Embed Size (px)
Citation preview

Journal for Healthcare Quality4
Closing the Gap in Children’s Quality
Measures: A Collaborative Model
Ellen Schwalenstocker, Hema Bisarya, Stephen T. Lawless, Lisa Simpson, Cheri Throop, Donna Payne
Attention to the production of comparative
information on healthcare quality has esca-
lated over the last 3 decades. However, children
are frequently missing from national efforts to
measure and report on quality. Over a decade
ago, a summary of workshops conducted by
the National Research Council and Institute of
Medicine (IOM) concluded that “additional
indicators are needed to assess the quality of
children’s health care” (Durch, 1996, p. 52).
This need also was identified by the President’s
Advisory Commission on Consumer Protection
and Quality in the Health Care Industry in
1998.
The Pediatric Data Quality Systems (Pedi-
QS) Collaborative was established in 2002
by the Child Health Corporation of America
(CHCA), Medical Management Planning/
BENCHmarking Effort for Networking
Children’s Hospitals (MMP/BENCH), and the
National Association of Children’s Hospitals
and Related Institutions (NACHRI), with input
from other organizations focused on quality
and children’s healthcare, to address this gap.
The collaborative designed a framework and
methodology for identifying improvement
opportunities and practices and established a
model for developing consensus-based measure
sets. The consensus model is particularly
important in light of methodological limitations
in developing quality measures and a limited
evidence base for pediatric care (Schuster et
al., 1997). In this article, we discuss the Pedi-QS
framework and methodology and the initial
measures identified through the collaborative.
We describe efforts to continually incorporate
learning into the methodology. We conclude
with future directions for advancing healthcare
quality measurement and improvement for
children and adolescents.
Why Do We Need Comparative Quality Information?In general, dissemination of comparative per-
formance information is expected to enhance
healthcare quality by (1) providing momentum
for providers to improve and (2) enabling con-
sumers to make informed choices (National
Quality Forum, 2002). Recent studies have sug-
gested that the first mechanism may be work-
ing. Publishing measures on adult healthcare
quality through initiatives such as the Hospital
Quality Alliance (HQA) Hospital Compare Web
site, Joint Commission’s Quality Check, and
Premier/Centers for Medicare and Medicaid
Services (CMS) pay-for-performance demon-
stration has been associated with improved
performance (Jha, Li, Orav, & Epstein, 2005;
Joint Commission, 2007). There is no reason
to expect that these same market mechanisms
would not be similarly effective for children’s
healthcare. And, just as in adult care, significant
gaps in children’s healthcare quality exist. For
example, a recent article by Mangione-Smith
et al. (2007) reported that children received
evidence-based care less than half of the time in
ambulatory care settings.
Why Are Children’s Measures Behind?Despite gaps in performance and evidence of
links between quality measurement, reporting,
and quality improvement, the lack of quality- of-
care measures for children and adolescents is
well recognized (Beal et al., 2004; Dougherty &
Simpson, 2004; Miller, Gergen, Honour, & Zhan,
2005). Major reasons for the lack of measures
include the small economic impact of children’s
healthcare on overall healthcare expenditures
and the unique methodological challenges in
Key WordsPedi-QS
Pediatric Data Quality Systems
performance improvementpublic reporting
quality improvementquality measurement
Abstract: The need for measures of the quality of healthcare
provided to children and adolescents is well documented.
However, children have been underrepresented in national
healthcare quality measurement and reporting efforts. The
Pediatric Data Quality Systems (Pedi-QS) Collaborative is
addressing this gap. Two consensus measure sets and an
assessment of nursing-sensitive indicators in pediatric care
have been produced through the collaborative. The framework
and measure set development process are described. Lessons
learned from applying the process are summarized, and future
directions are suggested. Voluntary collaborative efforts are
vital for advancing children’s measures, and national support
and funding are also needed.
Journal for Healthcare Quality

Vol. 30 No. 5 September/October 2008 5
developing reliable and valid measures of quality
for children and adolescents.
On average, healthcare expenditures on
children accounted for $55 –$75 billion annu-
ally between 1997 and 2004, or 10%–12% of
total national health expenditures, and this
proportion has been dropping slightly over
time (Chevarley, Owens, Zodet, Simpson,
& McCormick, 2006; Simpson et al., 2004).
Advancement of quality initiatives among adults
has been strategically supported by the Medicare
program. Although Medicaid and the State
Children’s Health Insurance Program (SCHIP)
served almost one in every three children in
2005, these state–federal partnership programs
have not exerted national leadership on quality
issues (Simpson, Fairbrother, Hale, & Homer,
2007).
Methodological challenges to measurement
in pediatrics are well documented and include
the diversity and uniqueness of settings in which
children receive care (e.g., schools, day care
centers, community centers), developmental
factors, variations in the patterns of cost and
diagnoses associated with different age groups
within the pediatric population, small numbers
of children with specific conditions, and lack of
evidence regarding best practices (Agency for
Healthcare Research and Quality [AHRQ], n.d.;
Palmer & Miller, 2001).
A large proportion of quality measures that
do apply to children focus on preventive care
(Schuster et al., 1997; Simpson, Dougherty,
Krause, Ku, & Perrin, 2007). A study of
Medicaid and SCHIP directors in 40 states
conducted by Health Management Associates
(HMA) under contract with the National
Association of Children’s Hospitals (NACH)
found that a large majority (85%) of Medicaid
and SCHIP programs require one or more
National Committee for Quality Assurance
(NCQA) Healthcare Effectiveness Data and
Information Set (HEDIS) measures, most com-
monly preventive care measures (Duchon &
Smith, 2006). Only eight programs reported
using inpatient performance measures focused
on patient safety, processes of care, or infrastruc-
ture to support quality and safety.
Although no one would argue about the
importance of preventive care for children and
adolescents, the lack of standardized quality
measures available for reporting on acute and
chronic care, particularly in hospital settings,
is problematic. Mangione-Smith and McGlynn
(1998) noted that children with the most severe
conditions are “potentially the segment of the
pediatric population that can be most affected
by variations in the quality of care” and that
improvement in the care for these children “is
likely to have the largest impact on quality of life
and longevity” (p. 1059).
How Is Pedi-QS Closing the Gap?As leaders in children’s healthcare quality recog-
nized that children’s hospitals could be subjected
to measurement (and accreditation) using adult
measures unsuitable for pediatrics and, more
important, that insufficient measures for improv-
ing children’s healthcare quality existed, sev-
eral organizations came together to change the
dynamic. The Pedi-QS Collaborative effort was
formed to address the gap in quality measures,
focusing initially on measures for acute and
chronic care in hospital settings. On behalf of
all children’s hospitals, CHCA, MMP/BENCH,
and NACHRI met with the Joint Commission in
2002 to clarify requirements for children’s hospi-
tals with regard to core measurement and were
encouraged to propose core measures meaning-
ful for children’s healthcare.
With this charge, CHCA, MMP/BENCH,
and NACHRI convened representatives from
13 children’s hospitals and designed a frame-
work to identify improvement opportunities
and measures across multiple domains of qual-
ity and the continuum of patient and family
needs. Accordingly, the Pedi-QS framework is
designed within the context of the Institute of
Medicine’s (IOM) approach for developing a
national healthcare quality report, Envisioning the National Health Care Quality Report (Hurtado,
Swift, & Corrigan, 2001), which links the qual-
ity aims articulated in the IOM (2001) Crossing the Quality Chasm report and the patient needs
identified by the Foundation for Accountability
(FACCT). At this two-dimensional level, the
framework allows for the identification of prac-
tices and measures on areas that cut across
clinical conditions, settings of care, and types
of providers (e.g., coordination of care, medi-
cation safety). This is especially important in
children’s healthcare, given the methodological
challenges (e.g., small numbers of children with
specific clinical conditions) and unique aspects
of children’s healthcare described previously in
this article.
With the two dimensions of quality aims
and patient and family needs as the essential
foundation, other dimensions (e.g., clinical
conditions, service lines, provider types, care

Journal for Healthcare Quality6
settings) can be overlaid on the framework.
The overarching principle is that robust sets of
measures—whether or not these measures are
specific to a clinical condition or service line or
type of provider—will address all of the IOM
quality aims (safety, timeliness, effectiveness,
efficiency, equity, patient-centeredness) across
the continuum of patient and family needs. At
the time of its development, this multidimen-
sional framework of quality measurement was a
unique feature of our approach.
The addition of measures on pain is an exam-
ple of how the framework was used to identify
measures in the pediatric critical care setting.
Measures in use in existing pediatric critical care
data programs mostly addressed the quality aims
related to effectiveness (e.g., severity-adjusted
mortality, readmission rate) and efficiency (e.g.,
length of stay). The framework assisted the
panel in identifying the need for additional
measures on patient-centeredness, including
pain. In addition, the framework points to the
need for more measure development in the
areas of timeliness, equity, and patient safety.
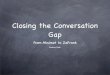
Through ongoing learning, the collaborative
has developed a seven-step process to establish
consensus-based measure sets (Figure 1). The
iterative process includes (1) issuing a call
for measures and synthesizing the results, (2)
convening experts to review and assess the mea-
sures against criteria and obtain consensus on
measures that should be moved forward, and (3)
soliciting broad feedback from children’s hospi-
tals and other stakeholders. The criteria used
to evaluate measures also were derived from
the IOM’s Envisioning the National Health Care Quality Report (Hurtado et al., 2001) and include
importance, scientific soundness, and feasibility.
To support the development of standardized
measures, the Pedi-QS method includes iden-
tifying the data elements to support each pro-
posed measure, including precise definitions of
numerators and denominators.
Testing, Building, and Expanding the Pedi-QS Framework and ApproachUsing this framework and methodology, the
Pedi-QS Collaborative has worked to close the
gap in children’s quality measures by evaluating
or making nationally available 25 inpatient
children’s quality measures or indicators (Table 1). The depth and breadth of the Pedi-QS process
has been spread to the pediatric community
in the United States and internationally.
Following calls for measures, 133 measures
were received. Input from 56 content experts,
including representatives of national healthcare
stakeholders, and widespread feedback from
the children’s hospital community contributed
to the final consensus-based recommendations
(Table 1). Today, the contributions of the Pedi-
QS Collaborative have resulted in measures
adopted by the Joint Commission, measures
endorsed by the National Quality Forum (NQF),
and measures approved by the Hospital Quality
Alliance (HQA). A publicly available Web site
(www.pediqs.com) provides the methodology,
framework, and consensus measure sets.
To illustrate how the Pedi-QS framework and
collaborative process have developed over time,
we now describe the development of measure
sets for children’s asthma care and pediatric crit-
ical care and the assessment of nursing-sensitive
indicators for pediatric hospital settings.
Testing the model using the lens of a clinical condition—children’s asthma care: Children’s asthma care was an
obvious starting point for testing the
Pedi-QS framework. Asthma is the most
common chronic disease among children
(AHRQ, 2002) and is the second most
common reason for admission among
children admitted to the hospital for
illness (Owens, Thompson, Elexihauser, &
Ryan, 2003). A well-established evidence
base exists to inform the identification of
Figure 1. The Pediatric Data Quality Systems (Pedi-QS) Process for Measure Evaluation
Create and convene multidisciplinary and stakeholder expert panel.
▼
Field call for measures to children’s hospitals.
▼
Review and categorize measures.
▼
Conduct stepwise and iterative process for specifying and assessing measures.
▼
Vet candidate measures across the larger group of children’s hospitals.
▼
Complete final review reflecting consensus by the expert panel.
▼
Inform pediatric community and national stakeholders of final results.

Vol. 30 No. 5 September/October 2008 7
measures (e.g., National Heart, Lung, and
Blood Institute, 2007). Following a 1-year
effort, six asthma care measures, as well as
the Pedi-QS framework and methodology,
were received enthusiastically by the
Joint Commission in December 2002. In
December 2006, the steadfast efforts of
the Pedi-QS Collaborative were recognized
with the Joint Commission’s adoption
of three of the children’s asthma care
measures. Beginning in July 2008, data on
two of these measures will be posted on
Hospital Compare for hospitals submitting
these measures as core ORYX measures to
the Joint Commission (Table 1).
Table 1. Measure Review—Version 2 (continued)
Date of Completion Review Process Measure Name Status
Priority Area: Asthma
2002 Convened content experts from 13 hospitals
Call for measures resulted in 33 measures used inter-nally by hospitals and/or available through vendors
Initial review narrowed to 9 measures
Six measures retained fol-lowing comment period (25 hospitals commented)
Joint Commission expert panel and pilot testing resulted in 3 measures for Joint Commission ORYX core measure set
1. Return to hospital (i.e., ED, OS, or inpa-tient admission) with same diagnosis within 7 days following inpatient discharge
Not retained as core measure following pilot testing
1a. Return to hospital with same diagnosis within 30 days following inpatient discharge
Not retained as core measure following pilot testing
2. Return to hospital with same diagnosis with-in 7 days following ED or observation stay
Not retained as core measure following pilot testing
2a. Return to hospital with same diagnosis within 30 days following ED or observa-tion stay
Not retained as core measure following pilot testing
3. Use of relievers for inpatient asthma Endorsed by NQF
Included in Joint Commission CAC core measure set
Included in Hospital Compare beginning in July 2008
4. Use of systemic corticosteroids for inpatient asthma
Endorsed by NQF
Included in Joint Commission CAC core measure set
Planned for inclusion in Hospital Compare in 2008*
5. Risk-adjusted length of stay Not retained as core measure following pilot testing
6. Home management plan of care discussed with patient/caregiver
Endorsed by NQF
Included in Joint Commission CAC core measure set
Planned for inclusion in Hospital Compare in 2008*
Priority Area: Pediatric Critical Care
2005 Convened 27 content experts, including multiple disciplines and representa-tives from Joint Commission
51 measures identified from call for measures
Expert subgroups formed to assess measures in specific areas
Public comment period included 290 respondents from 135 hospitals
1. PICU standardized mortality ratio Endorsed by NQF
2. PICU severity-adjusted length of stay Endorsed by NQF
3. PICU unplanned readmission rate Endorsed by NQF
4. Review of unplanned readmissions Endorsed by NQF
5. PICU pain assessment on admission Endorsed by NQF
5a. PICU periodic pain assessment Endorsed by NQF
6. PICU medication safety practice adoption Reviewed by NQF; not recom-mended for endorsement
7. PICU central line infection prevention prac-tice adoption
Reviewed by NQF; not recom-mended for endorsement
(continued)

Journal for Healthcare Quality8
Building on the model using the lens of service area—pediatric critical care: The Joint Commission’s acceptance of the
Pedi-QS framework set the stage for the
collaborative to identify and begin work
on additional priority areas. Pediatric criti-
cal care was selected as the second prior-
ity area as a result of input from workers
in children’s hospitals, the availability of
prospective measures from existing systems
and collaborative efforts, and alignment
with other national initiatives, including
the Joint Commission’s work on develop-
ing an adult critical care measure set. In
addition, the high cost, risk, and com-
plexity of pediatric critical care suggested
that it would be of interest to consumers
and payers as well as pediatric providers.
Building on learning from the development
of the children’s asthma care measure set,
experts were engaged at the outset of the
project through the establishment of a
multidisciplinary expert panel with broad
representation from providers (e.g., free-
standing children’s hospitals, children’s
hospitals within hospitals, diverse geograph-
ic locations) and areas of specific expertise
(e.g., risk adjustment), as well as the Joint
Commission. Using a Joint Commission
best practice for public comment, the Pedi-
QS collaborative developed a Web-based
tool to systematize and simplify data collec-
tion. More than 130 hospitals responded—
more than a fourfold increase as compared
with the response to the children’s asthma
care measure set. The expert panel was
reconvened to make final recommenda-
tions, resulting in a set of seven measures in
less than 14 months. Five of these measures
were recently endorsed by NQF (Table 1).
Expanding the field using the lens of pro-vider type—nursing-sensitive indicators: The third project undertaken by the Pedi-
QS collaborative was the assessment of
Table 1. Measure Review—Version 2 (continued)
Date of Completion Review Process Measure Name Status
Priority Area: Nursing-Sensitive Care
2007 Convened 16 experts, including representa-tives from American Nurses Association, Joint Commission, and National Database for Nursing Quality Indicators (NDNQI)
49 indicators used internally and/or available through vendors resulted from call for measures
219 respondents from 129 hospitals provided input during comment period
1. Nursing care hours per patient day Recommended for further testing
Endorsed by NQF
2. Skill mix Recommended for further testing
Endorsed by NQF
3. Percentage of RNs with BSN or higher Recommended for further testing
4. Percentage of agency/travelers worked Recommended for further testing
5. Unit vacancy Recommended for further testing
6. Voluntary turnover Recommended for further testing
Endorsed by NQF
7. Practice environment scale Recommended for further testing
Endorsed by NQF
8. Use of restraints Recommended for further testing
9. Pediatric pain assessment (on admission and periodically)
Recommended for further testing
10. Central line–associated bloodstream infection
Recommended for further testing
Endorsed by NQF
11. Prevalence of peripheral intravenous infiltrates
Recommended for further testing
12. PICU unplanned endotracheal extubation rate
Recommended for further testing
Note. ED = emergency department; OS = observation status; NQF = National Quality Forum; HQA = Hospital Quality Alliance; PICU =
pediatric intensive care unit; CAC = Children’s Asthma Care.
*For hospitals reporting measures to the Joint Commission

Vol. 30 No. 5 September/October 2008 9
nursing-sensitive indicators for children’s
hospital care. Selection of this priority
area was driven by external forces, includ-
ing the endorsement of an initial set of
consensus standards for nursing-sensitive
care by the NQF. There is growing evi-
dence of a negative association between
nurse staffing and adverse outcomes and
a positive association between nurse staff-
ing and patient experience with care
as well as nurse satisfaction. However,
most of this research has been conducted
in adult settings. Applying the Pedi-QS
methodology with a panel of nursing
experts, including representatives from
the Joint Commission and the American
Nurses Association, 12 nursing quality
indicators (Table 1) were identified as
potential measures. Unlike the first two
measure sets, feedback received during
the national comment period and from
the expert panel suggested that compre-
hensive pilot testing was needed prior to
using the indicators for the purposes of
comparative reporting of hospital perfor-
mance. Therefore, the output of this pro-
cess was a white paper identifying issues to
be addressed through pilot testing.
What Have We Learned?Over the last 5 years of the Pedi-QS experience,
we have encountered barriers and continuously
learned from them. Key barriers to develop-
ing and implementing the collaborative model
included (1) lack of agreement among stake-
holders on the purposes of measures, especially
with regard to what types of measures might
be used for public reporting; (2) challenges in
obtaining broad input and achieving consensus
among numerous stakeholders; (3) the degree
of rigor and resources required to precisely
define and evaluate quality measures; (4) the
lack of robust, validated, and tested measures to
enable populating the full Pedi-QS framework
(i.e., all quality aims for a given service area or
condition); and (5) the slow adoption of the
output of the collaborative by national entities
such as the NQF and HQA. To address the first
three of these challenges, we offer the following
strategies.
the Joint Commission in the pediatric critical
care measure project from the outset avoid-
ed the need for additional expert review and
a duplicative public comment period.
Although quality domains and patient
needs might be emphasized differently
in pediatrics than in adult care, the IOM
quality aims and FACCT patient needs
are as applicable to children as they are
to adults. Adapting existing frameworks
enabled the Pedi-QS Collaborative to
move forward quickly, and speaking the
same language facilitated the interface
with other national efforts.
involvement of experts from multiple dis-
ciplines early in the process enhanced the
meaningfulness as well as the credibility
and acceptance of the output.
consensus measures. It is important to
cast a wide net in seeking stakeholders’
comments on proposed measures. The
limited public input into the initial asth-
ma care set resulted in push-back from
several stakeholders.
Although collaboration can make the
development process slower, we hypoth-
esize that it will speed adoption.
Public policy interventions are needed to
address the last two challenges—the need for
the de novo development of robust, validated,
and tested quality measures and the widespread
adoption of pediatric measures at the national
level. Although the Pedi-QS Collaborative has
completed three substantive projects, movement
of measures into national reporting efforts has
been slow as a result of lack of resources and lack
of a focus on children. The pediatric community
is working to overcome these challenges.
What’s Next?The Pedi-QS Collaborative has demonstrated
early results, which are now ready for broader
application. The Alliance for Pediatric Quality
(the Alliance) was formed in 2006 by the
American Academy of Pediatrics, the American
Board of Pediatrics, CHCA, and NACHRI, build-
ing on the desire of all four organizations to
provide a unified physician and hospital voice
for pediatrics. We believe that this collaboration
is a distinctive competency of pediatrics.
The Alliance has embarked on a multiyear
collaboration to promote meaningful pediatric
improvement and to ensure that health informa-
tion technology works for children. In 2007, the
Alliance convened a national task force of quality

Journal for Healthcare Quality10
and safety leaders who identified four initial pri-
ority areas for improvement in pediatrics and cat-
alogued improvement initiatives and measures
associated with these priorities (obesity, patient
safety, neonatology, and chronic conditions).
How Has Pedi-QS Contributed to the Field?Accelerating the testing and refining of mea-
sures from improvement initiatives will pro-
vide meaningful measures that can be reviewed
and endorsed by national organizations, inform
consumers, and set expectations for the selec-
tion and improvement of quality healthcare for
children. Consumers will benefit from the avail-
ability of information about quality as they select
healthcare for their children as well as from care
improvements expected to result from compara-
tive reporting. Payers also will benefit from hav-
ing information on children’s healthcare quality.
This benefit is critically important, given that
children accounted for 50% of individuals served
by Medicaid in 2005 (Kaiser Family Foundation,
n.d.). States currently are relying on limited data
for assessing the quality of care provided to chil-
dren. Limitations in data and technology, as well
as the need for better measurement tools and
standards of care, were cited as barriers to quality
measurement and improvement by almost 30%
of state Medicaid and SCHIP directors in the
HMA study (Duchon & Smith, 2006).
Providers will benefit in at least two ways. Through
the development of standardized and meaningful
consensus measure sets, the burden of data collec-
tion will be reduced for providers. More important,
by having comparable information available, provid-
ers can learn how to improve.
ConclusionMarket forces will continue to drive public
reporting and pay-for-performance initiatives,
and there is evidence that these efforts can
provide the impetus for meaningful measurement
if combined with sound quality improvement
approaches. We are making progress, and
pediatrics is increasingly included in national
quality efforts. More than 35 pediatric experts are
now participating in technical advisory panels or
steering committees of NQF projects. However,
if children are to be meaningfully included in
these efforts, it is necessary for the people in the
pediatric healthcare community to continue to
work together to build the evidence for effective
care and meaningful measurement. Crosscutting
areas such as patient safety, care coordination,
efficiency, and equity are important and
promising areas for children’s healthcare quality
measure development.
Meaningful inclusion of children in national
quality initiatives also will require changes in
public policy. The U.S. government has greatly
influenced quality improvement, measurement,
and reporting through its work in developing
measures relevant to the Medicare population.
A similar investment is needed for children.
ReferencesAgency for Healthcare Research and Quality. (n.d.). Child
health care quality toolbox: Measuring quality in children’s health programs. [Electronic version]. Retrieved October 10, 2007, from www.ahrq.gov/chtoolbx/.
Agency for Healthcare Research and Quality. (2002). Children’s health highlights (AHRQ Pub. No. 03-P008). [Electronic version]. Retrieved October 10, 2007, from www.ahrq.gov/child/highlts/chhigh.pdf.
Beal, A. C., Co, J. P., Dougherty, D., Jorsling, T., Kam, J., Perrin, J., et al. (2004). Quality measures for children’s health care. Pediatrics, 113(1), 199–209.
Chevarley, F. M., Owens, P. L., Zodet, M. W., Simpson, L., & McCormick, M. C. (2006). Health care for children and youth in the United States: Annual report on patterns of coverage, utilization, quality, and expenditures by a county level of urban influence. Ambulatory Pediatrics, 6(5), 265–267.
Dougherty, D., & Simpson, L. (2004). Measuring the qual-ity of children’s healthcare: A prerequisite to action. Pediatrics, 113(1),185–196.
Duchon, L., & Smith, V. (2006). Quality performance mea-surement in Medicaid and SCHIP: Results of a 2006 nation-al survey of state officials. (Prepared for the National Association of Children’s Hospitals). Lansing, MI: Health Management Associates.
Durch, J. S. (ed.). (1996). Protecting and improving qual-ity of care for children under health care reform. In Paying attention to children in a changing health care system: Summaries of workshops (Chap. 3). Washington, DC: National Academy Press.
Hurtado, M. P., Swift, E. K., & Corrigan, J. M. (Eds.). (2001). Envisioning the national health care quality report. Washington, DC: National Academy Press.
Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
Jha, A. K., Li, Z., Orav, E. J., & Epstein, A. M. (2005). Care in U.S. hospitals—The Hospital Quality Alliance pro-gram. New England Journal of Medicine, 353(3), 265–274.
Joint Commission. (2007). Improving America’s hospitals: A report on quality and safety. [Electronic version] Retrieved March 30, 2007, from www.jointcommissionreport.org/print.aspx?print=1.
Kaiser Family Foundation. (n.d.). Distribution of Medicaid enrollees by enrollment group, FY 2004 [Electronic version]. Retrieved October 25, 2007, from www.statehealthfacts.org/comparebar.jsp?ind=200&cat=4.
Mangione-Smith, R., DeCristofaro, A. H., Setodji, C. M., Keesey, J., Klein, D. J., Adams, et al. (2007). The qual-ity of ambulatory care delivered to children in the United States. New England Journal of Medicine, 357(15), 1515–1551.
Mangione-Smith, R., & McGlynn, E. A. (1998). Assessing the quality of care provided to children. Health Services Research, 33(4), 1059–1090.
Miller, M. R., Gergen, P., Honour, M., & Zhan, C. (2005). Burden of illness in children and where we stand in measuring the quality of this health care. Ambulatory Pediatrics, 5(5), 268–278.

Vol. 30 No. 5 September/October 2008 11
National Heart, Lung, and Blood Institute. (2007). Expert panel report 3: Guidelines for the diagnosis and manage-ment of asthma. [Electronic version]. Retrieved October 23, 2007, from www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm.
National Quality Forum. (2002). A national framework for healthcare quality measurement and reporting. Washington, DC: Author.
Owens, P. L., Thompson, J., Elexihauser, A., & Ryan, K. (2003). Care of children and adolescents in U.S. hospitals. HCUP Fact Book No. 4. (AHRQ publication No. 04-0004). Rockville, MD: Agency for Healthcare Research and Quality.
Palmer, R. H., & Miller, M. R. (2001). Methodologic chal-lenges in developing and implementing measures of quality for child health care. Ambulatory Pediatrics, 1(1), 39–52.
President’s Advisory Commission on Consumer Protection and Quality in the Health Care Industry. (1998). Quality first: Better health care for all Americans. (Final Report to the President of the United States). Retrieved June 4, 2008, from www.hcqualitycommission.gov/final/.
Schuster, M. A., Asch, S. M., McGlynn, E. A., Kerr, E. A., Hardy, A. M., & Gifford, D. S. (1997). Development of a quality of care measurement system for children and adolescents. Archives of Pediatric and Adolescent Medicine, 151, 1085–1092.
Simpson, L., Dougherty, D., Krause, D., Ku, C. M., & Perrin, J. M. (2007). Measuring children’s healthcare quality. American Journal of Medical Quality, 22(2), 80–84.
Simpson, L., Fairbrother, G., Hale, S., & Homer, C. (2007, August). Reauthorizing SCHIP: Opportunities for promoting effective health coverage and high-quality care for children and adolescents. New York: Commonwealth Fund.
Simpson, L., Zodet, M. W., Chevarley, F. M., Owens, P., Dougherty, D., & McCormick, M. (2004). Health care for children and youth in the United States: 2002 report on trends in access, utilization, quality, and expenditures. Ambulatory Pediatrics, 4, 131–153.
Authors’ BiographiesEllen Schwalenstocker, PhD MBA, has been director of child health quality for the National Association of Children’s Hospitals and Related Institutions (NACHRI), Alexandria, VA, since 1997. She serves as NACHRI’s representative to the National Quality Forum.
Hema Bisarya, MHSA RD, is a director in the Solutions Team of Child Health Corporation of America, Shawnee Mission, KS. She joined CHCA in 2004.
Stephen T. Lawless, MD MBA, is the vice president for quality and safety for Nemours, Jacksonville, FL, a professor of pediatrics at Thomas Jefferson University, Philadelphia, PA, and staff pediatric critical care physician in the depart-ment of anesthesiology and critical care medicine at Alfred I. DuPont Hospital for Children, Wilmington, DE.
Lisa Simpson, MB MPH BCh, is a nationally known child health services and policy researcher and is currently the director of the Child Policy Research Center at Cincinnati Children’s Hospital Medical Center, Cincinnati, OH. Formerly, she served as the All Children’s Hospital Endowed Chair in Child Health Policy at the University of South Florida, Tampa, FL, and the deputy director of the Agency for Healthcare Research and Quality, Rockville, MD.
Cheri Throop, MHSA RN RHIT CPHQ, is a consultant with Healthcare Performance Improvement, Norfolk, VA. She was formerly director at Texas Medical Institute of Technology, Austin, TX, and chief quality and safety advisor for Child Health Corporation of America, Shawnee Mission, KS.
Donna Payne, FACHE, is a senior vice president for Child Health Corporation of America, Shawnee Mission, KS. She is a member of the executive committee for the Alliance for Pediatric Quality and a fellow in the American College of Health Care Executives.
For more information on this article, contact Donna Payne at [email protected].
Journal for Healthcare Quality is pleased to offer
the opportunity to earn continuing education
(CE) credit to those who read this article
and take the online posttest at www.nahq.
org/journal/ce. This continuing education
offering, JHQ 208, will provide 1 contact hour
to those who complete it appropriately.
Core CPHQ Examination Content AreaI. Management and Leadership