Embed Size (px)
Citation preview

Hindawi Publishing CorporationISRN EndocrinologyVolume 2013 Article ID 385940 6 pageshttpdxdoiorg1011552013385940
Clinical StudyThryroid Hormones and Hematological Indices Levels inThyroid Disorders Patients at Moi Teaching and ReferralHospital Western Kenya
M A Iddah1 B N Macharia2 A G Ngrsquowena3 A Keter4 and A V O Ofulla1
1 Department of Biomedical Science and Technology Maseno University PO Box 333-40105 Maseno Kenya2Department of Human Pathology School of Medicine Moi University PO Box 4606-30100 Eldoret Kenya3Department of Medical Physiology School of Medicine Maseno University PO Box 333-40105 Maseno Kenya4Department of Research USAID-AMPATH Partnership PO Box 4606-30100 Eldoret Kenya
Correspondence should be addressed to M A Iddah iddahaligmailcom
Received 18 February 2013 Accepted 19 March 2013
Academic Editors Z Bouizar Z Canturk and W C Hymer
Copyright copy 2013 M A Iddah et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Problem Statement Thyroid disorders are prevalent in western Kenya but the effects of disorders on thyroid hormones andhematological indices levels have not been documented Study Population Patients treated for thyroid disorders at the MTRHbetween January 2008 and December 2011 Objectives To determine the thyroid hormones and hematological indices levels inthyroid disorders patients at the MTRH western Kenya Methodology A retrospective study in which patient data and storedsamples of patients who presented with thyroid pathologies underwent thyroidectomy and histological examinations are doneThyroid stimulating hormone (TSH) thyroxine (T
4) and triiodothyronine (T
3) blood levels white blood cells (WBCs) red
blood cells (RBCs) platelet counts and hemoglobin (Hb) levels were analyzed Results Male female ratio was 1 109 with femalerepresenting 368 (95) The median age was 41 (IQR 32ndash48) with a range of 14ndash89 years HHormonal levels for immunologicalthyroid disease patients were higher (119875 = 00232 0040) for TSH and (T
3) for those aged 30ndash39 years respectively The WBCs
RBCs HGB and platelets in immunological thyroid disease were not statistically significant with P values of 0547 0205 0291and 0488 respectively Conclusion The presence of anaemia due to low RBCs in thyroid disease is not significantly associated withthyroid hormone with a P value of 0512
1 Introduction
Thyroid hormones (THs) play an important physiologicalrole in humans THs may regulate human hematopoiesis inthe bonemarrow [1]The association of thyroid disorders andabnormalities in hematological parameters is well knownIn 1979 Fein showed that Gravesrsquo disease is associated withanemia [2] Horton observed a decreased number of redblood cells (RBCs) in the peripheral blood (PB) of patientsafter thyroidectomy [3] Hypothyroidism can cause certainforms of anemia on the one hand or hyperproliferation ofimmature erythroid progenitors on the other hand The ane-mia is usually macrocytic hypochromic anemia of moderateseverity [3] In contrast anemia is not frequently observedin patients with hyperthyroidism whereas erythrocytosis is
fairly common [2 4] It has been found that all hematologicalparameters return to normal when a euthyroid state isachieved [5] As far as white blood cells and thrombocytesare concerned a slightly depressed total leucocyte countneutropaenia and thrombocytopenia have been observed inhypothyroid patients [6] Furthermore elevated normal orslightly depressed total leucocyte counts have been found inhyperthyroid patients with only a relative decrease in thenumber of neutrophils and a relative increase in the numberof eosinophils and mononuclear cells (MNCs) Neverthelesshyperplasia of all myeloid cell lines in hyperthyroidism andtheir hypoplasia in hypothyroidismwere reported byAxelrod[7]
With regard to lymphocytes triiodothyronine (T3) has
been shown to be a prerequisite for normal B-cell production
2 ISRN Endocrinology
in the bone marrow through its regulation of pro-B-cell pro-liferation [8ndash10] These observations confirmed the associa-tion between thyroid gland dysfunction and haematopoiesisPreviously published studies suggested that there is an essen-tial relationship between the hypothyroid state and low levelsof iron vitamin B
12 and folic acid in the human body [3 11]
Furthermore it has been postulated that the influence ofTHs on haematopoiesis involves an increased production oferythropoietin or haematopoietic factors by non erythroidcells [12 13] However a growing number of studies havedemonstrated a direct role of THs in normal human andanimal erythropoiesis [1 14ndash17]
2 Material and Methods
21 Study Site and Design This research was carried out atMoi Teaching andReferralHospital EldoretThis is a hospitalthat serves clients from all over North Rift parts of westernKenya and Nyanza province
This was a retrospective study in which all patients withthyroid pathologies andwho underwent thyroidectomy at theMTRH between 2008 and 2011 were included
22 Study Methods Data on thyroid hormones and hemato-logical indices was obtained from the medical recordsClinical data was obtained from the hospital record files forpurposes of documenting the disease trends over the pastfour years (2008ndash2011)
23 Ethical Considerations Institution review ethics com-mittee (IREC) approval was obtained before starting datacollection Findings were discussed with the relevant healthprovider Information was provided in appropriately accessi-ble language
24 Thyroid Hormone Measurements Triiodothyronine hor-mone (T
3) thyroxine hormone (T
4) and thyroid stimulating
hormone (TSH) levels were measured using Enzyme LinkedImmunosorbent Assay (ELISA) for quantitative determina-tion of hormones concentration in human serumplasmausing the methods of Helenius [18] Whole blood sam-ples were collected through venipuncture centrifuged at3000 rpm and then frozen at minus20∘C for storage if to bemeasured later
25 Determination of Hematological Profile Hemoglobinconcentrationwas determined by a colorimetricmethodwiththe addition of a sample centrifugation (1600timesg 5min)before reading [19] Erythrocytes (red blood cells) and throm-bocytes were counted simultaneously in a Neubauer chamberusing the modified Daciersquos fluid with the addition of bril-liant blue cresyl [20] Mean corpuscular volume and meanconcentration of corpuscular hemoglobin were calculatedaccordingly using the methods of [21]
The leukocyte concentration (white blood cells (WBCs))was obtained through the counting of these cells in aNeubauer chamber using heparinized blood Because hep-arin causes leukocyte destruction in ostrich blood [22]
the WBC concentration was also indirectly determined bya method described previously [23] Briefly leucocytes anderythrocytes were counted separately along the smear upto a total of 2000 cells a ratio was determined and theWBCs concentration was indirectly calculated using the redblood cells count performed as described previously Thedifferential count of leukocytes was made in blood smearsstained with Diff-Quick
26 Statistical Analysis Data analysis was done using STATAversion 10 SE (College Station TX USA) Categorical var-iables were summarized as frequencies (percentage) whilethe continuous variables were summarized as median (inter-quartile range) Nonparametric test of equality of medianswas used to compare the medians of different groupsWilcoxon rank-sum test was used to test whether any twogroups came from populations with the same distributionThe age was categorized at the median The comparison ofthe proportions was done using the test of proportions Thecutoffs for anaemia were taken as Hb lt 13 gdL for male andHb lt 12 gdL for female patients not pregnant (httpenwikipediaorgwikiAnemia accessed on 15th August 2012 at1200 noon) Apparently our sample did not contain any preg-nant woman The cutoffs for low WBCs and low plateletswere WBCs lt 4 k120583L and platelets lt 150M120583L respective-ly The red blood cells (RBCs) cutoffs were RBCs lt45M120583L for male and RBCs lt 42M120583L for femaleThese cutoffs were obtained from httpwwwchemocarecommanaginglow blood countsasp accessed on 15thAugust 2012 at 1200 noon The elevated levels of the hor-mones T
3 T4 and TSH were based on the following cutoffs
T3gt 42 ngdL T
4gt 18 ngdL and TSH gt 50mIUL
3 Results
There were 388 subjects aged between 14ndash89 years who wereeligible for analysis and were categorized as having beendiagnosed with thyroid gland disorders autoimmune thyroiddisease or not
Male female ratio was 1 109 with female representing368 (95) The median age was 41 (IQR 32ndash48) with a rangeof 14ndash89 years There were 80 (284 95 confidence limits231ndash337) anemic patients (Hb lt 13 gdL if male and Hblt 12 gdL if female) with a median Hb value of 132 gdL(IQR 119ndash140) The absolute WBCs count was less than4 k120583L in 13 (122) of the patients with median value of55 k120583L (IQR 42ndash73) Thrombocytopenia was seen in 5(47) patients withmedian platelet count of 296times 103M120583LThere were 10 (94) patients and 35 (327) patients withlow RBC respectivelyThemedian RBCs were 46 (IQR 44ndash49) There were elevated T
3 T4 and TSH in 11 (103) 18
(168) and 9 (84) patients respectively Hormonal levelsfor immunological thyroid disease patients were higher (119875 =00232 0040) The significance is seen in thyroid stimulatinghormone levels (TSH) and triiodothyronine hormone (T
3)
only for those aged 30ndash39 years respectively The WBCsRBCs HGB and platelets among the immunological thyroid
ISRN Endocrinology 3
Table 1 Distribution of the demographic characteristics hormones and hematological properties among the immunological thyroid diseasepatients
OverallImmunological status Test for
differenceVariable Immunological NonimmunologicalSample size (119899) Median (Q1ndashQ3) Sample size (119899) Median (Q1ndashQ3) Sample size (119899) Median (Q1ndashQ3) 119875 values
Age 369 40 (33ndash50) 22 40 (32ndash54) 347 41 (32ndash50) 0787TSH 333 14 (07ndash25) 22 26 (109ndash36) 311 15 (07ndash26) 0323T3 319 167 (092ndash28) 21 26 (17ndash31) 298 14 (09ndash32) 0009T4 327 108 (07ndash17) 21 14 (10ndash20) 306 101 (07ndash18) 0181WBC 252 52 (41ndash70) 23 54 (42ndash85) 229 55 (44ndash75) 0547RBC 252 46 (44ndash48) 23 45 (44ndash47) 229 46 (44ndash48) 0205HB 252 131 (116ndash139) 23 125 (98ndash136) 259 132 (124ndash139) 0291Plat 260 292 (224ndash390) 22 3675 (2205ndash5225) 238 290 (2265ndash3655) 0488
Table 2 Relationship between thyroid disorder and hematological profiles among the male patients
Variable Sample size Median (IQR) Immunological(119899 = 9 45)
Nonimmunological(119899 = 11 55)
Wilcoxon rank-sum test(119875 value)
Age 19 52 (37ndash73) 49 (39ndash68) 62 (32ndash74) 0788TSH 17 12 (06ndash24) 16 (02ndash28) 11 (08ndash25) 0474T3 16 16 (05ndash35) 09 (01ndash38) 16 (13ndash33) 0657T4 16 06 (02ndash16) 07 (02ndash12) 05 (02ndash22) 0614Wbc 1 51 (45ndash62) 56 (48ndash61) 48 (44ndash62) 0782Rbc 11 48 (44ndash48) 46 (45ndash49) 48 (44ndash48) 0853Hb 13 134 (118ndash138) 131 (103ndash140) 134 (116ndash138) 0826Platelets 12 345 (264ndash365) 345 (278ndash365) 307 (262ndash415) 0621
disease patients were WBC 52 (41ndash70) RBC 46 (44ndash48) HGB 131 (116ndash139) and platelets 292 (224ndash390)respectively compared to the nonimmunological thyroid dis-ease patients However the differences were not statisticallysignificant with 119875 values of 0547 0205 0291 and 0488respectively There were 9 (45) immunological patientsamong themale patientsThe hematological profiles as well asthe age for the immunological patients were not significantlydifferent from those of the nonimmunological thyroid diseasepatients
Table 1 shows the overall distributions of age hormonesand hematological properties which are also stratified bywhether immunological thyroid disease is present or absentThe median test showed that there was only statisticallysignificant difference in T
3between the two groups of
patientsTable 2 shows the relationship between thyroid disor-
ders and hematological profiles among the male patientsThere were 9(45) immunological patients among the malepatients The hematological profiles as well as the age for theimmunological patients were not significantly different fromthose of the non-immunological thyroid disease patients(Table 2) This may be attributable to the small number ofmale patients in this study Further the autoimmune thyroiddisease is rare among the male population
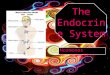
Figure 1 shows the thyroid stimulating hormone (TSH)levels of the subjects suffering from autoimmune thyroid
disease (Yes) and those not suffering from the autoimmunethyroid disease (No) stratified by age groups The TSHserum levels were high for those subjects suffering fromthe autoimmune thyroid disease across all the age groupsexcept for those aged 40ndash49 and 50ndash59 years However thedifferences were not statistically significant at 5 level ofsignificance except for those aged 30ndash39 years (119875 value =0023)
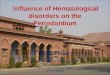
The triiodothyronine (T3) levels were high for those
subjects suffering from the autoimmune thyroid diseaseacross all the age groups except for those aged 40ndash49 and 50ndash59 years as shown in Figure 2 However the differences werenot statistically significant at 5 level of significance exceptfor those aged 30ndash39 years (119875 value = 0040)
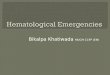
The thyroxine hormone (T4) levels were high for those
subjects suffering from the autoimmune thyroid diseaseacross all the age groups except for those aged 40ndash49 yearsas shown in Figure 3
The white blood cells and the red blood cells levels in thegroup suffering from autoimmune thyroid disease were lowsee Figure 4
The hemoglobin level of the subjects suffering fromimmunological thyroid disease was also low Figure 5 and thedifferences were not significant for the two groups (119875 value =0115)
The platelets levels were high for the subjects sufferingfrom the immunological thyroid disease (Figure 6) but these
4 ISRN Endocrinology
180
315
101
361
158128
252
198
103136
119875 value = 0506
119875 value = 0023
119875 value = 0535
119875 value = 0778
119875 value = 0734
0
1
2
3
4
No Yes No Yes No Yes No Yes No Yes
Med
ian
TSH
(mIU
L)
lt29 30ndash39 40ndash49 50ndash59 60gt
Figure 1 Thyroid stimulating hormone (TSH) levels among theimmunological thyroid disease patients
135
198
116
409
140170
273 256
206234
119875 value = 0525
119875 value = 0040
119875 value = 0885
119875 value = 0888119875 value = 0865
0
1
2
3
4
lt29No Yes No Yes No Yes No Yes No Yes
30ndash39 40ndash49 50ndash59 60gt
Med
ian
T3 (n
gdL
)
Figure 2 Triiodothyronine (T3) levels among the immunological
thyroid disease patients
differences were not statistically significant for the two groups(119875 value = 0313)
4 Discussion
Theanalyses for this study included all patients aged at least 14years who were undergoing thyroidectomy at Moi Teachingand Referral Hospital (MTRH) western Kenya between2008 and 2011 The primary outcome of interest was havingautoimmune thyroid disease (thyroiditis) The independentvariables were the demographic variables age and sex thethyroid hormones TSH T
3 and T
4 and hematological
profilesWe assessed the hematological profiles (WBCs RBCs
HGB and PLAT) in immunological thyroid disease patientsThe white blood cells and the red blood cells levels inthe group suffering from immunological thyroid diseasewere low Likewise the hemoglobin level of the subjectssuffering from immunological thyroid disease was low tooThe platelets levels were high for the subjects suffering fromthe autoimmune thyroid disease When the relationshipbetween thyroid disorders and hematological profile wasdetermined the hematological profiles as well as the age for
105
219
126148
092068
094116 118
200
119875 value = 0482
119875 value = 0341
119875 value = 0640119875 value = 0595
119875 value = 0062
0
05
1
15
2
No Yes No Yes No Yes No Yes No Yes
lt29 30ndash39 40ndash49 50ndash59 60gt
Med
ian
T4 (n
gdL
)
Figure 3Thyroxine hormone (T4) levels among the immunological
patients
555
461540
452
0
2
4
6
No Yes
WBC (119875 value = 0630)RBC (119875 value = 0376)
Med
ian
(per
litre
)
Figure 4 Levels of white blood cells and red blood cells for theimmunological thyroid disease patients
the immunological patients were not significantly differentfrom those of the nonimmunological thyroid disease patientsThis may be attributable to the small number of male patientsin this study Further the autoimmune thyroid disease is rareamong the male population Immunological conditions ofthose thyroid disorders are more common in females thanin males This explains the high number of females in thisstudy The disease is highly prevalent in females Male casesare few Apart from hormonal differences and cyclicity thephysiological roles of the thyroid gland are common in thetwo cases This explains why we included both sexes and notfemales alone The 5 of the males samples will not make adifference as seen from the analysis done
As far as the white blood cells and red blood cells countreduction are concerned this shows that the bone marrowis depressed and that thyroid hormones play an importantrole in the regulation of the human hematopoiesis in the bonemarrow This fact has also been shown to be evident in otherstudies [2] With regard to white blood cells triodothyronine(T3) hormone has been proven to be a prerequisite for
normal B-cell production in the bone marrow through itsregulation of pro-B-cell proliferation [8] The hemoglobin
ISRN Endocrinology 5
13201245
119875 value = 0115
0
5
10
15
No Yes
Med
ian
hem
oglo
bin
(gd
L)
Figure 5 Levels of hemoglobin for the immunological thyroiddisease patients
29000
36750119875 value = 0313
0
100
200
300
400
No Yes
Med
ian
plat
elet
s
Figure 6 Levels of platelets for the immunological patients units
level of the subjects suffering from immunological thyroidwas low too This clinically indicates a state of anemia Otherstudies have also shown that hypothyroidism causes anemiaor hyperproliferation of immature erythroid progenitors andthe anaemia is usually macrocytic hypochromic anaemia [3]The increase in the production of platelet can be attributedto the imbalance in the hematopoiesis which is a compen-satory mechanism [8] These observations have confirmedthe association between immunological thyroid disease andhematopoiesis and that hematological parameters are alteredin this condition Also it gives credence to the rejection ofour null hypothesis which states that hematological profilesin immunological thyroid diseases patients do not differ fromthose without immunological thyroid disease
5 Conclusion
The presence of anaemia in thyroid disease is associatedwith thyroid hormone Therefore thyroid hormones have asignificant influence on erythropoiesis The finding suggeststhat the molecular mechanism by which thyroid hormonesinfluence hematopoiesis may provide a basis for therapeuticintervention in thyroid diseases Immunological thyroid dis-ease patients tend to have higher levels of thyroid hormonalprofiles and low hematological profiles (WBCs RBCs andHB) though higher platelets compared to the nonimmuno-logical thyroid disease patients
References
[1] D W Golde N Bersch I J Chopra and M J Cline ldquoThyroidhormones stimulate erythropoiesis in vitrordquoThe British Journalof Haematology vol 37 no 2 pp 173ndash177 1977
[2] H G Fein and R S Rivlin ldquoAnemia in thyroid diseasesrdquoMedical Clinics of North America vol 59 no 5 pp 1133ndash11451975
[3] L Horton R J Coburn J M England and R L HimsworthldquoThe haematology of hypothyroidismrdquo Quarterly Journal ofMedicine vol 45 no 177 pp 101ndash123 1976
[4] R Corrocher M Querena A M Stanzial and G de SandreldquoMicrocytosis in hyperthyroidism haematological profile inthyroid disordersrdquo Haematologica vol 66 no 6 pp 779ndash7861981
[5] J A Perlman and P M Sternthal ldquoEffect of 131I on the anemiaof hyperthyroidismrdquo Journal of Chronic Diseases vol 36 no 5pp 405ndash412 1983
[6] C S P Lima D E Zantut Wittmann V Castro et al ldquoPancy-topenia in untreated patients with Gravesrsquo diseaserdquoThyroid vol16 no 4 pp 403ndash409 2006
[7] A R Axelrod and L Berman ldquoThe bone marrow in hyperthy-roidism and hypothyroidismrdquo Blood vol 6 no 5 pp 436ndash4531951
[8] M P Foster E Montecino-Rodriguez and K DorshkindldquoProliferation of bonemarrow pro-B cells is dependent on stim-ulation by the pituitarythyroid axisrdquo Journal of Immunologyvol 163 no 11 pp 5883ndash5890 1999
[9] C Arpin M Pihlgren A Fraichard et al ldquoEffects of T3R1205721and T3R1205722 gene deletion on T and B lymphocyte developmentrdquoJournal of Immunology vol 164 no 1 pp 152ndash160 2000
[10] KGrymuła E Paczkowska VDziedziejko et al ldquoThe influenceof 3310158405-triiodo-L-thyronine on human haematopoiesisrdquo CellProliferation vol 40 no 3 pp 302ndash315 2007
[11] J D Hines C H Halsted R C Griggs and J W HarrisldquoMegaloblastic anemia secondary to folate deficiency associatedwith hypothyroidismrdquo Annals of Internal Medicine vol 68 no4 pp 792ndash805 1968
[12] N Dainiak D Sutter and S Kreczko ldquoL-triiodothyronineaugments erythropoietic growth factor release from peripheralblood and bone marrow leukocytesrdquo Blood vol 68 no 6 pp1289ndash1297 1986
[13] J Fandrey H Pagel S Frede M Wolff and W JelkmannldquoThyroid hormones enhance hypoxia-induced erythropoietinproduction in vitrordquo Experimental Hematology vol 22 no 3pp 272ndash277 1994
[14] L A Malgor C C Blanc E Klainer et al ldquoDirect effects ofthyroid hormones on bone marrow erythroid cells of ratsrdquoBlood vol 45 no 5 pp 671ndash679 1975
[15] C Schroeder L Gibson M Zenke and H Beug ldquoModulationof normal erythroid differentiation by the endogenous thyroidhormone and retinoic acid receptors a possible target for v-erbA oncogene actionrdquoOncogene vol 7 no 2 pp 217ndash227 1992
[16] C Leberbauer F Boulme G Unfried J Huber H Beugand E W Mullner ldquoDifferent steroids co-regulate long-termexpansion versus terminal differentiation in primary humanerythroid progenitorsrdquo Blood vol 105 pp 85ndash94 2005
[17] M C Perrin J P Blanchet and G Mouchiroud ldquoModulationof human and mouse erythropoiesis by thyroid hormone andretinoic acid evidence for specific effects at different steps ofthe erythroid pathwayrdquo Hematology and Cell Therapy vol 39pp 19ndash26 1997
6 ISRN Endocrinology
[18] T Helenius and S Tikanoja ldquoA sensitive and practical immuno-radiometric assay of thyrotropinrdquo Clinical Chemistry vol 32no 3 pp 514ndash518 1986
[19] T W Campbell ldquoHematology of birdsrdquo in Veterinary Hema-tology and Clinical Chemistry M A Thrall Ed pp 225ndash258Lippincott Williams and Wilkins Philadelphia Pa USA 2004
[20] TW Campbell ldquoHematology of fishrdquo inVeterinary Hematologyand Clinical Chemistry M A Thrall Ed pp 277ndash290 Lippin-cott Williams ampWilkins Philadelphia Pa USA 2004
[21] N C JainEssentials ofHematology LeaampFebiger PhiladelphiaPa USA 1993
[22] R A Green and A Blue-McLendon ldquoRatite hematologyrdquo inPages in Schalmrsquos Veterinary Hematology pp 1201ndash1206 5thedition 2000
[23] M Tavares-Dias and F R Moraes ldquoHematological parametersfor the Brycon orbignyanus Valenciennes 1850 (OsteichthyesCharacidae) intensively bredrdquo Hidrobiologica vol 16 pp 271ndash274 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 ISRN Endocrinology
in the bone marrow through its regulation of pro-B-cell pro-liferation [8ndash10] These observations confirmed the associa-tion between thyroid gland dysfunction and haematopoiesisPreviously published studies suggested that there is an essen-tial relationship between the hypothyroid state and low levelsof iron vitamin B
12 and folic acid in the human body [3 11]
Furthermore it has been postulated that the influence ofTHs on haematopoiesis involves an increased production oferythropoietin or haematopoietic factors by non erythroidcells [12 13] However a growing number of studies havedemonstrated a direct role of THs in normal human andanimal erythropoiesis [1 14ndash17]
2 Material and Methods
21 Study Site and Design This research was carried out atMoi Teaching andReferralHospital EldoretThis is a hospitalthat serves clients from all over North Rift parts of westernKenya and Nyanza province
This was a retrospective study in which all patients withthyroid pathologies andwho underwent thyroidectomy at theMTRH between 2008 and 2011 were included
22 Study Methods Data on thyroid hormones and hemato-logical indices was obtained from the medical recordsClinical data was obtained from the hospital record files forpurposes of documenting the disease trends over the pastfour years (2008ndash2011)
23 Ethical Considerations Institution review ethics com-mittee (IREC) approval was obtained before starting datacollection Findings were discussed with the relevant healthprovider Information was provided in appropriately accessi-ble language
24 Thyroid Hormone Measurements Triiodothyronine hor-mone (T
3) thyroxine hormone (T
4) and thyroid stimulating
hormone (TSH) levels were measured using Enzyme LinkedImmunosorbent Assay (ELISA) for quantitative determina-tion of hormones concentration in human serumplasmausing the methods of Helenius [18] Whole blood sam-ples were collected through venipuncture centrifuged at3000 rpm and then frozen at minus20∘C for storage if to bemeasured later
25 Determination of Hematological Profile Hemoglobinconcentrationwas determined by a colorimetricmethodwiththe addition of a sample centrifugation (1600timesg 5min)before reading [19] Erythrocytes (red blood cells) and throm-bocytes were counted simultaneously in a Neubauer chamberusing the modified Daciersquos fluid with the addition of bril-liant blue cresyl [20] Mean corpuscular volume and meanconcentration of corpuscular hemoglobin were calculatedaccordingly using the methods of [21]
The leukocyte concentration (white blood cells (WBCs))was obtained through the counting of these cells in aNeubauer chamber using heparinized blood Because hep-arin causes leukocyte destruction in ostrich blood [22]
the WBC concentration was also indirectly determined bya method described previously [23] Briefly leucocytes anderythrocytes were counted separately along the smear upto a total of 2000 cells a ratio was determined and theWBCs concentration was indirectly calculated using the redblood cells count performed as described previously Thedifferential count of leukocytes was made in blood smearsstained with Diff-Quick
26 Statistical Analysis Data analysis was done using STATAversion 10 SE (College Station TX USA) Categorical var-iables were summarized as frequencies (percentage) whilethe continuous variables were summarized as median (inter-quartile range) Nonparametric test of equality of medianswas used to compare the medians of different groupsWilcoxon rank-sum test was used to test whether any twogroups came from populations with the same distributionThe age was categorized at the median The comparison ofthe proportions was done using the test of proportions Thecutoffs for anaemia were taken as Hb lt 13 gdL for male andHb lt 12 gdL for female patients not pregnant (httpenwikipediaorgwikiAnemia accessed on 15th August 2012 at1200 noon) Apparently our sample did not contain any preg-nant woman The cutoffs for low WBCs and low plateletswere WBCs lt 4 k120583L and platelets lt 150M120583L respective-ly The red blood cells (RBCs) cutoffs were RBCs lt45M120583L for male and RBCs lt 42M120583L for femaleThese cutoffs were obtained from httpwwwchemocarecommanaginglow blood countsasp accessed on 15thAugust 2012 at 1200 noon The elevated levels of the hor-mones T
3 T4 and TSH were based on the following cutoffs
T3gt 42 ngdL T
4gt 18 ngdL and TSH gt 50mIUL
3 Results
There were 388 subjects aged between 14ndash89 years who wereeligible for analysis and were categorized as having beendiagnosed with thyroid gland disorders autoimmune thyroiddisease or not
Male female ratio was 1 109 with female representing368 (95) The median age was 41 (IQR 32ndash48) with a rangeof 14ndash89 years There were 80 (284 95 confidence limits231ndash337) anemic patients (Hb lt 13 gdL if male and Hblt 12 gdL if female) with a median Hb value of 132 gdL(IQR 119ndash140) The absolute WBCs count was less than4 k120583L in 13 (122) of the patients with median value of55 k120583L (IQR 42ndash73) Thrombocytopenia was seen in 5(47) patients withmedian platelet count of 296times 103M120583LThere were 10 (94) patients and 35 (327) patients withlow RBC respectivelyThemedian RBCs were 46 (IQR 44ndash49) There were elevated T
3 T4 and TSH in 11 (103) 18
(168) and 9 (84) patients respectively Hormonal levelsfor immunological thyroid disease patients were higher (119875 =00232 0040) The significance is seen in thyroid stimulatinghormone levels (TSH) and triiodothyronine hormone (T
3)
only for those aged 30ndash39 years respectively The WBCsRBCs HGB and platelets among the immunological thyroid
ISRN Endocrinology 3
Table 1 Distribution of the demographic characteristics hormones and hematological properties among the immunological thyroid diseasepatients
OverallImmunological status Test for
differenceVariable Immunological NonimmunologicalSample size (119899) Median (Q1ndashQ3) Sample size (119899) Median (Q1ndashQ3) Sample size (119899) Median (Q1ndashQ3) 119875 values
Age 369 40 (33ndash50) 22 40 (32ndash54) 347 41 (32ndash50) 0787TSH 333 14 (07ndash25) 22 26 (109ndash36) 311 15 (07ndash26) 0323T3 319 167 (092ndash28) 21 26 (17ndash31) 298 14 (09ndash32) 0009T4 327 108 (07ndash17) 21 14 (10ndash20) 306 101 (07ndash18) 0181WBC 252 52 (41ndash70) 23 54 (42ndash85) 229 55 (44ndash75) 0547RBC 252 46 (44ndash48) 23 45 (44ndash47) 229 46 (44ndash48) 0205HB 252 131 (116ndash139) 23 125 (98ndash136) 259 132 (124ndash139) 0291Plat 260 292 (224ndash390) 22 3675 (2205ndash5225) 238 290 (2265ndash3655) 0488
Table 2 Relationship between thyroid disorder and hematological profiles among the male patients
Variable Sample size Median (IQR) Immunological(119899 = 9 45)
Nonimmunological(119899 = 11 55)
Wilcoxon rank-sum test(119875 value)
Age 19 52 (37ndash73) 49 (39ndash68) 62 (32ndash74) 0788TSH 17 12 (06ndash24) 16 (02ndash28) 11 (08ndash25) 0474T3 16 16 (05ndash35) 09 (01ndash38) 16 (13ndash33) 0657T4 16 06 (02ndash16) 07 (02ndash12) 05 (02ndash22) 0614Wbc 1 51 (45ndash62) 56 (48ndash61) 48 (44ndash62) 0782Rbc 11 48 (44ndash48) 46 (45ndash49) 48 (44ndash48) 0853Hb 13 134 (118ndash138) 131 (103ndash140) 134 (116ndash138) 0826Platelets 12 345 (264ndash365) 345 (278ndash365) 307 (262ndash415) 0621
disease patients were WBC 52 (41ndash70) RBC 46 (44ndash48) HGB 131 (116ndash139) and platelets 292 (224ndash390)respectively compared to the nonimmunological thyroid dis-ease patients However the differences were not statisticallysignificant with 119875 values of 0547 0205 0291 and 0488respectively There were 9 (45) immunological patientsamong themale patientsThe hematological profiles as well asthe age for the immunological patients were not significantlydifferent from those of the nonimmunological thyroid diseasepatients
Table 1 shows the overall distributions of age hormonesand hematological properties which are also stratified bywhether immunological thyroid disease is present or absentThe median test showed that there was only statisticallysignificant difference in T
3between the two groups of
patientsTable 2 shows the relationship between thyroid disor-
ders and hematological profiles among the male patientsThere were 9(45) immunological patients among the malepatients The hematological profiles as well as the age for theimmunological patients were not significantly different fromthose of the non-immunological thyroid disease patients(Table 2) This may be attributable to the small number ofmale patients in this study Further the autoimmune thyroiddisease is rare among the male population
Figure 1 shows the thyroid stimulating hormone (TSH)levels of the subjects suffering from autoimmune thyroid
disease (Yes) and those not suffering from the autoimmunethyroid disease (No) stratified by age groups The TSHserum levels were high for those subjects suffering fromthe autoimmune thyroid disease across all the age groupsexcept for those aged 40ndash49 and 50ndash59 years However thedifferences were not statistically significant at 5 level ofsignificance except for those aged 30ndash39 years (119875 value =0023)
The triiodothyronine (T3) levels were high for those
subjects suffering from the autoimmune thyroid diseaseacross all the age groups except for those aged 40ndash49 and 50ndash59 years as shown in Figure 2 However the differences werenot statistically significant at 5 level of significance exceptfor those aged 30ndash39 years (119875 value = 0040)
The thyroxine hormone (T4) levels were high for those
subjects suffering from the autoimmune thyroid diseaseacross all the age groups except for those aged 40ndash49 yearsas shown in Figure 3
The white blood cells and the red blood cells levels in thegroup suffering from autoimmune thyroid disease were lowsee Figure 4
The hemoglobin level of the subjects suffering fromimmunological thyroid disease was also low Figure 5 and thedifferences were not significant for the two groups (119875 value =0115)
The platelets levels were high for the subjects sufferingfrom the immunological thyroid disease (Figure 6) but these
4 ISRN Endocrinology
180
315
101
361
158128
252
198
103136
119875 value = 0506
119875 value = 0023
119875 value = 0535
119875 value = 0778
119875 value = 0734
0
1
2
3
4
No Yes No Yes No Yes No Yes No Yes
Med
ian
TSH
(mIU
L)
lt29 30ndash39 40ndash49 50ndash59 60gt
Figure 1 Thyroid stimulating hormone (TSH) levels among theimmunological thyroid disease patients
135
198
116
409
140170
273 256
206234
119875 value = 0525
119875 value = 0040
119875 value = 0885
119875 value = 0888119875 value = 0865
0
1
2
3
4
lt29No Yes No Yes No Yes No Yes No Yes
30ndash39 40ndash49 50ndash59 60gt
Med
ian
T3 (n
gdL
)
Figure 2 Triiodothyronine (T3) levels among the immunological
thyroid disease patients
differences were not statistically significant for the two groups(119875 value = 0313)
4 Discussion
Theanalyses for this study included all patients aged at least 14years who were undergoing thyroidectomy at Moi Teachingand Referral Hospital (MTRH) western Kenya between2008 and 2011 The primary outcome of interest was havingautoimmune thyroid disease (thyroiditis) The independentvariables were the demographic variables age and sex thethyroid hormones TSH T
3 and T
4 and hematological
profilesWe assessed the hematological profiles (WBCs RBCs
HGB and PLAT) in immunological thyroid disease patientsThe white blood cells and the red blood cells levels inthe group suffering from immunological thyroid diseasewere low Likewise the hemoglobin level of the subjectssuffering from immunological thyroid disease was low tooThe platelets levels were high for the subjects suffering fromthe autoimmune thyroid disease When the relationshipbetween thyroid disorders and hematological profile wasdetermined the hematological profiles as well as the age for
105
219
126148
092068
094116 118
200
119875 value = 0482
119875 value = 0341
119875 value = 0640119875 value = 0595
119875 value = 0062
0
05
1
15
2
No Yes No Yes No Yes No Yes No Yes
lt29 30ndash39 40ndash49 50ndash59 60gt
Med
ian
T4 (n
gdL
)
Figure 3Thyroxine hormone (T4) levels among the immunological
patients
555
461540
452
0
2
4
6
No Yes
WBC (119875 value = 0630)RBC (119875 value = 0376)
Med
ian
(per
litre
)
Figure 4 Levels of white blood cells and red blood cells for theimmunological thyroid disease patients
the immunological patients were not significantly differentfrom those of the nonimmunological thyroid disease patientsThis may be attributable to the small number of male patientsin this study Further the autoimmune thyroid disease is rareamong the male population Immunological conditions ofthose thyroid disorders are more common in females thanin males This explains the high number of females in thisstudy The disease is highly prevalent in females Male casesare few Apart from hormonal differences and cyclicity thephysiological roles of the thyroid gland are common in thetwo cases This explains why we included both sexes and notfemales alone The 5 of the males samples will not make adifference as seen from the analysis done
As far as the white blood cells and red blood cells countreduction are concerned this shows that the bone marrowis depressed and that thyroid hormones play an importantrole in the regulation of the human hematopoiesis in the bonemarrow This fact has also been shown to be evident in otherstudies [2] With regard to white blood cells triodothyronine(T3) hormone has been proven to be a prerequisite for
normal B-cell production in the bone marrow through itsregulation of pro-B-cell proliferation [8] The hemoglobin
ISRN Endocrinology 5
13201245
119875 value = 0115
0
5
10
15
No Yes
Med
ian
hem
oglo
bin
(gd
L)
Figure 5 Levels of hemoglobin for the immunological thyroiddisease patients
29000
36750119875 value = 0313
0
100
200
300
400
No Yes
Med
ian
plat
elet
s
Figure 6 Levels of platelets for the immunological patients units
level of the subjects suffering from immunological thyroidwas low too This clinically indicates a state of anemia Otherstudies have also shown that hypothyroidism causes anemiaor hyperproliferation of immature erythroid progenitors andthe anaemia is usually macrocytic hypochromic anaemia [3]The increase in the production of platelet can be attributedto the imbalance in the hematopoiesis which is a compen-satory mechanism [8] These observations have confirmedthe association between immunological thyroid disease andhematopoiesis and that hematological parameters are alteredin this condition Also it gives credence to the rejection ofour null hypothesis which states that hematological profilesin immunological thyroid diseases patients do not differ fromthose without immunological thyroid disease
5 Conclusion
The presence of anaemia in thyroid disease is associatedwith thyroid hormone Therefore thyroid hormones have asignificant influence on erythropoiesis The finding suggeststhat the molecular mechanism by which thyroid hormonesinfluence hematopoiesis may provide a basis for therapeuticintervention in thyroid diseases Immunological thyroid dis-ease patients tend to have higher levels of thyroid hormonalprofiles and low hematological profiles (WBCs RBCs andHB) though higher platelets compared to the nonimmuno-logical thyroid disease patients
References
[1] D W Golde N Bersch I J Chopra and M J Cline ldquoThyroidhormones stimulate erythropoiesis in vitrordquoThe British Journalof Haematology vol 37 no 2 pp 173ndash177 1977
[2] H G Fein and R S Rivlin ldquoAnemia in thyroid diseasesrdquoMedical Clinics of North America vol 59 no 5 pp 1133ndash11451975
[3] L Horton R J Coburn J M England and R L HimsworthldquoThe haematology of hypothyroidismrdquo Quarterly Journal ofMedicine vol 45 no 177 pp 101ndash123 1976
[4] R Corrocher M Querena A M Stanzial and G de SandreldquoMicrocytosis in hyperthyroidism haematological profile inthyroid disordersrdquo Haematologica vol 66 no 6 pp 779ndash7861981
[5] J A Perlman and P M Sternthal ldquoEffect of 131I on the anemiaof hyperthyroidismrdquo Journal of Chronic Diseases vol 36 no 5pp 405ndash412 1983
[6] C S P Lima D E Zantut Wittmann V Castro et al ldquoPancy-topenia in untreated patients with Gravesrsquo diseaserdquoThyroid vol16 no 4 pp 403ndash409 2006
[7] A R Axelrod and L Berman ldquoThe bone marrow in hyperthy-roidism and hypothyroidismrdquo Blood vol 6 no 5 pp 436ndash4531951
[8] M P Foster E Montecino-Rodriguez and K DorshkindldquoProliferation of bonemarrow pro-B cells is dependent on stim-ulation by the pituitarythyroid axisrdquo Journal of Immunologyvol 163 no 11 pp 5883ndash5890 1999
[9] C Arpin M Pihlgren A Fraichard et al ldquoEffects of T3R1205721and T3R1205722 gene deletion on T and B lymphocyte developmentrdquoJournal of Immunology vol 164 no 1 pp 152ndash160 2000
[10] KGrymuła E Paczkowska VDziedziejko et al ldquoThe influenceof 3310158405-triiodo-L-thyronine on human haematopoiesisrdquo CellProliferation vol 40 no 3 pp 302ndash315 2007
[11] J D Hines C H Halsted R C Griggs and J W HarrisldquoMegaloblastic anemia secondary to folate deficiency associatedwith hypothyroidismrdquo Annals of Internal Medicine vol 68 no4 pp 792ndash805 1968
[12] N Dainiak D Sutter and S Kreczko ldquoL-triiodothyronineaugments erythropoietic growth factor release from peripheralblood and bone marrow leukocytesrdquo Blood vol 68 no 6 pp1289ndash1297 1986
[13] J Fandrey H Pagel S Frede M Wolff and W JelkmannldquoThyroid hormones enhance hypoxia-induced erythropoietinproduction in vitrordquo Experimental Hematology vol 22 no 3pp 272ndash277 1994
[14] L A Malgor C C Blanc E Klainer et al ldquoDirect effects ofthyroid hormones on bone marrow erythroid cells of ratsrdquoBlood vol 45 no 5 pp 671ndash679 1975
[15] C Schroeder L Gibson M Zenke and H Beug ldquoModulationof normal erythroid differentiation by the endogenous thyroidhormone and retinoic acid receptors a possible target for v-erbA oncogene actionrdquoOncogene vol 7 no 2 pp 217ndash227 1992
[16] C Leberbauer F Boulme G Unfried J Huber H Beugand E W Mullner ldquoDifferent steroids co-regulate long-termexpansion versus terminal differentiation in primary humanerythroid progenitorsrdquo Blood vol 105 pp 85ndash94 2005
[17] M C Perrin J P Blanchet and G Mouchiroud ldquoModulationof human and mouse erythropoiesis by thyroid hormone andretinoic acid evidence for specific effects at different steps ofthe erythroid pathwayrdquo Hematology and Cell Therapy vol 39pp 19ndash26 1997
6 ISRN Endocrinology
[18] T Helenius and S Tikanoja ldquoA sensitive and practical immuno-radiometric assay of thyrotropinrdquo Clinical Chemistry vol 32no 3 pp 514ndash518 1986
[19] T W Campbell ldquoHematology of birdsrdquo in Veterinary Hema-tology and Clinical Chemistry M A Thrall Ed pp 225ndash258Lippincott Williams and Wilkins Philadelphia Pa USA 2004
[20] TW Campbell ldquoHematology of fishrdquo inVeterinary Hematologyand Clinical Chemistry M A Thrall Ed pp 277ndash290 Lippin-cott Williams ampWilkins Philadelphia Pa USA 2004
[21] N C JainEssentials ofHematology LeaampFebiger PhiladelphiaPa USA 1993
[22] R A Green and A Blue-McLendon ldquoRatite hematologyrdquo inPages in Schalmrsquos Veterinary Hematology pp 1201ndash1206 5thedition 2000
[23] M Tavares-Dias and F R Moraes ldquoHematological parametersfor the Brycon orbignyanus Valenciennes 1850 (OsteichthyesCharacidae) intensively bredrdquo Hidrobiologica vol 16 pp 271ndash274 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

ISRN Endocrinology 3
Table 1 Distribution of the demographic characteristics hormones and hematological properties among the immunological thyroid diseasepatients
OverallImmunological status Test for
differenceVariable Immunological NonimmunologicalSample size (119899) Median (Q1ndashQ3) Sample size (119899) Median (Q1ndashQ3) Sample size (119899) Median (Q1ndashQ3) 119875 values
Age 369 40 (33ndash50) 22 40 (32ndash54) 347 41 (32ndash50) 0787TSH 333 14 (07ndash25) 22 26 (109ndash36) 311 15 (07ndash26) 0323T3 319 167 (092ndash28) 21 26 (17ndash31) 298 14 (09ndash32) 0009T4 327 108 (07ndash17) 21 14 (10ndash20) 306 101 (07ndash18) 0181WBC 252 52 (41ndash70) 23 54 (42ndash85) 229 55 (44ndash75) 0547RBC 252 46 (44ndash48) 23 45 (44ndash47) 229 46 (44ndash48) 0205HB 252 131 (116ndash139) 23 125 (98ndash136) 259 132 (124ndash139) 0291Plat 260 292 (224ndash390) 22 3675 (2205ndash5225) 238 290 (2265ndash3655) 0488
Table 2 Relationship between thyroid disorder and hematological profiles among the male patients
Variable Sample size Median (IQR) Immunological(119899 = 9 45)
Nonimmunological(119899 = 11 55)
Wilcoxon rank-sum test(119875 value)
Age 19 52 (37ndash73) 49 (39ndash68) 62 (32ndash74) 0788TSH 17 12 (06ndash24) 16 (02ndash28) 11 (08ndash25) 0474T3 16 16 (05ndash35) 09 (01ndash38) 16 (13ndash33) 0657T4 16 06 (02ndash16) 07 (02ndash12) 05 (02ndash22) 0614Wbc 1 51 (45ndash62) 56 (48ndash61) 48 (44ndash62) 0782Rbc 11 48 (44ndash48) 46 (45ndash49) 48 (44ndash48) 0853Hb 13 134 (118ndash138) 131 (103ndash140) 134 (116ndash138) 0826Platelets 12 345 (264ndash365) 345 (278ndash365) 307 (262ndash415) 0621
disease patients were WBC 52 (41ndash70) RBC 46 (44ndash48) HGB 131 (116ndash139) and platelets 292 (224ndash390)respectively compared to the nonimmunological thyroid dis-ease patients However the differences were not statisticallysignificant with 119875 values of 0547 0205 0291 and 0488respectively There were 9 (45) immunological patientsamong themale patientsThe hematological profiles as well asthe age for the immunological patients were not significantlydifferent from those of the nonimmunological thyroid diseasepatients
Table 1 shows the overall distributions of age hormonesand hematological properties which are also stratified bywhether immunological thyroid disease is present or absentThe median test showed that there was only statisticallysignificant difference in T
3between the two groups of
patientsTable 2 shows the relationship between thyroid disor-
ders and hematological profiles among the male patientsThere were 9(45) immunological patients among the malepatients The hematological profiles as well as the age for theimmunological patients were not significantly different fromthose of the non-immunological thyroid disease patients(Table 2) This may be attributable to the small number ofmale patients in this study Further the autoimmune thyroiddisease is rare among the male population
Figure 1 shows the thyroid stimulating hormone (TSH)levels of the subjects suffering from autoimmune thyroid
disease (Yes) and those not suffering from the autoimmunethyroid disease (No) stratified by age groups The TSHserum levels were high for those subjects suffering fromthe autoimmune thyroid disease across all the age groupsexcept for those aged 40ndash49 and 50ndash59 years However thedifferences were not statistically significant at 5 level ofsignificance except for those aged 30ndash39 years (119875 value =0023)
The triiodothyronine (T3) levels were high for those
subjects suffering from the autoimmune thyroid diseaseacross all the age groups except for those aged 40ndash49 and 50ndash59 years as shown in Figure 2 However the differences werenot statistically significant at 5 level of significance exceptfor those aged 30ndash39 years (119875 value = 0040)
The thyroxine hormone (T4) levels were high for those
subjects suffering from the autoimmune thyroid diseaseacross all the age groups except for those aged 40ndash49 yearsas shown in Figure 3
The white blood cells and the red blood cells levels in thegroup suffering from autoimmune thyroid disease were lowsee Figure 4
The hemoglobin level of the subjects suffering fromimmunological thyroid disease was also low Figure 5 and thedifferences were not significant for the two groups (119875 value =0115)
The platelets levels were high for the subjects sufferingfrom the immunological thyroid disease (Figure 6) but these
4 ISRN Endocrinology
180
315
101
361
158128
252
198
103136
119875 value = 0506
119875 value = 0023
119875 value = 0535
119875 value = 0778
119875 value = 0734
0
1
2
3
4
No Yes No Yes No Yes No Yes No Yes
Med
ian
TSH
(mIU
L)
lt29 30ndash39 40ndash49 50ndash59 60gt
Figure 1 Thyroid stimulating hormone (TSH) levels among theimmunological thyroid disease patients
135
198
116
409
140170
273 256
206234
119875 value = 0525
119875 value = 0040
119875 value = 0885
119875 value = 0888119875 value = 0865
0
1
2
3
4
lt29No Yes No Yes No Yes No Yes No Yes
30ndash39 40ndash49 50ndash59 60gt
Med
ian
T3 (n
gdL
)
Figure 2 Triiodothyronine (T3) levels among the immunological
thyroid disease patients
differences were not statistically significant for the two groups(119875 value = 0313)
4 Discussion
Theanalyses for this study included all patients aged at least 14years who were undergoing thyroidectomy at Moi Teachingand Referral Hospital (MTRH) western Kenya between2008 and 2011 The primary outcome of interest was havingautoimmune thyroid disease (thyroiditis) The independentvariables were the demographic variables age and sex thethyroid hormones TSH T
3 and T
4 and hematological
profilesWe assessed the hematological profiles (WBCs RBCs
HGB and PLAT) in immunological thyroid disease patientsThe white blood cells and the red blood cells levels inthe group suffering from immunological thyroid diseasewere low Likewise the hemoglobin level of the subjectssuffering from immunological thyroid disease was low tooThe platelets levels were high for the subjects suffering fromthe autoimmune thyroid disease When the relationshipbetween thyroid disorders and hematological profile wasdetermined the hematological profiles as well as the age for
105
219
126148
092068
094116 118
200
119875 value = 0482
119875 value = 0341
119875 value = 0640119875 value = 0595
119875 value = 0062
0
05
1
15
2
No Yes No Yes No Yes No Yes No Yes
lt29 30ndash39 40ndash49 50ndash59 60gt
Med
ian
T4 (n
gdL
)
Figure 3Thyroxine hormone (T4) levels among the immunological
patients
555
461540
452
0
2
4
6
No Yes
WBC (119875 value = 0630)RBC (119875 value = 0376)
Med
ian
(per
litre
)
Figure 4 Levels of white blood cells and red blood cells for theimmunological thyroid disease patients
the immunological patients were not significantly differentfrom those of the nonimmunological thyroid disease patientsThis may be attributable to the small number of male patientsin this study Further the autoimmune thyroid disease is rareamong the male population Immunological conditions ofthose thyroid disorders are more common in females thanin males This explains the high number of females in thisstudy The disease is highly prevalent in females Male casesare few Apart from hormonal differences and cyclicity thephysiological roles of the thyroid gland are common in thetwo cases This explains why we included both sexes and notfemales alone The 5 of the males samples will not make adifference as seen from the analysis done
As far as the white blood cells and red blood cells countreduction are concerned this shows that the bone marrowis depressed and that thyroid hormones play an importantrole in the regulation of the human hematopoiesis in the bonemarrow This fact has also been shown to be evident in otherstudies [2] With regard to white blood cells triodothyronine(T3) hormone has been proven to be a prerequisite for
normal B-cell production in the bone marrow through itsregulation of pro-B-cell proliferation [8] The hemoglobin
ISRN Endocrinology 5
13201245
119875 value = 0115
0
5
10
15
No Yes
Med
ian
hem
oglo
bin
(gd
L)
Figure 5 Levels of hemoglobin for the immunological thyroiddisease patients
29000
36750119875 value = 0313
0
100
200
300
400
No Yes
Med
ian
plat
elet
s
Figure 6 Levels of platelets for the immunological patients units
level of the subjects suffering from immunological thyroidwas low too This clinically indicates a state of anemia Otherstudies have also shown that hypothyroidism causes anemiaor hyperproliferation of immature erythroid progenitors andthe anaemia is usually macrocytic hypochromic anaemia [3]The increase in the production of platelet can be attributedto the imbalance in the hematopoiesis which is a compen-satory mechanism [8] These observations have confirmedthe association between immunological thyroid disease andhematopoiesis and that hematological parameters are alteredin this condition Also it gives credence to the rejection ofour null hypothesis which states that hematological profilesin immunological thyroid diseases patients do not differ fromthose without immunological thyroid disease
5 Conclusion
The presence of anaemia in thyroid disease is associatedwith thyroid hormone Therefore thyroid hormones have asignificant influence on erythropoiesis The finding suggeststhat the molecular mechanism by which thyroid hormonesinfluence hematopoiesis may provide a basis for therapeuticintervention in thyroid diseases Immunological thyroid dis-ease patients tend to have higher levels of thyroid hormonalprofiles and low hematological profiles (WBCs RBCs andHB) though higher platelets compared to the nonimmuno-logical thyroid disease patients
References
[1] D W Golde N Bersch I J Chopra and M J Cline ldquoThyroidhormones stimulate erythropoiesis in vitrordquoThe British Journalof Haematology vol 37 no 2 pp 173ndash177 1977
[2] H G Fein and R S Rivlin ldquoAnemia in thyroid diseasesrdquoMedical Clinics of North America vol 59 no 5 pp 1133ndash11451975
[3] L Horton R J Coburn J M England and R L HimsworthldquoThe haematology of hypothyroidismrdquo Quarterly Journal ofMedicine vol 45 no 177 pp 101ndash123 1976
[4] R Corrocher M Querena A M Stanzial and G de SandreldquoMicrocytosis in hyperthyroidism haematological profile inthyroid disordersrdquo Haematologica vol 66 no 6 pp 779ndash7861981
[5] J A Perlman and P M Sternthal ldquoEffect of 131I on the anemiaof hyperthyroidismrdquo Journal of Chronic Diseases vol 36 no 5pp 405ndash412 1983
[6] C S P Lima D E Zantut Wittmann V Castro et al ldquoPancy-topenia in untreated patients with Gravesrsquo diseaserdquoThyroid vol16 no 4 pp 403ndash409 2006
[7] A R Axelrod and L Berman ldquoThe bone marrow in hyperthy-roidism and hypothyroidismrdquo Blood vol 6 no 5 pp 436ndash4531951
[8] M P Foster E Montecino-Rodriguez and K DorshkindldquoProliferation of bonemarrow pro-B cells is dependent on stim-ulation by the pituitarythyroid axisrdquo Journal of Immunologyvol 163 no 11 pp 5883ndash5890 1999
[9] C Arpin M Pihlgren A Fraichard et al ldquoEffects of T3R1205721and T3R1205722 gene deletion on T and B lymphocyte developmentrdquoJournal of Immunology vol 164 no 1 pp 152ndash160 2000
[10] KGrymuła E Paczkowska VDziedziejko et al ldquoThe influenceof 3310158405-triiodo-L-thyronine on human haematopoiesisrdquo CellProliferation vol 40 no 3 pp 302ndash315 2007
[11] J D Hines C H Halsted R C Griggs and J W HarrisldquoMegaloblastic anemia secondary to folate deficiency associatedwith hypothyroidismrdquo Annals of Internal Medicine vol 68 no4 pp 792ndash805 1968
[12] N Dainiak D Sutter and S Kreczko ldquoL-triiodothyronineaugments erythropoietic growth factor release from peripheralblood and bone marrow leukocytesrdquo Blood vol 68 no 6 pp1289ndash1297 1986
[13] J Fandrey H Pagel S Frede M Wolff and W JelkmannldquoThyroid hormones enhance hypoxia-induced erythropoietinproduction in vitrordquo Experimental Hematology vol 22 no 3pp 272ndash277 1994
[14] L A Malgor C C Blanc E Klainer et al ldquoDirect effects ofthyroid hormones on bone marrow erythroid cells of ratsrdquoBlood vol 45 no 5 pp 671ndash679 1975
[15] C Schroeder L Gibson M Zenke and H Beug ldquoModulationof normal erythroid differentiation by the endogenous thyroidhormone and retinoic acid receptors a possible target for v-erbA oncogene actionrdquoOncogene vol 7 no 2 pp 217ndash227 1992
[16] C Leberbauer F Boulme G Unfried J Huber H Beugand E W Mullner ldquoDifferent steroids co-regulate long-termexpansion versus terminal differentiation in primary humanerythroid progenitorsrdquo Blood vol 105 pp 85ndash94 2005
[17] M C Perrin J P Blanchet and G Mouchiroud ldquoModulationof human and mouse erythropoiesis by thyroid hormone andretinoic acid evidence for specific effects at different steps ofthe erythroid pathwayrdquo Hematology and Cell Therapy vol 39pp 19ndash26 1997
6 ISRN Endocrinology
[18] T Helenius and S Tikanoja ldquoA sensitive and practical immuno-radiometric assay of thyrotropinrdquo Clinical Chemistry vol 32no 3 pp 514ndash518 1986
[19] T W Campbell ldquoHematology of birdsrdquo in Veterinary Hema-tology and Clinical Chemistry M A Thrall Ed pp 225ndash258Lippincott Williams and Wilkins Philadelphia Pa USA 2004
[20] TW Campbell ldquoHematology of fishrdquo inVeterinary Hematologyand Clinical Chemistry M A Thrall Ed pp 277ndash290 Lippin-cott Williams ampWilkins Philadelphia Pa USA 2004
[21] N C JainEssentials ofHematology LeaampFebiger PhiladelphiaPa USA 1993
[22] R A Green and A Blue-McLendon ldquoRatite hematologyrdquo inPages in Schalmrsquos Veterinary Hematology pp 1201ndash1206 5thedition 2000
[23] M Tavares-Dias and F R Moraes ldquoHematological parametersfor the Brycon orbignyanus Valenciennes 1850 (OsteichthyesCharacidae) intensively bredrdquo Hidrobiologica vol 16 pp 271ndash274 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 ISRN Endocrinology
180
315
101
361
158128
252
198
103136
119875 value = 0506
119875 value = 0023
119875 value = 0535
119875 value = 0778
119875 value = 0734
0
1
2
3
4
No Yes No Yes No Yes No Yes No Yes
Med
ian
TSH
(mIU
L)
lt29 30ndash39 40ndash49 50ndash59 60gt
Figure 1 Thyroid stimulating hormone (TSH) levels among theimmunological thyroid disease patients
135
198
116
409
140170
273 256
206234
119875 value = 0525
119875 value = 0040
119875 value = 0885
119875 value = 0888119875 value = 0865
0
1
2
3
4
lt29No Yes No Yes No Yes No Yes No Yes
30ndash39 40ndash49 50ndash59 60gt
Med
ian
T3 (n
gdL
)
Figure 2 Triiodothyronine (T3) levels among the immunological
thyroid disease patients
differences were not statistically significant for the two groups(119875 value = 0313)
4 Discussion
Theanalyses for this study included all patients aged at least 14years who were undergoing thyroidectomy at Moi Teachingand Referral Hospital (MTRH) western Kenya between2008 and 2011 The primary outcome of interest was havingautoimmune thyroid disease (thyroiditis) The independentvariables were the demographic variables age and sex thethyroid hormones TSH T
3 and T
4 and hematological
profilesWe assessed the hematological profiles (WBCs RBCs
HGB and PLAT) in immunological thyroid disease patientsThe white blood cells and the red blood cells levels inthe group suffering from immunological thyroid diseasewere low Likewise the hemoglobin level of the subjectssuffering from immunological thyroid disease was low tooThe platelets levels were high for the subjects suffering fromthe autoimmune thyroid disease When the relationshipbetween thyroid disorders and hematological profile wasdetermined the hematological profiles as well as the age for
105
219
126148
092068
094116 118
200
119875 value = 0482
119875 value = 0341
119875 value = 0640119875 value = 0595
119875 value = 0062
0
05
1
15
2
No Yes No Yes No Yes No Yes No Yes
lt29 30ndash39 40ndash49 50ndash59 60gt
Med
ian
T4 (n
gdL
)
Figure 3Thyroxine hormone (T4) levels among the immunological
patients
555
461540
452
0
2
4
6
No Yes
WBC (119875 value = 0630)RBC (119875 value = 0376)
Med
ian
(per
litre
)
Figure 4 Levels of white blood cells and red blood cells for theimmunological thyroid disease patients
the immunological patients were not significantly differentfrom those of the nonimmunological thyroid disease patientsThis may be attributable to the small number of male patientsin this study Further the autoimmune thyroid disease is rareamong the male population Immunological conditions ofthose thyroid disorders are more common in females thanin males This explains the high number of females in thisstudy The disease is highly prevalent in females Male casesare few Apart from hormonal differences and cyclicity thephysiological roles of the thyroid gland are common in thetwo cases This explains why we included both sexes and notfemales alone The 5 of the males samples will not make adifference as seen from the analysis done
As far as the white blood cells and red blood cells countreduction are concerned this shows that the bone marrowis depressed and that thyroid hormones play an importantrole in the regulation of the human hematopoiesis in the bonemarrow This fact has also been shown to be evident in otherstudies [2] With regard to white blood cells triodothyronine(T3) hormone has been proven to be a prerequisite for
normal B-cell production in the bone marrow through itsregulation of pro-B-cell proliferation [8] The hemoglobin
ISRN Endocrinology 5
13201245
119875 value = 0115
0
5
10
15
No Yes
Med
ian
hem
oglo
bin
(gd
L)
Figure 5 Levels of hemoglobin for the immunological thyroiddisease patients
29000
36750119875 value = 0313
0
100
200
300
400
No Yes
Med
ian
plat
elet
s
Figure 6 Levels of platelets for the immunological patients units
level of the subjects suffering from immunological thyroidwas low too This clinically indicates a state of anemia Otherstudies have also shown that hypothyroidism causes anemiaor hyperproliferation of immature erythroid progenitors andthe anaemia is usually macrocytic hypochromic anaemia [3]The increase in the production of platelet can be attributedto the imbalance in the hematopoiesis which is a compen-satory mechanism [8] These observations have confirmedthe association between immunological thyroid disease andhematopoiesis and that hematological parameters are alteredin this condition Also it gives credence to the rejection ofour null hypothesis which states that hematological profilesin immunological thyroid diseases patients do not differ fromthose without immunological thyroid disease
5 Conclusion
The presence of anaemia in thyroid disease is associatedwith thyroid hormone Therefore thyroid hormones have asignificant influence on erythropoiesis The finding suggeststhat the molecular mechanism by which thyroid hormonesinfluence hematopoiesis may provide a basis for therapeuticintervention in thyroid diseases Immunological thyroid dis-ease patients tend to have higher levels of thyroid hormonalprofiles and low hematological profiles (WBCs RBCs andHB) though higher platelets compared to the nonimmuno-logical thyroid disease patients
References
[1] D W Golde N Bersch I J Chopra and M J Cline ldquoThyroidhormones stimulate erythropoiesis in vitrordquoThe British Journalof Haematology vol 37 no 2 pp 173ndash177 1977
[2] H G Fein and R S Rivlin ldquoAnemia in thyroid diseasesrdquoMedical Clinics of North America vol 59 no 5 pp 1133ndash11451975
[3] L Horton R J Coburn J M England and R L HimsworthldquoThe haematology of hypothyroidismrdquo Quarterly Journal ofMedicine vol 45 no 177 pp 101ndash123 1976
[4] R Corrocher M Querena A M Stanzial and G de SandreldquoMicrocytosis in hyperthyroidism haematological profile inthyroid disordersrdquo Haematologica vol 66 no 6 pp 779ndash7861981
[5] J A Perlman and P M Sternthal ldquoEffect of 131I on the anemiaof hyperthyroidismrdquo Journal of Chronic Diseases vol 36 no 5pp 405ndash412 1983
[6] C S P Lima D E Zantut Wittmann V Castro et al ldquoPancy-topenia in untreated patients with Gravesrsquo diseaserdquoThyroid vol16 no 4 pp 403ndash409 2006
[7] A R Axelrod and L Berman ldquoThe bone marrow in hyperthy-roidism and hypothyroidismrdquo Blood vol 6 no 5 pp 436ndash4531951
[8] M P Foster E Montecino-Rodriguez and K DorshkindldquoProliferation of bonemarrow pro-B cells is dependent on stim-ulation by the pituitarythyroid axisrdquo Journal of Immunologyvol 163 no 11 pp 5883ndash5890 1999
[9] C Arpin M Pihlgren A Fraichard et al ldquoEffects of T3R1205721and T3R1205722 gene deletion on T and B lymphocyte developmentrdquoJournal of Immunology vol 164 no 1 pp 152ndash160 2000
[10] KGrymuła E Paczkowska VDziedziejko et al ldquoThe influenceof 3310158405-triiodo-L-thyronine on human haematopoiesisrdquo CellProliferation vol 40 no 3 pp 302ndash315 2007
[11] J D Hines C H Halsted R C Griggs and J W HarrisldquoMegaloblastic anemia secondary to folate deficiency associatedwith hypothyroidismrdquo Annals of Internal Medicine vol 68 no4 pp 792ndash805 1968
[12] N Dainiak D Sutter and S Kreczko ldquoL-triiodothyronineaugments erythropoietic growth factor release from peripheralblood and bone marrow leukocytesrdquo Blood vol 68 no 6 pp1289ndash1297 1986
[13] J Fandrey H Pagel S Frede M Wolff and W JelkmannldquoThyroid hormones enhance hypoxia-induced erythropoietinproduction in vitrordquo Experimental Hematology vol 22 no 3pp 272ndash277 1994
[14] L A Malgor C C Blanc E Klainer et al ldquoDirect effects ofthyroid hormones on bone marrow erythroid cells of ratsrdquoBlood vol 45 no 5 pp 671ndash679 1975
[15] C Schroeder L Gibson M Zenke and H Beug ldquoModulationof normal erythroid differentiation by the endogenous thyroidhormone and retinoic acid receptors a possible target for v-erbA oncogene actionrdquoOncogene vol 7 no 2 pp 217ndash227 1992
[16] C Leberbauer F Boulme G Unfried J Huber H Beugand E W Mullner ldquoDifferent steroids co-regulate long-termexpansion versus terminal differentiation in primary humanerythroid progenitorsrdquo Blood vol 105 pp 85ndash94 2005
[17] M C Perrin J P Blanchet and G Mouchiroud ldquoModulationof human and mouse erythropoiesis by thyroid hormone andretinoic acid evidence for specific effects at different steps ofthe erythroid pathwayrdquo Hematology and Cell Therapy vol 39pp 19ndash26 1997
6 ISRN Endocrinology
[18] T Helenius and S Tikanoja ldquoA sensitive and practical immuno-radiometric assay of thyrotropinrdquo Clinical Chemistry vol 32no 3 pp 514ndash518 1986
[19] T W Campbell ldquoHematology of birdsrdquo in Veterinary Hema-tology and Clinical Chemistry M A Thrall Ed pp 225ndash258Lippincott Williams and Wilkins Philadelphia Pa USA 2004
[20] TW Campbell ldquoHematology of fishrdquo inVeterinary Hematologyand Clinical Chemistry M A Thrall Ed pp 277ndash290 Lippin-cott Williams ampWilkins Philadelphia Pa USA 2004
[21] N C JainEssentials ofHematology LeaampFebiger PhiladelphiaPa USA 1993
[22] R A Green and A Blue-McLendon ldquoRatite hematologyrdquo inPages in Schalmrsquos Veterinary Hematology pp 1201ndash1206 5thedition 2000
[23] M Tavares-Dias and F R Moraes ldquoHematological parametersfor the Brycon orbignyanus Valenciennes 1850 (OsteichthyesCharacidae) intensively bredrdquo Hidrobiologica vol 16 pp 271ndash274 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

ISRN Endocrinology 5
13201245
119875 value = 0115
0
5
10
15
No Yes
Med
ian
hem
oglo
bin
(gd
L)
Figure 5 Levels of hemoglobin for the immunological thyroiddisease patients
29000
36750119875 value = 0313
0
100
200
300
400
No Yes
Med
ian
plat
elet
s
Figure 6 Levels of platelets for the immunological patients units
level of the subjects suffering from immunological thyroidwas low too This clinically indicates a state of anemia Otherstudies have also shown that hypothyroidism causes anemiaor hyperproliferation of immature erythroid progenitors andthe anaemia is usually macrocytic hypochromic anaemia [3]The increase in the production of platelet can be attributedto the imbalance in the hematopoiesis which is a compen-satory mechanism [8] These observations have confirmedthe association between immunological thyroid disease andhematopoiesis and that hematological parameters are alteredin this condition Also it gives credence to the rejection ofour null hypothesis which states that hematological profilesin immunological thyroid diseases patients do not differ fromthose without immunological thyroid disease
5 Conclusion
The presence of anaemia in thyroid disease is associatedwith thyroid hormone Therefore thyroid hormones have asignificant influence on erythropoiesis The finding suggeststhat the molecular mechanism by which thyroid hormonesinfluence hematopoiesis may provide a basis for therapeuticintervention in thyroid diseases Immunological thyroid dis-ease patients tend to have higher levels of thyroid hormonalprofiles and low hematological profiles (WBCs RBCs andHB) though higher platelets compared to the nonimmuno-logical thyroid disease patients
References
[1] D W Golde N Bersch I J Chopra and M J Cline ldquoThyroidhormones stimulate erythropoiesis in vitrordquoThe British Journalof Haematology vol 37 no 2 pp 173ndash177 1977
[2] H G Fein and R S Rivlin ldquoAnemia in thyroid diseasesrdquoMedical Clinics of North America vol 59 no 5 pp 1133ndash11451975
[3] L Horton R J Coburn J M England and R L HimsworthldquoThe haematology of hypothyroidismrdquo Quarterly Journal ofMedicine vol 45 no 177 pp 101ndash123 1976
[4] R Corrocher M Querena A M Stanzial and G de SandreldquoMicrocytosis in hyperthyroidism haematological profile inthyroid disordersrdquo Haematologica vol 66 no 6 pp 779ndash7861981
[5] J A Perlman and P M Sternthal ldquoEffect of 131I on the anemiaof hyperthyroidismrdquo Journal of Chronic Diseases vol 36 no 5pp 405ndash412 1983
[6] C S P Lima D E Zantut Wittmann V Castro et al ldquoPancy-topenia in untreated patients with Gravesrsquo diseaserdquoThyroid vol16 no 4 pp 403ndash409 2006
[7] A R Axelrod and L Berman ldquoThe bone marrow in hyperthy-roidism and hypothyroidismrdquo Blood vol 6 no 5 pp 436ndash4531951
[8] M P Foster E Montecino-Rodriguez and K DorshkindldquoProliferation of bonemarrow pro-B cells is dependent on stim-ulation by the pituitarythyroid axisrdquo Journal of Immunologyvol 163 no 11 pp 5883ndash5890 1999
[9] C Arpin M Pihlgren A Fraichard et al ldquoEffects of T3R1205721and T3R1205722 gene deletion on T and B lymphocyte developmentrdquoJournal of Immunology vol 164 no 1 pp 152ndash160 2000
[10] KGrymuła E Paczkowska VDziedziejko et al ldquoThe influenceof 3310158405-triiodo-L-thyronine on human haematopoiesisrdquo CellProliferation vol 40 no 3 pp 302ndash315 2007
[11] J D Hines C H Halsted R C Griggs and J W HarrisldquoMegaloblastic anemia secondary to folate deficiency associatedwith hypothyroidismrdquo Annals of Internal Medicine vol 68 no4 pp 792ndash805 1968
[12] N Dainiak D Sutter and S Kreczko ldquoL-triiodothyronineaugments erythropoietic growth factor release from peripheralblood and bone marrow leukocytesrdquo Blood vol 68 no 6 pp1289ndash1297 1986
[13] J Fandrey H Pagel S Frede M Wolff and W JelkmannldquoThyroid hormones enhance hypoxia-induced erythropoietinproduction in vitrordquo Experimental Hematology vol 22 no 3pp 272ndash277 1994
[14] L A Malgor C C Blanc E Klainer et al ldquoDirect effects ofthyroid hormones on bone marrow erythroid cells of ratsrdquoBlood vol 45 no 5 pp 671ndash679 1975
[15] C Schroeder L Gibson M Zenke and H Beug ldquoModulationof normal erythroid differentiation by the endogenous thyroidhormone and retinoic acid receptors a possible target for v-erbA oncogene actionrdquoOncogene vol 7 no 2 pp 217ndash227 1992
[16] C Leberbauer F Boulme G Unfried J Huber H Beugand E W Mullner ldquoDifferent steroids co-regulate long-termexpansion versus terminal differentiation in primary humanerythroid progenitorsrdquo Blood vol 105 pp 85ndash94 2005
[17] M C Perrin J P Blanchet and G Mouchiroud ldquoModulationof human and mouse erythropoiesis by thyroid hormone andretinoic acid evidence for specific effects at different steps ofthe erythroid pathwayrdquo Hematology and Cell Therapy vol 39pp 19ndash26 1997
6 ISRN Endocrinology
[18] T Helenius and S Tikanoja ldquoA sensitive and practical immuno-radiometric assay of thyrotropinrdquo Clinical Chemistry vol 32no 3 pp 514ndash518 1986
[19] T W Campbell ldquoHematology of birdsrdquo in Veterinary Hema-tology and Clinical Chemistry M A Thrall Ed pp 225ndash258Lippincott Williams and Wilkins Philadelphia Pa USA 2004
[20] TW Campbell ldquoHematology of fishrdquo inVeterinary Hematologyand Clinical Chemistry M A Thrall Ed pp 277ndash290 Lippin-cott Williams ampWilkins Philadelphia Pa USA 2004
[21] N C JainEssentials ofHematology LeaampFebiger PhiladelphiaPa USA 1993
[22] R A Green and A Blue-McLendon ldquoRatite hematologyrdquo inPages in Schalmrsquos Veterinary Hematology pp 1201ndash1206 5thedition 2000
[23] M Tavares-Dias and F R Moraes ldquoHematological parametersfor the Brycon orbignyanus Valenciennes 1850 (OsteichthyesCharacidae) intensively bredrdquo Hidrobiologica vol 16 pp 271ndash274 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 ISRN Endocrinology
[18] T Helenius and S Tikanoja ldquoA sensitive and practical immuno-radiometric assay of thyrotropinrdquo Clinical Chemistry vol 32no 3 pp 514ndash518 1986
[19] T W Campbell ldquoHematology of birdsrdquo in Veterinary Hema-tology and Clinical Chemistry M A Thrall Ed pp 225ndash258Lippincott Williams and Wilkins Philadelphia Pa USA 2004
[20] TW Campbell ldquoHematology of fishrdquo inVeterinary Hematologyand Clinical Chemistry M A Thrall Ed pp 277ndash290 Lippin-cott Williams ampWilkins Philadelphia Pa USA 2004
[21] N C JainEssentials ofHematology LeaampFebiger PhiladelphiaPa USA 1993
[22] R A Green and A Blue-McLendon ldquoRatite hematologyrdquo inPages in Schalmrsquos Veterinary Hematology pp 1201ndash1206 5thedition 2000
[23] M Tavares-Dias and F R Moraes ldquoHematological parametersfor the Brycon orbignyanus Valenciennes 1850 (OsteichthyesCharacidae) intensively bredrdquo Hidrobiologica vol 16 pp 271ndash274 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom