Embed Size (px)
Citation preview

How to cite this article: A N Bagate, V V Deshmukh, S L Gaikwad, D S Jadhav, A G Valand. Clinicopathological study of head and neck
lesions in a rural tertiary care centre. MedPulse International Journal of Pathology. October 2017; 4(1): 01-06.
https://www.medpulse.in/Pathology/
Original Research Article
Clinicopathological study of head and neck lesions
in a rural tertiary care centre
A N Bagate1, V V Deshmukh
2*, S L Gaikwad
3, D S Jadhav
4, A G Valand
5
1Associate Professor,
2Tutor,
3,4Associate Professor,
5Professor and Head, Department of Pathology, Swami Ramanand Teerth Rural
Government Medical College Ambajogai, Maharashtra, INDIA.
Email: [email protected]
Abstract Background: Head neck lesion is the frequently found presentation of patients seen in clinical practice. The head and
neck pathology is very important as diverse diseases occur in various organs located in close proximity to each other.
Aim: This study is conducted to document the clinicopathological aspects of head and neck lesions, frequency as
compared to other lesions, analyse the data regarding the relative proportion of non neoplastic and neoplastic lesions.
Material Method: Head and neck lesions were divided under nine groups: 1. Thyroid 2.Salivary glands 3.Lymph nodes
4.Nose, paranasal sinuses and nasopharynx 5.Oral cavity and oropharynx Hypopharynx and larynx 6.Ear 7.Eye 8.Skin
and 9. Soft tissue. Information regarding history, clinical findings and diagnosis was collected and studied with gross and
light microscopic findings Result: Out of 370 cases of head and neck region 216 cases were classified as non neoplastic
(58.4%), 83 cases as benign (22.4%), and 71cases as malignant (19.2%). Among all head and neck lesions Females
(54.3%) outnumbered males (45.7%). Non neoplastic lesions contributed 58.4% and neoplastic lesions contributed
41.6%. Benign lesions contributed 53.9% and malignant lesions contributed 46.1% of total number of neoplastic lesions.
Among all benign lesions Females (54.2%) outnumbered Males (45.8 %). Among all malignant lesions Males (52.1%)
outnumbered Females (47.9%) Conclusion: Among all the head and neck lesions, non neoplastic lesions were
predominant with a female preponderance. Benign tumors were in excess of malignant tumors. Malignant tumours were
common in elderly men and benign tumours were common in middle aged females.
Key Words: Clinicopathological, Head, Neck, Rural, Tertiary.
*Address for Correspondence:
Dr. V V Deshmukh, Tutor, Department of Pathology, Swami Ramanand Teerth Rural Government Medical College Ambajogai,
Maharashtra, INDIA.
Email: [email protected]
Received Date: 29/07/2017 Revised Date: 14/08/2017 Accepted Date: 27/09/2017
DOI: https://doi.org/10.26611/105411
INTRODUCTION Pathology of head and neck is an easy sounding title for
complex subject matter. The head and neck pathology is
very important as diverse diseases occur in various organs
located in close proximity to each other between base of
skull and thoracic aperture. Thus, “Lesions of head and
neck” constitute wide range of diseases encountered in
the anatomically complex region extending from the
frontal sinuses, orbits, roof of the sphenoidal sinuses and
clivus proximally to the upper borders of the sternal
manubrium, clavicles and first ribs distally. This includes
the ears, eyes, upper aero digestive tract, salivary glands,
dental apparatus, thyroid and parathyroid glands, as well
as all the epithelial, fibrous, fatty, muscular, vascular,
lymphoid, cartilaginous, osseous and neural tissues or
structures related to them. Reason for assembling all these
different organs under head and neck is that the proximity
of the organs makes it difficult for the surgical pathologist
to focus one of these organs and neglect the pathology of
others which are only a centimeter apart. Another reason,
however, is that the upper respiratory tract and the upper
digestive tract, which meet in the larynx, have some basic
diseases in common.1
The most important among these
are malignant neoplasms occurring in several anatomical
sites in head and neck region such as oral cavity, ear,
scalp, nasal cavities, paranasal sinuses, nasopharynx,
Access this article online
Quick Response Code:
Website:
www.medpulse.in
Accessed Date:
04 October 2017

MedPulse International Journal of Pathology, Print ISSN: 2550-7605, Volume 4, Issue 1, October 2017 pp 01-06
MedPulse International Journal of Pathology, Print ISSN: 2550-7605, Volume 4, Issue 1, October 2017 Page 2
hypopharynx, oropharynx and salivary glands. They are
characterised by diverse patterns of biological behaviour
and well established association with tobacco and alcohol
use.2
Since many patients first come to medical attention
because of discovery of lump in neck, the proper
diagnostic approach to such lesions is of paramount
importance. Such tumors should always be considered of
utmost gravity until a definite cause is established.3
MATERIAL AND METHOD It is a prospective study of 370 cases belonging to head
and neck at a tertiary care rural hospital and medical
college over a period of 2 years from July 2014 to June
2016. The lesions of head and neck region were selected
on basis of clinical history, examination findings and
clinical diagnosis; which were then subjected to biopsy,
curative surgery and detail gross and histopathological
examination. Head and neck lesions were divided under
following nine groups. 1. Thyroid 2.Salivary glands
3.Lymph nodes 4.Nose, paranasal sinuses and
nasopharynx 5.Oral cavity and oropharynx Hypopharynx
and larynx 6.Ear 7.Eye 8.Skin and 9. Soft tissue. Patients
who were treated conservatively or patients referred to
other hospitals were excluded from this study.
Information regarding history, clinical examination
findings and clinical diagnosis was collected. Surgical
specimens obtained were subjected to histopathological
tissue processing and paraffin blocks were prepared, 3 to
5 micron thick sections were cut from each paraffin block
and stained with hematoxylin and eosin stain.
RESULTS The present study includes a total of 370 head and neck
lesions during study period 2 years Frequency: Out of
total 4764 cases, 370 cases belonged to head and neck
region contributing 7.8%. Age wise distribution:
Maximum numbers of cases were in the age group 21-40
years [159 cases (43%)]. Minimum numbers of cases
were in age group > 60 years [42 cases (11.4%)]. Non
neoplastic lesions of head and neck occurred in all age
groups with peak distribution in the age group of 21-40
years [94 cases (43.5%)]. The youngest patient was 1
years old while the oldest was 88 years of age. Mean age
was 36.2 years. Neoplastic lesions of head and neck
occurred in all age groups with peak distribution in the
age group of 21-40 years [65 cases (42.2%)]. The
youngest patient was 5 years old while the oldest was 86
years of age. Mean age was 44.6 years. Benign tumors of
head and neck occurred in all age groups with peak
distribution in the age group of 21-40 years [37 cases
(44.6%)]. The youngest patient was 5 years old while
oldest was 75 years old. The mean age was 39.5 years.
Malignant head and neck lesions occurred in all age
groups, most commonly in age group of 21-40 years [28
cases (39.4%)], followed by age group 41-60 years[26
cases (36.6%)]. The youngest patient was 20 years old
while the oldest patient was 86 years old. 59.2% of cases
were above 40 years. The mean age was 50.6 years.
Sex wise distribution: Out of 370 cases, females (201
cases) outnumbered males (169 cases) contributing 54.3%
and 45.7% respectively. The M: F ratio was 1:1.2.
Females [122cases (56.5%)] outnumbered males [94
cases (43.5%)] with M: F ratio of 1:1.3 among all non
neoplastic lesions. Females [79 cases (51.3%)]
outnumbered males [75 cases (48.7%)] with M: F ratio of
1:1.1 among all neoplastic lesions. Females [45 cases
54.2%)] outnumbered males [38 cases (45.8%)] with M:
F ratio of 1:1.2 among all benign tumours. Males [37
cases (52.1%)] outnumbered females [34 cases (47.9%)]
with M: F ratio of 1.1:1 among all malignant lesions.
Distribution according to Site: Frequency of head and
neck lesions was maximum in Skin and soft tissue region
[122 cases (33%)] and minimum in hypopharynx and
larynx region [4 cases (1.1%)], second most common
lesions are in thyroid region [91 cases (24.6%)].
Distribution of non neoplastic and neoplastic lesions: Of total 370 cases, 216 (58.4%) were non neoplastic and
154 (41.6%) were neoplastic. Goiter (diffuse and
multinodular) was the most common non neoplastic
lesion [43 cases (19.9%)], followed by nonspecific
inflammatory lesions [40 cases (18.5%)].
Distribution of benign and malignant tumours: Of
total 154 neoplastic cases, 83 (53.9%) were benign and 71
(46.1%) were malignant. Follicular adenoma of thyroid
and Lipoma were the most common benign tumours [11
cases each (13.3%)], followed by Haemangioma [10
cases (12.1%)]. Squamous cell carcinoma at various sites
was the most common malignancy observed, [38 cases
53.5%] followed by papillary carcinoma of thyroid [14
cases (19.7%)].
Distribution according to clinical presentation: In the
present study the commonest complaint was swelling,
which was present in 296 cases (80%), followed by
ulcerous growth in 22 cases (6%) and ear discharge in 12
cases (3.2%)
Duration of complaints: Duration of complaints was
between 1 months -1 year in 85.4% of cases, less than
1month in 7.6% of cases, 1-3 years in 4.9% of cases, and
>3 years in 2.2% of cases.
Table 1: Age- wise distribution of head and neck lesions
Age in years (Range) No. of cases Percentage (%)
0-20 60 16.2
21-40 159 43.0
41-60 109 29.5
> 60 42 11.4
Total 370 100

A N Bagate, V V Deshmukh
Copyright © 2017, Medpulse Publishing Corporation,
Table 2: Sex- wise distribution of head and neck lesions
Sex No. of cases Percentage (%)
Male 169 45.7
Female 201 54.3
Total 370 100
Table 3: Age and sex wise distribution of non neoplastic and
neoplastic lesions
Non neoplastic Neoplastic
Benign Malignant
Age (Years)
0-20 45 13
21-40 94 37
41-60 63 21
> 60 14 12
Total 216 83
Mean age 36.2 39.5
Sex
M 94 38
F 122 45
Total 216 83
M:F 1:1.3 1:1.2 1.1:1
Table 4: Distribution of head and neck lesions according to site
Sr. Site of lesion Frequency (No
of cases)
1 Thyroid 91
2 Salivary glands 21
3 Lymph nodes 28
4 Nose, paranasal sinuses
and nasopharynx 13
5 Oral cavity and
oropharynx 66
6 Hypopharynx and larynx 04
7 Ear 19
8 Eye 08
9 Skin and soft tissue 122
Total 370
Table 5: Distribution of head and neck lesions according to clinical
presentation
Complaints No. of cases Percentage (%)
Swelling 296
Sore throat 11
Ulcer 11
Ulcerous growth 22
White patch 03
Change in voice 03
Nasal obstruction 08
Ear ache 02
Ear discharge 12
Headache 01
Epiphora 01
Total 370
, V V Deshmukh, S L Gaikwad, D S Jadhav, A G Valand
Copyright © 2017, Medpulse Publishing Corporation, MedPulse International Journal of Pathology, Volume 4, Issue 1
wise distribution of head and neck lesions
Percentage (%)
45.7
54.3
100
Age and sex wise distribution of non neoplastic and
Neoplastic Total
Malignant
01 59
28 159
26 110
16 42
71 370
50.6
37 169
34 201
71 370
1.1:1
Distribution of head and neck lesions according to site
Frequency (No Percentage
(%)
24.6
5.7
7.6
3.5
17.8
1.1
5.1
2.2
33.0
100.0
Distribution of head and neck lesions according to clinical
Percentage (%)
80.0
3.0
3.0
6.0
0.8
0.8
2.2
0.5
3.2
0.3
0.3
100
Table 6: Duration of complaints of head and neck lesions
Duration of head and neck
lesions No. of cases
<1 month
1month-1 year
1-3 years
>3 years
Total
Figure 1: Age-wise distribution of head and neck lesions
Figure 2: Sex- wise distribution of head and neck lesions
Figure 3: Distribution of head and neck lesions according to site
16%
43%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
0-20 21-40p
erc
en
tag
e
age in years
Female54.3%
3.5%
1.1%
5.1%
2.2%
Thyroid
Salivary glands
Lymph nodes
Nose, paranasal sinuses and …
Oral cavity and oropharynx
Hypopharynx and larynx
Ear
Eye
Skin and soft tissue
, Issue 1 October 2017
of complaints of head and neck lesions
No. of cases Percentage (%)
28 7.6
316 85.4
18 4.9
08 2.2
370 100
wise distribution of head and neck lesions
wise distribution of head and neck lesions
Distribution of head and neck lesions according to site
30%
11%
41-60 >60
age in years
Male45.7%
24.6%
5.7%
7.6%
3.5%
17.8%
5.1%
2.2%
33.0%

MedPulse International Journal
MedPulse International Journal of Pathology, Print ISSN:
Figure 4: Distribution of head and neck lesions according to clinical
presentation
Figure 5: Duration of complaints of head and neck lesions
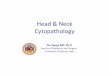
Figure 6: Papillary carcinoma thyroid –photomicrograph showing
papillae lined by single layer of cuboidal cell having Orphan Annie
eyed nuclei. (H and E, 40 X)
2.97
2.97
5.95
0.81
0.81
2.16
0.54
3.24
0.27
0.27
0 20 40 60
Swelling
Sore throat
Ulcer
Ulcerous growth
White patch
Change in voice
Nasal obstruction
Ear ache
Ear discharge
Headache
Epiphora
percentage
0
10
20
30
40
50
60
70
80
90
<1 month 1month-1 year 1-3 years
Pe
rce
nta
ge
Duration
Journal of Pathology, Print ISSN: 2550-7605, Volume 4, Issue 1, October 2017 pp 01
ISSN: 2550-7605, Volume 4, Issue 1, October 2017
Distribution of head and neck lesions according to clinical
and neck lesions
photomicrograph showing
papillae lined by single layer of cuboidal cell having Orphan Annie
Figure 2: Mucoepidermoid carcinoma
mucous, squamous, and intermediate cells. Mucin filled spaces
can be clearly seen. (H
Figure 3: Lymphoma (DLBCL)- Clinical photograph of a 75 year old
female patient presented with right submandibular swelling since
6 month
Figure 3a: Lymphoma (DLBCL) - Photomicrograph showing areas of
sinus histio-cytosis admixed with darkly stained small to large
undifferentiated cells.(H
80
80 100
>3 years
2017 pp 01-06
Page 4
Mucoepidermoid carcinoma-Photomicrograph showing
squamous, and intermediate cells. Mucin filled spaces
can be clearly seen. (H and E, 10X)
Clinical photograph of a 75 year old
female patient presented with right submandibular swelling since
Photomicrograph showing areas of
cytosis admixed with darkly stained small to large
undifferentiated cells.(H and E, 40X)

A N Bagate, V V Deshmukh
Copyright © 2017, Medpulse Publishing Corporation,
Figure 4: Tuberculous lymphadenitis- Photomicrograph showing
shows langhans giant cells, caseous necrosis and epitheloid cells.
(H and E, 40X)
DISCUSSION The present study was carried out in the Department of
Pathology of Government Medical College and Hospital
during a period from July 2014 to June 2016
head and neck lesions were studied. They formed
all the lesions. Of these 216 cases were non
cases were benign and 71 cases were malignant
contributing 58.4%, 22.4% and 19.2% respectively.
percentage of non neoplastic lesions [216 cases (58.4%)]
in our study was relatively more than that in study by
Popat VC et al (2010)4
[26 cases (24.3%)] and the
percentage of benign lesions in study by Popat VC
(2010)4 [43 cases (42.7%)]
was relatively more than that
in our study [83 cases (22.4%)]. Age wise distribution of
head and neck lesions in our study was comparable with
study by Popat VC et al (2010)4. In the present study,
females outnumbered males with M: F ratio of 1:1.2.
Males had slight preponderance in a study by Popat VC
al (2010)4
with M: F ratio of 1.01:1, which can be
explained by difference in the sample size. In our study
the most common site of occurrence of head and neck
lesions is Skin and soft tissue [120 cases (3
study by Popat VC et al (2010)4
most common site of
lesion was thyroid [32 cases (31.06%)] which is second
most common site of lesion in our study [91 cases
(24.6%)], this difference can be explained with variation
in sample size and rural setup of our study The
descending order of occurrence of head and neck lesion at
various sites was Skin and soft tissue > Thyroid > Oral
cavity and oropharynx > Lymph nodes > Salivary glands
> Ear > Nose, paranasal sinus and nasopharynx > Eye >
Hypopharynx and larynx. The frequency of occurrence of
thyroid lesions in our study [91 cases (24.6%)] was
comparable with study by Popat VC et al
reported one case of Diffuse large B cell lymphoma
(DLBCL) in salivary (submandibular) gland.
diagnosis of Diffuse large B cell lymphoma confirmed on
, V V Deshmukh, S L Gaikwad, D S Jadhav, A G Valand
Copyright © 2017, Medpulse Publishing Corporation, MedPulse International Journal of Pathology, Volume 4, Issue 1
Photomicrograph showing
necrosis and epitheloid cells.
The present study was carried out in the Department of
Pathology of Government Medical College and Hospital
July 2014 to June 2016.Total 370
They formed 7.8% of
all the lesions. Of these 216 cases were non-neoplastic, 83
cases were benign and 71 cases were malignant
, 22.4% and 19.2% respectively. The
percentage of non neoplastic lesions [216 cases (58.4%)]
elatively more than that in study by
[26 cases (24.3%)] and the
percentage of benign lesions in study by Popat VC et al
was relatively more than that
in our study [83 cases (22.4%)]. Age wise distribution of
head and neck lesions in our study was comparable with
In the present study,
females outnumbered males with M: F ratio of 1:1.2.
had slight preponderance in a study by Popat VC et
with M: F ratio of 1.01:1, which can be
explained by difference in the sample size. In our study
the most common site of occurrence of head and neck
lesions is Skin and soft tissue [120 cases (32.4%)]. In
most common site of
[32 cases (31.06%)] which is second
most common site of lesion in our study [91 cases
(24.6%)], this difference can be explained with variation
of our study The
descending order of occurrence of head and neck lesion at
various sites was Skin and soft tissue > Thyroid > Oral
cavity and oropharynx > Lymph nodes > Salivary glands
> Ear > Nose, paranasal sinus and nasopharynx > Eye >
larynx. The frequency of occurrence of
thyroid lesions in our study [91 cases (24.6%)] was
20104. We also
reported one case of Diffuse large B cell lymphoma
(DLBCL) in salivary (submandibular) gland. The
Diffuse large B cell lymphoma confirmed on
immunohistochemistry with large lymphoid cells
positive for Cd20/Bcl2/MUM1/Bcl6 with focal immunore
activity for c-myc. The large lymphoid cells are
immunonegative for CD3/CD10.The Ki67 proliferative
index was approximately 95%.In a study by
Faur et al(2009)5, the frequency of occurrence of
lymphoma among salivary gland neoplasm is 0.98%( 2
cases out of 204 neoplastic salivary gland lesions) while
in our study it is 8.3% [1 case out of 12
salivary gland lesions]. The difference is due to variation
in sample size and rarity of the lesion.
case of Rosai Dorfman disease in a 35 years female
presented with single, non- tender neck lymph node
enlargement. Riyaz N. et al 2005
unusual case of multifocal Rosai Dorfman Disease in a 25
year male presented with asymptomatic skin lesions and
multiple neck swellings. Bhat GM
S et al 20088
also reported similar cases in their studies.
In present study the commonest complaint was swelling
[296 cases (80%)] followed by ulcerous growth [22 cases
(6%)], ear discharge [12 cases (3.2%)], sore throat and
ulcer [11cases (3%) each], nasal obstruction [8 cases
(2.1%)], white patch and change in
each], earache [2cases(0.5%)], ear discharge and
headache [1 case(0.3%) each].In a study
al (2010)4, 75 cases (72.8%) presented with swelling and
other common presentations included dysphagia,
odynophagia, hoarsness of voice(change in voice). The
findings of study by Popat VC
with our study. According to Chavan SS
of 147 cases of benign nasal masses studied nasal
obstruction and nasal drainage were the most common
symptoms observed [83 cases (56.46%)]. According
Misra V et al (2009)10
, who studied sections from 776
lesions of oral cavity, the lesions commonly presented as
white patches in leukoplakia and oral submucosal
fibrosis, and as a growth in squamous cell pap
squamous cell carcinoma.
CONCLUSION Among all the lesions, head and neck lesions contribute a
noticeable percentage. Among all the head and neck
lesions, non neoplastic lesions were predominant with a
female preponderance. Goiter was the most c
neoplastic lesion and usually middle aged females were
affected more. Most of the patients presented with the
complaint of swelling in head and neck region. Benign
tumors were in excess of malignant tumors. The most
common benign tumours were fol
thyroid and lipoma followed by haemangioma. The most
common malignant tumor was squamous cell carcinoma
at various sites and then followed by papillary carcinoma
of thyroid. Malignant tumours were common in elderly
, Issue 1 October 2017
immunohistochemistry with large lymphoid cells immune
positive for Cd20/Bcl2/MUM1/Bcl6 with focal immunore
The large lymphoid cells are
immunonegative for CD3/CD10.The Ki67 proliferative
was approximately 95%.In a study by Alexandra
the frequency of occurrence of
lymphoma among salivary gland neoplasm is 0.98%( 2
cases out of 204 neoplastic salivary gland lesions) while
[1 case out of 12 neoplastic
salivary gland lesions]. The difference is due to variation
in sample size and rarity of the lesion. We reported a rare
case of Rosai Dorfman disease in a 35 years female
tender neck lymph node
20056
also reported an
unusual case of multifocal Rosai Dorfman Disease in a 25
year male presented with asymptomatic skin lesions and
multiple neck swellings. Bhat GM et al 20047
and Kharrat
also reported similar cases in their studies.
In present study the commonest complaint was swelling
[296 cases (80%)] followed by ulcerous growth [22 cases
(6%)], ear discharge [12 cases (3.2%)], sore throat and
ulcer [11cases (3%) each], nasal obstruction [8 cases
(2.1%)], white patch and change in voice [3cases (0.8%)
each], earache [2cases(0.5%)], ear discharge and
[1 case(0.3%) each].In a study by Popat VC et
75 cases (72.8%) presented with swelling and
other common presentations included dysphagia,
hoarsness of voice(change in voice). The
Popat VC et al were comparable
Chavan SS et al (2012)9, out
of 147 cases of benign nasal masses studied nasal
obstruction and nasal drainage were the most common
ptoms observed [83 cases (56.46%)]. According to
who studied sections from 776
lesions of oral cavity, the lesions commonly presented as
white patches in leukoplakia and oral submucosal
fibrosis, and as a growth in squamous cell papilloma and
Among all the lesions, head and neck lesions contribute a
noticeable percentage. Among all the head and neck
lesions, non neoplastic lesions were predominant with a
female preponderance. Goiter was the most common non
neoplastic lesion and usually middle aged females were
affected more. Most of the patients presented with the
complaint of swelling in head and neck region. Benign
tumors were in excess of malignant tumors. The most
common benign tumours were follicular adenoma of
thyroid and lipoma followed by haemangioma. The most
common malignant tumor was squamous cell carcinoma
at various sites and then followed by papillary carcinoma
Malignant tumours were common in elderly

MedPulse International Journal of Pathology, Print ISSN: 2550-7605, Volume 4, Issue 1, October 2017 pp 01-06
MedPulse International Journal of Pathology, Print ISSN: 2550-7605, Volume 4, Issue 1, October 2017 Page 6
men and benign tumours were common in middle aged
females. The histopathological pattern of various head
and neck lesions ranges from simple nonspecific
inflammatory lesions to highly malignant fatal lesions.
Hematoxylin and Eosin staining remain the best for the
primary histopathological diagnosis.
Immunohistochemistry is very helpful in accurate
categorization of lesion when there is dilemma in
histopathological diagnosis. The results of our study were
comparable with the most of the other similar studies.
The drawback of this study was that the present data
being hospital generated cannot be regarded as
representative of the incidence of head and neck lesions
in the general population.
REFERENCES 1. Cardesa A slootweg P. Pathology of head and Neck. New
York: Springer Verlang Berlin Heidelberg; 2006.
2. Adeyemi BF, Adekunle L V, Kolude BM, Akang EEU,
Lawoyin JO. Head and neck cancer-a clinicopathological
study in a tertiary care center. J Natl Med Assoc.
2008;100(6):690–7.
3. Freund HR. Principles of Head and Neck Surgery. 2nd
ed. New York. Appleton-Century-Crofts; 1979.
4. Popat VC, Vora D, Shah H. Clinico – Pathological
Correlation Of Neck Lesions – A Study Of 103 Cases.
Internet J Head Neck Surg [Internet]. 2010;4(2):1–12.
Available from: https://ispub.com/IJHNS/4/2/4131#
5. Faur A, Lazar E, Cornianu M, Dema A, Lazureanu C,
Muresan A, et al. Primary malignant non-Hodgkin ’ s
lymphomas of salivary glands. Rom J Morphol Embryol.
2009;50(4):693–9.
6. Riyaz N, Khader A, Sarita S. Rosai-Dorfman syndrome.
Indian J Dermatol Venereol Leprol. 2005;71(5):342–4.
7. Bhatt JV, Shah JM, Shah F. Clinico-Pathological Profile
of Cervial Lymphadenopathy.
8. Kharrat S, Sahtout S, Oukhai M, Mekni E, Trabelsi S,
Haouet S,Besbes G. Multifocal Rosai-Dorfman disease: a
case report. Fr ORL. 2008;94: 395-8.
9. Chavan SS, Deshmukh S, Pawar V, Sarvade K, Kirpan
V, Kumbhakarna NR SM. Case Study of
Clinicopathological Correlation of Benign Sinonasal
Masses. World Artic Ear, Nose Throat. 2012;5(1).
10. Misra V, Singh PA, Lal N, Agarwal P, Singh M.
Changing Pattern of Oral Cavity Lesions and Personal
Habits Over a Decade: Hospital Based Record Analysis
from Allahabad. Indian J Community Med. 2009 Oct
9;34(4):321–5.
Source of Support: None Declared
Conflict of Interest: None Declared