-
7/21/2019 Clostridium Difficile Epidemiology
1/36
Clostridium diffic
ISHA BHATT
DEPARTMENT OF EPIDEMIOLOGY AND BIOSTATISDREXEL UNIVERSITY SCHOOL
OF PUBLIC HEA
MAY, 2014
-
7/21/2019 Clostridium Difficile Epidemiology
2/36
OverviewClinical context and terminologyMicrobiology
Pathogenesis and reservoirs
Disease definition, syndromes , outcomes
Diagnosis and treatmentSurveillance and prevention
strategies
Impact
-
7/21/2019 Clostridium Difficile Epidemiology
3/36
History:First cases of C.diff infections reported as far back as
1890sFirst isolated in the stools of infants and described by Hall
aOToole in 1935 as Bacillus difficile.
In 1978, Bartlett et al, demonstrated a link between C.diff
tcases of pseudomembranous colitis after antibiotic use.
The years 20032005 saw several outbreaks in Canada anKingdom
2004First International Clostridium difficile symposium(F
-
7/21/2019 Clostridium Difficile Epidemiology
4/36
cro o ogy Gram positive
Motile ,obligate
anaerobe Spore and Toxin
producing
Normal gut floraespecially in
infants andelderly
Multiple strains
Also known asC.diff
Source:
http://www.bioquell.com/technology/microbiology/clostridium-diffic
-
7/21/2019 Clostridium Difficile Epidemiology
5/36
Culture : Isolation MedCCFA: first proposedBA with lysed horse
blood:Opaque grey-white colonies
TCCFA: Enhances sporulation
CDMN Selective Agar: C.difficile grows better
Buchanensbroth
-
7/21/2019 Clostridium Difficile Epidemiology
6/36
Terminology:Antibiotic-associated diarrhea : C.diff is only one
of the etfactors (10%-25%). Others include MRSA, Klebsiella, E.coli
in
Clostridium difficile infections (CDI) : diarrhea associated
positive stool culture and toxin assays
Clostridium difficile associated diarrhea (CDAD): used
interchangeably with CDI.Pseudomembranous colitis: fulminant
CDI, severe and oftConfirmed endoscopically
Toxic megacolon: also diagnosed by CT and endoscopy.
Mperforation and death
-
7/21/2019 Clostridium Difficile Epidemiology
7/36
Reservoir :~2% normal adult gut flora
1070% colonization in newborns and infants (50%)
Exogenous reservoir : animals feces
Spores : highly resistant to destruction and disinfection
Most acquired disease causing strains are in hospital
settingthrough HCW hands
Increased colonization rates in hospitalized patients or
thosterm care facilities after antibiotic exposure (10- 25 %)
-
7/21/2019 Clostridium Difficile Epidemiology
8/36
Risk Factors :Patients in hospitals and long-term care
facilitExposure to antibiotics
Elderly
Children >1 yearPeripartum women
History of Inflammatory bowel diseases
-
7/21/2019 Clostridium Difficile Epidemiology
9/36
-
7/21/2019 Clostridium Difficile Epidemiology
10/36
Antibiotics implicatedHigh Frequency Medium frequency Low
Freq
Ampicillin Erythromycin Chloramphe
Amoxicillin Other macrolides Metronidazo
Clindamycin Sulphonamides Rifampin
Fluoroquinolones Tetracycline
Cephalosporins Vancomycin
-
7/21/2019 Clostridium Difficile Epidemiology
11/36
-
7/21/2019 Clostridium Difficile Epidemiology
12/36
Transmission:Primary mode of transmission:Fecal-Oral route
Direct contact: Hands of healthcare workers
Patient to patient transmission
Family and/or visitor introduction
Asymptomatic carriers
Indirect transmission via fomitesProcedural transmission:through
improperly sterilizedrectal thermometers andendoscopic tubes and
intubation
-
7/21/2019 Clostridium Difficile Epidemiology
13/36
CDI : Symptoms
CDI have a wide range of clinical presentationIngestion of
C.diff may lead to excretion or asymptocolonization of healthy
individuals
Manifested disease may be mild, moderate to sever
life-threatening consequencesRelapses are not uncommon in
healthcare settings
Mild t M d t S
-
7/21/2019 Clostridium Difficile Epidemiology
14/36
Mild to Moderate cases Severe case
Fever Pain, fever, diarrhea, inc
Abdominal pain Blood in stool
Diarrhea (>10 bowel movements
per day)
Electrolyte imbalance
Increased WBCs Paralytic ileus
Dehydration Toxic megacolon
Pseudomembranous co
Perforation
Death
-
7/21/2019 Clostridium Difficile Epidemiology
15/36
Pathogenesis:Disruption of normal protective gut flora
Ingestion of spores and colonization of C.dif
Toxin production A and B
Damage to the cytoskeletal structures, loss of t
junctions leading to mucosal injury , inflammat
increased fluid secretion
Colitis and diarrhea
-
7/21/2019 Clostridium Difficile Epidemiology
16/36
Onset and Progressio
Source:
http://www.cdc.gov/HAI/pdfs/cdiff/Cohen-IDSA-SHEA-CDI-guidelines-2010.pdf
-
7/21/2019 Clostridium Difficile Epidemiology
17/36
Course :Onset usually >3 days - ~7 daysLatent period
difficult to determine due toasymptomatic carriers
Acute infection lasts for more than 10 days an
continues depending on severity and extent ofmucosal damage
Infection may progress to complete resolutionrecurrence or in
severe cases coma or death
C d fi i i I id
-
7/21/2019 Clostridium Difficile Epidemiology
18/36
Case definition: Incide
Presence of symptoms (usually diarrheai.e >10 bomovements per
day)
AND
Either Stool test result positivefor C. difficile toxins or tC.
difficile
ORor colonoscopic evidence of pseudomembranous c
Source :
http://www.cdc.gov/HAI/pdfs/cdiff/Cohen-IDSA-SHEA-CDI-guidelines-2010.pdf
-
7/21/2019 Clostridium Difficile Epidemiology
19/36
Probable case: prompt to isolaand testConsider presumptive
isolation for patients with > 3 unformed swithin 24 hours
Send specimen for testing and presumptively isolate patient
peresults
Positive predictive value of testing will also be optimized if
focpatients with >3 unformed stools within 24 hours
Exception: patient with possible recurrent CDI (isolate and
testfirst unformed stool)
Source : CDC SHEA Guildelines, 2012
Di i L b t
-
7/21/2019 Clostridium Difficile Epidemiology
20/36
Diagnosis : LaboratoryTestingTissue Culture Cytotoxin Assay :
Gold standard to identify toxinsamples in Vero cells
Toxigenic Culture 4-6 isolates to CMC
24 hr. filtrate for toxin detection ( fast )
Enzyme Immunoassay for toxin detection ( Toxin A and B )
Glutamate dehydrogenase detection : characteristic enzyme prby
C.diff
PCRtoxin gene detection, greater sensitivity and specificity
Li it ti t L b t
-
7/21/2019 Clostridium Difficile Epidemiology
21/36
Limitations to Laboratortesting:Cytotoxin assays have low
sensitivity and specificityStool culturetime-consuming
GDH : risk of cross reaction
Recommendation for best predictive outcome :
-Screening for GDH
-Followed by culture for C.diff or EIA toxin assay
-
7/21/2019 Clostridium Difficile Epidemiology
22/36
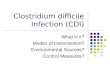
Radiologic testing :
Accordion Signevidence ofPseudomembracolitis
E d i T ti
-
7/21/2019 Clostridium Difficile Epidemiology
23/36
Endoscopic Testing :Colonoscopy
Evidence suggeof PMC
-
7/21/2019 Clostridium Difficile Epidemiology
24/36
Treatment :
Discontinue the offending agentstop the antimitreatment !!
Start supportive treatment simultaneously : Fluid symptomatic
treatment
If not resolved with conservative therapyStart or
metronidazole for 10 days or VancomycinWhen both vancomycin and
metronidazole fail : acombination therapy
-
7/21/2019 Clostridium Difficile Epidemiology
25/36
:Probioticsefficacy undetermined
Fecal micro biota transplant : risk of transplantother
pathogens
IV immunoglobulinspassive immunizationespecially for
Immunocompromised
Surgical approach : in severe fulminant casesresection of
necrotic colon to prevent sepsis
New Antibiotic: Fidaxomycin
reven on: ore
-
7/21/2019 Clostridium Difficile Epidemiology
26/36
reven on: orestrategies Judicious use of high potency
antibiotics Contact Precautions for duration of diarrhea
Hand hygiene in compliance with CDC/WHO
Cleaning and disinfection of equipment and envir
Laboratory-based alert system for immediate notof positive test
results
Educate about CDI: HCP, housekeeping, administrpatients,
familiesSource:
http://www.cdc.gov/ncidod/dhqp/id_CdiffFAQ_HCP.html
Dubberke et al. Infect Control Hosp Epidemiol 2008;29:S81-92
Prevention: Supplement
-
7/21/2019 Clostridium Difficile Epidemiology
27/36
Prevention: SupplementstrategiesExtend use of Contact
Precautions beyond duration of diarrhe48 hours)
Presumptive isolation for symptomatic patients
pendingconfirmation of CDI
Evaluate and optimize testing for CDI : for faster and
accuratdiagnosis
Implement soap and water for hand hygiene before exiting patient
with CDI
Implement universal glove use on units with high CDI rates
Use sodium hypochlorite (bleach)for spores
-
7/21/2019 Clostridium Difficile Epidemiology
28/36
CDI : Incidence and Epidemiolog(US)Increased incidence (2.7
cases per
1,000 discharges in 1997 to 6.8 casesper 1,000 discharges in
2001)
Increased severity (0.15 to 0.60 casesper 1,000 discharges) of
CDI
23% annual increase in CDI-related
hospitalizations between 2000 and2005, associated with an
increasedage-adjusted, annual case-fatality rateof 0.2% over the
study period
Changing trends and
-
7/21/2019 Clostridium Difficile Epidemiology
29/36
Changing trends andcauses:The proportion of children with
toxin-positive stool increased from 46% in 2001 to 64% in 2006.
Prior to 1990, predominant strain was toxinotype0/ribotype
001
Now: ribotype 027 (BI/NAP1/027) is associated with
increased virulence, mortality and morbidityIncrease incidence
in previously considered non-higgroups
-
7/21/2019 Clostridium Difficile Epidemiology
30/36
Surveillance :
To layout case definitions for Healthcare facilitacquired CDI
and community acquired CDI
Use these as universal guidelines to survey thdisease in
populations across the country and
worldDevise prevention strategies to curb the epide
Surveillance and
-
7/21/2019 Clostridium Difficile Epidemiology
31/36
Surveillance andreporting :
EIP : Emerging Infections program - surveillanrepresentative of
the whole country.
NHSN : National Healthcare Safety Networkentered from
hospitals
HHS Action Plan : targets towards reducing HAincluding CDI
-
7/21/2019 Clostridium Difficile Epidemiology
32/36
Impact on Health care
CDI may have resulted in $4.8 billion excess costs in US
acute-care facilities
Per person cost increases by $2000- $due to prolonged hospital
stay andadditional testing
Increased risk of recurrence
-
7/21/2019 Clostridium Difficile Epidemiology
33/36
-
7/21/2019 Clostridium Difficile Epidemiology
34/36
Global impactNew MRSA
Similar increase in CDI worldwideacross North AEurope and
Asia
New strain in Asia O17 in addition to O27
Globally difficult surveillance : no universal case
definitions, diagnostic gold standards, inadequate reporting ad
collection
Ongoing research and cumulative efforts to comba
References :
-
7/21/2019 Clostridium Difficile Epidemiology
35/36
References:Bartlett, J. G., & Gerding, D. N. (2008).
Clinical recognition and diagnosis of clostridium
dinfection.Clinical Infectious Diseases, 46(Supplement 1), S12-S18.
doi:10.1086/521863
Centers for Disease Control and Prevention (CDC). (2012). Vital
signs: Preventing clostridinfections.MMWR.Morbidity and Mortality
Weekly Report, 61(9), 157-162. doi:mm6109
Cohen, S. H., Gerding, D. N., Johnson, S., Kelly, C. P., Loo, V.
G., L Clifford McDonald, M., .H. (2010). Clinical practice
guidelines for clostridium difficile infection in adults: 2010
upsociety for healthcare epidemiology of america (SHEA) and the
infectious diseases socie(IDSA).Infection Control and Hospital
Epidemiology, 31(5), 431-455.
HALL, I. C., & O'TOOLE, E. (1935). Intestinal flora in
new-born infantswith a description opathogenic anaerobe, bacillus
difficilis.American Journal of Diseases of Children,49(2), 3
Kelly, C. P., & LaMont, J. T. (2008). Clostridium
difficilemore difficult than ever.New Enof Medicine, 359(18),
1932-1940.
L Clifford McDonald, M., Coignard, B., Dubberke, E., Song, X.,
Horan, T., Kutty, P. K., & AdClostridium difficile Surveillance
Working Group. (2007). Recommendations for surveillaclostridium
difficileassociated disease.Infection Control and Hospital
Epidemiology, 28(
Lessa, F. C., Gould, C. V., & McDonald, L. C. (2012).
Current status of clostridium difficile epidemiology.Clinical
Infectious Diseases : An Official Publication of the Infectious
DiseaAmerica, 55 Suppl 2, S65-70. doi:10.1093/cid/cis319 [doi]
-
7/21/2019 Clostridium Difficile Epidemiology
36/36
Thank you