Embed Size (px)
Citation preview
Available online at www.sciencedirect.com
Annals of Diagnostic Pathology 16 (2012) 323–329
Clinicopathologic correlation of vitamin D receptor expression withretinoid X receptor and MIB-1 expression in primary and
metastatic osteosarcomaRyan Gallagher, BSa, John Keighley, PhDb, Jakica Tancabelic, MDc,⁎, 1,
Rama Garimella, PhDa,d, David Pinson, DVM, PhDa,Kimberly Templeton, MDe, Ossama Tawfik, MD, PhDa,⁎
aDepartment of Pathology and Laboratory Medicine, Kansas University Medical Center, Kansas City, KSbDepartment of Biostatistics, Kansas University Medical Center, Kansas City, KScDepartment of Pediatrics, Kansas University Medical Center, Kansas City, KS
dDepartment of Dietetics and Nutrition, Kansas University Medical Center, Kansas City, KSeDepartment of Orthopedic Surgery, Kansas University Medical Center, Kansas City, KS
Abstract Vitamin D, in addition to its effects on bone, is important in cell cycle regulation. Vitamin D receptor
⁎ CorrespondingMedicine, The Unive66160. Tel.: +1 913 5
E-mail address: o1 Current affiliatio
ogist, Stormont Vail H8th Ave, Topeka, KS.
1092-9134/$ – see frodoi:10.1016/j.anndiag
(VDR) has been identified in breast, prostate, and colon cancers, as well as in canine and humanosteosarcoma (OS) cell lines; however, it has not been well investigated in human OS-archivedspecimens. We correlated VDR, retinoid X receptor (RXR), and MIB-1 (Ki-67) expression in 110archived OS cases with several clinicopathologic parameters including patient's age, sex, tumorlocation, tumor grade, and type and metastatic status. The expression of VDR and RXR wasidentified in human OS tissue obtained from primary and metastatic OS archival tissue. Nostatistically significant difference was found in VDR expression in relation with tumor grade, type,age, sex, or location. The expression of RXR was highest in higher-grade (P = .0006) and metastatictumors but remained unchanged when correlated with tumor type, age, sex, or location. Theexpression of MIB-1 was statistically elevated in higher-grade tumors (P = .001), patients 25 years oryounger (P = .04), tumors located in extremities (P = .005), and metastatic lesions, but was notimpacted by tumor type or patient's sex. Proliferative activity was significantly reduced aftertreatment, as the mean MIB-1 expression dropped from 11% in primary biopsy samples to 6% inresection specimens. There appears to be a relationship between proliferative tumor activity andtumor grade, location, and metastasis. Additional studies on the analysis of the effects of vitamin Dand RXR on OS proliferation, apoptosis, and differentiation are critical to further evaluate theirpotential role in OS treatment.
© 2012 Elsevier Inc. All rights reserved.Keywords: Osteosarcoma; Vitamin D receptor; Retinoid X receptor; MIB-1 (Ki-67)
author. Department of Pathology and Laboratoryrsity of Kansas Medical Center, Kansas City, KS88 1185; fax: +1 913 588 [email protected] (O. Tawfik).n for Dr Tancabelic: Pediatric Hematologist/Oncol-ealth Care, Cotton O'Neil Cancer Center, 1414 SW
nt matter © 2012 Elsevier Inc. All rights reserved.path.2012.01.001
1. Introduction
Osteosarcoma (OS) is a highly malignant, aggressivetumor of the bone, with a peak incidence in the second andthird decades of life; it accounts for approximately 45% ofall bone sarcomas [1]. The etiology of OS is, for the mostpart, unknown, except for tumors occurring in the fifth andsixth decades of life, which frequently occur secondary toradiation therapy or arising in a background of a preexistingbenign condition such as Paget disease. Up to 10% of

324 R. Gallagher et al. / Annals of Diagnostic Pathology 16 (2012) 323–329
patients have documented metastasis at presentation.Pathologic diagnosis is established with either a core-needleor open biopsy. The 5-year survival rate of 70% hasremained essentially the same since the introduction ofhigh-dose chemotherapy, with 30% of patients stilldeveloping metastasis after treatment and ultimately suc-cumbing to their disease [2]. Evaluation of prognosis ofpatients with OS is limited to clinical parameters, whereasmolecular markers of tumor aggressiveness have yet to bedefinitively identified.
The initial diagnostic biopsy is usually followed byneoadjuvant chemotherapy. Surgery is then performed,either amputation of the affected limb or limb salvagetherapy, depending on the site and size of the tumor. Thechemotherapy regimen typically consists of 4 agents(methotrexate, ifosfamide, doxorubicin, and cisplatin).Each of the 4 agents can cause significant posttreatmenttoxicities including cardiotoxicity (doxorubicin), ototoxicityand nephrotoxicity (cisplatin and ifosfamide), and hepato-toxicity (methotrexate).
A variety of compounds induce differentiation, loss ofproliferative capacity, and loss of oncogenicity in tumors.These differentiation-inducing agents can bring cancer cellsto a point of maturity where the cells lose the ability to divideand go through programed cell death (apoptosis). This differsfrom the use of cytotoxic drugs, which prevent cell division.Vitamin D (vit D) and retinoids have been shown to inducedifferentiation of a large number of human and caninemalignancies [3,4].
Vitamin D is a steroid hormone synthesized in the skinfrom 7-dehydrocholesterol in the presence of UV-B light. Itis also obtained from dietary sources such as fortified dairyproducts. Once synthesized or absorbed, it is metabolized bythe liver and, subsequently, by the kidney into its mostbiologically active form, 1,25-dihydroxyvitamin D (calci-triol). Calcitriol, in turn, plays an important role in thedevelopment and maintenance of healthy bones. Actions of1,25-dihydroxyvitamin D3 (1,25(OH)2D3) are mediated bythe vit D receptor (VDR), a nuclear phosphoprotein thatbinds 1,25(OH)2D3 with high affinity. This alters the ligandbinding domain of the VDR and results in a strongheterodimerization with retinoid X receptors (RXRs).Retinoid X receptor is a nuclear protein that binds variousretinoids, a family of polyisoprenoid lipids that includesvitamin A. It is an intrinsic component of the VDR complexthat is required in the transcription of vit D–responsive geneproducts [5]. The resulting 1,25(OH)2D3–VDR-RXR com-plex promotes vit D–responsive element binding andtranscription of vit D–promoted gene products [6].
Vitamin D and its analogs have been recently describedas having a significant antitumor activity in vivo and in vitroin murine squamous cell carcinoma, human xenograftprostatic adenocarcinoma, metastatic prostatic adenocarci-noma, human pancreatic, lung and breast cancer, andmultiple myeloma [7-10]. Vitamin D compounds enhancedthe effect of chemotherapy agents including platinum
analogs, taxanes, antimetabolites, alkylating agents, andtopoisomerase inhibitors [9]. Several in vivo and in vitrostudies suggest that vit D antiproliferative effects areassociated with G0/G1 arrest, induction of apoptosis,differentiation, modulation of growth factor–mediatedsignaling in tumor cells, and tumor vasculature. In a phaseIII trial, administration of calcitriol (a vit D analog),dexamethasone, and carboplatin to patients with hormonerefractory prostate cancer induced a significant improvementin prostate-specific antigen response. In addition, dailyadministration of 400 IU of vit D3 and calcium 1500 mg topatients with colon polyps induced a significant reduction inproliferation measured by Ki-67 [11].
At this point, the antiproliferative role of vit D therapy inhuman OS is, for the most part, speculative. Moreover, themechanism of action in these tumors remains controversial.Recent research has demonstrated the presence of VDR in avariety of cancers including breast cancer, prostate cancer,lung cancer, melanoma, and colorectal cancer [12-15].Similar studies have not been done to demonstrate thepresence of VDR in human OS in vivo.
The purpose of this study is to immunohistochemicallyevaluate the expression of VDRs in human OS, as apreliminary study of the potential use of vit D as an adjunctin the treatment of OS. In addition, we attempted to correlateVDR expression with RXR, underlyingmechanisms involvedin tumor proliferation using MIB-1 as a marker, comparingthese with several clinicopathologic parameters includinghistologic grade, tumor type, and location in primary andmetastatic lesions, along with patient's age and sex.
2. Materials and methods
2.1. Patient cohort
Data on a consecutive cohort of patients treated for OSbetween 1988 and 2007 were collected, including patient'sage at diagnosis, sex, presence of metastatic disease atdiagnosis, and the primary tumor site. One hundred tensamples were used from a total of 65 patients with OS. Thisretrospective study was approved by the institutionalresearch committee at the University of Kansas MedicalCenter. These samples included primary biopsies (48),resection specimens after therapy (35), and metastatic lesions(27). The mean age of our patient population was 27 years(range, 6-83 years). Forty-one patients were 25 years oryounger. Thirty-one patients were female, and 34 were male.
Primary tumor locations were femur (36), tibia (13),maxilla (7), scapula/shoulder (6), humerus (4), oropharynx(2), ilium (2), fibula (2), spine (2), and site unknown (9). Alltumors were either grade II (40) or grade III (70). Fifty-eighttumors were of the conventional type; 26, chondroblastic;12, giant cell variant; 9, fibroblastic; 3, telangiectatic; and 2,epithelioid type.
There were 27 samples of metastatic disease collectedfrom 20 patients. All had high-grade OS with lung metastasis
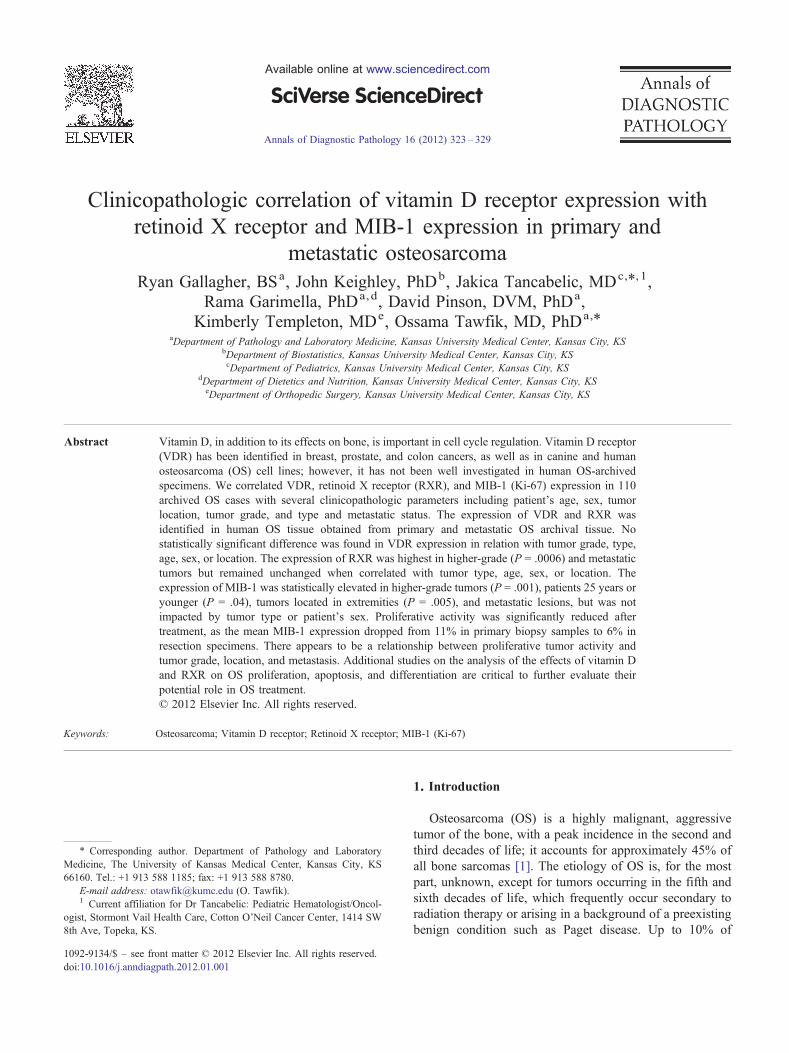
ig. 1. Representative examples of VDR expression in human OSmmunostain,magnification ×200). (A) Low expression. (B)High expression.
325R. Gallagher et al. / Annals of Diagnostic Pathology 16 (2012) 323–329
in most patients (17/20 patients). Other metastatic sitesincluded soft tissue, urinary bladder, skin, and small bowel.
2.2. Immunohistochemical data
Tissue blocks with the most representative and well-preserved areas of tumors were selected for immunohis-tochemistry (IHC) studies for VDR, RXR, and MIB-1,using Dako autostainer (Dako, Carpinteria, Calif). Thetissue blocks were cut to 5-μm sections, deparaffinized,and heat treated for antigen retrieval; hematoxylin wasused as a counter stain. Appropriate positive and negativecontrols for each marker were included. Positive controlsfor the markers were selected from surgical specimenssuch as breast carcinoma, prostate carcinoma, andmelanocytic tumor cases normally received in the surgicalpathology laboratory. The individual antibodies, vendor,titration titer, time of titration, epitope retrieval method,and method of detection that had been used are shownin Table 1.
Positive IHC reactions are defined as a positivecytoplasmic staining for VDR (Fig. 1) and a positivenuclear staining for RXR (Fig. 2) and MIB-1 (Fig. 3). Themethod of Grizzle et al [16] was used to determine theimmunostain score for VDR. Cytoplasmic staining intensitywas scored from 0 to 3. The percentage of positive cells ateach intensity level was multiplied by the appropriateintensity score; these values were summed and then dividedby the total number of cells to obtain a weighted averagescore between 0 and 3. This method has been proven to bemore representative than the usual 0 to 3+ staining intensitybecause it takes into consideration both antigen presenceand changes in antigen expression for the lesion. It alsotakes into account all relevant areas on the slides. Forproliferation index of MIB-1 and percent positivity forRXR, the percentage of nuclei with immunopositivity wasdetermined using the proliferation index program of theChromaVision Automated Cellular Imaging System (SanJuan Capistrano, Calif).
2.3. Statistical analysis
Means and SDs for the VDR, RXR, and MIB-1 arepresented. In addition, the medians are presented becausethe data for all 3 outcomes showed evidence of nonnormaldistributions. Accordingly, nonparametric statistics and
Table 1Individual antibodies, vendor, titer, time of titration, epitope retrieval method, and
Antibody Manufacturer Titer/Incubat
VDR Santa Cruz Biotechnology,Inc, Santa Cruz, Calif
1:500/30 min
RXR retinoid receptor Lab Vision Neomarkers,Fremont, Calif
1:300/60 min
Ki-67 (MIB-1) Dako 1:200/30 min
F(i
tests were used in the analysis. Spearman correlationcoefficients were calculated as a measure of associationbetween the different markers. Correlations were calculatedfor various classification variables such as grade, sex, andspecimen type. Wilcoxon rank sum and Kruskal-Wallistests were used to test for differences in median levelswithin a marker for the different levels of the classificationvariables. If evidence of a difference was found using theKruskal-Wallis tests, then the Wilcoxon rank sum testswere used in a pair-wise method to determine which
method of detection
ion Pretreatment Detection
None Envision + antirabbit; Dako
Citrate pH 6.0, BiocareDecloaking Chamber 5″
Envision + antimouse; Dako
Citrate pH 6.0, BiocareDecloaking Chamber 5″
Envision + antimouse; Dako
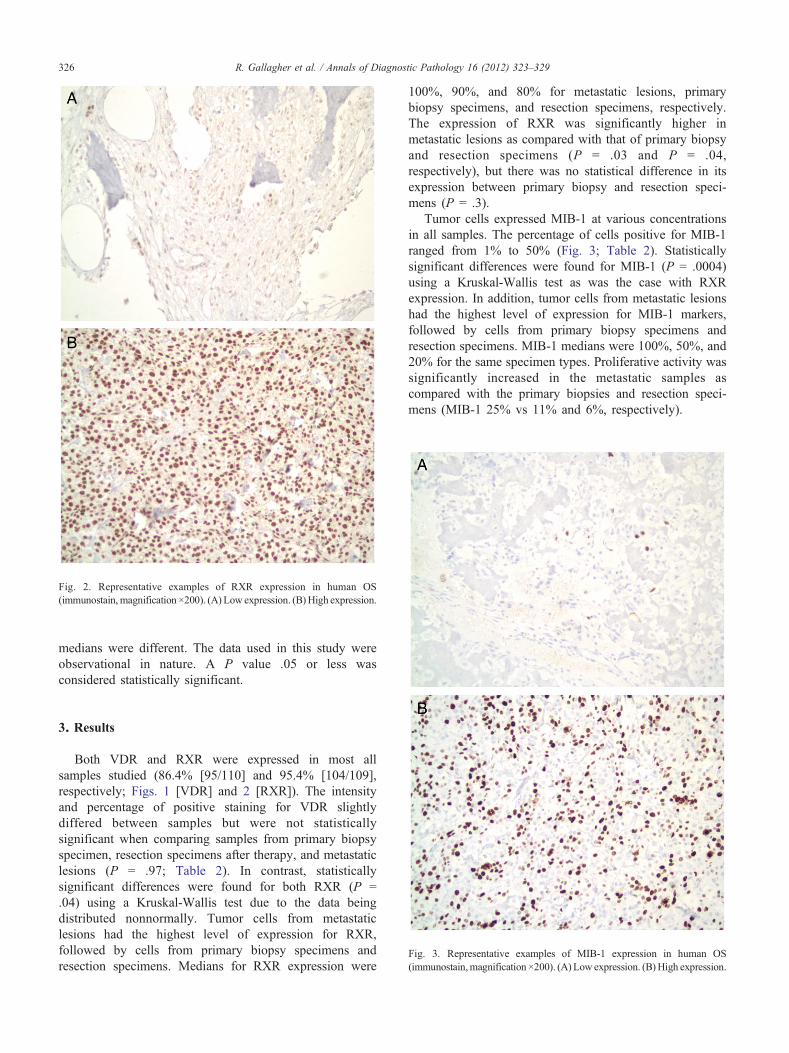
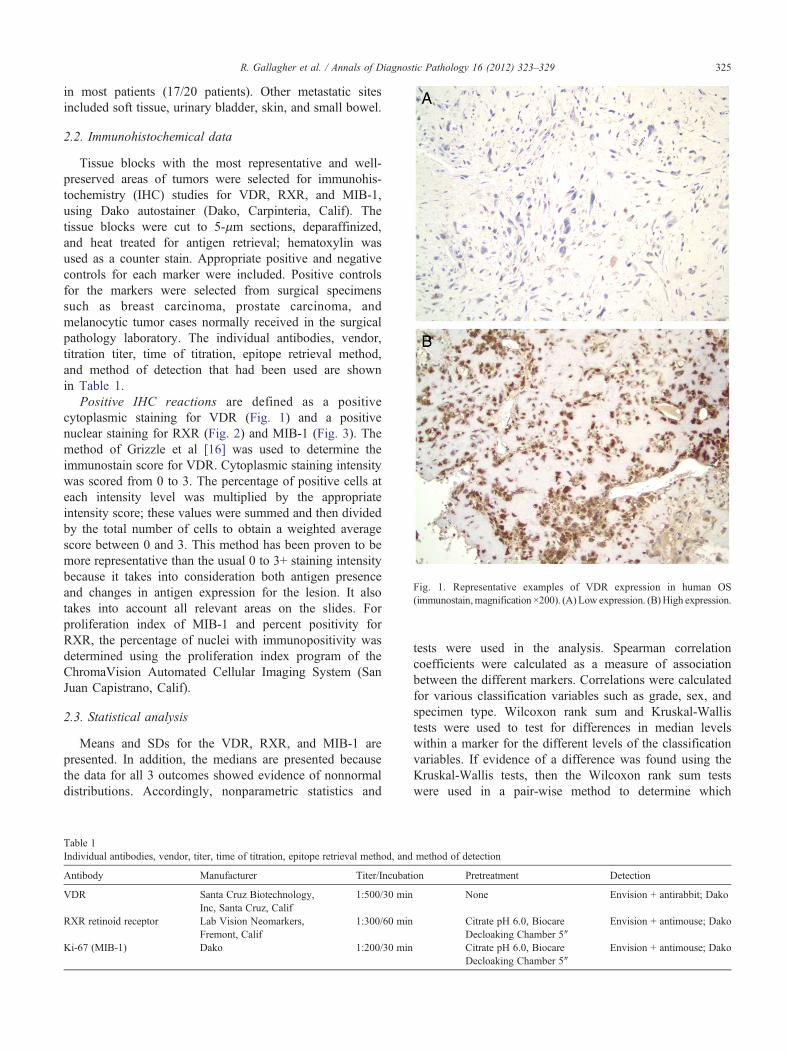
Fig. 2. Representative examples of RXR expression in human OS(immunostain, magnification ×200). (A) Low expression. (B)High expression.
326 R. Gallagher et al. / Annals of Diagnostic Pathology 16 (2012) 323–329
medians were different. The data used in this study wereobservational in nature. A P value .05 or less wasconsidered statistically significant.
Fig. 3. Representative examples of MIB-1 expression in human OS(immunostain,magnification ×200). (A) Low expression. (B)High expression.
3. Results
Both VDR and RXR were expressed in most allsamples studied (86.4% [95/110] and 95.4% [104/109],respectively; Figs. 1 [VDR] and 2 [RXR]). The intensityand percentage of positive staining for VDR slightlydiffered between samples but were not statisticallysignificant when comparing samples from primary biopsyspecimen, resection specimens after therapy, and metastaticlesions (P = .97; Table 2). In contrast, statisticallysignificant differences were found for both RXR (P =.04) using a Kruskal-Wallis test due to the data beingdistributed nonnormally. Tumor cells from metastaticlesions had the highest level of expression for RXR,followed by cells from primary biopsy specimens andresection specimens. Medians for RXR expression were
100%, 90%, and 80% for metastatic lesions, primarybiopsy specimens, and resection specimens, respectively.The expression of RXR was significantly higher inmetastatic lesions as compared with that of primary biopsyand resection specimens (P = .03 and P = .04,respectively), but there was no statistical difference in itsexpression between primary biopsy and resection speci-mens (P = .3).
Tumor cells expressed MIB-1 at various concentrationsin all samples. The percentage of cells positive for MIB-1ranged from 1% to 50% (Fig. 3; Table 2). Statisticallysignificant differences were found for MIB-1 (P = .0004)using a Kruskal-Wallis test as was the case with RXRexpression. In addition, tumor cells from metastatic lesionshad the highest level of expression for MIB-1 markers,followed by cells from primary biopsy specimens andresection specimens. MIB-1 medians were 100%, 50%, and20% for the same specimen types. Proliferative activity wassignificantly increased in the metastatic samples ascompared with the primary biopsies and resection speci-mens (MIB-1 25% vs 11% and 6%, respectively).

Table 2Expression of VDR, RXR, and MIB-1 in OS specimens
Specimen type VDR RXR MIB-1
Proportionexpressinga
Meanintensityb
Proportionexpressinga
Meanpositivity
Proportionexpressinga
Meanpositivity
Primary biopsy 83.3% (40/48) 1.41 97.9% (47/48) 81% 96.3% (47/48) 11%Posttherapy resection 91.4% (32/35) 1.49 88.2% (30/34) 67% 70.6% (24/34) 6%Metastasis 85.2% (23/27) 1.44 100% (27/27) 87% 100% (27/27) 25%Total 86.4% (95/110) 1.44 95.4% (104/109) 78.2% 88.9% (97/109) 12.8%
a Percentage of tumors expressing the marker within each group and number of positive samples compared with the total number of samples studied pergroup in parentheses.
b Mean staining intensity of VDR in each group.
327R. Gallagher et al. / Annals of Diagnostic Pathology 16 (2012) 323–329
3.1. VDR, RXR, and MIB-1 expression in relation with thedifferent histopathologic and clinical parameters
All tumors were graded as intermediate (grade 2) or high-grade (grade 3) lesions based on cellularity, cytologic atypia,and mitotic figures following the World Health Organizationclassification of malignant bone tumors. No statisticallysignificant difference in VDR expression was found betweenhistologic tumor grades (P = .76; n = 110). In contrast, grade3 tumors had statistically significant higher levels ofexpression for RXR and MIB-1 (P = .0006 and P = .0001,respectively). None of the markers studied showed anysignificant correlation with the different tumor types.
In correlating the expression of the different markers withpatient's age, sex, and tumor location, we elected to use dataobtained from the primary biopsy specimens only. This wasdone to avoid any bias in reporting the same patients morethan once in the results. Our results show that patients 25years or younger had a higher mean rank MIB-1 score (P =.04) as compared with older patients. Neither VDR nor RXRexpression was statistically different between the 2 agegroups (P = .97 and P = .24, respectively). With regards tosex, there were no significant differences between males andfemales for the 3 markers studied. However, there was aslightly higher RXR expression in female patients ascompared with male patients (P = .06). No statisticallysignificant difference in VDR or RXR expression was foundwhen their expression was correlated between tumors arisingin the extremities vs other locations (P = .57 and P = .68,respectively). In contrast, tumors arising in the extremitieswere more proliferative and expressed higher MIB-1 levels(P = .005).
The expression of VDR had a negative correlation of−0.15 with MIB-1, which was not statistically significant(P = .43). There was no correlation between VDR expressionand RXR expression (P = .14). Furthermore, RXR had apositive correlation with MIB-1 expression (P b .0001).Patients with OS located in the femur had an increasedexpression of MIB-1 (P = .05) when compared with patientswith the primary tumor in other bones.
We also evaluated the percentage of tumor necrosis inresected specimens as a valuable parameter for response toneoadjuvant chemotherapy and correlated it with MIB-1 and
RXR expression. Most of the resected specimens showedmore than 50% tumor necrosis (22.35 specimens). Six resectedtumors had more than 10% necrosis. The remaining 7specimens had between 11% and 49% tumor necrosis. Therewere no correlations between response to therapy, asmeasuredby tumor necrosis, and either the MIB-1 or RXR values.
4. Discussion
Differentiation therapy as a method of controllingneoplastic growth is a concept that has recently generatedmuch interest among investigators. Vitamin D, in particular,has been the subject of intensive research, both in itsmethods of action and its effects on various humanneoplasms [5,17-22]. Multiple studies have demonstratedthat vit D can affect the rate of proliferation, degree ofapoptosis, and the phenotype of numerous neoplastic celllines. These studies report variable effects and degrees ofresponse between different tumor types and within cell linesof the same tumor type [7,18,19,23].
In a study by Valrance et al [10] regarding human breastcancer, it was found that proapoptotic and antiproliferativeeffects were induced in some but not all cell lines treatedwith vit D. Valrance et al [10] noted that the nonresponsivecell lines were those that lacked the expression of VDR.Although the manner in which vit D is able to induceapoptosis and reduce proliferation in neoplastic cell lines isyet unknown, the efficacy of vit D therapy is dependent onthe expression of the VDR within the target population ofcells [10,17,18].
Previous studies by Barroga et al [7,23] reported thestimulation of a canine OS cell line with vit D analogs andretinoids to differentiate into a more mature phenotype thatshowed evidence of increased apoptosis and decreasedproliferation of cells. Although these studies support theefficacy of vit D as a therapeutic agent for canine OS, allresearch was conducted on cell lines derived from a singlespontaneous canine OS. Because the success of vit D therapydepends on the expression of the VDR, it is necessary todetermine if VDR expression is high enough in a significantportion of spontaneous OSs to warrant further research intovit D as a potential therapeutic agent.

328 R. Gallagher et al. / Annals of Diagnostic Pathology 16 (2012) 323–329
In this study, we have demonstrated that VDR expressioncan be confirmed in paraffin-embedded archival OS tissueusing IHC. Although the presence of VDR in malignant cellshas been shown previously in cell culture [24], our studyused archival tissue obtained at the time of diagnosis. Inaddition, we looked for possible correlations between VDRand clinical indices as well as between VDR, MIB-1, amarker of proliferation, and RXR. The results of our studyshowed VDR and RXR are ubiquitously expressed in mostof the OSs studied with no relationship with age or sex of thepatients. In contrast, MIB-1 expression was variable. Patients25 years or younger had more aggressive, more mitoticallyactive tumors as compared with older patients. Althoughseveral studies have suggested that factors such as age, sex,tumor site, and/or size are of possible prognostic signifi-cance, critical evaluation of the literature demonstrated thatonly tumor necrosis after chemotherapy has predictivevalues [25-27]. Significant differences in MIB-1 expressionwere noted among primary tumors, treated tumors, andmetastatic lesions: treatment resulted in reduction of tumorproliferative activity, while tumor progression such asmetastasis was associated with increased proliferativeactivity. Our results were in agreement with a previouslyreported study that suggested a possible prognostic signif-icance for MIB-1 in the development of pulmonarymetastases in OS [28]. In addition, proliferative activitywas noted to be associated with tumor grade andaggressiveness. These findings could be of clinical signif-icance to help monitor disease progression and response totreatment as is the case with other tumors such as breast afterchemotherapy and radiation.
We found that primary tumors located in the extremities(primarily femur) had significantly higher MIB-1 activitycompared with tumors originating in other sites. Similarfindings were noted by other investigators where they foundthat tumors from long bones from the extremities had higherproliferative activities when they were compared with thosefrom jaw OS using different proliferative markers such as Ki-67 and AgNOR [28-30].
The presence of VDR on OS cells may indicate thatthese cells recognize and can potentially respond to vit D.In light of the role of vit D in cell cycle regulation andapoptosis, this finding warrants additional investigationbecause vit D may prove to be an additional therapeuticmodality for the treatment of OS. This would be particularlyattractive, considering the low risk of adverse effects fromthe use of vit D.
The limitations of this study include a small sample sizefor some of the tumor types and the lack of patient serum vitD levels (25-hydroxy or 1,25-dihydroxyvitamin D) at thetime of diagnosis. These levels can impact the expression ofVDR in normal tissue. However, we do not know if OStissue similarly reflects systemic vit D levels or actsindependently of these levels.
In conclusion, we demonstrated the presence of VDRin most archival paraffin-embedded human OS samples.
Our ongoing studies at this time are focused on in vitroanalysis of the effects of vit D on OS cell-line proliferation,apoptosis, and differentiation. Results of this continuedwork, as well as recent research showing synergism intreating canines with OS with vit D and chemotherapy [31],may indicate another venue in potentially improving theoverall survival in patients with OS. Tailoring treatment to atumor's histopathologic and molecular characteristics mayresult in improved responsiveness to therapy and overallsurvival while decreasing treatment adverse effects.
References
[1] Mirabello L, Troisi RJ, Savage SA. Osteosarcoma incidence andsurvival rates from 1973 to 2004: data from the Surveillance,Epidemiology, and End Results Program. Cancer 2009;115:1531-43.
[2] Bacci G, Picci P, Ferrari S, et al. Primary chemotherapy anddelayed surgery for nonmetastatic osteosarcoma of the extremities.Results in 164 patients preoperatively treated with high doses ofmethotrexate followed by cisplatin and doxorubicin. Cancer 1993;72:3227-38.
[3] St-Arnaud R. The direct role of vitamin D on bone homeostasis. ArchBiochem Biophys 2008;473:225-30.
[4] Thorne J, Campbell MJ. The vitamin D receptor in cancer. Proc NutrSoc 2008;67:115-27.
[5] Wang K, Chen S, XieW, et al. Retinoids induce cytochrome P450 3A4through RXR/VDR-mediated pathway. Biochem Pharmacol 2008;75:2204-13.
[6] Haussler MR, Haussler CA, Jurutka PW, et al. The vitamin D hormoneand its nuclear receptor:molecular actions and disease states. J Endocrinol1997;154(Suppl):S57-73.
[7] Barroga EF, Kadosawa T, Asano K, et al. Apoptosis induction of POScanine osteosarcoma cells by vitamin D and retinoids. J Vet Med Sci1998;60:1269-72.
[8] Barroga EF, Kadosawa T, Okumura M, Fujinaga T. Inhibitory effectsof 22-oxa-calcitriol and all-trans retinoic acid on the growth of a canineosteosarcoma derived cell-line in vivo and its pulmonary metastasis invivo. Res Vet Sci 2000;68:79-87.
[9] Trump DL, Muindi J, Fakih M, et al. Vitamin D compounds: clinicaldevelopment as cancer therapy and prevention agents. Anticancer Res2006;26(4A):2551-6.
[10] Valrance ME, Brunet AH, Welsh J. Vitamin D receptor–dependentinhibition of mammary tumor growth by EB1089 and ultravioletradiation in vivo. Endocrinology 2007;148:4887-94.
[11] Schwartz GG, Skinner HG. Vitamin D status and cancer: new insights.Curr Opin Clin Nutr Metab Care 2007;10:6-11.
[12] Barroso E, Fernandez LP, Milne RL, et al. Genetic analysis of thevitamin D receptor gene in two epithelial cancers: melanoma and breastcancer case-control studies. BMC Cancer 2008;8:385.
[13] Menezes RJ, Cheney RT, Husain A, et al. Vitamin D receptorexpression in normal, premalignant, and malignant human lung tissue.Cancer Epidemiol Biomarkers Prev 2008;17:1104-10.
[14] Raimondi S, Johansson H, Maisonneuve P, et al. Review and meta-analysis on vitamin D receptor polymorphisms and cancer risk.Carcinogenesis 2009;30:1170-80.
[15] Thomas MG, Sylvester PA, Newcomb P, et al. Vitamin D receptorexpression in colorectal cancer. J Clin Pathol 1999;52:181-3.
[16] Grizzle WE, Myers RB, Arnold MM, et al. Evaluation of biomarkers inbreast and prostate cancer. J Cell Biochem Suppl 1994;19:259-66.
[17] Coffman FD, Studzinski GP. Differentiation-related mechanismswhich suppress DNA replication. Exp Cell Res 1999;248:58-73.
[18] Fleet JC. Molecular actions of vitamin D contributing to cancerprevention. Mol Aspects Med 2008;29:388-96.

329R. Gallagher et al. / Annals of Diagnostic Pathology 16 (2012) 323–329
[19] Gocek E, Studzinski GP. Vitamin D and differentiation in cancer. CritRev Clin Lab Sci 2009;46:190-209.
[20] Kommagani R, Whitlatch A, Leonard MK, et al. p73 is essential forvitamin D–mediated osteoblastic differentiation. Cell Death Differ2010;17:398-407.
[21] Ng K, Wolpin BM, Meyerhardt JA, et al. Prospective study ofpredictors of vitamin D status and survival in patients with colorectalcancer. Br J Cancer 2009;101:916-23.
[22] Zugel U, Steinmeyer A, May E, et al. Immunomodulation by a novel,dissociated vitamin D analogue. Exp Dermatol 2009;18:619-27.
[23] Barroga EF, Kadosawa T, Okumura M, et al. Influence of vitamin Dand retinoids on the induction of functional differentiation in vitro ofcanine osteosarcoma clonal cells. Vet J 2000;159:186-93.
[24] Colston K, Colston MJ, Feldman D. 1,25-Dihydroxyvitamin D3 andmalignant melanoma: the presence of receptors and inhibition of cellgrowth in culture. Endocrinology 1981;108:1083-6.
[25] Glasser DB, Lane JM, Huvos AG, et al. Survival, prognosis andtherapeutic response in osteogenic sarcoma. Cancer 1992;270:8-14.
[26] Petrilli A, Gentil F, Epelman S, et al. Increased survival, limbpreservation and prognostic factors for osteosarcoma. Cancer 1991;68:733-7.
[27] Davis AM, Bell RS, Goodwin PJ. Prognostic factors in “classical”osteosarcoma: a critical appraisal. J Clin Oncol 1994;12:423-31.
[28] Hernandez-Rodriguez NA, Correa E, Sotelo R, et al. Ki-67: aproliferative marker that may predict pulmonary metastases andmortality of primary osteosarcoma. Cancer Detect Prev 2001;25:210-5.
[29] Jawad SN, Abdullah BH. Proliferative, apoptotic and angiogenicpotentials in jaws and long bone osteosarcomas: a comparativeimmunohistochemical study. J Oral Pathol Med 2010;39:681-6.
[30] Paparella MS, Brandizzi D, Araujo ES, et al. Evaluation of nucleolarorganizer regions in maxillary osteosarcoma. Acta Odontol Latinoam2007;20:55-60.
[31] Rassnick KM, Muindi JR, Johnson CS, et al. In vitro and in vivoevaluation of combined calcitriol and cisplatin in dogs withspontaneously occurring tumors. Cancer Chemother Pharmacol 2008;62:881-91.





























