Embed Size (px)
Citation preview

1Clinical Strategies for Type 1
Clinical Strategies for Type 1 Diabetes: Pumps, Multiple Daily
Injection Regimens AmylinInjection Regimens, Amylin Analogs and Continuous
Glucose Monitoring
Jeremy Pettus, MDEndocrinologist
Assistant Professor of MedicineUniversity of California, San Diego
Diabetes in the
Pre-Insulin EraEra

2Clinical Strategies for Type 1
Risk Of Developing Type 1 Diabetes
General Population 0.3%
Sibling 4%
Mother 2 – 3%
Father 6 – 8%
Identical Twins ~50%
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.
Natural History and Cause of Type 1 Diabetes
Autoimmune condition100% Insulin making cells
Putative Trigger
Immune System Dysfunctionof the pancreas
Immune System Dysfunction
Circulating Auto Antibodies (ICA, GAD)
Symptoms
Genetic predisposition
Damage to the cells of the pancreas
Pre-diabetes Diabetes
Time = months to a few yearsPettus J, Edelman SV. (2013) Adjunctive Therapies. In The American Diabetes Association/JDRF Type 1 Diabetes Sourcebook (319-340). VA: American Diabetes Association

3Clinical Strategies for Type 1
Type 1 Diabetes: Important Treatment Themes
1 In addition to getting the A1c below 7% try1. In addition to getting the A1c below 7%, try to reduce the daily glucose fluctuations in your patients (hyper- and hypoglycemia)
2. The insulin regimen should mimic what happens in a non-diabetic state
3 Look out for other autoimmune conditions3. Look out for other autoimmune conditions (low thyroid levels, celiac)
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.
Physiologic Insulin, Glucagon and Amylin Secretion
Systemic Circulation
LiverPancreas
InsulinPortal Vein
InsulinAmylin
Glucagon
Beta Cell
Alpha CellPettus J, Edelman SV. (2013) Adjunctive Therapies. In The American Diabetes
Association/JDRF Type 1 Diabetes Sourcebook (319-340). VA: American Diabetes Association

4Clinical Strategies for Type 1
Physiologic Insulin Secretion and Glucose Levels In Healthy Subjects
50
Bolus Insulin (40 to 60% of TTD)
Insulin(µU/mL)
Glucose150
100
50
25
0 Basal Insulin: HGO(40 to 60% of TDD)
Breakfast Lunch Dinner
Glucose(mg/dL) 50
07 8 9 10 11 12 1 2 3 4 5 6 7 8 9A.M. P.M.
Basal Glucose
Time of Day
Edelman SV, Henry RR. Diagnosis and management of type 2 diabetes. 12th Edition. Professional Communications, Inc., Greenwich, CT. 288 pages, 2014.
Basal/Bolus Treatment Program With Rapid and Long-Acting Analogs Glulisine
OrInsulin AspartBreakfast Lunch Dinner
Insu
lin A
ctio
n
Insulin AspartOr
Insulin LisproOr
Inhaled InsulinU-100/300
Glargine/Levemir
4:004:00 16:0016:00 20:00 20:00 24:0024:00 4:004:00 8:008:0012:0012:008:008:00TimeTime
Glargine/Levemir
Adapted with permission from Leahy J. In: Leahy J, Cefalu W, eds. Insulin Therapy. New York: Marcel Dekker; 2002:87-112. Nathan DM. N Engl J Med 2002;347:1342-1349.

5Clinical Strategies for Type 1
d k h l h
Lilly Pens: Memoir & Kwikpen
Convenient
Discreet
NovoNordisk: NovoPen Echo & FlexTouch
f l Protects insulin from light, heat and agitation
Sanofi-Aventis: SoloStar
First InsulinInsulin Pump
1964

6Clinical Strategies for Type 1
2nd Generation Insulin PumpsInsulin Pumps
in the early 70s
Animas VibeT d T Sli
Insulin Pump Options
Tandem T-SlimAsante SnapMedtronic 530GOmniPod

7Clinical Strategies for Type 1

8Clinical Strategies for Type 1
Body
Traditional Insulin Pump Components
Body Insulin reservoir Tubing Insertion catheter
Battery compartment
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.
Infusion sites need to be
Infusion Sites
need to be changed every two to three days
Quick release catheters
Auto inserters
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.

9Clinical Strategies for Type 1
Improved glycemic control◦ More precise, physiologic insulin delivery◦ Greater ability to handle dawn phenomenon, stress
and other conditions that alter insulin requirements
Insulin Pumps: Advantages
q◦ “Smart features” help to estimate insulin doses and
reduce errors, i.e. stacking insulin In some situations (but not all), freedom and
flexibility in lifestyle◦ Eliminate multiple daily injections (1 stick every 3
days). Very easy to respond to CGM results.days). Very easy to respond to CGM results.◦ Reduce restrictions on eating, exercise and sleeping
patterns: could have the same benefits with MDI◦ Greater flexibility with sports, travel, work schedule
and other activities (not with water sports)Edelman, Taking Control Of Your Diabetes 4th edition. 2013 and Walsh JA, Roberts R. Pumping Insulin 5th edition. 2011.
Bolus Options With Pump Therapy
Standard Square Wave
Dual Wave
InsulinTime
1. Standard: quickly absorbed foods2. Square Wave: gastroparesis, fatty meals, Pramlintide (symlin)3. Dual Wave: combination of rapid and slowly absorbed meals
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.

10Clinical Strategies for Type 1
Variable Basal Rate Capability(Total daily basal dose/24)-(10 to 20%)
Breakfast Lunch Dinnern
Basal infusion
Bolus Bolus Dual Wave Bolus
1
Plas
ma
insu
lin
3
4:004:00 16:0016:00 20:00 20:00 24:0024:00 4:004:00 8:008:0012:0012:008:008:00
TimeTime
Basal infusion
2Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition ProfessionalCommunications Inc., Greenwich, CT. 544 pages, 2013.
Which patient below is NOT a good pump candidate?
A A pediatric ICU doctor with type 1 who works a 12 A p yphour graveyard shift (6pm to 6am) 10 days a month
B A US postal worker with type 1 who delivers mail primarily by foot
C A woman with type 1 who is 20 weeks pregnant with poor controlwith poor control
D An obese 68 year old male with type 2 diabetes currently on multiple daily injections

11Clinical Strategies for Type 1
Determine the Correct Bolus Dosing (you should already have this part done on MDI)
Use what the patient was doing on MDI therapy (easiest way to start)
Carbohydrate counting (Insulin to CHO ratio) is helpful but not 100% necessary: Insulin to carbohydrate ratio: I:CHOU f ti f t i t t l Use of a correction factor is a great tool: Correction factor (CF) also called the insulin sensitivity factor (ISF)
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.
Start with a ratio of 1:15 for insulin sensitive type 1 diabetics
Insulin to Carbohydrate Ratio Calculation: I:CHO
diabetics Start with a ratio of 1:10 for insulin resistant type 2
diabetics Formula: divide Total daily insulin dose into 500 Example: 34 year old male with type 1 diabetes
currently on 25 units of glargine (Lantus) every night and 20 to 25 units of insulin aspart (NovoLog)night and 20 to 25 units of insulin aspart (NovoLog)each day: 500/50=10 So the initial Insulin to carb ratio is 1:10
Walsh JA, Roberts R. Pumping Insulin 5th edition. 2011.

12Clinical Strategies for Type 1
Giving your patients a correction factor is a very practical tool whether they are on a pump or not
Correction Factor (CF) or Insulin Sensitivity Factor (ISP)
The CF is an estimate of how much the BS will drop with one unit of fast acting insulinThe CF usually 1:50 for insulin sensitive (<50u) patients and 1:25 for insulin resistant patients
The CF can be estimated by taking the total daily insulin dose and dividing it into 1800 (the 1800 rule)You also need to pick a target glucose level for the patient (between 100 and 150)
Walsh JA, Roberts R. Pumping Insulin 5th edition. 2011.
Used at meal time AND for unexpected
Example of Determining the Correction Factor
Used at meal time AND for unexpected hyperglycemia in between meals
21 year old female on insulin glargine 15 units at night and taking approximately 15 –20 units a day in boluses with insulin glulisine◦ (1800/35 units = 51)~ CF 1:50

13Clinical Strategies for Type 1
Multiple basal rates
Generic Features of Insulin Pumps
Square and dual wave bolus features Calculate a suggested bolus based on individual data input (Insulin:CHOratio and correction factor)
Insulin on-board feature (helps to Insulin on board feature (helps to avoid “stacking” insulin)
Occlusion and reservoir alarmsEdelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.
Ability to deliver very low basal rates (0 025 units/hour)
Advanced Features of Insulin Pumps Animas Vibe
(0.025 units/hour) for insulin sensitive patients
Easy to visualize LCD screen and very small size
Tactile bolusing/touch
Tandem T-Slim
Medtronic 530Gbolusing/touch screen
Pump acts as a billboard to display CGM results
Tubeless on body pump
Omnipod
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.

14Clinical Strategies for Type 1
Advanced Features of Insulin Pumps (continued)Glucose meter and pump have bidirectional communication
Animas 2020 Ping Medtronic Paradigm
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.

15Clinical Strategies for Type 1
Straightforward and Simple Ways to Start Insulin Pump Therapy
1. Get the patient adjusted as best as you can on a MDI1. Get the patient adjusted as best as you can on a MDI regimen with basal insulin (eg. U-100/300glargine [Lantus/Toujeo] or detemir [Levemir])2. Patient chooses a pump and the pump support people will help with insurance issues (they are good at this)
3. Determine the basal rate based on the total daily3. Determine the basal rate based on the total daily basal insulin dose (no change in boluses)
4. The pump trainer takes over and can help (0 to 100%) with the initial adjustments
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.
74 year old female with type 1 diabetes for 10 years (LADA) on insulin glargine, 18 units qhs
Case 1: Barbara
g g , q Bolus dosing based on
carbohydrates (1 unit: 15 grams) Correction factor (1:50) with a
goal of 125mg/dL Last 3 A1c values between 7.5-
8.0% She has excessive fluctuations
with exercise She is very active and requested
an insulin pump

16Clinical Strategies for Type 1
Her initial basal rate was calculated as 18 units (minus 10% because her A1c was
Case 1: Barbara (continued)
over 7.5%) divided by 24 = 0.675 u/hr No change with her bolus doses for now She wanted a pump without tubing Once the patient received the pump and
supplies in the mail a trainer got her upsupplies in the mail, a trainer got her up and running
What adjustment would you suggest for Barbara?
B L D HS ~3 amDay 1 227 121 143 164 142
A Increase the insulin to carbohydrate ratio at dinner time
Day 1 227 121 143 164 142Day 2 203 152 144 144 161
Day 3 198 124 132 135 133
Day 4 188
A Increase the insulin to carbohydrate ratio at dinner time
B Increase the correction factor at breakfast time
C Increase the basal rate by 20% starting at 10pm to 7am
D Increase the basal rate by 20% starting at 3am to 7am

17Clinical Strategies for Type 1
56 year old male with type 2 diabetes for 21 years on insulin detemir 38 units qhs
Case 2: David
detemir 38 units qhs Bolus given as 10 units with each
meal and then he uses a correction dose if he is high (1:25) with a goal of 150mg/dL.
A1c has not been below 8.5%. He is tired of the multiple injections He is tired of the multiple injections
and travels frequently for his job. Centrally obese with a BMI of 30 Also treated for hypertension,
dyslipidemia
His initial basal rate was calculated as 38 units divided by 24 = 1.58 u/hr
No change with his bolus doses but was given
Case 2: David (continued)
No change with his bolus doses but was given some information on carbohydrate counting
He wanted a pump that held 300 units since his he did not want to change his syringe and tubing more than every three days
His HCP was sent Letter of Medical Necessity His HCP was sent Letter of Medical Necessity by the pump company and a pump trainer got him up and running.

18Clinical Strategies for Type 1
What adjustment would you suggest for David?
B L D HSD 1 137 135 223 143
A Increase the pre-meal dose of fast acting insulin from 10 to 15 units before breakfast, lunch and dinner
Day 1 137 135 223 143Day 2 123 142 191 124Day 3 118 128 186 117Day 4 195 121 211
B Increase the pre-meal dose of fast acting insulin from 10 to 15 units before breakfast only
C Increase the basal rate by 20% during the day between lunch and dinner (12 noon to 6pm)
D Increase the pre-meal dose of fast acting insulin from 10 to 15 units before lunch only
A disruption in short acting insulin delivery due to a dislodged catheter, blockage, or an empty reservoir can result in a fairly rapid rise in glucose concentration
Disadvantages of Pump Therapy
rapid rise in glucose concentration◦ Severe hyperglycemia◦ Ketoacidosis
Cost of the insulin pumps◦ Pump costs approximately $3,500 to $5,000 (pay as you go
with the Omnipod)◦ Monthly cost of $30 to $40 due to batteries, infusion lines,
i d dh i tsyringes, and adhesive tape Minor skin irritation or infections at the insulin pump catheter
insertion site Very occasional abscess
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.

19Clinical Strategies for Type 1
T h l h k
Continuous Glucose Monitoring (CGM)
Technology that can take some of the unpredictability and frustration out of diabetes management
400
Excessive Glucose Fluctuations
Mean A1C=6.7%
9 People with Type 1 Diabetes on BLINDED CGM
400
100
200
300Glucose
Concentration (mg/dL)
12:00 AM
4:00 AM
8:00 AM
12:00 PM
4:00 PM
8:00 PM
12:00 AM
0
24-hour CGMS glucose sensor data Type 1 diabetes (N=9)
40
Impact on Pramlintide on Glucose Fluctuations and PostPrandial Glucose, Glucagon, and Triglyceride Excursions Among Patients with Type 1 Diabetes Intensively Treatedwith Insulin Pumps, Levetans et al., Diabetes, 2003, American Diabetes Association diabetesjournals.org http://care.diabetesjournals.org/content/26/1/1.short

20Clinical Strategies for Type 1
Medtronic 530G with Enlite sensor
Dexcom G4 Platinum
N=322 with baseline A1c > 7% A significant drop in A1c @ 6 months occurred for those who
averaged > 6 days/week CGM use (p<0.001 in each age group) Also observed was a significant reduction in hypoglycemia
JDRF: Predictive Factors of CGM
Also observed was a significant reduction in hypoglycemia
0 6
-0.4
-0.2
0.0
0.2
e in
A1c
(%
)
<4 d/weekChange in A1c %
0.2
0.0
-0.2
0 4
8-14 years15-24 years
< 25 years
The Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group. Continuous glucose monitoring and intensive treatment of type 1 diabetes. N Engl J Med; 359;1464-1476 2008.
-0.8
-0.6
Ch
ang
<4.0 days/week 4.0-<6.0 days/week ≥6.0 days/week
4-6 d/week6-7 d/week
in A1c % -0.4
-0.6
-0.8

21Clinical Strategies for Type 1
Constant: Your glucose is steady (not increasing/decreasing more than 1 mg/dLeach minute)
No change in calculation
Slowly rising: Your glucose is rising 1-2 30 to 50% higher
How CGM and Trending Information Can Affect Our Decisions (CF/I:CHO)
Slowly rising: Your glucose is rising 1 2 mg/dL each minute
30 to 50% higher
Rising: Your glucose is rising 2-3 mg/dLeach minute
50 to 150% higher
Rapidly Rising: Your glucose is rising more than 3mg/dL each minute
100 to 200% higher
Slowly Falling: Your glucose is falling 1-2 mg/dL each minute VariablesFalling: Your glucose is falling 2 3 mg/dL BS Level
Meal Type/SizeExercise Duration
& Intensity
Falling: Your glucose is falling 2-3 mg/dLeach minuteRapidly Falling: Your glucose is falling more than 3 mg/dL each minute
No Arrow
No Rate of Change Information: The receivercannot always calculate how fast your glucose is rising or falling
Herrmann K, Frias JP, Edelman SV, Lutz K, Shan K, Chen S, Maggs D, Kolterman OG. Pramlintide improved measures of glycemic control and body weight in patients with type 1 diabetes mellitus undergoing continuous subcutaneous insulin infusion therapy. Postgraduate Medicine. 123(3), 2013.

22Clinical Strategies for Type 1
35 year old male with type 1 diabetes for 20 years CHO to insulin ratio 10:1 CF 1:30 gosl 120 mg/dl
Case 3: Jeremy
Post “Snack” BS of 220mg/dL at 4:00 p.m. (snack at 3:30 p.m., no insulin given with snack)
Jeremy’s CGM Guidelines◦ Correction factor 1:30
Case 3: Jeremy (continued)
◦ Correction factor 1:30◦ Target glucose 120 mg/dL◦ 220-120/30 = 3.3 units
N t A bl d f 220 d tNote: A blood sugar of 220 does not lead to any symptoms

23Clinical Strategies for Type 1
Which option below is the best suggestion for Jeremy to follow at 4:00 pm?
A Watch and wait (give no additional insulin)B Walk for an hour at a brisk paceC Give a correction dose of 3.3 unitsD Give a correction dose greater than 3.3 units
Change in mean Insulin Dose Based on 2 ARROWS UP: Survey of 300 CGM users
3.2 units 7.2 units7.2 units
J. Pettus, D.A. Price, K.J. Hill, S. Edelman (2014), Diabetes Technology & Therapeutics. February 2014, 16(S1): A-76 page 198
Need to confirm BS value with a glucose meter before giving insulin

24Clinical Strategies for Type 1
How CGM and Trending Information Can Affect Dosing Decisions
3.2 units
140% Mean Increase
7.2 units
48% Mean Decrease1.5 units
J. Pettus, D.A. Price, K.J. Hill, S. Edelman (2014), Diabetes Technology & Therapeutics. February 2014, 16(S1): A-76 page 198
Robyn is a 24 year old type 1 diabetic for 5 years on insulin glargine
She eats pizza at 12:00 MN and takes 5 units of fast acting insulin
Case 4: Robyn
Her high glucose alert goes off at 2:15am and her BS is275mg/dl.
Her CF is 1:40 with a goal of 120mg/dLRobyn gave a correction bolus of 325-120/40= 5.1 units

25Clinical Strategies for Type 1
Robyn looks at her Dexcom (CGM) at 3am and her BS was now over 350mg/dl and she gave herself another “Rage Bolus” 5.0 units.
At 8:00 am she had a hypoglycemic reaction and needed
Case 4: Robyn
yp g yto ingest glucose tabs
First bolus 12 Midnight: 5 units for pizza Second bolus 2:15 a.m.: 5 unit correction
“Stacking The Dose”
dose Third bolus 3:00 a.m.: 5 more units

26Clinical Strategies for Type 1
No safety concerns as more information is better than no
Concerns To Address With CGM
information is better than no information
Alarm fatigueAlert high and low settingsHigh and low snooze alarmsHigh and low snooze alarms Take advantage of the Share system
Stacking
Wait at least 90 minutes before a second dose We need a faster on/off insulin (technosphere
An Object in Motion Stays in Motion: Turnaround Time
/ ( p[Afrezza])
SubQinsulin isinsulin is not physiologic

27Clinical Strategies for Type 1
Inhaled Insulin, Afrezza
Pk h hPk
Pd
Technosphere/Inhaled Insulin
(Afrezza)VS
Rapid ActingAnaloguePd
Santos Cavaiola T, Edelman SV. Inhaled insulin: A breath of fresh air? A review of inhaled insulin. Clinical Therapeutics. 2014. 36(8)
(Insulin Human) Inhalation Powder Black Box Warning
(Spirometry at baseline, 6 months, then yearly)
WARNING: RISK OF ACUTE BRONCHOSPASM IN S C O C G S SPATIENTS WITH CHRONIC LUNG DISEASE
• Acute bronchospasm has been observed in patients with asthma and COPD using Afrezza
• Afrezza is contraindicated in patients with chronic lung disease such as asthma or COPDlung disease such as asthma or COPD
• Before initiating Afrezza, perform a detailed medical history, physical examination, and spirometry (FEV1) to identify potential lung disease in all patients
Afrezza full prescribing information: http://www.accessdata.fda.gov/drugsatfda_docs/label/2014/022472lbl.pdf

28Clinical Strategies for Type 1
Who would benefit the most from a CGM device?
A A person with type 2 diabetes and hypoglycemia unawarenesshypoglycemia unawareness
B A person with type 1 diabetes (A1C 6.9%) and with widely fluctuating and unpredictable glucose values
C A person with type 2 diabetes on orals and basal insulin at night
D A two year old child with type 1 diabetes
E A, B and D
Total daily basal and bolus doses Ins to carb ratio
Important Questions To Ask
s to ca b at o Correction factor (Insulin sensitivity ratio) If on a pump….do you disconnect and for
how long, basal rates, how often do you change out your infusion sets, and do you use the square wave or dual bolus features
CGM issues: check upper and lower alert limits as well as checking the snooze alarm

29Clinical Strategies for Type 1
Snooze Alert: very important
Statistical Summary• Glucose exposure (mean and eA1C) • Variability (SD & IQR)• % in target, above and below
Ambulatory Glucose Profile (AGP)
Visual Display• Modal day (14 if possible)• 5 glucose curves
Median (orange line),25th & 75th % (solid lines)10th a& 90th %(dotted lines)
75th
25th
10th
90th
50th
Daily View• Thumbnail view - Calendar format
Work vs. non-workWeekend vs. weekday
• Target range
10th
Diabetes Technology and TherapeuticsVol 15:2 2013

30Clinical Strategies for Type 1
AGP Statistics
Bergenstal, et. al, Diabetes Technology and TherapeuticsVol. 15:2 2013
What is Normal?
32 subjects with32 subjects with normal glucose
metabolism
(confirmed by OGTT and HOMA) monitored for 30
days.
Bergenstal, et. al, DiabetesTechnology and Therapeutics Vol. 15:2 2013

31Clinical Strategies for Type 1
AGP Uncontrolled Type 1 Diabetes
Bergenstal, et. al, Diabetes Technology and Therapeutics Vol. 15:2 2013
Identifying Glycemic Trouble SpotsAmbulatory Glucose Profile (AGP)
Where am2
75th
25th
10th
90th
50th
1
Where am I high?
2
Where is there3Where am I Low?
Where is there a lot of variability?
3
Bergenstal, et. al, Diabetes Technology and Therapeutics Vol. 15:2 2013

32Clinical Strategies for Type 1
Physiologic Insulin and Amylin Secretion After Meals
l
Meal Meal Meal
Amylin
Insulin
Plasma insulin (pM)
Plasma amylin(pM)
30
25
20
15
600
400
20010
5
7 am Midnight5 pm12 noon
Time
200
0
Koda et al, Diabetes. 1995; 44 (s1): 23BA.Weyer et al. Curr Pharm Des. 2001;7:1353-1373
Regulation of Blood Glucose Levels After Meals By Amylin (Symlin) Reduces the appetite
and leads to weight lossloss
The reduced
Suppression of glucagon levels from the alpha cells of the pancreas
Amylin is co-released with insulin after
ingestion of food
Stomach motility is normalized
glucagon levels help to control excessive glucose production by the liver
Edelman SV, Henry RR. Diagnosis and management of type 2 diabetes. Eleventh Edition. Professional Communications, Inc., Greenwich, CT. 288 pages, 2011.

33Clinical Strategies for Type 1
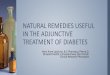
Pramlintide Reduces FBG, PPG and Glucose Fluctuations
220
140
160
180
200
Glu
cose
(m
g/dL
)
*
*
*
*
** *
insulin alone
insulin plus pramlitide120
pre-bf post-bf pre-lu post-lu pre-di post-di bedtime
Clinical Practice Study, 120 g SYMLINbf, breakfast; lu, lunch; di, dinnerN=166; *p-values for all data points <0.05Data on file, Amylin Pharmaceuticals, Inc.
* insulin plus pramlitide
Edelman, S, Lush, C, Kesty, N, Burns, C, Weyer, C, Frias, J. Progressive Reduction in Body Weight with Pramlintide Therapy in Obese Subjects with Type 2 Diabetes Treated with Diet and Exercise and/or Metformin. Diabetes. 56 (Suppl 1):1826-P.
4.0
5.0
Pramlintide + Insulin: Effect on Sustained Weight Loss
Insulin alone: weight gain
-3.0
-2.0
-1.0
0.0
1.0
2.0
3.0
Weightchange
(lbs)insulin plus pramlintide: weight loss
* **
**
-5.0
-4.0
0 13 26 39 52
Week
Edelman, S, Lush, C, Kesty, N, Burns, C, Weyer, C, Frias, J. Progressive Reduction in Body Weight with PramlintideTherapy in Obese Subjects with Type 2 Diabetes Treated with Diet and Exercise and/or Metformin. Diabetes. 56 (Suppl1):1826-P.
P<0.001 Between Groups

34Clinical Strategies for Type 1
Practical Clinical and Safety Tips for Patients Initiating Pramlintide in Type 1 and Type 2 Diabetes
Start with a low dose and titrate slowly to avoid nausea, which is the only side effect directly related towhich is the only side effect directly related to pramlintide
Take pramlintide with the main part of the meal Decrease the amount of fast-acting insulin by 30% to
50% when initiating pramlintide to avoid an insulin induced hypoglycemic reaction.
Use the extended bolus if on pump therapy Use the extended bolus if on pump therapy Be prepared to go through some interesting
psychological changes with regard to eating when initiating pramlintide
Edelman, Steven, Hirsch, Irl, Pettus, Jeremy; Practical Management of Type 1 Diabetes Second Edition, Professional Communications, Inc; 2014 Chapter 12 Pages 239-264
Physiologic insulin delivery: MDI or h
Components of a Complete Therapeutic Regimen
pump therapy Amylin replacement with pramlintide(Symlin) if appropriate
Home and continuous glucose monitoring (HGM and CGM)monitoring (HGM and CGM)
Self management: education, carb counting, correction factor, sick day rules, ect.
Edelman SV, Henry RR. Diagnosis and management of type 2 diabetes. 12th
Edition. Professional Communications, Inc., Greenwich, CT. 288 pages, 2014.

35Clinical Strategies for Type 1
Diagnosis and Treatment Of Type 1 Diabetes by Steven Edelman, Irl Hirsch and Jeremy Pettus , Professional Communications www.pcibooks.com
Additional Information
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.◦ Physiologic insulin delivery: Chapter 8*◦ Pump therapy: Chapter 9*
C i l i i Ch 12*◦ Continuous glucose monitoring: Chapter 12*◦ Home glucose monitoring: Chapter 10*◦ Carbohydrate counting: Chapter 5*◦ Pramlilntide (Symlin) Chapter 8*