Embed Size (px)
Citation preview

Clinical Update
New & updated guidelines Significant traffic light updates Significant safety issues Other issues Feedback from practices

Clinical Guidelines
COPD Guideline - UPDATED
Format changed to make more primary care focused and concise.
Information included on recently licensed LAMAs and LABA/LAMA combination inhalers.

COPD Guideline - UPDATED
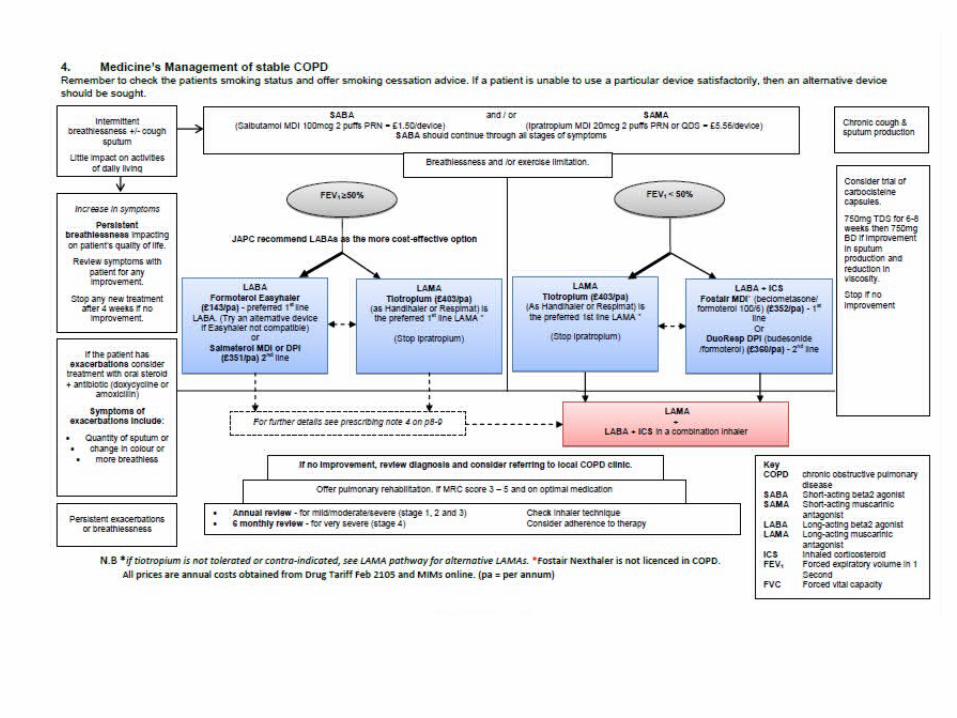
For patients with FEV1<50%, LABA + LAMA may be considered if ICS contra-indicated, declined or not tolerated, and LAMA alone not effective.
Limited evidence to suggest lung function and symptoms may be improved, but not mortality or exacerbations.
In the small number of patients where combination is to be used, cheaper to prescribe as a combination inhaler and may improve compliance e.g. Aclidinium & formoterol (Duaklir Genuair)Glycopyrronium & indacaterol (Ultibro)
COPD Guideline - UPDATED
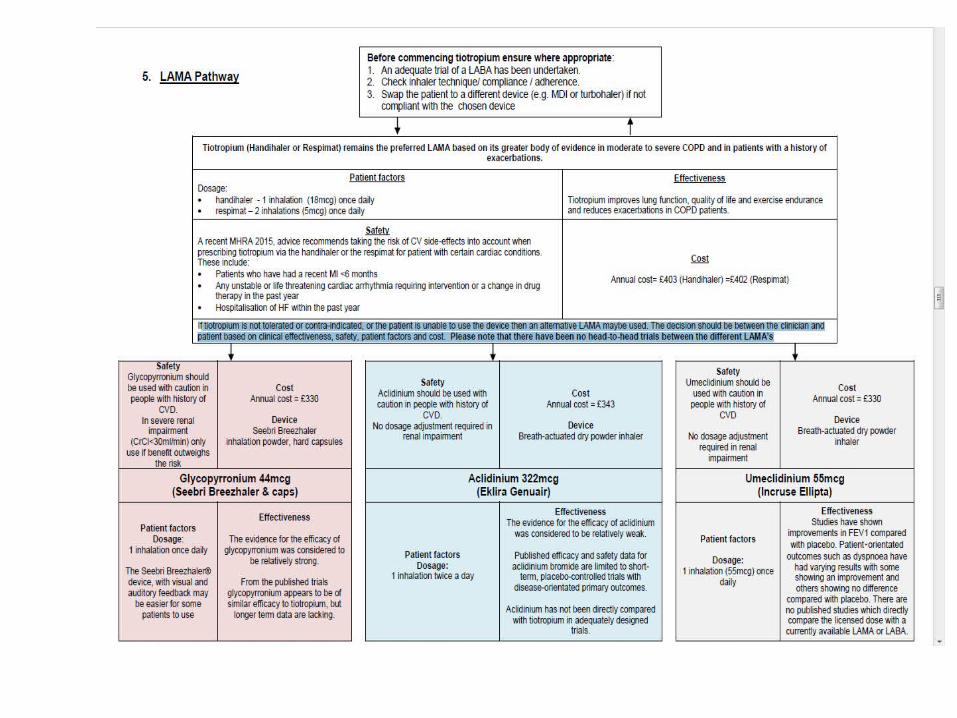
Tiotropium (Handihaler or Respimat) remains the preferred LAMA based on its greater body of evidence in moderate to severe COPD and in patients with a history of exacerbations.
If tiotropium is not tolerated, contra-indicated, or the patient is unable to use the device then an alternative LAMA may be used.
The decision should be based on clinical effectiveness, safety, patient factors and cost.
Please note that there have been no head-to-head trials between the different LAMA’s
Management of infective exacerbation of bronchiectasis in adults - NEW When antibacterial therapy may be indicated:
should be a deterioration in symptoms - the presence of purulent sputum alone, or the isolation of a pathogen alone is not necessarily an indication for antibiotic treatment, particularly in adults.
Which antibacterial: if required immediately check previous sputum
results to guide choice (table in guideline), otherwise amoxicillin, clarithromycin or doxycycline. When sputum results available check response to empirical treatment before changing treatment.
Referral criteria for hospital admission.
Management of recurrent UTIs in adult females - UPDATED
Includes information on patient groups that require a longer 5 to 10 day antibiotic course:

Continence Appliance formulary - UPDATED
Updated with cost-effective product choices by continence working group.
Pilot on-going with Continence specialist nurses reviewing specific patients across north Derbyshire and Hardwick.

Algorithm for the treatment of refractory chronic constipation - NEW
Shows the place in therapy of lubiprostone and prucalopride in line with relevant NICE TAs.
All patients – exclude other causes, diet and lifestyle, 6 month trial of two laxatives at full dose.
Women: prucalopride – BROWN after gastro consultant/specialist initiation. GPs may continue to prescribe as per algorithm. Secondary care review 12 monthly.
Men: Lubiprostone – RED i.e. hospital initiation and ongoing prescribing

Management of dyspepsia and GORD - UPDATED
Based on NICE GORD guideline and suspected cancer guideline
Expected on website soon
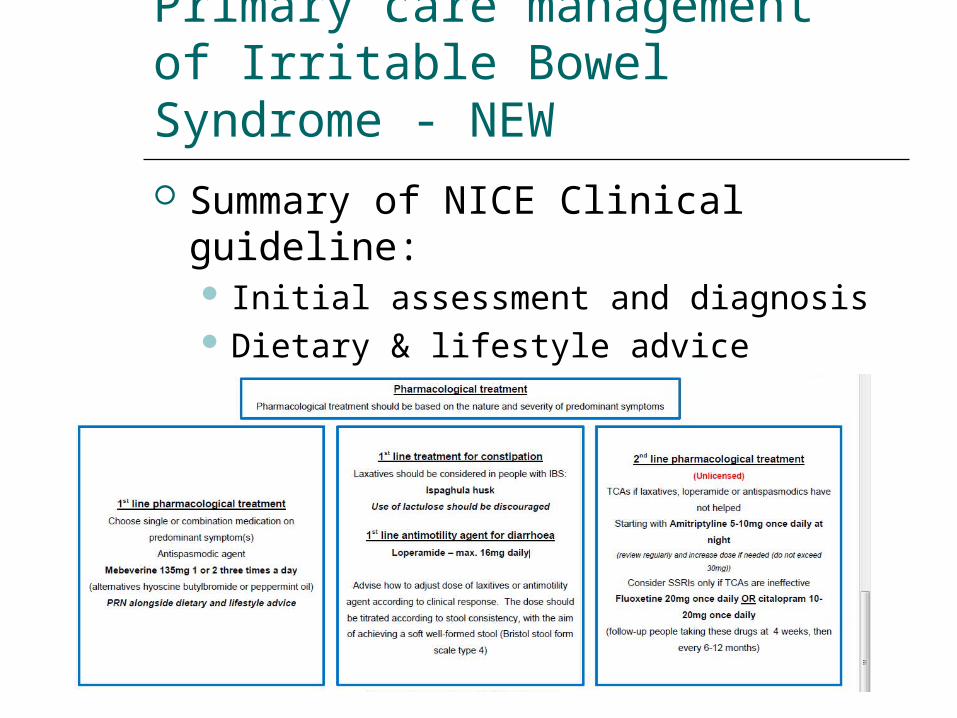
Primary care management of Irritable Bowel Syndrome - NEW
Summary of NICE Clinical guideline: Initial assessment and diagnosis Dietary & lifestyle advice Pharmacological treatment:

Significant Traffic Light Changes

Significant traffic light updates: RED
Grazax (oral grass pollen extract) for children with hay fever due to grass or tree pollen - reclassified from BLACK to RED. Prescribing will be undertaken by paediatric specialist allergy clinic. Patients should be on maximal medical treatment for at least one season prior to referral for assessment for Grazax.Referral guideline for use with DTHFT which includes off-label doses of antihistamines and montelukast, as well as nasal steroids and eye-drops if necessary.Plan to develop county wide referral guidelines for use with Sheffield.

Significant traffic light updates: RED
Sildenafil for digital ulcers in systemic sclerosis – RED. Off-label.
Budesonide multimatrix (Cortiment) - RED. Oral treatment for UC with a topical action in the colon.
Relatively weak evidence, place in therapy currently unclear.
Acute course for 8 weeks.
Significant traffic light updates: RED
Lofexidine – reclassified from amber. No prescribing outside Derby City.
Significant traffic light updates: GREEN
Brinzolamide 1% & brimonidine 0.2% eye-drops (Simbrinza) – Green after specialist initiationBrinzolamide (carbonic anhydrase inhibitor) and brimonidine (alpha 2 agonist) used third or fourth line (prostaglandins and beta-blockers first and second line).Combination product reduces exposure to preservatives and improves compliance.Glaucoma and ocular hypertension with suspected glaucoma treatment algorithms to be developed.

Significant traffic light updates: GREEN
Apixaban – Green after specialist initiation for the treatment and secondary prevention of DVT and/or PE.
Cabergoline and quinagolide - Green after consultant initiation for hyperprolactinaemia. Reclassified from amber. Prescribing guidance developed. Monitoring to be undertaken by secondary care (periodic monitoring of prolactin levels and repeat ECHO).
Significant traffic light updates: BLACK
Levosertlevonorgestrol IUS licensed for heavy menstrual bleeding and contraception.Only licensed for 3 years (Mirena 5 years)No clinical benefit over Mirena.Levonorgestrel IUS should be prescribed as the brand Mirena to ensure most cost-effective product dispensed and to avoid confusion.

Miscellaneous
IMPROVE-IT studyEzetimibe 10 + simva 40 following ACS vs simva 40 alone.Limited patient orientated outcomes – NNT of 50 over 5 years to prevent death or CV event.Effect due to lipid lowering.Current guidance now for atorva 80 which will provide greater lipid lowering at reduced cost.

Miscellaneous
BMA duty of care – guidance issued and shared with JAPC Responsibility for ensuring results are acted upon rests with person requesting the test (not acceptable for hospital doctors to ask GPs to find out results that hospital had ordered).Doctor recommending a prescription should provide counselling on side-effects and precautions and ensure any necessary monitoring is agreed between primary and secondary care clinicians. However, all prescribers must also be aware that the ultimate responsibility for the prescription lies with the prescribing doctor and cannot be delegated.
Miscellaneous
BreathMOR studyHeart failure study to assess the benefit of MR morphine on breathlessness in severely symptomatic patients.CRH is a recruitment site.GPs may be asked to continue MR morphine 10mg twice daily.
Miscellaneous
Meningitis B vaccinationFrom Sep 15 meningitis B vaccination (Bexsero) will be offered as part of the national program at two, four and 12 months.Fever is more common when the MenB vaccine is given with the other routine vaccines at two and four months.Three doses of paracetamol are recommended following the vaccination at 2 and 4 months to reduce fever.
Miscellaneous
Currently paracetamol licences cover the treatment of pain and fever, not prophylaxis, and state that no more than two 60mg doses of paracetamol should be given to infants aged 2 to 3 months, without seeking the advice of a doctor or pharmacist. Note: very prem babies born before 32 weeks will require individual dose prescribed by GP in line with cBNF
The CHM support the off-label use of paracetamol in this specific circumstance.
PHE have published resources recommending that paracetamol should be purchased OTC.
Miscellanous
Gliptins and joint painUS FDA have advised that gliptins may cause joint pain that can be severe and disabling.Symptoms may occur one day to years after starting treatment but are usually relieved within a month of discontinuing treatment.

Miscellaneous
Medicines management website now has a section for care homes and social care.

Other issues
Oxycodone high strength incident
Care needs to be taken when prescribing liquid preparations with normal and concentrated strengths e.g. oxycodone / morphine / methadone
A protocol can be put on the clinical system to alert prescribers when prescribing the concentrated product to check it is intended. Ask your medicines management technician for details.
Pregabalin – spend is increasing significantly
Recommended only for use when gabapentin has been tried, has been beneficial for the patient but they have been unable to tolerate it.
NDCCG spend on pregabalin is 20% higher this year than last year.
Is it being used in line with guidance?
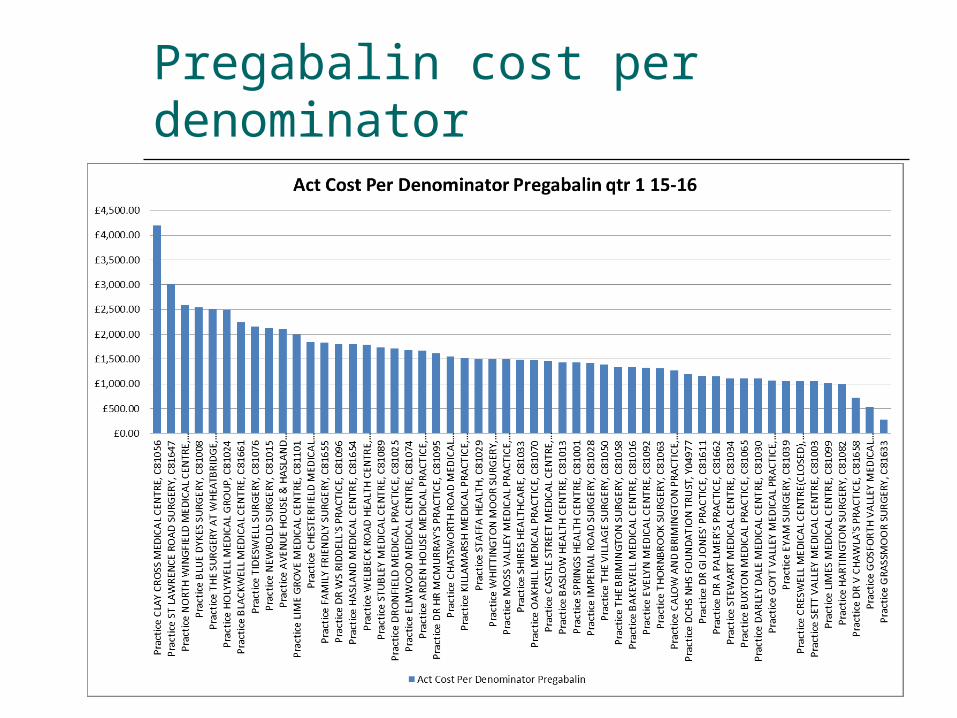
Pregabalin cost per denominator

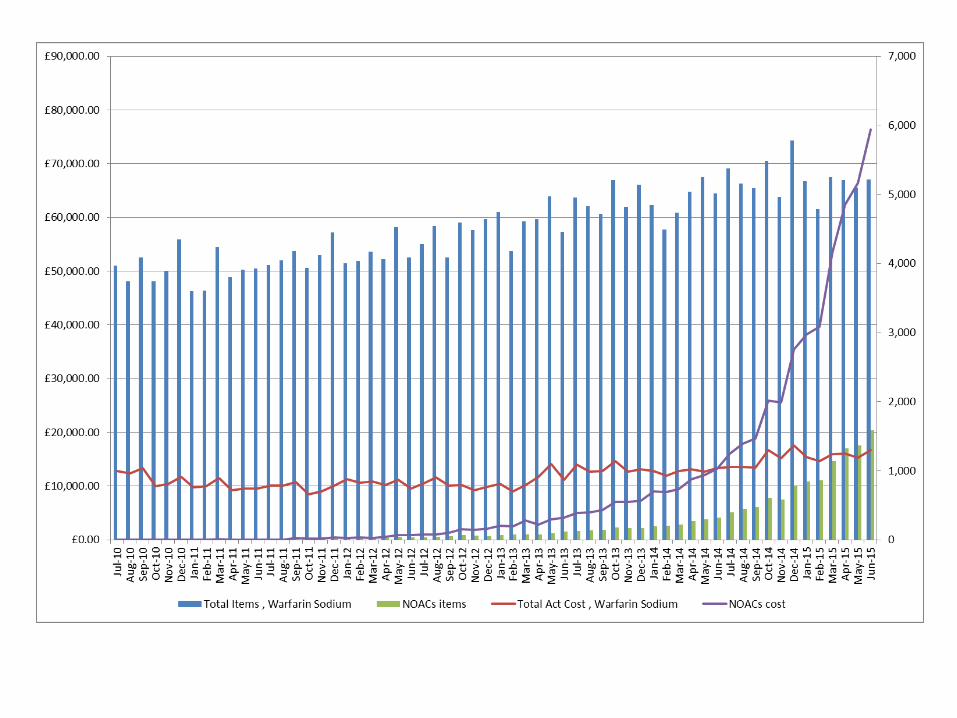
NOACs
Jon can offer practice training session on NOACs and AF resources
Significant increase in use of NOACs
Desmopressin for nocturnal enuresis
Primary nocturnal enuresis - only tablets are licensed. For prescribing advice see NICE CG 111 on the management of bedwetting in children and young people.
See BNF for CSM warning regarding hyponatraemic convulsions: Patients being treated for primary nocturnal enuresis should be warned to avoid fluid overload (limit fluid intake from 1 hour before until 8 hours after administration and avoid ingesting during swimming) and to stop taking desmopressin during an episode of vomiting and diarrhoea (until fluid balance normal). The risk of hyponatraemic convulsions can also be minimised by keeping the recommended starting doses and by avoiding concomitant use of drugs which increase secretion of vasopressin (e.g. tricyclics)

Molloscum contagiosum posters and leaflets in GP waiting rooms
Leaflets recommend treatment with Molludab, however…
JAPC advice is that this is a common, self-limiting condition which usually doesn’t require treatment.
Lesions clear up within 12 to 18 months and generally affects pre-school children.

Molloscum contagiosum posters and leaflets in GP waiting rooms
Molludab is RED in Derbyshire for very specific circumstances (HIV positive patients with extensive lesions, eye lid-margin or ocular lesions and adults with anogenital lesions indications) by consultants or specialists (including GPSIs and dermatology champions).
Practices may wish to remove the information, or ensure that routine prescribing is not recommended except in very specific circumstances by specialists.
Available OTC but £23.49
Significant Safety Updates
Drug safety Update – June 15
SGLT2 inhibitors (canagliflozin, dapagliflozin, empagliflozin): risk of diabetic ketoacidosis.Licensed for adults with Type 2 diabetes.Serious cases of DKA reported, often with only moderately raised blood glucose (< 14 mmol/L) i.e. atypical presentation.Half of cases occurred during first 2 months; some shortly after stopping.One third of cases involved off-label use in type 1 diabetes.
Drug safety Update – June 15
MHRA advice is toTest for ketones in patients with acidosis symptoms even if plasma glucose levels are near-normal.Stop SGLT2 inhibitor treatment if DKA is suspected.Inform patients of signs of DKA and to seek immediate medical help (nausea, vomiting, anorexia, abdo pain, thirst, difficulty breathing, unusual fatigue/sleepiness)

Drug safety Update – June 15High dose ibuprofen (≥2400mg/day): small increase in cardiovascular risk (heart-attack and stroke).Risk similar to COX-2 inhibitors and diclofenac.No increased risk with doses up to 1200mg/day; limited data with doses between 1200mg and 2400mg/day.Possible interaction between ibuprofen and low-dose aspirin?Ibuprofen competitively inhibits the effect of low dose aspirin on platelet aggregation, data does not support a clinically meaningful interaction, however possibility cannot be ruled out with long-term use.

Drug safety Update – June 15
Intrauterine contraception : risk factors for uterine perforation.Perforation occurs rarely (less than 1 in 1000 women).Applies to both levonorgestrel-releasing IUSs (Mirena, Levosert, Jaydess) and copper IUDs. Most important risk factors are insertion during lactation and insertion in the 36 weeks after giving birth (but benefits still strongly outweigh risks).Most often occurs during insertion but might not be detected until some time later.
Drug safety Update – June 15
Inform women that symptoms include:Severe pelvic pain after insertionPain or heavy bleeding after insertion that continues for more than a few weeks.Sudden changes in periods.Pain during sexNot being able to feel the threads (N.B. partial perforation may have occurred if the threads can still be seen – consider if severe pain following insertion).

Drug safety Update – July 15
Denosumab 60mg and 120mg or intravenous bisphosphonates: osteonecrosis of the jaw – further measures to minimise risk.Patient reminder cards are being introduced which should be provided before prescribing.Denosumab 120mg (RED – cancer indication) contraindicated in patients with unhealed lesions from dental or oral surgery.
Drug safety Update – July 15
For all patients, explain risk and advise on precautions to take: Tell doctor of any problems with mouth, teeth or
dentures. Maintain good oral hygiene. Inform doctor or dentist that receiving
denosumab or IV bisphosphonate if dental treatment or surgery needed.
Inform doctor or dentist if any problems during treatment e.g. loose teeth, pain, swelling, non-healing sores or discharge.
Drug safety Update – July 15
Xalatan (latanaprost): increased reporting of eye-irritation since reformulation.pH reduced in 2013 to allow long-term storage at room temperature.Increased reports of eye-irritation.Not an issue with the generic.
New Yellow card app for reporting suspected side-effectsFree, download via iTunes or PlayStore.
Drug safety Update – August 15
Simeprevir with sofosbuvir (used for hepatitis C): risk of severe bradycardia and heart block when taken with amiodaroneconcomitant use should be avoided unless other antiarrhythmics cannot be given due to a risk of severe bradycardia and heart block if taken together.Extension on previous advice on some combination therapies for hepatitis C.