Embed Size (px)
Citation preview

International Journal of
Radiation Oncologybiology physics
www.redjournal.org
Clinical Investigation: Genitourinary Cancer
ClinicalePathologic Stage Discrepancy in Bladder CancerPatients Treated With Radical Cystectomy: Results Fromthe National Cancer Data BasePhillip J. Gray, MD,*,y Chun Chieh Lin, PhD, MBA,z Ahmedin Jemal, DVM, PhD,z
William U. Shipley, MD,* Stacey A. Fedewa, MPH,z Adam S. Kibel, MD,x
Jonathan E. Rosenberg, MD,k Ashish M. Kamat, MD,{ Katherine S. Virgo, PhD, MBA,#
Michael L. Blute, MD,** Anthony L. Zietman, MD,* and Jason A. Efstathiou, MD, DPhil*
*Department of Radiation Oncology, Massachusetts General Hospital, Boston, Massachusetts; yHarvard RadiationOncology Program, Boston, Massachusetts; zSurveillance and Health Services Research Program, American Cancer Society,Atlanta, Georgia; xDivision of Urology, Brigham and Women’s Hospital/Dana-Farber Cancer Institute, Boston,Massachusetts; kGenitourinary Oncology Service, Department of Medicine, Memorial Sloan-Kettering Cancer Center, NewYork, New York; {Division of Surgery, Department of Urology, University of Texas MD Anderson Cancer Center, Houston,Texas; #Department of Health Policy and Management, Emory University, Atlanta, Georgia; and **Department ofUrology, Massachusetts General Hospital, Boston, Massachusetts
Received Oct 24, 2013, and in revised form Dec 26, 2013. Accepted for publication Jan 4, 2014.
Summary
Accurate clinical staging inpatients with bladder canceris vital for preoperative riskstratification but is evenmore important when select-ing patients for nonoperativetherapies such as chemo-radiotherapy. In an analysisof 16,953 patients undergo-ing radical cystectomy, aclinicalepathologic stagediscrepancy rate of 47.8%was identified. Female sex,advanced age, and moreextensive lymphadenectomywere associated with higher
Reprint requests to: Jason A. Efstathiou, M
General Hospital, Department of Radiation O
Cox 3, Boston, MA 02114. Tel: (617) 726-5
partners.org
Int J Radiation Oncol Biol Phys, Vol. 88, No. 5
0360-3016/$ - see front matter � 2014 Elsevie
http://dx.doi.org/10.1016/j.ijrobp.2014.01.001
Purpose: To examine the accuracy of clinical staging and its effects on outcome in bladder can-cer (BC) patients treated with radical cystectomy (RC), using a large national database.Methods and Materials: A total of 16,953 patients with BC without distant metastases treatedwith RC from 1998 to 2009 were analyzed. Factors associated with clinicalepathologic stagediscrepancy were assessed by multivariate generalized estimating equation models. Survivalanalysis was conducted for patients treated between 1998 and 2004 (nZ7270) using theKaplan-Meier method and Cox proportional hazards models.Results: At RC 41.9% of patients were upstaged, whereas 5.9% were downstaged. Upstagingwas more common in females, the elderly, and in patients who underwent a more extensive lym-phadenectomy. Downstaging was less common in patients treated at community centers, in theelderly, and in Hispanics. Receipt of preoperative chemotherapy was highly associated withdownstaging. Five-year overall survival rates for patients with clinical stages 0, I, II, III, andIV were 67.2%, 62.9%, 50.4%, 36.9%, and 27.2%, respectively, whereas those for the samepathologic stages were 70.8%, 75.8%, 63.7%, 41.5%, and 24.7%, respectively. On multivariateanalysis, upstaging was associated with increased 5-year mortality (hazard ratio [HR] 1.80,P<.001), but downstaging was not associated with survival (HR 0.88, PZ.160). In contrast,more extensive lymphadenectomy was associated with decreased 5-year mortality (HR 0.76for �10 lymph nodes examined, P<.001), as was treatment at an National Cancer Instituteede-signated cancer center (HR 0.90, PZ.042).
D, DPhil, Massachusetts
ncology, 100 Blossom St,
866; E-mail: jefstathiou@
Conflicts of interest: A.M.K. serves as a consultant for Sanofi.
Supplementary material for this article can be found at
www.redjournal.org.
, pp. 1048e1056, 2014
r Inc. All rights reserved.

Volume 88 � Number 5 � 2014 Clinical staging in bladder cancer 1049
rates of upstaging. Patho-
logic upstaging was associ-ated with 80% excessmortality.Conclusions: Clinicalepathologic stage discrepancy in BC patients is remarkably commonacross the United States. These findings should be considered when selecting patients for pre-operative or nonoperative management strategies and when comparing the outcomes of bladdersparing approaches to RC. � 2014 Elsevier Inc.
Introduction
Cancer of the urinary bladder is a common cancer, with 72,570new cases estimated in the United States in 2013 (1). Althoughmost cases of non-muscle-invasive bladder cancer are managedeffectively with transurethral resection and intravesical therapy, upto 40% of patients develop treatment-refractory disease (2). Forthese patients and all patients with muscle invasion at diagnosis,radiation therapy (RC) is the most common treatment received (3).Despite this, nonoperative strategies, especially chemoradiationtherapy , are widely practiced, with long-term outcomes compa-rable to those with cystectomy in many series (4-6).
Accurate clinical staging is vital for preoperative risk stratifi-cation and proper selection for neoadjuvant chemotherapy. Ac-curate clinical stage is even more vital to appropriately selectpatients for nonoperative management strategies such as chemo-radiation therapy. By definition, such therapies do not have thebenefit of determining final pathologic stage. As such, the successof such therapies and the design of clinical trials to test novelnonoperative treatments are wholly dependent on the accuracy ofthe assigned clinical stage. Several previous reports have sug-gested high rates of clinicalepathologic stage discrepancy inbladder cancer patients (7-14). These series, however, typicallycontain limited numbers of patients treated at a single large aca-demic center where therapy and outcomes can vary significantlycompared with nationwide practices (3, 15, 16). Additionally,most prospective cystectomy series fail to report survival by initialclinical stage. We sought to investigate the accuracy of clinicalstaging and its effect on outcome in bladder cancer patients treatedwith RC using the National Cancer Data Base (NCDB).
Methods and Materials
Data source
The NCDB, jointly sponsored by the American College of Sur-geons and the American Cancer Society, is a hospital-based reg-istry that serves as a comprehensive clinical surveillance resourcethat derives its data from the 1500 Commission on Cancereaccredited programs in the United States and Puerto Rico. Assuch, the NCDB captures approximately 70% of incident cancersin the United States each year, making it one of the most powerfuland generalizable cancer databases in the world. Ongoing vali-dation of NCDB data accuracy and quality is performed throughinternal monitoring, site surveys, and data quality reviews (17).Data coding methods have been described previously (3, 18).Institutional review board approval was obtained to conduct thisstudy on deidentified data.
Inclusion/exclusion criteria
We extracted data on individuals undergoing RC for a new diag-nosis of bladder cancer between January 1, 1998 and December
31, 2009 for whom full clinical and pathologic staging data wereavailable (nZ18,659). Patients with all American Joint Commit-tee on Cancer (AJCC), sixth edition, stages were included; how-ever, those with clinical evidence of distant metastatic disease(cM1) were excluded (nZ571). Patients with data missing on sex(nZ7), facility type (nZ831), or geographic region (nZ186)were excluded. Those with uncommon forms of US gov-ernmentesponsored insurance (nZ106) or treated at pediatriccenters (nZ5) were also excluded owing to low patient numbersrelative to the cohort as a whole. A total of 16,953 patients met allof the study criteria and were included in the primary analysis.
Variable definition
Race was categorized as non-Hispanic white, Hispanic, black, orother. Region of residence was recorded per the 4 US Censusregions (19). Patient insurance was categorized as private,Medicaid, young (age <65 years) Medicare, older (age �65 years)Medicare, or uninsured. Facility type and volume designationshave been described previously (3, 20). Educational achievementwas defined as the percentage of residents per ZIP code without ahigh school diploma. Data regarding the extent of lymphadenec-tomy was not available, and so the number of lymph nodes (LNs)examined was used as a surrogate. Tumor grade and histologywere obtained from the individual treating centers. Preoperativechemotherapy was defined as receipt of chemotherapy up to 180days before RC, whereas postoperative chemotherapy was up to180 days after RC. Hydronephrosis/hydroureter was identifiedusing International Classification of Diseases, Ninth Revision,Clinical Modification diagnosis codes 591.00 and 593.50.Upstaging was defined as any stage group increase in overallpathologic stage relative to clinical stage, whereas downstagingwas any decrease. For analyses limited to T stage, discrepancywas defined as a full-stage change (ie, T2/T3 rather thanT3a/T3b).
Statistical analysis
Multivariate generalized estimating equation models using anexchangeable correlation matrix to account for facility clusteringwere used to identify variables associated with stage discrepancy.Given the large number of patients and events, all potentiallyrelevant variables were included in the models. A P value <.05was considered significant. Statistical analysis was performedusing SAS, version 9.3 (SAS Institute, Cary, NC). Kaplan-Meiersurvival curves were constructed using Sigmaplot, version 11.0.
Owing to the nature of data reporting in the NCDB, 5-yearsurvival data were only available for patients treated between 1998and 2004. Of the 7456 patients from this period, 186 were missingdata needed to calculate follow-up time, leaving 7270 patients foranalysis. Survival was compared using the Kaplan-Meier method,and log-rank P values were reported. Pairwise comparisons wereperformed using the Holm-Sidak method to adjust for multiple

Table 1 Patient characteristics
Characteristic n (%)
SexMale 12,501 (73.7)Female 4452 (26.3)
RaceWhite 13,908 (82.0)Hispanic 420 (2.5)Black 889 (5.2)Other 305 (1.8)Missing 1431 (8.4)
Age (y)<60 4413 (26.0)60-69 5348 (31.6)70-79 5371 (31.7)�80 1821 (10.7)
Insurance statusUninsured 457 (2.7)Medicaid 618 (3.7)Younger Medicare 667 (3.9)Older Medicare 8049 (47.5)Private 6342 (37.4)Missing 820 (4.8)
RegionNortheast 3775 (22.3)Midwest 4882 (28.8)South 5284 (31.2)West 3012 (17.8)
Facility typeCommunity cancer center 1886 (11.1)Comprehensive cancer center 6582 (38.8)Teaching/research 4369 (25.8)NCI-designated center 4116 (24.3)
Treatment year1998-2004 7456 (44.0)2005-2009 9497 (56.0)
Tumor grade1 299 (1.8)2 1226 (7.2)3-4 15,428 (91.0)
HistologyUrothelial 15,314 (90.3)Squamous 801 (4.7)Adenocarcinoma 448 (2.6)Carcinoma NOS 337 (2.0)Other 390 (2.3)
TreatmentRC alone 12,597 (74.3)RC/CT 3705 (21.9)CT/RC 651 (3.8)
Lymph nodes examined0 1616 (9.5)1-9 6735 (39.7)�10 7586 (44.8)Unknown 1016 (6.0)
Abbreviations: CT Z chemotherapy; NCI Z National Cancer
Institute; NOS Z not otherwise specified; RC Z radical cystectomy.
Gray et al. International Journal of Radiation Oncology � Biology � Physics1050
comparisons. Cox proportional hazards models were used toidentify independent predictors of survival.
Results
Patient characteristics
Patient characteristics are shown in Table 1. Median patient agewas 67 years. The majority (74.3%) of patients received RC alone.Postoperative chemotherapy was used in 21.9% of patients,whereas 3.8% received preoperative chemotherapy.
Staging and stage discrepancy
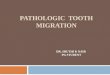
Discrepancies in overall AJCC stage were common (Fig. 1A, B;tabulated data available in Table e1, available online). Stagediscrepancy was found in 47.8% of patients: 41.9% upstaging and5.9% downstaging. Upstaging rates for clinical stage 0, I, II, andIII were 35.2%, 46.4%, 51.1%, and 22.7%, respectively. Down-staging rates for clinical stage I, II, III, and IV were 4.6%, 5.0%,9.0%, and 13.0%, respectively. Analysis by T stage is shown inFigure 1C and D (tabulated data available in Table e2). Thisanalysis demonstrated a similar discrepancy rate of 44.4% (37.9%upstaging and 6.5% downstaging). A total of 93.3% of patientswere clinically node-negative, and of these, 19.3% were upstagedto node-positive at RC. Of those patients who were clinicallynode-positive, 11.7% were found to be pathologically node-negative (full data available in Table e3).
Factors associated with stage discrepancy
Table 2 shows multivariate analysis of factors associated withupstaging. Upstaging was more common in females (odds ratio[OR] 1.09, PZ.031), and its prevalence rose with age (OR 1.29for age �80 vs <60 years, PZ.001). Upstaging increased whenmore LNs were examined (OR 1.87 for �10 LNs examined vs0, P<.001). Upstaging was also associated with higher gradeand nonurothelial histology. Receipt of preoperative chemo-therapy had no significant effect on upstaging rates. Becauseinformation on hydronephrosis/hydroureter was only availablefor patients diagnosed between 2003 and 2009, we conducted asensitivity analysis on this subpopulation, which demonstratedthat hydronephrosis/hydroureter was also associated withupstaging (OR 1.65, P<.001).
Table 3 shows multivariate analysis of factors associated withdownstaging. Downstaging was inversely associated with age,Hispanic race (OR 0.58 vs whites, PZ.010), and nonurothelialhistology. Patients treated at community centers or communitycomprehensive centers were less likely to be downstaged (OR0.64, PZ.008 and OR 0.76, PZ.024, respectively). There was astatistical trend toward increased odds of downstaging at NationalCancer Institute (NCI)-designated cancer centers (OR 1.32,PZ.069). Patients who received preoperative chemotherapy weremuch more likely to be downstaged at RC (OR 2.31, P<.001).
Receipt of preoperative chemotherapy was inversely associatedwith age, with 4.7% of patients aged <60 years receivingchemotherapy compared with 2.8% of those aged �80 years(PZ.002). Given concern that differential exposure and use of anypreoperative therapy was the major driver of our downstagingmodel, we constructed a second model omitting all patients who
received preoperative chemotherapy. Only 3 factors changedsignificantly in this model: geographic region (no longer signifi-cantly associated), carcinoma not otherwise specified histology

Fig. 1. Stage distribution in bladder cancer patients. (A) Overall American Joint Committee on Cancer (AJCC) clinical stage, (B) overallAJCC pathologic stage, (C) clinical tumor (T) stage, (D) pathologic tumor (T) stage.
Volume 88 � Number 5 � 2014 Clinical staging in bladder cancer 1051
(adjusted OR 0.55, PZ.024), and receipt of therapy at an NCI-designated center (adjusted OR 1.43, PZ.025).
Survival analyses
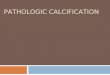
Median follow-up for all patients was 43 months; 76% of sur-viving patients had full 5-year follow-up. Kaplan-Meier survivalcurves by clinical stage and stratified by stage discrepancy areshown in Figure 2, with tabulated data available in Table e4. Five-year overall survival (OS) rates for clinical stage 0, I, II, III, andIV were 67.2%, 62.9%, 50.4%, 36.9%, and 27.2%, respectively.Stage discrepancy resulted in significant survival differences forall patients (P<.001). Pairwise comparisons revealed thatupstaging was associated with decreased survival for all stages.Downstaging resulted in improved survival only in those patientswith clinical stage III or IV disease (P<.001 and PZ.014,respectively). Five-year OS rates for pathologic stage 0, I, II, III,and IV were 70.8%, 75.8%, 63.7%, 41.5%, and 24.7%, respec-tively. For patients with a given pathologic stage, having had theirclinical stage downstaged typically resulted in lower 5-year OSrates compared with those with stage concordance. These differ-ences, however, did not reach statistical significance, though astatistical trend was present in those with pathologic stage IIIdisease. Five-year OS rates for those who were upstaged to a
particular pathologic stage group were similar to those with stageconcordance within that group who remained within a given stage.Full data are available in Table e5.
Multivariate Cox regression analysis is shown in Table 4.Upstaging was associated with increased hazard for death at 5 years(hazard ratio [HR] 1.80, P<.001), but downstaging was not signif-icantly associated with survival (HR 0.88, PZ.160). Black race andtreatment in regions within the lowest quartile of educationalachievement were associated with increased hazard for death (HR1.30, P<.001; HR 1.17, PZ.006, respectively), as was any form ofnonprivate insurance. High tumor grade was also associated withincreased risk of death (HR 1.64, PZ.004). Patients with�10 LNsexamined had decreased risk of death (HR 0.76 vs 0 LNs examined,P<.001). Five-year survival rates for 0, 1-9, and�10 LNs examinedwere 45.5%, 47.3%, and 55.4%, respectively (P<.001).
Treatment at an NCI-designated cancer center was associatedwith improved survival relative to teaching/research facilities (HR0.90, PZ.042). Finally, use of chemotherapy preoperatively orpostoperatively was associated with increased risk of death (HR1.28, PZ.022 and HR 1.23, P<.001, respectively). Use of pre-operative chemotherapy was more common in clinical stage IVpatients relative to other groups (6.8% vs 3.6%, P<.001). Giventhe concern that our model included patients who underwent RCsolely with palliative intent, we constructed an additional modelthat excluded clinically node-positive patients treated with

Table 2 Multivariate analysis of factors predictive ofupstaging at time of cystectomy
Characteristic OR 95% CI P
SexMale 1Female 1.09 1.01-1.17 .031*
Age group (y)<60 160-69 1.08 0.99-1.18 .09770-79 1.19 1.07-1.32 .002*
�80 1.29 1.12-1.47 .001*
RaceWhite 1Hispanic 0.88 0.71-1.09 .229Black 1.05 0.92-1.20 .481Other 0.98 0.75-1.28 .884Missing 0.96 0.79-1.15 .654
Geographic regionNortheast 1Midwest 0.90 0.79-1.04 .149South 0.83 0.72-0.94 .006*
West 0.88 0.76-1.02 .093Diagnosis period1998-2004 12005-2009 0.95 0.88-1.03 .219
Tumor grade1 12 1.46 1.08-1.99 .015*
3-4 2.17 1.63-2.89 <.001*
Unknown 0.54 0.46-0.63 <.001*
Lymph nodes examined0 11-9 1.59 1.4-1.8 <.001*
�10 1.87 1.64-2.13 <.001*
Unknown 1.51 1.26-1.82 <.001*
MorphologyUrothelial 1Squamous 1.31 1.11-1.54 .002*
Adenocarcinoma 1.26 1.02-1.56 .029*
Carcinoma NOS 1.21 0.97-1.51 .091Other 0.96 0.56-1.66 .883
Facility typeTeaching/research 1Community cancer center 0.99 0.82-1.19 .905Comprehensive cancer center 1.07 0.94-1.21 .311NCI-designated center 1.01 0.86-1.19 .882
Facility volumeHigh 1Medium 0.95 0.77-1.18 .645Low 0.98 0.85-1.12 .756
TreatmentNo preoperative chemotherapy 1Preoperative chemotherapy 0.88 0.74-1.05 .167
Abbreviations: CI Z confidence interval; OR Z odds ratio. Other
abbreviations as in Table 1.
* Statistically significant.
Table 3 Multivariate analysis of factors predictive ofdownstaging at time of cystectomy
Characteristic OR 95% CI P
SexMale 1Female 0.87 0.73-1.02 .088
Age group (y)<60 160-69 0.9 0.74-1.08 .24670-79 0.66 0.52-0.84 .001*
�80 0.50 0.36-0.68 <.001*
RaceWhite 1Hispanic 0.58 0.36-0.94 .010*
Black 0.86 0.61-1.20 .373Other 0.93 0.57-1.52 .762Missing 1.12 0.83-1.52 .470
Geographic regionNortheast 1Midwest 0.94 0.72-1.22 .637South 0.98 0.77-1.25 .877West 0.68 0.49-0.94 .019*
Diagnosis period1998-2004 12005-2009 1.16 0.98-1.38 .092
Tumor grade1 12 0.91 0.55-1.49 .7103-4 0.73 0.47-1.13 .206Unknown 1.07 0.8-1.43 .636
Lymph nodes examined0 11-9 0.86 0.68-1.1 .251�10 0.97 0.76-1.25 .822Unknown 1.23 0.87-1.76 .262
MorphologyUrothelial 1Squamous 0.56 0.36-0.86 .003*
Adenocarcinoma 0.30 0.14-0.63 <.001*
Carcinoma NOS 0.64 0.36-1.14 .077Other 0.57 0.12-2.74 .384
Facility typeTeaching/research 1Community cancer center 0.64 0.46-0.89 .008*
Comprehensive cancer center 0.76 0.61-0.96 .024*
NCI-designated center 1.32 0.99-1.77 .069Facility volumeHigh 1Medium 0.92 0.59-1.44 .724Low 0.92 0.71-1.19 .510
TreatmentNo preoperative chemotherapy 1Preoperative chemotherapy 2.31 1.72-3.10 <.001*
Abbreviations as in Tables 1 and 2.
* Statistically significant.
Gray et al. International Journal of Radiation Oncology � Biology � Physics1052
preoperative chemotherapy from our model (nZ72). In this modelpreoperative chemotherapy was no longer significantly associatedwith survival (HR 1.21, PZ.138). No other significant changes in
the other covariates were identified. Exclusion of all patientsreceiving preoperative chemotherapy from the Cox regressionmodel also did not significantly change the hazard ratios for any ofthe included covariates.

Fig. 2. Kaplan-Meier overall survival curves for (A) all clinical stages, and by stage discrepancy for (B) clinical stage 0, (C) clinical stageI, (D) clinical stage II, (E) clinical stage III, and (F) clinical stage IV.
Volume 88 � Number 5 � 2014 Clinical staging in bladder cancer 1053
Discussion
Using contemporary data from the NCDB, including data fromacademic and community centers, we present here the largeststudy to date describing clinical staging in bladder cancer. Weidentify that nearly half of bladder cancer patients undergoing RChave a pathologic stage discordant with their clinical stage. Thishigh level of discrepancy has important implications for prog-nostication, therapy selection, and risk stratification in the designof clinical trials investigating novel nonoperative therapies forbladder cancer. As previously stated, such therapies lack thebenefit of final pathologic stage, and so significant rates ofdiscrepancy between clinical stage and pathologic stage make itextremely difficult to accurately compare the outcomes forpatients treated with chemoradiation therapy or other nonoperativeapproaches to those treated with RC.
The rate of upstaging in our series (41.9%) is consistent withother studies, which ranged between 25% and 54% (7-10, 12-14,21, 22). Our findings that advanced age, hydronephrosis/hydro-ureter, and nonurothelial histology are associated with increasedupstaging are also consistent with previous studies (11, 23, 24).The association of advanced age with upstaging is particularlyimportant because patients referred for chemoradiation therapyare often significantly older than those who undergo RC. Thisfinding may suggest that elderly patients may not be undergoingan adequate staging workup before surgery, but it may also
suggest that a unique biology is present in elderly patients withbladder cancer. We also identify female sex as a risk factor forupstaging in our cohort. This may be related to differential timingof diagnosis because women presenting with hematuria may firstundergo an extensive gynecologic workup, delaying the finaldiagnosis of bladder cancer (25). This delay can allow formicroscopic progression of disease before definitive treatment andmay at least partially account for this finding.
Our rate of downstaging (5.9%) was lower than that in all of theaforementioned published series, which ranged from 7% to 33%.All of these previous studies relied on data accumulated from largeacademic centers. As our data demonstrate, downstaging is muchless common at community centers (which constitute the bulk oftreating institutions in the United States). The high rates ofdownstaging at large academic centers may be related to greateruse of preoperative chemotherapy (though this was controlled for)and/or increased aggressiveness of initial or repeat transurethralresection of the bladder tumor. Large centers may also morefrequently use advanced imaging techniques such as MRI, whichcan over-call the extent of disease (26). Despite this, downstaginghas been shown to have a positive impact on outcome regardless ofstage, and so more aggressive use of staging studies should notnecessarily be discouraged on the basis of this finding (27).Although higher rates of downstaging were present at NCI-designated cancer centers, this was controlled for in our multi-variate model, and so other factors are likely responsible for the

Table 4 Multivariate Cox regression analysis of factorsaffecting overall survival
Characteristic Hazard ratio 95% CI P
Stage discrepancyStage agreement 1Upstaged 1.80 1.67-1.93 <.001*
Downstaged 0.88 0.73-1.05 .160RaceWhite 1Hispanic 1.15 0.92-1.45 .223Black 1.30 1.12-1.50 <.001*
Other 0.91 0.67-1.24 .550InsurancePrivate 1Uninsured 1.48 1.18-1.86 <.001*
Medicaid 1.40 1.13-1.72 <.001*
Young Medicare 1.42 1.19-1.70 <.001*
Older Medicare 1.17 1.06-1.29 <.001*
Tumor grade1 12 1.40 0.98-1.99 .5503-4 1.64 1.17-2.31 .004*
Unknown 0.73 0.60-0.88 .001*
Lymph nodes examined0 11-9 0.91 0.82-1.02 .094�10 0.76 0.68-0.86 <.001*
Unknown 0.89 0.77-1.02 .095Facility typeTeaching/research 1Community cancer center 1.04 0.91-1.18 .613Comprehensive cancercenter
1.08 0.99-1.18 .089
NCI-designated center 0.90 0.81-1.00 .042*
Number in region withouthigh school diploma
<14% 1.0014%-19.9% 1.04 0.95-1.14 .45220%-28.9% 1.07 0.97-1.17 .190�29% 1.17 1.04-1.30 .006*
Facility volumeHigh 1Medium 1.17 1.04-1.28 .004*
Low 1.04 0.86-1.26 .664Use of chemotherapyRadical cystectomyonly
1
Preoperativechemotherapy
1.28 1.04-1.59 .022*
Postoperativechemotherapy
1.23 1.12-1.34 <.001*
Abbreviations as in Tables 1 and 2.
Models also adjusted for treatment year and geographic location. Sex,
histology, and age were adjusted for in-strata owing to violation of the
proportional hazards assumption.
* Statistically significant.
Gray et al. International Journal of Radiation Oncology � Biology � Physics1054
superior survival outcomes seen at such centers. The low rate ofdownstaging in Hispanics has been reported previously (28).Interestingly, the same trend was not present in black patients, who
are also more likely to present with advanced disease (29). Aswould be expected, receipt of preoperative chemotherapy wasassociated with higher rates of downstaging. Interestingly, receiptof such therapy did not significantly affect the risk for upstaging,suggesting that intensification of preoperative treatment is likelynot a sufficient method to address the high rates of discrepancypresent in this population.
In addition to identifying markers of poor socioeconomic sta-tus, which have long been associated with poor survival in cancerpatients, our analysis of factors independently associated withsurvival also produced several results worthy of discussion. Theseinclude the finding that a greater number of examined LNs wasassociated with a lower HR for death, despite being associatedwith higher rates of upstaging. Our results confirm those of smallerseries identifying superior outcomes when a greater number ofLNs are removed at RC and support the role of aggressive lym-phadenectomy until data from prospective trials become available(30, 31). Additionally, our data suggest that more accurate studiesare needed to assess for occult lymph node involvement and that apotential benefit may exist for addressing the pelvic lymph nodesin patients managed by chemoradiation therapy.
We also identified receipt of chemotherapy as associated with anincreased hazard for death. Patients selected to receive chemo-therapy are more likely to have advanced disease, and so this mayrepresent confounding by indication not fully addressed by ourmultivariate model. Our finding that preoperative chemotherapyleads to poor survival seems to conflict with level 1 evidence to thecontrary (32, 33). For patients with LN involvement, chemotherapymay be used as the primary modality of therapy, with RC reservedfor those with favorable responses or in need of local palliation.Such treatment would fall under our definition of preoperativechemotherapy. When we excluded these patients in an adjustedmodel this finding was no longer statistically significant, althoughthis could be due to decreased power. Of note, the NCDB does notrecord the type of chemotherapy received, and less-aggressiveregimens (common during the analyzed era) may have resulted inpoorer outcomes for patients (34). As such, these findings must beinterpreted with caution and, given the high rates of upstagingoverall, the trend towards increased utilization of neoadjuvantchemotherapy seems justified. Additionally, given the high degreeof upstaging present in patients initially diagnosed with non-mus-cle-invasive disease, further studies should be performed to assessthe benefit of preoperative chemotherapy in this subgroup.
Our study has several limitations, including those presentwithin any retrospective large database study, such as selectionbias and the potential for miscoding. Additionally, although theNCDB contains a wide array of useful data, it is not all-inclusive,and we are unable to comment on factors such as imaging mo-dalities or clinical examinations used to determine clinical stage orthe extent of transurethral resection. Variation in such practices atdifferent center types could affect clinical stage; however, stagediscrepancy remains a significant problem across all analyzedtreatment facilities. Additionally, the NCDB is also limited to dataobtained from Commission on Cancereaccredited facilities,which may not include some small rural facilities. Finally, ourstudy is limited by the outcomes data present in the NCDB, whichdoes not allow us to comment on patterns of failure. Althoughsuch endpoints are useful, OS remains the most robust clinicalendpoint. Despite these limitations, our cohort is significantlylarger than all previous studies and captures data from center typesacross the United States, including small community practices.Thus, our findings may be more broadly generalizable.

Volume 88 � Number 5 � 2014 Clinical staging in bladder cancer 1055
Conclusions
Accurate clinical staging is a matter of concern in all cancers forwhich limited pathologic information may be available (eg, biopsysampling for prostate cancer, sentinel LN biopsy in breast cancer,nodal staging in lung cancer) and/or where preoperative therapyhas become commonplace (eg, rectal adenocarcinoma, locallyadvanced breast cancer, tumors of the head and neck). Our studyprovides strong evidence confirming that current clinical stagingin bladder cancer is inadequate, resulting in high rates of stagediscrepancy across the United States. This high rate of discor-dance results in large differences in survival for a given clinicalstage compared with the same pathologic stage, especially forthose with stage I and II disease. These data should therefore betaken into account in the design of future clinical trials, especiallythose investigating nonoperative management strategies such aschemoradiotherapy, as such studies must compare their outcomesto radical cystectomy without the benefit of pathologic stage. Thischallenge in identifying patients with more advanced disease atpresentation highlights the need for improved clinical staging,including the further development of novel imaging modalitiesand biomarkers of tumor behavior.
References
1. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer
J Clin 2013;63:11-30.
2. Herr HW, Schwalb DM, Zhang ZF, et al. Intravesical bacillus
Calmette-Guerin therapy prevents tumor progression and death from
superficial bladder cancer: Ten-year follow-up of a prospective ran-
domized trial. J Clin Oncol 1995;13:1404-1408.
3. Gray PJ, Fedewa SA, Shipley WU, et al. Use of potentially curative
therapies for muscle-invasive bladder cancer in the United States:
Results from the National Cancer Data Base. Eur Urol 2013;63:
823-829.
4. Efstathiou JA, Spiegel DY, Shipley WU, et al. Long-term outcomes of
selective bladder preservation by combined-modality therapy for
invasive bladder cancer: The MGH experience. Eur Urol 2012;61:
705-711.
5. James ND, Hussain SA, Hall E, et al. Radiotherapy with or without
chemotherapy in muscle-invasive bladder cancer. N Engl J Med 2012;
366:1477-1488.
6. Rodel C, Grabenbauer GG, Kuhn R, et al. Combined-modality treat-
ment and selective organ preservation in invasive bladder cancer:
Long-term results. J Clin Oncol 2002;20:3061-3071.
7. Svatek RS, Shariat SF, Novara G, et al. Discrepancy between clinical
and pathological stage: External validation of the impact on prognosis
in an international radical cystectomy cohort. BJU Int 2011;107:
898-904.
8. Canter D, Long C, Kutikov A, et al. Clinicopathological outcomes
after radical cystectomy for clinical T2 urothelial carcinoma: Further
evidence to support the use of neoadjuvant chemotherapy. BJU Int
2011;107:58-62.
9. Ploeg M, Kiemeney LA, Smits GA, et al. Discrepancy between clin-
ical staging through bimanual palpation and pathological staging after
cystectomy. Urol Oncol 2012;30:247-251.
10. McLaughlin S, Shephard J, Wallen E, et al. Comparison of the clinical
and pathologic staging in patients undergoing radical cystectomy for
bladder cancer. Int Braz J Urol 2007;33:25-31. discussion 31e22.
11. Nielsen ME, Shariat SF, Karakiewicz PI, et al. Advanced age is
associated with poorer bladder cancer-specific survival in patients
treated with radical cystectomy. Eur Urol 2007;51:699-706. discussion
706-698.
12. Shariat SF, Palapattu GS, Karakiewicz PI, et al. Discrepancy
between clinical and pathologic stage: Impact on prognosis
after radical cystectomy. Eur Urol 2007;51:137-149. discussion
149-151.
13. Dutta SC, Smith JA Jr, Shappell SB, et al. Clinical under staging of
high risk nonmuscle invasive urothelial carcinoma treated with radical
cystectomy. J Urol 2001;166:490-493.
14. Pagano F, Bassi P, Galetti TP, et al. Results of contemporary radical
cystectomy for invasive bladder cancer: A clinicopathological study
with an emphasis on the inadequacy of the tumor, nodes and metas-
tases classification. J Urol 1991;145:45-50.
15. Goossens-Laan CA, Visser O, Hulshof MC, et al. Survival after
treatment for carcinoma invading bladder muscle: A Dutch
population-based study on the impact of hospital volume. BJU Int
2012;110:226-232.
16. Hollenbeck BK, Daignault S, Dunn RL, et al. Getting under the hood
of the volume-outcome relationship for radical cystectomy. J Urol
2007;177:2095-2099. discussion 2099.
17. Bilimoria KY, Bentrem DJ, Stewart AK, et al. Comparison of com-
mission on cancer-approved and -nonapproved hospitals in the United
States: Implications for studies that use the National Cancer Data
Base. J Clin Oncol 2009;27:4177-4181.
18. Fedeli U, Fedewa SA, Ward EM. Treatment of muscle invasive
bladder cancer: Evidence from the National Cancer Database, 2003 to
2007. J Urol 2011;185:72-78.
19. US Census Regions; 2012. p. https://www.census.gov/geo/www/us_
regdiv.pdf.
20. Fedewa SA, Ward EM, Stewart AK, et al. Delays in adjuvant
chemotherapy treatment among patients with breast cancer are more
likely in African American and Hispanic populations: A national
cohort study 2004-2006. J Clin Oncol 2010;28:4135-4141.
21. Ficarra V, Dalpiaz O, Alrabi N, et al. Correlation between clinical and
pathological staging in a series of radical cystectomies for bladder
carcinoma. BJU Int 2005;95:786-790.
22. Hollenbeck BK, Miller DC, Dunn RL, et al. The effects of stage
divergence on survival after radical cystectomy for urothelial cancer.
Urol Oncol 2005;23:77-81.
23. Turker P, Bostrom PJ, Wroclawski ML, et al. Upstaging of uro-
thelial cancer at the time of radical cystectomy: Factors associ-
ated with upstaging and its effect on outcome. BJU Int 2012;110:
804-811.
24. Mitra AP, Skinner EC, Miranda G, et al. A precystectomy decision
model to predict pathological upstaging and oncological outcomes in
clinical stage T2 bladder cancer. BJU Int 2013;111:240-248.
25. Johnson EK, Daignault S, Zhang Y, et al. Patterns of hematuria referral
to urologists: Does a gender disparity exist? Urology 2008;72:498-
502. discussion 502-503.
26. Daneshmand S, Ahmadi H, Huynh LN, et al. Preoperative staging of
invasive bladder cancer with dynamic gadolinium-enhanced magnetic
resonance imaging: Results from a prospective study. Urology 2012;
80:1313-1318.
27. Kassouf W, Spiess PE, Brown GA, et al. P0 stage at radical cys-
tectomy for bladder cancer is associated with improved outcome
independent of traditional clinical risk factors. Eur Urol 2007;52:
769-774.
28. Manoharan M, Ayyathurai R, de Los Santos R, et al. Presentation and
outcome following radical cystectomy in Hispanics with bladder
cancer. Int Braz J Urol 2008;34:691-698. discussion 698.
29. Scosyrev E, Noyes K, Feng C, et al. Sex and racial differences in
bladder cancer presentation and mortality in the US. Cancer 2009;115:
68-74.
30. Wright JL, Lin DW, Porter MP. The association between extent
of lymphadenectomy and survival among patients with lymph
node metastases undergoing radical cystectomy. Cancer 2008;
112:2401-2408.
31. Herr HW, Bochner BH, Dalbagni G, et al. Impact of the number of
lymph nodes retrieved on outcome in patients with muscle invasive
bladder cancer. J Urol 2002;167:1295-1298.

Gray et al. International Journal of Radiation Oncology � Biology � Physics1056
32. Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant
chemotherapy plus cystectomy compared with cystectomy alone
for locally advanced bladder cancer. N Engl J Med 2003;349:
859-866.
33. Griffiths G, Hall R, Sylvester R, et al. International phase III trial
assessing neoadjuvant cisplatin, methotrexate, and vinblastine
chemotherapy for muscle-invasive bladder cancer: Long-term results
of the BA06 30894 trial. J Clin Oncol 2011;29:2171-2177.
34. Weight CJ, Garcia JA, Hansel DE, et al. Lack of pathologic down-
staging with neoadjuvant chemotherapy for muscle-invasive urothe-
lial carcinoma of the bladder: A contemporary series. Cancer 2009;
115:792-799.