Embed Size (px)
Citation preview

CLL what do I need to know as an Internist in 2018
Taimur Sher MD
Associate Professor of Medicine
Mayo Clinic

• 70 y/o white male for yearly medical evaluation
• Doing well and healthy
• Past medical history
Hypertension
Dyslipidemia
Coronary artery disease
• Normal exam
• CBC:
Hb 12.5
WBC 12.6
Platelet count 156/ uL
Absolute lymphocyte count: 7.1
Absolute neutrophil count 3.5
Case 1

Case 2
• 48 y/o female with 6 months of weight loss, elbow and knee swelling and itchy rash
• 1 year ago rheumatoid arthritis. On Mtx.
• Mother died of non-hodgkin lymphoma.
• Exam: Chronically ill appearing female, inflamed elbow and knee.
• CBC: Hb 7.8; WC 15. platelet 105. ALC 10.5
• CRP-105; Beta-2 microglobulin 14
• Flow: CD 5+, CD 23+ kappa
restricted B-cells.

Chronic Lymphocytic Leukemia (CLL)
• Most prevalent adult B-cell leukemia in west (~15,000 cases / year)
• Median age at diagnosis is 72yrs
• Presentation:
• Incidental
• Disease related tumor burden
• Autoimmune phenomenon
• Infections
Ries LAG et al. http://seer.cancer.gov/csr/1975_2004/, based on November 2006 SEER data submission. Accessed September 17, 2007; Stilgenbauer S. Hematology. 2004;1:164-170.
Lymph Nodes
CD23+
Bone marrow Blood

• ALC: >5,000/µL—mature-appearing lymphocytes
• Immunophenotype
CD5+ / CD19+ / CD23+ / surface Ig light-chain restricted ( or )
• BM biopsy: not required for diagnosis
>30% lymphocytes on aspirate
• What do I order for work up?
CBC with diff
Flow cytometry peripheral blood
Liver and renal function
LDH, beta-2 microglobulin
Quantitative Igs
FISH in peripheral blood
Somatic hypermutation
CLL Diagnosis

Prognostic Versus Predictive Factors
• Prognostic factor
Situation, condition, or characteristic used to estimate overall outcome of disease, independent of treatment
• Predictive factor
Situation, condition, or characteristic that predicts the efficacy of a therapy
Prognostic factor that provides information on effect of a treatment

Prognostic Factors Associated With Inferior Survival in CLL
• FISH cytogenetic abnormalities
17p deletion
11q deletion
• Complex cytogenetic abnormalities
• Unmutated (<2% homology to germline) IgHV
• Expression of ZAP-70 (20% positive)
• Expression of CD38 (30% positive)

Clinical Stage
• Rai staging
Stage 0 Lymphocytosis
Stage I Lys+adenopathy
Stage II Lys+ Splenomegaly
Stage III Anemia
Stage IV Thrombocytopenia

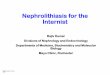
FISH: Cytogenetics are important
Months
100
80
60
40
20
0
0 12 24 36 48 60 72 84 96 108 120 132 144 156 168 180
Pa
tien
ts S
urv
ivin
g, %
17p deletion
11q deletion 12q trisomy
Normal 13q deletion as
sole abnormality
Months 1. Dohner et al. N Engl J Med. 2000;343:1910.

Su
rviv
ing
, %
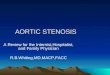
Survival of CLL Patients With Mutated Versus Unmutated IgHV Gene
1. Hamblin TJ et al. Blood. 1999;94:1848-1854.
All Patients (N = 84) Stage-A CLL Patients (n = 62)
Su
rviv
ing
, %
0 50 100 150 200 250 300 0
20
40
60
80
100
Months
P = .0008
Months
P = .001
0 50 100 150 200 250 300 0
20
40
60
80
100
Mutated
Unmutated Unmutated
Mutated

CLL-International Prognostic Index (CLL-IPI)
Variable Adverse Factor Grading
TP53 / 17p Mutated/deleted 4
IgHV status Unmutated 2
B2M >3.5 mg/L 2
Clinical stage Binet B/C or Rai II-IV 1
Age > 65 y 1
Prognostic score 0-10
Risk Group Score
Low 0-1
Intermediate 2-3
High 4-6
Very high 7-10 1. The International CLL-IPI Working Group. Lancet Oncol. 2016.

1. The International CLL-IPI Working Group. Lancet Oncol. 2016;17:779-790.
CLL-IPI: OS Outcomes
100
0 0
20
60
80
40
24 156 12
Time From Study Entry, mo
OS
, %
Training Dataset
P < .0001
48 60 72 84 96 108 120 132 144 36
341 331 0 339 279 270 224 169 118 81 40 20 8 320
474 441 1 452 352 312 232 143 83 52 27 13 5 415
337 284 0 314 205 178 120 69 40 19 12 4 1 256
62 31 — 46 16 13 5 3 0 —
— — —
25
Low risk
Intermediate risk
High risk
Very high risk
Number at risk
100
0 0
20
60
80
40
24 156 12
Time From Study Entry, mo
OS
, %
MAYO Cohort
P < .0001
48 60 72 84 96 108 120 132 144 36
390 316 3 338 259 226 188 151 105 64 34 19 7 288
272 224 0 247 178 146 111 81 46 27 12 1 1 198
149 110 — 127 82 64 44 28 14 9 3 0 — 100
27 18 — 24 5 1 1 1 0 — — — — 12
Low risk
Intermediate risk
High risk
Very high risk
Number at risk
100
0 0
20
60
80
40
24 156 12
Time From Study Entry, mo
Internal-Validation Dataset
P < .0001
48 60 72 84 96 108 120 132 144 36
186 173 0 181 152 146 125 84 56 39 26 11 3 168
200 180 0 191 137 125 88 55 35 22 10 5 1 168
147 117 0 130 84 69 52 24 17 13 6 2 1 98
52 30 —
43 14 8 2 1 1 0 — — — 20
Low risk
Intermediate risk
High risk
Very high risk
Number at risk
100
0 0
20
60
80
40
24 156 12
Time From Study Entry, mo
SCAN Cohort
P < .0001
48 60 72 84 96 108 120 132 144 36
242 237 80 238 228 223 220 210 192 168 159 144 115 233
104 99 12 103 89 78 71 61 46 42 35 25 17 95
56 51 2 55 39 36 32 25 16 11 10 6 3 47
14 8 — 10 7 4 3 1 1 0 — — — 7
Low risk
Intermediate risk
High risk
Very high risk
Number at risk
Low risk
Intermediate risk
High Risk
Very high risk

Multivariable Model for Time-to-First CLL Treatment (N = 687; 193 treated)
Characteristic HR P
IgHV mutation status (UM vs M) 10.68 <.0001
Diameter of largest cervical LN (cm) 1.32 <.0001
FISH category (11q del vs others) 1.86 .001
FISH category (17p del vs others) 2.12 .01
Number of involved LN sites (3 vs <3) 1.64 .004
LDH (IU/L/100) for IgHV mutated 2.36 .002
Wierda WG et al. J Clin Oncol. 2011;29:4088-4095.

CLL-IPI: Time-to-First CLL Treatment Outcomes1
Low risk Intermediate risk High risk Very high risk
264 253 9 2 44 21 238 261
110 93 2 4 4 73 108
25 17 2 13 23
4 2 1 4
Low risk
Intermediate risk
High risk
Very high risk
Number at risk
74
8
2 1
222 182 151 213
54 31 20 42
10 5 3 7
1 1 1 1
105
12
2
1
390 291 4 2 25 13 257 324
272 140 1 0 110 174
149 59 1 41 77
27 3 2 7
50
3
2 0
219 155 117 183
88 41 23 66
32 10 4 19
1 0
79
11
2
242 202 81 54 111 101 195 212
104 45 8 6 38 70
56 10 2 6 19
14 3 2 4
118
10
2 2
190 168 155 173
28 21 18 23
5 4 4 4
1 1
141
12
3
1 0
5
2
3
1
100
0 0 36
50
156 132
20
60
Tim
e to
Fir
st T
rea
tmen
t, %
90
80
40
30
10
70
144 84 120 48 12
Watch-and-Wait Patients
108 24 60 72 96
P < .0001
100
0 0 36
50
156 132
20
60
90
80
40
30
10
70
144 84 120 48 12
MAYO Cohort
108 24 60 72 96
P < .0001
100
0 0 36
50
156 132
20
60
Tim
e to
Fir
st T
rea
tmen
t, %
90
80
40
30
10
70
144 84 120 48 12
SCAN Cohort
108 24 60 72 96
P < .0001
Time From Diagnosis, mo Time From Diagnosis, mo Time From Diagnosis, mo
1. The International CLL-IPI Working Group. Lancet Oncol. 2016;17:779-790.

IWCLL-NCI: Indications to Initiate Treatment for CLL1
• Constitutional symptoms referable to CLL
• Progressive marrow failure
• Autoimmune anemia +/- thrombocytopenia poorly responsive to steroids or other treatment
• Massive (>6 cm) or progressive splenomegaly
• Massive (>10 cm) or progressive lymphadenopathy
• Progressive lymphocytosis, >50% increase over 2 months or LDT <6 months
• NO EARLY TREATMENT, EVEN FOR HIGH-RISK PATIENTS
1. Hallek M et al. Blood. 2008;111:5446-5456.

Treatment

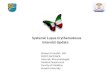
The cancer cell… does not live in isolation

Cell proliferation survival, and migration
B-cell receptor
CD
79
B
CD
79
A
BTK Blnk
Lyn Syk
Fyn PLCγ2
CD19
CD38
Toll-like receptor(s)
MYD88 L265P
MYD88 L265P
TIR
AP
IRAK4
IRAK1
TRAF6
p50
PI3K p85
PIP3 AKT
mTOR
RAS
RAF
MEK
IkBa
p60 PKC
IP3 DAG
ERK / MAPK NFAT
Ca++
MYC NFkB 4E-BP1
SK60
Proteasome
T-cells
Bcl-2 BAX
BIM
PD-L1 PD-1
?
BTK
FOXO3a p53 IkB
XPO1 p53 IkB FOXO3a
Centrosome
Aurora kinase
p53 MYC IkBa
AKT
Deactivated/degraded
CAR T-cells

1960s / 1970s
Alkylating agents – Chlorambucil – Cyclophosphamide
2000s
Chemoimmunotherapy (FCR) Alemtuzumab CD20 mAbs Bendamustine
1990s
Combination chemotherapy
Evolution of Therapy for CLL
1980s
Purine nucleosides – Fludarabine – Pentostatin – Cladribine
2010s
Small molecule inhibitors – BCR pathway – Bcl-2

Factors affecting treatment choice
Patient related
• Age
• Medical comorbidities
• Concurrent medications
Drug interactions
• Logistics
Disease related
• Cytogenetic risk: FISH
TP 53/ 17p deletion
11q deletion
• IgVH mutation status

CLL10: PFS Outcomes With FCR Versus BR1
1. Eichhorst B et al. ASH 2014.

Choice of initial CIT in younger patients: BR vs. FCR
• FCR superior to BR with respect response rate and progression free survival
• No OS benefit, though survival analysis not mature
• Severe neutropenia and infections more frequently observed with FCR (84% and 39%) vs BR (59% and 25%, respectively)
• Increased frequency of infectious complications and cytopenias with FCR was more pronounced in patients aged >65 y
• No PFS benefit for FCR in patients aged >65 y
1. Eichhorst B et al. ASH 2014.

Predictive factor: PFS by IgHV Mutation Status1
P<0.0001
PF
S, %
Time, y
0
25
50
75
100
0 1 2 3 4 8 9 10 5 6 7 11 12 13 14 15 16
1. Thompson PA et al. Blood. 2016;127:303-309.

Minimal Residual Disease and IgHV Mutation Status1
100
0
0
50
90
20
60
PF
S, %
Months
90
70
40
30
10
6 12
80
84 78 72 66 60 54 48 42 36 30 24 18
IgHV M, MRD neg IgHV UM, MRD neg IgHV M, MRD pos IgHV UM, MRD pos
1. Thompson PA. MDACC unpublished.
P = .02

Phase 3 CLL11 Trial: Obinutuzumab Plus Chlorambucil in Newly Diagnosed CLL1
1:2:2
1. Goede V et al. N Engl J Med. 2014;370:1101-1110.
• Patients with newly diagnosed CLL and significant comorbidities
– CIRS score >6 and/or estimated CrCl <70 mL/min
– N = 781
Chlorambucil 0.5 mg/kg PO, d 1 and 15, x 6 cycles
Obinutuzumab 1,000 mg IV cycle 1, d 1, 8, 15; cycles 2-6 d 1 plus chlorambucil
Rituximab 375 mg/m2 IV, cycle 1 on d 1; 500 mg/m2 cycles 2-6, d 1 plus chlorambucil

CLL11: PFS Outcomes1
Obinutuzumab/chlorambucil was associated with prolonged PFS vs chlorambucil (left) and rituximab/chlorambucil (right)
Obin/Chl vs Chl
Obin/Chl vs Ritux/Chl
1. Goede V et al. N Engl J Med.. 2014;370:1101-1110

Updated CLL11 Results: OS1
No statistically significant difference in OS is noted vs rituximab/chlorambucila
Time to next treatment for obin/chl is about 48 mo
Obinutuzumab/chlorambucil was associated with
significant OS benefit vs chlorambucila

Ibrutinib vs Chlorambucil
All patients All d(11q)
Ibrutinib led to 99% reduction in risk of progression or death in high-risk del(11q) subgroup (82% reduction in those without del(11q) compared with chemotherapy
88% reduction in risk of progression or death in for patients randomized to ibrutinib
1. Barr PM et al. ASH 2016.

Venetoclax in Relapsed CLL: Progression-Free Survival and Duration of Response1
1. Roberts AW et al. N Engl J Med. 2016;374:311-322.

Current “Standards of Care” for the CLL Patient
• Untreated, high-risk: watch and wait
• First-line therapy
Del(17p): ibrutinib
“Elderly”: chlorambucil + CD20 mAb
Fit CIT-eligible: FCR / BR
• Salvage treatments for active disease, including del(17p)
BTK inhibitor (ibrutinib)
PI3K inhibitor (idelalisib) + rituximab
• Rel / Ref del(17p): venetoclax
• Richter’s transformation: intensive CIT, then allo-SCT

Novel agents what to look for
• Ibrutinib:
Oral agent; targets Bruton’s tyrosine kinase
Effective for 17p deletion
Atrial fibrillation
Bleeding
Infections
• Venetoclax:
Oral agent; targets Bcl2
Tumor lysis syndrome
Drug interactions
Cytopenias

Summary
• CLL is the most common adult leukemia
• Diagnosis is made by flowcytometry evaluation of the blood
• FISH studies and IgVH somatic hypermutation are most important prognostic/predictive markers: 17 p deletion, 11q deletion and unmutated are bad
• Not everybody needs treatment at diagnosis
• Chemo-immunotherapy is the frontline of treatment- Age is important
• Ibrutinib is effective in 17p- watch for Afib and bleeding
• Venetoclax is highly effective watch for infections, drug interactions, tumor lysis syndrome