed.

2000
Ford
, Will
iam
Co
mpr
ehen
sive
refo
rm to
incr
ease
com
mer
cial
psy
chia
tric
insu
ranc
e co
ver-
age
mus
t inc
lude
cha
ngin
g th
e de
finiti
on o
f med
ical
nec
essi
ty b
y re
orie
ntin
gin
sure
rs fr
om a
n ac
ute
care
mod
el to
a m
odel
that
pro
vide
s bo
th c
are
for
acut
e ep
isod
es a
nd lo
nger
-term
car
e de
sign
ed to
man
age
chro
nic
cond
ition
s.Su
ch lo
nger
-term
man
agem
ent i
nclu
des
deliv
erin
g se
rvic
es d
esig
ned
toav
oid
futu
re a
cute
epi
sode
s. C
omm
erci
al in
sura
nce
ough
t to
unde
rsta
nd th
ata
legi
timat
e fu
nctio
n of
psy
chia
tric
serv
ices
is to
mai
ntai
n be
havi
oral
hea
lth in
addi
tion
to re
turn
ing
som
eone
to h
ealth
afte
r an
acut
e ep
isod
e. F
ord
prop
osed
the
conc
ept o
f “tre
atm
ent n
eces
sity
” or
“cl
inic
al n
eces
sity
” to
enc
ompa
ssth
is b
road
er v
iew
of t
he g
oals
of p
sych
iatri
c se
rvic
es. T
reat
men
t nec
essi
tyre
quire
s a
serv
ice
to b
e: fo
r the
trea
tmen
t of m
enta
l illn
ess
and
subs
tanc
eab
use
diso
rder
s, o
r sym
ptom
s of
thes
e di
sord
ers,
and
impa
irmen
ts in
day
-to-
day
func
tioni
ng re
late
d to
them
; for
the
purp
ose
of p
reve
ntin
g th
e ne
ed fo
r am
ore
inte
nsiv
e le
vel o
f psy
chia
tric
care
; for
the
purp
ose
of p
reve
ntin
g re
laps
eof
per
sons
with
psy
chia
tric
diso
rder
s; c
onsi
sten
t with
gen
eral
ly a
ccep
ted
clin
ical
pra
ctic
e fo
r psy
chia
tric
diso
rder
s; a
nd n
ot s
olel
y fo
r the
pat
ient
’s or
prov
ider
’s co
nven
ienc
e.
The
conc
ept o
f med
ical
nec
essi
ty is
one
tool
used
by
third
-par
ty p
ayer
s to
con
tain
thei
rfin
anci
al ri
sk in
a s
eem
ingl
y no
narb
itrar
ym
anne
r. Th
e de
finiti
ons
tend
to re
flect
corp
orat
ion
philo
soph
ies
that
wou
ld n
eed
toch
ange
to a
chie
ve re
al p
arity
.
“Med
ical
Nec
essi
ty a
ndPs
ychi
atric
Man
aged
Car
e”
The
Psyc
hiat
ricCl
inic
s of
Nor
thAm
eric
a23
(2):3
09–3
17
Special Report48
1999
Nat
iona
l Hea
lthLa
w P
rogr
amM
edic
ally
nec
essa
ry c
are
is th
e ca
re w
hich
, in
the
opin
ion
of th
e tre
atin
gph
ysic
ian,
is re
ason
ably
nee
ded:
to p
reve
nt th
e on
set o
r wor
seni
ng o
f an
illne
ss, c
ondi
tion,
or d
isab
ility
; to
esta
blis
h a
diag
nosi
s; to
pro
vide
pal
liativ
e,cu
rativ
e, o
r res
tora
tive
treat
men
t for
phy
sica
l and
/or m
enta
l hea
lth c
ondi
tions
;an
d to
ass
ist t
he in
divi
dual
to a
chie
ve o
r mai
ntai
n m
axim
um fu
nctio
nal c
apac
ityin
per
form
ing
daily
act
iviti
es, t
akin
g in
to a
ccou
nt b
oth
the
func
tiona
l cap
acity
of th
e in
divi
dual
and
thos
e fu
nctio
nal c
apac
ities
that
are
app
ropr
iate
for i
ndi-
vidu
als
of th
e sa
me
age.
“Med
ical
Nec
essi
tyDe
finiti
on,
Mod
elM
edic
aid
Man
aged
Car
eCo
ntra
ctPr
ovis
ions
”
1999
Corli
n, R
icha
rd
“Med
ical
nec
essi
ty”
mea
ns: “
Heal
th c
are
serv
ices
or p
rodu
cts
that
a p
rude
ntph
ysic
ian
wou
ld p
rovi
de to
a p
atie
nt fo
r the
pur
pose
of p
reve
ntin
g, d
iagn
osin
gor
trea
ting
an il
lnes
s, in
jury
, dis
ease
or i
ts s
ympt
oms
in a
man
ner t
hat i
s:(1
) in
acco
rdan
ce w
ith g
ener
ally
acc
epte
d st
anda
rds
of m
edic
al p
ract
ice;
(2)c
linic
ally
app
ropr
iate
in te
rms
of ty
pe, f
requ
ency
, ext
ent,
site
, and
dur
atio
n;an
d (3
) not
prim
arily
for t
he c
onve
nien
ce o
f the
pat
ient
, phy
sici
an, o
r oth
erhe
alth
car
e pr
ovid
er.”
“Sta
tem
ent o
fth
eAM
A to
the
Com
mitt
eeon
Heal
th,
Educ
atio
n, L
abor
and
Pens
ions
,U.
S. S
enat
e”
Year
Auth
orTi
tle, S
ourc
eSu
mm
ary/
Abst
ract
Med
ical
Nec
essi
ty D
efin
ition
1
Tab
le 1
. Co
nti
nu
ed
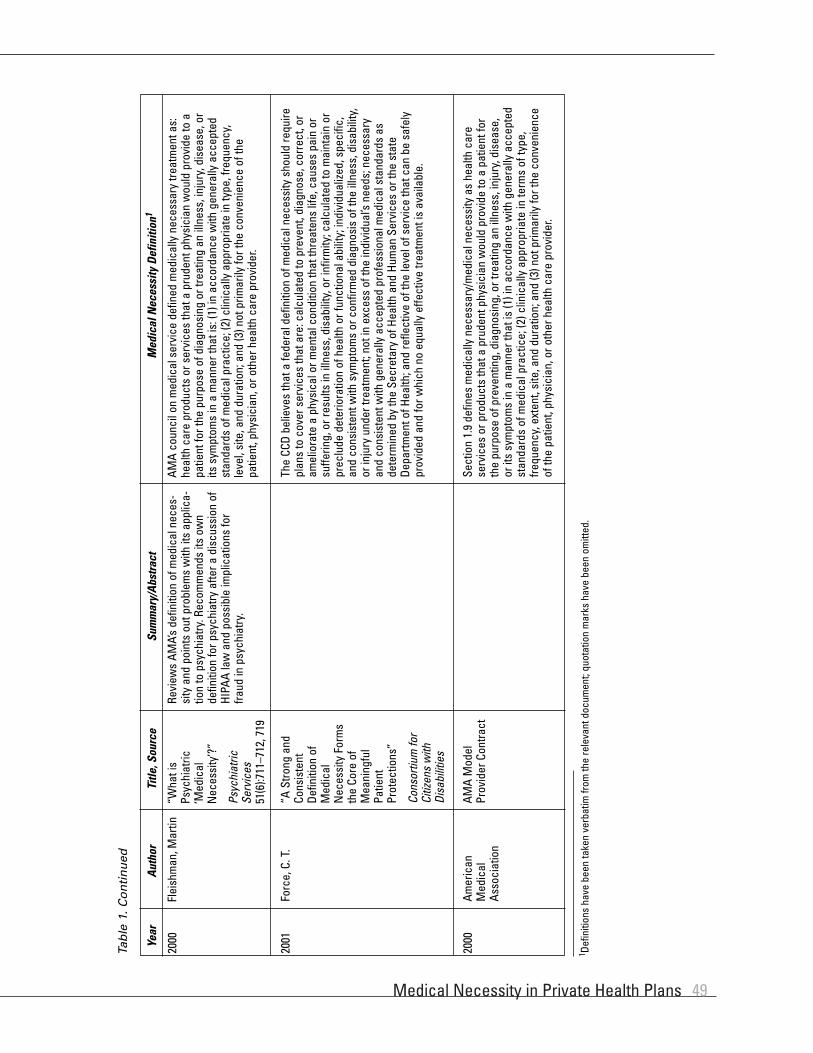
Medical Necessity in Private Health Plans 49
Year
Auth
orTi
tle, S
ourc
eSu
mm
ary/
Abst
ract
Med
ical
Nec
essi
ty D
efin
ition
1
Tab
le 1
. Co
nti
nu
ed
2000
Flei
shm
an, M
artin
AM
A co
unci
l on
med
ical
ser
vice
def
ined
med
ical
ly n
eces
sary
trea
tmen
t as:
heal
th c
are
prod
ucts
or s
ervi
ces
that
a p
rude
nt p
hysi
cian
wou
ld p
rovi
de to
apa
tient
for t
he p
urpo
se o
f dia
gnos
ing
or tr
eatin
g an
illn
ess,
inju
ry, d
isea
se, o
rits
sym
ptom
s in
a m
anne
r tha
t is:
(1) i
n ac
cord
ance
with
gen
eral
ly a
ccep
ted
stan
dard
s of
med
ical
pra
ctic
e; (2
) clin
ical
ly a
ppro
pria
te in
type
, fre
quen
cy,
leve
l, si
te, a
nd d
urat
ion;
and
(3) n
ot p
rimar
ily fo
r the
con
veni
ence
of t
hepa
tient
, phy
sici
an, o
r oth
er h
ealth
car
e pr
ovid
er.
Revi
ews
AMA’
s de
finiti
on o
f med
ical
nec
es-
sity
and
poi
nts
out p
robl
ems
with
its
appl
ica-
tion
to p
sych
iatry
. Rec
omm
ends
its
own
defin
ition
for p
sych
iatry
afte
r a d
iscu
ssio
n of
HIPA
A la
w a
nd p
ossi
ble
impl
icat
ions
for
fraud
in p
sych
iatry
.
“Wha
t is
Psyc
hiat
ric‘M
edic
alN
eces
sity
’?”
Psyc
hiat
ricSe
rvic
es51
(6):7
11–7
12, 7
19
2001
Forc
e, C
. T.
The
CCD
belie
ves
that
a fe
dera
l def
initi
on o
f med
ical
nec
essi
ty s
houl
d re
quire
plan
s to
cov
er s
ervi
ces
that
are
: cal
cula
ted
to p
reve
nt, d
iagn
ose,
cor
rect
, or
amel
iora
te a
phy
sica
l or m
enta
l con
ditio
n th
at th
reat
ens
life,
cau
ses
pain
or
suffe
ring,
or r
esul
ts in
illn
ess,
dis
abili
ty, o
r inf
irmity
; cal
cula
ted
to m
aint
ain
orpr
eclu
de d
eter
iora
tion
of h
ealth
or f
unct
iona
l abi
lity;
indi
vidu
alize
d, s
peci
fic,
and
cons
iste
nt w
ith s
ympt
oms
or c
onfir
med
dia
gnos
is o
f the
illn
ess,
dis
abili
ty,
or in
jury
und
er tr
eatm
ent;
not i
n ex
cess
of t
he in
divi
dual
’s ne
eds;
nec
essa
ryan
d co
nsis
tent
with
gen
eral
ly a
ccep
ted
prof
essi
onal
med
ical
sta
ndar
ds a
sde
term
ined
by
the
Secr
etar
y of
Hea
lth a
nd H
uman
Ser
vice
s or
the
stat
eDe
partm
ent o
f Hea
lth; a
nd re
flect
ive
of th
e le
vel o
f ser
vice
that
can
be
safe
lypr
ovid
ed a
nd fo
r whi
ch n
o eq
ually
effe
ctiv
e tre
atm
ent i
s av
aila
ble.
“A S
trong
and
Cons
iste
ntDe
finiti
on o
fM
edic
alN
eces
sity
For
ms
the
Core
of
Mea
ning
ful
Patie
ntPr
otec
tions
”
Cons
ortiu
m fo
rCi
tizen
s w
ithDi
sabi
litie
s
2000
Amer
ican
Med
ical
Asso
ciat
ion
Sect
ion
1.9
defin
es m
edic
ally
nec
essa
ry/m
edic
al n
eces
sity
as
heal
th c
are
serv
ices
or p
rodu
cts
that
a p
rude
nt p
hysi
cian
wou
ld p
rovi
de to
a p
atie
nt fo
rth
e pu
rpos
e of
pre
vent
ing,
dia
gnos
ing,
or t
reat
ing
an il
lnes
s, in
jury
, dis
ease
,or
its s
ympt
oms
in a
man
ner t
hat i
s (1
) in
acco
rdan
ce w
ith g
ener
ally
acc
epte
dst
anda
rds
of m
edic
al p
ract
ice;
(2) c
linic
ally
app
ropr
iate
in te
rms
of ty
pe,
frequ
ency
, ext
ent,
site
, and
dur
atio
n; a
nd (3
) not
prim
arily
for t
he c
onve
nien
ceof
the
patie
nt, p
hysi
cian
, or o
ther
hea
lth c
are
prov
ider
.
AMA
Mod
elPr
ovid
er C
ontra
ct
1 Defin
ition
s ha
ve b
een
take
n ve
rbat
im fr
om th
e re
leva
nt d
ocum
ent;
quot
atio
n m
arks
hav
e be
en o
mitt
ed.

Special Report50
2000
Unite
d Be
havi
oral
Heal
thSo
urce
: UBH
Cons
ent
Agre
emen
t with
Mai
ne B
urea
uof
Insu
ranc
e
Med
ical
Nec
essi
ty—
heal
th c
are
serv
ices
and
sup
plie
s th
at a
re d
eter
min
ed b
y th
e Pl
an to
be
med
ical
ly a
ppro
pria
te, a
nd (1
) nec
essa
ry to
mee
tth
eba
sic
heal
th n
eeds
of t
he c
over
ed p
erso
n; (2
) ren
dere
d in
the
type
of s
ettin
g ap
prop
riate
for t
he d
eliv
ery
of th
e he
alth
ser
vice
; (3)
con
sist
ent
inty
pe, f
requ
ency
, and
dur
atio
n of
trea
tmen
t with
Uni
ted
Beha
vior
al H
ealth
gui
delin
es; (
4) c
onsi
sten
t with
the
diag
nosi
s of
the
cond
ition
;(5
)req
uire
d fo
r rea
sons
oth
er th
an th
e co
mfo
rt or
con
veni
ence
of t
he c
over
ed p
erso
n or
his
or h
er p
hysi
cian
; and
(6) o
f dem
onst
rate
d m
edic
alva
lue.
[Ava
ilabl
eat
: http
://w
ww
.sta
te.m
e.us
/pfr/
ins/
ins0
0300
5.ht
m]
1999
Cign
a Be
havi
oral
Heal
th C
are
Sour
ce: C
igna
’s“L
evel
of C
are
Guid
elin
es fo
rM
enta
l Hea
lthan
d Su
bsta
nce
Abus
eTr
eatm
ent”
In c
onsi
derin
g th
e ap
prop
riate
ness
of a
ny le
vel o
f car
e, th
e fo
ur b
asic
ele
men
ts o
f Med
ical
Nec
essi
ty s
houl
d be
pre
sent
: (1)
a d
iagn
osis
as
defin
edby
sta
ndar
d di
agno
stic
nom
encl
atur
es (D
SM-IV
or i
ts e
quiv
alen
t in
ICD-
9-CM
) and
an
indi
vidu
alize
d tre
atm
ent p
lan
appr
opria
te fo
r the
parti
cipa
nt’s
illne
ss o
r con
ditio
n; (2
) a re
ason
able
exp
ecta
tion
that
the
parti
cipa
nt’s
illne
ss, c
ondi
tion,
or l
evel
of f
unct
ioni
ng w
ill im
prov
e th
roug
htre
atm
ent;
(3)t
he tr
eatm
ent i
s sa
fe a
nd e
ffect
ive
acco
rdin
g to
nat
iona
lly a
ccep
ted
stan
dard
clin
ical
evi
denc
e ge
nera
lly re
cogn
ized
by m
enta
lhe
alth
or s
ubst
ance
abu
se p
rofe
ssio
nals
; and
(4) i
t is
the
mos
t app
ropr
iate
and
cos
t-effe
ctiv
e le
vel o
f car
e th
at c
an s
afel
y be
pro
vide
d fo
r the
parti
cipa
nt’s
imm
edia
te c
ondi
tion.
[Ava
ilabl
e at
: http
s://a
pps.
cign
abeh
avio
ral.c
om/w
eb/b
asic
site
/pro
vide
r/pdf
/Lev
elof
Care
Guid
elin
es_2
003.
pdf]
2000
High
mar
k Bl
ueCr
oss
Blue
Shi
eld
(from
AHR
Qre
port
on c
over
-ag
e de
cisi
ons)
Year
Sour
ceM
edic
al N
eces
sity
Def
initi
on1
2000
Anon
ymou
sM
anag
edBe
havi
oral
Hea
lthPl
an P
rovi
der
Pack
et
“Med
ical
Nec
essi
ty”
is u
sed
here
to m
ean
care
whi
ch th
at is
det
erm
ined
to b
e ef
fect
ive,
app
ropr
iate
and
nec
essa
ry to
trea
t a g
iven
pat
ient
’sdi
sord
er. F
or a
ll le
vels
and
type
s of
car
e, th
e de
finiti
on is
as
follo
ws:
(1) t
he p
atie
nt m
ust h
ave
been
dia
gnos
ed w
ith a
psy
chia
tric
illne
ss b
y a
licen
sed
men
tal h
ealth
pro
fess
iona
l; (2
) sym
ptom
s of
this
illn
ess
mus
t acc
ord
with
thos
e de
scrib
ed in
the
DSM
-IV; (
3) th
e di
agno
sis
mus
t hav
ebe
enar
rived
at p
rior t
o ad
mis
sion
in a
face
-to-fa
ce e
ncou
nter
bet
wee
n th
e pr
ofes
sion
al a
nd p
atie
nt. [
Not
e: T
he c
ompa
ny d
efin
es s
epar
ate
adm
issi
on a
nd c
ontin
uing
car
e cr
iteria
by
type
of s
ervi
ce, e
.g.,
inpa
tient
and
out
patie
nt p
sych
iatri
c tre
atm
ent,
subs
tanc
e de
pend
ence
trea
tmen
t,re
side
ntia
l tre
atm
ent,
met
hado
ne m
aint
enan
ce, e
lect
roco
nvul
sive
ther
apy,
psy
chol
ogic
al te
stin
g, e
tc.]
2001
Valu
eOpt
ions
Prov
ider
s M
anua
l(a
vaila
ble
onlin
e)
Med
ical
ly n
eces
sary
trea
tmen
t is
that
whi
ch is
: int
ende
d to
pre
vent
, dia
gnos
e, c
orre
ct, c
ure,
alle
viat
e, o
r pre
clud
e de
terio
ratio
n of
a d
iagn
osab
leco
nditi
on (I
CD-9
or D
SM-IV
) tha
t thr
eate
ns li
fe, c
ause
s pa
in o
r suf
ferin
g, o
r res
ults
in il
lnes
s or
infir
mity
; exp
ecte
d to
impr
ove
an in
divi
dual
’s co
n-di
tion
or le
vel o
f fun
ctio
ning
; ind
ivid
ualiz
ed, s
peci
fic, a
nd c
onsi
sten
t with
sym
ptom
s an
d di
agno
sis,
and
not
in e
xces
s of
pat
ient
’s ne
eds;
ess
entia
lan
d co
nsis
tent
with
nat
iona
lly a
ccep
ted
stan
dard
evi
denc
e ge
nera
lly re
cogn
ized
by m
enta
l hea
lth o
r sub
stan
ce a
buse
car
e pr
ofes
sion
s or
publ
icat
ions
; ref
lect
ive
of a
leve
l of s
ervi
ce th
at is
saf
e, w
here
no
equa
lly e
ffect
ive,
mor
e co
nser
vativ
e, a
nd le
ss c
ostly
trea
tmen
t is
avai
labl
e;no
tprim
arily
inte
nded
for t
he c
onve
nien
ce o
f the
reci
pien
t, ca
reta
ker,
or p
rovi
der;
no m
ore
inte
nsiv
e or
rest
rictiv
e th
an n
eces
sary
to b
alan
cesa
fety
, effe
ctiv
enes
s, a
nd e
ffici
ency
; and
not
a s
ubst
itute
for n
on-tr
eatm
ent s
ervi
ces
addr
essi
ng e
nviro
nmen
tal f
acto
rs.
Tab
le 2
. Med
ical
Nec
essi
ty D
efin
itio
ns:
Man
aged
Car
e In
du
stry
Cove
rage
pro
cess
—co
ntra
ctua
l def
initi
on o
f med
ical
nec
essi
ty, w
hich
incl
udes
the
follo
win
g cr
iteria
for e
stab
lishi
ng th
e m
edic
al n
eces
sity
of
ase
rvic
e: a
ppro
pria
te fo
r sym
ptom
s, d
iagn
osis
, and
trea
tmen
t of a
con
ditio
n, il
lnes
s, o
r inj
ury;
pro
vide
d fo
r dia
gnos
is, d
irect
car
e, o
r tre
atm
ent;
inac
cord
ance
with
the
stan
dard
s of
goo
d m
edic
al p
ract
ice;
not
prim
arily
for t
he c
onve
nien
ce o
f the
mem
ber o
r mem
ber’s
pro
vide
r; th
e m
ost
appr
opria
te s
uppl
y or
leve
l of s
ervi
ce th
at c
an b
e sa
fely
pro
vide
d to
the
mem
ber.
To d
eter
min
e w
hat s
ervi
ces
mee
t thi
s de
finiti
on, H
ighm
ark
has
anin
form
atio
n-ga
ther
ing
proc
ess
that
incl
udes
sys
tem
atic
revi
ews
of p
ublis
hed
liter
atur
e, a
con
sulti
ng p
rogr
am w
ith p
ract
icin
g ph
ysic
ians
,re
view
of c
over
age
deci
sion
s by
Hig
hmar
k m
anag
ers,
revi
ew b
y an
inde
pend
ent M
edic
al A
ffairs
Com
mitt
ee.

Medical Necessity in Private Health Plans 51
Year
Case
Med
ical
Nec
essi
ty D
efin
ition
1
Tab
le 3
. Med
ical
Nec
essi
ty D
efin
itio
ns
Iden
tifi
ed in
Cas
e La
w (
So
rted
by
Cas
e N
ame)
1996
Banc
roft
v.Te
cum
seh
Prod
ucts
Com
pany
Cove
red
char
ges
incl
ude
only
thos
e in
curr
ed fo
r ser
vice
s or
item
s sp
ecifi
cally
reco
mm
ende
d by
a li
cens
ed p
hysi
cian
as
nece
ssar
y fo
r the
dia
gnos
is,
care
, or t
reat
men
t of a
phy
sica
l or m
enta
l con
ditio
n, a
nd fa
lling
with
in th
e Pl
an g
uide
lines
. For
a s
ervi
ce to
be
dete
rmin
ed a
s ne
cess
ary
for m
edic
alca
re, i
t mus
t be
wid
ely
acce
pted
by
med
ical
pro
fess
iona
ls in
the
Unite
d St
ates
as
effe
ctiv
e, a
ppro
pria
te, a
nd e
ssen
tial u
nder
reco
gnize
d he
alth
care
sta
ndar
ds.
1994
Blue
Cro
ss a
ndBl
ue S
hiel
d of
Virg
inia
v.
Kath
arin
e Ke
ller
A m
edic
ally
nec
essa
ry s
ervi
ce is
one
requ
ired
to id
entif
y or
trea
t an
illne
ss, i
njur
y, o
r pre
gnan
cy-r
elat
ed c
ondi
tion
whi
ch a
Pro
vide
r has
dia
gnos
edor
reas
onab
ly s
uspe
cts.
To
be m
edic
ally
nec
essa
ry, t
he s
ervi
ce m
ust:
be c
onsi
sten
t with
the
diag
nosi
s of
you
r con
ditio
n; b
e in
acc
orda
nce
with
the
stan
dard
s of
goo
d m
edic
al p
ract
ice;
not
be
for t
he c
onve
nien
ce o
f the
pat
ient
, the
pat
ient
’s fa
mily
, or t
he P
rovi
der;
and
be p
erfo
rmed
in th
e le
ast
cost
ly s
ettin
g re
quire
d by
you
r med
ical
con
ditio
n.
1996
Bedr
ick
v.Tr
avel
ers
Insu
ranc
e
The
Trav
eler
s de
term
ines
, in
its d
iscr
etio
n, if
a s
ervi
ce o
r sup
ply
is m
edic
ally
nec
essa
ry fo
r the
dia
gnos
is a
nd tr
eatm
ent o
f an
acci
dent
al in
jury
or
sick
ness
. Thi
s de
term
inat
ion
is b
ased
on
and
cons
iste
nt w
ith s
tand
ards
app
rove
d by
Tra
vele
rs m
edic
al p
erso
nnel
. The
se s
tand
ards
are
dev
elop
ed,
in p
art,
with
con
side
ratio
n to
whe
ther
the
serv
ice
or s
uppl
y m
eets
the
follo
win
g: *
It is
app
ropr
iate
and
requ
ired
for t
he d
iagn
osis
or t
reat
men
t of
the
acci
dent
al in
jury
or s
ickn
ess.
*It
is s
afe
and
effe
ctiv
e ac
cord
ing
to a
ccep
ted
clin
ical
evi
denc
e re
porte
d by
gen
eral
ly re
cogn
ized
med
ical
prof
essi
onal
s an
d pu
blic
atio
ns. *
Ther
e is
not
a le
ss in
tens
ive
or m
ore
appr
opria
te d
iagn
ostic
or t
reat
men
t alte
rnat
ive
that
cou
ld h
ave
been
use
din
lieu
of th
e se
rvic
e or
sup
ply
give
n. A
det
erm
inat
ion
that
a s
ervi
ce o
r sup
ply
is n
ot m
edic
ally
nec
essa
ry m
ay a
pply
to th
e en
tire
serv
ice
or s
uppl
yor
to a
ny p
art o
f the
ser
vice
or s
uppl
y.
1993
Dettm
er C
linic
v.
Asso
ciat
edIn
sura
nce
Com
pani
es, I
nc.
The
grou
p co
ntra
ct d
efin
es “
med
ical
ly n
eces
sary
” or
“m
edic
al n
eces
sity
” as
thos
e: s
ervi
ces
or s
uppl
ies,
pro
vide
d by
a P
rovi
der,
Faci
lity,
or
Prov
ider
Indi
vidu
al, w
hich
are
requ
ired
for t
reat
men
t of i
llnes
s, in
jury
, dis
ease
d co
nditi
on, o
r im
pairm
ent a
nd a
re: (
a) c
onsi
sten
t with
the
Insu
red’
sdi
agno
sis
or s
ympt
oms;
(b) a
ppro
pria
te tr
eatm
ent a
ccor
ding
to g
ener
ally
acc
epte
d st
anda
rds
of m
edic
al p
ract
ice;
(c) n
ot p
rovi
ded
only
as
aco
nven
ienc
e to
the
Insu
red
or P
rovi
der (
d) n
ot In
vest
igat
iona
l or u
npro
ven;
and
(e) n
ot e
xces
sive
in s
cope
, dur
atio
n, o
r int
ensi
ty to
pro
vide
saf
e,ad
equa
te, a
nd a
ppro
pria
te tr
eatm
ent t
o th
e In
sure
d. A
ny s
ervi
ce o
r sup
ply
prov
ided
at a
Pro
vide
r Fac
ility
will
not
be
cons
ider
ed m
edic
ally
nece
ssar
y if
the
Insu
red’
s sy
mpt
oms
or c
ondi
tion
indi
cate
that
it w
ould
be
safe
to p
rovi
de th
e se
rvic
e or
sup
ply
in a
less
com
preh
ensi
ve s
ettin
g.Th
e fa
ct th
at a
ny p
artic
ular
Pro
vide
r Ind
ivid
ual m
ay p
resc
ribe,
ord
er, r
ecom
men
d, o
r app
rove
a s
ervi
ce, s
uppl
y, o
r lev
el o
f car
e do
es n
ot, o
fits
elf,
mak
e su
ch tr
eatm
ent m
edic
ally
nec
essa
ry o
r mak
e th
e ch
arge
a C
over
ed C
harg
e un
der t
his
Cont
ract
.
1996
Esda
le v
.Am
eric
anCo
mm
unity
Mut
ual I
nsur
ance
Com
pany
Med
ical
ly n
eces
sary
mea
ns re
com
men
ded
by a
lice
nsed
phy
sici
an a
nd c
omm
only
reco
gnize
d in
the
licen
sed
phys
icia
n’s
prof
essi
on a
s pr
oper
care
or tr
eatm
ent.
Med
ical
ly N
eces
sary
doe
s no
t mea
n a
proc
edur
e th
at is
dee
med
exp
erim
enta
l or i
nves
tigat
iona
l in
natu
re b
y an
y ap
prop
riate
tech
nolo
gica
l ass
essm
ent b
ody
esta
blis
hed
by a
ny s
tate
or f
eder
al g
over
nmen
t.
1993
Evan
s v.
Blu
eCr
oss
Blue
Shi
eld
of S
outh
Car
olin
a
Med
ical
ly N
eces
sary
: ben
efits
are
pay
able
for s
ervi
ces
or s
uppl
ies
that
are
med
ical
ly n
eces
sary
. The
sim
ple
fact
that
a p
hysi
cian
has
per
form
edor
pres
crib
ed s
omet
hing
doe
s no
t mea
n th
at it
is m
edic
ally
nec
essa
ry. S
ome
serv
ices
or s
uppl
ies
that
you
get
may
not
be
cove
red
unde
r you
rin
sura
nce
heal
th p
olic
y. E
xpen
ses
for t
he fo
llow
ing
will
not
be
paid
: *S
urge
ry ju
st to
mak
e yo
u lo
ok b
ette
r (us
ually
cal
led
cosm
etic
sur
gery
) *E
xper
imen
tal s
urge
ry o
r ser
vice
s, s
uch
as a
cupu
nctu
re o
r sex
cha
nge
*Ser
vice
s or
sup
plie
s th
at a
re n
ot m
edic
ally
nec
essa
ry, i
nclu
ding
luxu
ry o
r con
veni
ence
item
s an
d tra
vel e
xpen
ses
(exc
ept t
hose
pro
vide
d fo
r hum
an o
rgan
tran
spla
nts)
.
1 Defin
ition
s ar
e ve
rbat
im fr
om c
ase
law
; quo
tatio
n m
arks
hav
e be
en o
mitt
ed.

Special Report52
1992
Farle
y v.
Ben
efit
Trus
t Life
Insu
ranc
eCo
mpa
ny
The
insu
ranc
e co
ntra
ct d
efin
es “
med
ical
ly n
eces
sary
” tre
atm
ent a
s “d
rugs
, the
rapi
es, o
r oth
er tr
eatm
ents
that
are
requ
ired
and
appr
opria
te c
are
for t
he s
ickn
ess
or th
e in
jury
; and
that
are
giv
en in
acc
orda
nce
with
gen
eral
ly a
ccep
ted
prin
cipl
es o
f med
ical
pra
ctic
e in
the
U.S.
at t
he ti
me
furn
ishe
d; a
nd th
at a
re a
ppro
ved
for r
eim
burs
emen
t by
the
Heal
th C
are
Fina
ncin
g Ad
min
istra
tion;
and
that
are
not
exp
erim
enta
l, ed
ucat
iona
l, or
inve
stig
atio
nal;
and
that
are
not
furn
ishe
d in
con
nect
ion
with
med
ical
or o
ther
rese
arch
.”
1993
Flor
ence
Nig
htin
gale
Nur
sing
Ser
vice
,In
c. v
. Blu
e Cr
oss
Blue
Shi
eld
ofAl
abam
a
Med
ical
ly N
eces
sary
mea
ns th
e us
e of
a H
ospi
tal o
r the
furn
ishi
ng o
f oth
er s
ervi
ces
or s
uppl
ies
whi
ch a
re n
eces
sary
to tr
eat a
Mem
ber’s
illn
ess
orin
jury
. To
be m
edic
ally
nec
essa
ry, t
he s
ervi
ces
and
supp
lies
furn
ishe
d m
ust (
as d
eter
min
ed b
y th
e Cl
aim
s Ad
min
istra
tor):
be
appr
opria
te a
ndne
cess
ary
for t
he s
ympt
oms,
dia
gnos
is, o
r tre
atm
ent o
f the
Mem
ber’s
con
ditio
n, d
isea
se, a
ilmen
t, or
inju
ry; b
e pr
ovid
ed fo
r the
dia
gnos
is o
r dire
ctca
re o
f the
Mem
ber’s
med
ical
con
ditio
n; b
e in
acc
orda
nce
with
sta
ndar
ds o
f goo
d m
edic
al p
ract
ice
acce
pted
by
the
orga
nize
d m
edic
al c
omm
unity
;an
d no
t be
sole
ly fo
r the
con
veni
ence
of t
he M
embe
r, hi
s fa
mily
, his
Phy
sici
an o
r ano
ther
pro
vide
r of s
ervi
ces;
not
be
expe
rimen
tal o
r inv
estig
ativ
e;an
d be
per
form
ed in
the
leas
t cos
tly s
ettin
g th
e M
embe
r’s m
edic
al c
ondi
tion
requ
ires.
1994
Feni
o v.
Mut
ual o
fOm
aha
Insu
ranc
eCo
mpa
ny
“Med
ical
ly N
eces
sary
” se
rvic
e or
sup
ply
mea
ns o
ne w
hich
: (a)
is a
ppro
pria
te a
nd c
onsi
sten
t with
the
diag
nosi
s in
acc
ord
with
acc
epte
d st
anda
rds
of c
omm
unity
pra
ctic
e; (b
) is
not c
onsi
dere
d ex
perim
enta
l or i
nves
tigat
ive;
(c) c
ould
not
hav
e be
en o
mitt
ed w
ithou
t adv
erse
ly a
ffect
ing
the
insu
red
pers
on’s
cond
ition
or q
ualit
y of
med
ical
car
e.
Year
Case
Med
ical
Nec
essi
ty D
efin
ition
1
Tab
le 3
. Co
nti
nu
ed
1996
Harr
ison
v. A
etna
Life
Insu
ranc
eCo
mpa
ny
“Nec
essa
ry”
mea
ns a
ser
vice
or s
uppl
y w
hich
is n
eces
sary
for t
he: d
iagn
osis
; or c
are;
or t
reat
men
t; of
the
phys
ical
or m
enta
l con
ditio
n in
volv
ed.
Itm
ust b
e w
idel
y ac
cept
ed p
rofe
ssio
nally
in th
e Un
ited
Stat
es a
s: e
ffect
ive;
and
app
ropr
iate
; and
ess
entia
l; ba
sed
upon
reco
gnize
d st
anda
rds
ofth
ehe
alth
car
e sp
ecia
lty in
volv
ed.
1995
Gret
he v
.Tr
ustm
ark
Insu
ranc
eCo
mpa
ny
The
term
“M
edic
ally
Nec
essa
ry”
as u
sed
abov
e m
eans
: dru
gs, t
hera
pies
, or o
ther
trea
tmen
ts th
at a
re re
quire
d an
d ap
prop
riate
for c
are
of th
esi
ckne
ss o
r the
inju
ry; a
nd th
at a
re g
iven
in a
ccor
danc
e w
ith g
ener
ally
acc
epte
d pr
inci
ples
of m
edic
al p
ract
ice
in th
e U.
S. a
t the
tim
e fu
rnis
hed;
and
that
are
reim
burs
ed b
y M
edic
are;
and
are
not
dee
med
to b
e ex
perim
enta
l, ed
ucat
iona
l, or
inve
stig
atio
nal i
n na
ture
by
any
appr
opria
te te
chno
-lo
gica
l ass
essm
ent b
ody
esta
blis
hed
by a
ny s
tate
or f
eder
al g
over
nmen
t; an
d th
at a
re n
ot fu
rnis
hed
in c
onne
ctio
n w
ith m
edic
al o
r oth
er re
sear
ch.
2001
Hund
ley
v.W
enze
lM
edic
ally
nec
essa
ry m
eans
that
a s
ervi
ce o
r sup
ply
is n
eces
sary
and
app
ropr
iate
for t
he d
iagn
osis
and
trea
tmen
t of a
n ill
ness
or i
njur
y ba
sed
on g
ener
ally
acc
epte
d cu
rren
t med
ical
pra
ctic
e. A
ser
vice
or s
uppl
y w
ill n
ot b
e co
nsid
ered
med
ical
ly n
eces
sary
if a
ny o
f the
follo
win
g ap
ply:
(1)I
t is
prov
ided
onl
y as
a c
onve
nien
ce to
the
cove
red
pers
on o
r pro
vide
r; (2
) It i
s no
t app
ropr
iate
trea
tmen
t for
the
cove
red
pers
on’s
diag
nosi
sor
sym
ptom
s; (3
) It e
xcee
ds (i
n sc
ope,
dur
atio
n, o
r int
ensi
ty) t
he le
vel o
f car
e th
at is
nee
ded
to p
rovi
de s
afe,
ade
quat
e, a
nd a
ppro
pria
te d
iagn
osis
or tr
eatm
ent;
(4) I
t is
part
of a
n ex
perim
enta
l tre
atm
ent.
The
fact
that
any
par
ticul
ar d
octo
r may
pre
scrib
e, o
rder
, rec
omm
end,
or a
ppro
ve a
serv
ice
or s
uppl
ydo
es n
ot, o
f its
elf,
mak
e th
e se
rvic
e or
sup
ply
med
ical
ly n
eces
sary
.
2000
Julia
no v
. HM
O of
New
Jer
sey,
Inc.
,db
a U.
S.He
alth
Care
The
Cont
ract
def
ines
“M
edic
ally
Nec
essa
ry o
r Med
ical
Nec
essi
ty”
as a
ppro
pria
te a
nd n
eces
sary
ser
vice
s as
def
ined
by
HMO
whi
ch a
re re
nder
edto
a M
embe
r for
a c
ondi
tion
requ
iring
, acc
ordi
ng to
gen
eral
ly a
ccep
ted
prin
cipl
es o
f goo
d m
edic
al p
ract
ice,
the
diag
nosi
s or
dire
ct c
are
and
treat
-m
ent o
f an
illne
ss o
r inj
ury
and
whi
ch a
re n
ot p
rovi
ded
only
as
a co
nven
ienc
e.

Medical Necessity in Private Health Plans 53
Year
Case
Med
ical
Nec
essi
ty D
efin
ition
1
Tab
le 3
. Co
nti
nu
ed
1998
Killi
an v
s.He
alth
Sour
cePr
ovid
ent
Adm
inis
trato
rs,
Inc.
Med
ical
ly N
eces
sary
and
/or M
edic
al N
eces
sity
—Se
rvic
es o
r sup
plie
s pr
ovid
ed b
y a:
(1) H
ospi
tal,
(2) P
hysi
cian
, or (
3) o
ther
qua
lifie
d pr
ovid
er...
are
med
ical
ly n
eces
sary
if th
ey a
re: (
1) re
quire
d fo
r the
dia
gnos
is a
nd/o
r tre
atm
ent o
f the
par
ticul
ar c
ondi
tion,
dis
ease
, inj
ury
or il
lnes
s; (2
) con
sist
ent
with
the
sym
ptom
or d
iagn
osis
and
trea
tmen
t of t
he c
ondi
tion,
dis
ease
, inj
ury,
or i
llnes
s; (3
) com
mon
ly a
nd u
sual
ly n
oted
thro
ugho
ut th
e m
edic
alfie
ld a
s pr
oper
to tr
eat t
he d
iagn
osed
con
ditio
n, d
isea
se, i
njur
y, o
r illn
ess;
and
(4) t
he m
ost f
ittin
g su
pply
or l
evel
of s
ervi
ce w
hich
can
be
safe
lygi
ven.
1998
McG
raw
v.
Prud
entia
lIn
sura
nce
To b
e co
nsid
ered
“ne
eded
”, a
ser
vice
or s
uppl
y m
ust b
e de
term
ined
by
Prud
entia
l to
mee
t all
of th
ese
test
s: (a
) It i
s or
dere
d by
a D
octo
r; (b
) It i
sre
cogn
ized
thro
ugho
ut th
e Do
ctor
’s pr
ofes
sion
as
safe
and
effe
ctiv
e, is
requ
ired
for t
he d
iagn
osis
or t
reat
men
t of t
he p
artic
ular
sic
knes
s or
inju
ry,
and
is e
mpl
oyed
app
ropr
iate
ly in
a m
anne
r and
set
ting
cons
iste
nt w
ith g
ener
ally
acc
epte
d Un
ited
Stat
es m
edic
al s
tand
ards
; (c)
It is
nei
ther
edu
-ca
tiona
l nor
exp
erim
enta
l or i
nves
tigat
iona
l in
natu
re. T
he c
ase
also
men
tions
: “As
we
read
the
reco
rd, P
rude
ntia
l has
mod
ified
its
defin
ition
of
“med
ical
nec
essa
ry”
with
the
addi
tiona
l req
uire
men
t the
trea
tmen
t pro
vide
a m
easu
rabl
e an
d su
bsta
ntia
l inc
reas
e in
func
tiona
l abi
lity
for a
con
di-
tion
havi
ng p
oten
tial f
or s
igni
fican
t im
prov
emen
t.”
1995
Korn
man
v. B
lue
Cros
s Bl
ue S
hiel
dof
Lou
isia
na
1985
pol
icy
defin
es “
med
ical
ly n
eces
sary
” as
hea
lth s
ervi
ces
whi
ch: a
re a
ppro
pria
te a
nd c
onsi
sten
t with
the
diag
nosi
s an
d w
hich
, in
acco
rdan
cew
ith a
ccep
ted
med
ical
sta
ndar
ds in
the
Stat
e of
Lou
isia
na, c
ould
not
hav
e be
en o
mitt
ed w
ithou
t adv
erse
ly a
nd s
ever
ely
affe
ctin
g th
e pa
tient
’sco
nditi
on; a
re n
ot p
rimar
ily c
usto
dial
car
e; a
re a
ppro
pria
te a
nd c
an b
e sa
fely
use
d un
der t
he c
ircum
stan
ces.
Inpa
tient
hos
pita
l ser
vice
s sh
ould
be
used
onl
y w
hen
a le
sser
equ
ippe
d fa
cilit
y (e
.g.,
outp
atie
nt h
ospi
tal s
ervi
ces,
phy
sici
an’s
offic
e, e
tc) c
ould
adv
erse
ly a
nd s
ever
ely
affe
ct th
e pa
tient
’sco
nditi
on. 1
987
polic
y: “
Med
ical
ly N
eces
sary
” m
eans
a s
ervi
ce o
r tre
atm
ent w
hich
, in
the
judg
men
t of t
he p
lan:
(1) I
s ap
prop
riate
and
con
sist
ent
with
the
diag
nosi
s an
d w
hich
, in
acco
rdan
ce w
ith a
ccep
ted
med
ical
sta
ndar
ds in
the
Stat
e of
Lou
isia
na, c
ould
not
hav
e be
en o
mitt
ed w
ithou
tad
vers
ely
affe
ctin
g th
e pa
tient
’s co
nditi
on o
r the
qua
lity
of m
edic
al c
are
rend
ered
; (2)
Is n
ot p
rimar
ily c
usto
dial
car
e; a
nd (3
) as
to in
stitu
tiona
l car
e,co
uld
not h
ave
been
pro
vide
d in
a p
hysi
cian
’s of
fice,
in th
e ou
tpat
ient
dep
artm
ent o
f a h
ospi
tal,
or in
a le
sser
faci
lity
with
out a
ffect
ing
the
patie
nt’s
cond
ition
or q
ualit
y of
med
ical
car
e re
nder
ed.
1999
Milo
ne v
.Ex
clus
ive
Heal
thca
re, I
nc.
A m
edic
ally
nec
essa
ry s
ervi
ce o
r sup
ply
mea
ns o
ne w
hich
is o
rder
ed o
r aut
horiz
ed b
y th
e Pr
imar
y Ca
re P
hysi
cian
, and
with
the
Prim
ary
Care
Phys
icia
n, o
ur m
edic
al s
taff
or o
ur M
edic
al D
irect
or a
nd/o
r a q
ualif
ied
party
or e
ntity
sel
ecte
d by
us
dete
rmin
es is
: (1)
pro
vide
d fo
r the
dia
gnos
isor
dire
ct tr
eatm
ent o
f an
inju
ry o
r sic
knes
s; (2
) app
ropr
iate
and
con
sist
ent w
ith th
e sy
mpt
oms
and
findi
ngs
or d
iagn
osis
and
trea
tmen
t of t
hem
embe
r’s in
jury
or s
ickn
ess;
(3) p
rovi
ded
in a
ccor
d w
ith g
ener
ally
acc
epte
d m
edic
al p
ract
ice
on a
nat
iona
l bas
is; a
nd (4
) the
mos
t app
ropr
iate
supp
ly o
r lev
el o
f ser
vice
whi
ch c
an b
e pr
ovid
ed o
n a
cost
-effe
ctiv
e ba
sis
(incl
udin
g, b
ut n
ot li
mite
d to
, inp
atie
nt v
s. o
utpa
tient
car
e, e
lect
ric v
s.m
anua
l whe
elch
air,
surg
ical
vs.
med
ical
or o
ther
type
s of
car
e). T
he fa
ct th
at th
e m
embe
r’s p
hysi
cian
pre
scrib
es s
ervi
ces
or s
uppl
ies
does
not
auto
mat
ical
ly m
ean
such
ser
vice
s or
sup
plie
s ar
e m
edic
ally
nec
essa
ry a
nd c
over
ed b
y th
e Co
ntra
ct.
2001
Milo
ne v
.Ex
clus
ive
Heal
thCa
re, I
nc.
The
Plan
def
ines
med
ical
nec
essi
ty a
s fo
llow
s: A
med
ical
ly n
eces
sary
ser
vice
or s
uppl
y m
eans
one
whi
ch is
ord
ered
or a
utho
rized
by
the
Prim
ary
Care
Phy
sici
an, a
nd w
hich
the
Prim
ary
Care
Phy
sici
an, o
ur m
edic
al s
taff
or o
ur M
edic
al D
irect
or a
nd/o
r a q
ualif
ied
party
or e
ntity
sel
ecte
d by
us
dete
rmin
es is
: (a)
pro
vide
d fo
r the
dia
gnos
is o
r dire
ct tr
eatm
ent o
f an
inju
ry o
r sic
knes
s; (b
) app
ropr
iate
and
con
sist
ent w
ith th
e sy
mpt
oms
and
find-
ings
or d
iagn
osis
and
trea
tmen
t of t
he m
embe
r’s in
jury
or s
ickn
ess;
(c) p
rovi
ded
in a
ccor
d w
ith g
ener
ally
acc
epte
d m
edic
al p
ract
ice
on a
nat
iona
lba
sis;
and
(d) t
he m
ost a
ppro
pria
te s
uppl
y or
leve
l of s
ervi
ce w
hich
can
be
prov
ided
on
a co
st-e
ffect
ive
basi
s (in
clud
ing,
but
not
lim
ited
to, i
npat
ient
vs. o
utpa
tient
car
e, e
lect
ric v
s. m
anua
l whe
elch
air,
surg
ical
vs.
med
ical
or o
ther
type
s of
car
e). T
he fa
ct th
at th
e m
embe
r’s p
hysi
cian
pre
scrib
esse
rvic
es o
r sup
plie
s do
es n
ot a
utom
atic
ally
mea
n su
ch s
ervi
ces
or s
uppl
ies
are
med
ical
ly n
eces
sary
and
cov
ered
by
the
Cont
ract
.
1 Defin
ition
s ha
ve b
een
take
n ve
rbat
im fr
om th
e re
leva
nt d
ocum
ent;
quot
atio
n m
arks
hav
e be
en o
mitt
ed.

Special Report54
1994
Nor
thw
est
Laun
dry
and
Dry
Clea
ners
Hea
lthan
d W
elfa
re T
rust
Fund
v. B
urzy
nski
To b
e “m
edic
ally
nec
essa
ry”
unde
r the
Pla
n, a
trea
tmen
t mus
t mee
t tw
o re
quire
men
ts, m
easu
red
unde
r Ore
gon
law
. Firs
t, th
e tre
atm
ent m
ust
be“a
ppro
pria
te a
nd c
onsi
sten
t with
the
diag
nosi
s (in
acc
ord
with
acc
epte
d st
anda
rds
of c
omm
unity
pra
ctic
e).”
Sec
ond,
“m
edic
ally
nec
essa
ry”
treat
men
ts “
coul
d no
t be
omitt
ed w
ithou
t adv
erse
ly a
ffect
ing
the
cove
red
pers
on’s
cond
ition
or t
he q
ualit
y of
med
ical
car
e.”
2002
Rush
Pru
dent
ial
HMO,
Inc.
,Pe
titio
ner v
.De
bra
C. M
oran
et a
l.
A se
rvic
e is
cov
ered
as
“med
ical
ly n
eces
sary
” if
Rush
find
s:(a
) [Th
e se
rvic
e] is
furn
ishe
d or
aut
horiz
ed b
y a
Parti
cipa
ting
Doct
or fo
r the
dia
gnos
is o
r the
trea
tmen
t of a
Sic
knes
s or
Inju
ry o
r for
the
mai
nte-
nanc
e of
a p
erso
n’s
good
hea
lth.
(b) T
he p
reva
iling
opi
nion
with
in th
e ap
prop
riate
spe
cial
ty o
f the
Uni
ted
Stat
es m
edic
al p
rofe
ssio
n is
that
[the
ser
vice
] is
safe
and
effe
ctiv
e fo
rits
inte
nded
use
, and
that
its
omis
sion
wou
ld a
dver
sely
affe
ct th
e pe
rson
’s m
edic
al c
ondi
tion.
(c) I
t is
furn
ishe
d by
a p
rovi
der w
ith a
ppro
pria
te tr
aini
ng, e
xper
ienc
e, s
taff
and
faci
litie
s to
furn
ish
that
par
ticul
ar s
ervi
ce o
r sup
ply.
1997
Nic
hols
v.
Trus
tmar
kIn
sura
nce
Com
pany
Bene
fits
will
be
paid
onl
y fo
r “m
edic
ally
nec
essa
ry”
care
and
trea
tmen
t of s
ickn
ess
and
inju
ry. A
s us
ed a
bove
, ‘m
edic
ally
nec
essa
ry’ m
eans
:dr
ugs,
ther
apie
s, o
r oth
er tr
eatm
ents
that
are
requ
ired
and
appr
opria
te fo
r car
e of
the
sick
ness
or t
he in
jury
; and
that
are
giv
en in
acc
orda
nce
with
gene
rally
acc
epte
d pr
inci
ples
of m
edic
al p
ract
ice
in th
e U.
S. a
t the
tim
e fu
rnis
hed;
and
that
are
app
rove
d fo
r rei
mbu
rsem
ent b
y th
e He
alth
Car
eFi
nanc
ing
Adm
inis
tratio
n; a
nd th
at a
re n
ot e
xper
imen
tal,
educ
atio
nal,
or in
vest
igat
iona
l; an
d th
at a
re n
ot fu
rnis
hed
in c
onne
ctio
n w
ith m
edic
al o
rot
her r
esea
rch.
Year
Case
Med
ical
Nec
essi
ty D
efin
ition
1
Tab
le 3
. Co
nti
nu
ed
1993
Scal
aman
dre
v.Ox
ford
Hea
lthPl
ans,
Inc.
Med
ical
ly n
eces
sary
ser
vice
s an
d/or
sup
plie
s ar
e de
fined
as:
the
use
of s
ervi
ces
or s
uppl
ies
as p
rovi
ded
by a
hos
pita
l, sk
illed
nur
sing
faci
lity,
phys
icia
n, o
r oth
er p
rovi
der r
equi
red
to id
entif
y or
trea
t a M
embe
r’s il
lnes
s or
inju
ry a
nd w
hich
, as
dete
rmin
ed b
y th
e M
edic
al D
irect
or, a
re:
(1)C
onsi
sten
t with
the
sym
ptom
s or
dia
gnos
is a
nd tr
eatm
ent o
f the
Cov
ered
Per
son’
s co
nditi
on, d
isea
se, a
ilmen
t or i
njur
y; (2
) App
ropr
iate
with
rega
rd to
sta
ndar
ds o
f goo
d m
edic
al p
ract
ice;
(3) N
ot s
olel
y fo
r the
con
veni
ence
of t
he C
over
ed P
erso
n, h
is o
r her
phy
sici
an, h
ospi
tal,
or o
ther
heal
th c
are
prov
ider
; and
(4) T
he m
ost a
ppro
pria
te s
uppl
y or
leve
l of s
ervi
ce w
hich
can
be
safe
ly p
rovi
ded
to th
e Co
vere
d Pe
rson
. Whe
n sp
ecifi
-ca
lly a
pplie
d to
an
inpa
tient
, it f
urth
er m
eans
that
the
Cove
red
Pers
on’s
med
ical
sym
ptom
s or
con
ditio
n re
quire
s th
at th
e di
agno
sis
or tr
eatm
ent
cann
ot b
e sa
fely
pro
vide
d to
the
Cove
red
Pers
on a
s an
out
patie
nt.
1997
Soph
ie v
. Lin
coln
Nat
iona
l Life
Insu
ranc
eCo
mpa
ny
Med
ical
ly n
eces
sary
is d
efin
ed a
s: T
he e
xten
t of s
ervi
ces
requ
ired
to d
iagn
ose
or tr
eat a
Bod
ily In
jury
or S
ickn
ess
whi
ch is
kno
wn
to b
e sa
fe a
ndef
fect
ive
by m
ost Q
ualif
ied
Prac
titio
ners
who
are
lice
nsed
to d
iagn
ose
or tr
eat t
hat B
odily
Inju
ry o
r Sic
knes
s. S
uch
serv
ices
mus
t be
perfo
rmed
inth
e le
ast c
ostly
set
ting
requ
ired
by th
e pa
tient
’s co
nditi
on, a
nd m
ust n
ot b
e pr
ovid
ed p
rimar
ily fo
r the
con
veni
ence
of t
he p
atie
nt o
f the
Qua
lifie
dPr
actit
ione
r.
2001
Smith
v. N
ewpo
rtN
ews
Ship
build
ing
Heal
th P
lan
The
Plan
def
ines
‘nec
essa
ry’ a
s fo
llow
s: A
ser
vice
or s
uppl
y is
nec
essa
ry if
it is
for t
he d
iagn
osis
, car
e, o
r tre
atm
ent o
f a p
hysi
cal o
r men
tal c
ondi
-tio
n an
d w
idel
y ac
cept
ed p
rofe
ssio
nally
in th
e U.
S. a
s ef
fect
ive,
app
ropr
iate
, and
ess
entia
l, ba
sed
upon
reco
gnize
d st
anda
rds
of th
e he
alth
car
esp
ecia
lty in
volv
ed.

Medical Necessity in Private Health Plans 55
Tab
le 3
. Co
nti
nu
ed
Year
Case
Med
ical
Nec
essi
ty D
efin
ition
1
1994
Whi
tehe
ad v
.Fe
dera
l Exp
ress
Corp
orat
ion
Elig
ible
exp
ense
s fo
r tre
atm
ent o
f an
illne
ss o
r inj
ury
mus
t be
med
ical
ly n
eces
sary
und
er a
ll pl
an o
ptio
ns. M
edic
al n
eces
sity
is d
eter
min
ed b
y th
ecl
aim
s pa
ying
adm
inis
trato
r. Ca
re th
at is
med
ical
ly n
eces
sary
may
incl
ude,
but
is n
ot li
mite
d to
, car
e th
at is
: *co
mm
only
and
cus
tom
arily
reco
gnize
das
sta
ndar
ds o
f goo
d pr
actic
e; *
appr
opria
te a
nd c
onsi
sten
t with
the
diag
nosi
s or
trea
tmen
t of a
n ill
ness
or i
njur
y; *
appr
opria
te s
uppl
y or
leve
l of
serv
ice
that
can
be
safe
ly p
rovi
ded.
1998
Win
nega
v. N
orth
Cent
ral H
ealth
Prot
ectio
n Pl
an
Med
ical
ly n
eces
sary
ser
vice
s or
sup
plie
s ar
e de
fined
as:
(a) R
equi
red
for d
iagn
osis
or t
reat
men
t of t
he il
lnes
s or
sym
ptom
s; (b
) pro
vide
d fo
r the
diag
nosi
s or
dire
ct c
are
and
treat
men
t of t
he il
lnes
s; (c
) With
in th
e st
anda
rds
of n
orm
al m
edic
al p
ract
ice;
(d) N
ot p
rimar
ily fo
r the
con
veni
ence
of
the
Parti
cipa
nt o
r any
pro
vide
r; an
d (e
) a s
uppl
y or
leve
l of s
ervi
ces
requ
ired
to p
rovi
de s
afe
and
adeq
uate
car
e.
1996
Sven
v. P
rinci
pal
Mut
ual L
ifeIn
sura
nce
Com
pany
“Med
ical
ly N
eces
sary
Car
e” is
def
ined
as:
any
con
finem
ent,
treat
men
t, or
ser
vice
that
is p
resc
ribed
by
a ph
ysic
ian
and
dete
rmin
ed b
y th
eCo
mpa
ny [P
rinci
pal]
to b
e: (a
) nec
essa
ry a
nd a
ppro
pria
te; a
nd (b
) non
-exp
erim
enta
l and
non
-inve
stig
atio
nal a
nd n
ot in
con
flict
with
acc
epte
dm
edic
al s
tand
ards
.
1997
Squi
llace
v.
Wyo
min
g St
ate
Empl
oyee
and
Offic
ials
Gro
upIn
sura
nce
Boar
dof
Adm
inis
tratio
n
“Med
ical
ly N
eces
sary
” m
eans
any
ser
vice
s an
d su
pplie
s pr
ovid
ed fo
r the
dia
gnos
is a
nd tr
eatm
ent o
f a s
peci
fic il
lnes
s, in
jury
, or c
ondi
tion.
Suc
hse
rvic
es a
nd s
uppl
ies
mus
t be:
ord
ered
by
a do
ctor
; req
uire
d fo
r the
trea
tmen
t or m
anag
emen
t of a
med
ical
sym
ptom
or c
ondi
tion;
the
mos
t effi
-ci
ent a
nd e
cono
mic
al s
ervi
ce w
hich
can
saf
ely
be p
rovi
ded
to s
uch
pers
on; a
nd p
rovi
ded
in a
ccor
danc
e w
ith a
ppro
ved
and
gene
rally
acc
epte
dm
edic
al o
r sur
gica
l pra
ctic
e. W
e m
ay re
quire
pro
of in
writ
ing
satis
fact
orily
to u
s th
at a
ny ty
pe o
f tre
atm
ent,
serv
ice,
or s
uppy
rece
ived
is m
edic
ally
nece
ssar
y. M
edic
al n
eces
sity
will
be
dete
rmin
ed s
olel
y by
us.
The
fact
that
a d
octo
r may
pre
scrib
e, o
rder
, rec
omm
end,
or a
ppro
ve a
ser
vice
doe
sno
t, in
itse
lf, m
ake
such
ser
vice
or s
uppl
y m
edic
ally
nec
essa
ry.
1 Defin
ition
s ha
ve b
een
take
n ve
rbat
im fr
om th
e re
leva
nt d
ocum
ent;
quot
atio
n m
arks
hav
e be
en o
mitt
ed.

Special Report56
Tab
le 4
. Med
ical
Nec
essi
ty D
efin
itio
ns
Co
nta
ined
in S
tate
Sta
tute
s an
d R
egu
lati
on
s
Alab
ama
Non
eN
one
Stat
eSt
atut
e/Re
gula
tion
Med
ical
Nec
essi
ty D
efin
ition
1
Calif
orni
aCa
l. W
el. &
Inst
.Co
de§
1405
9.5
(200
1)
“Med
ical
ly n
eces
sary
” or
“m
edic
al n
eces
sity
”: A
ser
vice
is “
med
ical
ly n
eces
sary
” or
a “
med
ical
nec
essi
ty”
whe
n it
is re
ason
able
and
nece
ssar
yto
pro
tect
life
, to
prev
ent s
igni
fican
t illn
ess
or s
igni
fican
t dis
abili
ty, o
r to
alle
viat
e se
vere
pai
n.
Dela
war
e16
Del
. Cod
e §
9119
(200
0)
(IRO
Stat
ute)
For t
he p
urpo
se o
f thi
s ac
t, “m
edic
al n
eces
sity
” m
eans
the
prov
idin
g of
cov
ered
hea
lth s
ervi
ces
or p
rodu
cts
that
a p
rude
nt p
hysi
cian
wou
ldpr
ovid
e to
a p
atie
nt fo
r the
pur
pose
of d
iagn
osin
g or
trea
ting
an il
lnes
s, in
jury
, or d
isea
se o
r its
sym
ptom
s, in
a m
anne
r tha
t is:
(1
) In
acco
rdan
ce w
ith th
e ge
nera
lly a
ccep
ted
stan
dard
s of
med
ical
pra
ctic
e; (2
) Con
sist
ent w
ith th
e sy
mpt
oms
or tr
eatm
ent o
f the
con
ditio
n;an
d (3
) Not
sol
ely
for a
nyon
e’s
conv
enie
nce.
Arka
nsas
Ark.
Cod
e §
23-9
9-50
7 (2
001)
(b
) The
term
“m
edic
al n
eces
sity
” as
app
lied
to b
enef
its fo
r men
tal i
llnes
s an
d de
velo
pmen
tal d
isor
ders
mea
ns: (
1) R
easo
nabl
e an
d ne
cess
ary
for t
he d
iagn
osis
or t
reat
men
t of a
men
tal i
llnes
s, o
r to
impr
ove
or to
mai
ntai
n or
to p
reve
nt d
eter
iora
tion
of fu
nctio
ning
resu
lting
from
the
illne
ss o
r dev
elop
men
tal d
isor
der;
(2) F
urni
shed
in th
e m
ost a
ppro
pria
te a
nd le
ast r
estri
ctiv
e se
tting
in w
hich
ser
vice
s ca
n be
saf
ely
prov
ided
;(3
) The
mos
t app
ropr
iate
leve
l or s
uppl
y of
ser
vice
whi
ch c
an s
afel
y be
pro
vide
d; a
nd (4
) Cou
ld n
ot h
ave
been
om
itted
with
out a
dver
sely
affe
ctin
g th
e in
divi
dual
’s m
enta
l or p
hysi
cal h
ealth
, or b
oth,
or t
he q
ualit
y of
car
e re
nder
ed.
Alas
kaN
one
Non
e
Arizo
naN
one
Non
e
Colo
rado
Non
eN
one
Conn
ectic
utN
one
Non
e
Dist
rict o
fCo
lum
bia
Non
eN
one
Flor
ida
Fla.
Sta
t. §
627.
732
(200
1)“M
edic
ally
nec
essa
ry”
refe
rs to
a m
edic
al s
ervi
ce o
r sup
ply
that
a p
rude
nt p
hysi
cian
wou
ld p
rovi
de fo
r the
pur
pose
of p
reve
ntin
g, d
iagn
osin
g,or
trea
ting
an il
lnes
s, in
jury
, dis
ease
, or s
ympt
om in
a m
anne
r tha
t is:
(a) I
n ac
cord
ance
with
gen
eral
ly a
ccep
ted
stan
dard
s of
med
ical
pra
ctic
e;(b
) Clin
ical
ly a
ppro
pria
te in
term
s of
type
, fre
quen
cy, e
xten
t, si
te, a
nd d
urat
ion;
and
(c) N
ot p
rimar
ily fo
r the
con
veni
ence
of t
he p
atie
nt, p
hysi
-ci
an, o
r oth
er h
ealth
car
e pr
ovid
er.
Geor
gia
O.C.
G.A.
§
33-2
0A-3
1(2
000)
(IRO
Stat
ute)
(5) “
Med
ical
nec
essi
ty,”
“m
edic
ally
nec
essa
ry c
are,
” or
“m
edic
ally
nec
essa
ry a
nd a
ppro
pria
te”
mea
ns c
are
base
d up
on g
ener
ally
acc
epte
dm
edic
al p
ract
ices
in li
ght o
f con
ditio
ns a
t the
tim
e of
trea
tmen
t whi
ch is
: (A)
App
ropr
iate
and
con
sist
ent w
ith th
e di
agno
sis
and
the
omis
sion
ofw
hich
cou
ld a
dver
sely
affe
ct o
r fai
l to
impr
ove
the
elig
ible
enr
olle
e’s
cond
ition
; (B)
Com
patib
le w
ith th
e st
anda
rds
of a
ccep
tabl
e m
edic
alpr
actic
e in
the
Unite
d St
ates
; (C)
Pro
vide
d in
a s
afe
and
appr
opria
te s
ettin
g gi
ven
the
natu
re o
f the
dia
gnos
is a
nd th
e se
verit
y of
the
sym
ptom
s;(D
) Not
pro
vide
d so
lely
for t
he c
onve
nien
ce o
f the
elig
ible
enr
olle
e or
the
conv
enie
nce
of th
e he
alth
car
e pr
ovid
er o
r hos
pita
l; an
d (E
) Not
prim
arily
cus
todi
al c
are,
unl
ess
cust
odia
l car
e is
a c
over
ed b
enef
it un
der t
he e
ligib
le e
nrol
lee’
s ev
iden
ce o
f cov
erag
e.

Medical Necessity in Private Health Plans 57
1De
finiti
ons
have
bee
n ta
ken
verb
atim
from
the
rele
vant
doc
umen
t; qu
otat
ion
mar
ks h
ave
been
om
itted
.
Haw
aii
HRS
§ 43
2E-1
.4(2
000)
(IRO
Stat
ute)
Med
ical
nec
essi
ty (b
) A h
ealth
inte
rven
tion
is m
edic
ally
nec
essa
ry if
it is
reco
mm
ende
d by
the
treat
ing
phys
icia
n or
trea
ting
licen
sed
heal
thca
re p
rovi
der,
is a
ppro
ved
by th
e he
alth
pla
n’s
med
ical
dire
ctor
or p
hysi
cian
des
igne
e, a
nd is
: (1)
For
the
purp
ose
of tr
eatin
g a
med
ical
con
di-
tion;
(2) T
he m
ost a
ppro
pria
te d
eliv
ery
or le
vel o
f ser
vice
, con
side
ring
pote
ntia
l ben
efits
and
har
ms
to th
e pa
tient
; (3)
Kno
wn
to b
e ef
fect
ive
inim
prov
ing
heal
th o
utco
mes
; pro
vide
d th
at: (
A) E
ffect
iven
ess
is d
eter
min
ed fi
rst b
y sc
ient
ific
evid
ence
; (B)
If n
o sc
ient
ific
evid
ence
exi
sts,
then
by p
rofe
ssio
nal s
tand
ards
of c
are;
and
(C) I
f no
prof
essi
onal
sta
ndar
ds o
f car
e ex
ist o
r if t
hey
exis
t but
are
out
date
d or
con
tradi
ctor
y, th
en b
yex
pert
opin
ion;
and
(4) C
ost-e
ffect
ive
for t
he m
edic
al c
ondi
tion
bein
g tre
ated
com
pare
d to
alte
rnat
ive
heal
th in
terv
entio
ns, i
nclu
ding
no
inte
r-ve
ntio
n. F
or th
e pu
rpos
es o
f thi
s pa
ragr
aph,
cos
t-effe
ctiv
e sh
all n
ot n
eces
saril
y m
ean
low
est p
rice.
Stat
eSt
atut
e/Re
gula
tion
Med
ical
Nec
essi
ty D
efin
ition
1
Illin
ois
215
ILCS
105
/2(2
001)
“Med
ical
ly n
eces
sary
” m
eans
that
a s
ervi
ce, d
rug,
or s
uppl
y is
nec
essa
ry a
nd a
ppro
pria
te fo
r the
dia
gnos
is o
r tre
atm
ent o
f an
illne
ss o
r inj
ury
in a
ccor
d w
ith g
ener
ally
acc
epte
d st
anda
rds
of m
edic
al p
ract
ice
at th
e tim
e th
e se
rvic
e, d
rug,
or s
uppl
y is
pro
vide
d. W
hen
spec
ifica
lly a
pplie
dto
a c
onfin
emen
t it f
urth
er m
eans
that
the
diag
nosi
s or
trea
tmen
t of t
he c
over
ed p
erso
n’s
med
ical
sym
ptom
s or
con
ditio
n ca
nnot
be
safe
lypr
ovid
ed to
that
per
son
as a
n ou
tpat
ient
. A s
ervi
ce, d
rug,
or s
uppl
y sh
all n
ot b
e m
edic
ally
nec
essa
ry if
it: (
i) is
inve
stig
atio
nal,
expe
rimen
tal,
orfo
r res
earc
h pu
rpos
es; o
r (ii)
is p
rovi
ded
sole
ly fo
r the
con
veni
ence
of t
he p
atie
nt, t
he p
atie
nt’s
fam
ily, p
hysi
cian
, hos
pita
l, or
any
oth
er p
rovi
der;
or (i
ii) e
xcee
ds in
sco
pe, d
urat
ion,
or i
nten
sity
that
leve
l of c
are
that
is n
eede
d to
pro
vide
saf
e, a
dequ
ate,
and
app
ropr
iate
dia
gnos
is o
r tre
at-
men
t; or
(iv)
cou
ld h
ave
been
om
itted
with
out a
dver
sely
affe
ctin
g th
e co
vere
d pe
rson
’s co
nditi
on o
r the
qua
lity
of m
edic
al c
are;
or (
v) in
volv
esth
e us
e of
a m
edic
al d
evic
e, d
rug,
or s
ubst
ance
not
form
ally
app
rove
d by
the
Unite
d St
ates
Foo
d an
d Dr
ug A
dmin
istra
tion.
Indi
ana
Non
eN
one
Idah
oN
one
Non
e
Tab
le 4
. Co
nti
nu
ed
Iow
aIo
wa
Code
514
J.5
Med
ical
nec
essi
ty is
def
ined
as
the
insu
rer’s
pla
n de
fines
it.
Kans
asN
one
Non
e
Kent
ucky
Non
eN
one
Loui
sian
aN
one
Non
e
Mai
ne24
-A M
.R.S
. §
4301
-A (1
1)(2
000)
Med
ical
Nec
essi
ty. “
Med
ical
nec
essi
ty”
mea
ns h
ealth
car
e se
rvic
es o
r pro
duct
s th
at a
pru
dent
phy
sici
an o
r oth
er h
ealth
car
e pr
actit
ione
rw
ould
pro
vide
to a
n en
rolle
e fo
r the
pur
pose
of p
reve
ntin
g, d
iagn
osin
g, o
r tre
atin
g an
illn
ess,
inju
ry, d
isea
se, o
r the
sym
ptom
s of
an
illne
ss,
inju
ry, o
r dis
ease
in a
man
ner t
hat i
s: (A
) In
acco
rdan
ce w
ith g
ener
ally
acc
epte
d st
anda
rds
of m
edic
al p
ract
ice;
(B) C
linic
ally
app
ropr
iate
inte
rms
of ty
pe, f
requ
ency
, ext
ent,
site
, and
dur
atio
n; a
nd (C
) Not
prim
arily
for t
he c
onve
nien
ce o
f the
enr
olle
e or
phy
sici
an o
r oth
er h
ealth
car
epr
actit
ione
r.
Mar
ylan
dCO
MAR
§ 10
.09.
62.0
1(2
001)
(Med
icai
dM
anag
ed C
are
Regu
latio
ns)
“Med
ical
nec
essi
ty”
mea
ns w
hat i
s m
edic
ally
nec
essa
ry a
nd a
ppro
pria
te.

Special Report58
Tab
le 4
. Co
nti
nu
ed
Mas
sach
uset
tsM
ass.
Ann
. Law
sch
. 176
O (1
) (20
01)
(IRO
Stat
ute)
“Med
ical
nec
essi
ty”
or “
med
ical
ly n
eces
sary
.” h
ealth
car
e se
rvic
es th
at a
re c
onsi
sten
t with
gen
eral
ly a
ccep
ted
prin
cipl
es o
f pro
fess
iona
lm
edic
al p
ract
ice.
Stat
eSt
atut
e/Re
gula
tion
Med
ical
Nec
essi
ty D
efin
ition
1
Min
neso
taM
inn.
Sta
t. §
62Q.
53(2
000)
(IRO
Sta
tute
)“M
edic
ally
nec
essa
ry c
are”
mea
ns h
ealth
car
e se
rvic
es a
ppro
pria
te, i
n te
rms
of ty
pe, f
requ
ency
, lev
el, s
ettin
g, a
nd d
urat
ion,
to th
e en
rolle
e’s
diag
nosi
s or
con
ditio
n, a
nd d
iagn
ostic
test
ing
and
prev
entiv
e se
rvic
es. M
edic
ally
nec
essa
ry c
are
mus
t be
cons
iste
nt w
ith g
ener
ally
acc
epte
dpr
actic
e pa
ram
eter
s as
det
erm
ined
by
heal
th c
are
prov
ider
s in
the
sam
e or
sim
ilar g
ener
al s
peci
alty
as
typi
cally
man
ages
the
cond
ition
, pro
ce-
dure
, or t
reat
men
t at i
ssue
and
mus
t: (1
) hel
p re
stor
e or
mai
ntai
n th
e en
rolle
e’s
heal
th; o
r (2)
pre
vent
det
erio
ratio
n of
the
enro
llee’
s co
nditi
on.
Mis
siss
ippi
Non
eN
one
Mic
higa
nN
one
Non
e
Mis
sour
iN
one
Non
e
Mon
tana
Non
eN
one
Neb
rask
aN
one
Non
e
Nev
ada
Non
eN
one
New
Ham
pshi
reN
one
Non
e
New
Jer
sey
Non
eN
one
New
Mex
ico
Non
eN
one
New
Yor
kPr
opos
edLe
gisl
atio
n
A.50
48a
(200
1)(In
Ass
embl
yCo
mm
ittee
on
Rule
s as
of
Janu
ary
9, 2
002)
PROP
OSED
DEF
INIT
ION
:“m
edic
ally
nec
essa
ry”
mea
ns, w
ith re
spec
t to
a he
alth
car
e se
rvic
e, th
at it
has
bee
n re
ason
ably
det
erm
ined
, and
coul
d be
sho
wn,
by
the
enro
llee’
s he
alth
car
e pr
ofes
sion
al in
con
sulta
tion
with
the
patie
nt, o
r cou
ld b
e re
ason
ably
det
erm
ined
and
sho
wn
by a
hea
lth c
are
prof
essi
onal
in c
onsu
ltatio
n w
ith th
e pa
tient
, to
be c
onsi
sten
t with
the
enro
llee’
s co
nditi
on, c
ircum
stan
ces
and
best
inte
r-es
ts in
rela
tion
to ty
pe, f
requ
ency
, site
and
dur
atio
n, a
nd w
ith p
rofe
ssio
nal h
ealth
car
e pr
actic
e, u
nles
s it
is re
ason
ably
sho
wn
by m
eans
of
subs
tant
ial m
edic
al a
nd s
cien
tific
lite
ratu
re, a
nd c
onsi
derin
g th
e en
rolle
e’s
cond
ition
, circ
umst
ance
s an
d be
st in
tere
sts,
that
eith
er (a
) tha
tth
e he
alth
car
e se
rvic
e w
ould
be
unsa
fe o
r ine
ffect
ive,
or (
b) th
at th
e he
alth
car
e pl
an’s
pref
erre
d he
alth
car
e se
rvic
e or
no
serv
ice
wou
ldle
ad to
an
equa
lly g
ood
outc
ome.
“M
edic
al n
eces
sity
” is
the
qual
ity o
f bei
ng m
edic
ally
nec
essa
ry. A
ll de
finiti
ons
in s
ectio
n fo
rty-n
ine
hund
red
of th
is c
hapt
er s
hall
appl
y to
this
sub
divi
sion
.

Medical Necessity in Private Health Plans 59
Nor
thCa
rolin
aG.
S. §
58-
3-20
0(b)
M
edic
al N
eces
sity
—An
insu
rer t
hat l
imits
its
heal
th b
enef
it pl
an c
over
age
to m
edic
ally
nec
essa
ry s
ervi
ces
and
supp
lies
shal
l def
ine
“med
ical
lyne
cess
ary
serv
ices
or s
uppl
ies”
in it
s he
alth
ben
efit
plan
as
thos
e co
vere
d se
rvic
es o
r sup
plie
s th
at a
re: (
1) P
rovi
ded
for t
he d
iagn
osis
, tre
at-
men
t, cu
re, o
r rel
ief o
f a c
ondi
tion,
illn
ess,
inju
ry, o
r dis
ease
; and
, exc
ept a
s al
low
ed u
nder
G.S
.58-
3-25
5, n
ot fo
r exp
erim
enta
l, in
vest
igat
iona
l,or
cos
met
ic p
urpo
ses.
(2) N
eces
sary
for a
nd a
ppro
pria
te to
the
diag
nosi
s, tr
eatm
ent,
cure
, or r
elie
f of a
hea
lth c
ondi
tion,
illn
ess,
inju
ry,
dise
ase,
or i
ts s
ympt
oms.
(3) W
ithin
gen
eral
ly a
ccep
ted
stan
dard
s of
med
ical
car
e in
the
com
mun
ity. (
4) N
ot s
olel
y fo
r the
con
veni
ence
ofth
ein
sure
d, th
e in
sure
d’s
fam
ily, o
r the
pro
vide
r. Fo
r med
ical
ly n
eces
sary
ser
vice
s, n
othi
ng in
this
sub
sect
ion
prec
lude
s an
insu
rer f
rom
com
parin
g th
e co
st-e
ffect
iven
ess
of a
ltern
ativ
e se
rvic
es o
r sup
plie
s w
hen
dete
rmin
ing
whi
ch o
f the
ser
vice
s or
sup
plie
s w
ill b
e co
vere
d.
Stat
eSt
atut
e/Re
gula
tion
Med
ical
Nec
essi
ty D
efin
ition
1
Ohio
Non
eN
one
Okla
hom
aO.
A.C.
§ 31
7:30
-5-4
6(2
000)
(S
tatu
te
rega
rdin
g in
patie
nt
psyc
hiat
ric
faci
litie
s)
(B) M
edic
al n
eces
sity
crit
eria
for a
cute
psy
chia
tric
adm
issi
ons.
Acu
te p
sych
iatri
c ad
mis
sion
s fo
r chi
ldre
n 13
or o
lder
mus
t mee
t the
term
s an
dco
nditi
ons
cont
aine
d in
(i),
(ii),
(iii)
and
two
of th
e (iv
)(I) t
o (v
)(III)
of t
his
subp
arag
raph
. Chi
ldre
n 12
or y
oung
er m
ust m
eet t
he te
rms
or c
ondi
tions
cont
aine
d in
(i),
(ii),
(iii)
and
one
of (i
v)(I)
to (i
v)(IV
), an
d on
e of
(v)(I
) to
(v)(I
II) o
f thi
s su
bpar
agra
ph.
(i) A
ny D
SM-IV
-R A
xis
1 pr
imar
y di
agno
sis
with
the
exce
ptio
n of
V-c
odes
, adj
ustm
ent d
isor
ders
, and
sub
stan
ce re
late
d di
sord
ers,
acc
ompa
nied
by a
det
aile
d de
scrip
tion
of th
e sy
mpt
oms
supp
ortin
g th
e di
agno
sis.
In li
eu o
f a q
ualif
ying
Axi
s I d
iagn
osis
, chi
ldre
n 18
-21
year
s of
age
may
have
an
Axis
II d
iagn
osis
of a
ny p
erso
nalit
y di
sord
er.
(ii) C
ondi
tions
are
dire
ctly
attr
ibut
able
to a
men
tal d
isor
der a
s th
e pr
imar
y ne
ed fo
r pro
fess
iona
l atte
ntio
n (th
is d
oes
not i
nclu
de p
lace
men
tis
sues
, crim
inal
beh
avio
r, st
atus
offe
nses
). Ad
just
men
t or s
ubst
ance
rela
ted
diso
rder
may
be
a se
cond
ary
Axis
I di
agno
sis.
(iii)
It ha
s be
en d
eter
min
ed b
y th
e Ga
teke
eper
that
the
curr
ent d
isab
ling
sym
ptom
s co
uld
not h
ave
been
man
aged
or h
ave
not b
een
man
age-
able
in a
less
er in
tens
ive
treat
men
t pro
gram
.
(iv) W
ithin
the
past
48
hour
s th
e be
havi
ors
pres
ent a
n im
min
ent l
ife th
reat
enin
g em
erge
ncy
such
as
evid
ence
d by
:
(I) S
peci
fical
ly d
escr
ibed
sui
cide
atte
mpt
s, s
uici
de in
tent
, or s
erio
us th
reat
by
the
patie
nt.
(II) S
peci
fical
ly d
escr
ibed
pat
tern
s of
esc
alat
ing
inci
dent
s of
sel
f-mut
ilatin
g be
havi
ors.
(III)
Spec
ifica
lly d
escr
ibed
epi
sode
s of
unp
rovo
ked
sign
ifica
nt p
hysi
cal a
ggre
ssio
n an
d pa
ttern
s of
esc
alat
ing
phys
ical
agg
ress
ion
in in
tens
ityan
d du
ratio
n.
(IV) S
peci
fical
ly d
escr
ibed
epi
sode
s of
inca
paci
tatin
g de
pres
sion
or p
sych
osis
that
resu
lt in
an
inab
ility
to fu
nctio
n or
car
e fo
r bas
ic n
eeds
.
(v) R
equi
res
secu
re 2
4-ho
ur n
ursi
ng/m
edic
al s
uper
visi
on a
s ev
iden
ced
by:
(I) S
tabi
lizat
ion
of a
cute
psy
chia
tric
sym
ptom
s.
(II) N
eeds
ext
ensi
ve tr
eatm
ent u
nder
phy
sici
an d
irect
ion.
(III)
Phys
iolo
gica
l evi
denc
e or
exp
ecta
tion
of w
ithdr
awal
sym
ptom
s w
hich
requ
ire 2
4-ho
ur m
edic
al s
uper
visi
on.
(C) M
edic
al n
eces
sity
crit
eria
for c
ontin
ued
stay
—ac
ute
psyc
hiat
ric a
dmis
sion
. Con
tinue
d st
ay—
acut
e ps
ychi
atric
adm
issi
ons
mus
t mee
t all
ofth
e co
nditi
ons
set f
orth
in (i
) to
(iv) o
f thi
s su
bpar
agra
ph.
Nor
th D
akot
aN
one
Non
e
Tab
le 4
. Co
nti
nu
ed
1De
finiti
ons
have
bee
n ta
ken
verb
atim
from
the
rele
vant
doc
umen
t; qu
otat
ion
mar
ks h
ave
been
om
itted
.
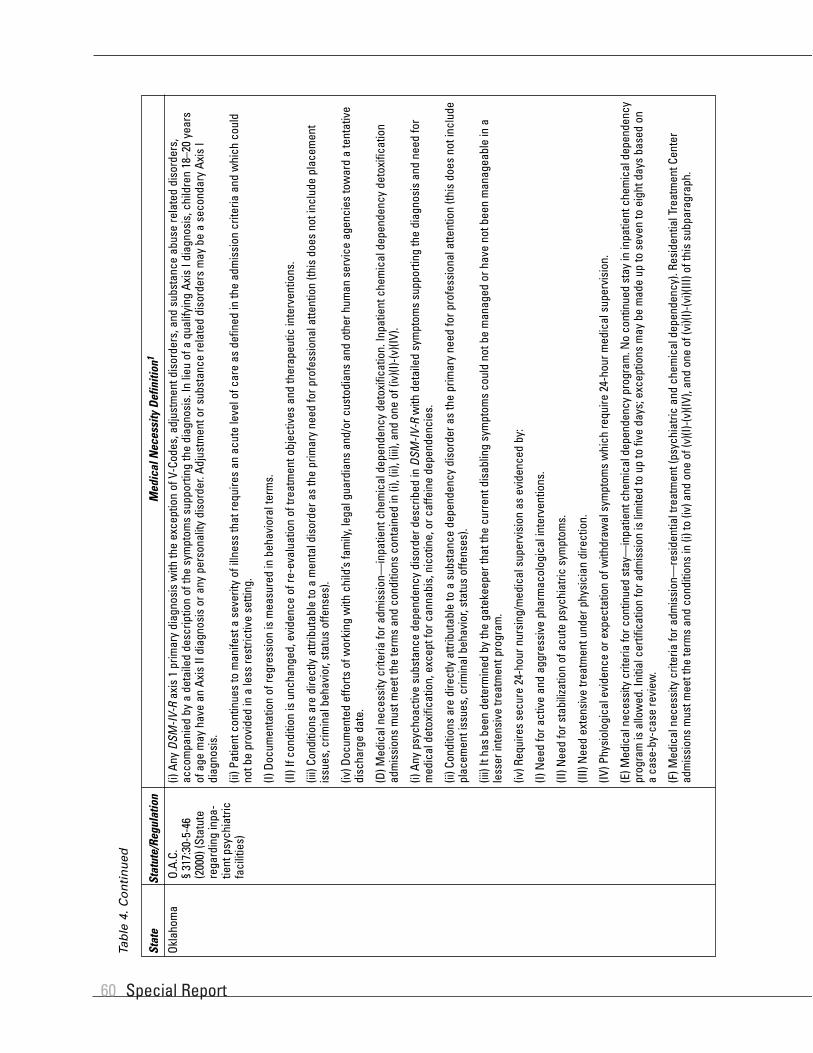
Special Report60
Tab
le 4
. Co
nti
nu
ed
Okla
hom
aO.
A.C.
§ 31
7:30
-5-4
6(2
000)
(Sta
tute
rega
rdin
g in
pa-
tient
psy
chia
tric
faci
litie
s)
(i) A
ny D
SM-IV
-Rax
is 1
prim
ary
diag
nosi
s w
ith th
e ex
cept
ion
of V
-Cod
es, a
djus
tmen
t dis
orde
rs, a
nd s
ubst
ance
abu
se re
late
d di
sord
ers,
acco
mpa
nied
by
a de
taile
d de
scrip
tion
of th
e sy
mpt
oms
supp
ortin
g th
e di
agno
sis.
In li
eu o
f a q
ualif
ying
Axi
s I d
iagn
osis
, chi
ldre
n 18
–20
year
sof
age
may
hav
e an
Axi
s II
diag
nosi
s or
any
per
sona
lity
diso
rder
. Adj
ustm
ent o
r sub
stan
ce re
late
d di
sord
ers
may
be
a se
cond
ary
Axis
Idi
agno
sis.
(ii) P
atie
nt c
ontin
ues
to m
anife
st a
sev
erity
of i
llnes
s th
at re
quire
s an
acu
te le
vel o
f car
e as
def
ined
in th
e ad
mis
sion
crit
eria
and
whi
ch c
ould
not b
e pr
ovid
ed in
a le
ss re
stric
tive
setti
ng.
(I) D
ocum
enta
tion
of re
gres
sion
is m
easu
red
in b
ehav
iora
l ter
ms.
(II) I
f con
ditio
n is
unc
hang
ed, e
vide
nce
of re
-eva
luat
ion
of tr
eatm
ent o
bjec
tives
and
ther
apeu
tic in
terv
entio
ns.
(iii)
Cond
ition
s ar
e di
rect
ly a
ttrib
utab
le to
a m
enta
l dis
orde
r as
the
prim
ary
need
for p
rofe
ssio
nal a
ttent
ion
(this
doe
s no
t inc
lude
pla
cem
ent
issu
es, c
rimin
al b
ehav
ior,
stat
us o
ffens
es).
(iv) D
ocum
ente
d ef
forts
of w
orki
ng w
ith c
hild
’s fa
mily
, leg
al g
uard
ians
and
/or c
usto
dian
s an
d ot
her h
uman
ser
vice
age
ncie
s to
war
d a
tent
ativ
edi
scha
rge
date
.
(D) M
edic
al n
eces
sity
crit
eria
for a
dmis
sion
—in
patie
nt c
hem
ical
dep
ende
ncy
deto
xific
atio
n. In
patie
nt c
hem
ical
dep
ende
ncy
deto
xific
atio
nad
mis
sion
s m
ust m
eet t
he te
rms
and
cond
ition
s co
ntai
ned
in (i
), (ii
), (ii
i), a
nd o
ne o
f (iv
)(I)-(
v)(IV
).
(i) A
ny p
sych
oact
ive
subs
tanc
e de
pend
ency
dis
orde
r des
crib
ed in
DSM
-IV-R
with
det
aile
d sy
mpt
oms
supp
ortin
g th
e di
agno
sis
and
need
for
med
ical
det
oxifi
catio
n, e
xcep
t for
can
nabi
s, n
icot
ine,
or c
affe
ine
depe
nden
cies
.
(ii) C
ondi
tions
are
dire
ctly
attr
ibut
able
to a
sub
stan
ce d
epen
denc
y di
sord
er a
s th
e pr
imar
y ne
ed fo
r pro
fess
iona
l atte
ntio
n (th
is d
oes
not i
nclu
depl
acem
ent i
ssue
s, c
rimin
al b
ehav
ior,
stat
us o
ffens
es).
(iii)
It ha
s be
en d
eter
min
ed b
y th
e ga
teke
eper
that
the
curr
ent d
isab
ling
sym
ptom
s co
uld
not b
e m
anag
ed o
r hav
e no
t bee
n m
anag
eabl
e in
ale
sser
inte
nsiv
e tre
atm
ent p
rogr
am.
(iv) R
equi
res
secu
re 2
4-ho
ur n
ursi
ng/m
edic
al s
uper
visi
on a
s ev
iden
ced
by:
(I) N
eed
for a
ctiv
e an
d ag
gres
sive
pha
rmac
olog
ical
inte
rven
tions
.
(II) N
eed
for s
tabi
lizat
ion
of a
cute
psy
chia
tric
sym
ptom
s.
(III)
Nee
d ex
tens
ive
treat
men
t und
er p
hysi
cian
dire
ctio
n.
(IV) P
hysi
olog
ical
evi
denc
e or
exp
ecta
tion
of w
ithdr
awal
sym
ptom
s w
hich
requ
ire 2
4-ho
ur m
edic
al s
uper
visi
on.
(E)M
edic
al n
eces
sity
crit
eria
for c
ontin
ued
stay
—in
patie
nt c
hem
ical
dep
ende
ncy
prog
ram
. No
cont
inue
d st
ay in
inpa
tient
che
mic
al d
epen
denc
ypr
ogra
m is
allo
wed
. Ini
tial c
ertif
icat
ion
for a
dmis
sion
is li
mite
d to
up
to fi
ve d
ays;
exc
eptio
ns m
ay b
e m
ade
up to
sev
en to
eig
ht d
ays
base
d on
aca
se-b
y-ca
se re
view
.
(F) M
edic
al n
eces
sity
crit
eria
for a
dmis
sion
—re
side
ntia
l tre
atm
ent (
psyc
hiat
ric a
nd c
hem
ical
dep
ende
ncy)
. Res
iden
tial T
reat
men
t Cen
ter
adm
issi
ons
mus
t mee
t the
term
s an
d co
nditi
ons
in (i
) to
(iv) a
nd o
ne o
f (v)
(I)-(v
)(IV)
, and
one
of (
vi)(I
)-(vi
)(III)
of t
his
subp
arag
raph
.
Stat
eSt
atut
e/Re
gula
tion
Med
ical
Nec
essi
ty D
efin
ition
1

Medical Necessity in Private Health Plans 61
Okla
hom
aO.
A.C.
§ 31
7:30
-5-4
6(2
000)
(Sta
tute
rega
rdin
g in
pa-
tient
psy
chia
tric
faci
litie
s)
(i) A
ny D
SM-IV
-RAx
is 1
prim
ary
diag
nosi
s w
ith th
e ex
cept
ion
of V
-cod
es, a
djus
tmen
t dis
orde
rs, a
nd s
ubst
ance
rela
ted
diso
rder
s, a
ccom
pani
edby
det
aile
d sy
mpt
oms
supp
ortin
g th
e di
agno
sis.
In li
eu o
f a q
ualif
ying
Axi
s I d
iagn
osis
, chi
ldre
n 18
–20
year
s of
age
may
hav
e an
Axi
s II
diag
nosi
sor
any
per
sona
lity
diso
rder
. Adj
ustm
ent o
r sub
stan
ce re
late
d di
sord
ers
may
be
a se
cond
ary
Axis
I di
agno
sis.
(ii) C
ondi
tions
are
dire
ctly
attr
ibut
ed to
a m
enta
l dis
orde
r as
the
prim
ary
reas
on fo
r pro
fess
iona
l atte
ntio
n (th
is d
oes
not i
nclu
de p
lace
men
tis
sues
, crim
inal
beh
avio
r, st
atus
offe
nses
).
(iii)
Patie
nt h
as e
ither
rece
ived
trea
tmen
t in
an a
cute
car
e se
tting
or i
t has
bee
n de
term
ined
by
the
gate
keep
er th
at th
e cu
rren
t dis
ablin
gsy
mpt
oms
coul
d no
t or h
ave
not b
een
man
agea
ble
in a
less
inte
nsiv
e tre
atm
ent p
rogr
am.
(iv) C
hild
mus
t be
med
ical
ly s
tabl
e.
(v) P
atie
nt d
emon
stra
tes
esca
latin
g pa
ttern
of s
elf i
njur
ious
or a
ssau
ltive
beh
avio
rs a
s ev
iden
ced
by:
(I) S
uici
dal i
deat
ion
and/
or th
reat
.
(II) H
isto
ry o
f or c
urre
nt s
elf-i
njur
ious
beh
avio
r.
(III)
Serio
us th
reat
s or
evi
denc
e of
phy
sica
l agg
ress
ion.
(IV) C
urre
nt in
capa
cita
ting
psyc
hosi
s or
dep
ress
ion.
(vi)
Requ
ires
24-h
our o
bser
vatio
n an
d tre
atm
ent a
s ev
iden
ced
by:
(I) In
tens
ive
beha
vior
al m
anag
emen
t.
(II) I
nten
sive
trea
tmen
t with
the
fam
ily/g
uard
ian
and
child
in a
stru
ctur
ed m
ilieu
.
(III)
Inte
nsiv
e tre
atm
ent i
n pr
epar
atio
n fo
r re-
entry
into
com
mun
ity.
(G) M
edic
al n
eces
sity
crit
eria
for c
ontin
ued
stay
—re
side
ntia
l tre
atm
ent c
ente
r. Co
ntin
ued
stay
resi
dent
ial t
reat
men
t cen
ter a
dmis
sion
s m
ust
mee
t the
term
s an
d co
nditi
ons
cont
aine
d in
(i);
(ii);
and
eith
er (i
ii) o
r (iv
); an
d (v
); an
d (v
i) of
this
sub
para
grap
h.
(i) A
ny D
SM-IV
-RAx
is 1
prim
ary
diag
nosi
s w
ith th
e ex
cept
ion
of V
cod
es, a
djus
tmen
t dis
orde
rs, a
nd s
ubst
ance
abu
se re
late
d di
sord
ers,
acco
mpa
nied
by
deta
iled
sym
ptom
s su
ppor
ting
the
diag
nosi
s. In
lieu
of a
qua
lifyi
ng A
xis
I dia
gnos
is, c
hild
ren
18–2
0 ye
ars
of a
ge m
ay h
ave
anAx
is II
dia
gnos
is o
f any
per
sona
lity
diso
rder
.
(ii) C
ondi
tions
are
dire
ctly
attr
ibut
ed to
a m
enta
l dis
orde
r as
the
prim
ary
reas
on fo
r con
tinue
d st
ay (t
his
does
not
incl
ude
plac
emen
t iss
ues,
crim
inal
beh
avio
r, st
atus
offe
nses
).
(iii)
Patie
nt is
mak
ing
mea
sura
ble
prog
ress
tow
ard
the
treat
men
t obj
ectiv
es s
peci
fied
in th
e tre
atm
ent p
lan.
(I) P
rogr
ess
is m
easu
red
in b
ehav
iora
l ter
ms
and
refle
cted
in th
e pa
tient
’s tre
atm
ent a
nd d
isch
arge
pla
ns.
(II) P
atie
nt h
as m
ade
gain
s to
war
d so
cial
resp
onsi
bilit
y an
d in
depe
nden
ce.
(III)
Ther
e is
act
ive,
ong
oing
psy
chia
tric
treat
men
t and
doc
umen
ted
prog
ress
tow
ard
the
treat
men
t obj
ectiv
e an
d di
scha
rge.
(IV) T
here
are
doc
umen
ted
effo
rts a
nd e
vide
nce
of a
ctiv
e in
volv
emen
t with
the
fam
ily, g
uard
ian,
chi
ld w
elfa
re w
orke
r, ex
tend
ed fa
mily
, etc
.
Stat
eSt
atut
e/Re
gula
tion
Med
ical
Nec
essi
ty D
efin
ition
1
Tab
le 4
. Co
nti
nu
ed
1De
finiti
ons
have
bee
n ta
ken
verb
atim
from
the
rele
vant
doc
umen
t; qu
otat
ion
mar
ks h
ave
been
om
itted
.

Special Report62
Tab
le 4
. Co
nti
nu
ed
Okla
hom
aO.
A.C.
§ 31
7:30
-5-4
6(2
000)
(Sta
tute
rega
rdin
g in
pa-
tient
psy
chia
tric
faci
litie
s)
(iv) C
hild
’s co
nditi
on h
as re
mai
ned
unch
ange
d or
wor
sene
d.
(I) D
ocum
enta
tion
of re
gres
sion
is m
easu
red
in b
ehav
iora
l ter
ms.
(II) I
f con
ditio
n is
unc
hang
ed, t
here
is e
vide
nce
of re
-eva
luat
ion
of th
e tre
atm
ent o
bjec
tives
and
ther
apeu
tic in
terv
entio
ns.
(v) T
here
is d
ocum
ente
d co
ntin
uing
nee
d fo
r 24-
hour
obs
erva
tion
and
treat
men
t as
evid
ence
d by
:
(I) In
tens
ive
beha
vior
al m
anag
emen
t.
(II) I
nten
sive
trea
tmen
t with
the
fam
ily/g
uard
ian
and
child
in a
stru
ctur
ed m
ilieu
.
(III)
Inte
nsiv
e tre
atm
ent i
n pr
epar
atio
n fo
r re-
entry
into
com
mun
ity.
(vi)
Docu
men
ted
effo
rts o
f wor
king
with
chi
ld’s
fam
ily, l
egal
gua
rdia
n an
d/or
cus
todi
an a
nd o
ther
hum
an s
ervi
ce a
genc
ies
tow
ard
a te
ntat
ive
disc
harg
e da
te.
(A) P
re-a
utho
rizat
ion
and
exte
nsio
n pr
oced
ures
. Pre
-adm
issi
on a
utho
rizat
ion
for i
npat
ient
psy
chia
tric
serv
ices
mus
t be
requ
este
d fro
mth
eOH
CA d
esig
nate
d ag
ent.
The
OHCA
or d
esig
nate
d ag
ent w
ill e
valu
ate
and
rend
er a
dec
isio
n w
ithin
24
hour
s of
rece
ivin
g th
e re
ques
t.A
Certi
ficat
e of
Nee
d w
ill b
e is
sued
by
the
OHCA
or i
ts d
esig
nate
d ag
ent,
if th
e re
cipi
ent m
eets
med
ical
nec
essi
ty c
riter
ia.
(B) E
xten
sion
requ
ests
(psy
chia
tric)
mus
t be
mad
e th
roug
h th
e OH
CA d
esig
nate
d ag
ent.
All r
eque
sts
shal
l be
mad
e pr
ior t
o th
e ex
pira
tion
ofth
eap
prov
ed e
xten
sion
follo
win
g th
e gu
idel
ines
in th
e Ga
teke
epin
g M
anua
l. Ex
tens
ion
requ
ests
for t
he c
ontin
ued
stay
of a
chi
ld w
ho h
asbe
enin
an
acut
e ps
ychi
atric
pro
gram
for a
per
iod
of th
irty
(30)
day
s w
ill re
quire
a fa
ce to
face
eva
luat
ion
by th
e ga
teke
eper
. Req
uest
s fo
rth
eco
ntin
ued
stay
of a
chi
ld w
ho h
as b
een
in a
n ac
ute
psyc
hiat
ric p
rogr
am fo
r a p
erio
d of
six
ty (6
0) d
ays
will
requ
ire a
revi
ew o
f all
treat
men
tdo
cum
enta
tion
com
plet
ed b
y th
e OH
CA d
esig
nate
d ag
ent.
(C) I
f a d
enia
l dec
isio
n is
mad
e, a
reco
nsid
erat
ion
requ
est m
ay b
e m
ade
dire
ctly
to th
e OH
CA d
esig
nate
d ag
ent w
ithin
ten
(10)
wor
king
days
ofno
tific
atio
n of
the
deni
al. T
he a
gent
will
retu
rn a
dec
isio
n w
ithin
ten
(10)
wor
king
day
s fro
m th
e tim
e of
rece
ivin
g th
e re
cons
ider
atio
nre
ques
t.If
the
deni
al d
ecis
ion
is u
phel
d, th
e de
nial
can
be
appe
aled
to th
e Ok
laho
ma
Heal
th C
are
Auth
ority
with
in 2
0 w
orki
ng d
ays
ofno
tific
atio
n of
the
deni
al b
y th
e OH
CA d
esig
nate
d ag
ent.
Stat
eSt
atut
e/Re
gula
tion
Med
ical
Nec
essi
ty D
efin
ition
1
Oreg
onN
one
Non
e
Penn
sylv
ania
Non
eN
one
Rhod
e Is
land
Non
eN
one
Sout
hCa
rolin
aN
one
Non
e

Medical Necessity in Private Health Plans 63
Sout
h Da
kota
S.D.
Cod
ified
Law
s 28
-13-
27.1
(200
1)
Med
ical
ly n
eces
sary
hos
pita
l ser
vice
s ar
e se
rvic
es p
rovi
ded
in a
hos
pita
l whi
ch m
eet t
he fo
llow
ing
crite
ria: (
1) A
re c
onsi
sten
t with
the
pers
on’s
sym
ptom
s, d
iagn
osis
, con
ditio
n, o
r inj
ury;
(2) A
re re
cogn
ized
as th
e pr
evai
ling
stan
dard
and
are
con
sist
ent w
ith g
ener
ally
acc
epte
dpr
ofes
sion
al m
edic
al s
tand
ards
of t
he p
rovi
der’s
pee
r gro
up; (
3) A
re p
rovi
ded
in re
spon
se to
a li
fe-th
reat
enin
g co
nditi
on; t
o tre
at p
ain,
inju
ry,
illne
ss, o
r inf
ectio
n; to
trea
t a c
ondi
tion
whi
ch w
ould
resu
lt in
phy
sica
l or m
enta
l dis
abili
ty; o
r to
achi
eve
a le
vel o
f phy
sica
l or m
enta
l fun
ctio
nco
nsis
tent
with
pre
vaili
ng s
tand
ards
for t
he d
iagn
osis
or c
ondi
tion;
(4) A
re n
ot fu
rnis
hed
prim
arily
for t
he c
onve
nien
ce o
f the
per
son
or th
epr
ovid
er; a
nd (5
) The
re is
no
othe
r equ
ally
effe
ctiv
e co
urse
of t
reat
men
t ava
ilabl
e or
sui
tabl
e fo
r the
per
son
need
ing
the
serv
ices
whi
ch is
mor
eco
nser
vativ
e or
sub
stan
tially
less
cos
tly. A
cou
rt sh
all r
ely
on th
e at
tend
ing
phys
icia
n’s
dete
rmin
atio
n as
to m
edic
al n
eces
sity
of h
ospi
tal
serv
ices
unl
ess
evid
ence
exi
sts
to th
e co
ntra
ry.
Stat
eSt
atut
e/Re
gula
tion
Med
ical
Nec
essi
ty D
efin
ition
1
Texa
sN
one
Non
e
Utah
Non
eN
one
Tenn
esse
eN
one
Non
e
Tab
le 4
. Co
nti
nu
ed
Verm
ont
Non
eN
one
Virg
inia
Va. C
ode
Ann.
§38
.2-5
800
(200
1)(IR
O St
atut
e)
“Med
ical
nec
essi
ty”
or “
med
ical
ly n
eces
sary
” m
eans
app
ropr
iate
and
nec
essa
ry h
ealth
car
e se
rvic
es w
hich
are
rend
ered
for a
ny c
ondi
tion
whi
ch, a
ccor
ding
to g
ener
ally
acc
epte
d pr
inci
ples
of g
ood
med
ical
pra
ctic
e, re
quire
s th
e di
agno
sis
or d
irect
car
e an
d tre
atm
ent o
f an
illne
ss,
inju
ry, o
r pre
gnan
cy-r
elat
ed c
ondi
tion,
and
are
not
pro
vide
d on
ly a
s a
conv
enie
nce.
Was
hing
ton
Rev.
Cod
e W
ash.
§ 71
.34.
020
(200
1)(m
enta
l hea
lthse
rvic
es fo
rm
inor
s)
Med
ical
nec
essi
ty fo
r inp
atie
nt c
are
mea
ns a
requ
este
d se
rvic
e w
hich
is re
ason
ably
cal
cula
ted
to: (
a) D
iagn
ose,
cor
rect
, cur
e or
alle
viat
e a
men
tal d
isor
der;
or (b
) pre
vent
the
wor
seni
ng o
f men
tal c
ondi
tions
that
end
ange
r life
or c
ause
suf
ferin
g an
d pa
in, o
r res
ult i
n ill
ness
or i
nfirm
ityor
thre
aten
to c
ause
or a
ggra
vate
a h
andi
cap,
or c
ause
phy
sica
l def
orm
ity o
r mal
func
tion,
and
ther
e is
no
adeq
uate
less
rest
rictiv
e al
tern
ativ
eav
aila
ble.
Wes
t Virg
inia
Non
eN
one
Wis
cons
inN
one
Non
e
Wyo
min
gN
one
Non
e
1De
finiti
ons
have
bee
n ta
ken
verb
atim
from
the
rele
vant
doc
umen
t; qu
otat
ion
mar
ks h
ave
been
om
itted
.

Special Report64
Alab
ama
Tab
le 5
. Sta
te In
dep
end
ent
Rev
iew
Sta
tute
s an
d R
egu
lati
on
s
Alas
ka√
Alas
ka S
tat.
§ 21
.07.
050
(200
1)Ar
izona
√Ar
izona
Rev
. Sta
t. §
20-2
537
(200
1)Ar
kans
asCa
lifor
nia
√√
Cal.
Ins.
Cod
e §
1016
9 (2
001)
Pro
pose
d Re
gula
tion
at C
al. R
eg. L
aw B
ulle
tin 2
001-
39 C
RLB
500
(Sep
t. 28
, 200
1)Co
lora
do√
√Co
lo. R
ev. S
tat.
§ 10
-16-
113.
5 Co
lo. I
ns. R
eg. 4
-2-2
1 (2
000)
Conn
ectic
ut√
√Co
nn. G
en. S
tat.
§ 38
a-47
8n (2
001)
Conn
. Age
ncie
s Re
gs. §
§ 38
a-47
8n-1
to 5
(200
1)De
law
are
√De
l Cod
e tit
. 16
§ 91
19 (2
001)
Dist
rict o
fCo
lum
bia
√D.
C. C
ode
§ 44
-301
.07
(200
1)
Flor
ida
√Fl
. Sta
t. §§
408
.705
6 (2
001)
Geor
gia
√Ga
. Cod
e §
33-2
0A-3
2 (2
001)
Haw
aii
√Hi
. Rev
. Sta
t. §
432E
-6 (2
001)
Idah
oIll
inoi
s√
215
Ill. C
omp.
Sta
t. 12
5, §
4-1
0 (2
001)
Indi
ana
√In
d. C
ode
§ 27
-13-
10.1
-1 (2
001)
Iow
a√
Iow
a Co
de §
§ 51
4J.1
to .1
4 (2
001)
Kans
as√
Kan.
Sta
t. §§
40-
22a1
3-16
(200
0)Ke
ntuc
ky√
Ky. S
tat.
§ 30
4.17
A-62
3 (2
001)
Loui
sian
a√
La. R
ev. S
tat.
§ 22
:308
1 (2
001)
Mai
ne√
Me.
Rev
. Sta
t. tit
. 24-
A §
4323
(200
1)M
aryl
and
√√
Md.
Ins.
Cod
e §
15-1
0A-0
3 (2
001)
Mas
sach
uset
ts√
√M
ass.
Gen
. Law
s ch
. 176
0, §
14
(200
1) 1
05 C
.M.R
. 128
.00
(200
1)
Mic
higa
n√
Mic
h. C
omp.
Law
s §§
550
.190
1-19
29 (2
001)
Min
neso
ta√
Min
n. S
tat.
§ 62
Q.73
(200
0)
Mis
siss
ippi
Mis
sour
i√
√M
o. R
ev. S
tat.
§ 37
6.13
85 (2
000)
20
C.S.
R. 1
00-5
.020
(200
1)
Mon
tana
√√
Mon
t. Co
de §
33-
37-1
02 (2
001)
Mon
t. Ad
min
. R. §
37.
108.
315
(200
1)
IRO
Stat
ute
IRO
Regu
latio
ns
Juris
dict
ion
(√if
yes)
(√if
yes)
Cita
tions

Medical Necessity in Private Health Plans 65
Tab
le 5
. Co
nti
nu
ed
IRO
Stat
ute
IRO
Regu
latio
ns
Juris
dict
ion
(√if
yes)
(√if
yes)
Cita
tions
Neb
rask
aN
evad
aN
ewHa
mps
hire
√N
.H. R
ev. S
tat.
420-
J:5
(200
0)
New
Jer
sey
√√
N.J
. Sta
t. §§
26:
2S-1
1 to
26:
2S-1
2 (2
001)
N.J
. Adm
. Cod
e §
8:38
A-3.
6
New
Mex
ico
√√
N.M
. Sta
t. An
n. §
59-
A-57
-1 (2
001)
N.M
. Adm
. Cod
e tit
. 13,
§ 1
0.17
.24
(200
1)
New
Yor
k√
√N
.Y. I
ns. L
aw §
491
0 (2
001)
11
N.Y
.C.R
.R. §
410
.1 (2
001)
Nor
th C
arol
ina
√20
01 N
.C. S
ess.
Law
s 44
6 (S
.B. 1
99) (
2001
)
Nor
th D
akot
a
Ohio
√Oh
io R
ev. C
ode
§ 17
51.8
4 (2
001)
Okla
hom
a√
Okla
. Sta
t. tit
. 63,
§ 2
528.
3 (2
001)
Oreg
on√
Or. L
egis
. ch.
266
(effe
ctiv
e da
te J
uly
1, 2
002)
Penn
sylv
ania
√√
40 P
a. S
tat.
§ 99
1.21
62 (2
001)
28
Pa. C
ode
§ 9.
501
(200
1)Rh
ode
Isla
nd√
√R.
I. Ge
n. L
aws
§ 23
-17.
12-1
0 (2
001)
R23
-17.
12-I-
UR (2
001)
Sout
hCa
rolin
a√
S.C.
Cod
e §§
38-
71-1
910-
2060
Sout
h Da
kota
Tenn
esse
e√
Tenn
. Cod
e §
56-3
2-22
7 (2
001)
Texa
s√
√Te
x. In
s. C
ode
art.
21.5
8A 2
8 Te
x. A
dm. C
ode
12.5
(200
1)Ut
ah√
√Ut
ah C
ode
§ 31
A-22
-629
(200
1) P
ropo
sed
Regu
latio
n at
200
1-23
Uta
h Bu
ll. 1
26 (D
ec. 1
, 200
1)Ve
rmon
t√
√Fo
r Phy
sica
l Hea
lth S
ervi
ces:
Fo
r Men
tal H
ealth
Ser
vice
s:
VT. S
tat.
tit. 8
, § 4
089f
(200
1)VT
. Sta
t. Ti
t. 8,
§ 4
089a
(200
1)Re
gula
tion
H-99
-1 (2
001)
Re
gula
tion
95-2
(200
1)
Virg
inia
√√
Va. C
ode
§§ 3
8.2-
5900
– 5
905
(200
1) 1
4 VA
C 5-
215-
10 (2
001)
Was
hing
ton
√√
Was
h. R
ev. C
ode
§ 48
.43.
535
(200
1) W
AC §
246
-305
-050
(200
1)W
est V
irgin
ia√
W.V
a. C
ode
§ 33
-25C
-6 (e
ffect
ive
July
1, 2
002)
Wis
cons
in
Wyo
min
g

Special Report66
Tab
le 6
. Med
ical
Nec
essi
ty D
efin
itio
ns:
Sta
te In
sura
nce
Law
s an
d IR
O S
tatu
tes
Med
ical
Nec
essi
ty
Defin
ition
inM
edic
al N
eces
sity
Insu
ranc
e Co
nten
t IR
O St
atut
eDe
finiti
on in
IRO
Stat
eSt
atut
es (Y
/N)
(Y/N
)St
atut
eIR
O St
atut
e De
finiti
on
Alab
ama
NN
Alas
kaN
YN
Arizo
naN
YN
Arka
nsas
YN
Calif
orni
aY
YN
Colo
rado
NY
N
Conn
ectic
utN
YN
For t
he p
urpo
se o
f thi
s ac
t, “m
edic
al n
eces
sity
” m
eans
the
prov
idin
g of
cov
ered
heal
th s
ervi
ces
or p
rodu
cts
that
a p
rude
nt p
hysi
cian
wou
ld p
rovi
de to
a p
atie
nt fo
rth
e pu
rpos
e of
dia
gnos
ing
or tr
eatin
g an
illn
ess,
inju
ry, o
r dis
ease
or i
ts s
ympt
oms,
ina
man
ner t
hat i
s: (1
) In
acco
rdan
ce w
ith th
e ge
nera
lly a
ccep
ted
stan
dard
s of
med
ical
pra
ctic
e; (2
) Con
sist
ent w
ith th
e sy
mpt
oms
or tr
eatm
ent o
f the
con
ditio
n;an
d(3
) Not
sol
ely
for a
nyon
e’s
conv
enie
nce.
16
Del.
Code
§ 9
119
(200
0)
Dela
war
eN
YY
Dist
rict o
fCo
lum
bia
NY
N
Flor
ida
YY
N
Geor
gia
NY
Y(5
) “M
edic
al n
eces
sity
,” “
med
ical
ly n
eces
sary
car
e,”
or “
med
ical
ly n
eces
sary
and
appr
opria
te”
mea
ns c
are
base
d up
on g
ener
ally
acc
epte
d m
edic
al p
ract
ices
in li
ght
of c
ondi
tions
at t
he ti
me
of tr
eatm
ent w
hich
is: (
A) A
ppro
pria
te a
nd c
onsi
sten
t with
the
diag
nosi
s an
d th
e om
issi
on o
f whi
ch c
ould
adv
erse
ly a
ffect
or f
ail t
o im
prov
eth
eel
igib
le e
nrol
lee’
s co
nditi
on; (
B) C
ompa
tible
with
the
stan
dard
s of
acc
epta
ble
med
ical
pra
ctic
e in
the
Unite
d St
ates
; (C)
Pro
vide
d in
a s
afe
and
appr
opria
te s
ettin
ggi
ven
the
natu
re o
f the
dia
gnos
is a
nd th
e se
verit
y of
the
sym
ptom
s; (D
) Not
pro
vide
dso
lely
for t
he c
onve
nien
ce o
f the
elig
ible
enr
olle
e or
the
conv
enie
nce
of th
e he
alth
care
pro
vide
r or h
ospi
tal;
and
(E) N
ot p
rimar
ily c
usto
dial
car
e, u
nles
s cu
stod
ial c
are
is a
cov
ered
ben
efit
unde
r the
elig
ible
enr
olle
e’s
evid
ence
of c
over
age.
O.
C.G.
A. §
33-
20A-
31 (2
000)

Medical Necessity in Private Health Plans 67
Tab
le 6
. Co
nti
nu
ed
Med
ical
Nec
essi
ty
Defin
ition
inM
edic
al N
eces
sity
Insu
ranc
e Co
nten
t IR
O St
atut
eDe
finiti
on in
IRO
Stat
eSt
atut
es (Y
/N)
(Y/N
)St
atut
eIR
O St
atut
e De
finiti
onHa
wai
iN
YM
edic
al n
eces
sity
(b) A
hea
lth in
terv
entio
n is
med
ical
ly n
eces
sary
if it
is re
com
-m
ende
d by
the
treat
ing
phys
icia
n or
trea
ting
licen
sed
heal
th c
are
prov
ider
, is
appr
oved
by
the
heal
th p
lan’
s m
edic
al d
irect
or o
r phy
sici
an d
esig
nee,
and
is: (
1) F
orth
e pu
rpos
e of
trea
ting
a m
edic
al c
ondi
tion;
(2) T
he m
ost a
ppro
pria
te d
eliv
ery
or le
vel
of s
ervi
ce, c
onsi
derin
g po
tent
ial b
enef
its a
nd h
arm
s to
the
patie
nt; (
3) K
now
n to
be
effe
ctiv
e in
impr
ovin
g he
alth
out
com
es; p
rovi
ded
that
: (A)
Effe
ctiv
enes
s is
det
erm
ined
first
by
scie
ntifi
c ev
iden
ce; (
B) If
no
scie
ntifi
c ev
iden
ce e
xist
s, th
en b
y pr
ofes
sion
alst
anda
rds
of c
are;
and
(C) I
f no
prof
essi
onal
sta
ndar
ds o
f car
e ex
ist o
r if t
hey
exis
tbu
t are
out
date
d or
con
tradi
ctor
y, th
en b
y ex
pert
opin
ion;
and
(4) C
ost-e
ffect
ive
for
the
med
ical
con
ditio
n be
ing
treat
ed c
ompa
red
to a
ltern
ativ
e he
alth
inte
rven
tions
,in
clud
ing
no in
terv
entio
n. F
or th
e pu
rpos
es o
f thi
s pa
ragr
aph,
cos
t-effe
ctiv
e sh
all n
otne
cess
arily
mea
n lo
wes
t pric
e. H
RS §
432
E-1.
4 (2
000)
Y
Idah
oN
N
Illin
ois
YY
N
Indi
ana
YY
N
Med
ical
nec
essi
ty is
def
ined
as
the
insu
rer’s
pla
n de
fines
it. I
owa
Code
514
J.5
Iow
aN
YY
Kans
asN
YN
Kent
ucky
NY
N
Loui
sian
aN
YN
“Med
ical
ly n
eces
sary
hea
lth c
are”
mea
ns h
ealth
car
e se
rvic
es o
r pro
duct
s pr
ovid
edto
an
enro
llee
for t
he p
urpo
se o
f pre
vent
ing,
dia
gnos
ing
or tr
eatin
g an
illn
ess,
inju
ryor
dis
ease
or t
he s
ympt
oms
of a
n ill
ness
, inj
ury
or d
isea
se in
a m
anne
r tha
t is
(A)c
onsi
sten
t with
gen
eral
ly a
ccep
ted
stan
dard
s of
med
ical
pra
ctic
e; (B
) clin
ical
lyap
prop
riate
in te
rms
of ty
pe, f
requ
ency
, ext
ent,
site
and
dur
atio
n; (C
) dem
onst
rate
dth
roug
h sc
ient
ific
evid
ence
to b
e ef
fect
ive
in im
prov
ing
heal
th o
utco
mes
; (D)
repr
e-se
ntat
ive
of “
best
pra
ctic
es”
in th
e m
edic
al p
rofe
ssio
n; a
nd (E
) not
prim
arily
for t
heco
nven
ienc
e of
the
enro
llee
or p
hysi
cian
or o
ther
hea
lth c
are
prac
titio
ner.
24-A
MRS
A §
4301
-A(1
0-A)
.
Mai
neN
YY
Mar
ylan
dY
YN
Mas
sach
uset
tsN
YY
“Med
ical
nec
essi
ty”
or “
med
ical
ly n
eces
sary
,” h
ealth
car
e se
rvic
es th
at a
re c
onsi
s-te
nt w
ith g
ener
ally
acc
epte
d pr
inci
ples
of p
rofe
ssio
nal m
edic
al p
ract
ice.
Mas
s. A
nn.
Law
s ch
. 176
O (1
) (20
01)
Mic
higa
nN
YN
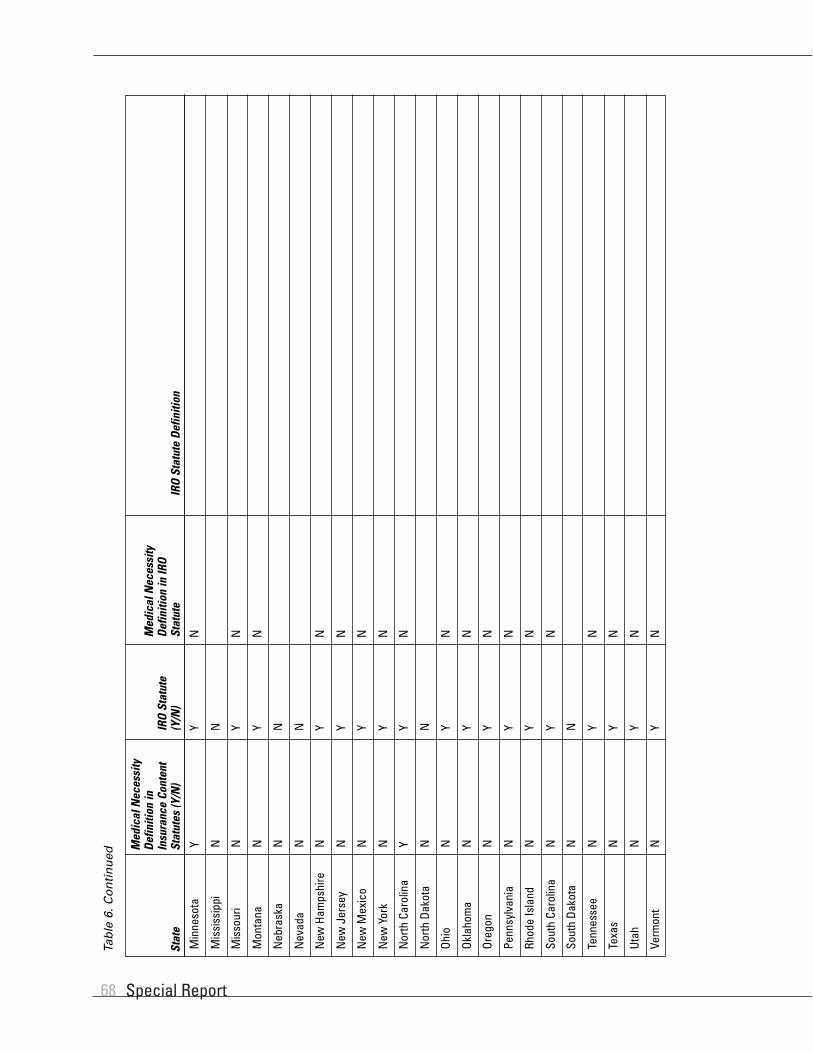
Special Report68
Tab
le 6
. Co
nti
nu
ed
Med
ical
Nec
essi
ty
Defin
ition
inM
edic
al N
eces
sity
Insu
ranc
e Co
nten
t IR
O St
atut
eDe
finiti
on in
IRO
Stat
eSt
atut
es (Y
/N)
(Y/N
)St
atut
eIR
O St
atut
e De
finiti
on
Min
neso
taY
YN
Mis
siss
ippi
NN
Mis
sour
iN
YN
Mon
tana
NY
N
Neb
rask
aN
N
Nev
ada
NN
New
Ham
pshi
reN
YN
New
Jer
sey
NY
N
New
Mex
ico
NY
N
New
Yor
kN
YN
Nor
th C
arol
ina
YY
N
Nor
th D
akot
aN
N
Ohio
NY
N
Okla
hom
aN
YN
Oreg
onN
YN
Penn
sylv
ania
NY
N
Rhod
e Is
land
NY
N
Sout
h Ca
rolin
aN
YN
Sout
h Da
kota
NN
Tenn
esse
eN
YN
Texa
sN
YN
Utah
NY
N
Verm
ont
NY
N

Medical Necessity in Private Health Plans 69
Tab
le 6
. Co
nti
nu
ed
Med
ical
Nec
essi
ty
Defin
ition
inM
edic
al N
eces
sity
Insu
ranc
e Co
nten
t IR
O St
atut
eDe
finiti
on in
IRO
Stat
eSt
atut
es (Y
/N)
(Y/N
)St
atut
eIR
O St
atut
e De
finiti
on
Virg
inia
NY
Y“M
edic
al n
eces
sity
” or
“m
edic
ally
nec
essa
ry”
mea
ns a
ppro
pria
te a
nd n
eces
sary
heal
th c
are
serv
ices
whi
ch a
re re
nder
ed fo
r any
con
ditio
n w
hich
, acc
ordi
ng to
gene
rally
acc
epte
d pr
inci
ples
of g
ood
med
ical
pra
ctic
e, re
quire
s th
e di
agno
sis
ordi
rect
car
e an
d tre
atm
ent o
f an
illne
ss, i
njur
y, o
r pre
gnan
cy-r
elat
ed c
ondi
tion,
and
are
not p
rovi
ded
only
as
a co
nven
ienc
e. V
a. C
ode
Ann.
§ 3
8.2-
5800
(200
1)
Was
hing
ton
NY
N
Wes
t Virg
inia
NY
N
Wis
cons
inN
N
Wyo
min
gN
N
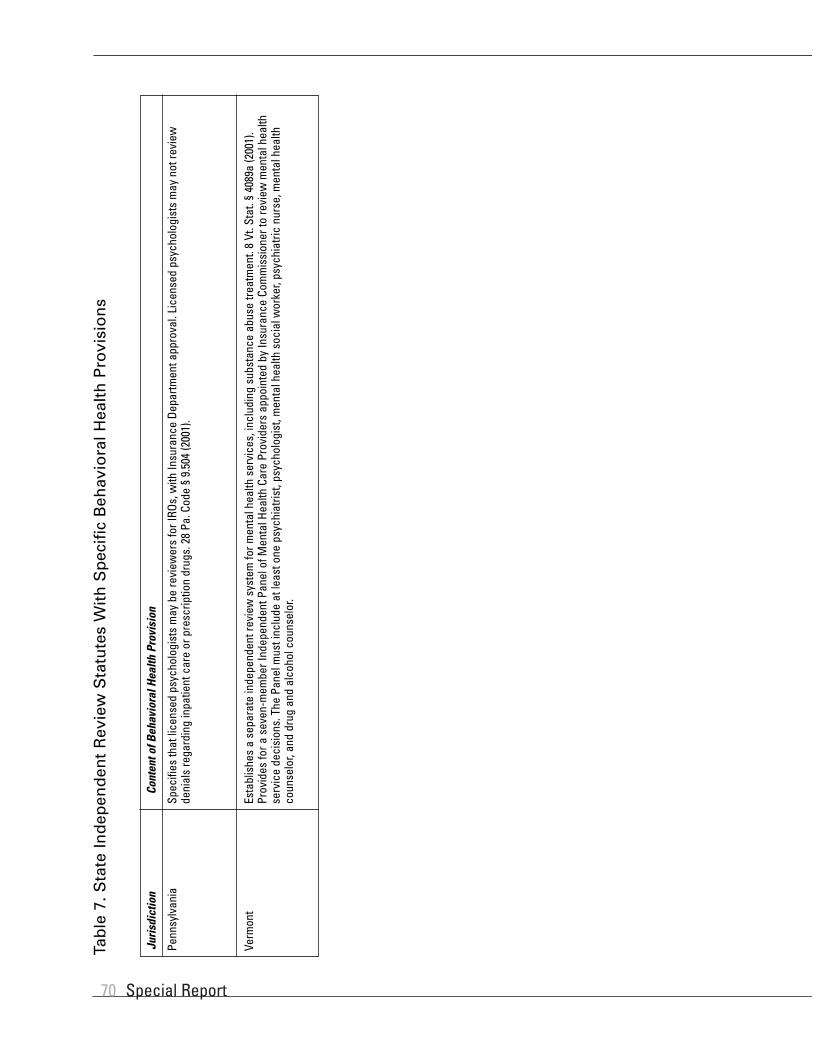
Special Report70
Penn
sylv
ania
Spec
ifies
that
lice
nsed
psy
chol
ogis
ts m
ay b
e re
view
ers
for I
ROs,
with
Insu
ranc
e De
partm
ent a
ppro
val.
Lice
nsed
psy
chol
ogis
ts m
ay n
ot re
view
deni
als
rega
rdin
g in
patie
nt c
are
or p
resc
riptio
n dr
ugs.
28
Pa. C
ode
§ 9.
504
(200
1).
Juris
dict
ion
Cont
ent o
f Beh
avio
ral H
ealth
Pro
visi
on
Verm
ont
Esta
blis
hes
a se
para
te in
depe
nden
t rev
iew
sys
tem
for m
enta
l hea
lth s
ervi
ces,
incl
udin
g su
bsta
nce
abus
e tre
atm
ent.
8 Vt
. Sta
t. §
4089
a (2
001)
.Pr
ovid
es fo
r a s
even
-mem
ber I
ndep
ende
nt P
anel
of M
enta
l Hea
lth C
are
Prov
ider
s ap
poin
ted
by In
sura
nce
Com
mis
sion
er to
revi
ew m
enta
l hea
lthse
rvic
e de
cisi
ons.
The
Pan
el m
ust i
nclu
de a
t lea
st o
ne p
sych
iatri
st, p
sych
olog
ist,
men
tal h
ealth
soc
ial w
orke
r, ps
ychi
atric
nur
se, m
enta
l hea
lthco
unse
lor,
and
drug
and
alc
ohol
cou
nsel
or.
Tab
le 7
. Sta
te In
dep
end
ent
Rev
iew
Sta
tute
s W
ith
Sp
ecif
ic B
ehav
iora
l Hea
lth
Pro
visi
on
s

Medical Necessity in Private Health Plans 71
Tab
le 8
. Qu
alif
icat
ion
s o
f E
xter
nal
Rev
iew
er in
Sta
te IR
O S
tatu
tes
Requ
irem
ent
that
Rev
iew
er H
ave
Conf
lict o
fEn
tity
that
Re
leva
nt E
xper
tise
Inte
rest
Sele
cts
or P
artic
ular
Cas
e?Pr
ohib
ition
Ju
risdi
ctio
nRe
view
erRe
view
er(√
if ye
s)(√
if ye
s)
Certi
fied
appe
alag
ency
usin
gpa
nels
of“t
wo
clin
ical
peer
s.”
Agen
cym
ustb
ece
rtifie
dby
a p
rivat
e st
anda
rd-s
ettin
g or
gani
zatio
n ap
prov
ed b
y De
partm
ent o
f Hea
lth o
r ahe
alth
insu
rer o
pera
ting
in s
tate
.
Alas
ka√
Arizo
na√
√IR
O us
ing
phys
icia
ns a
nd o
ther
hea
lth p
rofe
ssio
nals
lice
nsed
in A
rizon
a or
ano
ther
stat
e (if
boa
rd-c
ertif
ied
or e
ligib
le).
IRO
certi
fied
by In
sura
nce
Com
mis
sion
er a
nd u
sing
hea
lth c
are
prov
ider
s lic
ense
d in
Calif
orni
a an
d bo
ard-
certi
fied.
Calif
orni
a√
√
IRO
certi
fied
by In
sura
nce
Com
mis
sion
er a
nd u
sing
phy
sici
ans
or o
ther
hea
lth c
are
prof
essi
onal
s.Co
lora
do√
√
IRO
may
incl
ude
med
ical
pee
r rev
iew
org
aniza
tions
, ind
epen
dent
util
izatio
n re
view
com
pani
es, o
r nat
iona
lly re
cogn
ized
heal
th e
xper
ts o
r ins
titut
ions
app
rove
d by
the
Insu
ranc
e Co
mm
issi
oner
.
Conn
ectic
ut√
√
IRO
certi
fied
by S
ecre
tary
of H
ealth
or a
ccre
dite
d by
an
inde
pend
ent n
atio
nal
accr
editi
ng o
rgan
izatio
n an
d in
clud
es li
cens
ed a
nd b
oard
-cer
tifie
d ph
ysic
ians
or
othe
r app
ropr
iate
hea
lth c
are
prov
ider
s.
Dela
war
e√
√
IRO
cons
istin
g of
at l
east
two
phys
icia
ns li
cens
ed in
D.C
., M
aryl
and,
or V
irgin
ia(e
xcep
tions
whe
nne
cess
ary
due
toth
eco
nditi
onun
derr
evie
w)w
hoha
vem
eani
ngfu
lex
perie
nce
in p
rior u
tiliza
tion
revi
ew.
Dist
rict o
fCo
lum
bia
√√
(not
ed “
whe
nne
cess
ary”
)
IRO
pane
l con
sist
ing
of in
divi
dual
s fro
m th
e Ag
ency
for H
ealth
Car
e Ad
min
istra
tion,
the
Depa
rtmen
t of I
nsur
ance
, a c
onsu
mer
, a p
hysi
cian
app
oint
ed b
y th
e Go
vern
or,
phys
icia
ns w
ith re
leva
nt e
xper
tise
to c
ase
at is
sue
(rota
ting
pool
), an
d a
med
ical
dire
ctor
from
an
MCO
(not
a p
arty
) and
a p
rimar
y ca
re p
hysi
cian
.
Flor
ida
√
IRO
with
lice
nsed
and
boa
rd-c
ertif
ied
heal
th c
are
prov
ider
s ce
rtifie
d by
the
Depa
rtmen
t of H
ealth
Pla
nnin
g Di
visi
on.
Geor
gia
√√
Thre
e-m
embe
r pan
el a
ppoi
nted
by
the
Insu
ranc
e Co
mm
issi
oner
and
com
pose
dof
are
pres
enta
tive
from
the
man
aged
car
e pl
an n
ot in
volv
ed in
the
com
plai
nt, a
prov
ider
lice
nsed
in H
awai
i not
invo
lved
in th
e co
mpl
aint
, and
the
Com
mis
sion
eror
Com
mis
sion
er’s
desi
gnee
. Th
e Co
mm
issi
oner
may
als
o re
tain
an
IRO
to a
ssis
tin
the
revi
ew.
Haw
aii
√
MCO
Depa
rtmen
t of
Heal
th
Depa
rtmen
t of
Insu
ranc
e
Depa
rtmen
t of
Insu
ranc
e
Depa
rtmen
t of
Insu
ranc
e
Depa
rtmen
t of
Heal
th
Depa
rtmen
t of
Insu
ranc
e
Agen
cy fo
r Hea
lthCa
re A
dmin
istra
tion
Depa
rtmen
t of
Heal
th P
lann
ing
Divi
sion
Com
mis
sion
er o
fIn
sura
nce

Special Report72
Tab
le 8
. Co
nti
nu
ed
Requ
irem
ent
that
Rev
iew
er H
ave
Conf
lict o
fEn
tity
that
Re
leva
nt E
xper
tise
Inte
rest
Sele
cts
or P
artic
ular
Cas
e?Pr
ohib
ition
Ju
risdi
ctio
nRe
view
erRe
view
er(√
if ye
s)(√
if ye
s)
A ph
ysic
ian
who
hol
ds th
e sa
me
clas
s of
lice
nse
as th
e pa
tient
’s pr
imar
y ca
re p
hysi
-ci
an a
nd w
ho is
app
oint
ed b
y th
e pa
tient
, the
prim
ary
care
phy
sici
an, a
nd th
e M
CO.
Illin
ois
MCO
IRO
certi
fied
by th
e De
partm
ent o
f Ins
uran
ce a
ssig
ns a
med
ical
revi
ew p
rofe
ssio
nal
who
is li
cens
ed a
nd b
oard
cer
tifie
d in
app
licab
le s
peci
alty
for t
he a
ppea
l and
who
has
know
ledg
e ab
out t
he p
ropo
sed
serv
ice
at is
sue.
Indi
ana
MCO
(but
mus
t go
thro
ugh
the
entir
elis
t of c
ertif
ied
IROs
befo
re s
elec
ting
the
sam
e on
e ag
ain)
√√
IROs
cer
tifie
d by
the
Insu
ranc
e Co
mm
issi
oner
may
incl
ude
(but
are
not
lim
ited
to)
med
ical
pee
r rev
iew
org
aniza
tions
and
nat
iona
lly re
cogn
ized
heal
th e
xper
ts o
rin
stitu
tion.
Ind
ivid
ual r
evie
wer
mus
t hol
d ap
plic
able
hea
lth c
are
licen
se a
nd b
ebo
ard-
certi
fied.
Iow
aM
CO s
elec
ts fr
omlis
t of c
ertif
ied
IROs
√√
IRO
unde
r con
tract
with
Com
mis
sion
er o
f Ins
uran
ce.
IRO
mus
t hav
e ex
perie
nce
inad
min
iste
ring
Kans
as h
ealth
pro
gram
s or
be
a na
tiona
lly a
ccre
dite
d ex
tern
al re
view
orga
niza
tion
that
use
s Ka
nsas
hea
lth c
are
prov
ider
s to
con
duct
the
revi
ew (u
nles
s no
Kans
as p
rovi
ders
are
qua
lifie
d an
d cr
eden
tiale
d in
the
spec
ialty
at i
ssue
in th
e ca
se)
Kans
asCo
mm
issi
oner
of
Insu
ranc
e√
√
IROs
mus
t use
a re
view
er(s
) with
the
appr
opria
te li
cens
e, b
oard
cer
tific
atio
n, a
ndcl
inic
al e
xper
ienc
e ap
plic
able
to th
e m
edic
al c
ondi
tion
unde
r rev
iew
.Ke
ntuc
ky1
Depa
rtmen
t of
Insu
ranc
e √
√
IRO
mus
t be
licen
sed
by th
e In
sura
nce
Com
mis
sion
er a
nd h
ave
qual
ified
and
impa
r-tia
l clin
ical
pee
r rev
iew
ers
who
hol
d ap
prop
riate
lice
nses
and
boa
rd c
ertif
icat
ion
inth
e sp
ecia
lty a
t iss
ue a
nd h
ave
clin
ical
exp
ertis
e in
the
rele
vant
med
ical
con
ditio
n.
Loui
sian
aM
CO√
√
IRO
mus
t hav
e qu
alifi
ed a
nd im
parti
al re
view
ers
who
hol
d ap
plic
able
lice
nses
and
boar
d ce
rtific
atio
n w
ith re
spec
t to
the
adve
rse
heal
th c
are
treat
men
t und
er re
view
.M
aine
Insu
ranc
e Bu
reau
√√
The
Com
mis
sion
er m
ay m
ake
a de
term
inat
ion
on a
pat
ient
’s ap
peal
or d
esig
nate
anIR
O to
do
so.
An IR
O m
ust h
ave
qual
ified
and
impa
rtial
revi
ewer
s w
ho h
old
appl
icab
le li
cens
es a
nd b
oard
cer
tific
atio
n w
ith re
spec
t to
the
adve
rse
heal
th c
are
treat
men
t und
er re
view
.
Mar
ylan
dCo
mm
issi
oner
of
Insu
ranc
e√
√
Depa
rtmen
t of P
ublic
Hea
lth’s
Offic
e of
Pat
ient
Pro
tect
ion
cont
ract
s w
ith “
unre
late
dan
d ob
ject
ive”
revi
ew a
genc
ies
and
refe
rs a
ppea
ls to
them
on
a ra
ndom
bas
is.
Revi
ewer
s ar
e to
be
activ
ely
prac
ticin
g he
alth
car
e pr
ofes
sion
als
in th
e sa
me
orsi
mila
r spe
cial
ty w
ho ty
pica
lly tr
eat t
he m
edic
al c
ondi
tion,
per
form
the
proc
edur
eor
prov
ide
the
treat
men
t und
er re
view
.
Mas
sach
uset
tsDe
partm
ent o
fPu
blic
Hea
lth,
Offic
e of
Pat
ient
Prot
ectio
n
√√
1A
patie
nt c
anno
t obt
ain
an e
xter
nal r
evie
w if
the
subj
ect o
f the
pat
ient
’s ad
vers
e de
term
inat
ion
has
prev
ious
ly g
one
thro
ugh
the
exte
rnal
revi
ew p
roce
ss a
nd th
e in
depe
nden
tre
view
ent
ity fo
und
in fa
vor o
f the
insu
rer a
nd n
o ne
w c
linic
al e
vide
nce
is a
vaila
ble.
Ken
. Rev
. Sta
t. ß
304.
17A-
623(
6).
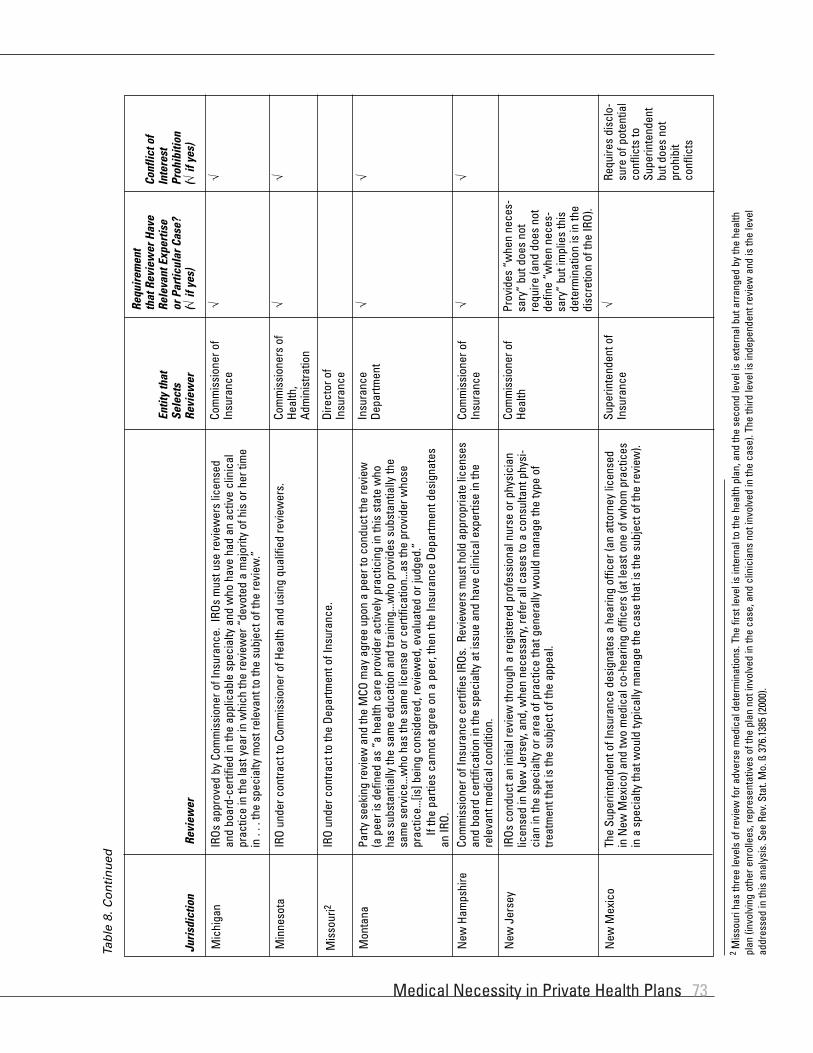
Medical Necessity in Private Health Plans 73
Tab
le 8
. Co
nti
nu
ed
Requ
irem
ent
that
Rev
iew
er H
ave
Conf
lict o
fEn
tity
that
Re
leva
nt E
xper
tise
Inte
rest
Sele
cts
or P
artic
ular
Cas
e?Pr
ohib
ition
Ju
risdi
ctio
nRe
view
erRe
view
er(√
if ye
s)(√
if ye
s)
IROs
app
rove
d by
Com
mis
sion
er o
f Ins
uran
ce.
IROs
mus
t use
revi
ewer
s lic
ense
dan
d bo
ard-
certi
fied
in th
e ap
plic
able
spe
cial
ty a
nd w
ho h
ave
had
an a
ctiv
e cl
inic
alpr
actic
e in
the
last
yea
r in
whi
ch th
e re
view
er “
devo
ted
a m
ajor
ity o
f his
or h
er ti
me
in .
. . th
e sp
ecia
lty m
ost r
elev
ant t
o th
e su
bjec
t of t
he re
view
.”
Mic
higa
nCo
mm
issi
oner
of
Insu
ranc
e√
√
IRO
unde
r con
tract
to C
omm
issi
oner
of H
ealth
and
usi
ng q
ualif
ied
revi
ewer
s.M
inne
sota
Com
mis
sion
ers
ofHe
alth
,Ad
min
istra
tion
√√
IRO
unde
r con
tract
to th
e De
partm
ent o
f Ins
uran
ce.
Mis
sour
i2Di
rect
or o
fIn
sura
nce
Party
see
king
revi
ew a
nd th
e M
CO m
ay a
gree
upo
n a
peer
to c
ondu
ct th
e re
view
(ape
er is
def
ined
as
“a h
ealth
car
e pr
ovid
er a
ctiv
ely
prac
ticin
g in
this
sta
te w
hoha
ssu
bsta
ntia
lly th
e sa
me
educ
atio
n an
d tra
inin
g...w
ho p
rovi
des
subs
tant
ially
the
sam
e se
rvic
e...w
ho h
as th
e sa
me
licen
se o
r cer
tific
atio
n...a
s th
e pr
ovid
er w
hose
prac
tice.
..[is
] bei
ng c
onsi
dere
d, re
view
ed, e
valu
ated
or j
udge
d.”
If th
e pa
rties
can
not a
gree
on
a pe
er, t
hen
the
Insu
ranc
e De
partm
ent d
esig
nate
san
IRO.
Mon
tana
Insu
ranc
eDe
partm
ent
√√
Com
mis
sion
er o
f Ins
uran
ce c
ertif
ies
IROs
. Re
view
ers
mus
t hol
d ap
prop
riate
lice
nses
and
boar
d ce
rtific
atio
n in
the
spec
ialty
at i
ssue
and
hav
e cl
inic
al e
xper
tise
in th
ere
leva
nt m
edic
al c
ondi
tion.
New
Ham
pshi
reCo
mm
issi
oner
of
Insu
ranc
e√
√
IROs
con
duct
an
initi
al re
view
thro
ugh
a re
gist
ered
pro
fess
iona
l nur
se o
r phy
sici
anlic
ense
d in
New
Jer
sey,
and
, whe
n ne
cess
ary,
refe
r all
case
s to
a c
onsu
ltant
phy
si-
cian
in th
e sp
ecia
lty o
r are
a of
pra
ctic
e th
at g
ener
ally
wou
ld m
anag
e th
e ty
pe o
ftre
atm
ent t
hat i
s th
e su
bjec
t of t
he a
ppea
l.
New
Jer
sey
Com
mis
sion
er o
fHe
alth
Prov
ides
“w
hen
nece
s-sa
ry”
but d
oes
not
requ
ire (a
nd d
oes
not
defin
e “w
hen
nece
s-sa
ry”
but i
mpl
ies
this
dete
rmin
atio
n is
in th
edi
scre
tion
of th
e IR
O).
The
Supe
rinte
nden
t of I
nsur
ance
des
igna
tes
a he
arin
g of
ficer
(an
atto
rney
lice
nsed
in N
ew M
exic
o) a
nd tw
o m
edic
al c
o-he
arin
g of
ficer
s (a
t lea
st o
ne o
f who
m p
ract
ices
in a
spe
cial
ty th
at w
ould
typi
cally
man
age
the
case
that
is th
e su
bjec
t of t
he re
view
).
New
Mex
ico
Supe
rinte
nden
t of
Insu
ranc
eRe
quire
s di
sclo
-su
re o
f pot
entia
lco
nflic
ts to
Supe
rinte
nden
tbu
t doe
s no
tpr
ohib
itco
nflic
ts
√
2M
isso
uri h
as th
ree
leve
ls o
f rev
iew
for a
dver
se m
edic
al d
eter
min
atio
ns. T
he fi
rst l
evel
is in
tern
al to
the
heal
th p
lan,
and
the
seco
nd le
vel i
s ex
tern
al b
ut a
rran
ged
by th
e he
alth
plan
(inv
olvi
ng o
ther
enr
olle
es, r
epre
sent
ativ
es o
f the
pla
n no
t inv
olve
d in
the
case
, and
clin
icia
ns n
ot in
volv
ed in
the
case
). Th
e th
ird le
vel i
s in
depe
nden
t rev
iew
and
is th
e le
vel
addr
esse
d in
this
ana
lysi
s. S
ee R
ev. S
tat.
Mo.
ß 3
76.1
385
(200
0).

Special Report74
Requ
irem
ent
that
Rev
iew
er H
ave
Conf
lict o
fEn
tity
that
Re
leva
nt E
xper
tise
Inte
rest
Sele
cts
or P
artic
ular
Cas
e?Pr
ohib
ition
Ju
risdi
ctio
nRe
view
erRe
view
er(√
if ye
s)(√
if ye
s)
The
Supe
rinte
nden
t of I
nsur
ance
and
the
Com
mis
sion
er o
f Hea
lth c
ertif
y IR
Os a
ndra
ndom
ly a
ssig
n ap
peal
s to
them
. IR
O re
view
ers
mus
t hav
e th
e ap
prop
riate
lice
nse,
boar
d ce
rtific
atio
n, a
nd c
linic
al e
xper
ienc
e ap
plic
able
to th
e m
edic
al c
ondi
tion
unde
rre
view
.
New
Yor
kSu
perin
tend
ent
ofIn
sura
nce
and
Com
mis
sion
er o
fHe
alth
√√
Insu
ranc
e Co
mm
issi
oner
ass
igns
IRO
on a
rota
ting
basi
s fro
m li
st o
f app
rove
dor
gani
zatio
ns. I
RO re
view
ers
mus
t hav
e th
e ap
prop
riate
lice
nse,
boa
rd c
ertif
icat
ion,
and
clin
ical
exp
erie
nce
appl
icab
le to
the
med
ical
con
ditio
n un
der r
evie
w.
Nor
th C
arol
ina
Insu
ranc
eCo
mm
issi
oner
√√
Insu
ranc
e Su
perin
tend
ent a
ccre
dits
IROs
and
mai
ntai
ns a
list
of a
ppro
ved
orga
niza
-tio
ns.
Upon
a re
ques
t for
ext
erna
l app
eal,
Supe
rinte
nden
t pro
vide
s tw
o IR
Os c
hose
nat
rand
om fr
om th
e lis
t, an
d th
e M
CO c
hoos
es o
ne o
f the
m.
One
revi
ewer
con
duct
sth
e re
view
(unl
ess
the
MCO
or I
RO d
eter
min
es th
at m
ore
than
one
is n
eces
sary
),an
dth
e re
view
er(s
) mus
t hav
e th
e ap
prop
riate
lice
nse,
boa
rd c
ertif
icat
ion,
and
clin
ical
exp
erie
nce
appl
icab
le to
the
med
ical
con
ditio
n un
der r
evie
w.
Ohio
Insu
ranc
eSu
perin
tend
ent
(MCO
cho
oses
amon
g tw
o IR
Osse
lect
ed a
tra
ndom
)
√√
MCO
sel
ects
IRO
from
a li
st o
f org
aniza
tions
cer
tifie
d by
the
Depa
rtmen
t of H
ealth
.Re
view
ers
have
the
appr
opria
te li
cens
e, b
oard
cer
tific
atio
n, a
nd c
linic
al e
xper
ienc
eap
plic
able
to th
e m
edic
al c
ondi
tion
unde
r rev
iew
.
Okla
hom
aM
CO c
hoos
es fr
omDe
partm
ent o
fHe
alth
-cer
tifie
dor
gani
zatio
ns.
√√
Whe
n le
gisl
atio
n be
com
es e
ffect
ive
(Jul
y 1,
200
2), D
irect
or o
f Bus
ines
s an
dCo
nsum
er A
ffairs
Dep
artm
ent w
ill c
ontra
ct w
ith IR
Os q
ualif
ied
unde
r reg
ulat
ions
tobe
dev
elop
ed p
rior t
o Ju
ly 1
, 200
2.
Oreg
onDi
rect
or o
fBu
sine
ss a
ndCo
nsum
er A
ffairs
Depa
rtmen
t
To B
eDe
term
ined
To B
e De
term
ined
Insu
ranc
e Co
mm
issi
oner
ass
igns
IRO
on a
rota
ting
basi
s fro
m li
st o
f app
rove
d or
gani
-za
tions
. IRO
revi
ewer
s m
ust h
ave
the
appr
opria
te li
cens
e, b
oard
cer
tific
atio
n, a
ndcl
inic
al e
xper
ienc
e ap
plic
able
to th
e m
edic
al c
ondi
tion
unde
r rev
iew
. Re
view
ers
may
incl
ude
licen
sed
psyc
holo
gist
s (a
lthou
gh th
ey c
anno
t rev
iew
den
ials
of i
npat
ient
care
or p
resc
riptio
n dr
ugs)
.
If In
sura
nce
Com
mis
sion
er fa
ils to
ass
ign
an IR
O w
ithin
2 b
usin
ess
days
of t
here
ques
t for
revi
ew, t
he M
CO m
ay a
ssig
n an
IRO
from
list
of o
rgan
izatio
ns a
ppro
ved
byIn
sura
nce
Depa
rtmen
t.
Penn
sylv
ania
3In
sura
nce
Com
mis
sion
er (o
rM
CO if
Insu
ranc
eCo
mm
issi
oner
fails
to a
ssig
n IR
O w
ithin
2 bu
sine
ss d
ays
ofre
ques
t for
ext
erna
lre
view
)
√√
Insu
ranc
e De
partm
ent c
ertif
ies
IROs
. Re
view
er m
ust b
e a
phys
icia
n, d
entis
t, or
oth
erhe
alth
car
e pr
ofes
sion
al o
f the
spe
cial
ty re
leva
nt to
the
care
or s
ervi
ce u
nder
revi
ew.
Rhod
e Is
land
Desi
gnat
ed b
yIn
sura
nce
Dire
ctor
√√
Tab
le 8
. Co
nti
nu
ed
3Pe
nnsy
lvan
ia a
llow
s an
MCO
and
pro
vide
r to
agre
e to
an
alte
rnat
e di
sput
e re
solu
tion
syst
em in
a w
ritte
n co
ntra
ct if
the
Insu
ranc
e De
partm
ent a
ppro
ves
of th
e al
tern
ate
syst
em.
40Pa
. Sta
t. ß
991.
2162
.

Medical Necessity in Private Health Plans 75
Tab
le 8
. Co
nti
nu
ed
Requ
irem
ent
that
Rev
iew
er H
ave
Conf
lict o
fEn
tity
that
Re
leva
nt E
xper
tise
Inte
rest
Sele
cts
or P
artic
ular
Cas
e?Pr
ohib
ition
Ju
risdi
ctio
nRe
view
erRe
view
er(√
if ye
s)(√
if ye
s)
Insu
ranc
e De
partm
ent m
aint
ains
list
of a
ppro
ved
IROs
and
des
igna
tes
IRO
upon
requ
est f
or e
xter
nal r
evie
w.
IRO
revi
ewer
s m
ust h
ave
the
appr
opria
te li
cens
e,bo
ard
certi
ficat
ion,
and
clin
ical
exp
erie
nce
(with
in th
e pa
st th
ree
year
s) a
pplic
able
toth
e m
edic
al c
ondi
tion
unde
r rev
iew
.
Sout
h Ca
rolin
aIn
sura
nce
Depa
rtmen
t√
√
MCO
des
igna
tes
IRO,
whi
ch m
ust b
e im
parti
al a
nd u
se re
view
ers
that
hav
e th
eap
prop
riate
lice
nse
and
boar
d ce
rtific
atio
n ap
plic
able
to th
e m
edic
al c
ondi
tion
unde
rre
view
.
Tenn
esse
eM
CO√
√
Depa
rtmen
t of I
nsur
ance
ass
igns
IROs
rand
omly
from
an
appr
oved
list
. Re
view
ers
mus
t be
in a
ctiv
e pr
actic
e an
d ha
ve th
e ap
prop
riate
lice
nse
and
boar
d ce
rtific
atio
nap
plic
able
to th
e m
edic
al c
ondi
tion
unde
r rev
iew
.
Texa
sDe
partm
ent o
fIn
sura
nce
√√
MCO
des
igna
tes
IRO,
whi
ch m
ust b
e im
parti
al.
Utah
MCO
Com
mis
sion
er o
f Dep
artm
ent o
f Ban
king
, Ins
uran
ce, S
ecur
ities
, and
Hea
lth C
are
Adm
inis
tratio
n (B
ISHC
A) d
esig
nate
s IR
Os.
Revi
ewer
s m
ust b
e in
act
ive
prac
tice
and
have
the
appr
opria
te li
cens
e an
d bo
ard
certi
ficat
ion
appl
icab
le to
the
med
ical
cond
ition
und
er re
view
.
An In
depe
nden
t Pan
el o
f Men
tal H
ealth
Car
e Pr
ovid
ers
revi
ews
deci
sion
sin
volv
ing
men
tal h
ealth
ser
vice
s, in
clud
ing
drug
and
alc
ohol
trea
tmen
t.
Verm
ont
Com
mis
sion
er o
fBI
SHCA
√√
IROs
con
tract
with
the
Bure
au o
f Ins
uran
ce.
Revi
ewer
s m
ust h
ave
the
appr
opria
telic
ense
and
boa
rd c
ertif
icat
ion
appl
icab
le to
the
med
ical
con
ditio
n un
der r
evie
w.
Virg
inia
Bure
au o
fIn
sura
nce
√√
Depa
rtmen
t of H
ealth
cer
tifie
s IR
Os a
nd m
aint
ains
regi
stry
for a
ssig
nmen
t.Re
view
ers
mus
t hav
e fiv
e ye
ars
of c
linic
al e
xper
ienc
e an
d ha
ve th
e ap
prop
riate
licen
se a
nd b
oard
cer
tific
atio
n ap
plic
able
to th
e m
edic
al c
ondi
tion.
Und
er re
view
.
Was
hing
ton
Depa
rtmen
t of
Heal
th√
√
The
Depa
rtmen
t of I
nsur
ance
cer
tifie
s IR
Os, w
hich
mus
t use
at l
east
one
phy
sici
anor
othe
r hea
lth c
are
prov
ider
kno
wle
dgea
ble
abou
t the
hea
lth c
are
serv
ice
unde
rre
view
.
Wes
t Virg
inia
4De
partm
ent o
fIn
sura
nce
√√
4W
est V
irgin
ia a
llow
s M
COs
an e
xem
ptio
n fro
m th
e IR
O st
atut
e if
the
MCO
has
an
exte
rnal
revi
ew p
lan
appr
oved
by
the
Depa
rtmen
t of I
nsur
ance
. W
. Va.
Cod
e ß
33-2
5C-6
.

Special Report76
If St
anda
rd is
De
Nov
o or
Not
Spe
cifie
d,
Juris
dict
ion
De N
ovo
Othe
rCa
n In
sure
d Su
bmit
Addi
tiona
l Evi
denc
e? (√
if ye
s)
√Al
aska
√Ar
izona
Calif
orni
a√ √
√Co
lora
do
Conn
ectic
ut√ √
Dela
war
e
Dist
rict o
f Col
umbi
a√
(Insu
red
can
also
requ
est a
hea
ring
befo
re IR
O.)
Flor
ida
Geor
gia
√
Haw
aii
Illin
ois
√In
dian
a
√Io
wa
√ √Ka
nsas
Kent
ucky
√
Loui
sian
a
Mai
ne√
(Pat
ient
may
atte
nd th
e ex
tern
al re
view
, ask
que
stio
ns o
f the
insu
ranc
e co
mpa
ny re
pres
enta
tive,
and
use
outs
ide
assi
stan
ce s
uch
as c
ouns
el [a
t the
pat
ient
’s ex
pens
e].)
Mas
sach
uset
ts
√M
ichi
gan
√ √M
inne
sota
Mis
sour
i√
Mon
tana
√√
New
Ham
pshi
re
Tab
le 9
. In
dep
end
ent
Rev
iew
s: S
tan
dar
d o
f R
evie
w f
or
Med
ical
Nec
essi
ty D
eter
min
atio
ns
√M
aryl
and1
1M
aryl
and’
s IR
O st
atut
e pl
aces
the
burd
en o
f pro
of o
n th
e M
CO to
dem
onst
rate
that
its
initi
al a
dver
se d
ecis
ion
was
cor
rect
. M
d. In
s. C
ode
Ann.
ß 1
5-10
A-03
(e) (
2001
).

Medical Necessity in Private Health Plans 77
Tab
le 9
. Co
nti
nu
ed
If St
anda
rd is
De
Nov
o or
Not
Spe
cifie
d,
Juris
dict
ion
De N
ovo
Othe
rCa
n In
sure
d Su
bmit
Addi
tiona
l Evi
denc
e? (√
if ye
s)
New
Jer
sey
√(H
earin
g of
ficer
and
co-
med
ical
hea
ring
offic
ers
cond
uct h
earin
g w
ith w
itnes
ses
and
pres
enta
tion
of e
vide
nce.
)N
ew M
exic
o
√N
ew Y
ork
Nor
th C
arol
ina
√ √Oh
io
Okla
hom
a√ To
Be
Dete
rmin
edOr
egon
Penn
sylv
ania
√
Rhod
e Is
land
√So
uth
Caro
lina
√
Tenn
esse
e
Texa
s√
Utah
Verm
ont
√
Virg
inia
Was
hing
ton
√
Wes
t Virg
inia


Medical Necessity in Private Health Plans 79
1992
Eddy
, Dav
id
An a
ccou
nt o
f how
ana
lysi
s of
cos
t-effe
ctiv
enes
s w
as u
sed
to c
hang
e pr
actic
e gu
idel
ines
on
high
and
low
osm
olar
radi
ogra
phic
con
trast
age
nts
at K
aise
r. Di
fficu
lties
with
ana
lysi
s an
d bu
y-in
are
disc
usse
d. T
he g
ener
al lo
gist
ics
of th
e an
alys
is it
self
are
desc
ribed
, as
are
the
lines
of t
houg
htbe
hind
eac
h st
ep o
f the
ana
lysi
s.
JAM
A 26
8(18
): 25
75–2
582
Clin
ical
Dec
isio
nM
akin
g: F
rom
Theo
ry to
Prac
tice.
Appl
ying
Cos
tEf
fect
iven
ess
Anal
ysis
, the
Insi
de S
tory
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
1993
Ande
rson
, G. F
.,an
d M
. A. H
all
Ther
e is
the
expe
ctat
ion
that
out
com
es re
sear
ch a
nd th
e pr
omul
gatio
n of
med
ical
pra
ctic
e gu
ide-
lines
will
be
able
to id
entif
y an
d ho
pefu
lly re
duce
the
amou
nt o
f unn
eces
sary
or i
napp
ropr
iate
med
ical
car
e th
roug
h a
varie
ty o
f met
hods
, inc
ludi
ng u
tiliza
tion
revi
ew. H
owev
er, t
he c
ourts
for
mul
tifar
ious
reas
ons
have
freq
uent
ly o
vertu
rned
pas
t effo
rts b
y pu
blic
and
priv
ate
insu
rers
to d
eny
clai
ms
on th
e ba
sis
of fo
rmal
tech
nolo
gy a
sses
smen
ts o
r pra
ctic
e gu
idel
ines
. Thi
s pa
per e
xam
ines
the
cour
t’s re
luct
ance
to a
ccep
t a v
arie
ty o
f tec
hnol
ogy
asse
ssm
ent m
etho
ds in
cov
erag
e po
licy
deci
sion
s. T
he p
aper
revi
ews
the
optio
ns th
at h
ave
been
pro
pose
d to
rest
rict j
udic
ial i
nvol
vem
ent
in th
e fo
rmul
atio
n of
cov
erag
e po
licy
and
then
pro
pose
s a
new
opt
ion
that
em
ploy
s a
mor
e pr
ecis
eta
xono
my
of m
edic
al p
ract
ice
asse
ssm
ent.
Amer
ican
Jou
rnal
ofPu
blic
Hea
lth83
:163
5–16
39
Med
ical
Tech
nolo
gyAs
sess
men
t and
Prac
tice
Guid
elin
es: T
heir
Day
in C
ourt
1992
Hall,
Mar
k, a
ndGe
rard
And
erso
n EX
CERP
TS:
... T
ishn
a, I
was
told
, had
virt
ually
no
chan
ce o
f sur
vivi
ng th
e re
laps
ed W
ilms’
tum
or [o
f the
kid
ney]
from
whi
ch s
he is
suf
ferin
g an
d Bl
ue C
ross
/Blu
e Sh
ield
had
den
ied
cove
rage
for a
utol
ogou
s bo
nem
arro
w tr
ansp
lant
(“AB
MT”
) with
acc
ompa
nyin
g hi
gh d
ose
chem
othe
rapy
, a tr
eatm
ent w
hich
coul
d w
ell p
rolo
ng a
nd q
uite
pos
sibl
y sa
ve h
er li
fe a
nd w
hich
, con
cede
dly,
pro
vide
d he
r onl
y re
al-
istic
hop
e of
eith
er. .
.. In
abo
ut a
doz
en s
imila
r cas
es, h
owev
er, j
udge
s ha
ve ru
led
that
the
use
ofAB
MT
is s
till e
xper
imen
tal a
nd d
enie
d co
vera
ge. .
.. Fr
om a
lega
l per
spec
tive,
how
ever
, the
seru
lings
are
mer
ely
the
late
st in
a lo
ng s
erie
s of
ord
inar
y co
ntra
ct d
ispu
tes
over
the
inte
rpre
tatio
nof
term
s su
ch a
s “m
edic
al n
eces
sity
” or
“ex
perim
enta
l,” w
hich
det
erm
ine
the
cove
rage
of h
ealth
insu
ranc
e po
licie
s. ..
. In
addi
tion
to th
is h
uman
itaria
n ob
ject
ive,
the
cour
ts h
ave
been
con
cern
edab
out t
he p
erce
ived
unf
airn
ess
of a
retro
activ
e de
nial
of c
over
age
afte
r a p
atie
nt h
as re
lied
on h
isph
ysic
ian’
s ad
vice
and
incu
rred
a b
ill fo
r tre
atm
ent l
ater
foun
d by
the
insu
rer t
o be
inap
prop
riate
....
An
asse
ssm
ent t
hat a
tech
nolo
gy is
“ex
perim
enta
l” a
t one
tim
e m
ust b
e m
odifi
ed if
add
ition
alre
sear
ch o
r clin
ical
find
ings
val
idat
e (o
r rep
udia
te) i
ts e
ffect
iven
ess.
...
Univ
ersi
ty o
fPe
nnsy
lvan
ia L
awRe
view
140
U P
a.L.
Rev.
1637
Mod
els
ofRa
tioni
ng: H
ealth
Insu
rers
’As
sess
men
t of
Med
ical
Nec
essi
ty
Ap
pen
dix
A. S
elec
ted
Pu
blis
hed
Lit
erat
ure
on
Med
ical
Nec
essi
ty (
So
rted
by
Year
)

Special Report80
1994
Sabi
n, J
ames
E.,
and
Nor
man
Dani
els
The
auth
ors
pose
d th
e qu
estio
n, “
Shou
ld m
enta
l hea
lth in
sura
nce
cove
r onl
y di
sord
ers
foun
din
DSM
-IV, o
r sho
uld
it be
ext
ende
d to
trea
tmen
t for
ord
inar
y sh
ynes
s, u
nhap
pine
ss, a
nd o
ther
resp
onse
s to
life
’s ha
rd k
nock
s?”
Thro
ugh
the
use
of s
ix il
lust
rativ
e ca
se s
tudi
es, t
he a
utho
rsex
amin
ed th
e re
ason
ing
behi
nd th
e de
term
inat
ions
of m
edic
al n
eces
sity
. The
arti
cle
incl
udes
adi
scus
sion
of a
recu
rren
t con
flict
bet
wee
n “h
ard-
line”
and
“ex
pans
ive”
vie
ws
of m
edic
al n
eces
-si
ty, n
otin
g th
at it
freq
uent
ly re
flect
s un
reco
gnize
d m
oral
dis
agre
emen
t abo
ut th
e ta
rget
s of
clin
ical
inte
rven
tion
and
the
ultim
ate
goal
s of
psy
chia
tric
treat
men
t. Th
e au
thor
s pr
esen
t thr
ee m
odel
sfo
rdef
inin
g m
edic
al n
eces
sity
and
arg
ue a
def
ensi
ble
ratio
nale
for t
he “
norm
al”
mod
el, w
hich
com
pris
es a
targ
et o
f a m
edic
ally
def
ined
dev
iatio
n in
tend
ed to
dec
reas
e th
e im
pact
of d
isea
seor
disa
bilit
y. T
hree
test
s of
med
ical
nec
essi
ty a
re o
ffere
d: (1
) Doe
s it
mak
e di
stin
ctio
ns th
e pu
blic
and
clin
icia
ns re
gard
as
fair?
(2) C
an it
be
adm
inis
tere
d in
the
real
wor
ld?
(3) D
oes
it le
ad to
resu
ltsth
at s
ocie
ty c
an a
fford
? In
the
auth
ors’
vie
w, a
typi
cal m
edic
al n
eces
sity
def
initi
on in
the
“nor
mal
” m
odel
wou
ld b
e “t
hose
men
tal h
ealth
ser
vice
s w
hich
are
ess
entia
l for
the
treat
men
tof
a M
embe
r’s m
enta
l hea
lth d
isor
der a
s de
fined
by
the
DSM
-IVin
acc
orda
nce
with
gen
eral
lyac
cept
ed m
enta
l hea
lth p
ract
ice.
” Th
e au
thor
s co
nclu
de th
at th
e DS
M-IV
stan
dard
pro
vide
sw
orka
ble
boun
darie
s fo
r med
ical
nec
essi
ty d
efin
ition
s to
the
exte
nt th
at th
ey a
re th
e re
sult
of a
high
ly p
ublic
pro
cess
ope
n to
sci
entif
ic s
crut
iny,
fiel
d te
stin
g, a
nd re
petit
ive
criti
cism
ove
r tim
e.
Hast
ings
Cen
ter R
epor
t24
(6):5
–13
Dete
rmin
ing
“Med
ical
Nec
essi
ty”
inM
enta
l Hea
lthPr
actic
e
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
Ap
pen
dix
A. C
on
tin
ued

Medical Necessity in Private Health Plans 81
1994
Eddy
, Dav
id M
. EX
CERP
T: “
[...]
whe
n de
term
inin
g th
e ap
prop
riate
use
of a
n in
terv
entio
n, w
e w
ill n
eed
to c
hang
eou
r way
of t
hink
ing
from
qua
litat
ive
reas
onin
g to
qua
ntita
tive
reas
onin
g. T
o a
grea
t ext
ent,
the
pred
icam
ent w
e fa
ce to
day
is th
e re
sult
of q
ualit
ativ
e re
ason
ing
that
ass
umes
that
if a
pra
ctic
em
ight
hav
e an
y be
nefit
it s
houl
d be
don
e—th
e “c
riter
ion
of p
oten
tial b
enef
it.”
Beca
use
this
type
ofre
ason
ing
does
not
try
to d
eter
min
e th
e am
ount
of v
alue
a p
ract
ice
prov
ides
—se
para
ting
thos
ew
ith h
igh
valu
e fro
m th
ose
with
sm
all v
alue
—it
has
left
us w
ith th
e la
rge
inef
ficie
ncie
s th
at w
ese
ein
our
pra
ctic
es to
day.
To
take
adv
anta
ge o
f the
se in
effic
ienc
ies,
we
will
hav
e to
dev
elop
bette
r ski
lls fo
r qua
ntita
tive
reas
onin
g. It
is n
o co
inci
denc
e th
at e
very
exa
mpl
e in
this
arti
cle
was
stud
ded
with
num
bers
; it i
s no
t pos
sibl
e to
det
erm
ine
how
muc
h be
nefit
will
be
gain
ed o
r how
muc
h co
st w
ill b
e sa
ved
by a
tran
sfer
with
out e
stim
atin
g th
e be
nefit
s or
the
cost
s.
“[...
] we
will
nee
d to
cha
nge
from
focu
sing
on
indi
vidu
als
to fo
cusi
ng o
n po
pula
tions
—fro
m “
indi
-vi
dual
-bas
ed”
deci
sion
mak
ing
to “
popu
latio
n-ba
sed”
dec
isio
n m
akin
g. In
par
ticul
ar, p
ract
ition
ers
need
to d
evel
op a
n al
legi
ance
to th
e en
tire
mem
bers
hip
of th
e he
alth
pla
n. T
his
will
be
diffi
cult
fort
hose
who
see
them
selv
es a
s se
rvin
g as
thei
r pat
ient
s’ a
dvoc
ate
in a
stru
ggle
with
adm
inis
-tra
tors
and
insu
rers
. Tha
t per
cept
ion
is in
corr
ect.
Whe
n ph
ysic
ians
hoa
rd re
sour
ces
for t
heir
own
patie
nts,
they
are
not
taki
ng fr
om a
dmin
istra
tors
or i
nsur
ers;
they
are
taki
ng fr
om o
ther
pat
ient
s.If
each
pra
ctiti
oner
is c
once
rned
onl
y ab
out h
is o
r her
indi
vidu
al p
atie
nt, w
ithou
t con
cern
for t
heim
pact
of h
is o
r her
dec
isio
ns o
n ot
her p
atie
nts,
the
resu
lt w
ill n
ot b
e lo
wer
cos
ts a
nd h
ighe
rqu
ality
, but
hig
her c
osts
and
low
er q
ualit
y.
“If h
ealth
pla
ns a
nd in
divi
dual
pra
ctiti
oner
s ar
e to
suc
ceed
in m
akin
g tra
nsfe
rs th
at in
crea
sequ
ality
whi
le re
duci
ng c
osts
, the
y w
ill n
eed
both
gui
danc
e an
d pr
otec
tion.
Gui
danc
e w
ill b
ene
eded
toen
sure
that
dec
isio
ns a
re c
onsi
sten
t and
hav
e th
e de
sire
d ef
fect
s. P
rote
ctio
n w
ill b
ene
eded
tode
fend
bot
h pl
ans
and
prac
titio
ners
whe
n th
ey m
ake
and
impl
emen
t con
trove
rsia
lde
cisi
ons.
The
bes
t way
to a
ddre
ss b
oth
thos
e ne
eds
is to
dev
elop
exp
licit
crite
ria th
at w
ill s
ort
out h
igh-
valu
e pr
actic
es fr
om th
ose
that
hav
e lit
tle o
r no
valu
e an
d w
ill s
uppo
rt tra
nsfe
rs fr
omon
e to
the
othe
r. Cu
rren
tly, t
he c
lose
st w
e ge
t to
such
crit
eria
are
thro
ugh
vagu
e an
d va
riabl
ete
rms
such
as
“med
ical
ly n
eces
sary
” an
d “m
edic
ally
app
ropr
iate
.” B
ut th
ese
are
far t
oo v
ague
and
varia
bly
inte
rpre
ted.
If w
e ar
e to
con
trol c
osts
whi
le p
rese
rvin
g qu
ality
, the
firs
t nee
d is
tode
velo
p be
tter c
riter
ia fo
r ben
efit
lang
uage
.”
JAM
A 27
2(10
) Fr
om T
heor
yto
Prac
tice:
Ratio
ning
Reso
urce
s W
hile
Impr
ovin
g Qu
ality
:Ho
w to
Get
Mor
efo
r Les
s
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
Ap
pen
dix
A. C
on
tin
ued

Special Report82
1997
Hest
er, T
hom
asW
.Th
e go
als
of th
is p
aper
are
to p
rovi
de th
e re
ader
with
an
unde
rsta
ndin
g an
d ra
tiona
le fo
r the
appr
opria
te u
se o
f tre
atm
ent a
lgor
ithm
s fo
r peo
ple
with
ser
ious
men
tal i
llnes
s. It
sug
gest
s ef
fec-
tive
stra
tegi
es fo
r usi
ng tr
eatm
ent a
lgor
ithm
s to
impr
ove
the
qual
ity o
f tre
atm
ent a
nd to
incr
ease
the
acco
unta
bilit
y of
med
icat
ion
treat
men
t. Th
e pa
per a
lso
addr
esse
s po
tent
ial d
ange
rs in
dev
el-
opin
g pr
actic
e gu
idel
ines
and
pro
vide
s ad
vice
for a
void
ing
thes
e pi
tfalls
. Iss
ues
rela
ted
to le
gal
mat
ters
and
man
aged
car
e co
ntra
ctin
g ar
e di
scus
sed
brie
fly.
MAS
MHP
D Re
sear
chIn
stitu
te R
epor
tAl
gorit
hms
and
the
Med
icat
ion
Trea
tmen
t of
Peop
le w
ithSe
rious
Men
tal
Illne
ss
1995
Berg
thol
d,Li
nda
A.Th
e te
rm m
edic
al n
eces
sity
has
bee
n m
ainl
y a
plac
ehol
der i
n in
sura
nce
plan
s fo
r ove
r thi
rty y
ears
.M
ore
rece
ntly
, the
nat
iona
l hea
lth c
are
refo
rm d
ebat
e an
d lit
igat
ion
over
den
ials
of c
ostly
exp
eri-
men
tal t
reat
men
ts h
ave
brok
en th
e te
rm o
ut in
to o
pen
disc
ussi
on a
bout
wha
t a n
eces
sary
ser
vice
is a
nd w
ho s
houl
d de
cide
if it
is c
over
ed. T
his
pape
r sum
mar
izes
the
hist
ory
of th
e te
rm a
nd it
sev
olut
ion
from
an
insu
ranc
e co
ncep
t con
trolle
d by
pra
ctic
ing
phys
icia
ns to
a ra
tioni
ng to
ol u
sed
by in
sura
nce
adm
inis
trato
rs. H
ow d
id n
atio
nal r
efor
m e
fforts
add
ress
this
term
inol
ogy,
and
how
shou
ld w
e de
fine
med
ical
nec
essi
ty in
a c
hang
ing
deliv
ery
syst
em?
Heal
th A
ffairs
14(
4):
180–
190
Med
ical
Nec
essi
ty:
DoW
eN
eed
It?
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
1997
Gros
s, J
oshu
a M
.Kn
owle
dge
of th
e ba
sic
econ
omic
fact
ors
unde
rlyin
g m
anag
ed m
enta
l hea
lth c
are
dire
ctly
impa
cts
the
clin
ical
pra
ctiti
oner
s’ a
bilit
y to
mak
e co
nstru
ctiv
e ch
ange
s in
the
syst
em. T
o ai
d un
ders
tand
ing
this
arti
cle
intro
duce
s th
e m
anag
ed c
are
mar
ketp
lace
mod
el, t
he in
tera
ctiv
e re
latio
nshi
p be
twee
nm
edic
al n
eces
sity
and
pat
ient
co-
paym
ent,
and
dem
and
man
agem
ent e
cono
mic
s. T
he a
utho
ren
cour
ages
pra
ctiti
oner
s to
dev
elop
stra
tegi
es to
ove
rcom
e sp
ecifi
c ec
onom
ic o
bsta
cles
that
prev
ent t
he p
rom
otio
n of
gro
up p
sych
othe
rapy
.
Inte
rnat
iona
l Jou
rnal
ofGr
oup
Psyc
hoth
erap
y47
(4):4
99–5
07
Prom
otin
g Gr
oup
Psyc
hoth
erap
y in
Man
aged
Car
e:Ba
sic
Econ
omic
Prin
cipl
es fo
rth
eCl
inic
alPr
actit
ione
r
1996
Eddy
, Dav
id
The
idea
that
ben
efit
lang
uage
is o
ne o
f the
mos
t im
porta
nt d
eter
min
ants
of t
he q
ualit
y an
d co
stof
care
is a
t the
cor
e of
this
pap
er. S
ampl
e la
ngua
ge is
sup
plie
d de
scrib
ing
heal
th in
terv
entio
n,m
edic
al c
ondi
tion,
hea
lth o
utco
mes
, suf
ficie
nt e
vide
nce,
and
cos
t effe
ctiv
enes
s. It
is n
oted
that
the
crite
ria a
re in
terc
onne
cted
and
poi
nts
to s
ome
of th
e sh
ortc
omin
gs o
f the
pro
pose
d la
ngua
ge.
JAM
ACl
inic
al D
ecis
ion
Mak
ing:
Fro
mTh
eory
toPr
actic
e. B
enef
itLa
ngua
ge:
Crite
ria T
hat W
illIm
prov
e Qu
ality
Whi
le R
educ
ing
Cost
s
Ap
pen
dix
A. C
on
tin
ued

Medical Necessity in Private Health Plans 83
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
1997
Mor
an, D
onal
dW
.Al
thou
gh th
ere
is g
row
ing
dem
and
for r
egul
atio
n of
the
man
aged
car
e in
dust
ry, r
egul
ator
y pr
opo-
nent
s ha
ve y
et to
arti
cula
te a
cle
ar th
eory
of r
egul
atio
n. M
ost o
bser
vers
ack
now
ledg
e co
nsum
erin
form
atio
n pr
oble
ms
that
regu
latio
n co
uld
addr
ess,
but
ther
e is
no
cons
ensu
s re
gard
ing
regu
la-
tion
of th
e br
oade
r pub
lic c
once
rn a
bout
rest
rictiv
e m
edic
al-n
eces
sity
det
erm
inat
ions
by
heal
thpl
ans.
Con
cern
s ab
out t
hese
issu
es—
whi
ch fa
ll w
ithin
the
gray
are
as o
f div
erge
nt c
linic
al o
pin-
ion—
may
be
diffi
cult
or im
poss
ible
to a
ddre
ss b
y ex
plic
it re
gula
tion.
If p
olic
ymak
ers
forb
ear o
nre
gula
tion
of m
edic
al n
eces
sity
det
erm
inat
ions
, priv
ate
mar
ket i
nnov
atio
n m
ay u
ltim
atel
y re
med
yth
is p
robl
em.
Heal
th A
ffairs
16(
6):7
–21
Fede
ral
Regu
latio
n of
Man
aged
Car
e:An
Impu
lse
inSe
arch
of a
Theo
ry?
1997
Jaco
bson
,Pe
terD
.,St
even
Asch
,Pe
ter A
.Gl
assm
an,
Kary
nE.
Mod
el,
and
John
B.
Hern
ande
z
This
pap
er re
ports
on
a qu
alita
tive
stud
y of
how
hea
lth c
are
prov
ider
s in
the
stat
es o
f Was
hing
ton
and
Oreg
on d
efin
e an
d im
plem
ent m
edic
al n
eces
sity
. Bas
ed o
n a
serie
s of
sem
i-stru
ctur
ed in
ter-
view
s, w
e fo
und
that
few
insu
rers
or h
ealth
car
e pl
ans
in o
ur s
ampl
e at
tem
pted
to re
solv
e th
eam
bigu
ities
inhe
rent
in d
efin
ing
med
ical
nec
essi
ty. M
ore
impo
rtant
ly, o
ur re
sults
sug
gest
that
phys
icia
ns in
man
aged
car
e pl
ans
wer
e no
t usi
ng g
ener
al d
efin
ition
s of
med
ical
nec
essi
ty to
mak
ecl
inic
al d
ecis
ions
, but
inst
ead
relie
d on
util
izatio
n m
anag
emen
t tec
hniq
ues
to g
uide
the
use
of m
edic
al re
sour
ces.
We
conc
lude
that
med
ical
nec
essi
ty a
s an
org
anizi
ng p
rinci
ple
for
clin
ical
pra
ctic
e de
cisi
on-m
akin
g is
like
ly to
con
tinue
to e
rode
in a
man
aged
car
e en
viro
nmen
t.
Inqu
iry 3
4:14
3–15
4De
finin
g an
dIm
plem
entin
gM
edic
alN
eces
sity
inW
ashi
ngto
n St
ate
and
Oreg
on
Ap
pen
dix
A. C
on
tin
ued
1998
Ande
rson
, G. F
.,an
d M
. A. H
all
OBJE
CTIV
ES: T
he a
utho
rs e
xam
ined
how
the
cour
ts h
ave
resp
onde
d to
pub
lic a
nd p
rivat
ein
sure
rs’ u
se o
f med
ical
app
ropr
iate
ness
crit
eria
to e
stab
lish
cove
rage
and
pay
men
t pol
icie
s.
MET
HODS
: A s
truct
ured
revi
ew o
f all
fede
ral a
nd s
tate
cou
rt he
alth
insu
ranc
e ca
ses
deci
ded
betw
een
1960
and
Jun
e 19
94 th
at in
volv
ed a
dis
pute
invo
lvin
g m
edic
al a
ppro
pria
tene
ss w
aspe
rform
ed. A
tota
l of 3
,215
pub
lishe
d co
urt d
ecis
ions
wer
e an
alyz
ed, o
f whi
ch 2
03 m
et th
ecr
iteria
of re
leva
nce
and
124
expl
icitl
y m
entio
ned
med
ical
app
ropr
iate
ness
crit
eria
. The
mai
nou
tcom
e va
riabl
e w
as w
heth
er th
e co
urt o
rder
ed th
e in
sure
r to
prov
ide
cove
rage
.
RESU
LTS:
In 1
85 c
ases
, ade
finiti
ve d
ecis
ion
was
rend
ered
, and
the
insu
rer w
as re
quire
dto
pay
in57
% o
f the
dec
isio
ns. W
heth
er th
e in
sure
r rel
ied
on a
n as
sess
men
t or n
ot, w
heth
erth
eas
sess
men
t pro
cess
was
form
al o
r inf
orm
al, a
nd w
ho c
ondu
cted
the
asse
ssm
ent d
idno
tapp
ear t
o in
fluen
ce c
ourts
’ dec
isio
ns, n
or d
id th
e sp
ecifi
city
of t
he c
over
age
excl
usio
n.Si
gnifi
cant
pre
dict
ors
of c
ourts
ord
erin
g co
vera
ge w
ere
cour
t jur
isdi
ctio
n, c
ontra
ct la
ngua
geas
sign
ing
disc
retio
n to
the
insu
rer,
seve
rity
of p
atie
nt’s
cond
ition
, and
whe
ther
the
treat
men
tap
pear
ed to
wor
k fo
r the
par
ticul
ar p
atie
nt.
CON
CLUS
ION
S:Fo
r pra
ctic
e gu
idel
ines
to b
e ac
cept
ed b
y th
e co
urts
, it i
s m
ore
impo
rtant
tofo
cus
on h
ow in
sura
nce
cont
ract
s ar
e w
ritte
n th
an o
n ho
w m
edic
al a
sses
smen
ts a
re p
erfo
rmed
.
Med
ical
Car
e36
(8):1
295–
1302
Whe
n Co
urts
Revi
ew M
edic
alAp
prop
riate
ness

Special Report84
1998
Mill
er, M
onic
aTh
e re
port
revi
ews
the
term
s ‘m
edic
al n
eces
sity
’ and
‘med
ical
ly n
eces
sary
car
e’ a
s th
ey a
redi
scus
sed
in N
ew Y
ork
case
law
. The
y co
nten
d th
at th
e ju
dici
al, c
ontra
ctua
l, an
d st
atut
ory
deve
lopm
ents
in N
ew Y
ork
crea
ted
a st
anda
rd o
f car
e th
at w
as lo
wer
than
the
negl
igen
cest
anda
rd.
Foun
datio
n fo
r the
Adva
ncem
ent o
fIn
nova
tive
Med
icin
eRe
port
Rese
arch
:Th
eDe
bate
Over
Med
ical
Nec
essi
ty in
Case
Law
and
Gove
rnm
ent/
Indu
stry
For
ums
1998
The
Nat
iona
lHe
alth
Law
Prog
ram
Prov
ides
NHe
LP’s
mod
el m
edic
al n
eces
sity
lang
uage
.Th
e N
atio
nal H
ealth
Law
Prog
ram
Rep
ort
Med
ical
Nec
essi
tyDe
finiti
onM
odel
Med
icai
dM
anag
ed C
are
Cont
ract
Prov
isio
ns
1998
Moh
l, Pa
ul C
. Le
tter f
rom
the
edito
r dis
cuss
ing
phys
icia
n cu
lpab
ility
in e
ngen
derin
g HM
Os a
nd m
edic
alne
cess
ity d
efin
ition
s.Ps
ychi
atric
Ser
vice
s49
(11)
:139
1M
edic
alN
eces
sity
:A
Mov
ing
Targ
et
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
1998
Ford
, Will
iam
Di
scus
ses
the
impa
ct o
f man
aged
car
e m
edic
al n
eces
sity
def
initi
ons
on p
sych
iatri
c ca
re.
Poin
tsto
som
e po
ssib
le re
ason
s w
hy B
HMOs
focu
s on
cut
ting
shor
t-ter
m c
osts
rath
er th
anm
anag
ing
long
-term
cos
ts, i
nclu
ding
sho
rt co
ntra
ct te
rms
and
labo
r-in
tens
ive
revi
ews.
Psyc
hiat
ric S
ervi
ces
49(2
):183
–184
Med
ical
Nec
essi
ty:
ItsIm
pact
inM
anag
ed M
enta
lHe
alth
Car
e
1998
Chod
off,
Paul
Man
aged
car
e an
d, s
peci
fical
ly, t
he n
eed
to c
onfo
rm to
med
ical
nec
essi
ty re
quire
men
ts h
ave
had
a dr
amat
ic e
ffect
on
the
med
ical
and
psy
chia
tric
prac
tice,
esp
ecia
lly o
n ps
ycho
ther
apy.
The
auth
or d
escr
ibes
the
prog
ress
ion
of th
e co
ncep
t of m
edic
al n
eces
sity
from
a s
impl
e ac
coun
ting
ofse
rvic
es re
imbu
rsab
le b
y in
sura
nce
com
pani
es to
an
ambi
guou
s te
rm w
ithou
t def
initi
onal
cons
ensu
s. H
e de
scrib
es it
s re
latio
nshi
p to
the
med
ical
mod
el a
nd d
iscu
sses
the
inco
ngru
itybe
twee
n m
edic
al n
eces
sity
and
cer
tain
asp
ects
of p
sych
othe
rapy
. He
prop
oses
a b
road
erco
ncep
t—he
alth
nec
essi
ty—
base
d on
an
eval
uatio
n of
the
adva
ntag
es, d
isad
vant
ages
, and
cost
sof
med
ical
and
psy
chia
tric
serv
ices
.
Psyc
hiat
ric S
ervi
ces
49(1
1):1
481–
1483
Med
ical
Nec
essi
ty a
ndPs
ycho
ther
apy
Ap
pen
dix
A. C
on
tin
ued
1998
Olso
n, K
risti
Disc
usse
s po
ssib
le c
onse
quen
ces
of u
sing
an
evid
ence
-bas
ed s
tand
ard
for d
eter
min
ing
med
ical
nece
ssity
. It p
oint
s to
the
fact
that
man
y co
mm
only
use
d pr
actic
es w
ill fa
il to
mee
t evi
denc
e-ba
sed
crite
ria. I
t als
o is
con
cern
ed th
at m
inor
ity g
roup
s, c
hild
ren,
and
wom
en, w
ho a
re h
isto
rical
lylim
ited
in a
cces
s to
car
e an
d tri
als,
will
suf
fer d
ispr
opor
tiona
tely
und
er e
vide
nce-
base
d cr
iteria
.
The
Nat
iona
l Hea
lthLa
wPr
ogra
m R
epor
tTh
e Th
reat
of
Evid
ence
-Bas
edDe
finiti
ons
ofM
edic
alN
eces
sity

Medical Necessity in Private Health Plans 85
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
Ap
pen
dix
A. C
on
tin
ued
1999
Berg
thol
d,Li
nda
A.Po
licy
pape
r dis
cuss
ing
the
prob
lem
s in
here
nt in
def
inin
g th
e te
rm “
med
ical
nec
essi
ty.”
She
poin
ts o
ut th
at th
e pr
oces
s by
whi
ch d
ecis
ions
are
mad
e is
far m
ore
impo
rtant
to u
nder
stan
dan
dim
prov
e th
an th
e te
rmin
olog
y us
ed to
des
crib
e th
ose
deci
sion
s, th
at th
ere
is s
ubst
antia
lva
riatio
n in
the
way
med
ical
nec
essi
ty is
def
ined
and
use
d in
priv
ate
cont
ract
, and
that
ther
eis
cons
ider
able
dis
crep
ancy
bet
wee
n co
ntra
ctua
l def
initi
ons
and
the
way
thos
e de
finiti
ons
are
appl
ied
in p
ract
ice.
Her
fina
l rec
omm
enda
tion
is th
at th
e Se
nate
not
def
ine
the
term
s in
sta
tute
.Ra
ther
they
sho
uld
appo
int a
bro
ader
gro
up o
f sta
keho
lder
s to
take
on
the
task
.
US S
enat
e Co
mm
ittee
onHe
alth
, Edu
catio
n,La
bor,
and
Pens
ions
Repo
rt
Test
imon
y to
the
US S
enat
eCo
mm
ittee
onHe
alth
,Ed
ucat
ion,
Lab
or,
and
Pens
ions
:M
edic
alN
eces
sity
:Fr
omTh
eory
toPr
actic
e
1998
Rose
nbau
m,
Sara
, et a
l.Co
ntai
ns c
ompi
led
list a
nd a
naly
sis
of m
edic
al n
eces
sity
def
initi
ons
cont
aine
d in
sta
te M
edic
aid
man
aged
car
e co
ntra
cts.
Cent
er fo
r Hea
lthSe
rvic
es R
esea
rch
and
Polic
y
Neg
otia
ting
the
New
Hea
lthCa
reSy
stem
: AN
atio
nwid
e St
udy
of M
edic
aid
Man
aged
Car
eCo
ntra
cts
1999
Berm
an, S
teve
BACK
GROU
ND:
Mor
e th
an 2
00 h
ealth
car
e po
licym
aker
s an
d re
sear
cher
s, c
linic
ians
, qua
lity
prof
essi
onal
s, a
nd o
ther
repr
esen
tativ
es o
f man
aged
car
e or
gani
zatio
ns, g
over
nmen
t, an
dac
adem
ia a
ttend
ed th
e fif
th a
nnua
l Bui
ldin
g Br
idge
s co
nfer
ence
, “Th
e He
alth
Car
e Pu
zzle
: Usi
ngRe
sear
ch to
Brid
ge th
e Ga
p Be
twee
n Pe
rcep
tion
and
Real
ity,”
in C
hica
go, A
pril
11–1
3, 1
999.
Spon
sore
d by
the
Amer
ican
Ass
ocia
tion
of H
ealth
Pla
ns a
nd th
e Ag
ency
for H
ealth
Car
e Po
licy
and
Rese
arch
—an
d no
w, t
he C
ente
rs fo
r Dis
ease
Con
trol a
nd P
reve
ntio
n—th
ese
annu
al c
onfe
r-en
ces
are
inte
nded
to p
rom
ote
rese
arch
in m
easu
ring
the
qual
ity a
nd e
ffect
iven
ess
of th
e se
rvic
eshe
alth
pla
ns p
rovi
de. S
elec
ted
plen
ary
sess
ions
from
the
conf
eren
ce a
re re
pres
ente
d in
this
repo
rt. K
EYN
OTE
ADDR
ESS:
“Th
ree
wor
thy
obje
ctiv
es”
for m
anag
ed c
are—
harm
onize
pra
ctic
egu
idel
ines
, dev
elop
evi
denc
e-ba
sed
co-p
ays
or p
rice
stru
ctur
e fo
r dru
gs, a
nd d
emys
tify
med
ical
nece
ssity
—w
ere
disc
usse
d. P
LEN
ARY:
A P
OPUL
ATIO
N H
EALT
H PE
RSPE
CTIV
E: P
opul
atio
n-ba
sed
care
is d
esig
ned
to id
entif
y ef
fect
ive
clin
ical
and
ser
vice
inte
rven
tions
and
ens
ure
thei
r effi
cien
tde
liver
y, id
entif
y in
effe
ctiv
e in
terv
entio
ns a
nd m
inim
ize
thei
r use
, and
mon
itor o
utco
mes
and
chan
ge p
ract
ice
if ou
tcom
es a
re s
ub-o
ptim
al. Y
et c
erta
in q
uest
ions
nee
d to
be
aske
d ab
out h
owto
put t
his
stra
tegy
in p
lace
, esp
ecia
lly, “
Why
sho
uld
any
indi
vidu
al o
r pot
entia
l pat
ient
be
will
ing
to b
e tre
ated
in a
pop
ulat
ion-
base
d de
liver
y sy
stem
?” T
HE F
INAN
CIAL
AN
D SC
IEN
TIFI
C EV
IDEN
CEBE
HIN
D PR
EVEN
TION
: The
con
cept
s of
sci
entif
ic e
vide
nce
and
finan
cial
evi
denc
e fo
r pre
vent
ion
wer
e re
view
ed a
nd a
pplie
d in
sce
nario
s of
the
effe
ctiv
enes
s an
d co
st-e
ffect
iven
ess
of s
elec
ted
prev
entiv
e ca
re s
ervi
ces.
Edu
catio
n ef
forts
are
nee
ded
to p
rom
ote
the
use
of e
ffect
ive
inte
rven
-tio
ns a
nd e
ncou
rage
que
stio
ning
of i
nter
vent
ions
with
unp
rove
n or
less
impo
rtant
effe
ctiv
enes
san
d po
or c
ost-e
ffect
iven
ess.
The
Join
t Com
mis
sion
Jour
nal o
n Qu
ality
Impr
ovem
ent 2
5(8)
:43
4–44
2
Mea
surin
g an
dIm
prov
ing
the
Qual
ity o
f Car
eof
Heal
th P
lans
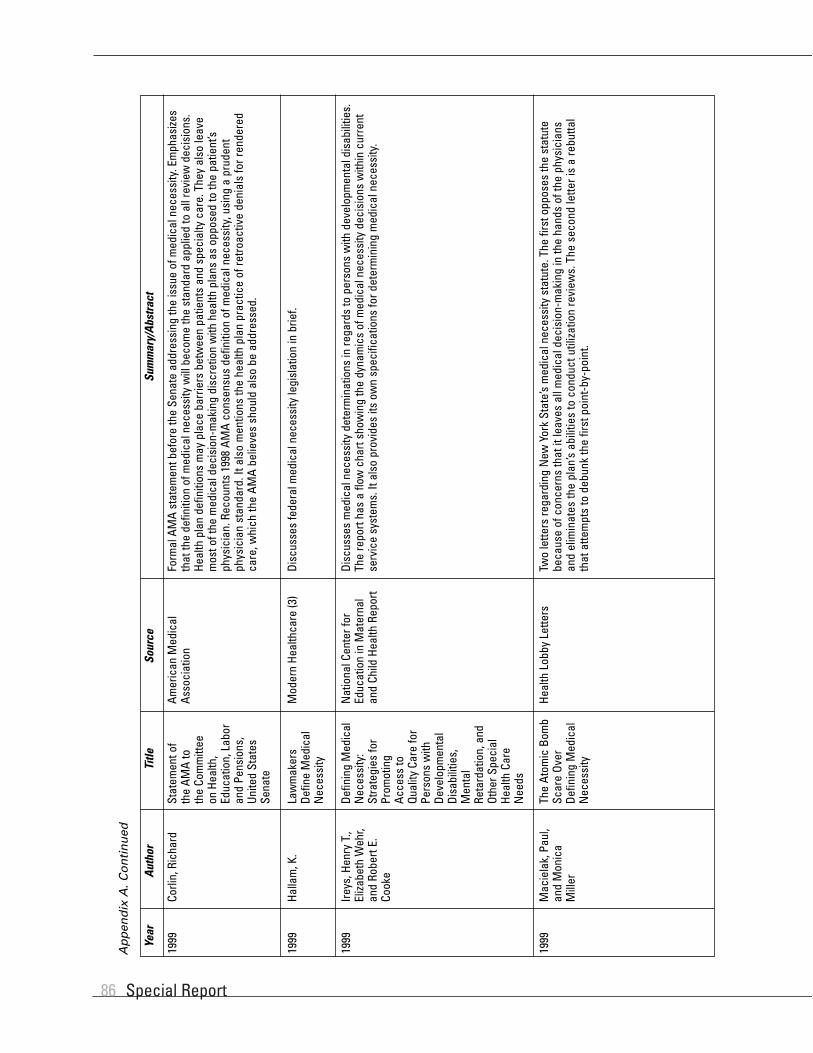
Special Report86
1999
Halla
m, K
.Di
scus
ses
fede
ral m
edic
al n
eces
sity
legi
slat
ion
in b
rief.
Mod
ern
Heal
thca
re (3
)La
wm
aker
sDe
fine
Med
ical
Nec
essi
ty
1999
Corli
n, R
icha
rdFo
rmal
AM
A st
atem
ent b
efor
e th
e Se
nate
add
ress
ing
the
issu
e of
med
ical
nec
essi
ty. E
mph
asize
sth
at th
e de
finiti
on o
f med
ical
nec
essi
ty w
ill b
ecom
e th
e st
anda
rd a
pplie
d to
all
revi
ew d
ecis
ions
.He
alth
pla
n de
finiti
ons
may
pla
ce b
arrie
rs b
etw
een
patie
nts
and
spec
ialty
car
e. T
hey
also
leav
em
ost o
f the
med
ical
dec
isio
n-m
akin
g di
scre
tion
with
hea
lth p
lans
as
oppo
sed
to th
e pa
tient
’sph
ysic
ian.
Rec
ount
s 19
98 A
MA
cons
ensu
s de
finiti
on o
f med
ical
nec
essi
ty, u
sing
a p
rude
ntph
ysic
ian
stan
dard
. It a
lso
men
tions
the
heal
th p
lan
prac
tice
of re
troac
tive
deni
als
for r
ende
red
care
, whi
ch th
e AM
A be
lieve
s sh
ould
als
o be
add
ress
ed.
Amer
ican
Med
ical
Asso
ciat
ion
Stat
emen
t of
the
AMA
toth
eCo
mm
ittee
onHe
alth
,Ed
ucat
ion,
Lab
oran
d Pe
nsio
ns,
Unite
d St
ates
Sena
te
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
Ap
pen
dix
A. C
on
tin
ued
1999
Ireys
, Hen
ry T
.,El
izabe
th W
ehr,
and
Robe
rt E.
Cook
e
Disc
usse
s m
edic
al n
eces
sity
det
erm
inat
ions
in re
gard
s to
per
sons
with
dev
elop
men
tal d
isab
ilitie
s.Th
e re
port
has
a flo
w c
hart
show
ing
the
dyna
mic
s of
med
ical
nec
essi
ty d
ecis
ions
with
in c
urre
ntse
rvic
e sy
stem
s. It
als
o pr
ovid
es it
s ow
n sp
ecifi
catio
ns fo
r det
erm
inin
g m
edic
al n
eces
sity
.
Nat
iona
l Cen
ter f
orEd
ucat
ion
in M
ater
nal
and
Child
Hea
lth R
epor
t
Defin
ing
Med
ical
Nec
essi
ty:
Stra
tegi
es fo
rPr
omot
ing
Acce
ss to
Qual
ityCa
re fo
rPe
rson
s w
ithDe
velo
pmen
tal
Disa
bilit
ies,
Men
tal
Reta
rdat
ion,
and
Othe
r Spe
cial
Heal
th C
are
Nee
ds
1999
Mac
iela
k, P
aul,
and
Mon
ica
Mill
er
Two
lette
rs re
gard
ing
New
Yor
k St
ate’
s m
edic
al n
eces
sity
sta
tute
. The
firs
t opp
oses
the
stat
ute
beca
use
of c
once
rns
that
it le
aves
all
med
ical
dec
isio
n-m
akin
g in
the
hand
s of
the
phys
icia
nsan
d el
imin
ates
the
plan
’s ab
ilitie
s to
con
duct
util
izatio
n re
view
s. T
he s
econ
d le
tter i
s a
rebu
ttal
that
atte
mpt
s to
deb
unk
the
first
poi
nt-b
y-po
int.
Heal
th L
obby
Let
ters
The
Atom
ic B
omb
Scar
e Ov
erDe
finin
g M
edic
alN
eces
sity

Medical Necessity in Private Health Plans 87
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
Ap
pen
dix
A. C
on
tin
ued
1999
Rose
nbau
m, S
., D.
Fra
nkfo
rd,
B. M
oore
, an
d P.
Bor
zi
In th
e au
thor
s’ v
iew
, an
insu
rer s
houl
d be
abl
e to
set
asi
de th
e re
com
men
datio
ns o
f a tr
eatin
gph
ysic
ian
only
in re
stric
ted
circ
umst
ance
s. D
ecis
ions
abo
ut c
over
age
shou
ld c
ontin
ue to
be
wei
ghed
aga
inst
clin
ical
ly a
ccep
ted
stan
dard
s of
med
ical
pra
ctic
e. A
n in
sure
r’s d
ecis
ion
shou
ldbe
law
ful o
nly
if th
e in
sure
r can
pro
ve th
at th
e de
cisi
on re
sts
on v
alid
and
relia
ble
evid
ence
that
isre
leva
nt to
a p
atie
nt’s
indi
vidu
al c
ircum
stan
ces.
The
aut
hors
adv
ocat
e ne
ither
a re
turn
to to
tal
auto
nom
y fo
r tre
atin
g ph
ysic
ians
in d
eter
min
ing
insu
ranc
e co
vera
ge n
or a
sys
tem
in w
hich
insu
rers
dec
ide
on c
over
age
acco
rdin
g to
crit
eria
that
are
tota
lly in
depe
nden
t of p
rofe
ssio
nal
stan
dard
s of
clin
ical
pra
ctic
e. R
athe
r, th
ey p
ropo
se m
aint
aini
ng th
e m
iddl
e po
sitio
n re
pres
ente
dby
cur
rent
law
. Thi
s m
iddl
e po
sitio
n re
quire
s in
sure
rs to
act
reas
onab
ly a
nd w
eigh
s th
e re
ason
-ab
lene
ss o
f the
ir co
nduc
t aga
inst
pro
fess
iona
l sta
ndar
ds o
f pra
ctic
e as
refle
cted
by
valid
and
relia
ble
evid
ence
.
The
New
Eng
land
Jour
nal o
f Med
icin
e34
0(3)
:229
–232
Who
Sho
uld
Dete
rmin
e W
hen
Heal
th C
are
IsM
edic
ally
Nec
essa
ry?
1999
Rovn
er, J
ulie
Di
scus
ses
the
gene
ral b
ackg
roun
d of
the
curr
ent m
edic
al n
eces
sity
deb
ate
in b
rief.
Busi
ness
and
Hea
lth (2
6)M
edic
alN
eces
sity
Tak
esCe
nter
Sta
ge
1999
Sing
er, S
ara
J.,
Lind
a A.
Berg
thol
d,Ca
rolV
orha
us,
Alai
n En
thov
en,
etal
.
This
is a
n in
-dep
th re
port
look
ing
into
the
ques
tion
of m
edic
al n
eces
sity
. It d
eals
with
the
vari-
atio
n an
d in
cons
iste
ncie
s of
def
initi
ons
that
the
vario
us s
take
hold
ers
have
. It n
otes
a p
auci
tyof
rese
arch
rega
rdin
g he
alth
pla
n de
cisi
on-m
akin
g an
d w
heth
er m
edic
al n
eces
sity
def
initi
ons
play
are
al ro
le in
dec
isio
n-m
akin
g. It
doc
umen
ts a
num
ber o
f con
fere
nces
and
orig
inal
rese
arch
,ev
entu
ally
con
clud
ing
with
a c
onse
nsus
for a
mod
el d
ecis
ion-
mak
ing
proc
ess
and
med
ical
nece
ssity
def
initi
ons.
It c
oncl
udes
by
revi
ewin
g th
e va
rious
sta
keho
lder
s, th
eir c
once
rns,
and
wha
t act
ions
they
cou
ld ta
ke to
dec
reas
e m
edic
al n
eces
sity
var
iabi
lity.
Stan
ford
Uni
vers
ityRe
port
Decr
easi
ngVa
riatio
nin
Med
ical
Nec
essi
tyDe
cisi
on M
akin
g
2000
Alle
n, K
athr
ynTh
is re
port
exam
ines
the
impl
emen
tatio
n an
d ef
fect
s to
dat
e of
the
fede
ral p
arity
law
, and
focu
ses
on: (
1) e
mpl
oyer
s’ c
ompl
ianc
e an
d th
e ch
ange
s m
ade
to th
eir h
ealth
ben
efit
plan
s, (2
) wha
t is
know
n ab
out t
he c
osts
of c
ompl
ying
with
the
law
, and
(3) t
he o
vers
ight
role
s of
HHS
and
DOL
inen
forc
ing
the
law
. In
brie
f, th
ey fo
und
that
mos
t em
ploy
ers
com
ply
with
the
law
; how
ever
, the
yha
ve b
ecom
e m
ore
rest
rictiv
e in
the
num
ber o
f hos
pita
l day
s or
out
patie
nt v
isits
cov
ered
for
men
tal h
ealth
whe
n co
mpa
red
with
trad
ition
al m
edic
al b
enef
its. F
ew e
mpl
oyer
s re
porte
d th
at th
ela
w h
as re
sulte
d in
hig
her c
osts
. Fin
ally
, the
rece
nt la
ws
have
exp
ande
d DO
L’s ro
le in
regu
latin
ghe
alth
ben
efits
.
Unite
d St
ates
Gen
eral
Acco
untin
g Of
fice
Repo
rt
Empl
oyer
s’M
enta
l Hea
lthBe
nefit
s Re
mai
nLi
mite
d De
spite
New
Fed
eral
Stan
dard
s

Special Report88
2000
Ford
, Will
iam
Th
e co
ncep
t of m
edic
al n
eces
sity
is a
pro
visi
on o
f com
mer
cial
insu
ranc
e co
ntra
cts
and
fede
ral
gove
rnm
ent M
edic
aid
requ
irem
ents
that
lim
its th
e pa
ymen
t to
only
thos
e se
rvic
es th
at a
re e
ssen
-tia
l for
trea
ting
a pe
rson
’s si
ckne
ss, i
njur
y, o
r con
ditio
n. T
he c
once
pt o
f med
ical
nec
essi
ty is
one
tool
use
d by
third
-par
ty p
ayer
s to
con
tain
thei
r fin
anci
al ri
sk in
a s
eem
ingl
y no
n-ar
bitra
ry m
anne
r.Al
so, t
he d
efin
ition
s of
med
ical
nec
essi
ty u
sed
by c
omm
erci
al in
sure
rs o
r by
the
fede
ral g
over
n-m
ent r
efle
ct th
eir p
rodu
ct’s
or p
rogr
am’s
philo
soph
ies.
Exp
andi
ng c
omm
erci
al in
sura
nce
orM
edic
aid
psyc
hiat
ric c
over
age
wou
ld re
quire
cha
ngin
g th
ose
philo
soph
ies.
As
long
as
soci
ety
isfa
ced
with
a g
reat
er d
eman
d fo
r hea
lth-r
elat
ed s
ervi
ce th
an re
sour
ces
to m
eet t
hem
, suc
hsy
stem
s of
ratio
ning
will
be
used
. Eve
n w
ith fu
ll pa
rity
for p
sych
iatri
c be
nefit
s, m
echa
nism
s w
illbe
used
by
paye
rs to
lim
it or
con
trol d
eman
d, th
ereb
y co
ntro
lling
fina
ncia
l ris
k. T
he s
hort-
term
chal
leng
e fo
r psy
chia
tric
advo
cate
s is
to s
ecur
e th
e m
ost a
ccep
tabl
e de
finiti
ons
of m
edic
alne
cess
ity fr
om th
ird-p
arty
pay
ers.
The
long
-term
cha
lleng
e fo
r MH/
SA a
dvoc
ates
and
for a
llhe
alth
care
adv
ocat
es, i
s to
dev
elop
a s
yste
m th
at p
ays
for t
he g
reat
est n
umbe
r of q
ualit
y se
r-vi
ces
for t
he g
reat
est n
umbe
r of p
eopl
e in
nee
d, in
an
affo
rdab
le m
anne
r, re
gard
less
of d
iagn
osis
.
Psyc
hiat
ric C
linic
sof
Nor
th A
mer
ica
23(2
):309
–317
Med
ical
Nec
essi
ty a
ndPs
ychi
atric
Man
aged
Car
e
2000
Heal
th In
sura
nce
Asso
ciat
ion
ofAm
eric
a
This
pol
icy
piec
e sc
ripte
d on
beh
alf o
f the
HIA
A hi
ghlig
hts
the
prob
lem
s of
allo
win
g m
edic
alne
cess
ity to
be
defin
ed b
y ph
ysic
ians
rath
er th
an in
sure
rs. E
ssen
tially
, it a
rgue
s th
at le
gisl
atio
nch
angi
ng th
e st
atus
quo
wou
ld: (
1) u
nder
min
e ut
iliza
tion
man
agem
ent a
nd in
crea
se c
osts
,(2
)enc
oura
ge fr
aud
and
abus
e, (3
) und
erm
ine
qual
ity a
nd p
erha
ps e
ven
expo
se p
atie
nts
toda
nger
, and
(4) u
nder
min
e co
ntra
ct la
w. I
n th
e en
d th
ey c
oncl
ude
that
pla
cing
det
erm
inat
ion
pow
ers
back
squa
rely
in th
e ha
nds
of p
rovi
ders
will
sim
ply
undo
all
the
prog
ress
mad
e in
hea
lthca
re s
ince
its
depa
rture
from
wid
espr
ead
fee-
for-
serv
ice
arra
ngem
ents
.
Heal
th In
sura
nce
Asso
ciat
ion
of A
mer
ica
Repo
rt
“Med
ical
Nec
essi
ty”
and
Heal
th P
lan
Cont
ract
s
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
2000
Flei
shm
an, M
artin
This
arti
cle
revi
ews
AMA’
s de
finiti
on o
f med
ical
nec
essi
ty a
nd p
oint
s ou
t pro
blem
s of
its
appl
ica-
tion
to p
sych
iatry
. It a
lso
reco
mm
ends
its
own
defin
ition
for p
sych
iatry
afte
r a d
iscu
ssio
n of
HIPA
Ala
w a
nd p
ossi
ble
impl
icat
ions
for f
raud
in p
sych
iatry
.
Psyc
hiat
ric S
ervi
ces
51(6
): 71
1–71
2, 7
19W
hat i
sPs
ychi
atric
“Med
ical
Nec
essi
ty”?
2000
Apga
r, Kr
iste
nRe
ason
erPr
epar
ed fo
r OPM
, thi
s re
port
desc
ribed
how
larg
e co
rpor
atio
ns w
ere
stru
ctur
ing
thei
r ins
uran
cepl
ans
in o
rder
to d
eal w
ith n
ew m
enta
l hea
lth p
arity
legi
slat
ion.
It d
iscu
sses
a ‘b
ig p
ictu
re’
appr
oach
, rep
orte
dly
focu
sing
on
keep
ing
empl
oyee
s he
alth
y an
d w
ell i
n or
der t
o av
oid
late
rpr
oble
ms
with
abs
ente
eism
, dis
abili
ty, a
nd lo
st p
rodu
ctiv
ity. E
ight
em
ploy
ers
wer
e st
udie
d:Am
eric
an A
irlin
es, A
T&T,
Delta
Airl
ines
, Eas
tman
Kod
ak, I
BM, G
ener
al M
otor
s, th
e M
assa
chus
etts
Grou
p In
sura
nce
Com
mis
sion
, and
Pep
siCo
. The
y hi
ghlig
ht w
hat t
hey
belie
ve to
be
esse
ntia
lm
echa
nism
s to
pro
vidi
ng p
arity
in c
are
as w
ell a
s id
entif
y pr
oble
mat
ic a
reas
. The
aut
hor
disc
usse
sth
e us
e of
man
aged
beh
avio
ral c
are
carv
e-ou
ts. T
he d
ocum
ent e
nds
by m
akin
gre
com
men
datio
ns re
gard
ing
how
OPM
sho
uld
stru
ctur
e fu
ture
insu
ranc
e pr
ogra
ms.
Offic
e of
Per
sonn
elM
anag
emen
t Rep
ort
Larg
e Em
ploy
erEx
perie
nces
and
Best
Pra
ctic
esin
Desi
gn,
Adm
inis
tratio
n,an
d Ev
alua
tion
ofM
enta
l Hea
lthan
d Su
bsta
nce
Abus
e Be
nefit
s:A
Look
at P
arity
in E
mpl
oyer
-Sp
onso
red
Heal
thBe
nefit
Pro
gram
s
Ap
pen
dix
A. C
on
tin
ued

Medical Necessity in Private Health Plans 89
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
2000
Hill,
Hug
h,An
nette
Han
son,
and
Bren
tO’
Conn
ell
This
repo
rt su
mm
arize
s a
sess
ion
that
eva
luat
ed th
e pr
oces
ses
for m
akin
g co
vera
ge d
ecis
ions
inpr
ivat
e, S
tate
, and
Fed
eral
ven
ues.
Hig
hmar
k Bl
ue C
ross
Blu
e Sh
ield
des
crib
es th
eir d
ecis
ion-
mak
ing
proc
ess,
bui
lt ar
ound
a c
ontra
ctua
l def
initi
on o
f ‘m
edic
al n
eces
sity
,’ w
hich
it p
rovi
des.
The
Mas
sach
uset
ts M
edic
aid
mod
el is
bas
ed o
n st
atut
ory
defin
ition
s of
med
ical
nec
essi
tyan
dev
iden
ce-b
ased
ass
essm
ents
of n
ew in
terv
entio
ns. H
CFA
is a
lso
desc
ribed
, dra
win
g its
auth
orita
tive
pow
ers
from
sec
tion
1862
of t
he S
ocia
l Sec
urity
Act
. Ser
vice
s or
tech
nolo
gies
that
fulfi
ll th
ecr
iteria
of t
he d
efin
ition
are
div
ided
into
55
stat
utor
ily d
efin
ed b
enef
it ca
tego
ries.
AHRQ
Use
r Lia
ison
Prog
ram
Rep
ort
Cove
rage
Deci
sion
s
2000
AMA
Priv
ate
Sect
or A
dvoc
acy
Grou
p
This
doc
umen
t con
tain
s th
e AM
A m
odel
def
initi
on o
f med
ical
nec
essi
ty a
nd d
iscu
sses
the
need
forp
rovi
ding
a d
efin
ition
that
refle
cts
a cl
inic
al d
eter
min
atio
n ra
ther
than
a b
usin
ess
dete
rmin
atio
n.
AMA
Priv
ate
Advo
cacy
Grou
p Re
port
Med
ical
Nec
essi
ty
Ap
pen
dix
A. C
on
tin
ued
2000
Land
au, M
orris
This
sho
rt br
iefin
g on
the
natu
re o
f the
cur
rent
diff
icul
ties
in d
efin
ing
med
ical
nec
essi
tyco
nclu
des
that
a c
ompr
ehen
sive
app
roac
h th
at d
iffer
s fro
m th
ird p
arty
ratio
ning
sho
uld
beus
edin
form
ing
ade
cisi
on.
Heal
th L
aw a
nd P
olic
yIn
stitu
te R
epor
tTh
e Di
fficu
lties
inDe
finin
g M
edic
alN
eces
sity
2000
Sabi
n, J
ames
,an
d N
orm
anDa
niel
s
This
arti
cle
disc
usse
s ps
ychi
atric
pro
blem
s w
ith m
edic
al n
eces
sity
def
initi
ons
and
expr
esse
sa
need
for ‘
psyc
hoso
cial
nec
essi
ty’ e
xpan
sion
. It r
evie
ws
Iow
a’s
expe
rienc
e w
ith m
anag
edbe
havi
oral
hea
lth c
are
and
prog
nost
icat
es th
at p
sych
iatri
sts
will
be
forc
ed to
opt
out
of t
heou
tpat
ient
trea
tmen
t of t
he s
ever
ely
men
tal i
ll du
e to
cur
rent
BHM
O po
licie
s.
Psyc
hiat
ric S
ervi
ces
51(4
):445
–459
Publ
ic-S
ecto
rM
anag
edBe
havi
oral
Heal
thCa
re:
V.Re
defin
ing
“Med
ical
Nec
essi
ty”—
The
Iow
a Ex
perie
nce
2000
Satc
her,
Davi
dTh
is c
ompr
ehen
sive
repo
rt gi
ves
deta
iled
back
grou
nd in
to m
any
face
ts o
f men
tal h
ealth
car
e.Ch
apte
r 6, “
Orga
nizin
g an
d Fi
nanc
ing
Men
tal H
ealth
Ser
vice
s,”
give
s an
in-d
epth
ana
lysi
s of
the
econ
omic
stru
ctur
e an
d co
sts
of m
oder
n m
enta
l hea
lth c
are
with
com
paris
ons
to tr
aditi
onal
med
ical
hea
lth c
are.
The
doc
umen
t als
o ex
amin
es th
e is
sue
of m
enta
l hea
lth p
arity
, loo
king
at
legi
slat
ive
trend
s an
d co
sts.
Thr
ough
out t
he d
ocum
ent,
how
ever
, the
re is
no
disc
ussi
on o
f men
tal
heal
th m
edic
al n
eces
sity
.
Unite
d St
ates
Publ
icHe
alth
Serv
ice
Repo
rt
Men
tal H
ealth
:A
Repo
rt of
the
Surg
eon
Gene
ral
2000
Amer
ican
Psyc
hSy
stem
sTh
is p
acke
t of m
ater
ials
sen
t to
psyc
hiat
ric p
rovi
ders
con
tain
s ne
wsl
ette
rs a
bout
rece
nt c
hang
es,
a co
mpl
ete
copy
of t
he u
pdat
ed U
tiliza
tion
Man
agem
ent c
riter
ia, a
nd a
cop
y of
pol
icie
s an
d pr
oce-
dure
s re
gard
ing
coor
dina
tion
of c
are
and
prov
ider
app
eals
. Med
ical
nec
essi
ty is
def
ined
in lo
ose
term
s fo
r eac
h co
nditi
on; h
owev
er, a
sep
arat
e se
t of a
dmis
sion
crit
eria
als
o m
ust b
e m
et p
rior t
oad
mitt
ing
a pa
tient
for a
psy
chia
tric
cond
ition
or c
ontin
uing
car
e fo
r a p
rotra
cted
per
iod
of ti
me.
Amer
ican
Psyc
hSy
stem
sPr
ovid
erPa
cket
Amer
ican
Psyc
hSy
stem
sPr
ovid
er P
acke
t

Special Report90
2001
Nat
iona
lCo
mm
ittee
forQ
ualit
yAs
sura
nce
Thes
e ar
e th
e pu
blis
hed
guid
elin
es u
sed
by N
CQA
to a
ccre
dit M
BHOs
. Def
initi
ons
of m
edic
alne
cess
ity a
re n
ot s
ugge
sted
by
NCQ
A; th
e M
BHOs
’ def
initi
ons
sim
ply
mus
t be
acce
ssib
le a
ndin
clud
e pr
oced
ures
for a
pply
ing
crite
ria b
ased
on
the
need
s of
indi
vidu
al p
atie
nts
and
char
acte
r-is
tics
of th
e lo
cal d
eliv
ery
syst
em. N
CQA
does
def
ine
med
ical
nec
essi
ty d
enia
l and
und
ersc
ores
the
need
for M
BHOs
to u
se c
linic
al p
ract
ice
guid
elin
es.
Nat
iona
l Com
mitt
eefo
rQua
lity
Assu
ranc
eM
BHO
Hand
book
Stan
dard
s an
dSu
rvey
orGu
idel
ines
for
the
Accr
edita
tion
of M
BHOs
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
2001
Eddy
, Dav
idTh
e au
thor
dis
cuss
es th
e us
e of
bal
ance
she
ets
and
evid
ence
-bas
ed m
edic
ine
for c
linic
alde
cisi
on-m
akin
g. H
e po
ints
to th
eir a
bilit
y to
sum
mar
ize in
one
pla
ce a
ll th
e cr
itica
l inf
orm
atio
nne
eded
to m
ake
deci
sion
s as
a g
reat
stre
ngth
.
Kais
er P
erm
anen
teRe
port
How
Evi
denc
e-Ba
sed
Bala
nce
Shee
ts C
an H
elp
Mak
e De
cisi
ons
2001
Clea
ry, P
atric
kLe
tter t
o Se
nato
r Gre
gg o
n be
half
of N
atio
nal A
ssoc
iatio
n of
Man
ufac
ture
s. T
he le
tter s
peak
s ou
tag
ains
t S 5
43, t
he M
enta
l Hea
lth E
quita
ble
Trea
tmen
t Act
of 2
001.
The
y ar
gue
that
the
new
bill
wou
ld g
reat
ly e
xpan
d th
e pa
rity
law
s of
199
6 an
d w
ould
hav
e m
any
draw
back
s. C
osts
wou
ldin
crea
se, w
hile
oth
er b
enef
its w
ould
be
redu
ced
to m
eet t
he b
ill’s
requ
irem
ents
. The
y ar
gue
that
ther
e ar
e no
dis
cern
able
lim
its to
the
scop
e of
pot
entia
l cov
erag
e. T
hey
also
voi
ce c
once
rn o
ver
the
bill’s
pre
empt
ion
prov
isio
ns th
at w
ould
pre
serv
e St
ate
legi
slat
ion
and
exte
nd it
to E
RISA
pla
ns.
Nat
iona
l Ass
ocia
tion
ofM
anuf
actu
rers
Let
ter
Bene
fit M
anda
tes
Ap
pen
dix
A. C
on
tin
ued
2001
Flei
shm
an, M
artin
This
arti
cle
cons
ider
s th
e di
fficu
lties
of a
pply
ing
med
ical
nec
essi
ty d
efin
ition
s, in
clud
ing
the
AMA-
APA
defin
ition
, to
the
uniq
ue n
eeds
of t
he fi
eld
of p
sych
iatry
. The
term
‘ fo
r con
veni
ence
’is
foun
d to
be
a po
tent
ial o
bsta
cle
to p
rovi
ding
psy
chia
tric
care
. The
pap
er a
lso
lam
ents
the
lack
ofa
spec
ified
role
for e
xter
nal c
ontri
butio
ns fr
om fa
mili
es, s
ocia
l wor
kers
, and
non
-pro
fess
iona
lca
reta
kers
. The
arti
cle
voic
es c
once
rn o
ver t
he H
IPAA
alte
ratio
ns th
at m
ake
pena
lizat
ion
ofpr
ovid
ers
for m
edic
al fr
aud.
It p
oint
s to
ste
eper
fine
s, u
ncle
ar d
efin
ition
s of
med
ical
nec
essi
tyas
its s
tand
ard,
and
the
fact
that
no
spec
ific
inte
nt to
def
raud
is n
eces
sary
.
Psyc
hiat
ric T
imes
XVI
II:3
Med
icat
ion
Man
agem
ent,
Med
ical
Nec
essi
ty a
ndRe
side
ntia
l Car
e
2001
CCD
Task
For
ceOf
fers
a p
ropo
sed
CCD
med
ical
nec
essi
ty d
efin
ition
and
dis
cuss
es th
e im
plic
atio
ns s
uch
defin
i-tio
ns c
an h
ave
on th
e di
sabl
ed. I
t dis
cuss
es th
e ne
ed to
fabr
icat
e pr
otec
tions
to e
nsur
e th
atpa
tient
s w
ith d
isab
ilitie
s ge
t the
car
e th
ey n
eed.
The
y po
int t
o a
need
to a
ddre
ss fu
nctio
nal a
bilit
yin
any
fina
l nec
essi
ty d
efin
ition
.
Cons
ortiu
m fo
r Citi
zens
with
Dis
abili
ties
Repo
rtA
Stro
ng a
ndCo
nsis
tent
Defin
ition
of
Med
ical
Nec
essi
ty F
orm
sth
e Co
re o
fM
eani
ngfu
lPa
tient
Prot
ectio
ns

Medical Necessity in Private Health Plans 91
2001
Join
t Com
mis
sion
on A
ccre
dita
tion
of H
ealth
Care
Orga
niza
tions
This
man
ual l
ays
out t
he v
ario
us ri
ghts
of t
he b
enef
icia
ries,
resp
onse
mec
hani
sms,
and
eth
ical
outlo
ok th
at J
CAHO
eva
luat
es in
det
erm
inin
g if
an o
rgan
izatio
n re
ceiv
es a
ccre
dita
tion.
The
guid
elin
es d
o no
t offe
r any
sta
ndar
ds fo
r med
ical
nec
essi
ty d
efin
ition
s, b
ut ra
ther
cle
arly
def
ine
stan
dard
s re
gard
ing
the
med
ical
dec
isio
n-m
akin
g pr
oces
s an
d in
form
atio
n di
ssem
inat
ion.
Join
t Com
mis
sion
onAc
cred
itatio
nof
Heal
thCa
reOr
gani
zatio
nsM
COHa
ndbo
ok
2001
-200
2Co
mpr
ehen
sive
Accr
edita
tion
Man
ual f
orHe
alth
Care
Net
wor
ks
Year
Auth
orTi
tleSo
urce
Sum
mar
y/Ab
stra
ct
2001
Regi
er, D
arre
lTh
is A
PA re
port
to th
e Se
nate
on
the
need
for m
enta
l hea
lth p
arity
legi
slat
ion
rein
forc
es c
urre
ntun
ders
tand
ings
of t
he s
cien
tific
bas
is u
nder
lyin
g th
e ca
usal
mec
hani
sms
of m
enta
l dis
orde
rsan
dpr
ovid
es e
vide
nce
that
par
ity in
sura
nce
cove
rage
is a
fford
able
, add
ress
es a
spe
cific
mar
ket
failu
re, a
nd c
an s
uppo
rt co
st-e
ffect
ive
treat
men
t to
redu
ce d
isab
ility
.
Amer
ican
Psy
chia
tryAs
soci
atio
n Re
port
Stat
emen
t of
APA
Exec
utiv
eDi
rect
or to
US
Sena
te H
ealth
,Ed
ucat
ion,
Lab
or,
and
Pens
ions
Com
mitt
ee o
n‘P
arity
for M
enta
lHe
alth
Tre
atm
ent’
2001
Havi
ghur
st, C
lark
The
auth
or re
view
s Ja
cobs
on’s
pres
enta
tion
entit
led
“Cos
t-Effe
ctiv
enes
s An
alys
is in
the
Cour
ts:
Rece
nt T
rend
s an
d Fu
ture
Pro
spec
ts.”
Of n
ote,
he
disc
usse
s m
akin
g co
ntra
cts
mor
e ex
plic
it w
ithre
gard
to th
e us
e of
CEA
in c
over
age
deci
sion
s. H
avig
hurs
t men
tions
the
poss
ibili
ties
of s
yste
mat
icm
isre
pres
enta
tion
of b
enef
its b
y in
sure
rs u
sing
this
tech
niqu
e.
Jour
nal o
f Hea
lthPo
litic
s, P
olic
y,an
dLa
w26
:2
Evid
ence
: Its
Mea
ning
s in
Heal
th C
are
and
in L
aw. S
umm
ary
of th
e 10
Apr
il20
00 IO
M a
ndAH
RQ W
orks
hop
Ap
pen
dix
A. C
on
tin
ued
2001
Sing
er, S
ara
J.,
and
Lind
a A.
Berg
thol
d
Prev
ious
rese
arch
has
sho
wn
cons
ider
able
var
iabi
lity
in th
e pr
oces
s an
d cr
iteria
use
d fo
r dec
isio
nm
akin
g in
bot
h pu
blic
and
priv
ate
plan
s re
gard
ing
med
ical
nec
essi
ty. T
his
pape
r see
ks to
doc
u-m
ent d
iffer
ence
s in
dec
isio
n-m
akin
g cr
iteria
and
to e
xpla
in th
e re
latio
nshi
p be
twee
n co
ntra
ctua
lde
finiti
ons
and
the
way
dec
isio
ns a
re m
ade
in p
ract
ice.
The
inve
stig
ator
s us
ed d
escr
iptio
ns o
f‘b
est p
ract
ices
’ and
‘una
ccep
tabl
e va
riatio
ns’ f
rom
hea
lth p
lan
inte
rvie
ws
to p
rovi
de in
sigh
t int
oho
w m
edic
al n
eces
sity
dec
isio
ns a
re m
ade.
The
y al
so p
rodu
ced
a m
odel
con
tract
ual d
efin
ition
and
deci
sion
-mak
ing
proc
ess
base
d on
bes
t-pra
ctic
e m
odel
s.
Heal
th A
ffairs
20(1
):200
–206
Pros
pect
s fo
rIm
prov
edDe
cisi
on M
akin
gAb
out M
edic
alN
eces
sity
2001
Stur
m, R
olan
d Re
sear
ch p
aper
del
ving
into
the
issu
e of
the
cost
for h
ealth
insu
rers
to im
plem
ent m
enta
l hea
lthpa
rity.
The
ir re
sults
sug
gest
that
par
ity in
em
ploy
er-s
pons
ored
hea
lth p
lans
is n
ot v
ery
cost
ly u
nder
com
preh
ensi
ve m
anag
ed c
are.
Als
o da
ta d
o no
t sup
port
excl
udin
g su
bsta
nce
abus
e fro
m p
arity
effo
rts d
ue to
pro
hibi
tive
cost
, bec
ause
dec
oupl
ing
men
tal h
ealth
and
sub
stan
ce a
buse
car
e in
term
s of
ben
efits
can
not s
ave
any
mea
ning
ful a
mou
nt. T
hese
resu
lts m
ay n
ot a
pply
to u
nman
aged
inde
mni
ty p
lans
, and
they
may
onl
y ho
ld fo
r lar
ge e
mpl
oyer
s bu
t not
for i
ndiv
idua
ls o
r for
sm
all
grou
ps b
uyin
g in
sura
nce.
RAN
D He
alth
Rep
ort
The
Cost
s of
Cove
ring
Men
tal
Heal
th a
ndSu
bsta
nce
Abus
eCa
re a
t the
Sam
eLe
vel a
s M
edic
alCa
re in
Priv
ate
Insu
ranc
e Pl
ans
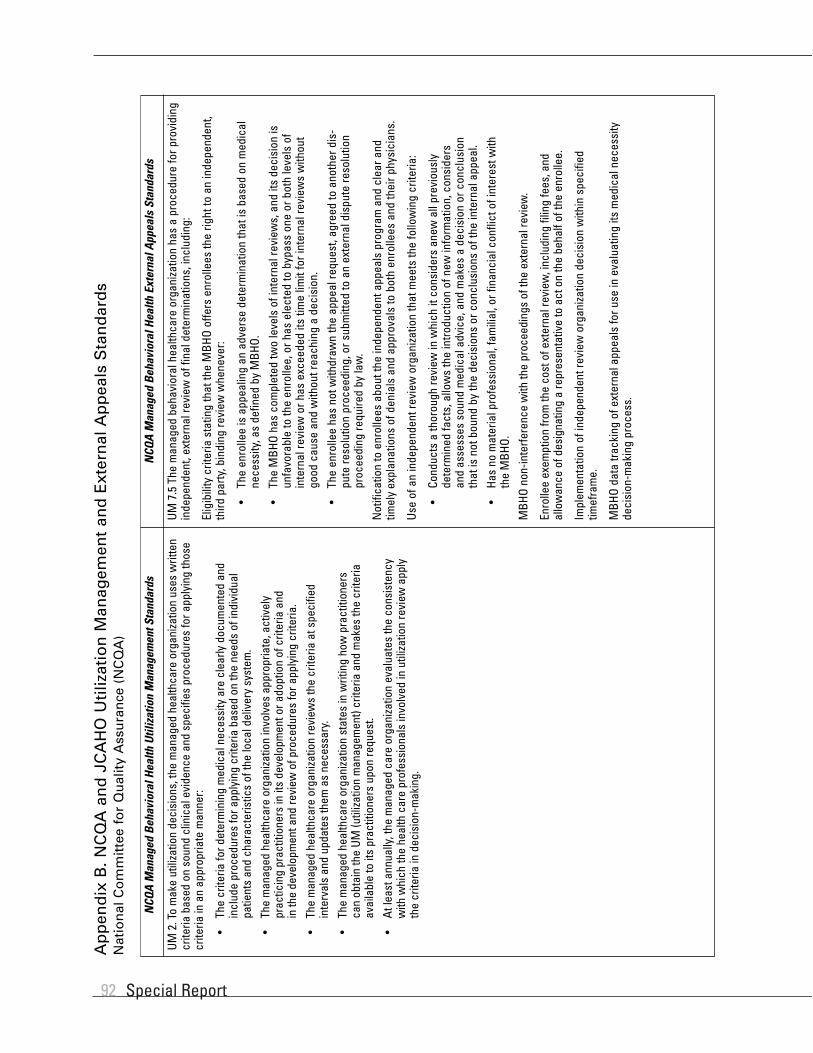
Special Report92
UM 2
. To
mak
e ut
iliza
tion
deci
sion
s, th
e m
anag
ed h
ealth
care
org
aniza
tion
uses
writ
ten
crite
ria b
ased
on
soun
d cl
inic
al e
vide
nce
and
spec
ifies
pro
cedu
res
for a
pply
ing
thos
ecr
iteria
in a
n ap
prop
riate
man
ner:
•Th
e cr
iteria
for d
eter
min
ing
med
ical
nec
essi
ty a
re c
lear
ly d
ocum
ente
d an
din
clud
e pr
oced
ures
for a
pply
ing
crite
ria b
ased
on
the
need
s of
indi
vidu
alpa
tient
s an
d ch
arac
teris
tics
of th
e lo
cal d
eliv
ery
syst
em.
•Th
e m
anag
ed h
ealth
care
org
aniza
tion
invo
lves
app
ropr
iate
, act
ivel
ypr
actic
ing
prac
titio
ners
in it
s de
velo
pmen
t or a
dopt
ion
of c
riter
ia a
ndin
the
deve
lopm
ent a
nd re
view
of p
roce
dure
s fo
r app
lyin
g cr
iteria
.
•Th
e m
anag
ed h
ealth
care
org
aniza
tion
revi
ews
the
crite
ria a
t spe
cifie
din
terv
als
and
upda
tes
them
as
nece
ssar
y.
•Th
e m
anag
ed h
ealth
care
org
aniza
tion
stat
es in
writ
ing
how
pra
ctiti
oner
sca
nob
tain
the
UM (u
tiliza
tion
man
agem
ent)
crite
ria a
nd m
akes
the
crite
riaav
aila
ble
to it
s pr
actit
ione
rs u
pon
requ
est.
•At
leas
t ann
ually
, the
man
aged
car
e or
gani
zatio
n ev
alua
tes
the
cons
iste
ncy
with
whi
ch th
e he
alth
car
e pr
ofes
sion
als
invo
lved
in u
tiliza
tion
revi
ew a
pply
the
crite
ria in
dec
isio
n-m
akin
g.
UM 7
.5 T
he m
anag
ed b
ehav
iora
l hea
lthca
re o
rgan
izatio
n ha
s a
proc
edur
e fo
r pro
vidi
ngin
depe
nden
t, ex
tern
al re
view
of f
inal
det
erm
inat
ions
, inc
ludi
ng:
Elig
ibili
ty c
riter
ia s
tatin
g th
at th
e M
BHO
offe
rs e
nrol
lees
the
right
to a
n in
depe
nden
t,th
ird p
arty
, bin
ding
revi
ew w
hene
ver:
•Th
e en
rolle
e is
app
ealin
g an
adv
erse
det
erm
inat
ion
that
is b
ased
on
med
ical
nece
ssity
, as
defin
ed b
y M
BHO.
•Th
e M
BHO
has
com
plet
ed tw
o le
vels
of i
nter
nal r
evie
ws,
and
its
deci
sion
isun
favo
rabl
e to
the
enro
llee,
or h
as e
lect
ed to
byp
ass
one
or b
oth
leve
ls o
fin
tern
al re
view
or h
as e
xcee
ded
its ti
me
limit
for i
nter
nal r
evie
ws
with
out
good
cau
se a
nd w
ithou
t rea
chin
g a
deci
sion
.
•Th
e en
rolle
e ha
s no
t with
draw
n th
e ap
peal
requ
est,
agre
ed to
ano
ther
dis
-pu
te re
solu
tion
proc
eedi
ng, o
r sub
mitt
ed to
an
exte
rnal
dis
pute
reso
lutio
npr
ocee
ding
requ
ired
by la
w.
Not
ifica
tion
to e
nrol
lees
abo
ut th
e in
depe
nden
t app
eals
pro
gram
and
cle
ar a
ndtim
ely
expl
anat
ions
of d
enia
ls a
nd a
ppro
vals
to b
oth
enro
llees
and
thei
r phy
sici
ans.
Use
of a
n in
depe
nden
t rev
iew
org
aniza
tion
that
mee
ts th
e fo
llow
ing
crite
ria:
•Co
nduc
ts a
thor
ough
revi
ew in
whi
ch it
con
side
rs a
new
all
prev
ious
lyde
term
ined
fact
s, a
llow
s th
e in
trodu
ctio
n of
new
info
rmat
ion,
con
side
rsan
das
sess
es s
ound
med
ical
adv
ice,
and
mak
es a
dec
isio
n or
con
clus
ion
that
is n
ot b
ound
by
the
deci
sion
s or
con
clus
ions
of t
he in
tern
al a
ppea
l.
•Ha
s no
mat
eria
l pro
fess
iona
l, fa
mili
al, o
r fin
anci
al c
onfli
ct o
f int
eres
t with
the
MBH
O.
MBH
O no
n-in
terfe
renc
e w
ith th
e pr
ocee
ding
s of
the
exte
rnal
revi
ew.
Enro
llee
exem
ptio
n fro
m th
e co
st o
f ext
erna
l rev
iew
, inc
ludi
ng fi
ling
fees
, and
allo
wan
ce o
f des
igna
ting
a re
pres
enta
tive
to a
ct o
n th
e be
half
of th
e en
rolle
e.
Impl
emen
tatio
n of
inde
pend
ent r
evie
w o
rgan
izatio
n de
cisi
on w
ithin
spe
cifie
dtim
efra
me.
MBH
O da
ta tr
acki
ng o
f ext
erna
l app
eals
for u
se in
eva
luat
ing
its m
edic
al n
eces
sity
deci
sion
-mak
ing
proc
ess.
NCQ
A M
anag
ed B
ehav
iora
l Hea
lth U
tiliz
atio
n M
anag
emen
t Sta
ndar
dsN
CQA
Man
aged
Beh
avio
ral H
ealth
Ext
erna
l App
eals
Sta
ndar
ds
Ap
pen
dix
B. N
CQ
A a
nd
JC
AH
O U
tiliz
atio
n M
anag
emen
t an
d E
xter
nal
Ap
pea
ls S
tan
dar
ds
Nat
ion
al C
om
mit
tee
for
Qu
alit
y A
ssu
ran
ce (
NC
QA
)

Medical Necessity in Private Health Plans 93
CC 1
: Hea
lth c
are
serv
ices
pro
vide
d di
rect
ly o
r by
arra
ngem
ent a
re a
ppro
pria
te:
•In
sco
pe to
mee
t the
hea
lth c
are
need
s of
the
popu
latio
n se
rved
.
•To
the
heal
th c
are
need
s, a
s in
fluen
ced
by s
ocio
-cul
tura
l cha
ract
eris
tics,
ofth
e po
pula
tion
serv
ed.
•To
the
netw
ork’s
mis
sion
.
•To
the
netw
ork’s
con
tract
ual o
blig
atio
ns.
CC 8
: Whe
n th
e ne
twor
k or
an
exte
rnal
ent
ity c
ondu
cts
a ut
iliza
tion
revi
ew o
f a li
cens
edin
depe
nden
t pra
ctiti
oner
’s or
a n
etw
ork
com
pone
nt’s
care
that
resu
lts in
den
ial o
fpa
ymen
t, de
cisi
ons
by th
e lic
ense
d in
depe
nden
t pra
ctiti
oner
or n
etw
ork
com
pone
ntre
gard
ing
ongo
ing
care
or d
isch
arge
are
bas
ed o
n th
e ca
re re
quire
d by
the
mem
ber’s
asse
ssed
nee
ds.
CC 8
.1: W
hen
utili
zatio
n re
view
resu
lts in
an
adve
rse
utili
zatio
n m
anag
emen
t dec
isio
n,th
e ne
twor
k pr
ovid
es th
e cr
iteria
for t
he d
ecis
ion
and
info
rmat
ion
rega
rdin
g ap
peal
toth
e lic
ense
d in
depe
nden
t pra
ctiti
oner
resp
onsi
ble
for t
he m
embe
r’s c
are.
JCAH
O pr
ovid
es e
xam
ples
of i
mpl
emen
tatio
n. “
Thes
e ex
ampl
es a
re s
impl
y id
eas
for
your
net
wor
k to
con
side
r.”
Exam
ple
of im
plem
enta
tion
for C
C 8:
The
netw
ork
requ
ests
the
revi
ew c
riter
ia u
sed
byan
y ex
tern
al e
ntity
that
car
ries
out a
util
izatio
n re
view
on
the
netw
ork’s
mem
bers
.Th
e re
view
crit
eria
are
mad
e av
aila
ble
to th
ose
with
in th
e ne
twor
k re
spon
sibl
e fo
rtre
atm
ent a
nd d
isch
arge
dec
isio
ns. W
hen
the
exte
rnal
util
izatio
n re
view
org
aniza
tion’
sre
com
men
datio
n co
nflic
ts w
ith th
e m
embe
r’s m
edic
al c
are
requ
irem
ents
, jus
tific
atio
nfo
r the
cou
rse
of a
ctio
n ta
ken
is d
ocum
ente
d. In
form
atio
n fro
m th
e ex
tern
al e
ntity
isco
llect
ed a
nd in
corp
orat
ed in
to th
e ne
twor
k’s a
sses
smen
t and
impr
ovem
ent a
ctiv
ities
.
RI 2
: The
net
wor
k pr
ovid
es fo
r mem
ber i
nvol
vem
ent i
n ca
re a
nd tr
eatm
ent d
ecis
ions
.
RI 2
.1: T
he n
etw
ork
prov
ides
an
auth
oriza
tion
proc
ess
for c
are
and
treat
men
t tha
t is
timel
y, e
ffici
ent,
and
mee
ts m
embe
r hea
lth c
are
need
s.
The
netw
ork’s
pro
cess
for a
utho
rizin
g ca
re a
nd tr
eatm
ent i
nclu
des:
•Pr
ovid
ing
mem
bers
with
a d
escr
iptio
n of
the
treat
men
t aut
horiz
atio
n pr
oces
s.
•Ha
ving
initi
al d
ecis
ions
mad
e by
an
appr
opria
tely
trai
ned
heal
th c
are
prof
essi
onal
usi
ng e
vide
nce-
base
d, n
etw
ork-
appr
oved
crit
eria
to a
utho
rize
adm
issi
on, c
are,
and
tran
sitio
n to
ano
ther
car
e se
tting
.
•Ha
ving
a p
hysi
cian
, den
tist,
or b
ehav
iora
l clin
icia
n re
view
all
initi
al tr
eatm
ent
auth
oriza
tion
deni
als
prio
r to
notif
ying
the
mem
ber o
r the
ir re
pres
enta
tive(
s)of
an
adve
rse
dete
rmin
atio
n.
RI 2
.2: T
he n
etw
ork
prov
ides
a m
etho
d fo
r res
olvi
ng d
isag
reem
ents
bet
wee
n th
ene
twor
k an
d th
e m
embe
r or d
esig
nate
d de
cisi
on m
aker
(s) r
egar
ding
car
e or
trea
tmen
tau
thor
izatio
n de
cisi
ons.
The
netw
ork’s
pro
cess
incl
udes
:
•In
form
ing
mem
bers
how
to s
eek
appe
als
of a
dver
se d
eter
min
atio
ns.
•De
fined
tim
efra
mes
in w
hich
the
mem
ber c
an a
ntic
ipat
e re
spon
se to
an
appe
al.
•Ap
peal
tim
efra
mes
that
are
app
ropr
iate
to th
e ur
genc
y of
the
mem
ber’s
heal
th c
are
need
s.
•An
app
eal r
evie
w p
anel
incl
udin
g he
alth
car
e pr
ofes
sion
als
who
are
app
ro-
pria
tely
trai
ned,
exp
erie
nced
, and
com
pete
nt w
ith re
spec
t to
the
care
and
treat
men
t inv
olve
d, a
nd w
ho w
ere
not i
nvol
ved
in th
e in
itial
det
erm
inat
ion.
•In
form
ing
mem
bers
abo
ut fu
rther
ste
ps a
vaila
ble
whe
n di
sagr
eem
ents
can
-no
t be
reso
lved
thro
ugh
the
treat
men
t aut
horiz
atio
n an
d ap
peal
pro
cess
,su
ch a
s an
inte
rnal
grie
vanc
e pr
oces
s, a
rbitr
atio
n, le
gal p
roce
edin
gs, a
ndan
y ot
her e
xter
nal r
evie
w p
roce
sses
.
RI 5
: The
net
wor
k pr
ovid
es fo
r the
rece
ipt a
nd re
solu
tion
of c
ompl
aint
s an
d gr
ieva
nces
from
mem
bers
in a
tim
ely
man
ner.
The
mem
ber h
as th
e rig
ht to
voi
ce c
ompl
aint
s w
ithou
t fea
r of r
ecrim
inat
ion
abou
t the
care
rece
ived
and
to h
ave
com
plai
nts
revi
ewed
and
, whe
neve
r pos
sibl
e, re
solv
ed.
This
right
and
the
way
it is
pro
tect
ed a
re e
xpla
ined
to th
e m
embe
r. Th
e ne
twor
k ha
sa
mea
ns o
f pro
vidi
ng fo
r the
follo
win
g:
•Pr
oced
ures
for r
egis
terin
g an
d m
anag
ing
com
plai
nts
and
grie
vanc
es,
incl
udin
g id
entif
ying
the
party
rece
ivin
g co
mpl
aint
s an
d gr
ieva
nces
.
•Ag
greg
atin
g an
d re
porti
ng a
ctio
ns ta
ken
on c
ompl
aint
s an
d gr
ieva
nces
.
•A
timel
y re
spon
se to
the
mem
ber,
subs
tant
ivel
y ad
dres
sing
the
actio
n ta
ken
on th
e co
mpl
aint
or g
rieva
nce.
•In
clud
ing
the
aggr
egat
e co
mpl
aint
and
grie
vanc
e in
form
atio
n in
per
form
ance
impr
ovem
ent a
ctiv
ities
.
•An
app
eal p
roce
ss fo
r grie
vanc
e de
cisi
ons.
•M
embe
r pro
tect
ion
from
any
san
ctio
ns o
r pen
altie
s re
sulti
ng s
olel
y or
prim
arily
from
usi
ng th
e co
mpl
aint
or g
rieva
nce
proc
ess.
JCAH
O Ut
iliza
tion
Man
agem
ent S
tand
ards
JCAH
O Ex
tern
al A
ppea
ls S
tand
ards
Ap
pen
dix
B. C
on
tin
ued
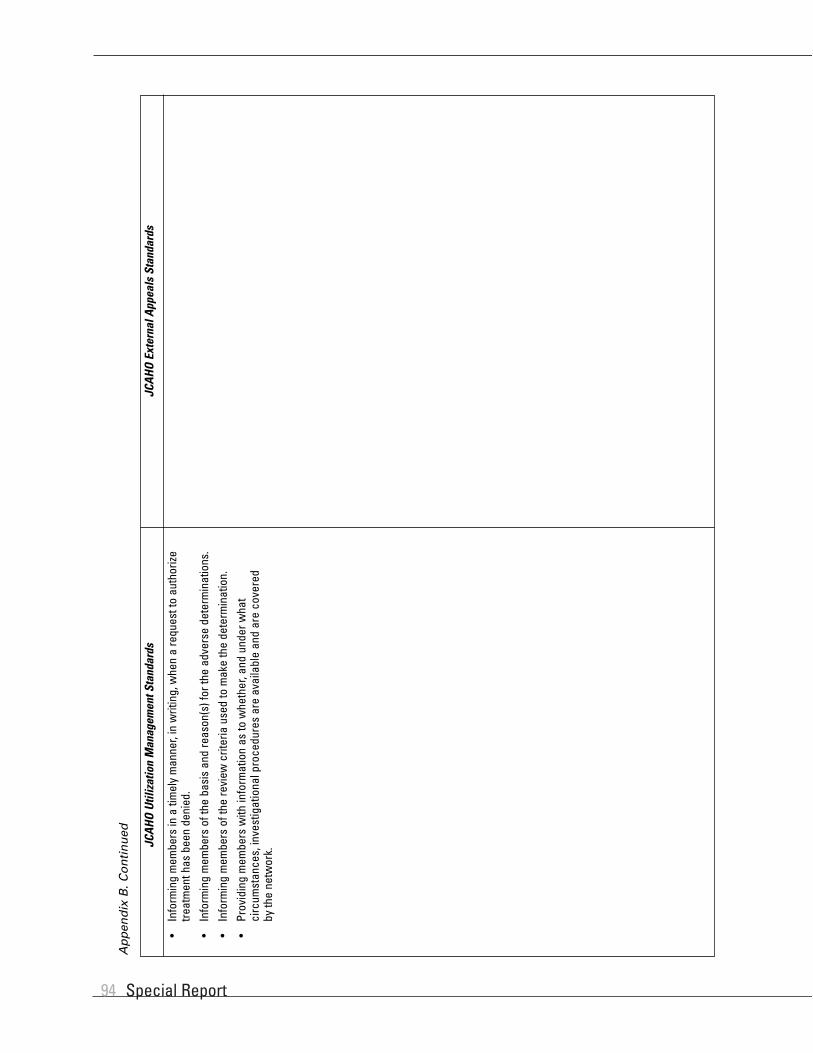
Special Report94
•In
form
ing
mem
bers
in a
tim
ely
man
ner,
in w
ritin
g, w
hen
a re
ques
t to
auth
orize
treat
men
t has
bee
n de
nied
.
•In
form
ing
mem
bers
of t
he b
asis
and
reas
on(s
) for
the
adve
rse
dete
rmin
atio
ns.
•In
form
ing
mem
bers
of t
he re
view
crit
eria
use
d to
mak
e th
e de
term
inat
ion.
•Pr
ovid
ing
mem
bers
with
info
rmat
ion
as to
whe
ther
, and
und
er w
hat
circ
umst
ance
s, in
vest
igat
iona
l pro
cedu
res
are
avai
labl
e an
d ar
e co
vere
dby
the
netw
ork.
JCAH
O Ut
iliza
tion
Man
agem
ent S
tand
ards
JCAH
O Ex
tern
al A
ppea
ls S
tand
ards
Ap
pen
dix
B. C
on
tin
ued

Medical Necessity in Private Health Plans 95
1996
Banc
roft
and
Banc
roft
v.Te
cum
seh
Prod
ucts
Soug
ht re
imbu
rsem
ent f
or b
reas
tre
duct
ion
surg
ery;
den
ied
onm
edic
al n
eces
sity
gro
unds
.
Cour
t fou
nd th
at P
lan
adm
inis
trato
rim
prop
erly
den
ied
bene
fits
in a
nar
bitra
ry a
nd c
apric
ious
man
ner.
Reve
rsed
.Ju
dgm
ent e
nter
ed fo
rth
e pl
aint
iff.
US D
istri
ct C
ourt
for t
he E
aste
rnDi
stric
t of
Mic
higa
n,So
uthe
rn D
ivis
ion
1999
Baue
r v. C
ount
ryLi
fe In
sura
nce
Soug
ht p
relim
inar
y an
d pe
rma-
nent
inju
nctio
n fo
r hig
h do
sech
emot
hera
py w
ith a
lloge
nic
bone
mar
row
tran
spla
nt a
fter
med
ical
nec
essi
ty d
enia
l.
Proc
edur
e fo
und
to b
e ex
perim
en-
tal a
nd th
us e
xclu
ded
from
the
polic
y. T
here
was
no
evid
ence
that
the
Plan
adm
inis
trato
r act
ed in
an
arbi
trary
or c
apric
ious
man
ner.
Affir
med
.Ju
dgm
ent e
nter
ed fo
rth
e Pl
an.
US D
istri
ct C
ourt
for N
orth
ern
Dist
rict o
f Illi
nois
1996
Bedr
ick
v.Tr
avel
ers
Insu
ranc
e
Appe
al o
f sum
mar
y ju
dgm
ent i
nfa
vor o
f Pla
n re
gard
ing
the
deni
alof
phy
sica
l, oc
cupa
tiona
l, an
dsp
eech
ther
apy
bene
fits.
On a
ppea
l, th
e co
urt f
ound
the
patie
nt d
id n
ot re
ceiv
e a
“ful
lan
dfa
ir” re
view
.
Reve
rsed
in p
art,
affir
med
in p
art.
Reve
rsed
judg
men
t in
rega
rds
to p
hysi
cal a
ndoc
cupa
tiona
l the
rapy
and
rem
ande
d w
ithin
stru
ctio
ns to
gra
ntsu
mm
ary
judg
men
t for
the
plai
ntiff
. Affi
rmed
all
othe
r asp
ects
of j
udg-
men
t, in
clud
ing
deni
alof
spee
ch b
enef
itssp
ecifi
cally
exc
lude
dun
der t
he c
ontra
ct.
US C
ourt
ofAp
peal
s,4t
hCi
rcui
t
1994
Blue
Cro
ss B
lue
Shie
ld o
f Virg
inia
v. K
elle
r
Appe
al o
f sum
mar
y ju
dgm
ent
awar
ded
to P
lan
rega
rdin
g de
nial
of b
enef
its o
n m
edic
al n
eces
sity
grou
nds.
Cour
t of A
ppea
ls fo
und
that
ther
ew
as n
o ev
iden
ce p
rese
nted
tosh
ow th
at th
e Pl
an a
buse
d its
disc
retio
n.
Affir
med
.Af
firm
ed lo
wer
cou
rt’s
sum
mar
y ju
dgm
ent.
Supr
eme
Cour
tof
Virg
inia
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C.
Liti
gat
ion
Reg
ard
ing
Med
ical
Nec
essi
ty D
efin
itio
ns
and
Pro
ced
ure
s (S
ort
ed b
y C
ase
Nam
e)
2001
Burr
ell v
. Uni
ted
Heal
th C
are
Insu
ranc
e
Mad
e ba
d fa
ith c
laim
rega
rdin
gde
nial
of c
over
age
of in
patie
ntst
ay fo
r pos
t-tra
umat
ic s
tress
diso
rder
. Pla
n ar
gued
that
refu
sal
was
bas
ed o
n bo
th m
edic
alne
cess
ity g
roun
ds a
s w
ell a
sin
elig
ible
trea
tmen
t fac
ility
.
Cour
t fou
nd th
at th
ere
was
no
clea
r evi
denc
e th
at th
e Pl
anac
ted
in a
n ar
bitra
ry o
r cap
ricio
usm
anne
r.
Affir
med
.Pa
rtial
sum
mar
y ju
dg-
men
t ent
ered
for P
lan.
US D
istri
ct C
ourt
for t
he E
aste
rnDi
stric
t of
Penn
sylv
ania

Special Report96
1996
Bush
man
v. S
tate
Mut
ual L
ife
Soug
ht in
junc
tion
in re
gard
sto
med
ical
nec
essi
ty d
enia
lof
high
-dos
e ch
emot
hera
pyan
dbo
ne m
arro
w tr
ansp
lant
.
Cour
t fou
nd th
at th
e po
licy
lang
uage
cle
arly
sta
ted
that
the
plai
ntiff
’s ill
ness
was
exc
lude
dfro
mco
vera
ge a
nd th
at th
e pl
aint
ifffa
iled
to s
how
that
the
Plan
act
edin
an
arbi
trary
and
cap
ricio
usm
anne
r.
Affir
med
.Su
mm
ary
judg
men
ten
tere
d fo
r the
Pla
n.US
Dis
trict
Cou
rtfo
r the
Nor
ther
nDi
stric
t of I
llino
is,
East
ern
Divi
sion
1993
Cam
elot
Car
e v.
Plan
ters
Life
save
rs
Soug
ht re
imbu
rsem
ent f
or c
are
deliv
ered
. Pla
n de
fined
pro
vide
ras
“pr
imar
ily”
a “c
usto
dial
car
e”fa
cilit
y an
d no
t a “
hosp
ital,”
and
ther
eby
expr
essl
y ex
clud
ed it
from
reim
burs
emen
t und
er th
ePl
an’s
cont
ract
.
Cour
t fou
nd th
at th
e su
mm
ary
Plan
desc
riptio
n de
fined
nei
ther
cus
to-
dial
nor
dom
icili
ary
care
that
was
excl
uded
from
cov
erag
e. It
foun
dth
e pr
ovid
er to
be
a ho
spita
l for
the
Plan
’s pu
rpos
es.
Reve
rsed
.Ju
dgm
ent e
nter
ed in
favo
r of p
lain
tiff.
US D
istri
ct C
ourt
for t
he N
orth
ern
Dist
rict o
f Illi
nois
,Ea
ster
n Di
visi
on
2000
Chem
acki
v.
Mei
jer,
Inc.
So
ught
reim
burs
emen
t for
imm
unot
hera
py a
nd a
llerg
yan
tigen
inje
ctio
ns a
fter m
edic
alne
cess
ity d
enia
l.
Clai
m fe
ll ou
tsid
e 1-
year
win
dow
follo
win
g de
nial
not
ifica
tion.
Pla
nad
min
istra
tor a
lso
was
foun
d no
tto
have
act
ed in
an
arbi
trary
and
capr
icio
us m
anne
r.
Affir
med
.Ju
dgm
ent e
nter
ed fo
rth
e Pl
an.
US D
istri
ct C
ourt,
Wes
tern
Dis
trict
of M
ichi
gan,
Sout
hern
Div
isio
n
1996
Cour
i v. G
uard
ian
Life
So
ught
den
tal b
enef
its d
enie
don
med
ical
nec
essi
ty g
roun
ds.
Plan
sou
ght s
umm
ary
judg
men
t.
Cour
t fou
nd th
at g
enui
ne is
sues
ofm
ater
ial f
act e
xist
ed re
gard
ing
whe
ther
the
insu
rer’s
act
ions
cons
titut
ed a
rbitr
ary
and
capr
i-ci
ous
cond
uct.
Reve
rsed
.Su
mm
ary
judg
men
t was
deni
ed.
US D
istri
ct C
ourt
for t
he N
orth
ern
Dist
rict o
f Illi
nois
,Ea
ster
n Di
visi
on
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C. C
on
tin
ued
1998
Croc
co v
. Xer
oxan
d Am
eric
anPs
ych
Man
agem
ent,
Inc.
Appe
al o
f jud
gmen
t in
favo
r of
plai
ntiff
rega
rdin
g th
e Pl
an’s
“ful
land
fair”
revi
ew g
uara
ntee
dun
der E
RISA
whe
n m
akin
gbe
nefit
det
erm
inat
ions
.
On a
ppea
l, th
e co
urt u
phel
d th
epr
evio
us ru
ling
that
the
Plan
’sad
min
istra
tor a
cted
in a
n ar
bitra
ryan
d ca
pric
ious
man
ner a
ndre
man
ded
the
case
for a
full
and
fair
revi
ew.
It al
so fo
und
that
Xero
x w
as n
ot th
e ad
min
istra
tor
in th
is c
ase,
dis
mis
sing
Xer
ox
from
the
suit.
Reve
rsed
.Af
firm
ed in
par
t,re
vers
ed in
par
t.US
Cou
rt of
Appe
als,
2nd
Circ
uit

Medical Necessity in Private Health Plans 97
1998
D’An
gelo
v.
Blue
Cros
sBl
ueSh
ield
of
Cent
ral N
ew Y
ork
Appe
al o
f jud
gmen
t in
favo
r of
plai
ntiff
rega
rdin
g be
nefit
s de
nied
on m
edic
al n
eces
sity
gro
unds
.Pl
an a
rgue
d th
at v
erdi
ct w
as n
otsu
ppor
ted
by le
gally
suf
ficie
ntev
iden
ce.
On a
ppea
l, th
e co
urt f
ound
that
the
evid
ence
was
lega
lly s
uffic
ient
.Re
vers
ed.
Affir
med
.Su
prem
e Co
urt
ofN
ew Y
ork,
Appe
llate
Divi
sion
, 3rd
Depa
rtmen
t
2000
Delm
arva
Hea
lthPl
an v
. Ace
to
Plan
sou
ght d
ecla
ratio
n th
at it
had
no d
uty
to p
rovi
de c
over
age
for a
lung
tran
spla
nt.
Cour
t fou
nd th
at th
e po
licy
did
not
expr
essl
y ex
clud
e th
e pr
oced
ure
and
that
a p
olic
yhol
der c
ould
reas
onab
ly e
xpec
t tha
t ser
vice
sne
cess
ary
to li
fe w
ould
be
prov
ided
.
Reve
rsed
.Su
mm
ary
judg
men
ten
tere
d fo
r Ace
to.
Cour
t of C
hanc
ery
of D
elaw
are,
New
Cast
le
1993
Dettm
er C
linic
v.
Asso
ciat
edIn
sura
nce
Chiro
prac
tor s
ough
t rei
mbu
rse-
men
t for
rend
ered
ser
vice
sde
nied
on
med
ical
nec
essi
tygr
ound
s.
Cour
t uph
eld
the
insu
rer’s
righ
t to
dete
rmin
e m
edic
al n
eces
sity
.Af
firm
ed.
Sum
mar
y ju
dgm
ent
awar
ded
to P
lan.
US D
istri
ct C
ourt
for t
he N
orth
ern
Dist
rict o
fIn
dian
a, S
outh
Bend
Div
isio
n
1992
Devi
lle N
ursi
ngSe
rvic
e v.
Met
ropo
litan
Life
Soug
ht re
imbu
rsem
ent f
or c
usto
-di
al c
are
serv
ices
den
ied
onm
edic
al n
eces
sity
gro
unds
.
Cour
t fou
nd th
at P
lan’
s co
ntra
ctua
lla
ngua
ge c
lear
ly s
tate
s th
at c
usto
-di
al c
are
is n
ot a
cov
ered
ser
vice
.Pl
an’s
deci
sion
was
not
arb
itrar
y or
capr
icio
us.
Affir
med
.Su
mm
ary
judg
men
ten
tere
d fo
r Pla
n.US
Dis
trict
Cou
rtfo
r the
Wes
tern
Dist
rict o
fLo
uisi
ana,
Lak
eCh
arle
s Di
visi
on
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C. C
on
tin
ued
1997
Dow
den
v. B
lue
Cros
s Bl
ue S
hiel
dof
Tex
as
Appe
al o
f sum
mar
y ju
dgm
ent i
nfa
vor o
f Pla
n re
gard
ing
the
deni
alof
exp
ense
s in
curr
ed in
trea
tmen
tof
sili
cone
bre
ast i
mpl
ant
com
plic
atio
ns.
On a
ppea
l, th
e co
urt a
ffirm
ed th
elo
wer
cou
rt’s
rulin
g, fi
ndin
g no
thin
gar
bitra
ry o
r cap
ricio
us in
the
deci
-si
on-m
akin
g pr
oces
s.
Affir
med
.Af
firm
ed.
US C
ourt
ofAp
peal
s,5t
hCi
rcui
t
1996
Esda
le v
.Am
eric
anCo
mm
unity
Mut
ual I
nsur
ance
Soug
ht b
enef
its fo
r hig
h-do
sech
emot
hera
py w
ith p
erip
hera
lst
em c
ell r
escu
e de
nied
on
med
ical
nec
essi
ty g
roun
dsas
expe
rimen
tal.
Plan
sou
ght
sum
mar
y ju
dgm
ent.
Cour
t fou
nd th
at e
vide
nce
pres
ente
d re
veal
ed th
at th
e ex
peri-
men
tal s
tatu
s of
the
treat
men
t was
uncl
ear i
n th
e lit
erat
ure.
Reve
rsed
.Su
mm
ary
judg
men
t was
deni
ed.
US D
istri
ct C
ourt
for t
he N
orth
ern
Dist
rict o
f Illi
nois
,Ea
ster
n Di
visi
on

Special Report98
1993
Evan
s v.
Blue
Cros
sBl
ueSh
ield
of
Sout
h Ca
rolin
a
Soug
ht re
imbu
rsem
ent f
or ra
dial
kera
toto
my
deni
ed o
n m
edic
alne
cess
ity g
roun
ds.
Cour
t fou
nd th
at th
e pr
oced
ure
did
not m
eet t
he re
quire
men
tsof
med
ical
nec
essi
ty s
et fo
rthby
the
cont
ract
.
Affir
med
.Ju
dgm
ent a
nd a
ttorn
ey’s
fees
aw
arde
d to
Pla
n.US
Dis
trict
Cou
rtfo
r the
Dis
trict
of
Sout
h Ca
rolin
a
1992
Farle
y v.
Bene
fitTr
ust L
ifeIn
sura
nce
Appe
al o
f jud
gmen
t in
favo
r of
Plan
rega
rdin
g th
e de
nial
of h
igh-
dose
che
mot
hera
py a
nd a
lloge
nic
bone
mar
row
tran
spla
nt o
nm
edic
al n
eces
sity
gro
unds
.
On a
ppea
l, th
e co
urt f
ound
that
th
e bu
rden
of p
roof
was
on
the
plai
ntiff
to s
how
that
the
proc
e-du
re w
as n
ot e
xper
imen
tal.
Affir
med
.Af
firm
ed.
US C
ourt
ofAp
peal
s,8t
hCi
rcui
t
1994
Feni
o v.
Mut
ualo
fOm
aha
Soug
ht p
relim
inar
y in
junc
tion
forh
igh-
dose
che
mot
hera
pyan
dal
loge
nic
bone
mar
row
trans
plan
t den
ied
on m
edic
alne
cess
ity g
roun
ds.
Cour
t fou
nd o
n re
view
of e
vide
nce
that
pat
ient
dem
onst
rate
d a
subs
tant
ial l
ikel
ihoo
d of
suc
cess
onth
e m
erits
.
Reve
rsed
.Pr
elim
inar
y in
junc
tion
orde
red
for p
lain
tiff.
US D
istri
ct C
ourt
for t
he S
outh
ern
Dist
rict o
f Flo
rida
1993
Flor
ence
Nig
htin
gale
Nur
sing
Ser
vice
v. B
lue
Cros
sBl
ue S
hiel
d of
Alab
ama
Soug
ht re
imbu
rsem
ent f
orse
rvic
es p
rovi
ded.
Pla
n ar
gued
that
ser
vice
s ch
arge
s w
ere
unre
ason
able
and
that
nur
sing
care
afte
r IV
rem
oval
was
not
med
ical
ly n
eces
sary
.
Cour
t fou
nd th
at th
e Pl
anad
min
istra
tor h
ad a
con
flict
of
inte
rest
that
tain
ted
his
judg
men
t.N
ursi
ngch
arge
s w
ere
foun
dto
bere
ason
able
.
Reve
rsed
.Pa
ymen
t aw
arde
d to
plai
ntiff
.US
Dis
trict
Cou
rtfo
r the
Nor
ther
nDi
stric
t of
Alab
ama,
Sout
hern
Div
isio
n
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C. C
on
tin
ued
1993
Fuja
v. B
enef
itTr
ust L
ife
Appe
al o
f jud
gmen
t in
favo
r of
plai
ntiff
rega
rdin
g th
e de
nial
of
“exp
erim
enta
l” c
ance
r the
rapy
on m
edic
al n
eces
sity
gro
unds
.
On a
ppea
l, th
e co
urt r
ever
sed
the
low
er c
ourt’
s in
terp
reta
tion
ofex
perim
enta
l, fin
ding
that
the
treat
men
t in
this
cas
e w
as c
lear
lyex
perim
enta
l.
Affir
med
.Re
vers
ed.
US C
ourt
ofAp
peal
s,7t
hCi
rcui
t
1995
Gret
he v
.Tr
ustm
ark
Insu
ranc
e
Soug
ht p
relim
inar
y in
junc
tion
and
bene
fits
for h
igh-
dose
chem
othe
rapy
and
allo
geni
cbo
nem
arro
w tr
ansp
lant
den
ied
on m
edic
al n
eces
sity
gro
unds
.
The
cour
t, af
ter d
e no
vo re
view
,fo
und
that
the
plai
ntiff
had
not
met
her b
urde
n of
est
ablis
hing
that
the
prop
osed
trea
tmen
tm
etal
lthe
crit
eria
for m
edic
alne
cess
ity a
s de
fined
by
the
polic
y.
Affir
med
.Pr
elim
inar
y in
junc
tion
was
den
ied.
US D
istri
ct C
ourt
for t
he N
orth
ern
Dist
rict o
f Illi
nois
,Ea
ster
n Di
visi
on
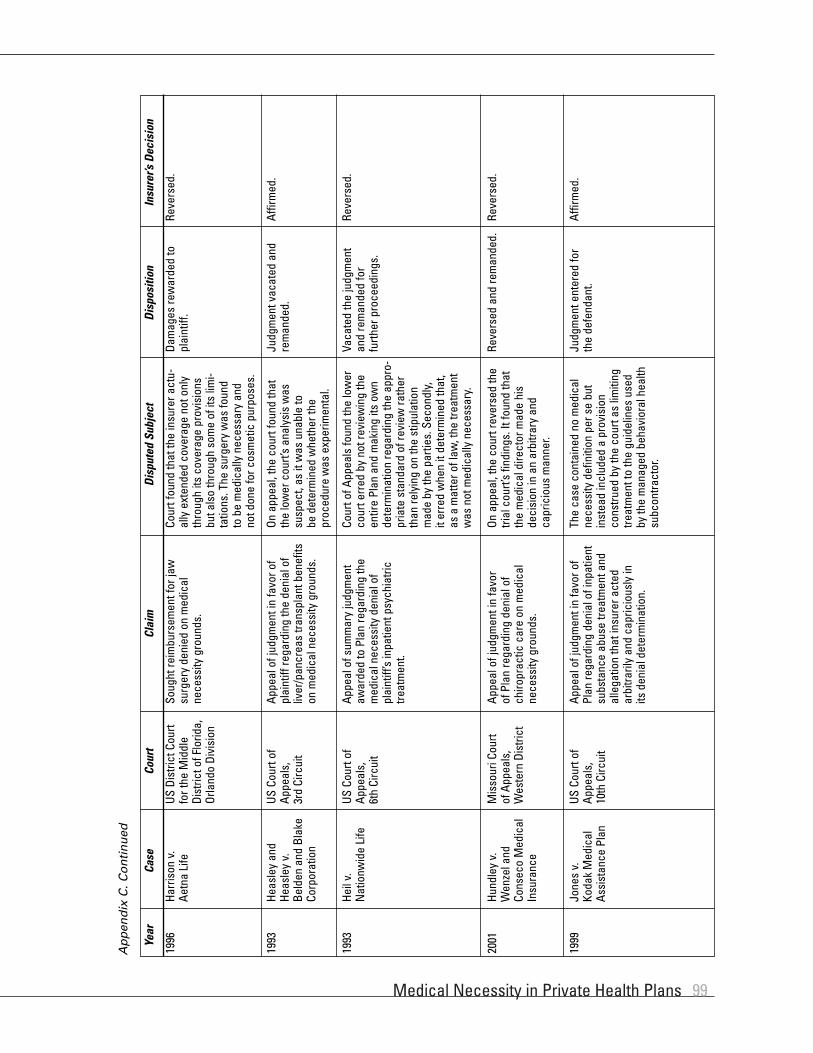
Medical Necessity in Private Health Plans 99
1996
Harr
ison
v.
Aetn
aLi
feSo
ught
reim
burs
emen
t for
jaw
surg
ery
deni
ed o
n m
edic
alne
cess
ity g
roun
ds.
Cour
t fou
nd th
at th
e in
sure
r act
u-al
ly e
xten
ded
cove
rage
not
onl
yth
roug
h its
cov
erag
e pr
ovis
ions
buta
lso
thro
ugh
som
e of
its
limi-
tatio
ns. T
he s
urge
ry w
as fo
und
tobe
med
ical
ly n
eces
sary
and
notd
one
for c
osm
etic
pur
pose
s.
Reve
rsed
.Da
mag
es re
war
ded
topl
aint
iff.
US D
istri
ct C
ourt
for t
he M
iddl
eDi
stric
t of F
lorid
a,Or
land
o Di
visi
on
1993
Heas
ley
and
Heas
ley
v.Be
lden
and
Blak
eCo
rpor
atio
n
Appe
al o
f jud
gmen
t in
favo
r of
plai
ntiff
rega
rdin
g th
e de
nial
of
liver
/pan
crea
s tra
nspl
ant b
enef
itson
med
ical
nec
essi
ty g
roun
ds.
On a
ppea
l, th
e co
urt f
ound
that
the
low
er c
ourt’
s an
alys
is w
assu
spec
t, as
it w
as u
nabl
e to
bede
term
ined
whe
ther
the
proc
edur
ew
as e
xper
imen
tal.
Affir
med
.Ju
dgm
ent v
acat
ed a
ndre
man
ded.
US C
ourt
ofAp
peal
s,3r
dCi
rcui
t
1993
Heil
v.N
atio
nwid
e Li
fe
Appe
al o
f sum
mar
y ju
dgm
ent
awar
ded
to P
lan
rega
rdin
g th
em
edic
al n
eces
sity
den
ial o
fpl
aint
iff’s
inpa
tient
psy
chia
tric
treat
men
t.
Cour
t of A
ppea
ls fo
und
the
low
erco
urt e
rred
by
not r
evie
win
g th
een
tire
Plan
and
mak
ing
its o
wn
dete
rmin
atio
n re
gard
ing
the
appr
o-pr
iate
sta
ndar
d of
revi
ew ra
ther
than
rely
ing
on th
e st
ipul
atio
nm
ade
by th
e pa
rties
. Sec
ondl
y,it
erre
d w
hen
it de
term
ined
that
,as
am
atte
r of l
aw, t
he tr
eatm
ent
was
not
med
ical
ly n
eces
sary
.
Reve
rsed
.Va
cate
d th
e ju
dgm
ent
and
rem
ande
d fo
rfu
rther
pro
ceed
ings
.
US C
ourt
ofAp
peal
s,6t
hCi
rcui
t
2001
Hund
ley
v.W
enze
l and
Cons
eco
Med
ical
Insu
ranc
e
Appe
al o
f jud
gmen
t in
favo
rof
Plan
rega
rdin
g de
nial
of
chiro
prac
tic c
are
on m
edic
alne
cess
itygr
ound
s.
On a
ppea
l, th
e co
urt r
ever
sed
the
trial
cou
rt’s
findi
ngs.
It fo
und
that
the
med
ical
dire
ctor
mad
e hi
sde
cisi
on in
an
arbi
trary
and
capr
icio
us m
anne
r.
Reve
rsed
.Re
vers
ed a
nd re
man
ded.
Mis
sour
i Cou
rtof
Appe
als,
Wes
tern
Dis
trict
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C. C
on
tin
ued
1999
Jone
s v.
Koda
kM
edic
alAs
sist
ance
Pla
n
Appe
al o
f jud
gmen
t in
favo
r of
Plan
rega
rdin
g de
nial
of i
npat
ient
subs
tanc
e ab
use
treat
men
t and
alle
gatio
n th
at in
sure
r act
edar
bitra
rily
and
capr
icio
usly
inits
deni
al d
eter
min
atio
n.
The
case
con
tain
ed n
o m
edic
alne
cess
ity d
efin
ition
per
se
but
inst
ead
incl
uded
a p
rovi
sion
cons
trued
by
the
cour
t as
limiti
ngtre
atm
ent t
o th
e gu
idel
ines
use
dby
the
man
aged
beh
avio
ral h
ealth
subc
ontra
ctor
.
Affir
med
.Ju
dgm
ent e
nter
ed fo
rth
e de
fend
ant.
US C
ourt
ofAp
peal
s,10
thCi
rcui
t

Special Report100
1999
Hunt
er v
. W
al-M
art S
tore
s So
ught
reim
burs
emen
t for
hyst
erec
tom
y tw
ice
deni
edby
Plan
on
med
ical
nec
essi
tygr
ound
s.
Plan
adm
inis
trato
r fou
nd to
hav
eab
used
his
dis
cret
ion
beca
use
the
invo
lved
phy
sici
ans
dete
rmin
edth
at th
e op
erat
ion
was
not
the
next
ther
apeu
tic s
tep,
rath
er th
ande
term
inin
g th
at th
e op
erat
ion
was
not m
edic
ally
nec
essa
ry.
Reve
rsed
.Ju
dgm
ent e
nter
ed fo
rpl
aint
iff.
US D
istri
ct C
ourt
for t
he E
aste
rnDi
stric
t of
Arka
nsas
,W
este
rn D
ivis
ion
2000
Julia
no v
. HM
Oof
New
Jer
sey
Appe
al o
f jud
gmen
t for
reim
-bu
rsem
ent f
or h
ome
nurs
ing
care
deni
ed o
n m
edic
al n
eces
sity
grou
nds.
Pla
n ar
gued
that
its
disc
retio
n al
low
s fo
r it t
o of
fer
care
at s
kille
d nu
rsin
g fa
cilit
ies
and
that
priv
ate
care
was
not
med
ical
ly n
eces
sary
.
Initi
al c
ourt
foun
d th
at th
e ra
tes
ofho
me
nurs
ing
wer
e ac
tual
ly le
ssth
an th
at o
f the
ski
lled
nurs
ing
faci
lity.
On
appe
al, t
he c
ourt
foun
dth
at a
dditi
onal
pro
ceed
ings
wer
ene
eded
to a
sses
s da
mag
es.
Reve
rsed
.Va
cate
d an
d re
man
ded.
US C
ourt
ofAp
peal
s,2n
dCi
rcui
t
1998
Killi
an a
nd K
illia
nv.
Hea
lthSo
urce
Ap
peal
of j
udgm
ent c
iting
arb
i-tra
ry a
nd c
apric
ious
beh
avio
rby
Plan
in re
gard
s to
den
ial o
fbr
east
can
cer t
reat
men
t on
med
ical
nec
essi
ty g
roun
ds.
On a
ppea
l, co
urt f
ound
the
Plan
tobe
arb
itrar
y an
d ca
pric
ious
inco
nsid
erin
g ad
ditio
nal e
vide
nce
afte
r dea
dlin
es, b
ut n
ot s
o in
mak
ing
its d
eter
min
atio
n.
Affir
med
.Ca
se w
as a
ffirm
ed in
part,
reve
rsed
in p
art,
and
rem
ande
d fo
rfu
rther
pro
ceed
ings
.
US C
ourt
ofAp
peal
s,6t
hCi
rcui
t
1993
Koen
ig v
.M
etro
polit
an L
ife
Soug
ht re
imbu
rsem
ent f
orsu
bsta
nce
abus
e ca
re d
enie
d by
Plan
. Pla
n ar
gued
that
pla
intif
fdi
dno
t exh
aust
inte
rnal
rem
edie
s.
The
cour
t fou
nd th
at th
e ev
iden
cesh
owed
that
con
tinue
d in
tern
alap
peal
atte
mpt
s w
ould
hav
epr
oven
futil
e an
d us
eles
s.
Reve
rsed
.Pl
an’s
mot
ion
to d
ism
iss
the
case
was
den
ied.
US D
istri
ct C
ourt
for t
he N
orth
ern
Dist
rict o
f Illi
nois
,Ea
ster
n Di
visi
on
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C. C
on
tin
ued
1992
Lehm
an v
.M
utua
lof O
mah
a So
ught
reim
burs
emen
t for
hig
h-do
se c
hem
othe
rapy
and
allo
geni
cbo
ne m
arro
w tr
ansp
lant
den
ied
on m
edic
al n
eces
sity
gro
unds
.
Cour
t fou
nd a
fter d
e no
vo re
view
that
the
evid
ence
pre
sent
edsu
gges
ted
that
the
proc
edur
e w
asex
perim
enta
l and
, the
refo
re, n
otco
vere
d un
der t
he P
lan’
s co
ntra
ct.
Affir
med
.Ju
dgm
ent e
nter
ed fo
rth
e Pl
an.
US D
istri
ct C
ourt
for t
he D
istri
ct o
fAr
izona
1999
Lew
is v
.Tr
ustm
ark
Insu
ranc
e
Appe
al o
f sum
mar
y ju
dgm
ent i
nfa
vor o
f Pla
n re
gard
ing
deni
alof
bene
fits
for h
igh-
dose
chem
othe
rapy
and
allo
geni
cbo
nem
arro
w tr
ansp
lant
on
med
ical
nec
essi
ty g
roun
ds.
On a
ppea
l, th
e co
urt w
as u
nabl
eto
conc
lude
that
the
Plan
was
unre
ason
able
in th
eir i
nter
pre-
tatio
nof
the
polic
y.
Affir
med
.Af
firm
ed.
US C
ourt
ofAp
peal
s,4t
hCi
rcui
t

Medical Necessity in Private Health Plans 101
1992
Man
n v.
Prud
entia
lIn
sura
nce
Soug
ht b
enef
its fo
r ute
rine
mon
itorin
g se
rvic
es d
enie
don
med
ical
nec
essi
ty g
roun
dsas
spec
ifica
lly e
xclu
ded.
Cour
t fou
nd th
at th
e pl
aint
ifffa
iled
to p
rovi
de e
vide
nce
that
the
Plan
’s de
cisi
on w
as a
rbitr
ary
orca
pric
ious
.
Affir
med
.Su
mm
ary
judg
men
ten
tere
d fo
r Pla
n.US
Dis
trict
Cou
rtfo
r the
Sou
ther
nDi
stric
t of F
lorid
a
1996
Mau
ne v
.In
tern
atio
nal
Brot
herh
ood
ofEl
ectri
cal
Wor
kers
Appe
al o
f sum
mar
y ju
dgm
ent i
nfa
vor o
f Pla
n re
gard
ing
the
deni
alof
ben
efits
for b
reas
t im
plan
tre
mov
al.
On a
ppea
l, th
e co
urt u
phel
d th
efin
ding
that
the
proc
edur
e w
asno
tmed
ical
ly n
eces
sary
. The
cour
tfou
nd th
e ca
se n
ot tr
ivia
l,re
vers
ing
the
lega
l fee
rulin
gs.
Affir
med
.Af
firm
ed in
par
t,re
vers
ed in
par
t.US
Cou
rt of
Appe
als,
8th
Circ
uit
1992
McG
ee v
.Eq
uico
r-Eq
uita
ble
HCA
Appe
al o
f jud
gmen
t in
favo
rof
Plan
rega
rdin
g de
nial
of
reha
bilit
ativ
e ca
re o
n m
edic
alne
cess
ity g
roun
ds.
On a
ppea
l, th
e co
urt a
ffirm
ed th
atth
e pa
tient
’s tra
nsfe
r sev
ered
rela
-tio
ns w
ith P
lan
phys
icia
ns a
ndpr
even
ted
the
Plan
from
mak
ing
nece
ssar
y pr
edet
erm
inat
ions
of
impr
ovem
ent a
s re
quire
d by
cont
ract
.
Affir
med
.Af
firm
ed.
US C
ourt
ofAp
peal
s,10
thCi
rcui
t
1998
McG
raw
v.
Prud
entia
lIn
sura
nce
Appe
al o
f sum
mar
y ju
dgm
ent i
nfa
vor o
f Pla
n re
gard
ing
the
deni
alof
phy
sica
l the
rapy
ben
efits
on
med
ical
nec
essi
ty g
roun
ds.
On a
ppea
l, th
e co
urt a
ffirm
edth
atER
ISA
gove
rned
act
ion
and
reve
rsed
con
clus
ion
that
den
ial
ofbe
nefit
s w
as n
ot a
rbitr
ary
and
capr
icio
us.
Reve
rsed
.Ca
se w
as a
ffirm
ed in
part,
reve
rsed
in p
art,
and
rem
ande
d fo
rfu
rther
pro
ceed
ings
.
US C
ourt
ofAp
peal
s,10
thCi
rcui
t
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C. C
on
tin
ued
1999
Med
itrus
t v.
Ster
ling
Chem
ical
s
Appe
al o
f sum
mar
y ju
dgm
ent i
nfa
vor o
f Pla
n re
gard
ing
deni
al o
fre
habi
litat
ive
care
on
med
ical
nece
ssity
gro
unds
.
Cour
t of A
ppea
ls fo
und
that
the
low
er c
ourt
had
appl
ied
the
corr
ect d
iscr
etio
nary
sta
ndar
dan
dth
at th
e Pl
an d
id n
ot a
ct in
an
arbi
trary
and
cap
ricio
us m
anne
r.
Affir
med
.Af
firm
ed s
umm
ary
judg
men
t in
favo
rof
Plan
.
US C
ourt
ofAp
peal
s,5t
hCi
rcui
t
1995
Mill
er v
.Un
ited
Wel
fare
Fund
Appe
al o
f jud
gmen
t in
favo
r of
plai
ntiff
rega
rdin
g th
e de
nial
priv
ate
nurs
ing
bene
fits
onm
edic
al n
eces
sity
gro
unds
.
On a
ppea
l, th
e co
urt u
phel
d th
atth
e Pl
an a
cted
arb
itrar
ily a
ndca
pric
ious
ly. I
t als
o fo
und
that
the
low
er c
ourt
erre
d by
con
side
ring
evid
ence
out
side
of t
he a
dmin
is-
trativ
e re
cord
.
Reve
rsed
.Ca
se w
as re
man
ded
totri
al c
ourt
with
inst
ruct
ions
.
US C
ourt
ofAp
peal
s,2n
dCi
rcui
t
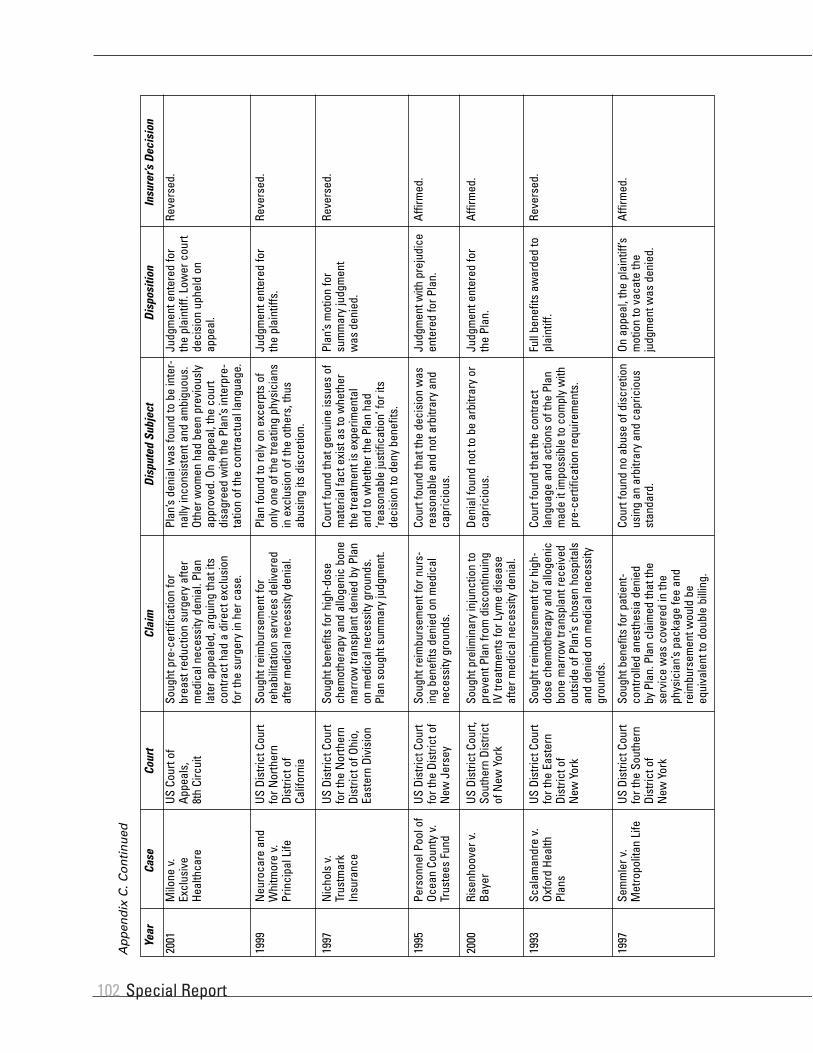
Special Report102
2001
Milo
ne v
.Ex
clus
ive
Heal
thca
re
Soug
ht p
re-c
ertif
icat
ion
for
brea
st re
duct
ion
surg
ery
afte
rm
edic
al n
eces
sity
den
ial.
Plan
late
r app
eale
d, a
rgui
ng th
at it
sco
ntra
ct h
ad a
dire
ct e
xclu
sion
for t
he s
urge
ry in
her
cas
e.
Plan
’s de
nial
was
foun
d to
be
inte
r-na
lly in
cons
iste
nt a
nd a
mbi
guou
s.Ot
her w
omen
had
bee
n pr
evio
usly
appr
oved
. On
appe
al, t
he c
ourt
disa
gree
d w
ith th
e Pl
an’s
inte
rpre
-ta
tion
of th
e co
ntra
ctua
l lan
guag
e.
Reve
rsed
.Ju
dgm
ent e
nter
ed fo
rth
e pl
aint
iff. L
ower
cou
rtde
cisi
on u
phel
d on
appe
al.
US C
ourt
ofAp
peal
s,8t
hCi
rcui
t
1999
Neu
roca
re a
ndW
hitm
ore
v.Pr
inci
pal L
ife
Soug
ht re
imbu
rsem
ent f
orre
habi
litat
ion
serv
ices
del
iver
edaf
ter m
edic
al n
eces
sity
den
ial.
Plan
foun
d to
rely
on
exce
rpts
of
only
one
of t
he tr
eatin
g ph
ysic
ians
in e
xclu
sion
of t
he o
ther
s, th
usab
usin
g its
dis
cret
ion.
Reve
rsed
.Ju
dgm
ent e
nter
ed fo
rth
e pl
aint
iffs.
US D
istri
ct C
ourt
for N
orth
ern
Dist
rict o
fCa
lifor
nia
1997
Nic
hols
v.
Trus
tmar
kIn
sura
nce
Soug
ht b
enef
its fo
r hig
h-do
sech
emot
hera
py a
nd a
lloge
nic
bone
mar
row
tran
spla
nt d
enie
d by
Pla
non
med
ical
nec
essi
ty g
roun
ds.
Plan
sou
ght s
umm
ary
judg
men
t.
Cour
t fou
nd th
at g
enui
ne is
sues
of
mat
eria
l fac
t exi
st a
s to
whe
ther
the
treat
men
t is
expe
rimen
tal
and
to w
heth
er th
e Pl
an h
ad‘re
ason
able
just
ifica
tion’
for i
tsde
cisi
on to
den
y be
nefit
s.
Reve
rsed
.Pl
an’s
mot
ion
for
sum
mar
y ju
dgm
ent
was
deni
ed.
US D
istri
ct C
ourt
for t
he N
orth
ern
Dist
rict o
f Ohi
o,Ea
ster
n Di
visi
on
1995
Pers
onne
l Poo
l of
Ocea
n Co
unty
v.
Trus
tees
Fun
d
Soug
ht re
imbu
rsem
ent f
or n
urs-
ing
bene
fits
deni
ed o
n m
edic
alne
cess
ity g
roun
ds.
Cour
t fou
nd th
at th
e de
cisi
on w
asre
ason
able
and
not
arb
itrar
y an
dca
pric
ious
.
Affir
med
.Ju
dgm
ent w
ith p
reju
dice
ente
red
for P
lan.
US D
istri
ct C
ourt
for t
he D
istri
ct o
fN
ew J
erse
y
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C. C
on
tin
ued
2000
Rise
nhoo
ver v
.Ba
yer
Soug
ht p
relim
inar
y in
junc
tion
topr
even
t Pla
n fro
m d
isco
ntin
uing
IV tr
eatm
ents
for L
yme
dise
ase
afte
r med
ical
nec
essi
ty d
enia
l.
Deni
al fo
und
not t
o be
arb
itrar
y or
capr
icio
us.
Affir
med
.Ju
dgm
ent e
nter
ed fo
rth
e Pl
an.
US D
istri
ct C
ourt,
Sout
hern
Dis
trict
of N
ew Y
ork
1993
Scal
aman
dre
v.Ox
ford
Hea
lthPl
ans
Soug
ht re
imbu
rsem
ent f
or h
igh-
dose
che
mot
hera
py a
nd a
lloge
nic
bone
mar
row
tran
spla
nt re
ceiv
edou
tsid
e of
Pla
n’s
chos
en h
ospi
tals
and
deni
ed o
n m
edic
al n
eces
sity
grou
nds.
Cour
t fou
nd th
at th
e co
ntra
ctla
ngua
ge a
nd a
ctio
ns o
f the
Pla
nm
ade
it im
poss
ible
to c
ompl
y w
ithpr
e-ce
rtific
atio
n re
quire
men
ts.
Reve
rsed
.Fu
ll be
nefit
s aw
arde
d to
plai
ntiff
.US
Dis
trict
Cou
rtfo
r the
Eas
tern
Dist
rict o
fN
ewYo
rk
1997
Sem
mle
r v.
Met
ropo
litan
Life
So
ught
ben
efits
for p
atie
nt-
cont
rolle
d an
esth
esia
den
ied
byPl
an. P
lan
clai
med
that
the
serv
ice
was
cov
ered
in th
eph
ysic
ian’
s pa
ckag
e fe
e an
dre
imbu
rsem
ent w
ould
be
equi
vale
nt to
dou
ble
billi
ng.
Cour
t fou
nd n
o ab
use
of d
iscr
etio
nus
ing
an a
rbitr
ary
and
capr
icio
usst
anda
rd.
Affir
med
.On
app
eal,
the
plai
ntiff
’sm
otio
n to
vac
ate
the
judg
men
t was
den
ied.
US D
istri
ct C
ourt
for t
he S
outh
ern
Dist
rict o
fN
ewYo
rk
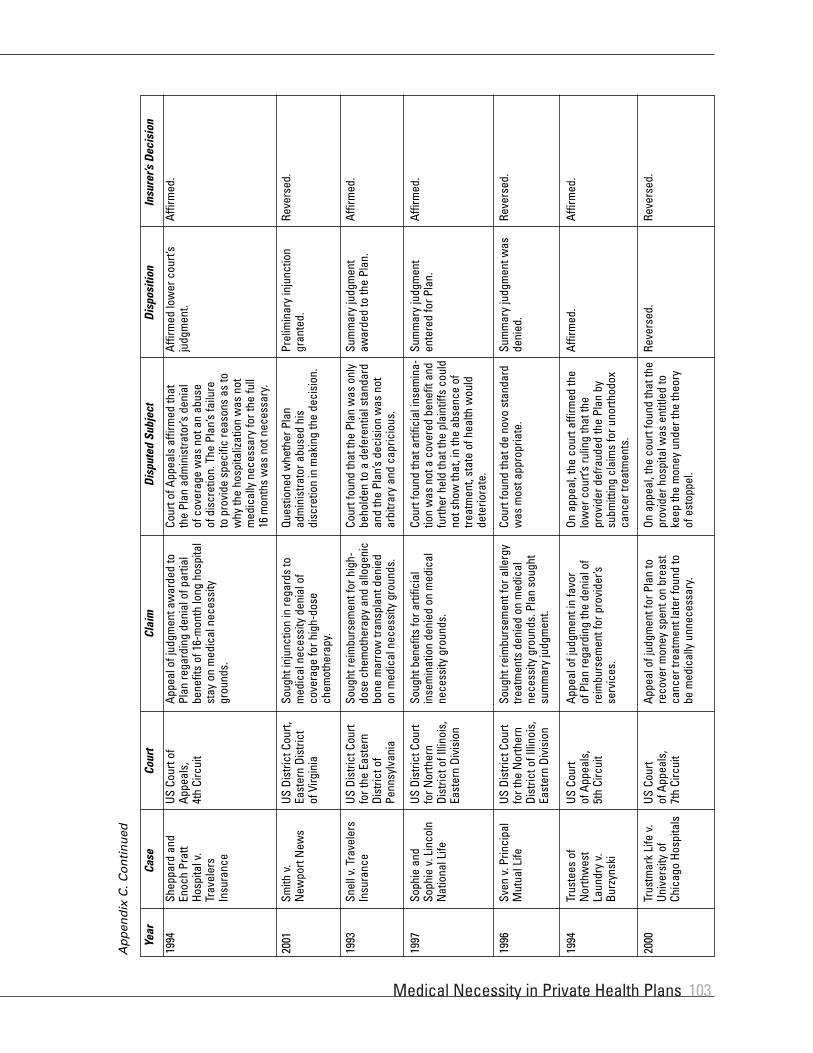
Medical Necessity in Private Health Plans 103
1994
Shep
pard
and
Enoc
h Pr
att
Hosp
ital v
.Tr
avel
ers
Insu
ranc
e
Appe
al o
f jud
gmen
t aw
arde
d to
Plan
rega
rdin
g de
nial
of p
artia
lbe
nefit
s of
16-
mon
th lo
ng h
ospi
tal
stay
on
med
ical
nec
essi
tygr
ound
s.
Cour
t of A
ppea
ls a
ffirm
ed th
atth
ePl
an a
dmin
istra
tor’s
den
ial
ofco
vera
ge w
as n
ot a
n ab
use
ofdi
scre
tion.
The
Pla
n’s
failu
reto
prov
ide
spec
ific
reas
ons
as to
why
the
hosp
italiz
atio
n w
as n
otm
edic
ally
nec
essa
ry fo
r the
full
16m
onth
s w
as n
ot n
eces
sary
.
Affir
med
.Af
firm
ed lo
wer
cou
rt’s
judg
men
t.US
Cou
rt of
Appe
als,
4th
Circ
uit
2001
Smith
v.
New
port
New
s So
ught
inju
nctio
n in
rega
rds
tom
edic
al n
eces
sity
den
ial o
fco
vera
ge fo
r hig
h-do
sech
emot
hera
py.
Ques
tione
d w
heth
er P
lan
adm
inis
trato
r abu
sed
his
disc
retio
nin
mak
ing
the
deci
sion
.
Reve
rsed
.Pr
elim
inar
y in
junc
tion
gran
ted.
US D
istri
ct C
ourt,
East
ern
Dist
rict
ofVi
rgin
ia
1993
Snel
l v. T
rave
lers
Insu
ranc
e So
ught
reim
burs
emen
t for
hig
h-do
se c
hem
othe
rapy
and
allo
geni
cbo
ne m
arro
w tr
ansp
lant
den
ied
on m
edic
al n
eces
sity
gro
unds
.
Cour
t fou
nd th
at th
e Pl
an w
as o
nly
beho
lden
to a
def
eren
tial s
tand
ard
and
the
Plan
’s de
cisi
on w
as n
otar
bitra
ry a
nd c
apric
ious
.
Affir
med
.Su
mm
ary
judg
men
taw
arde
d to
the
Plan
.US
Dis
trict
Cou
rtfo
r the
Eas
tern
Dist
rict o
fPe
nnsy
lvan
ia
1997
Soph
ie a
ndSo
phie
v. L
inco
lnN
atio
nal L
ife
Soug
ht b
enef
its fo
r arti
ficia
lin
sem
inat
ion
deni
ed o
n m
edic
alne
cess
ity g
roun
ds.
Cour
t fou
nd th
at a
rtific
ial i
nsem
ina-
tion
was
not
a c
over
ed b
enef
it an
dfu
rther
hel
d th
at th
e pl
aint
iffs
coul
dno
t sho
w th
at, i
n th
e ab
senc
e of
treat
men
t, st
ate
of h
ealth
wou
ldde
terio
rate
.
Affir
med
.Su
mm
ary
judg
men
ten
tere
d fo
r Pla
n.US
Dis
trict
Cou
rtfo
r Nor
ther
nDi
stric
t of I
llino
is,
East
ern
Divi
sion
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C. C
on
tin
ued
1996
Sven
v. P
rinci
pal
Mut
ual L
ife
Soug
ht re
imbu
rsem
ent f
or a
llerg
ytre
atm
ents
den
ied
on m
edic
alne
cess
ity g
roun
ds. P
lan
soug
htsu
mm
ary
judg
men
t.
Cour
t fou
nd th
at d
e no
vo s
tand
ard
was
mos
t app
ropr
iate
.Re
vers
ed.
Sum
mar
y ju
dgm
ent w
asde
nied
.US
Dis
trict
Cou
rtfo
r the
Nor
ther
nDi
stric
t of I
llino
is,
East
ern
Divi
sion
1994
Trus
tees
of
Nor
thw
est
Laun
dry
v.Bu
rzyn
ski
Appe
al o
f jud
gmen
t in
favo
rof
Plan
rega
rdin
g th
e de
nial
of
reim
burs
emen
t for
pro
vide
r’sse
rvic
es.
On a
ppea
l, th
e co
urt a
ffirm
ed th
elo
wer
cou
rt’s
rulin
g th
at th
epr
ovid
er d
efra
uded
the
Plan
by
subm
ittin
g cl
aim
s fo
r uno
rthod
oxca
ncer
trea
tmen
ts.
Affir
med
.Af
firm
ed.
US C
ourt
ofAp
peal
s,5t
hCi
rcui
t
2000
Trus
tmar
k Li
fe v
.Un
iver
sity
of
Chic
ago
Hosp
itals
Appe
al o
f jud
gmen
t for
Pla
n to
reco
ver m
oney
spe
nt o
n br
east
canc
er tr
eatm
ent l
ater
foun
d to
be m
edic
ally
unn
eces
sary
.
On a
ppea
l, th
e co
urt f
ound
that
the
prov
ider
hos
pita
l was
ent
itled
toke
ep th
e m
oney
und
er th
e th
eory
of
est
oppe
l.
Reve
rsed
.Re
vers
ed.
US C
ourt
ofAp
peal
s,7t
hCi
rcui
t

Special Report104
1999
Wel
lnes
s Ae
robi
cCl
inic
v. U
nite
dHe
alth
Care
Soug
ht re
imbu
rsem
ent f
orre
habi
litat
ion
serv
ices
del
iver
edaf
ter m
edic
al n
eces
sity
den
ial.
Deni
al o
f ben
efits
foun
d to
be
lega
lly c
orre
ct a
nd n
ot a
n ab
use
ofdi
scre
tion.
Affir
med
.Su
mm
ary
judg
men
t for
Plan
US D
istri
ct C
ourt
for E
aste
rnDi
stric
t of
Loui
sian
a
1994
Whi
tehe
ad v
.Fe
dera
l Exp
ress
So
ught
pre
limin
ary
inju
nctio
n fo
rhi
gh d
ose
chem
othe
rapy
with
perip
hera
l ste
m c
ell r
escu
ede
nied
on
med
ical
nec
essi
tygr
ound
s.
Cour
t fou
nd it
did
not
hav
e th
eau
thor
ity to
usu
rp th
e po
wer
of
Plan
to in
terp
ret c
ontra
ct te
rms.
It
did
not f
ind
that
the
Plan
act
ed
in a
n ar
bitra
ry a
nd c
apric
ious
man
ner.
Affir
med
.Pr
elim
inar
y in
junc
tion
deni
ed.
US D
istri
ct C
ourt
for t
he W
este
rnDi
stric
t of
Tenn
esse
e,W
este
rn D
ivis
ion
Year
Case
Cour
tCl
aim
Disp
uted
Sub
ject
Disp
ositi
onIn
sure
r’s D
ecis
ion
Ap
pen
dix
C. C
on
tin
ued

Medical Necessity in Private Health Plans 105
New
Yor
kA
sign
ifica
nt le
gal d
evel
opm
ent r
egar
ding
med
ical
nec
essi
ty w
as th
e se
ries
of O
ctob
er 2
001
settl
emen
t agr
eem
ents
reac
hed
betw
een
the
New
York
Sta
te A
ttorn
ey G
ener
al’s
Offic
e an
d si
x la
rge
MCO
s.1
Follo
win
g a
two-
year
inve
stig
atio
n in
to h
ow th
ese
MCO
s in
form
ed th
eir p
rovi
ders
and
enro
llees
of a
dver
se d
eter
min
atio
n de
cisi
ons
on th
e gr
ound
s of
med
ical
nec
essi
ty, A
ttorn
ey G
ener
al E
liot S
pitz
er fo
und
that
thes
e M
COs
wer
e no
tin
com
plia
nce
with
New
Yor
k St
ate’
s ut
iliza
tion
revi
ew la
w (d
iscu
ssed
in m
ore
deta
il in
Par
t 3 b
elow
). Th
e fo
cus
of th
e in
vest
igat
ion
was
on
the
proc
esse
s us
ed b
y th
e M
COs
in m
akin
g th
eir d
eter
min
atio
ns a
nd in
form
ing
prov
ider
s an
d en
rolle
es o
f the
m, r
athe
r tha
n th
e co
nten
t of t
he m
edic
alne
cess
ity d
efin
ition
s th
emse
lves
. Spi
tzer
’s of
fice
foun
d, fo
r exa
mpl
e, th
at M
COs
wer
e of
ten
deny
ing
auth
oriza
tion
or re
imbu
rsem
ent f
or in
patie
ntm
enta
l hea
lth a
nd s
ubst
ance
abu
se tr
eatm
ent a
nd o
fferin
g no
thin
g m
ore
than
a g
ener
ic e
xpla
natio
n th
at th
e se
rvic
e w
as “
not m
edic
ally
nec
es-
sary
.” T
here
was
ofte
n no
dis
clos
ure
of th
e un
derly
ing
reas
ons
or c
linic
al ra
tiona
le u
sed
by th
e M
COs
in m
akin
g th
eir d
ecis
ions
, whi
ch is
requ
ired
in N
ew Y
ork’s
util
izatio
n re
view
law
. An
exam
ple
of s
uch
an in
adeq
uate
dis
clos
ure,
as
cont
aine
d in
Exh
ibit
A of
the
settl
emen
t agr
eem
ents
, was
:
Deni
al o
f con
tinua
tion
of s
tay
at p
sych
iatri
c in
patie
nt fa
cilit
y: P
atie
nt w
as c
oope
rativ
e th
roug
hout
sta
y w
ith n
o ov
ert
psyc
hiat
ric s
ympt
om a
ccor
ding
to th
e at
tend
ing
Doct
or. M
edic
atio
n w
as d
isco
ntin
ued
durin
g th
e st
ay. T
his
refe
rral
doe
sno
tmee
t eith
er s
ever
ity o
f illn
ess,
or i
nten
sity
of s
ervi
ce a
nd is
ther
efor
e de
nied
.2
The
settl
emen
t agr
eem
ents
def
ined
“re
ason
s an
d cl
inic
al ra
tiona
le”
as fo
llow
s, s
tipul
atin
g co
nsid
erat
ion
of in
divi
dual
ized
med
ical
ass
essm
ents
and
disc
losu
re o
f suf
ficie
nt in
form
atio
n in
adv
erse
det
erm
inat
ion
notic
es:
“Rea
sons
and
Clin
ical
Rat
iona
le”
mea
ns th
e in
divi
dual
ized
med
ical
bas
is fo
r an
Adve
rse
Dete
rmin
atio
n. A
sta
tem
ent o
fRe
ason
s an
d Cl
inic
al R
atio
nale
mus
t dem
onst
rate
that
the
UR [U
tiliza
tion
Revi
ew] A
gent
mad
e an
indi
vidu
alize
d m
edic
alas
sess
men
t of t
he E
nrol
lee
by re
ferr
ing
to th
e sp
ecifi
c m
edic
al d
ata
rela
ting
to th
e En
rolle
e, w
hich
the
Clin
ical
Pee
r Rev
iew
erto
ok in
to c
onsi
dera
tion
whe
n m
akin
g th
e Ad
vers
e De
term
inat
ion.
Mer
ely
stat
ing
that
the
serv
ice
at is
sue
is n
ot m
edic
ally
nece
ssar
y is
not
suf
ficie
nt, n
or is
a s
tate
men
t tha
t the
pro
pose
d se
rvic
e do
es n
ot m
eet t
he U
R Ag
ent’s
crit
eria
. A s
tate
men
tof
Reas
ons
and
Clin
ical
Rat
iona
le m
ust b
e su
ffici
ently
spe
cific
to e
nabl
e th
e En
rolle
e an
d/or
the
Enro
llee’
s he
alth
car
epr
ovid
er to
mak
e an
info
rmed
dec
isio
n ab
out w
heth
er o
r not
to a
ppea
l the
Adv
erse
Det
erm
inat
ion
and
to d
eter
min
e th
eis
sue
or is
sues
to a
ddre
ss in
the
appe
al.3
Rath
er th
an ta
ke th
e ca
ses
to tr
ial,
the
Atto
rney
Gen
eral
’s Of
fice
and
the
MCO
s ag
reed
to s
ettle
out
of c
ourt.
Und
er th
e te
rms
of th
e se
ttlem
ent
agre
emen
ts, t
he M
COs
(whi
le a
dmitt
ing
no w
rong
doin
g) a
gree
d to
refo
rm th
eir n
otifi
catio
n pr
actic
es to
brin
g th
em in
to c
ompl
ianc
e w
ith s
tate
law
and
to e
ach
pay
$1 m
illio
n to
war
ds th
e co
st o
f the
inve
stig
atio
n. T
he A
ttorn
ey G
ener
al’s
offic
e w
ill c
ontin
ue to
mon
itor t
heir
prac
tices
unt
ilJa
nuar
y 20
04, w
ith a
pos
sibl
e on
e-ye
ar e
xten
sion
of t
he m
onito
ring
for M
COs
still
foun
d to
be
nonc
ompl
iant
.4
Stat
eDe
scrip
tion
Ap
pen
dix
D. S
tate
Inve
stig
atio
ns
and
Leg
al A
ctio
ns
Reg
ard
ing
Med
ical
Nec
essi
ty Is
sues
1Ae
tna/
U.S.
Hea
lthCa
re In
c./P
rude
ntia
l Hea
lth P
lan
of H
artfo
rd, C
T; E
xcel
lus
Heal
th P
lans
of R
oche
ster
; Gro
up H
ealth
Inc.
of M
anha
ttan;
HIP
Hea
lth P
lan
ofGr
eate
rNew
Yor
k, In
c.; O
xfor
d He
alth
Pla
ns o
f Tru
mbu
ll, C
T; a
nd V
ytra
Hea
lth P
lans
of L
ong
Isla
nd, I
nc. S
ee:“
Land
mar
k Ag
reem
ents
Giv
e Co
nsum
ers
New
Prot
ectio
ns in
HM
O Di
sput
es.”
NY
Atto
rney
Gen
eral
’s Of
fice
Pres
s Re
leas
e. O
ctob
er 1
6, 2
001.
Ava
ilabl
e at
http
://w
ww
.oag
.sta
te.n
y.us.
Acc
esse
d Oc
tobe
r 29,
200
1.2
Atto
rney
Gen
eral
of t
he S
tate
of N
ew Y
ork,
Hea
lth C
are
Bure
au. “
In th
e m
atte
r of G
roup
Hea
lth In
corp
orat
ed: A
ssur
ance
of D
isco
ntin
uanc
e Pu
rsua
nt to
Exec
utiv
e La
w S
ectio
n 63
, Sub
divi
sion
15
(Exh
ibit
A).”
Aug
ust 2
7, 2
001.
3Id
., p.
4.
4N
Y At
torn
ey G
ener
al’s
Offic
e Pr
ess
Rele
ase.
Oct
ober
16,
200
1. o
p. c
it.

Special Report106
Mai
neIn
200
0, b
oth
Unite
d Be
havi
oral
Hea
lth a
nd C
igna
Beh
avio
ral H
ealth
, Inc
., en
tere
d in
to c
onse
nt a
gree
men
ts w
ith th
e M
aine
Bur
eau
of In
sura
nce.
5
Heal
th p
lan
enro
llees
had
file
d co
mpl
aint
s w
ith th
e Bu
reau
con
cern
ing
deni
als
of c
over
age
base
d on
med
ical
nec
essi
ty g
roun
ds. A
sub
sequ
ent
dete
rmin
atio
n by
the
Bure
au th
at th
e de
nial
s w
ere
not i
n co
nfor
man
ce w
ith M
aine
rule
s re
gard
ing
utili
zatio
n re
view
led
to th
e ag
reem
ents
.
In th
e UB
H ca
se, t
wo
sepa
rate
enr
olle
es w
ere
deni
ed c
over
age
for m
enta
l tre
atm
ent o
f tw
o or
mor
e fa
mily
mem
bers
by
the
sam
e th
erap
ist.
Atth
etim
e, U
BH h
ad a
writ
ten
guid
elin
e th
at it
was
gen
eral
ly n
eces
sary
for f
amily
mem
bers
to re
ceiv
e co
ncur
rent
trea
tmen
t by
sepa
rate
ther
apis
ts. T
he B
urea
u fo
und
that
the
deni
al n
otic
es d
id n
ot a
dequ
atel
y co
nfor
m to
the
stat
e ag
ency
rule
s6in
that
they
did
not
con
tain
the
qual
ifyin
g cr
eden
tials
of t
he re
view
er; d
id n
ot in
clud
e a
stat
emen
t of t
he re
view
er’s
unde
rsta
ndin
g of
the
cons
umer
’s re
ason
s fo
r app
eal;
did
notc
lear
ly s
tate
the
deci
sion
and
clin
ical
ratio
nale
in s
uffic
ient
det
ail t
o al
low
the
cons
umer
s to
resp
ond
furth
er; d
id n
ot in
clud
e a
refe
renc
eto
the
evid
ence
or d
ocum
enta
tion
used
for t
he a
dver
se d
eter
min
atio
n; d
id n
ot in
clud
e a
desc
riptio
n of
the
proc
edur
es, t
ime
fram
es, a
ndco
nsum
ers’
righ
ts fo
r sec
ond
leve
l grie
vanc
e re
view
; and
did
not
incl
ude
a no
tice
of th
e rig
ht o
f the
con
sum
ers
to c
onta
ct th
e Bu
reau
of
Insu
ranc
e. U
BH w
as fi
ned
$10,
000,
and
furt
her a
djud
icat
ory
proc
eedi
ngs
wer
e dr
oppe
d.
In th
e Ci
gna
case
, an
enro
llee
was
den
ied
bene
fits
for t
he la
st th
ree
days
of h
er m
inor
chi
ld’s
five-
day
inpa
tient
sta
y at
a h
ospi
tal o
n th
egr
ound
sth
at th
e ch
ild o
sten
sibl
y co
uld
have
bee
n tra
nsfe
rred
to a
psy
chia
tric
faci
lity
afte
r the
firs
t 48
hour
s. O
n th
e fif
th d
ay, t
he c
hild
, who
was
suic
idal
, was
tran
sfer
red
to a
non
-Cig
na-c
ontra
cted
faci
lity
on th
e fir
st d
ay th
at fa
cilit
y ha
d a
vaca
nt b
ed. T
here
wer
e no
oth
er c
ontra
cted
or n
on-c
ontra
cted
faci
litie
s in
Cig
na’s
netw
ork
with
in 6
0 m
inut
es tr
avel
dis
tanc
e fro
m th
e en
rolle
e’s
hom
e (re
quire
d by
Mai
ne la
w).
Follo
win
ga
serie
s of
revi
ews
and
appe
als,
Cig
na re
vers
ed it
s or
igin
al d
enia
l nea
rly a
yea
r lat
er. T
he B
urea
u of
Insu
ranc
e fo
und
that
:
By re
vers
ing
its d
enia
l of b
enef
its, C
BH a
ckno
wle
dged
the
need
for h
oldi
ng C
onsu
mer
’s ch
ild o
n an
inpa
tient
bas
is u
ntil
her
mov
e to
Aca
dia.
Par
ticip
atio
n by
CBH
in th
e un
succ
essf
ul e
ffort
on J
uly
24th
for a
n im
med
iate
tran
sfer
sho
ws
it th
en k
new
or s
houl
d ha
ve k
now
n th
at: 1
) unt
il th
e tr
ansf
er c
ould
be
effe
cted
, it w
as m
edic
ally
nec
essa
ry fo
r the
chi
ld to
con
tinue
rece
ivin
g in
patie
nt c
are
at E
MM
C; a
nd 2
) CBH
’s gu
idel
ine
for t
rans
fer t
o a
psyc
hiat
ric fa
cilit
y w
ithin
48
hour
s of
adm
issi
onto
an a
cute
car
e ho
spita
l cou
ld n
ot b
e m
et w
here
, as
here
, thr
ough
no
faul
t of C
onsu
mer
ther
e w
as n
o ps
ychi
atric
faci
lity
reas
onab
ly a
vaila
ble
to a
ccep
t her
dau
ghte
r prio
r to
July
27t
h.
The
Bure
au a
lso
foun
d th
at th
e co
nten
t of C
igna
’s de
nial
lette
rs w
as n
ot in
con
form
ance
with
Mai
ne la
w, f
or m
any
of th
e sa
me
reas
ons
as th
eUB
H ca
se. C
igna
was
fine
d $5
,000
, and
furth
er a
djud
icat
ory
proc
eedi
ngs
wer
e dr
oppe
d.
In d
istin
guis
hing
thes
e tw
o ca
ses,
it is
not
able
that
in th
e UB
H ca
se, i
ts “
sepa
rate
ther
apis
ts”
guid
elin
e w
as n
ot c
alle
d in
to q
uest
ion
on th
egr
ound
s of
reas
onab
lene
ss o
r app
ropr
iate
ness
. Rat
her,
the
com
pany
was
cite
d fo
r def
icie
ncie
s in
the
proc
esse
s it
used
to n
otify
the
enro
llees
ofth
e be
nefit
den
ials
. In
the
Cign
a ca
se, h
owev
er, t
he B
urea
u fo
und
the
appl
icat
ion
of th
e “4
8-ho
ur ru
le”
for t
rans
fer i
n m
edic
al n
eces
sity
deci
sion
s to
be
subs
tant
ivel
y in
appr
opria
te in
ligh
t of t
he in
adeq
uacy
of t
he p
rovi
der n
etw
ork,
whi
ch d
id n
ot m
eet s
tate
sta
ndar
ds.
Ap
pen
dix
D. C
on
tin
ued
5In
RE:
Uni
ted
Beha
vior
al H
ealth
, Con
sent
Agr
eem
ent w
ith M
aine
Bur
eau
of In
sura
nce,
op.
cit.
In R
E: C
igna
Beh
avio
ral H
ealth
, Inc
., Co
nsen
t Agr
eem
ent w
ithM
aine
Bure
au o
f Ins
uran
ce, D
ocke
t No.
00-
3003
. Av
aila
ble
at h
ttp://
ww
w.s
tate
.me.
us/p
fr/in
s/in
s003
003.
htm
. Ac
cess
ed A
pril
17, 2
002.
6Bu
reau
of I
nsur
ance
Rul
e Ch
apte
r 850
(8) a
nd (9
).



DHHS Publication Number (SMA 03-3790)Printed 2003 Substance Abuse and Mental
Health Services Administration
CMHS8_01_Cover.qxd 5/9/2003 2:01 PM Page c4