-
7/30/2019 Clonidine Paper
1/8
Enhanced reduction in hyperalgesia by combinedadministration of
clonidine and TENS
Kathleen A. Sluka*, Prasant Chandran
Physical Therapy and Rehabilitation Science Graduate Program,
Neuroscience Graduate Program, Pain Research Program, 2600
Steindler Bldg.,
University of Iowa, Iowa City, IA 52242, USA
Received 26 April 2002; accepted 22 July 2002
Abstract
Transcutaneous electrical nerve stimulation (TENS) partially
reduces primary hyperalgesia and is frequency dependent such that
highfrequency TENS produces approximately a 30% reduction in
hyperalgesia whereas low frequency TENS has no effect. Both high
and low
frequency TENS completely reduce secondary hyperalgesia by
activation ofm and d- opioid receptors in the spinal cord and
rostralventral
medulla suggesting an opiate mediated analgesia. Clonidine in
combination with opiates produces a synergistic interaction such
that there is a
potentiated reduction in hyperalgesia. Thus, we tested if
combined application of clonidine with TENS would enhance the
reduction in
primary hyperalgesia. Male SpragueDawley rats were inflamed by
subcutaneous injection of 3% carrageenan into one hindpaw.
Withdrawal
latency to radiant heat and withdrawal threshold to mechanical
stimuli were assessed before and after inflammation and after
administration
of clonidine (0.0022 mg/kg, intraperitoneal (i.p.)) with either
low (4 Hz) or high (100 Hz) frequency TENS. Clonidine alone reduced
both
heat and mechanical hyperalgesia with ED50s of 0.02 and 1.0
mg/kg, respectively. In combination with either low or high
frequency TENS,
the doseresponse curve shifted to the left and was significantly
different from clonidine alone. The ED50s for heat and
mechanical
hyperalgesia following low frequency TENS with clonidine were
0.002 and 0.2 mg/kg, respectively and those following high
frequency
TENS with clonidine were 0.005 and 0.15 mg/kg, respectively.
Thus, combined use of clonidine and TENS enhances the reduction
in
analgesia produced by TENS and enhances the potency of
clonidine. It would thus be expected that one would reduce the side
effects of
clonidine and enhance analgesic efficacy with combinations of
pharmaceutical and non-pharmaceutical treatments.q
2002 InternationalAssociation for the Study of Pain. Published
by Elsevier Science B.V. All rights reserved.
Keywords: Pain; Noradrenaline; Adrenergic; Electrical
stimuli
1. Introduction
Transcutaneous electrical nerve stimulation (TENS), a
non-invasive analgesic modality which involves the cuta-
neous application of electrical currents, is used
extensively
to treat both acute and chronic pain arising from a variety
of
musculoskeletal conditions including inflammatory condi-
tions of the joints (see Robinson, 1996 for review).
Severalstudies show the effectiveness of TENS in reducing pain
in
people with rheumatoid and osteoarthritis (Manheimer et
al., 1978; Manheimer and Carlsson, 1979; Kumar and
Redford, 1982). Both low- and high-frequency TENS at
sensory or motor intensity applied to the inflamed knee
joints of rats completely reduces secondary hyperalgesia,
i.e. pain outside the site of injury (Sluka et al., 1998;
King
and Sluka, 2001). However, primary hyperalgesia is only
partially reduced by TENS (Gopalkrishnan and Sluka,
2000). In fact, high frequency TENS reduces primary
mechanical and heat hyperalgesia by approximately 30%
while low frequency TENS has no significant effect. Chan-
ging intensity or pulse duration does not further affect the
degree of antihyperalgesia produced by TENS (Gopalkrish-
nan and Sluka, 2000).
Both high frequency (100 Hz)(Woolf et al., 1977; Slukaet al.,
1999b; Kalra et al., 2001) and low (4 Hz) frequency
(Sjolund and Erikson, 1979; Sluka et al., 1999b; Kalra et
al.,
2001) TENS analgesia are opiate mediated. Specifically, the
antihyperalgesic effects of low and high frequency sensory
TENS are mediated spinally and supraspinally by m- and d-
opioid receptors, respectively (Sluka et al., 1999b; Kalra
et
al., 2001).
Systemic administration of clonidine produces antinoci-
ception and pain relief in animals and human subjects
(Dennis et al., 1980; Paalzow, 1974; Skingle et al., 1982;
Bonnet et al., 1990) by activation of alpha-2 adrenergic
Pain 100 (2002) 183190
0304-3959/02/$20.00 q 2002 International Association for the
Study of Pain. Published by Elsevier Science B.V. All rights
reserved.
PII: S0304-3959(02) 00294-4
www.elsevier.com/locate/pain
* Corresponding author. Tel.:11-319-335-9791;
fax:11-319-335-9707.
E-mail address: [email protected] (K.A. Sluka).
-
7/30/2019 Clonidine Paper
2/8
receptors (a2-AR) (Yaksh, 1985; Maze and Tranquili, 1991;
Danzebrink and Gebhart, 1990; Pertovaara, 1993; Proudfit,
1988; Yaksh, 1985) and reduces dorsal horn responses to
noxious stimuli (Fleetwood-Walker et al., 1985; Sullivan et
al., 1992; Willcockson et al., 1984). Hypotension, bradycar-
dia, respiratory depression, and sedation are recognized as
side effects associated with the use ofa2-adrenergic
agonists
especially clonidine (reviewed in Eisenach et al., 1996; van
Zweiter, 1999).
Intrathecally administered clonidine potentiates the anti-
nociception produced by intrathecally or systemically admi-
nistered morphine in behavioral and electrophysiological
studies (Fairbanks et al., 2000; Drasner and Fields, 1988;
Hylden and Wilcox, 1983; Omote et al., 1991; Ossipov et
al., 1989). Systemic administration of clonidine also
enhances morphine-induced antinociception as measured
in the tail flick assay (Ossipov et al., 1984; Spaulding et
al., 1979). Spinal d-opioid receptors are also involved in
the synergism between opiates and a2-AR agonists
(Omote et al., 1991; Roerig et al., 1992).Since, TENS works
through activation of centrally
located opioid receptors, coadministration of clonidine
should enhance the effects of TENS. Thus, this study will
test the hypothesis that systemic clonidine in combination
with TENS produces an increased reduction in primary
hyperalgesia produced by TENS.
2. Methods
All experiments have been approved by the Animal Care
and Use Committee at the University of Iowa and are in
accordance with the NIH guidelines for care and use oflaboratory
animals. Adult male SpragueDawley rats
(250400 g, Harlan, Indianapolis, IN) were used for the
study.
2.1. Induction of inflammation
The animals were acutely inflamed by a subcutaneous
injection of 3% carrageenan (0.05 ml) (lambda carrageenan,
Sigma), using a 23-guage needle, into the plantar aspect of
one hindpaw under brief halothane (24%) anesthesia
(Winter et al., 1962; Hargreaves et al., 1988).
2.2. Behavioral assessments
2.2.1. Paw withdrawal latency to thermal stimuli
The time taken by the rat to withdraw its paw, i.e. paw
withdrawal latency (PWL), in response to a radiant heat
source was recorded (Hargreaves et al., 1988; Sluka and
Westlund, 1993). Before beginning the testing, the animals
were placed in transparent lucite cubicles that allow mini-
mal movement (24.6 7.5 7.5 cm3), on an elevated glass
table, and allowed to acclimate for approximately 20
30 min. The radiant heat source, consisting of a high inten-
sity light source connected to a timer, was then positioned
under the glass table directly beneath one hindpaw.
Bilateral
PWL readings (to the nearest 0.01 s) for each paw consisting
offive trials were taken in 5 min intervals and then
averaged
to give the mean PWL. Previous studies have established the
validity (Hargreaves et al., 1988) and testretest
reliability
(r2 0:7, P 0:0001) (Sluka et al., 1999a). A cut-off of
20 s was kept to avoid tissue damage. The PWL readings
were taken bilaterally before inducing inflammation (base-
line), 4 h after injection of 3% carrageenan and after
admin-
istration of saline (control)/clonidine and/or TENS.
2.2.2. Paw withdrawal threshold to mechanical stimuli
using von Frey filament
Von Frey filaments of varying bending forces (1, 4, 5, 8,
12, 16, 32, 44, 56, 75, 104, 162 and 350 mN) were applied to
the plantar aspect of the rats paw between the third and the
fourth digits to test for a withdrawal threshold. The
animals
were placed in transparent lucite cubicles that allow mini-
mal movement (24.6 7.5 7.5 cm3) on an elevated
meshed platform. The von Frey filaments were individuallyapplied
at right angles to the plantar aspect of the paw
starting with the lowest bending force and progressing
upwards. Mechanical or paw withdrawal threshold i.e. the
lowest bending force at which the animal lifts its paw off
the
meshed platform was noted. Mechanical withdrawal thresh-
old was measured bilaterally. The number of trials was
restricted to two per filament (Sluka, 1997). Previous
studies
have established the testretest reliability for this method
of
testing (r2 0:7, P 0:0001) (Gopalkrishnan and Sluka,
2000). Before the induction of inflammation, 13% of the
rats responded to the 104 mN, 50% to the 162 mN and
37% animals respond to the 350 mN bending force. Theanimals
normally do not respond to bending forces below
104 mN. This threshold value reduces dramatically follow-
ing the induction of inflammation to values between 1 and
12 mN.
2.3. Experimental design
This experiment determined if coadministration of
systemic clonidine and local TENS stimulation produced a
potentiated antihyperalgesic effect. Four hours after induc-
tion of inflammation, rats were randomly divided into six
groups: (1) saline1 no TENS; (2) saline1 low frequency
TENS (4 Hz); (3) saline1 high frequency TENS (100 Hz);(4)
clonidine1 no TENS; (5) clonidine1 low frequency
TENS and (6) clonidine1 high frequency TENS. Different
doses (0.0022.0 mg/kg i.p.) of clonidine (Sigma) or saline
were injected intraperitoneally under light halothane (1
2%) anesthesia 4 h after the induction of inflammation just
prior to TENS administration. TENS (EMPI, Eclipse Plus)
was administered at either low frequency (4 Hz) or high
frequency (100 Hz). A control group did not receive
TENS (sham TENS group) but was anesthetized for
20 min. All other treatment parameters were kept constant
as follows: intensity (2 motor threshold), pulse-width
K.A. Sluka, P. Chandran / Pain 100 (2002) 183190184
-
7/30/2019 Clonidine Paper
3/8
(100 ms) and modulation (normal). Previous data show only
a frequency effect of TENS on primary hyperalgesia
(Gopalkrishnan and Sluka, 2000). All the TENS treatment
groups were treated at an intensity twice the motor
threshold
i.e. by inducing a visible muscle contraction and then
increasing the intensity by twice this level. Pregelled
elec-
trodes (diameter 1 cm) were applied on the dorsal and
plantar aspects of the hindpaw. After 20 min, the animals
were removed from anesthesia, the use of TENS was
discontinued, and the electrodes removed. The animals
were allowed to recover fully from the anesthesia before
testing.
2.4. Data analysis
Two factor (dose, treatment) repeated measures of analy-
sis of variance (ANOVA) was used to analyze percent
changes in PWL to heat and mechanical withdrawal thresh-
olds (P # 0:05). Posthoc test (Tukeys test) was performed
to assess changes between groups (P#
0:
05). The PWLvalues and the mechanical withdrawal thresholds
are
expressed as the percent inhibition of hyperalgesia such
that 100% is a full reversal of hyperalgesia, 0% is no
change
in hyperalgesia and .100% is analgesia (mean^ SEM).
Percent inhibition and PWL to heat are presented as the
mean^ SEM. Mechanical withdrawal threshold is repre-
sented as the median with the 25th and 75th percentiles.
ED50 values with confidence intervals were calculated on
the % inhibition and Emax was set at 100% (PharmTools
Pro).
3. Results
3.1. Control
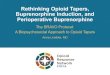
Subcutaneous injection of carrageenan into the paw
results in a reduced PWL to radiant heat. Four hours after
injection of carrageenan, the PWL to radiant heat decreased
to 3.97^ 0.36 s, which is a decrement of about 56 s from
baseline values (Fig. 1A). Treatment with high frequency
TENS significantly increased the PWL immediately after
treatment (P 0:001, paired t-test). In contast, treatment
with low frequency TENS has no effect on the decreased
PWL (P 0:12, paired t-test). In the group of animals that
did not receive TENS and were injected intraperitoneallywith
saline, there was no effect on the decreased PWL
(0.58^ 3.41%). The contralateral paw showed no differ-
ences in the withdrawal latency to heat after inflammation
or after treatment with TENS (Fig. 1A).
The paw withdrawal threshold to mechanical stimuli also
decreases to approximately 56.5 mN (median value) from
baseline values of 162350 mN (Fig. 1B). There was no
significant effect on the decreased withdrawal threshold in
animals that did not receive TENS (P 0:31, sign rank test)
or those that received either high frequency (P 0:06, sign
rank test) or low frequency (P 0:22, sign rank test) TENS.
The contralateral paw withdrawal threshold remained the
same in animals that did not receive TENS, or the groups
that received low and high frequency TENS (Fig. 1B).
3.2. TENS and clonidine
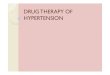
The PWL to radiant heat increased significantly on the
inflamed side following the systemic administration ofclonidine
(0.0022.0 mg/kg) (Fig. 2A) (F7:164 34:9,
P 0:0001). Clonidine at 0.2 mg/kg completely reversed
the hyperalgesia (113.05^ 12.5%) and significant increases
from saline occurred for 0.0062.0 mg/kg clonidine
(P, 0.0001). Lower doses of clonidine alone partially
reversed the hyperalgesia. There was a significant effect
K.A. Sluka, P. Chandran / Pain 100 (2002) 183190 185
Fig. 1. (A) PWL to radiant heat before the induction of in
flammation (base-
line), 4 h after induction of inflammation, and after
administration of TENS
(low frequencyP, high frequencyB and no TENSX). High
frequency TENS significantly increased the PWL to radiant heat
immedi-
ately after treatment. There was no significant difference from
4 h in the
groups that received low frequency or no TENS. The in flamed paw
is
represented by closed symbols whereas the uninflamed paw is
represented
by open symbols. Values are mean^ SEM. (B) Paw withdrawal
threshold
to mechanical stimuli before induction of inflammation
(baseline), 4 h after
induction of inflammation, and after administration of TENS
(low
frequencyL, high frequencyB and no TENSX). TENS had no
significant effect on the decreased withdrawal threshold to
mechanical
stimuli when compared to controls. The inflamed paw is
represented by
closed symbols whereas the uninflamed paw is represented by
open
symbols. Data are represented as the median with the 25th and
75th percen-
tiles.
-
7/30/2019 Clonidine Paper
4/8
for TENS treatment (F2;164 5:3, P 0:009) with signifi-
cant differences from the no TENS group for both low
(P 0:007) and high frequency (P 0:001) TENS. Thus,
the doseresponse curve for clonidine for changes in PWLto heat
shifted to the left following a combined administra-
tion of either low or high frequency TENS with clonidine.
The ED50 for clonidine without TENS was 0.02^ 0.01 mg/
kg. The ED50 following clonidine in combination with
TENS was significantly lower, 0.002^ 0.001 mg/kg for
low frequency TENS and 0.005^ 0.004 mg/kg for high
frequency TENS. This implies that a lower dose of clonidine
in combination with TENS is more effective in reversing the
hyperalgesia than when clonidine is administered alone.
Systemic administration of clonidine results in an
increase in the mechanical withdrawal threshold as
evidenced by a significant effect for dose (F7;164 32:6,
P 0:0001) such that doses 0.02 mg/kg (P 0:001) and
0.2 mg/kg (P 0:001), 0.6 mg/kg (P 0:001), and 2 mg/
kg (P 0:001) clonidine are significantly different from the
saline injected group (Fig. 2B). A significant effect for
change in mechanical withdrawal threshold occurred for
the inflamed paw following treatment with TENS
(F2;164 14:1; P 0:0001). Posthoc tests show that the
percent change in the mechanical withdrawal thresholds
for the groups that received both low (P 0:0001) and
high (P 0:0001) frequency TENS were significantly
different from the group that received clonidine without
TENS (Fig. 2B). The ED50 for clonidine without TENS
for the changes in mechanical threshold was
1.0^ 0.57 mg/kg. Following treatment with TENS and
clonidine, the ED50 was significantly less: low frequency
TENS 0.2^ 0.14 mg/kg and high frequency
0.15^ 0.09 mg/kg.
4. Discussion
In this study, TENS by itself has minimal (high
frequency) to no (low frequency) effects on primary
mechanical and thermal hyperalgesia and agrees with
previous studies from our laboratory (Gopalkrishnan and
Sluka, 2000). However, when the a-2 AR agonist, cloni-
dine, is given in combination with TENS there is an
increased inhibition of primary mechanical and thermal
hyperalgesia. Further, the ED50 values for clonidine are
significantly lower following combination with TENS
suggesting that the potency to clonidine is increased.
Thus, a lower dose of clonidine when given with TENScan produce
the same analgesic effect as a higher dose of
clonidine without TENS. Thus, we would expect that TENS
in combination with clonidine could result in a lower dose
of clonidine and thus reduced side effects of the drug.
4.1. TENS and opioids
TENS mediates antihyperalgesia and analgesia through
activation of the endogenous opioid systems (Woolf et al.,
1977; Han et al., 1984; Sjolund and Eriksson, 1979). There
is an increased release of beta-endorphins in the cerebrosp-
inal fluid and blood following treatment of TENS in both
animals and humans (Facchinetti et al., 1984; Han et al.,
1991; Hughes et al., 1984). Both high and low frequency
TENS activate opiate receptors in the spinal cord and the
rostral ventral medulla (RVM) to reduce hyperalgesia.
Specifically, low frequency activates m- and high frequency
TENS activates d-opioid receptors, both spinally and
supraspinally (Sluka et al., 1999b; Kalra et al., 2001).
4.2. Clonidine and analgesia
Clonidine administered intrathecally or systemically
produces an a2-AR mediated antinociceptive effect in
K.A. Sluka, P. Chandran / Pain 100 (2002) 183190186
Fig. 2. (A) Percent inhibition of the PWL to radiant heat for
the in flamed
paw after treatment with either clonidine plus no TENS (X),
clonidine plus
low frequency TENS (P) or clonidine plus high frequency TENS
(B).Values are mean^ SEM. Dose 0 represents either saline1 no TENS
or
saline1 low frequency TENS or saline1 high frequency TENS
(controls).
[*significantly different clonidine alone]. (B) Percent
inhibition of the paw
withdrawal threshold to mechanical stimuli for the inflamed paw
after
treatment with either clonidine plus no TENS (X), clonidine plus
low
frequency TENS (P) or clonidine plus high frequency TENS (B).
Data
are represented as the mean^ SEM. Dose 0 represents either
saline1 no
TENS or saline1 low frequency TENS or saline1 high frequency
TENS
(controls).
-
7/30/2019 Clonidine Paper
5/8
mice, rats, and humans (Hayes et al., 1986; Ossipov et al.,
1989; Spaulding et al., 1979; Buerkle et al., 1999).
Systemic
clonidine reduces acetylcholine induced abdominal contrac-
tions, reduces paw flinching in the formalin test, produces
analgesia in the hot plate test, tail immersion test, paw
pres-
sure test, and tail flick test in mice and rats (Hylden and
Wilkcox, 1983; Fielding et al., 1978; Spaulding et al.,
1979;
Skingle et al., 1982). Systemically administered clonidine
could produce analgesia by acting at peripheral or central
sites or both (Khasar et al., 1995; Yaksh, 1985; Nakamura
and Ferreira, 1988; Calvillo and Ghingnone, 1986;
Mastriami et al., 1989). Similar doses of systemic clonidine
produce an increase in the tail flick latency that still
occurs
after spinal transection suggesting the site of action is at
the
spinal cord level (Zemlan et al., 1980). Further, mechanical
and heat hyperalgesia induced by ongoing inflammation
produced by kaolin and carrageenan knee joint injection
or carrageenan paw inflammation is reduced by systemic
or intrathecally administered clonidine and a2-AR agonists
(Hylden et al., 1991; Buerkle et al., 1999). In fact, the
anti-nociception produced by systemically or intrathecally
admi-
nistered clonidine exhibit enhanced efficacy at the level of
the spinal cord for the inflamed paw (ED50 0.1 mg/kg,
i.p.) when compared to the contralateral (ED50 1.8 mg/
kg, i.p.) paw (Hylden et al., 1991). Opioids administered
systemically or supraspinally produce antinociception that
is dependent on the activation of spinal a2-adrenergic
recep-
tors (Yaksh, 1979; Camarata and Yaksh, 1982; Yaksh,
1985). Intrathecally administered clonidine and other a2-
AR agonists are clearly analgesic (Fairbanks et al., 2000;
Danzebrink and Gebhart, 1990; Hylden et al., 1991). Cloni-
dine administered supraspinally and intracerebroventricu-larly
has mixed results with some studies showing
analgesia (Lipman and Spencer, 1979) and others showing
no effect (Ossipov and Gebhart, 1983; Ossipov et al., 1984).
a2-AR agonists inhibit dorsal horn neuron activity,
spinothalamic tract cell activity, and release of substance
P and calcitonin gene-related in the lumbar spinal cord
suggesting a spinal mechanism of action. The antinocicep-
tive effect following spinal or systemic administration of
clonidine also occurs in human subjects (Coombs et al.,
1985; Paalzow, 1974; Lipman and Spencer, 1979; Tamsen
and Gordh, 1984; Bonnet et al., 1990).
4.3. Potentiation by combined administration ofa2-ARs and
opiates
The enhanced effectiveness of TENS in combination with
clonidine probably results from an interaction with the
opiate mediated analgesia produced by TENS and activation
of a2-AR in the central nervous system. Several studies
show potentiation of opiate mediated analgesia by coadmi-
nistration ofa2-AR agonists. Morphine or d-opioid agonists
administered intrathecally show a synergistic analgesic
effect with a2-AR agonists in several tests: abdominal
constriction test, tail flick test, substance P test, dorsal
horn neuron activity, and peripheral nerve injury (Fairbanks
et al., 2000; Bentley et al., 1983; Roerig et al.,
1992;Roerig,
1995; Wilcox et al., 1987; Sullivan et al., 1987; Solomon
and Gebhart 1988; Meert and De Kock, 1994; Joshi et al.,
2000; Spaulding et al., 1979). This potentiation of opiate
mediated analgesia is reversed by systemically or intrathe-
cally administered a2-AR antagonists (Ossipov et al., 1984,
1989, Solomon and Gebhart, 1988) and is reduced in
morphine tolerant rats (Roerig, 1995). In fact, a subanalge-
sic dose of intrathecal clonidine potentiates the
antinocicep-
tive effects of intrathecal morphine (Ossipov et al., 1989).
Isobolographic analysis of the doseresponse curves offixed
ratios of intrathecally administered morphine and clonidine
reveals a synergistic interaction of the two (Ossipov et
al.,
1990). Potentiation of morphine by clonidine also occurs
when both are given systemically (Spaulding et al., 1979).
Intravenous administration of the two drugs may be either
additive or supradditive depending on the dose ratio of
clonidine to morphine and the test used (Ossipov et al.,
1990). Thus, potentiation of TENS effects by clonidine ismost
likely a result of an interaction between a2-AR and
opioid receptors in the central nervous system.
Most of the early clinical studies which focused on study-
ing the interactions between a2-AR and opioid agonists
following epidural or intrathecal administration, show a
potentiation of the analgesic properties of opioids
following
the spinal administration ofa2-AR agonists (Delaunay et al.,
1993; Coombs et al., 1986; Rostaing et al., 1991). Clonidine
administration alone in human subjects is limited by signif-
icant side effects such as drowsiness and hypotension (for
review see Eisenach et al., 1996). However, combining
clonidine with opiates reduces these side effects, reducesthe
intake of opiates, and produces a longer lasting pain
relief (Rostaing et al., 1991). More recently, Goyagi et al.
(1999) demonstrated that combining the use of oral cloni-
dine and epidural morphine produces more potent and
longer lasting postoperative analgesia and decreased opiate
intake than either drug alone, without increasing the inci-
dence of adverse side effects such as nausea, pruritus,
respiratory depression, and bradycardia in patients under-
going total abdominal hysterectomy. Exogenous coadminis-
tration of two or more analgesic agents produces a greater
degree of analgesia, reduced side-effect profile and also a
reduction in the intake of opioids (Price et al., 1996). Thus,
a
combination of a2-AR and opioid agonists results in apotentiated
analgesic effect and reduced side effects due to
a reduction in dose of the exogenously administered
agonists.
4.4. Clinical implications
TENS, a non-invasive, inexpensive, safe, and easy-to-use
analgesic modality by itself may not be as effective an
analgesic agent as when it is combined with other treatment
modalities. TENS, clinically, is rarely administered in
isola-
tion. Combinations of pharmaceutical and non-pharmaceu-
K.A. Sluka, P. Chandran / Pain 100 (2002) 183190 187
-
7/30/2019 Clonidine Paper
6/8
tical treatments for pain control almost always occur. By
understanding mechanisms of action, clinicians may be able
to enhance the effects of non-pharmaceutical therapies and
reduce side effects of pharmaceutical agents to produce
better pain relief. Since TENS produces opiate mediated
analgesia, it follows that its concomitant usage with an
exogenously administered analgesic agent should produce
a greater degree of analgesia and so also a reduction in
dose
of the exogenously administered agent. Several studies have
shown that the intake of opiate analgesics is significantly
reduced in patients being administered with TENS (Solo-
mon et al., 1980; Wang et al., 1997). There is an increased
inhibition of primary thermal hyperalgesia in rats with
inflamed paws if TENS (both low and high frequency) is
used in combination with systemic morphine (0.33 mg/kg
i.p.). The doseresponse curve is shifted to the left
implying
a lower dose of systemically administered morphine is
effective when combined with TENS (Sluka, 2000). The
effectiveness of a reduced dose of morphine translates
clini-
cally into a reduced dosage and reduced side effects inpatients,
thus significantly reducing the unwanted side
effects associated with the use of opioids. In a group of
patients undergoing surgery, Wang et al. (1997) demon-
strate that following the administration of high frequency
TENS postoperatively, there is a reduction in symptoms
such as nausea, dizziness, and pruritus, associated with the
use of morphine, when compared to the administration of
morphine alone or administration of sham TENS group.
In summary, TENS when administered alone may not be
as effective an analgesic agent as when it is combined with
other treatment modalities. Concurrent usage of TENS
with an exogenously administered analgesic agent suchas
clonidine should produce a greater reduction in hyper-
algesia and pain. It would thus be expected that one would
reduce the side effects of clonidine and enhance analgesic
efficacy. Thus, these data suggest that judicious combina-
tions of pharmacological and non-pharmacological thera-
pies will reduce side effects and improve treatment for
pain.
Acknowledgements
This work was supported by grants from the Arthritis
Foundation and KO2AR02201. The authors wish to thankCharles
Cibula and Tammy Lisi for technical assistance,
and Carol Leigh for secretarial support.
References
Bentley GA, Newton SH, Starr J. Studies on the nociceptive
action of a-
agonist drugs and their interactions with opioid mechanisms. Br
J Phar-
macol 1983;79:125134.
Bonnet F, Boico O, Rostaing S, Loriferne JF, Saada M. Clonidine
induced
analgesia in postoperative patients: epidural versus
intramuscular
administration. Anesthesiology 1990;72(3):423427.
Buerkle M, Schapsmeier H, Bantel C, Marcus MAE, Wusten R, Van
Aken
H. Thermal and mechanical antinociceptive action of spinal vs
periph-
erally administered clonidine in the rat inflamed knee joint
model. Br J
Anesth 1999;83(3):436441.
Calvillo O, Ghignone M. Presynaptic effect of clonidine on
unmyelinated
afferent fibersin thespinalcord of thecat. NeurosciLett
1986;64:335339.
Camarata PJ, Yaksh TL. Characterization of spinal adrenergic
receptors
mediating the spinal effects produced by microinjection of
morphine
into the periaqueductal gray. Brain Res 1982;336:133142.
Coombs DW, Saunders RL, Fratkin J, Jensen LE, Murphy C.
Continuousintrathecal hydromorphone and clonidine for intractable
cancer pain. J
Neurosurg 1986;64:890894.
Coombs DW, Saunders RL, Lachance D, Savage S, Ragnarsson TS,
Jensen
LE. Intrathecal morphine tolerance: use of intrathecal
clonidine,
DADLE, and intraventricular morphine. Anesthesiology
1985;62:358363.
Danzebrink RM, Gebhart GF. Antinociceptive effects of
intrathecal adre-
noceptor agonists in a rat model of visceral nociception. J
Pharmacol
Exp Ther 1990;253:698705.
Delaunay L, Leppert C, Dechaubry V, Levron JC, Liu N, Bonnet
F.
Epidural clonidine decreases postoperative requirements for
epidural
fentanyl. Reg Anesth 1993;18:176180.
Dennis SG, Melzack R, Gutman S, Boucher F. Pain modulation by
adre-
nergic agents and morphine as measured by three pain tests. Life
Sci
1980;26:12471259.Drasner K, Fields HL. Synergy between the
antinociceptive effects of
intrathecal clonidine and systemic morphine in the rat. Pain
1988;32:309312.
Eisenach JC, DeKock M, Klimscha W. a2-Adrenergic agonists for
regional
anesthesia a clinical review of clonidine (19841995).
Anesthesiol-
ogy 1996;85:655674.
Facchinetti F, Sandrini G, Petraglia F, Alfonsi E, Nappi G,
Genazzani A.
Concomitant increase in nociceptive flexion reflex and plasma
opioids
following transcutaneous electrical nerve stimulation. Pain
1984;19:295303.
Fairbanks CA, Nguyen HO, Grocholski BM, Wilcox GL. Moxonidine,
a
selective imidazolinealpha2adrenergic receptor agonist,
produces
spinal synergistic antihyperalgesia with morphine in
nerve-injured
mice. Anesthesiology 2000;93(3):765773.
Fielding S, Wilker J, Hynes M, Szewczak M, Novick Jr WJ, Lal H.
A
comparison of clonidine with morphine for antinociceptive and
anti-
withdrawal actions. J Pharmacol Exp Ther 1978;207:899905.
Fleetwood-Walker SM, Mitchell R, Hope PJ, Molony V, Iggo A. An
a2-
receptor mediates the selective inhibition by noradrenaline of
nociciep-
tive responses of identified dorsal horn neurones. Brain Res
1985;334:243254.
Gopalkrishnan P, Sluka KA. Effects of varying frequency and
intensity of
TENS on primary hyperalgesia in rats. Arch Phys Med Rehabil
2000;81:984990.
Goyagi T, Makoto T, Nishikawa T. Oral clonidine premedication
enhances
postoperative analgesia by epidural morphine. Anesth Analg
1999;89:14871491.
Han JS, Chen XH, Sun SL, Xu XJ, Yuan Y, Yan SC, Hao JX, Terenius
L.
Effect of low- and high-frequency TENS on
MetenkephalinArgPhe
and dynorphin A immunoreactivity in human lumbar CSF. Pain
1991;47:295298.
Han JS, Xie GX, Ding ZX, Fan SG. High and low frequency
electroacu-
puncture analgesia are mediated by different opioid peptides.
Pain
1984;2(Suppl):543.
Hargreaves K, Dubner R, Brown F, Flores C, Joris JA. A new and
sensitive
method for measuring thermal nociception in cutaneous
hyperalgesia.
Pain 1988;32:7788.
Hayes AG, Skingle M, Tyers MB. Alpha-adrenoceptor-mediated
antinoci-
ception and sedation in the rat and dog. Neuropharmacology
1986;25:391396.
Hughes G, Lichstein P, Whitlock D, Harker C. Response of plasma
beta-
endorphins to transcutaneous electrical nerve stimulation in
healthy
subjects. Phys Ther 1984;64:10621066.
K.A. Sluka, P. Chandran / Pain 100 (2002) 183190188
-
7/30/2019 Clonidine Paper
7/8
Hylden JLK, Thomas DA, Iadarola MJ, Nahin RL, Dubner R. Spinal
opioid
analgesic effects are enhanced in a model of unilateral in
flammation/
hyperalgesia: possible involvement of noradrenergic mechanisms.
Eur J
Pharmacol 1991;194:135143.
Hylden JLK, Wilcox GL. Pharmacological characterization of
substance P-
induced nociception in mice: modulation by opioid and
noradrenergic
agonists at the spinal level. J Pharmacol Exp Ther
1983;226:398404.
Joshi W, Reuben SS, Kilaru PR, Sklar J, Maciolek H.
Postoperative analge-
sia for outpatient arthroscopic knee surgery with intrarticular
clonidine
and/or morphine. Anesth Analg 2000;90:11021106.
Kalra AB, Urban MO, Sluka KA. Blockade of opioid receptors in
rostral
ventral medulla prevents antihyperalgesia produced by
transcutaneous
electrical nerve stimulation (TENS). J Pharmacol Exp Ther
2001;298:257263.
Khasar SG, Green PG, Chou B, Levine JD. Peripheral nociceptive
effects of
alpha 2-adreneergic receptor agonists in the rat.
Neuroscience
1995;66:427432.
King EW, Sluka KA. The effect of varying frequency and intensity
of trans-
cutaneous electrical nerve stimulation on secondary mechanical
hyperal-
gesia in an animal model of inflammation. J Pain
2001;2:128133.
Kumar VN, Redford JB. Transcutaneous nerve stimulation in
rheumatoid
arthritis. Arch Phys Med Rehabil 1982;63:595596.
Lipman JJ, Spencer PSJ. Further evidence for a central site of
action for the
antinociceptive effect of clonidine-like drugs.
Neuropharmacology
1979;18:731733.
Manheimer C, Carlsson CA. The analgesic effect of transcutaneous
elec-
trical nerve stimulation (TNS) in-patients with rheumatoid
arthritis. A
comparative study of different pulse patterns. Pain
1979;6:329334.
Manheimer C, Lund S, Carlsson CA. The effect of transcutaneous
electrical
nerve stimulation (TNS) on joint pain in-patients with
rheumatoid
arthritis. Scand J Rheumatoid 1978;7:1316.
Mastrianni JA, Abbott FV, Kunos G. Activation of central
m-opioid recep-
tors is involved in clonidine analgesia in rats. Brain Res
1989;479:283
289.
Maze M, Tranquili W. Alpha-2 adrenoceptor agonists: defining the
role in
clinical anesthesia. Anesthesiology 1991;74:581605.
Meert TF, De Kock M. Potentiation of the analgesic properties of
fentanyl-
like opioids with alpha 2-adrenergic receptor agonists in rats.
Anesthe-siology 1994;81(3):677688.
Nakamura M, Ferreira S. Peripheral analgesic action of
clonidine: media-
tion by release of endogenous enkephalin-like substances. Eur J
Phar-
macol 1988;146:223228.
Omote K, Kitahata LM, Collins JG, Nakatani K, Nakagawa I.
Interaction
between opiate subtype and alpha-2 adrenergic agonists in
suppression
of noxiously evoked activity of WDR neurons in the spinal dorsal
horn.
Anesthesiology 1991;74:737743.
Ossipov MH, Gebhart GF. Absence of antinociceptive effect of
alpha-2
agonists microinjected in the periaqueductal gray of the rat.
Brain
Res 1983;289:349354.
Ossipov MH, Harris S, Lloyd P, Messineo E. An isobolographic
analysis of
the antinociceptive effect of systemically and intrathecally
administered
combinations of clonidine and opiates. J Pharamacol Exp Ther
1990;255:11071115.Ossipov MH, Malseed RT, Eisenman LM, Goldstein
FJ. Effect ofa2-adre-
nergic agonists upon central etorphine antinociception in the
cat. Brain
Res 1984;309:135142.
Ossipov MH, Suarez LJ, Spaulding TC. Antinociceptive
interactions
between alpha-2 adrenergic and opiate agonists at the spinal
level in
rodents. Anesth Analg 1989;68:194200.
Paalzow L. Analgesia produced by clonidine in mice and rats. J
Pharm
Pharmacol 1974;26:361362.
Pertovaara A. Antinocicpetion induced by alpha-2-adrenoceptor
agonists,
with special emphasis on medetomidine studies. Prog
Neurobiol
1993;40:691709.
Price DD, Mao J, Lu J, Caruso FS, Frenk H, Mayer DJ. Effects of
the
combined oral administration of NSAIDs and dextromethorphan
on
behavioral symptoms indicative of arthritic pain in rats.
Pain
1996;68:119127.
Proudfit HK. Pharmacologic evidence for the modulation of
nociception by
noradrenergic neurons. Prog Neurobiol 1988;77:357370.
Robinson AJ. Transcutaneous electrical nerve stimulation for the
control of
pain in musculoskeletal disorders. J Orthop Sports Phys Ther
1996;24:208227.
Roerig SC. Decreased spinal morphine/clonidine antinoceiceptive
syner-
gism in morphine tolerant mice. Life Sci
1995;56(5):PL115122.Roerig SC, Lei S, Kitto K, Hylden JK, Wilcox
GL. Spinal interactions
between opioid and noradrenergic agonists in mice:
multiplicativity
involves delta and alpha-2 receptors. J Pharmacol Exp Ther
1992;262(1):365374.
Rostaing S, Bonnet F, Levron JC, Vodiah J, Pluskwa F, Saada M.
Effect
of epidural clonidine on analgesia and pharmacokinetics of
epidural
fentanyl in postoperative patients. Anesthesiology
1991;75:420
425.
Sjolund B, Eriksson M. The influence of naloxone on analgesia
produced
by peripheral conditioning stimulation. Brain Res
1979;173:295301.
Skingle M, Hayes AG, Tyers MB. Antinociceptive activity of
clonidine in
the mouse, rat and dog. Life Sci 1982;31:11231132.
Sluka KA. Blockade of calcium channels can prevent the onset of
second-
ary hyperalgesia and allodynia induced by intradermal injection
of
capsaicin. Pain 1997;71:165178.Sluka KA. Systemic morphine in
combination with TENS produces an
increased analgesia in rats with acute inflammation. J Pain
2000;1:204211.
Sluka KA, Westlund K. Behavioral and immunohistochemical changes
in
an experimental arthritis model in rats. Pain
1993;55:367377.
Sluka KA, Bailey K, Bogush J, Olson R, Ricketts A. Treatment
with either
high or low frequency TENS reduces the secondary
hyperalgesia
observed after injection of kaolin and carrageenan into the knee
joint.
Pain 1998;77:97102.
Sluka KA, Christy MR, Peterson WL, Rudd SL, Troy SM.
Reduction
of pain-related behaviors with either cold or heat treatment in
an
animal model of acute arthritis. Arch Phys Med Rehabil
1999a;80:
313317.
Sluka KA, Deacon M, Stibal A, Strissel S, Terpstra A. Spinal
blockade of
opioid receptors prevents the analgesia produced by TENS in
arthritic
rats. J Pharmacol Exp Ther 1999b;289:840846.
Solomon RA, Viernstein MC, Long DM. Reduction of postoperative
pain
and narcotic use by transcutaneous electrical nerve stimulation.
Surgery
1980;87:142146.
Solomon RE, Gebhart GF. Intrathecal morphine and clonidine:
antinoci-
ceptive tolerance and cross-tolerance and effects on blood
pressure. J
Pharmacol Exp Ther 1988;245(2):444454.
Spaulding TC, Fielding S, Venafro JJ, Lal H. Antinociceptive
activity of
clonidine and its potentiation of morphine analgesia. Eur J
Pharmacol
1979;58:1925.
Sullivan AF, Dashwood MR, Dickenson AH. Alpha2-adrenoceptor
modu-
lation of nociception in rat spinal cord: location, effects and
interactions
with morphine. Eur J Pharmacol 1987;138:169177.
Sullivan AF, Kalso EA, Mcquay HJ, Dickenson AH. The
antinociceptive
actions of dexmedetomidine on dorsal horn neuronal responses in
the
anaesthetized rat. Eur J Pharmacol 1992;215:127133.
Tamsen A, Gordh Jr T. Epidural clonidine produces analgesia.
Lancet
1984;2:231232.
Van Zweiter PA. Centrally acting antihypertensive drugs.
Present
and future (review). Clin Exp Hypertens (NY) 1999;21(56):859
873.
Wang B, Tang J, White PF, Naruse R, Sloninsky A, Kariger R, Gold
J,
Wender RH. Effect of intensity of transcutaneous acupoint
electrical
stimulation on the postoperative analgesic requirement. Anesth
Analg
1997;85:406413.
Wilcox GL, Carlsson KH, Jochim A, Jurna I. Mutual potentiation
of anti-
nociceptive effects of morphine and clonidine in rat spinal
cord. Brain
Res 1987;405:8493.
K.A. Sluka, P. Chandran / Pain 100 (2002) 183190 189
-
7/30/2019 Clonidine Paper
8/8
Willcockson WS, Chung JM, Hori Y, Lee KH, Willis WD. Effects
of
iontophoretically released amino acids and amines on primate
spinotha-
lamic tract cells. J Neurosci 1984;4:732740.
Winter CA, Risley HA, Nuss GW. Carrageenan induced edema in hind
paw
of the rat as an assay for anti-inflammatory drugs. Proc Soc Exp
Biol
Med 1962;111:544547.
Woolf CJ, Barrett D, Mitchell D, Myers R. Naloxone-reversible
peripheral
electroanalgesia in intact and spinal rats. Eur J Pharmacol
1977;45:311
314.
Yaksh TL. Direct evidence that spinal serotonin and
noradrenaline term-
inals mediate the spinal antinociceptive effects of morphine in
the
periaqueductal grad. Brain Res 1979;160:180185.
Yaksh TL. Pharmacology of spinal adrenergic systems which
modulate
spinal nociceptive processing. Pharmacol Biochem Behav
1985;22:845858.
Zemlan FP, Corrigan SA, Pfaff DW. Noradrenergic and
serotonergic
mediation of spinal analgesia mechanisms. Eur J Pharmacol
1980;61:111124.
K.A. Sluka, P. Chandran / Pain 100 (2002) 183190190