Embed Size (px)
Citation preview
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 1
CME Baseline Curriculum Report October 14, 2010 For CME Activity: Managing Advanced Prostate Cancer in the Community Setting: A Case-based Curriculum Supported by an independent educational grant from Sanofi-Aventis Available at: http://cme.medscape.com/viewarticle/725210 Launched online: July 20, 2010
Table of Contents Executive Summary ........................................................................................................................................... 2
• Background • Method • Main Findings • Future Educational Focus
Faculty Insights & Recommendations ................................................................................................................ 2 Study Design/Methods ....................................................................................................................................... 3 Results and Analysis............................................................................................................................................ 5
• Castration-Resistant Prostate Cancer (CRPC) – Definition and Mechanisms • Management of CRPC • Maintenance of Bone Health • Emerging Therapies • Barriers and Educational Information
Summary of Assessment and Recommendations .............................................................................................. 17 Appendix A: Demographics ................................................................................................................................ 18 Appendix B: Full Cases & Data Tables ............................................................................................................... 19 Appendix C: References ...................................................................................................................................... 27
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 2
Executive Summary Background CE Outcomes, LLC, collaborated with Medscape to assess the clinical management of patients with advanced prostate cancer using a survey entitled Managing Advanced Prostate Cancer in the Community Setting: A Clinical Practice Assessment that posted July 20, 2010. Target Audience Oncologists and urologists Method With a clinical expert, a series of evidence-based performance indicators were developed. Case vignettes were utilized to assess change in performance. Clinical case responses were compared before and after participation with a similar group of nonparticipating physicians. Main Findings
• The majority of respondents did not appropriately classify a patient as castration-resistant. Furthermore,
knowledge deficits were noted particularly in the area of mechanism of action regarding receptor expression and the presence of enzymes that could affect treatment.
• Significant differences were noted in the management of patients with castration-resistant prostate cancer
(CRPC). This was reflected in the relatively low confidence levels in deciding the next step in treatment.
• Most of the respondents indicated overtreatment with zoledronic acid as well as the current indication of denosumab to lower vertebral fracture incidence in patients with CRPC.
• Approximately half of respondents were not aware of the survival benefits of cabazitaxel as well as the associated side effects of neutropenia.
Future Educational Focus Based on responses, future educational activities should focus on:
• Clinical identification of a patient with prostate cancer defined as castration resistant as well as current markers used for management and treatment.
• Recognizing the importance of secondary hormonal therapy in the treatment of CRPC. • Reviewing treatment options, particularly awareness of emerging antiandrogen therapies and their appropriate
selection in prostate cancer treatment. • The importance of maintaining bone health and the treatment regimens available to patients with prostate
cancer. • Utilizing new US Food and Drug Administration (FDA)-approved immunotherapy and chemotherapy agents as
well as understanding their mechanisms of action and potential side effects. Faculty Insights
& Recommendations
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 3
Study Design/Methods CE Outcomes, LLC, an independent assessment company, collaborated with Medscape to conduct an evidence-based clinical practice assessment. Based on the curriculum objectives, CE Outcomes, LLC, worked with a clinical expert to develop a series of measurable performance indicators referenced to guidelines, evidence-based citations, and clinical trial evidence. These performance indicators were used to develop case vignettes and questions to gather data on clinicians’ baseline knowledge, skills, attitudes, practice patterns, and barriers to optimal management. Results from recent research demonstrate case vignettes, compared with other methods of measuring processes of care such as chart review and standardized patients, provide a valid, cost-effective, and noninvasive method to measure a physician's processes of care.[1,2] Participant response data were gathered by Medscape and provided electronically to CE Outcomes for analysis. A statistical package for the social sciences (SPSS 17.0) was used in data extraction and transformation and statistical analyses. Participant responses were scored according to their concordance with the evidence-based performance measures. Overall mean scores and pooled standard deviations were calculated. These initial data serve as the “control” group and inform the ongoing curriculum with feedback on participants’ current level of practice. Reporting data are furnished on an aggregate level to maintain user confidentiality.
Performance indicators for this activity included:
• Prostate cancers progressing despite castrate levels of testosterone are considered castration resistant and not hormone refractory.[3]
• The androgen receptor remains active in patients who have developed castration-resistant disease, thus androgen deprivation therapy (ADT) should be continued. If initial ADT therapy has failed, an antiandrogen or ketoconazole may be beneficial.[4]
• The androgen receptor remains active in patients who have developed castration-resistant disease. Secondary hormonal therapy has not yet been shown to prolong survival in randomized trials. The benefit and safety of testosterone replacement therapy has not been demonstrated in men with moderate or rapid prostate-specific antigen (PSA) progression on ADT therapy.[4-6]
• In patients with CRPC, expression of several steroidogenic enzymes including CYP17A1 is upregulated and may sustain significant intratumoral androgen levels, despite androgen deprivation therapy.[5,7]
• Abiraterone acetate is well tolerated and demonstrates activity in CRPC, including in patients previously treated with ketoconazole. Abiraterone is associated with substantial drops in circulating androgens. Mineralocorticoid-associated toxicities including hypertension and hypokalemia are common (> 5%).[8-10]
• Zoledronic acid once yearly or alendronate daily or weekly are FDA-approved therapies for the treatment of osteoporosis in men.[11]
• Denosumab is associated with increased bone mineral density at all sites and a reduction in new vertebral fractures in men on ADT with nonmetastatic prostate cancer.[12-14]
• Sipuleucel-T is a cell-based vaccine composed of autologous antigen-presenting peripheral blood mononuclear cells (enriched for a dendritic cell fraction) that have been exposed to a recombinant protein consisting of granulocyte-macrophage colony-stimulating factor (GM-CSF) fused to prostatic-acid phosphatase (PAP), a protein expressed by prostate cancer cells.[14-16]
• In asymptomatic patients with metastatic castration-resistant prostate cancer, sipuleucel-T is associated with improved overall survival.[14-16]
• Ipilimumab is a human monoclonal antibody directed against CTLA-4 (cytotoxic T lymphocyte-associated antigen 4) that is currently under investigation for prostate cancer treatment.[16,17]
• Compared with mitoxantrone, cabazitaxel confers a significantly longer overall survival for patients with metastatic CRPC who have progressed after docetaxel therapy.[18,19]
• In the phase 3 TROPIC study, the most common side effects occurring at a grade 3 level or higher observed with cabazitaxel were febrile neutropenia (57%), diarrhea (6.2%), and fatigue (4.9%).[18]
• In the TAX-327 trial, side effects that were significantly more common with docetaxel every 3 weeks compared with mitoxantrone every 3 weeks include grade 3 or 4 neutropenia, alopecia, diarrhea, sensory neuropathy, and stomatitis.[20]
• In men with metastatic CRPC and evidence of disease progression after docetaxel therapy, cabazitaxel is associated with significantly longer overall survival than mitoxantrone.[18]
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 4
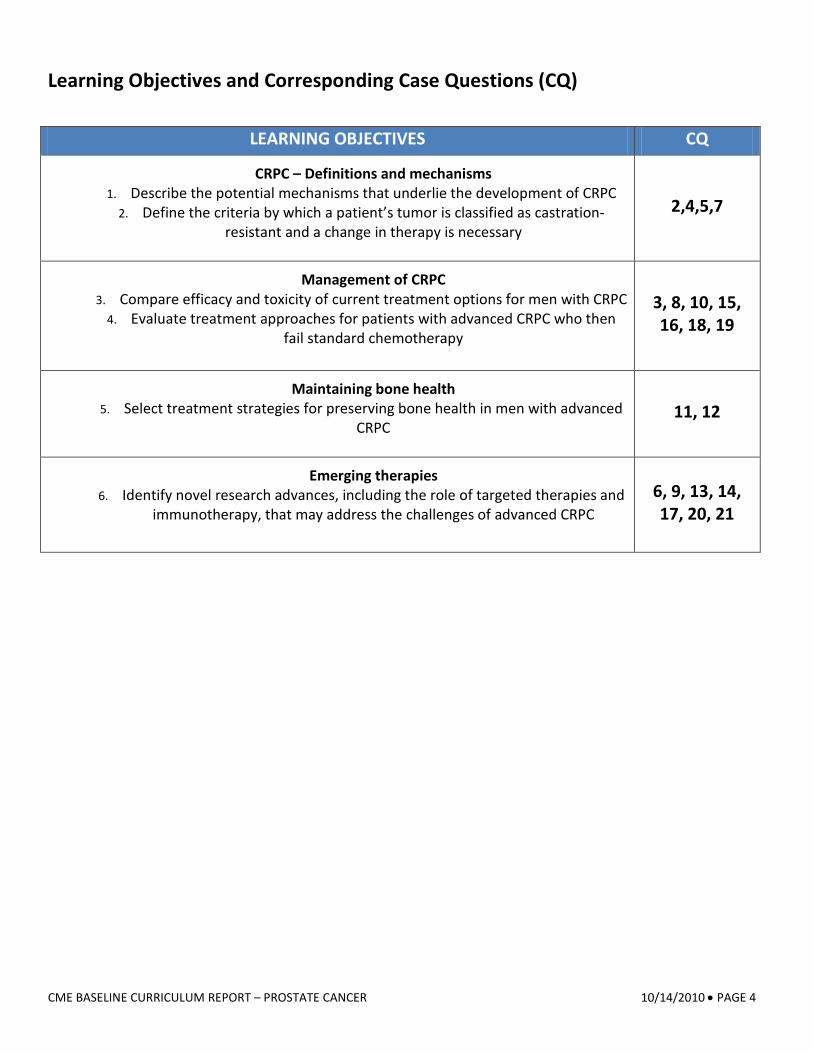
Learning Objectives and Corresponding Case Questions (CQ)
LEARNING OBJECTIVES CQ
CRPC – Definitions and mechanisms 1. Describe the potential mechanisms that underlie the development of CRPC
2. Define the criteria by which a patient’s tumor is classified as castration-resistant and a change in therapy is necessary
2,4,5,7
Management of CRPC 3. Compare efficacy and toxicity of current treatment options for men with CRPC
4. Evaluate treatment approaches for patients with advanced CRPC who then fail standard chemotherapy
3, 8, 10, 15, 16, 18, 19
Maintaining bone health 5. Select treatment strategies for preserving bone health in men with advanced
CRPC
11, 12
Emerging therapies 6. Identify novel research advances, including the role of targeted therapies and
immunotherapy, that may address the challenges of advanced CRPC
6, 9, 13, 14, 17, 20, 21
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 5
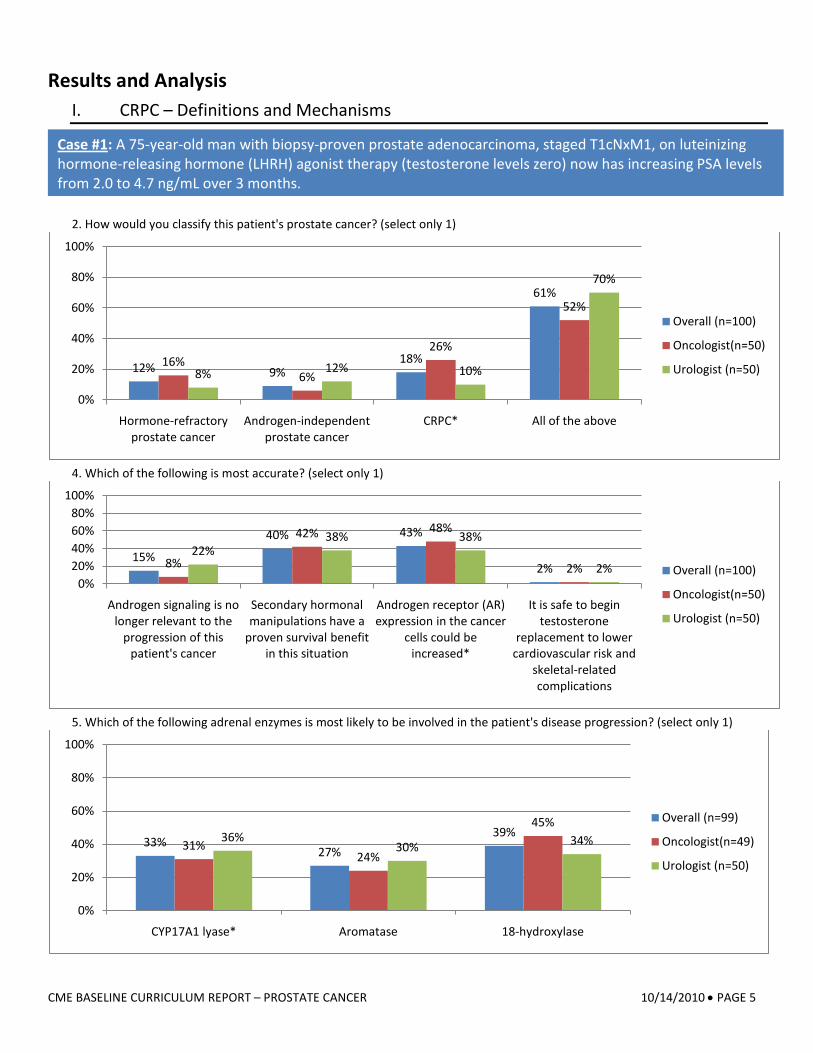
Results and Analysis I. CRPC – Definitions and Mechanisms
2. How would you classify this patient's prostate cancer? (select only 1)
4. Which of the following is most accurate? (select only 1)
5. Which of the following adrenal enzymes is most likely to be involved in the patient's disease progression? (select only 1)
12% 9%18%
61%
16%6%
26%
52%
8% 12% 10%
70%
0%
20%
40%
60%
80%
100%
Hormone-refractory prostate cancer
Androgen-independent prostate cancer
CRPC* All of the above
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
15%
40% 43%
2%8%
42% 48%
2%22%
38% 38%
2%0%
20%40%60%80%
100%
Androgen signaling is no longer relevant to the
progression of this patient's cancer
Secondary hormonal manipulations have a
proven survival benefit in this situation
Androgen receptor (AR) expression in the cancer
cells could be increased*
It is safe to begin testosterone
replacement to lower cardiovascular risk and
skeletal-related complications
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
33%27%
39%31%
24%
45%36%
30% 34%
0%
20%
40%
60%
80%
100%
CYP17A1 lyase* Aromatase 18-hydroxylase
Overall (n=99)
Oncologist(n=49)
Urologist (n=50)
Case #1: A 75-year-old man with biopsy-proven prostate adenocarcinoma, staged T1cNxM1, on luteinizing hormone-releasing hormone (LHRH) agonist therapy (testosterone levels zero) now has increasing PSA levels from 2.0 to 4.7 ng/mL over 3 months.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 6
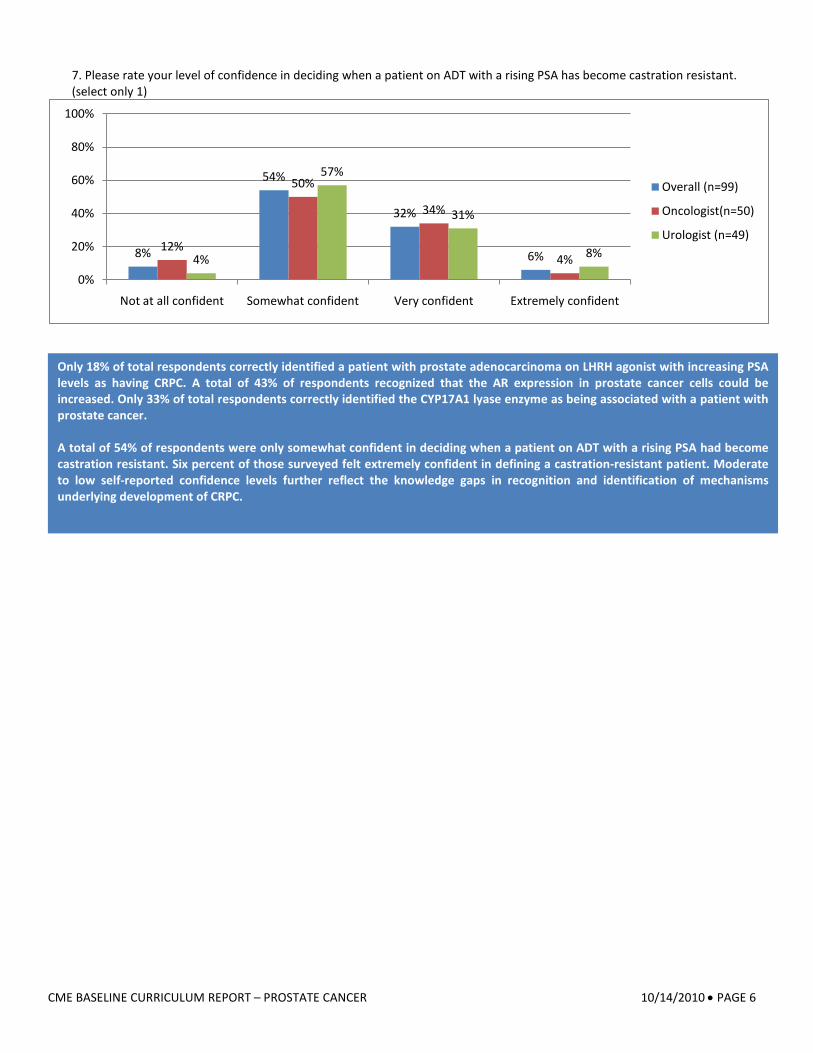
7. Please rate your level of confidence in deciding when a patient on ADT with a rising PSA has become castration resistant. (select only 1)
8%
54%
32%
6%12%
50%
34%
4%4%
57%
31%
8%
0%
20%
40%
60%
80%
100%
Not at all confident Somewhat confident Very confident Extremely confident
Overall (n=99)
Oncologist(n=50)
Urologist (n=49)
Only 18% of total respondents correctly identified a patient with prostate adenocarcinoma on LHRH agonist with increasing PSA levels as having CRPC. A total of 43% of respondents recognized that the AR expression in prostate cancer cells could be increased. Only 33% of total respondents correctly identified the CYP17A1 lyase enzyme as being associated with a patient with prostate cancer. A total of 54% of respondents were only somewhat confident in deciding when a patient on ADT with a rising PSA had become castration resistant. Six percent of those surveyed felt extremely confident in defining a castration-resistant patient. Moderate to low self-reported confidence levels further reflect the knowledge gaps in recognition and identification of mechanisms underlying development of CRPC.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 7
II. Management of CRPC
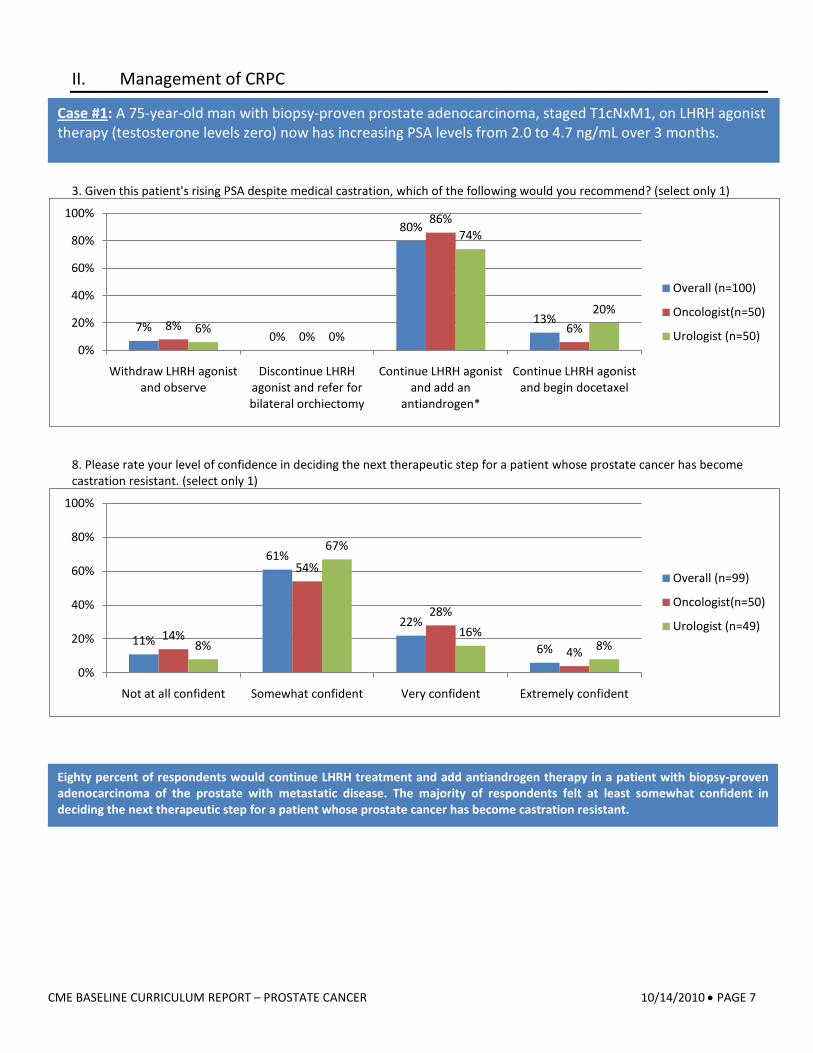
3. Given this patient's rising PSA despite medical castration, which of the following would you recommend? (select only 1)
8. Please rate your level of confidence in deciding the next therapeutic step for a patient whose prostate cancer has become castration resistant. (select only 1)
7%0%
80%
13%8%0%
86%
6%6% 0%
74%
20%
0%
20%
40%
60%
80%
100%
Withdraw LHRH agonist and observe
Discontinue LHRH agonist and refer for bilateral orchiectomy
Continue LHRH agonist and add an
antiandrogen*
Continue LHRH agonist and begin docetaxel
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
11%
61%
22%
6%14%
54%
28%
4%8%
67%
16%8%
0%
20%
40%
60%
80%
100%
Not at all confident Somewhat confident Very confident Extremely confident
Overall (n=99)
Oncologist(n=50)
Urologist (n=49)
Eighty percent of respondents would continue LHRH treatment and add antiandrogen therapy in a patient with biopsy-proven adenocarcinoma of the prostate with metastatic disease. The majority of respondents felt at least somewhat confident in deciding the next therapeutic step for a patient whose prostate cancer has become castration resistant.
Case #1: A 75-year-old man with biopsy-proven prostate adenocarcinoma, staged T1cNxM1, on LHRH agonist therapy (testosterone levels zero) now has increasing PSA levels from 2.0 to 4.7 ng/mL over 3 months.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 8
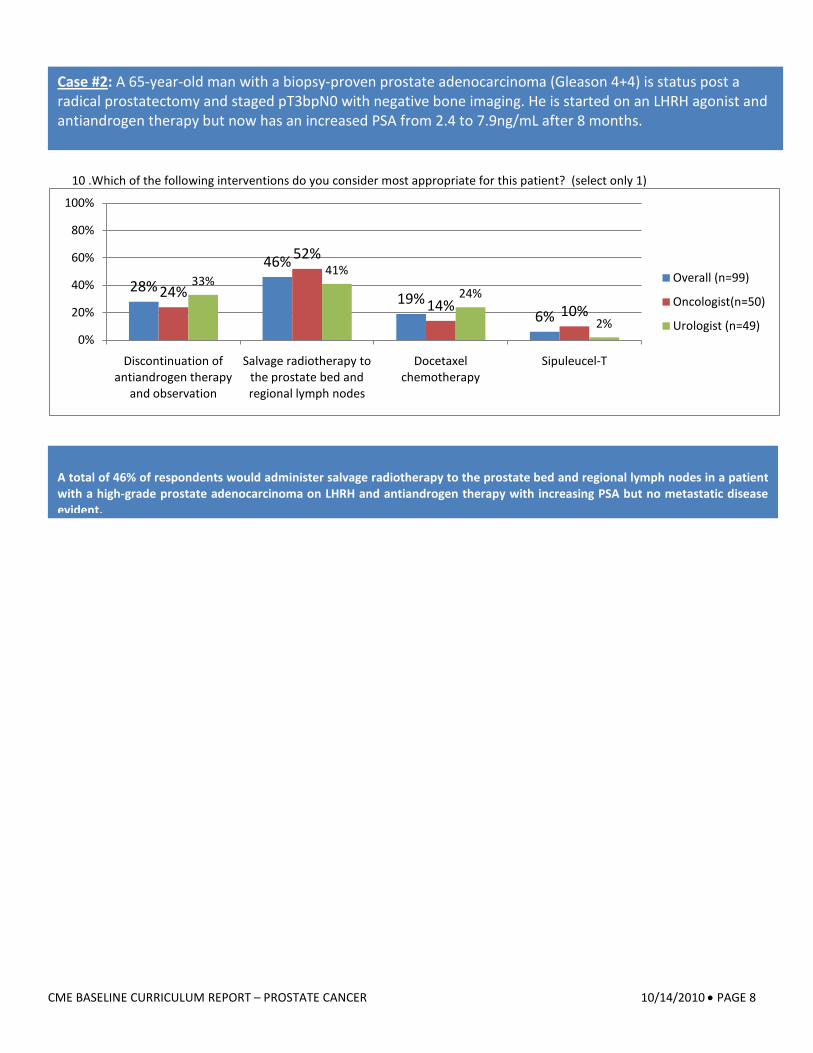
10 .Which of the following interventions do you consider most appropriate for this patient? (select only 1)
28%46%
19%6%
24%
52%
14% 10%
33%41%
24%
2%0%
20%
40%
60%
80%
100%
Discontinuation of antiandrogen therapy
and observation
Salvage radiotherapy to the prostate bed and regional lymph nodes
Docetaxel chemotherapy
Sipuleucel-T
Overall (n=99)
Oncologist(n=50)
Urologist (n=49)
A total of 46% of respondents would administer salvage radiotherapy to the prostate bed and regional lymph nodes in a patient with a high-grade prostate adenocarcinoma on LHRH and antiandrogen therapy with increasing PSA but no metastatic disease evident.
Case #2: A 65-year-old man with a biopsy-proven prostate adenocarcinoma (Gleason 4+4) is status post a radical prostatectomy and staged pT3bpN0 with negative bone imaging. He is started on an LHRH agonist and antiandrogen therapy but now has an increased PSA from 2.4 to 7.9ng/mL after 8 months.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 9
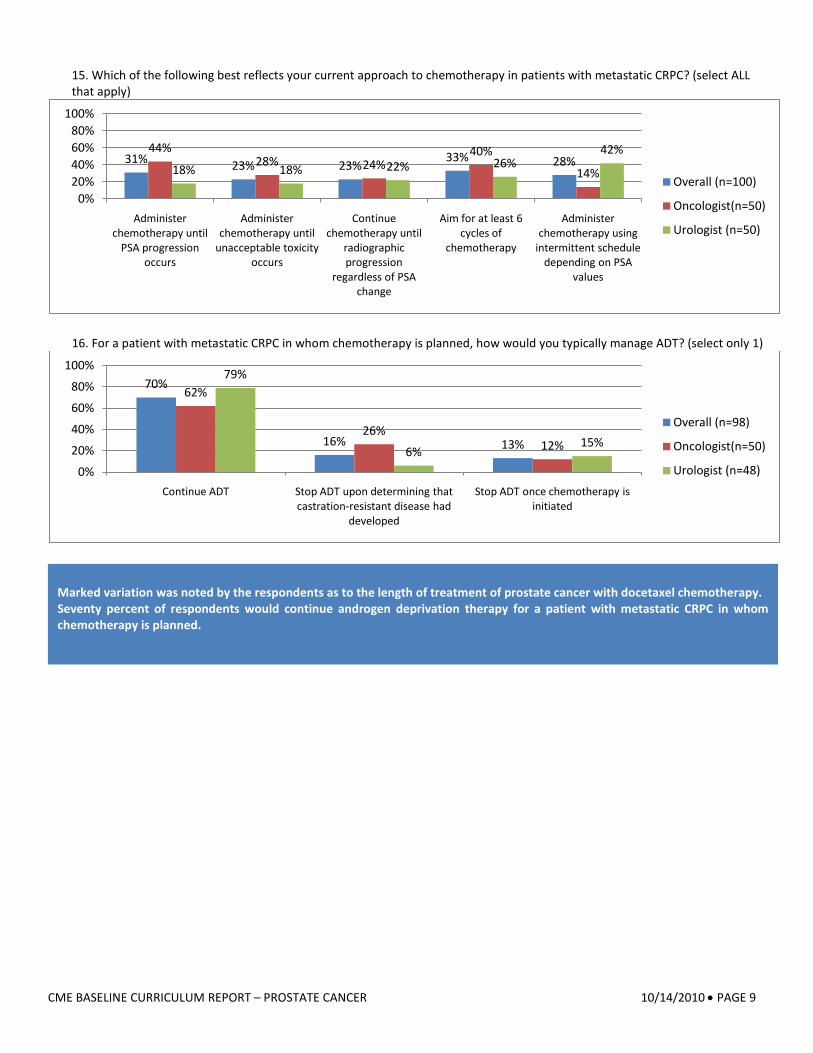
15. Which of the following best reflects your current approach to chemotherapy in patients with metastatic CRPC? (select ALL that apply)
16. For a patient with metastatic CRPC in whom chemotherapy is planned, how would you typically manage ADT? (select only 1)
31% 23% 23%33% 28%
44%28% 24%
40%
14%18% 18% 22% 26%42%
0%20%40%60%80%
100%
Administer chemotherapy until
PSA progression occurs
Administer chemotherapy until
unacceptable toxicity occurs
Continue chemotherapy until
radiographic progression
regardless of PSA change
Aim for at least 6 cycles of
chemotherapy
Administer chemotherapy using
intermittent schedule depending on PSA
values
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
70%
16% 13%
62%
26%12%
79%
6%15%
0%
20%
40%
60%
80%
100%
Continue ADT Stop ADT upon determining that castration-resistant disease had
developed
Stop ADT once chemotherapy is initiated
Overall (n=98)
Oncologist(n=50)
Urologist (n=48)
Marked variation was noted by the respondents as to the length of treatment of prostate cancer with docetaxel chemotherapy. Seventy percent of respondents would continue androgen deprivation therapy for a patient with metastatic CRPC in whom chemotherapy is planned.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 10
III. Maintenance of Bone Health
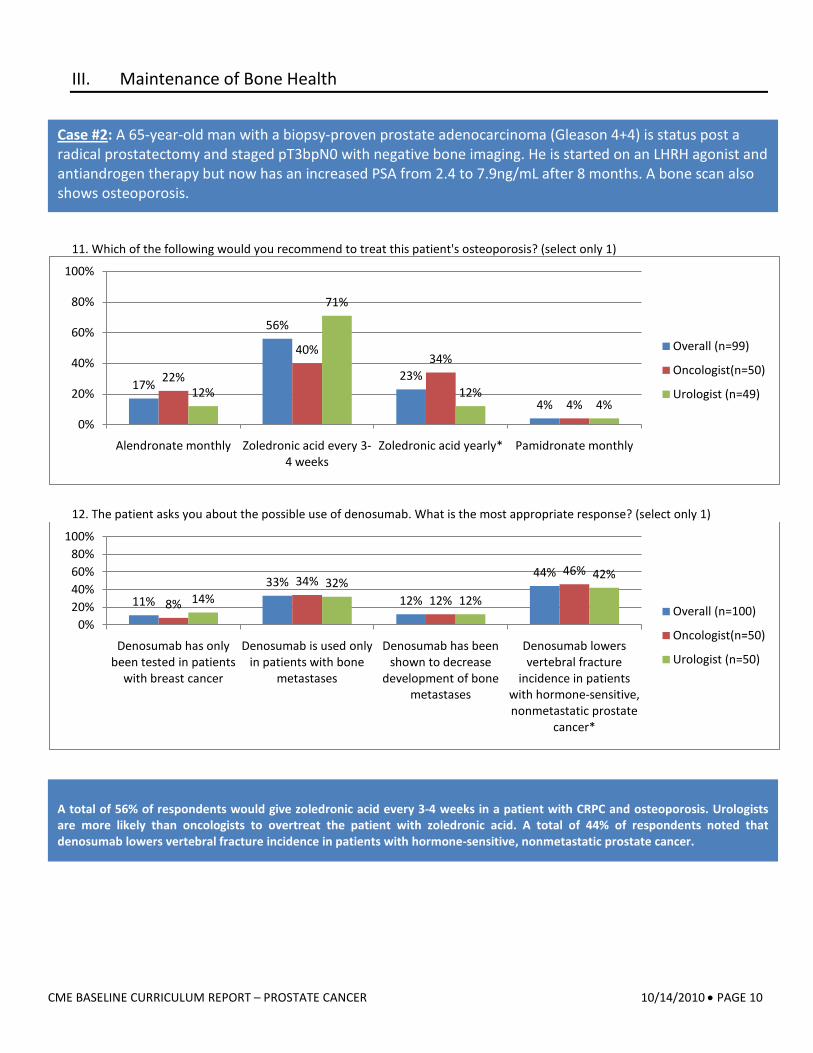
11. Which of the following would you recommend to treat this patient's osteoporosis? (select only 1)
12. The patient asks you about the possible use of denosumab. What is the most appropriate response? (select only 1)
17%
56%
23%
4%
22%
40%34%
4%12%
71%
12%4%
0%
20%
40%
60%
80%
100%
Alendronate monthly Zoledronic acid every 3-4 weeks
Zoledronic acid yearly* Pamidronate monthly
Overall (n=99)
Oncologist(n=50)
Urologist (n=49)
11%33%
12%
44%
8%
34%12%
46%
14%32%
12%
42%
0%20%40%60%80%
100%
Denosumab has only been tested in patients
with breast cancer
Denosumab is used only in patients with bone
metastases
Denosumab has been shown to decrease
development of bone metastases
Denosumab lowers vertebral fracture
incidence in patients with hormone-sensitive, nonmetastatic prostate
cancer*
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
A total of 56% of respondents would give zoledronic acid every 3-4 weeks in a patient with CRPC and osteoporosis. Urologists are more likely than oncologists to overtreat the patient with zoledronic acid. A total of 44% of respondents noted that denosumab lowers vertebral fracture incidence in patients with hormone-sensitive, nonmetastatic prostate cancer.
Case #2: A 65-year-old man with a biopsy-proven prostate adenocarcinoma (Gleason 4+4) is status post a radical prostatectomy and staged pT3bpN0 with negative bone imaging. He is started on an LHRH agonist and antiandrogen therapy but now has an increased PSA from 2.4 to 7.9ng/mL after 8 months. A bone scan also shows osteoporosis.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 11
IV. Emerging Therapies
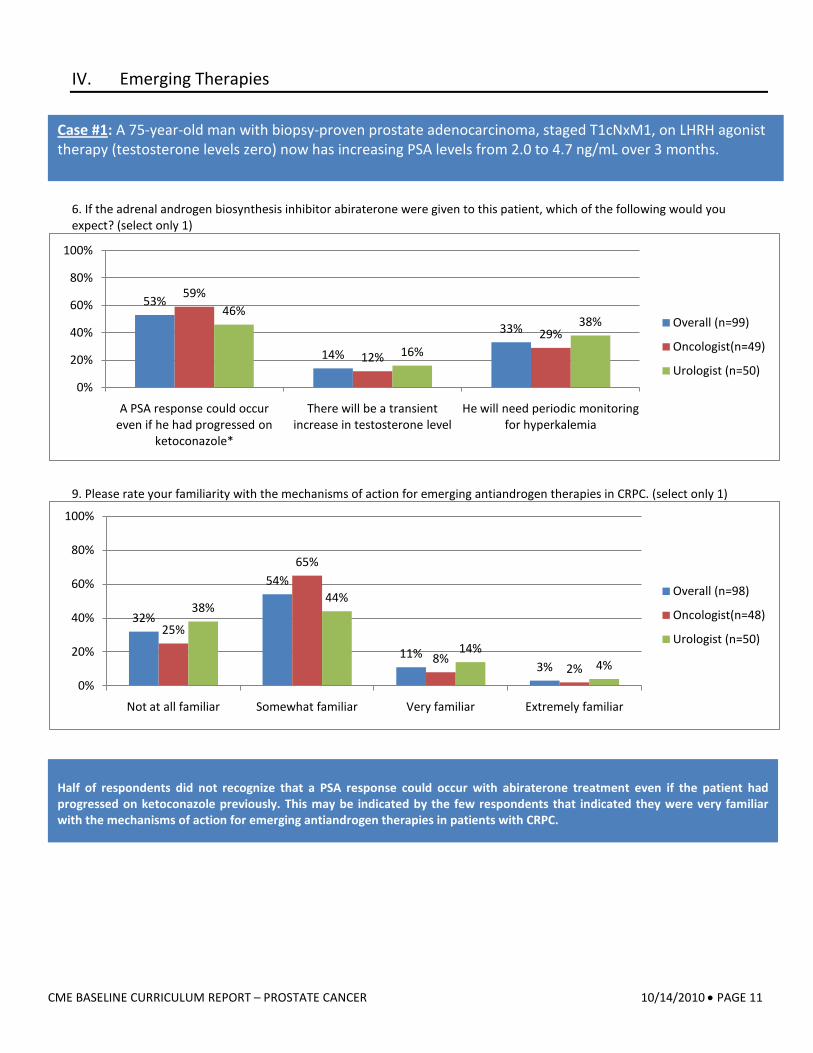
6. If the adrenal androgen biosynthesis inhibitor abiraterone were given to this patient, which of the following would you expect? (select only 1)
9. Please rate your familiarity with the mechanisms of action for emerging antiandrogen therapies in CRPC. (select only 1)
53%
14%
33%
59%
12%
29%
46%
16%
38%
0%
20%
40%
60%
80%
100%
A PSA response could occur even if he had progressed on
ketoconazole*
There will be a transient increase in testosterone level
He will need periodic monitoring for hyperkalemia
Overall (n=99)
Oncologist(n=49)
Urologist (n=50)
32%
54%
11%3%
25%
65%
8%2%
38%44%
14%4%
0%
20%
40%
60%
80%
100%
Not at all familiar Somewhat familiar Very familiar Extremely familiar
Overall (n=98)
Oncologist(n=48)
Urologist (n=50)
Half of respondents did not recognize that a PSA response could occur with abiraterone treatment even if the patient had progressed on ketoconazole previously. This may be indicated by the few respondents that indicated they were very familiar with the mechanisms of action for emerging antiandrogen therapies in patients with CRPC.
Case #1: A 75-year-old man with biopsy-proven prostate adenocarcinoma, staged T1cNxM1, on LHRH agonist therapy (testosterone levels zero) now has increasing PSA levels from 2.0 to 4.7 ng/mL over 3 months.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 12
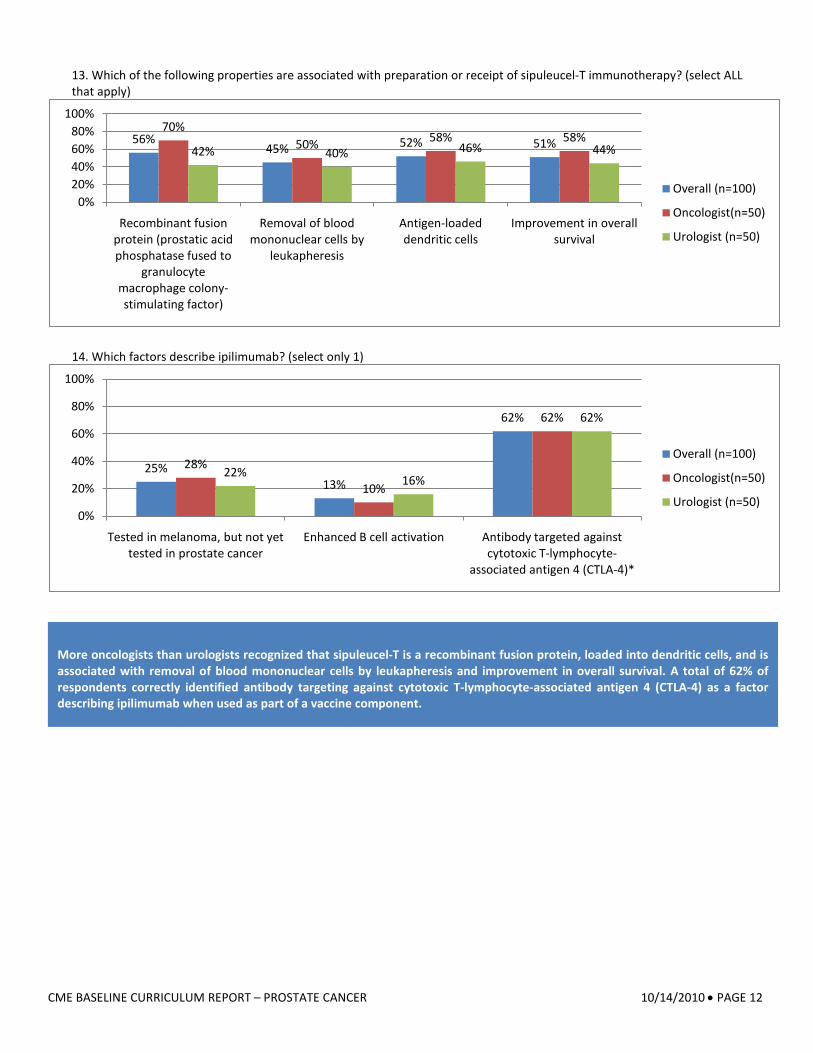
13. Which of the following properties are associated with preparation or receipt of sipuleucel-T immunotherapy? (select ALL that apply)
14. Which factors describe ipilimumab? (select only 1)
56%45% 52% 51%
70%50% 58% 58%
42% 40% 46% 44%
0%20%40%60%80%
100%
Recombinant fusion protein (prostatic acid phosphatase fused to
granulocyte macrophage colony-stimulating factor)
Removal of blood mononuclear cells by
leukapheresis
Antigen-loaded dendritic cells
Improvement in overall survival
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
25%13%
62%
28%
10%
62%
22% 16%
62%
0%
20%
40%
60%
80%
100%
Tested in melanoma, but not yet tested in prostate cancer
Enhanced B cell activation Antibody targeted against cytotoxic T-lymphocyte-
associated antigen 4 (CTLA-4)*
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
More oncologists than urologists recognized that sipuleucel-T is a recombinant fusion protein, loaded into dendritic cells, and is associated with removal of blood mononuclear cells by leukapheresis and improvement in overall survival. A total of 62% of respondents correctly identified antibody targeting against cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) as a factor describing ipilimumab when used as part of a vaccine component.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 13
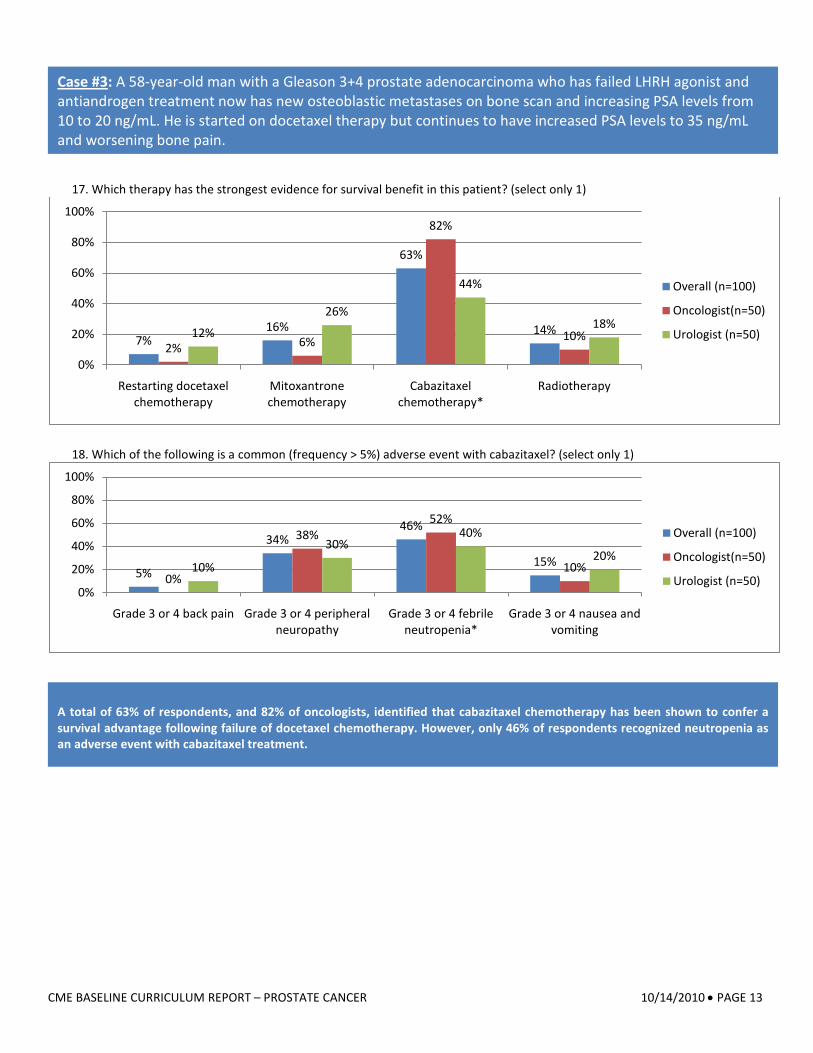
17. Which therapy has the strongest evidence for survival benefit in this patient? (select only 1)
18. Which of the following is a common (frequency > 5%) adverse event with cabazitaxel? (select only 1)
7%16%
63%
14%2% 6%
82%
10%12%
26%
44%
18%
0%
20%
40%
60%
80%
100%
Restarting docetaxel chemotherapy
Mitoxantrone chemotherapy
Cabazitaxel chemotherapy*
Radiotherapy
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
5%
34%46%
15%0%
38%52%
10%10%
30%40%
20%
0%
20%
40%
60%
80%
100%
Grade 3 or 4 back pain Grade 3 or 4 peripheral neuropathy
Grade 3 or 4 febrile neutropenia*
Grade 3 or 4 nausea and vomiting
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
A total of 63% of respondents, and 82% of oncologists, identified that cabazitaxel chemotherapy has been shown to confer a survival advantage following failure of docetaxel chemotherapy. However, only 46% of respondents recognized neutropenia as an adverse event with cabazitaxel treatment.
Case #3: A 58-year-old man with a Gleason 3+4 prostate adenocarcinoma who has failed LHRH agonist and antiandrogen treatment now has new osteoblastic metastases on bone scan and increasing PSA levels from 10 to 20 ng/mL. He is started on docetaxel therapy but continues to have increased PSA levels to 35 ng/mL and worsening bone pain.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 14
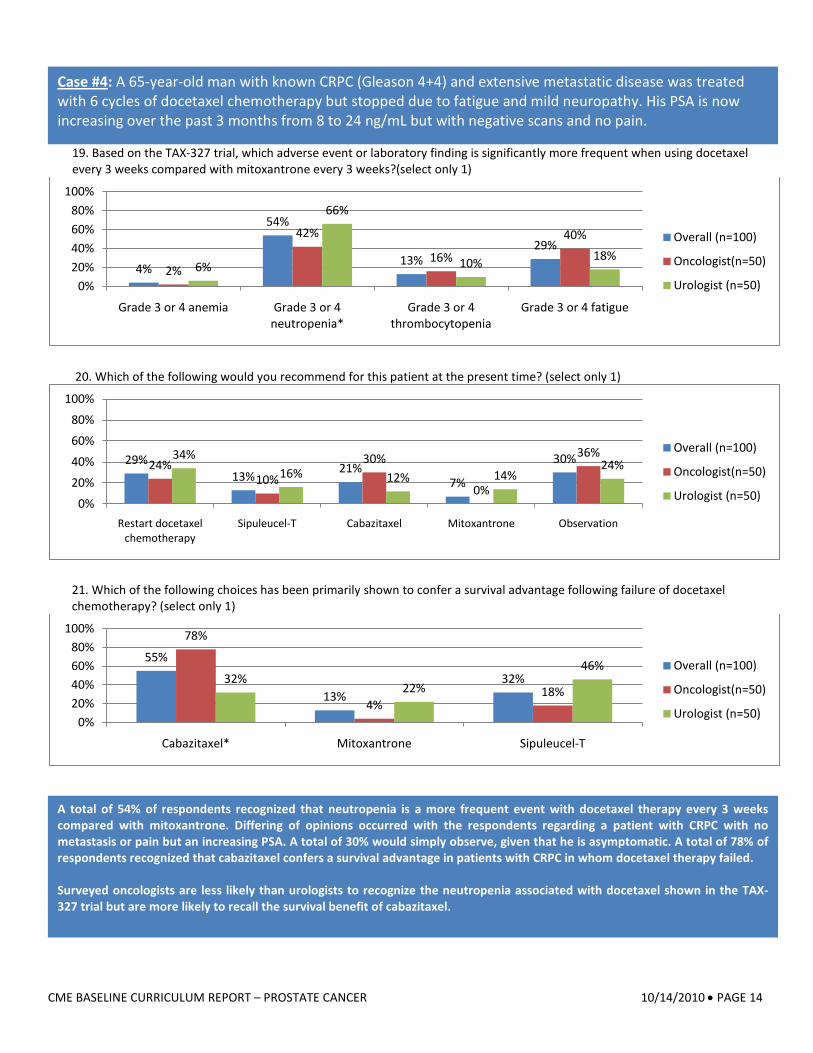
19. Based on the TAX-327 trial, which adverse event or laboratory finding is significantly more frequent when using docetaxel every 3 weeks compared with mitoxantrone every 3 weeks?(select only 1)
20. Which of the following would you recommend for this patient at the present time? (select only 1)
21. Which of the following choices has been primarily shown to confer a survival advantage following failure of docetaxel chemotherapy? (select only 1)
4%
54%
13%29%
2%
42%
16%
40%
6%
66%
10% 18%
0%20%40%60%80%
100%
Grade 3 or 4 anemia Grade 3 or 4 neutropenia*
Grade 3 or 4 thrombocytopenia
Grade 3 or 4 fatigue
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
29%13%
21%7%
30%24%10%
30%
0%
36%34%16% 12% 14%
24%
0%
20%
40%
60%
80%
100%
Restart docetaxel chemotherapy
Sipuleucel-T Cabazitaxel Mitoxantrone Observation
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
55%
13%32%
78%
4%18%
32%22%
46%
0%20%40%60%80%
100%
Cabazitaxel* Mitoxantrone Sipuleucel-T
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
A total of 54% of respondents recognized that neutropenia is a more frequent event with docetaxel therapy every 3 weeks compared with mitoxantrone. Differing of opinions occurred with the respondents regarding a patient with CRPC with no metastasis or pain but an increasing PSA. A total of 30% would simply observe, given that he is asymptomatic. A total of 78% of respondents recognized that cabazitaxel confers a survival advantage in patients with CRPC in whom docetaxel therapy failed. Surveyed oncologists are less likely than urologists to recognize the neutropenia associated with docetaxel shown in the TAX-327 trial but are more likely to recall the survival benefit of cabazitaxel.
Case #4: A 65-year-old man with known CRPC (Gleason 4+4) and extensive metastatic disease was treated with 6 cycles of docetaxel chemotherapy but stopped due to fatigue and mild neuropathy. His PSA is now increasing over the past 3 months from 8 to 24 ng/mL but with negative scans and no pain.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 15
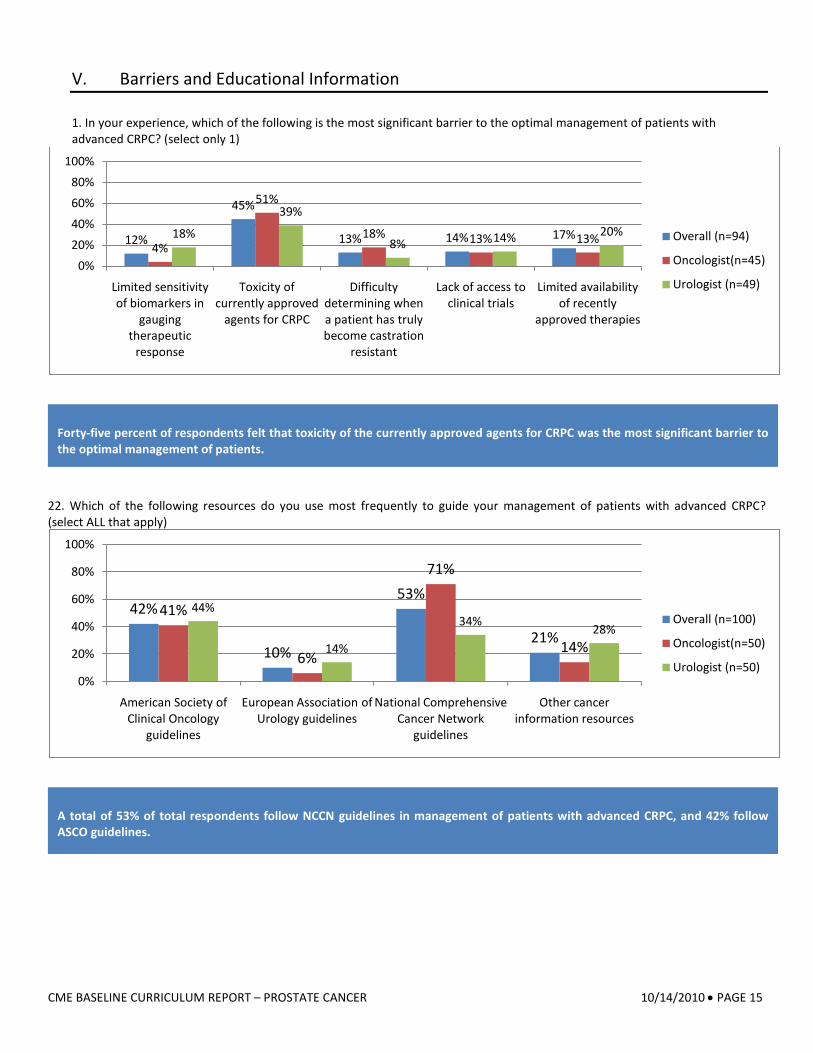
V. Barriers and Educational Information 1. In your experience, which of the following is the most significant barrier to the optimal management of patients with advanced CRPC? (select only 1)
22. Which of the following resources do you use most frequently to guide your management of patients with advanced CRPC? (select ALL that apply)
12%
45%
13% 14% 17%4%
51%
18% 13% 13%18%
39%
8% 14% 20%
0%20%40%60%80%
100%
Limited sensitivity of biomarkers in
gauging therapeutic
response
Toxicity of currently approved
agents for CRPC
Difficulty determining when a patient has truly become castration
resistant
Lack of access to clinical trials
Limited availability of recently
approved therapies
Overall (n=94)
Oncologist(n=45)
Urologist (n=49)
42%
10%
53%
21%
41%
6%
71%
14%
44%
14%
34% 28%
0%
20%
40%
60%
80%
100%
American Society of Clinical Oncology
guidelines
European Association of Urology guidelines
National Comprehensive Cancer Network
guidelines
Other cancer information resources
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
A total of 53% of total respondents follow NCCN guidelines in management of patients with advanced CRPC, and 42% follow ASCO guidelines.
Forty-five percent of respondents felt that toxicity of the currently approved agents for CRPC was the most significant barrier to the optimal management of patients.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 16
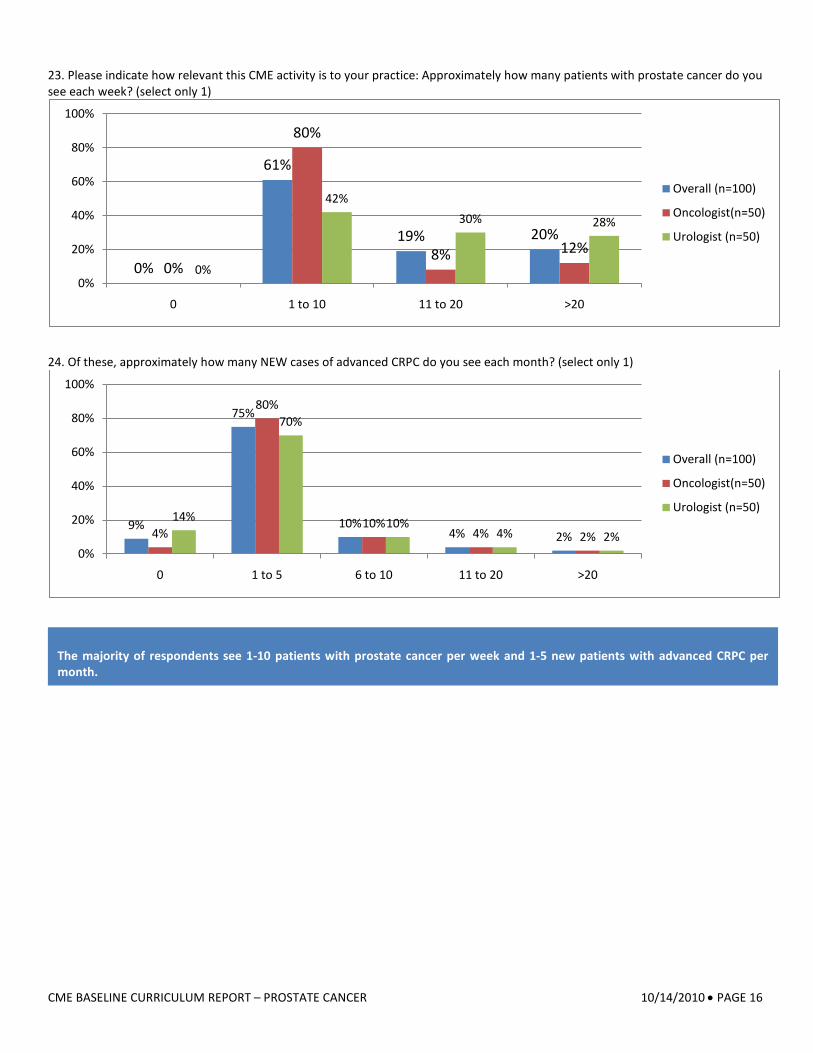
23. Please indicate how relevant this CME activity is to your practice: Approximately how many patients with prostate cancer do you see each week? (select only 1)
24. Of these, approximately how many NEW cases of advanced CRPC do you see each month? (select only 1)
0%
61%
19% 20%
0%
80%
8% 12%0%
42%30% 28%
0%
20%
40%
60%
80%
100%
0 1 to 10 11 to 20 >20
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
9%
75%
10%4% 2%4%
80%
10%4% 2%
14%
70%
10%4% 2%
0%
20%
40%
60%
80%
100%
0 1 to 5 6 to 10 11 to 20 >20
Overall (n=100)
Oncologist(n=50)
Urologist (n=50)
The majority of respondents see 1-10 patients with prostate cancer per week and 1-5 new patients with advanced CRPC per month.
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 17
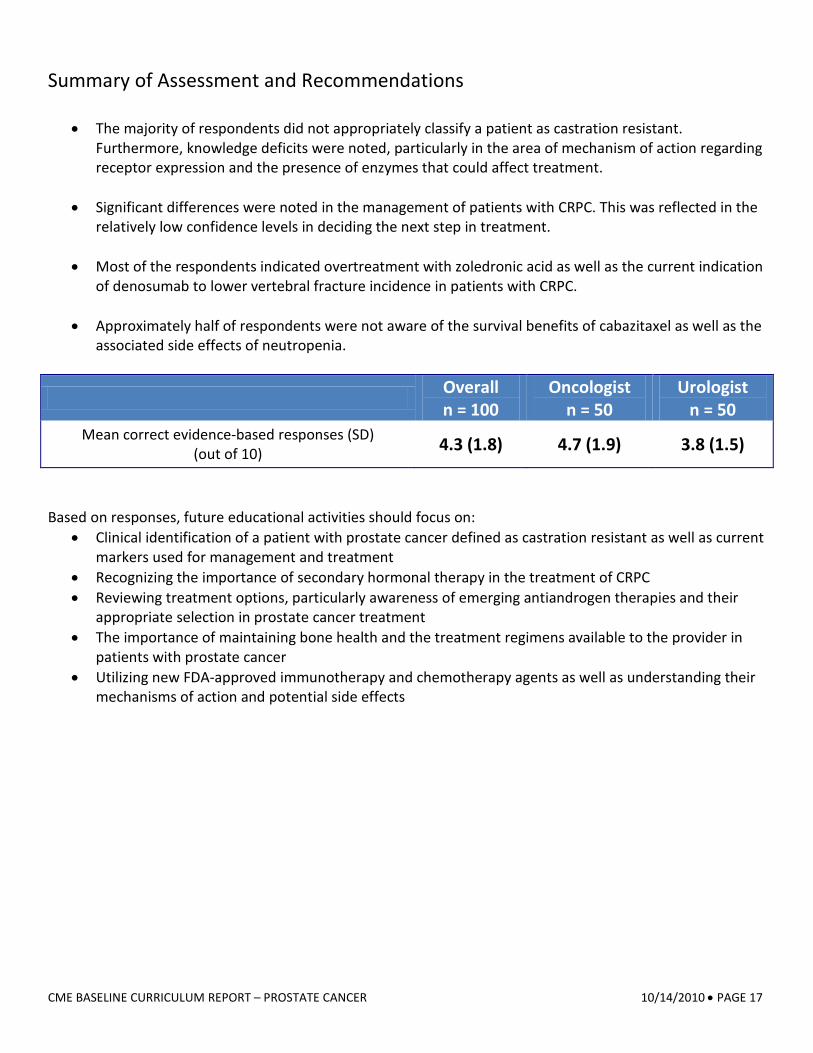
Summary of Assessment and Recommendations
• The majority of respondents did not appropriately classify a patient as castration resistant. Furthermore, knowledge deficits were noted, particularly in the area of mechanism of action regarding receptor expression and the presence of enzymes that could affect treatment.
• Significant differences were noted in the management of patients with CRPC. This was reflected in the
relatively low confidence levels in deciding the next step in treatment.
• Most of the respondents indicated overtreatment with zoledronic acid as well as the current indication of denosumab to lower vertebral fracture incidence in patients with CRPC.
• Approximately half of respondents were not aware of the survival benefits of cabazitaxel as well as the
associated side effects of neutropenia.
Overall n = 100
Oncologist n = 50
Urologist n = 50
Mean correct evidence-based responses (SD) (out of 10) 4.3 (1.8) 4.7 (1.9) 3.8 (1.5)
Based on responses, future educational activities should focus on:
• Clinical identification of a patient with prostate cancer defined as castration resistant as well as current markers used for management and treatment
• Recognizing the importance of secondary hormonal therapy in the treatment of CRPC • Reviewing treatment options, particularly awareness of emerging antiandrogen therapies and their
appropriate selection in prostate cancer treatment • The importance of maintaining bone health and the treatment regimens available to the provider in
patients with prostate cancer • Utilizing new FDA-approved immunotherapy and chemotherapy agents as well as understanding their
mechanisms of action and potential side effects
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 18
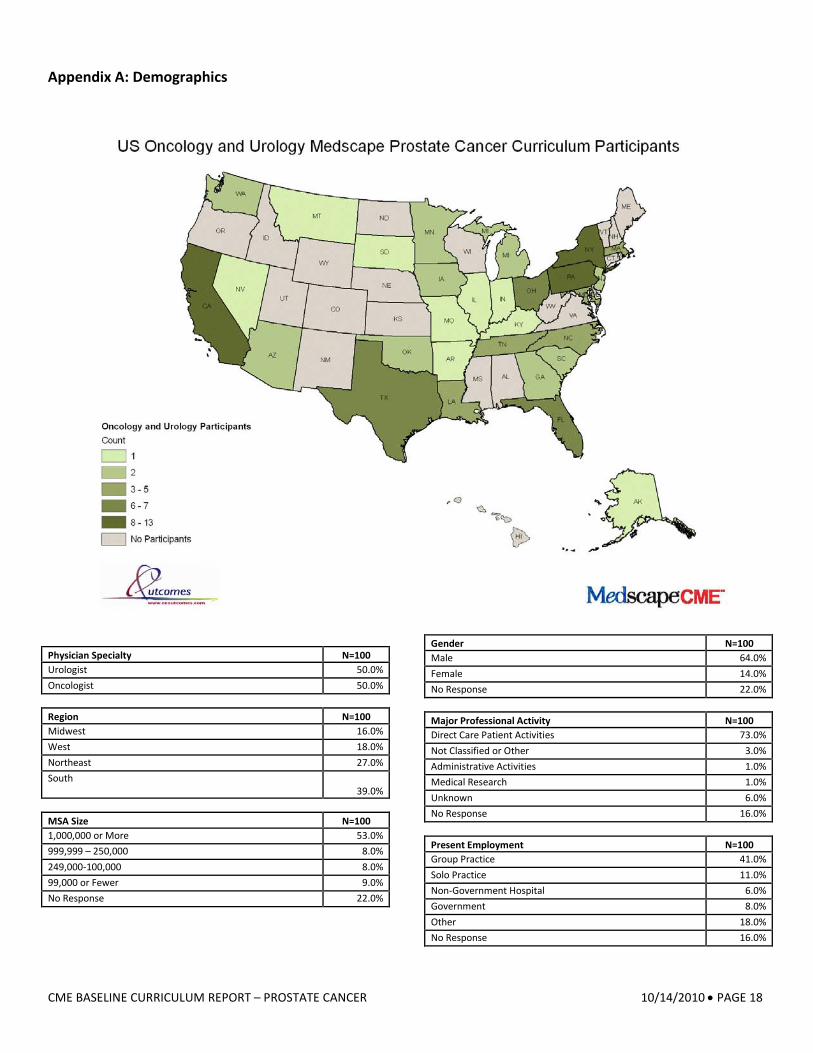
Appendix A: Demographics
Physician Specialty N=100 Urologist 50.0% Oncologist 50.0% Region N=100 Midwest 16.0% West 18.0% Northeast 27.0% South
39.0% MSA Size N=100 1,000,000 or More 53.0% 999,999 – 250,000 8.0% 249,000-100,000 8.0% 99,000 or Fewer 9.0% No Response 22.0%
Gender N=100 Male 64.0% Female 14.0% No Response 22.0% Major Professional Activity N=100 Direct Care Patient Activities 73.0% Not Classified or Other 3.0% Administrative Activities 1.0% Medical Research 1.0% Unknown 6.0% No Response 16.0%
Present Employment N=100 Group Practice 41.0% Solo Practice 11.0% Non-Government Hospital 6.0% Government 8.0% Other 18.0% No Response 16.0%
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 19
Appendix B: Full Cases and Data Tables Assessment Survey
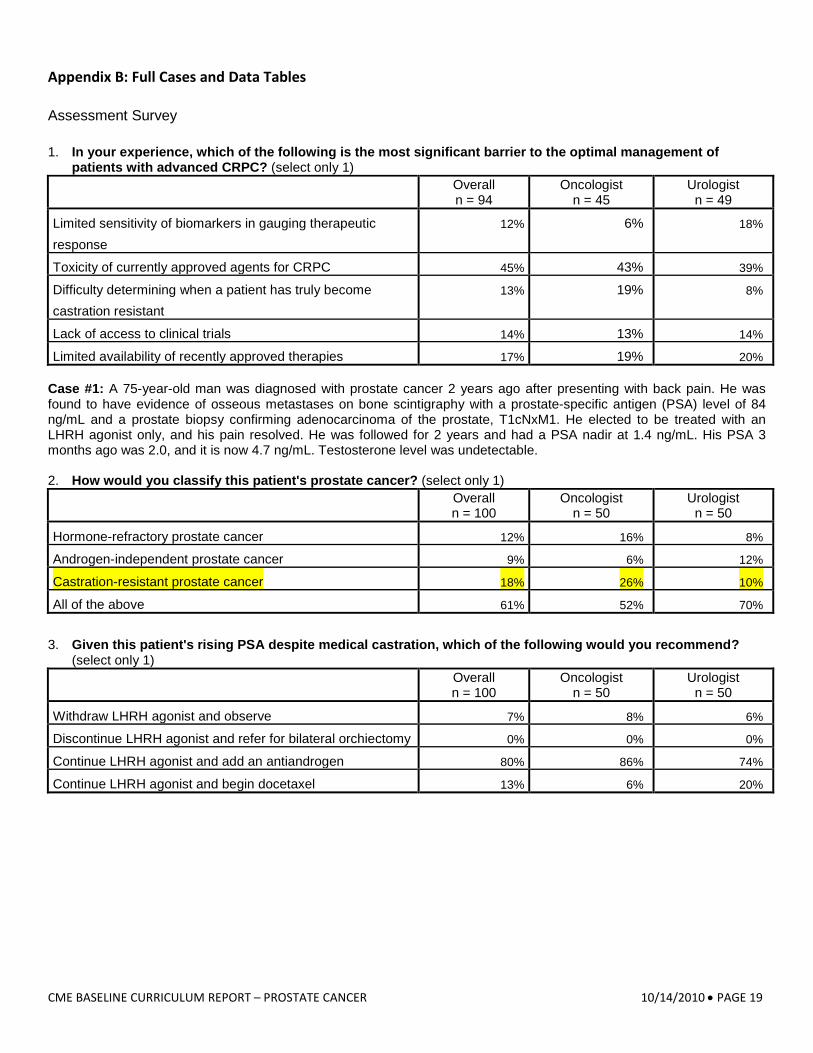
1. In your experience, which of the following is the most significant barrier to the optimal management of patients with advanced CRPC? (select only 1)
Overall n = 94
Oncologist n = 45
Urologist n = 49
Limited sensitivity of biomarkers in gauging therapeutic response
12% 6% 18%
Toxicity of currently approved agents for CRPC 45% 43% 39%
Difficulty determining when a patient has truly become castration resistant
13% 19% 8%
Lack of access to clinical trials 14% 13% 14%
Limited availability of recently approved therapies 17% 19% 20% Case #1: A 75-year-old man was diagnosed with prostate cancer 2 years ago after presenting with back pain. He was found to have evidence of osseous metastases on bone scintigraphy with a prostate-specific antigen (PSA) level of 84 ng/mL and a prostate biopsy confirming adenocarcinoma of the prostate, T1cNxM1. He elected to be treated with an LHRH agonist only, and his pain resolved. He was followed for 2 years and had a PSA nadir at 1.4 ng/mL. His PSA 3 months ago was 2.0, and it is now 4.7 ng/mL. Testosterone level was undetectable. 2. How would you classify this patient's prostate cancer? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Hormone-refractory prostate cancer 12% 16% 8%
Androgen-independent prostate cancer 9% 6% 12%
Castration-resistant prostate cancer 18% 26% 10%
All of the above 61% 52% 70%
3. Given this patient's rising PSA despite medical castration, which of the following would you recommend? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Withdraw LHRH agonist and observe 7% 8% 6%
Discontinue LHRH agonist and refer for bilateral orchiectomy 0% 0% 0%
Continue LHRH agonist and add an antiandrogen 80% 86% 74%
Continue LHRH agonist and begin docetaxel 13% 6% 20%
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 20
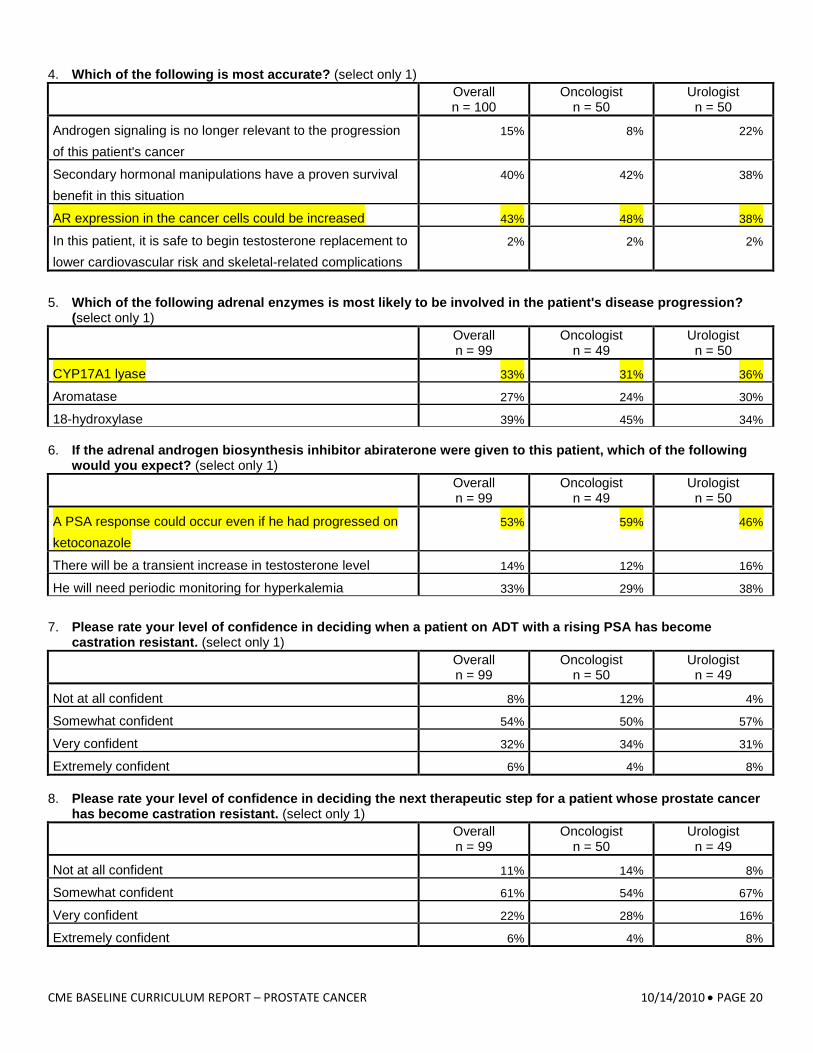
4. Which of the following is most accurate? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Androgen signaling is no longer relevant to the progression of this patient's cancer
15% 8% 22%
Secondary hormonal manipulations have a proven survival benefit in this situation
40% 42% 38%
AR expression in the cancer cells could be increased 43% 48% 38%
In this patient, it is safe to begin testosterone replacement to lower cardiovascular risk and skeletal-related complications
2% 2% 2%
5. Which of the following adrenal enzymes is most likely to be involved in the patient's disease progression? (select only 1)
Overall n = 99
Oncologist n = 49
Urologist n = 50
CYP17A1 lyase 33% 31% 36%
Aromatase 27% 24% 30%
18-hydroxylase 39% 45% 34% 6. If the adrenal androgen biosynthesis inhibitor abiraterone were given to this patient, which of the following
would you expect? (select only 1)
Overall n = 99
Oncologist n = 49
Urologist n = 50
A PSA response could occur even if he had progressed on ketoconazole
53% 59% 46%
There will be a transient increase in testosterone level 14% 12% 16%
He will need periodic monitoring for hyperkalemia 33% 29% 38%
7. Please rate your level of confidence in deciding when a patient on ADT with a rising PSA has become castration resistant. (select only 1)
Overall n = 99
Oncologist n = 50
Urologist n = 49
Not at all confident 8% 12% 4%
Somewhat confident 54% 50% 57%
Very confident 32% 34% 31%
Extremely confident 6% 4% 8% 8. Please rate your level of confidence in deciding the next therapeutic step for a patient whose prostate cancer
has become castration resistant. (select only 1)
Overall n = 99
Oncologist n = 50
Urologist n = 49
Not at all confident 11% 14% 8%
Somewhat confident 61% 54% 67%
Very confident 22% 28% 16%
Extremely confident 6% 4% 8%
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 21
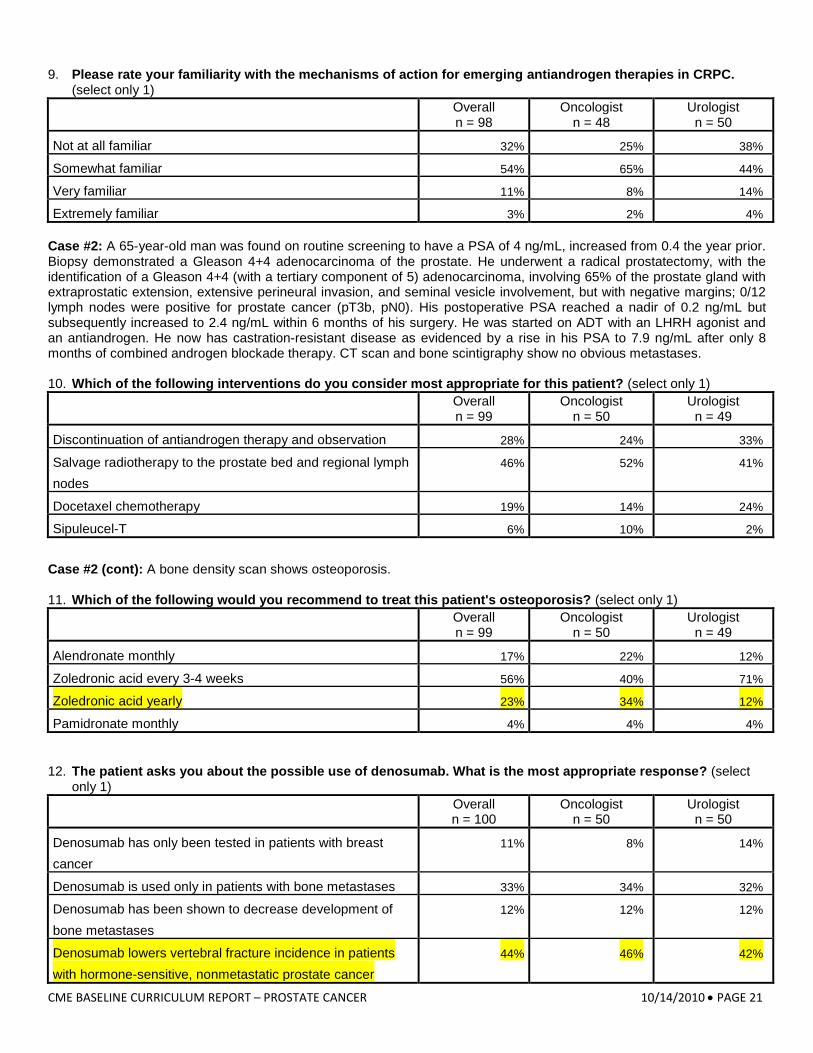
9. Please rate your familiarity with the mechanisms of action for emerging antiandrogen therapies in CRPC. (select only 1)
Overall n = 98
Oncologist n = 48
Urologist n = 50
Not at all familiar 32% 25% 38%
Somewhat familiar 54% 65% 44%
Very familiar 11% 8% 14%
Extremely familiar 3% 2% 4% Case #2: A 65-year-old man was found on routine screening to have a PSA of 4 ng/mL, increased from 0.4 the year prior. Biopsy demonstrated a Gleason 4+4 adenocarcinoma of the prostate. He underwent a radical prostatectomy, with the identification of a Gleason 4+4 (with a tertiary component of 5) adenocarcinoma, involving 65% of the prostate gland with extraprostatic extension, extensive perineural invasion, and seminal vesicle involvement, but with negative margins; 0/12 lymph nodes were positive for prostate cancer (pT3b, pN0). His postoperative PSA reached a nadir of 0.2 ng/mL but subsequently increased to 2.4 ng/mL within 6 months of his surgery. He was started on ADT with an LHRH agonist and an antiandrogen. He now has castration-resistant disease as evidenced by a rise in his PSA to 7.9 ng/mL after only 8 months of combined androgen blockade therapy. CT scan and bone scintigraphy show no obvious metastases. 10. Which of the following interventions do you consider most appropriate for this patient? (select only 1)
Overall n = 99
Oncologist n = 50
Urologist n = 49
Discontinuation of antiandrogen therapy and observation 28% 24% 33%
Salvage radiotherapy to the prostate bed and regional lymph nodes
46% 52% 41%
Docetaxel chemotherapy 19% 14% 24%
Sipuleucel-T 6% 10% 2%
Case #2 (cont): A bone density scan shows osteoporosis. 11. Which of the following would you recommend to treat this patient's osteoporosis? (select only 1)
Overall n = 99
Oncologist n = 50
Urologist n = 49
Alendronate monthly 17% 22% 12%
Zoledronic acid every 3-4 weeks 56% 40% 71%
Zoledronic acid yearly 23% 34% 12%
Pamidronate monthly 4% 4% 4% 12. The patient asks you about the possible use of denosumab. What is the most appropriate response? (select
only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Denosumab has only been tested in patients with breast cancer
11% 8% 14%
Denosumab is used only in patients with bone metastases 33% 34% 32%
Denosumab has been shown to decrease development of bone metastases
12% 12% 12%
Denosumab lowers vertebral fracture incidence in patients with hormone-sensitive, nonmetastatic prostate cancer
44% 46% 42%
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 22
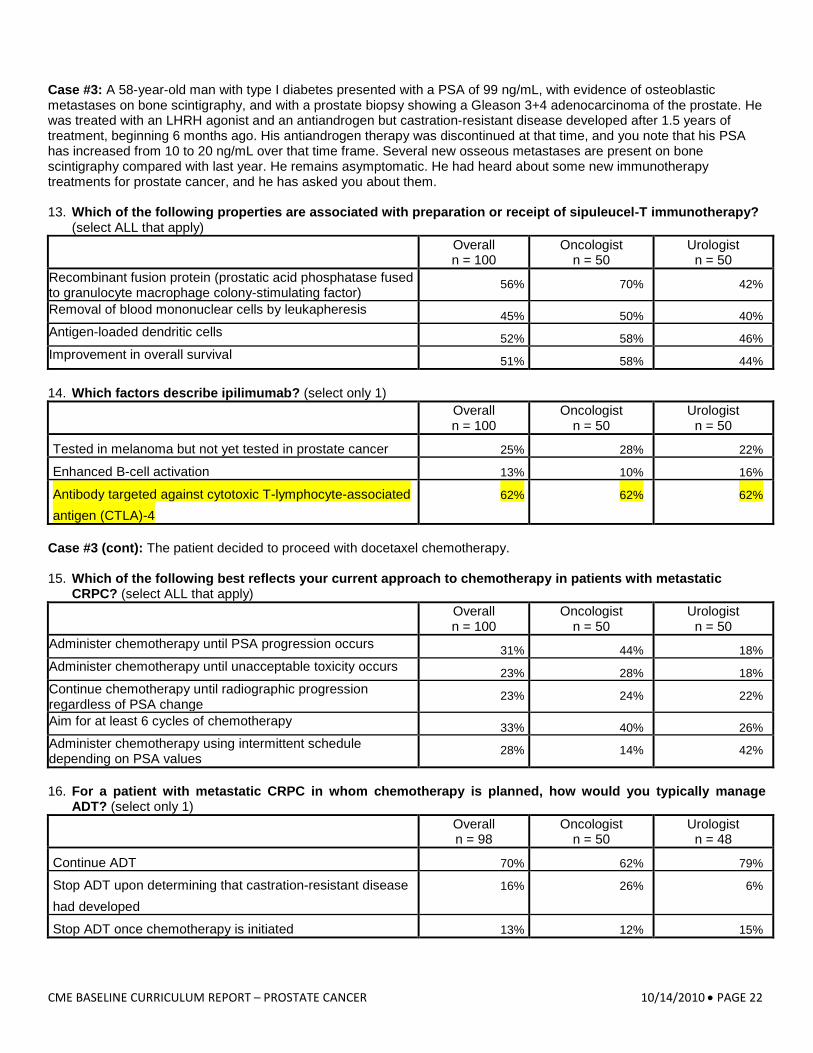
Case #3: A 58-year-old man with type I diabetes presented with a PSA of 99 ng/mL, with evidence of osteoblastic metastases on bone scintigraphy, and with a prostate biopsy showing a Gleason 3+4 adenocarcinoma of the prostate. He was treated with an LHRH agonist and an antiandrogen but castration-resistant disease developed after 1.5 years of treatment, beginning 6 months ago. His antiandrogen therapy was discontinued at that time, and you note that his PSA has increased from 10 to 20 ng/mL over that time frame. Several new osseous metastases are present on bone scintigraphy compared with last year. He remains asymptomatic. He had heard about some new immunotherapy treatments for prostate cancer, and he has asked you about them. 13. Which of the following properties are associated with preparation or receipt of sipuleucel-T immunotherapy?
(select ALL that apply)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Recombinant fusion protein (prostatic acid phosphatase fused to granulocyte macrophage colony-stimulating factor)
56% 70% 42%
Removal of blood mononuclear cells by leukapheresis 45% 50% 40% Antigen-loaded dendritic cells 52% 58% 46% Improvement in overall survival 51% 58% 44% 14. Which factors describe ipilimumab? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Tested in melanoma but not yet tested in prostate cancer 25% 28% 22%
Enhanced B-cell activation 13% 10% 16%
Antibody targeted against cytotoxic T-lymphocyte-associated antigen (CTLA)-4
62% 62% 62%
Case #3 (cont): The patient decided to proceed with docetaxel chemotherapy. 15. Which of the following best reflects your current approach to chemotherapy in patients with metastatic
CRPC? (select ALL that apply)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Administer chemotherapy until PSA progression occurs 31% 44% 18% Administer chemotherapy until unacceptable toxicity occurs 23% 28% 18% Continue chemotherapy until radiographic progression regardless of PSA change
23% 24% 22%
Aim for at least 6 cycles of chemotherapy 33% 40% 26% Administer chemotherapy using intermittent schedule depending on PSA values
28% 14% 42%
16. For a patient with metastatic CRPC in whom chemotherapy is planned, how would you typically manage
ADT? (select only 1)
Overall n = 98
Oncologist n = 50
Urologist n = 48
Continue ADT 70% 62% 79%
Stop ADT upon determining that castration-resistant disease had developed
16% 26% 6%
Stop ADT once chemotherapy is initiated 13% 12% 15%
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 23
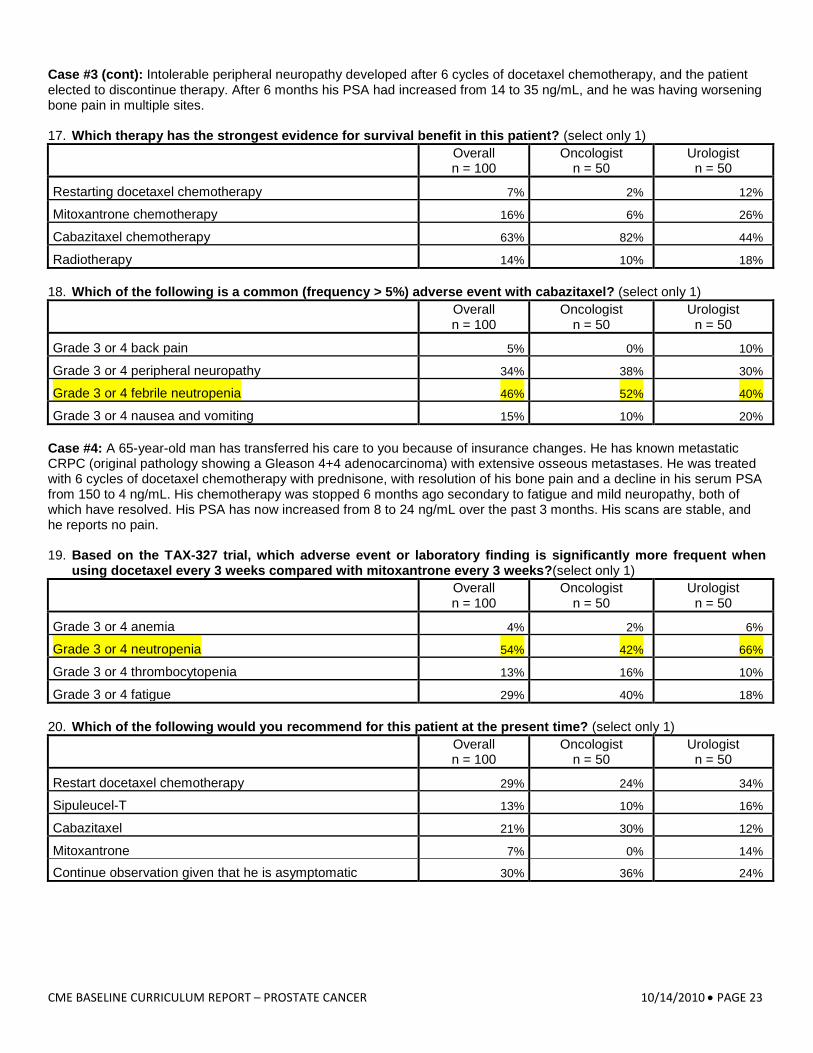
Case #3 (cont): Intolerable peripheral neuropathy developed after 6 cycles of docetaxel chemotherapy, and the patient elected to discontinue therapy. After 6 months his PSA had increased from 14 to 35 ng/mL, and he was having worsening bone pain in multiple sites. 17. Which therapy has the strongest evidence for survival benefit in this patient? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Restarting docetaxel chemotherapy 7% 2% 12%
Mitoxantrone chemotherapy 16% 6% 26%
Cabazitaxel chemotherapy 63% 82% 44%
Radiotherapy 14% 10% 18% 18. Which of the following is a common (frequency > 5%) adverse event with cabazitaxel? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Grade 3 or 4 back pain 5% 0% 10%
Grade 3 or 4 peripheral neuropathy 34% 38% 30%
Grade 3 or 4 febrile neutropenia 46% 52% 40%
Grade 3 or 4 nausea and vomiting 15% 10% 20% Case #4: A 65-year-old man has transferred his care to you because of insurance changes. He has known metastatic CRPC (original pathology showing a Gleason 4+4 adenocarcinoma) with extensive osseous metastases. He was treated with 6 cycles of docetaxel chemotherapy with prednisone, with resolution of his bone pain and a decline in his serum PSA from 150 to 4 ng/mL. His chemotherapy was stopped 6 months ago secondary to fatigue and mild neuropathy, both of which have resolved. His PSA has now increased from 8 to 24 ng/mL over the past 3 months. His scans are stable, and he reports no pain. 19. Based on the TAX-327 trial, which adverse event or laboratory finding is significantly more frequent when
using docetaxel every 3 weeks compared with mitoxantrone every 3 weeks?(select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Grade 3 or 4 anemia 4% 2% 6%
Grade 3 or 4 neutropenia 54% 42% 66%
Grade 3 or 4 thrombocytopenia 13% 16% 10%
Grade 3 or 4 fatigue 29% 40% 18% 20. Which of the following would you recommend for this patient at the present time? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Restart docetaxel chemotherapy 29% 24% 34%
Sipuleucel-T 13% 10% 16%
Cabazitaxel 21% 30% 12%
Mitoxantrone 7% 0% 14%
Continue observation given that he is asymptomatic 30% 36% 24%
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 24
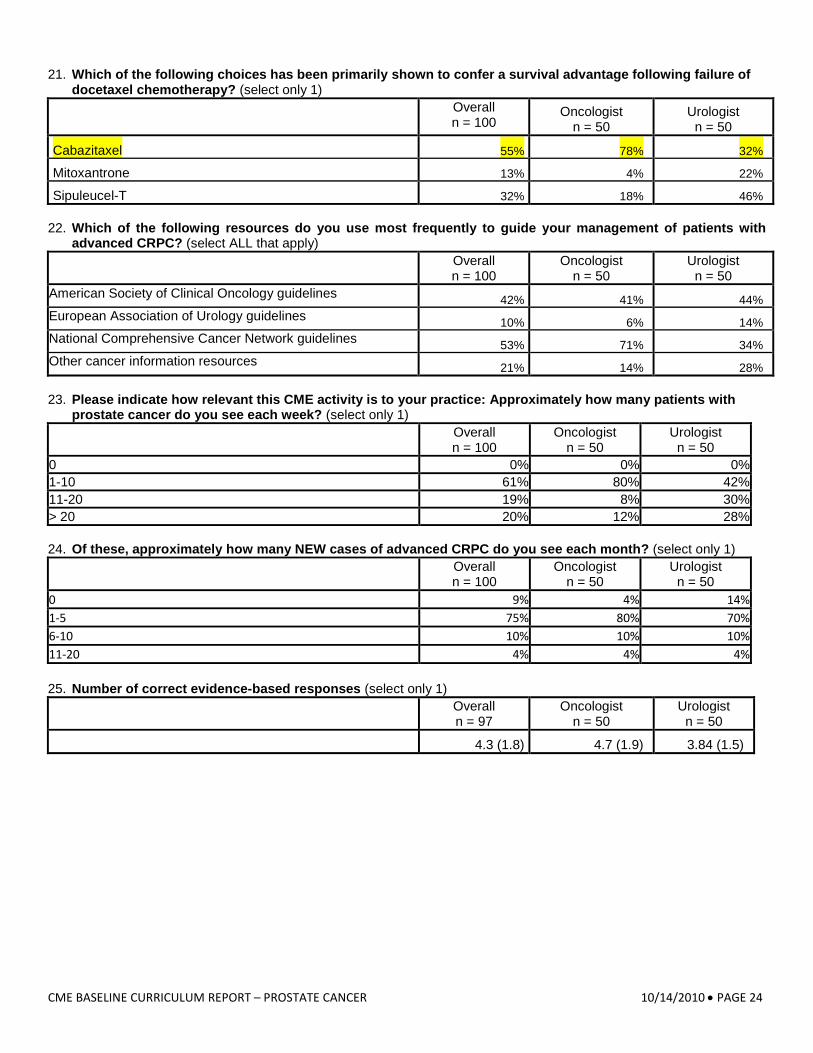
21. Which of the following choices has been primarily shown to confer a survival advantage following failure of docetaxel chemotherapy? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
Cabazitaxel 55% 78% 32%
Mitoxantrone 13% 4% 22%
Sipuleucel-T 32% 18% 46% 22. Which of the following resources do you use most frequently to guide your management of patients with
advanced CRPC? (select ALL that apply)
Overall n = 100
Oncologist n = 50
Urologist n = 50
American Society of Clinical Oncology guidelines 42% 41% 44% European Association of Urology guidelines 10% 6% 14% National Comprehensive Cancer Network guidelines 53% 71% 34% Other cancer information resources 21% 14% 28% 23. Please indicate how relevant this CME activity is to your practice: Approximately how many patients with
prostate cancer do you see each week? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
0 0% 0% 0% 1-10 61% 80% 42% 11-20 19% 8% 30% > 20 20% 12% 28% 24. Of these, approximately how many NEW cases of advanced CRPC do you see each month? (select only 1)
Overall n = 100
Oncologist n = 50
Urologist n = 50
0 9% 4% 14% 1-5 75% 80% 70% 6-10 10% 10% 10% 11-20 4% 4% 4% 25. Number of correct evidence-based responses (select only 1)
Overall n = 97
Oncologist n = 50
Urologist n = 50
4.3 (1.8) 4.7 (1.9) 3.84 (1.5)
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 25
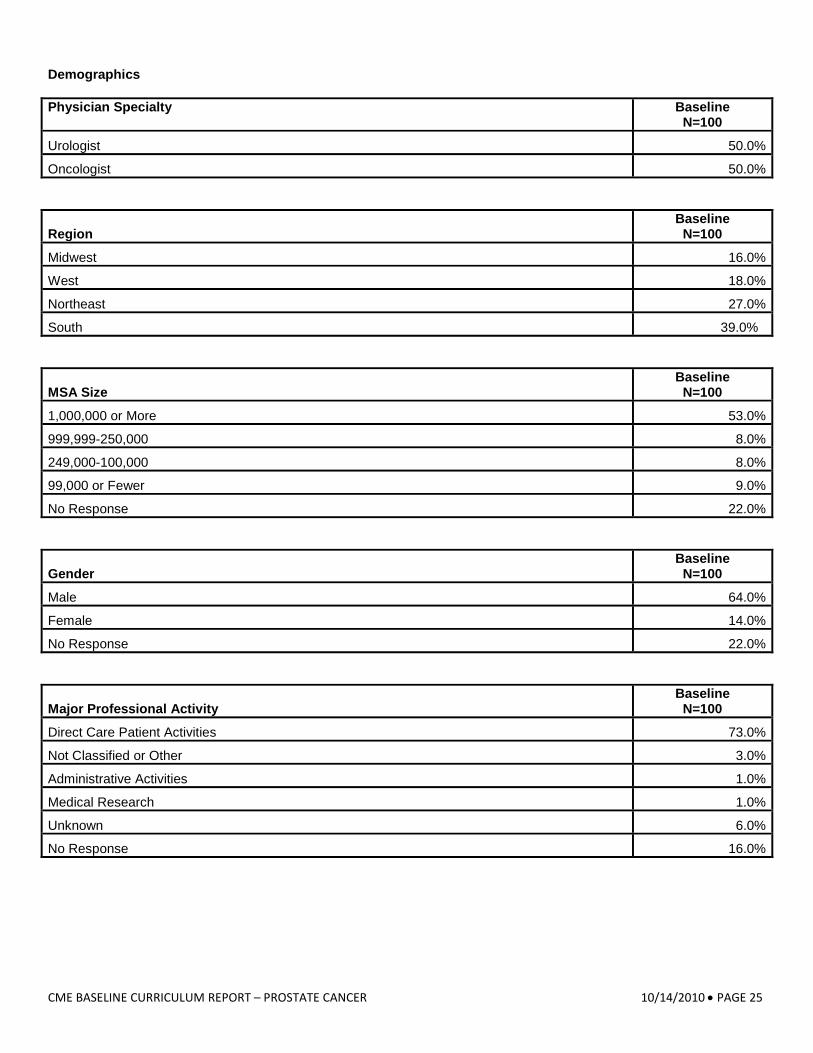
Demographics Physician Specialty
Baseline N=100
Urologist 50.0%
Oncologist 50.0%
Region Baseline
N=100
Midwest 16.0%
West 18.0%
Northeast 27.0%
South 39.0%
MSA Size Baseline
N=100
1,000,000 or More 53.0%
999,999-250,000 8.0%
249,000-100,000 8.0%
99,000 or Fewer 9.0%
No Response 22.0%
Gender Baseline
N=100
Male 64.0%
Female 14.0%
No Response 22.0%
Major Professional Activity Baseline
N=100
Direct Care Patient Activities 73.0%
Not Classified or Other 3.0%
Administrative Activities 1.0%
Medical Research 1.0%
Unknown 6.0%
No Response 16.0%
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 26
Present Employment Baseline
N=100
Group Practice 41.0%
Solo Practice 11.0%
Non-Government Hospital 6.0%
Government 8.0%
Other 18.0%
No Response 16.0%
CME BASELINE CURRICULUM REPORT – PROSTATE CANCER 10/14/2010 • PAGE 27
Appendix C: References
1. Peabody JW, Luck J, Glassman P, Dresselhaus TR, Lee M. Comparison of vignettes, standardized patients, and chart abstraction: a prospective validation study of 3 methods for measuring quality. JAMA. 2000,283:1715-1722.
2. Peabody JW, Luck J, Glassman P, et al. Measuring the quality of physician practice by using clinical vignettes: a prospective validation study. Ann Intern Med. 2004;141:771-780.
3. Scher HI, Halabi S, Tannock I, et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol. 2008;26:1148-1159.
4. National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology – v.2.2010. Prostate Cancer Early Detection. Available at: http://www.nccn.org/professionals/physician_gls/default.asp Accessed September 30, 2009 [registration required].
5. Mostaghel EA, Montgomery B, Nelson PS. Castration-resistant prostate cancer: targeting androgen metabolic pathways in recurrent disease. Urol Oncol.2009;27:251-257.
6. Szmulewitz RZ, Posadas EM, Manchen B, Stadler WM. A randomized, double-blind, placebo-controlled phase II study of testosterone replacement in men with asymptomatic castrate-resistant prostate cancer (PC). J Clin Oncol. 2010;28:15s. Abstract TPS241.
7. De Coster R, Wouters W, Bruynseels J. P450-dependent enzymes as targets for prostate cancer therapy. J Steroid Biochem Molec Biol. 1996;56:133-143.
8. Ryan CJ, Smith MR, Fong L, et al. Phase I clinical trial of the CYP17 inhibitor abiraterone acetate demonstrating clinical activity in patients with castration-resistant prostate cancer who received prior ketoconazole therapy. J Clin Oncol. 2010;28:1481-1488.
9. Agarwal N, Hutson TE, Vogelzang NJ, Sonpavde G. Abiraterone acetate: a promising drug for the treatment of castration-resistant prostate cancer. Future Oncol. 2010;6:665-679.
10. Danila DC, Morris MJ, de Bono JS, et al. Phase II multicenter study of abiraterone acetate plus prednisone therapy in patients with docetaxel-treated castration-resistant prostate cancer. Clin Oncol. 2010;28:1496-1501.
11. National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Washington, DC: National Osteoporosis Foundation; 2010. Available at: http://www.nof.org/sites/default/files/pdfs/NOF_ClinicianGuide2009_v7.pdf Accessed September 30, 2010.
12. Silver DS. Denosumab reduces the incidence of new vertebral fractures in men with prostate cancer. Curr Osteoporos Rep. 2010;8:1-3.
13. Fizazi K, Carducci MA, Smith MR, et al. A randomized phase III trial of denosumab versus zoledronic acid in patients with bone metastases from castration-resistant prostate cancer. J Clin Oncol. 2010;28:Abstract LBA4507.
14. Small EJ, Schellhammer PF, Higano CS, et al. Placebo-controlled phase III trial of immunologic therapy with sipuleucel-T (APC8015) in patients with metastatic, asymptomatic hormone refractory crostate cancer. J Clin Oncol. 2006;24:3089-3094.
15. Schellhammer PF, Higano C, Berger ER, Shore N, Small E, Penson D, Ferrari A, Sims R, Yuh L, Frohlich M, Kantoff P. A randomized, double-blind, placebo-controlled, multicenter, phase III trial of sipuleucel-T in men with metastatic, androgen independent prostatic adenocarcinoma. Program and abstracts of the American Urological Association Annual Meeting; April 25-30, 2009; Chicago, Illinois.
16. Antonarakis ES, Drake CG. Current status of immunological therapies for prostate cancer. Curr Opin Urol. 2010;20:241-246. 17. Madan RA, Mohebtash M, Arlen PM, et al. Overall survival (OS) analysis of a phase l trial of a vector-based vaccine (PSA-
TRICOM) and ipilimumab (Ipi) in the treatment of metastatic castration-resistant prostate cancer (mCRPC). J Clin Oncol. 2010;28:7s. Abstract 2550.
18. De Bono JS, Oudard S, et al. Cabazitaxel or mitoxantrone with prednisone in patients with metastatic castration-resistant prostate cancer (mCRPC) previously treated with docetaxel: final results of a multinational phase III trial (TROPIC). J Clin Oncol. 2010;28(15 suppl):Abstract 4508. (virtual meeting)
19. Sartor AO, Sartor EA, Davis N, Goeckeler W. Predictors of palliative response for samarium Sm-153 lexidronam: analysis of data from three randomized controlled blinded trials. Program and abstracts of the American Society of Clinical Oncology 2006 Cancer Symposium; June 2-6, 2006; Atlanta, Georgia. Abstract 267.
20. Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502-1512.