Embed Size (px)
Citation preview
Clinical Clinical Site specific IMRTSite specific IMRT
Bulent Aydogan, PhDBulent Aydogan, PhD
Department of Radiation and
Cellular Oncology
University of Chicago
Nov 2007 Antalya, Turkiye
➫ You can download the full-blown version of this talk which has site specific clinical IMRT info for H&N, Prostate and GYN from ASTRO website under the refresher courses.
➫ You can email me @
Target AudienceTarget Audience
Everybody
New to treating with IMRTNew to treating with IMRT
Planning to treat a new sitePlanning to treat a new site
Learn from others mistakes!Learn from others mistakes!
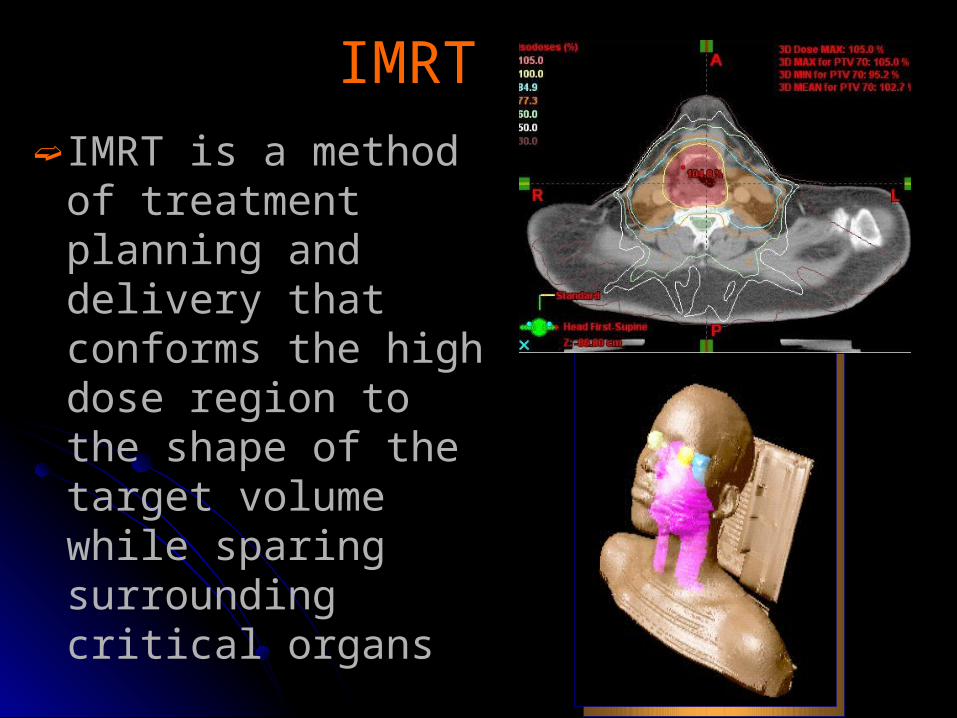
IMRTIMRT➫ IMRT is a method of
treatment planning and delivery that conforms the high dose region to the shape of the target volume while sparing surrounding critical organs
IMRT in numbersIMRT in numbers
➫In US☣80% are using☣80% started in the last 3-4 yrs☣90% non-user are planning to
use.
➫Outside of USA ☣Turkiye!
IMRT IMRT ALARMING RPC STATISTICSALARMING RPC STATISTICS
➫ Dose accuracy☣ Recommended 3% dose and 3mm
➫ RPC IMRT validation experience (ASTRO 2006 Abstract, A. Molineau et. al.)
☣ 155 inst. 196 irradiations☣ 7% dose and 4mm DTA☣ 54 failure ~>1/3 failed (33 on dose)

IMRT IMRT
PurposePurpose➫To illustrate how various aspects of
the IMRT planning process can influence the resultant treatment plan and delivery
➫To provide an update of IMRT planning techniques for gynecologic malignancies AND H&N, prostate
➫How IGRT influence IMRT process
SummarySummary
➫ IMRT treatment planning is a multi-step process
➫ Careful consideration throughout the entire process is necessary to ensure that an optimal plan is achieved
➫ Decisions made at the time of simulation, target and tissue delineation, planning and the delivery/verification process itself impact the overall plan
Simulation – Prone vs. Supine; Type of immobilization
Target and Tissue Delineation – Multiple imaging modalities
Treatment Planning/Optimization – Number of beams/orientation
Plan Evaluation – High conformity vs. dose homogeneity
Quality Assurance – Verification of calculated dose
Treatment Delivery/Verification – Verification scheme
Treatment Planning ProcessTreatment Planning Process
SUMMARYSUMMARY➫ IGRT
☣Changing the way we do IMRTʚ Marginsʚ Biological targetingʚ Intrafraction vs. interfraction ʚ Organ motion management
٩ Gating , IID
ʚ Adaptation
☣Requires more resources and careful planning
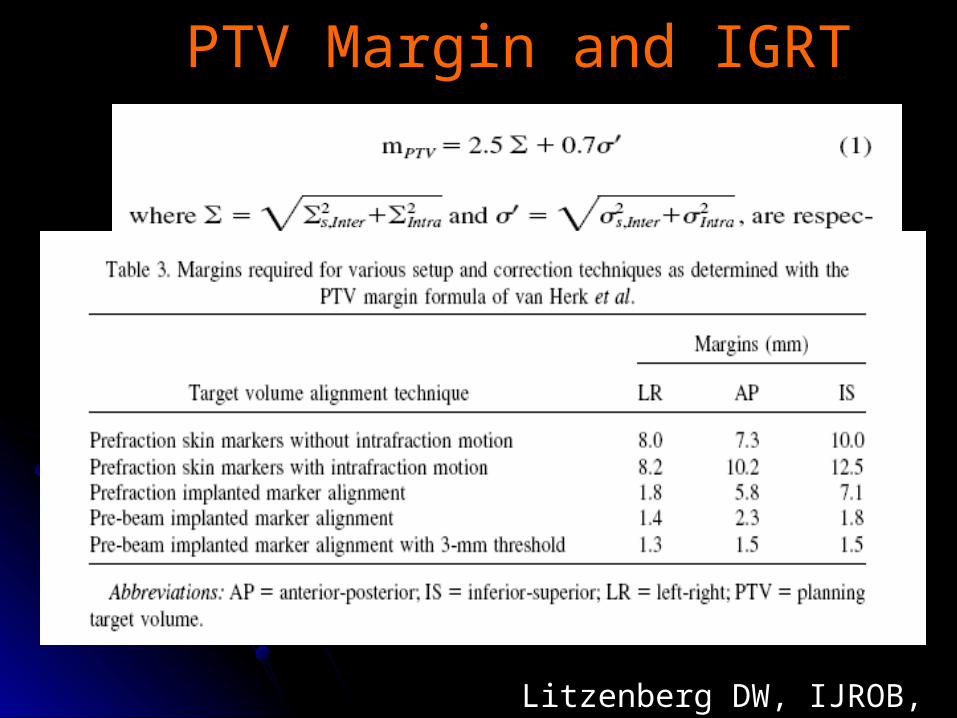
PTV Margin and IGRTPTV Margin and IGRT
Litzenberg DW, IJROB, 65(2), 2006
General issues In Treatment General issues In Treatment PlanningPlanning
➫Dose distribution depends☣Treatment planning system / optimization☣Dose calculation method
ʚ PBC, Superposition Convolution, MC
☣ User experience☣Realistic expectations (e.g., dose constraints)
☣Beam configuration, Energy?
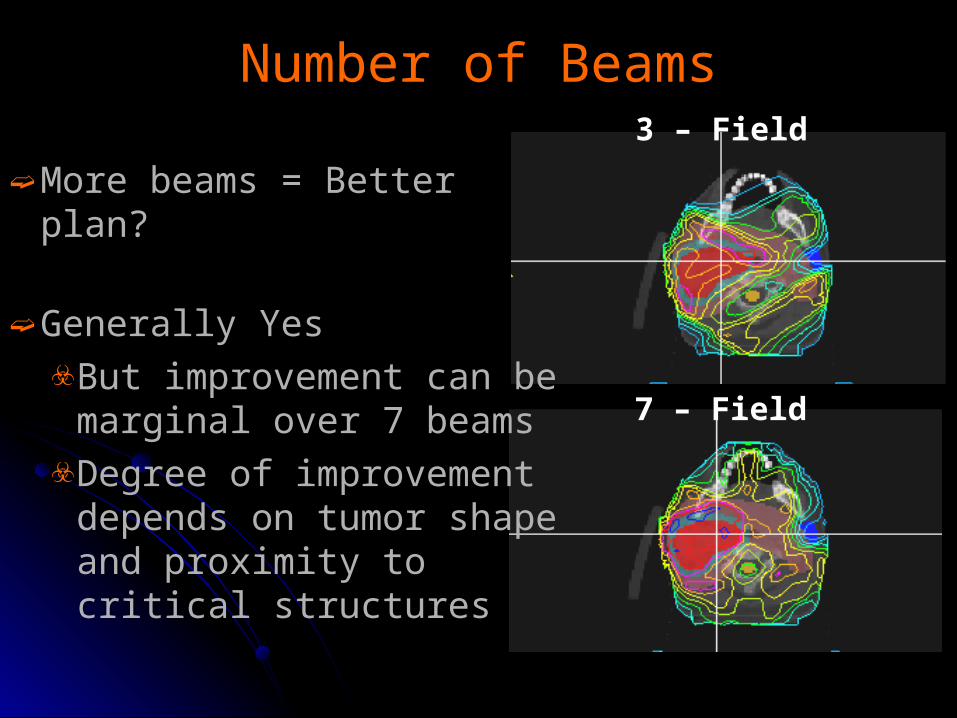
3 – Field
7 – Field
Number of BeamsNumber of Beams
➫ More beams = Better plan?
➫ Generally Yes☣But improvement can be
marginal over 7 beams☣Degree of improvement
depends on tumor shape and proximity to critical structures
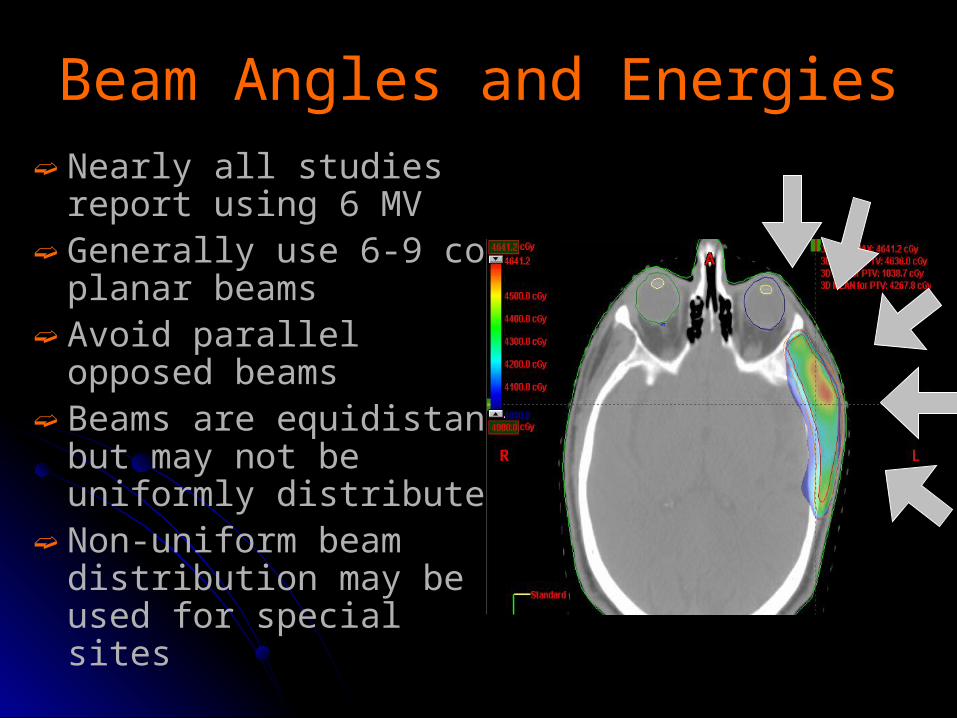
Beam Angles and Energies Beam Angles and Energies ➫ Nearly all studies report
using 6 MV➫ Generally use 6-9 co-
planar beams➫ Avoid parallel opposed
beams➫ Beams are equidistant but
may not be uniformly distributed
➫ Non-uniform beam distribution may be used for special sites
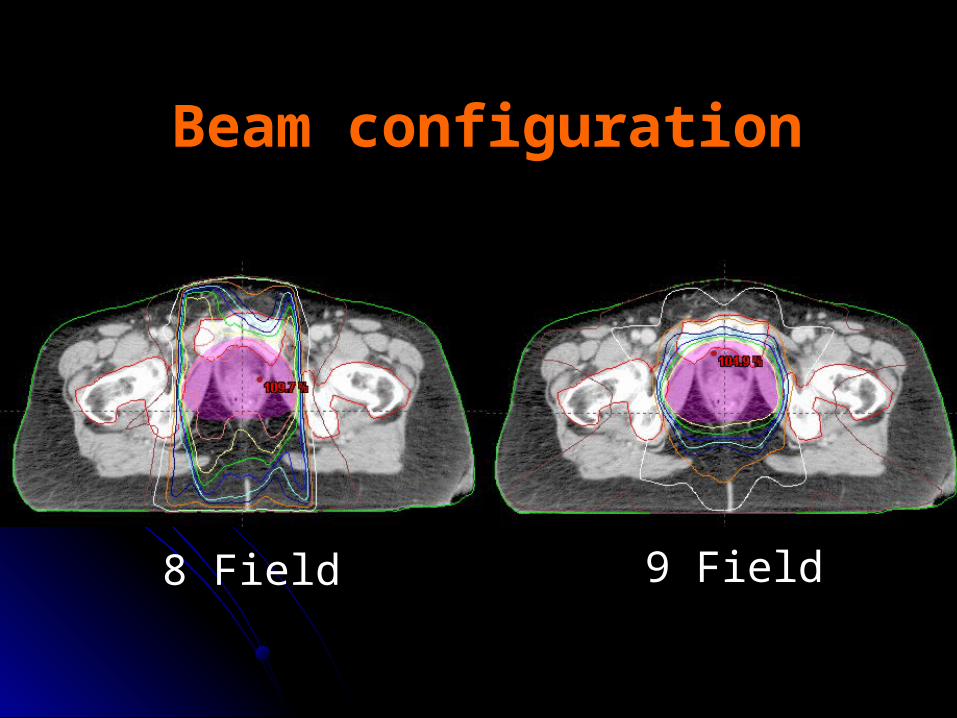
Beam configurationBeam configuration
9 Field8 Field
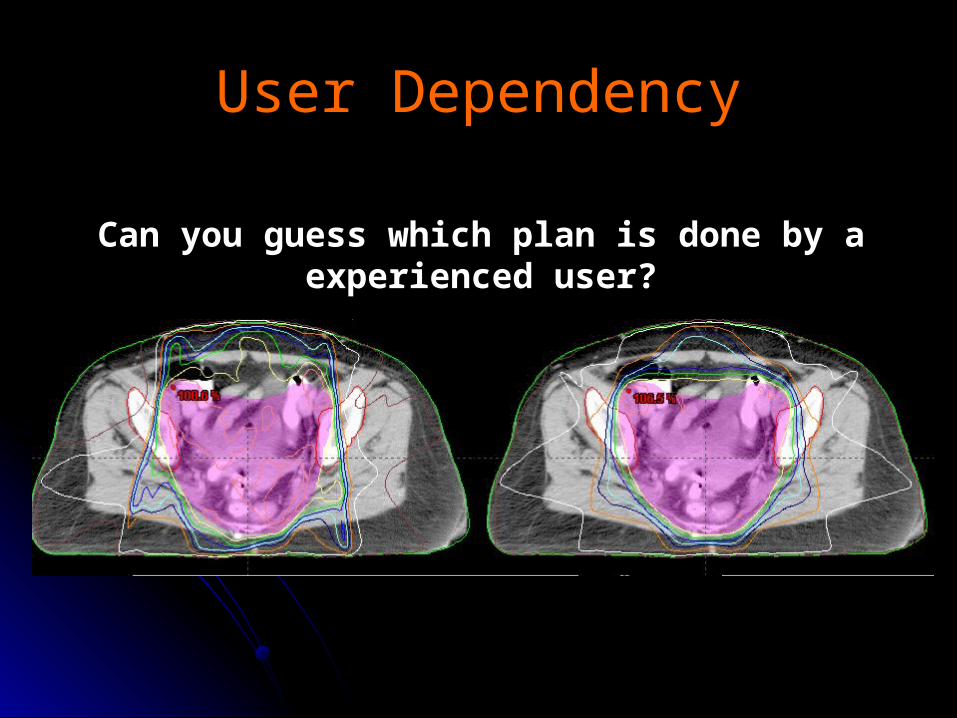
User DependencyUser Dependency
Can you guess which plan is done by a experienced user?
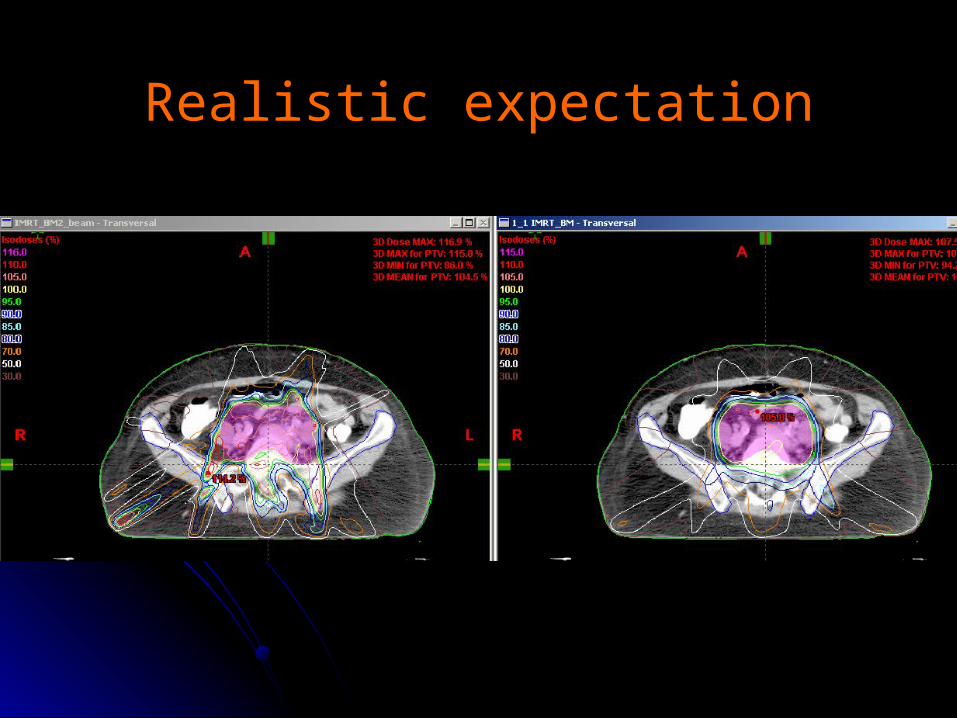
Realistic expectationRealistic expectation
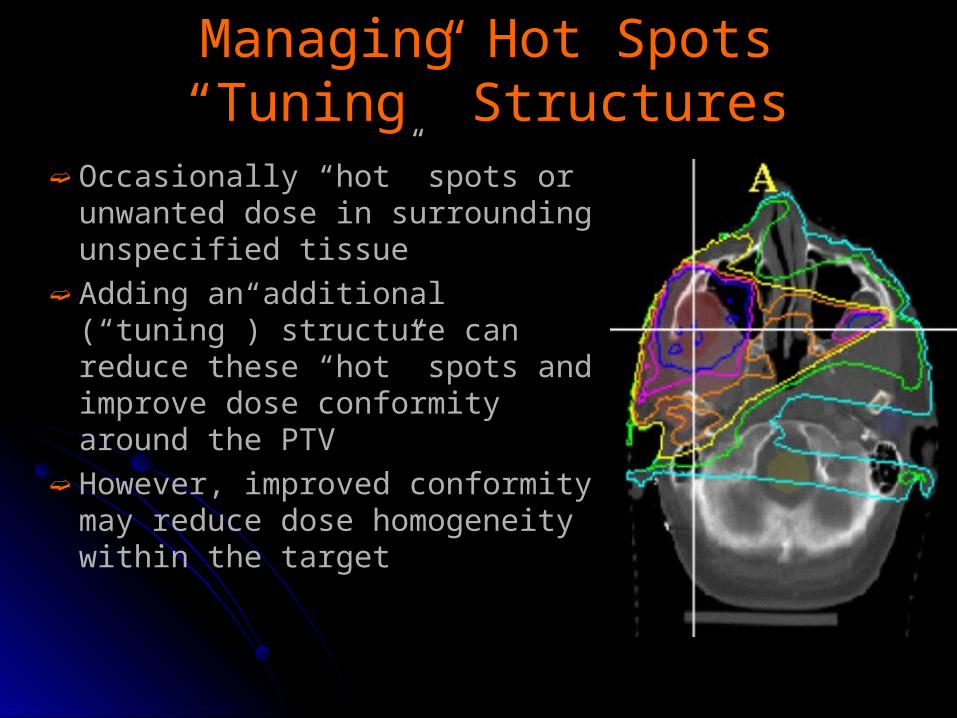
Managing Hot SpotsManaging Hot Spots“Tuning” Structures“Tuning” Structures
➫ Occasionally “hot” spots or unwanted dose in surrounding unspecified tissue
➫ Adding an additional (“tuning”) structure can reduce these “hot” spots and improve dose conformity around the PTV
➫ However, improved conformity may reduce dose homogeneity within the target
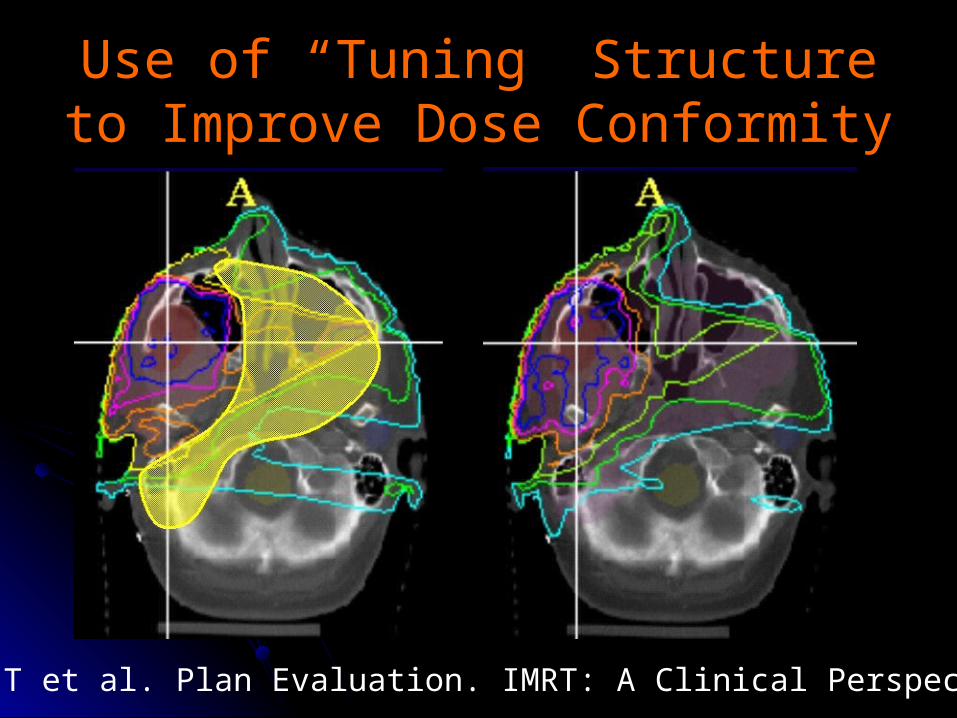
Use of “Tuning” Structure to Use of “Tuning” Structure to Improve Dose ConformityImprove Dose Conformity
Pawlicki T et al. Plan Evaluation. IMRT: A Clinical Perspective 2005
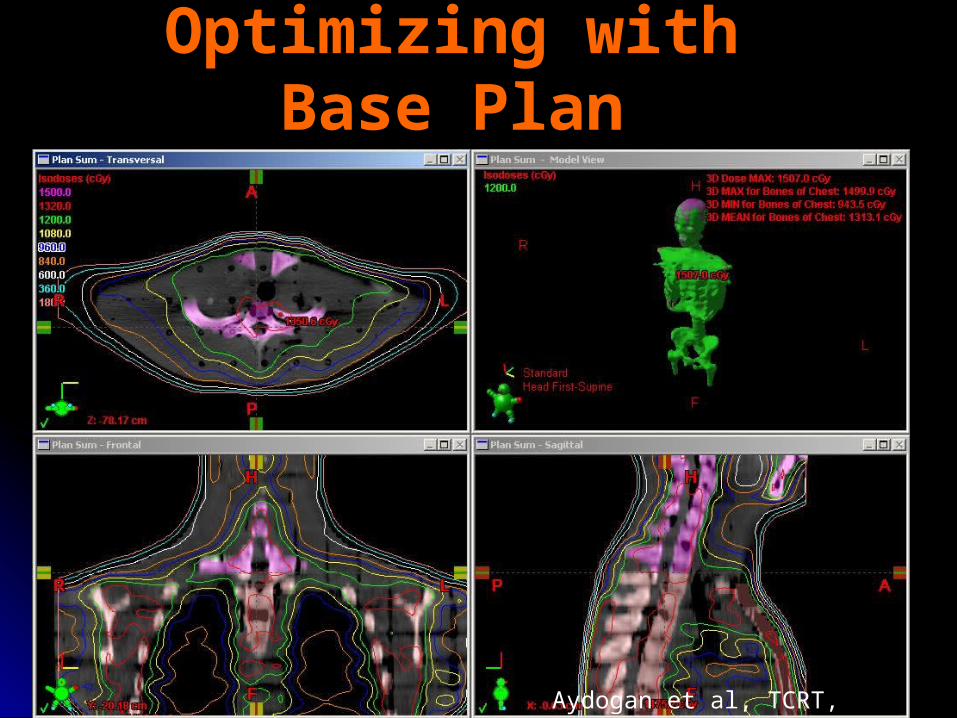
Optimizing with Optimizing with Base Plan Base Plan
Aydogan et al, TCRT, 2006
Fluence editingFluence editing
➫ It is very handy ➫Needs experience➫Exercise caution when using➫Works better for smaller hot
spots

IMRTIMRT for for
Gynecologic Gynecologic MalignanciesMalignancies
GYN IMRTGYN IMRT
➫Rationale☣Reduce volume of small bowel, bladder
and rectum irradiated☣Decrease volume of pelvic bone marrow
irradiated in patients receiving CRT☣Potentially useful in delivering higher than
conventional doses☣Alternative boost technique for patient
who are not amenable to BC
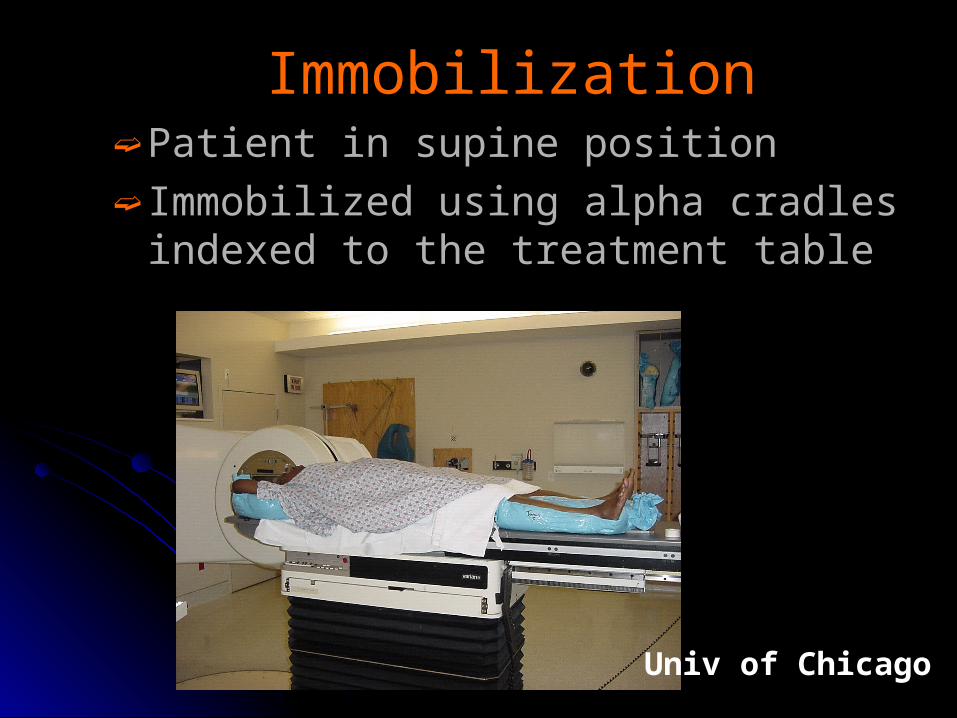
ImmobilizationImmobilization➫ Patient in supine position➫ Immobilized using alpha cradles
indexed to the treatment table
Univ of Chicago
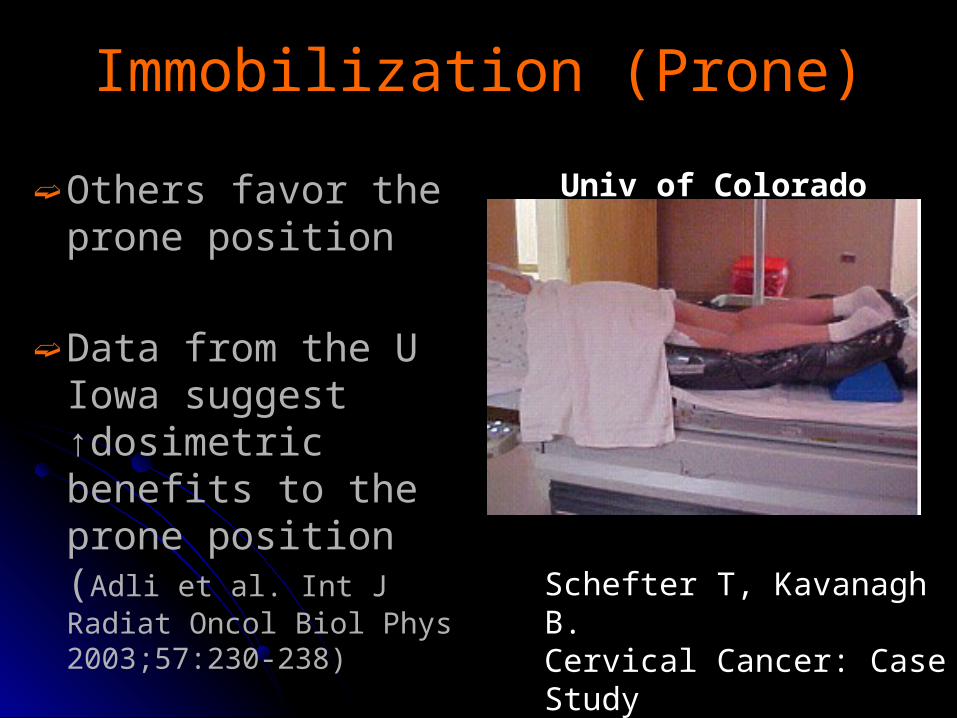
Immobilization (Prone)Immobilization (Prone)
➫ Others favor the prone position
➫ Data from the U Iowa suggest ↑dosimetric benefits to the prone position (Adli et al. Int J Radiat Oncol Biol Phys 2003;57:230-238)
Univ of Colorado
Schefter T, Kavanagh B.Cervical Cancer: Case Study IMRT: A Clinical Perspective 2005
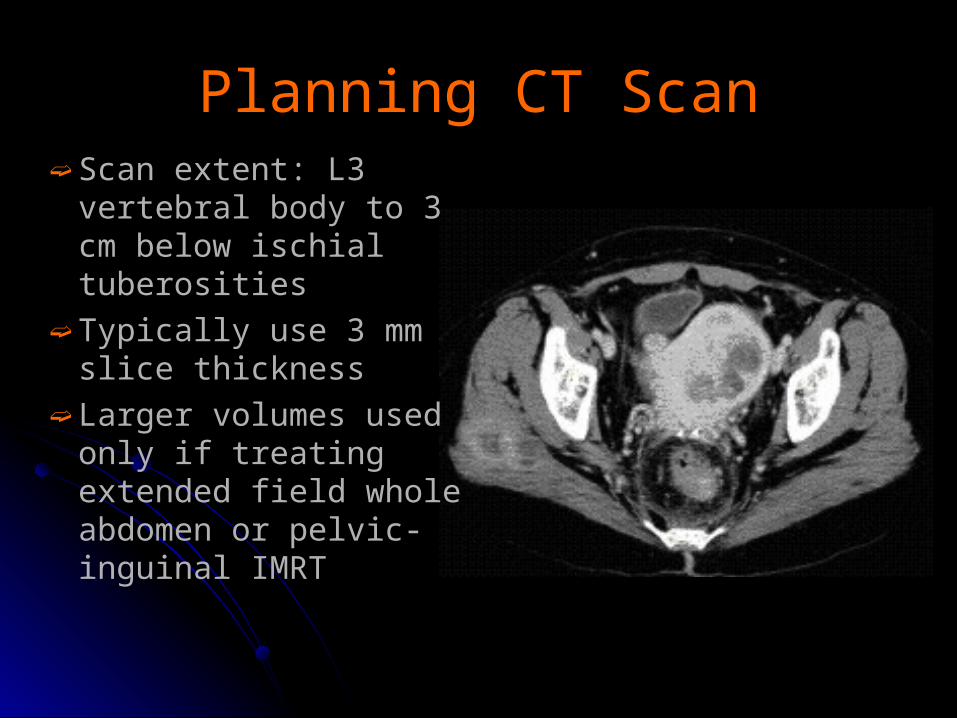
Planning CT ScanPlanning CT Scan➫ Scan extent: L3
vertebral body to 3 cm below ischial tuberosities
➫ Typically use 3 mm slice thickness
➫ Larger volumes used only if treating extended field whole abdomen or pelvic-inguinal IMRT
Contrast AdministrationContrast Administration
➫Oral, IV and rectal contrast are commonly used
➫ IV contrast is important to delineate vessels which serve as surrogates for lymph nodes
➫ Generally bladder contrast is not needed
Normal TissuesNormal Tissues
➫ Normal tissues delineated depends on the clinical case: In most cases, include:
Small bowel, rectum, bladder may be femoral heads
➫ In patients receiving concomitant or sequential chemotherapy, include the bone marrow (experimental)
➫ Kidneys and liver included only if treating more comprehensive fields
PTV ConsiderationsPTV Considerations➫ Organ motion in the inferior portion of the
CTV due to differential filling of the bladder and rectum
➫ Set-up uncertainty➫ Appropriate expansion remains unclear;
various reports ranging from 1 – 1.5 cm➫ At Univ of Chicago, we use a 1 cm
expansion➫ Less is known about normal tissues➫ Other centers (e.g., MD Anderson)
routinely expand normal tissues
Set-up UncertaintiesSet-up Uncertainties
➫ Dependent on type of immobilization➫ Therapist➫ University of Chicago immobilization: Alpha
cradle under legs and upper body with arms above head*
LR = 3.2 mm
SI = 3.7 mm
AP = 4.1 mm
* Haslam JJ et al. Med Dosim. 2005 Spring;30(1):36-42
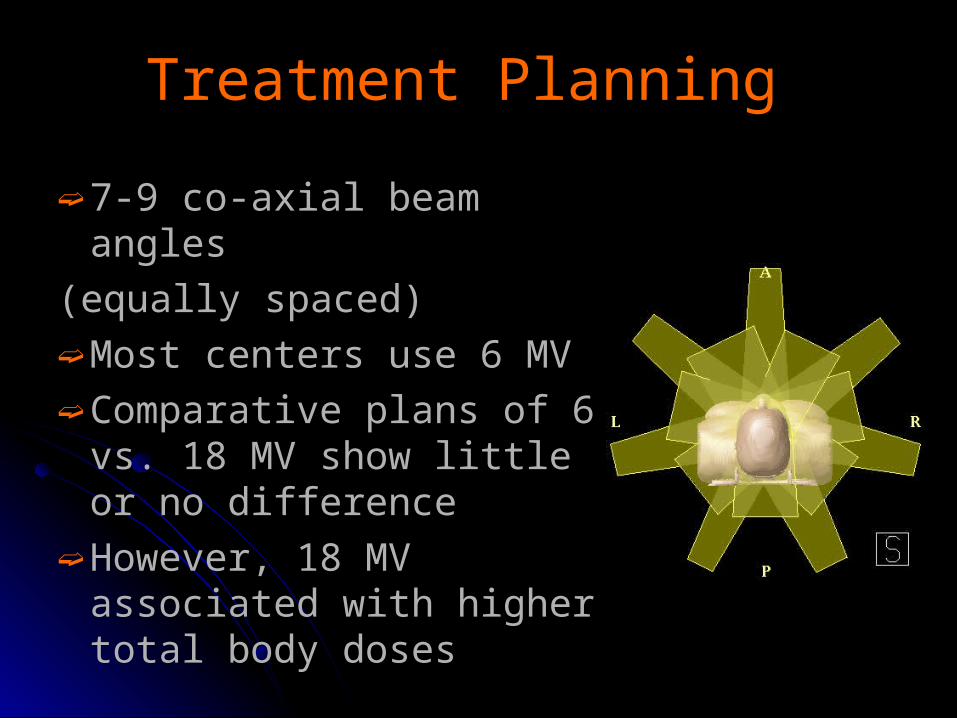
Treatment Planning Treatment Planning
➫ 7-9 co-axial beam angles
(equally spaced)➫ Most centers use 6 MV➫ Comparative plans of 6 vs.
18 MV show little or no difference
➫ However, 18 MV associated with higher total body doses
➫ Prescription dose: 45-50.4 Gy☣ 45 Gy in pts receiving vaginal brachytherapy☣ 45-50.4 Gy if external beam alone
➫ 1.8 Gy daily fractions ☣ Avoids hot spots > 2 Gy
➫ “Dose painting” (concomitant boost) remains experimental☣ Potentially useful in pts with high risk factors
(positive nodes and/or margins)
Treatment PlanningTreatment Planning
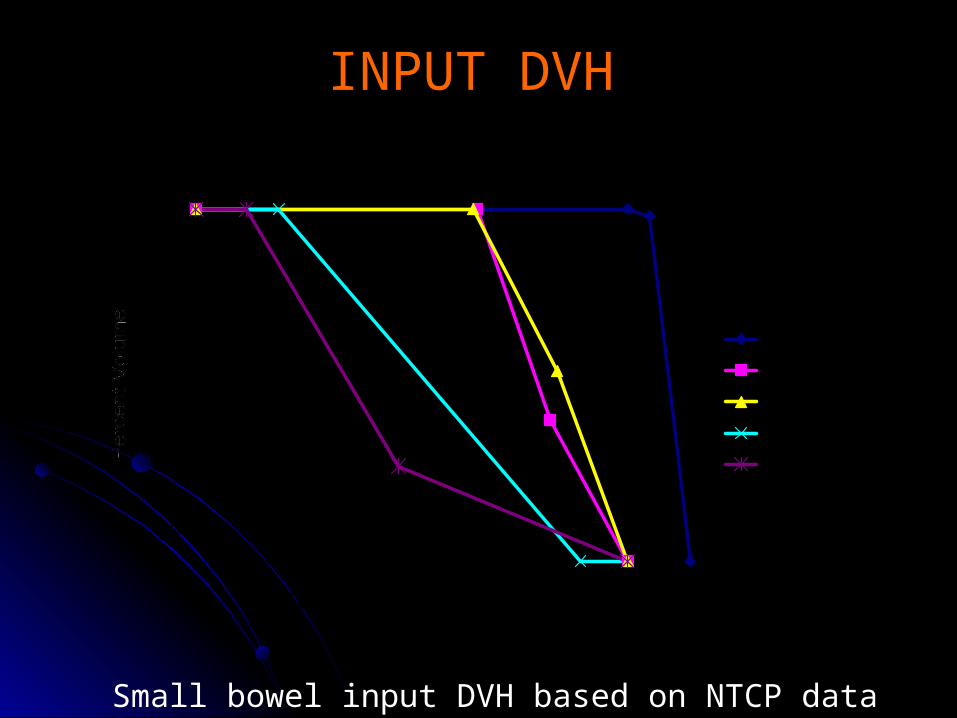
Gyne IMRT - Input DVHs
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50
Dose (Gy)
PTV
Bladder
Rectum
Small Bowel
Tissue
Small bowel input DVH based on NTCP data
INPUT DVH
2.3
100
4101
1
V
NTCP
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 100 200 300 400 500 600
Volume (cc)
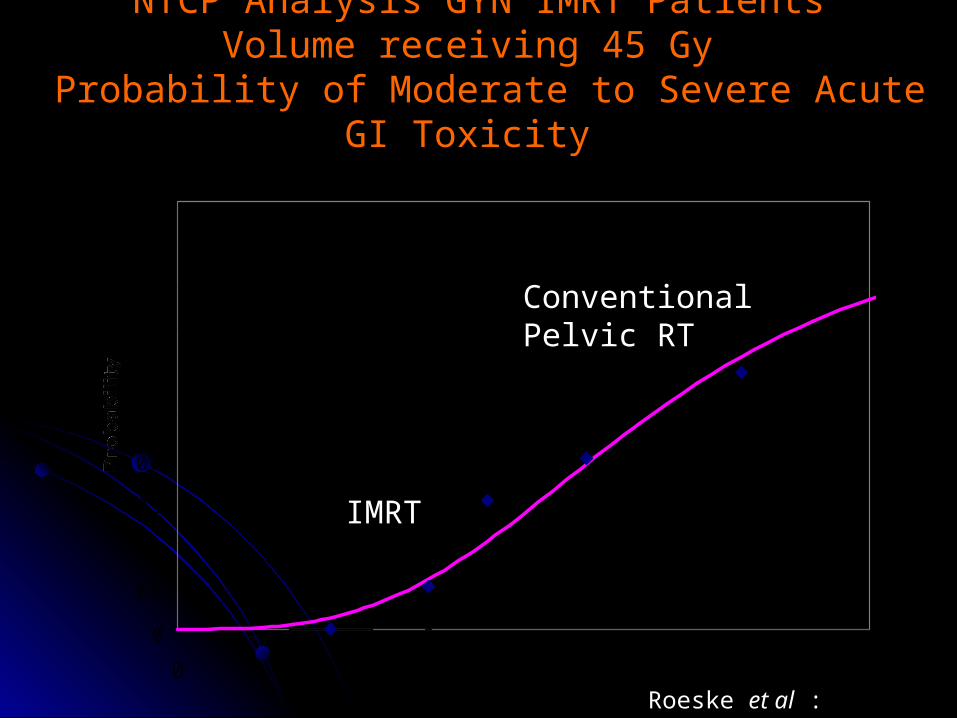
NTCP Analysis GYN IMRT PatientsNTCP Analysis GYN IMRT PatientsVolume receiving 45 Gy Volume receiving 45 Gy
Probability of Moderate to Severe Acute GI Toxicity Probability of Moderate to Severe Acute GI Toxicity
ConventionalPelvic RT
IMRT
Roeske et al : IJROB
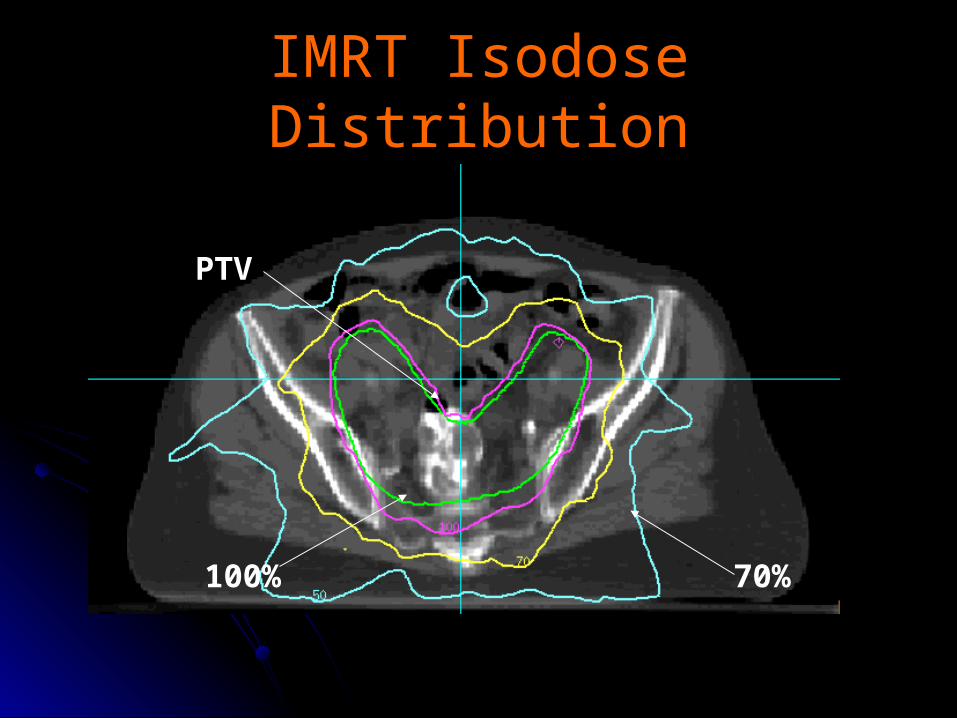
IMRT Isodose DistributionIMRT Isodose Distribution
PTV
100% 70%
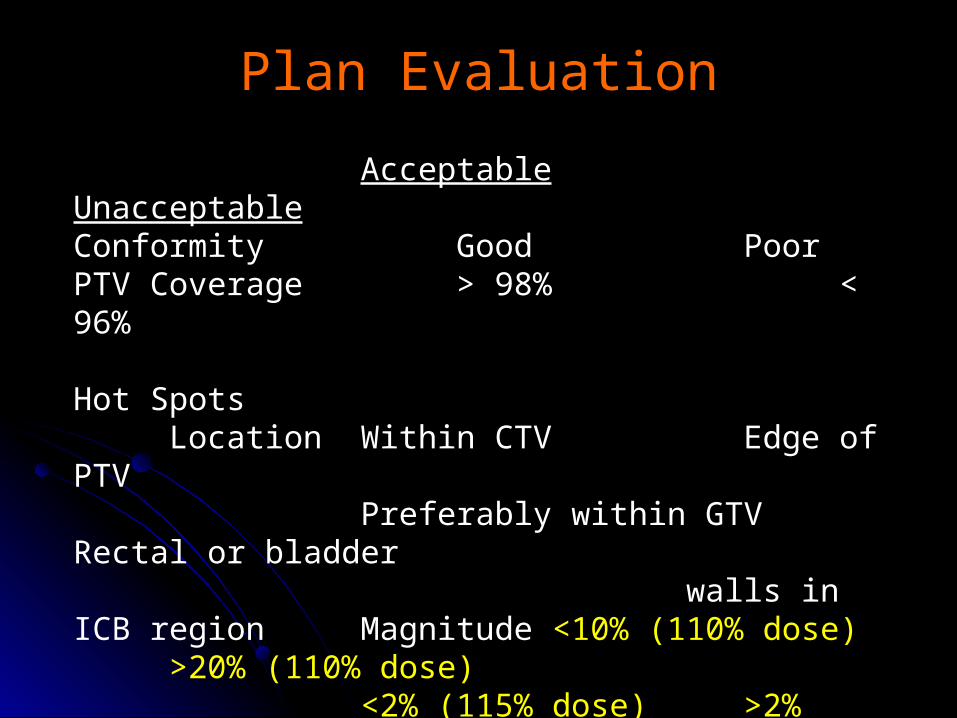
Acceptable UnacceptableConformity Good PoorPTV Coverage > 98% < 96%
Hot SpotsLocation Within CTV Edge of PTV
Preferably within GTV Rectal or bladder walls in ICB region
Magnitude <10% (110% dose) >20% (110% dose)<2% (115% dose) >2% (115% dose)
Cold SpotsLocation Edge of PTV Within CTV or GTVMagnitude <1% of the total dose none
Plan EvaluationPlan Evaluation
➫ A concern in the region of the vaginal cuff
➫ Two approaches are being studied at our institution to address this:☣ IGRT (CBCT)☣ Vaginal immobilization
➫ Now we simply avoid tight CTV volumes and use a 1 cm CTV→PTV expansion☣Produces very generous volumes
around the vaginal cuff
Organ MotionOrgan Motion
““Integrated Target Volume”Integrated Target Volume”
➫ A creative solution to the organ motion problem developed at MDAH
➫ Two planning scans: one with a full and one with an empty bladder
➫ Scans are then fused➫ An integrated target volume (ITV) is drawn
on the full bladder scan (encompassing the cuff and parametria on both scans)
➫ ITV is expanded by 0.5 cm → PTVITV
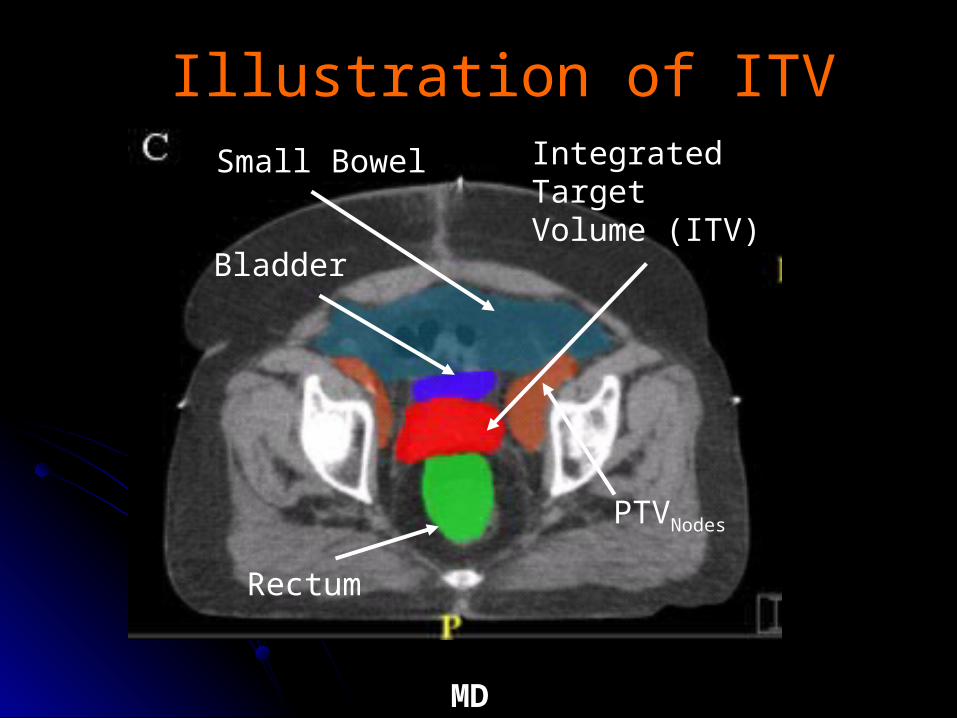
Small Bowel
Bladder
IntegratedTargetVolume (ITV)
PTVNodes
MD Anderson
Illustration of ITVIllustration of ITV
Rectum
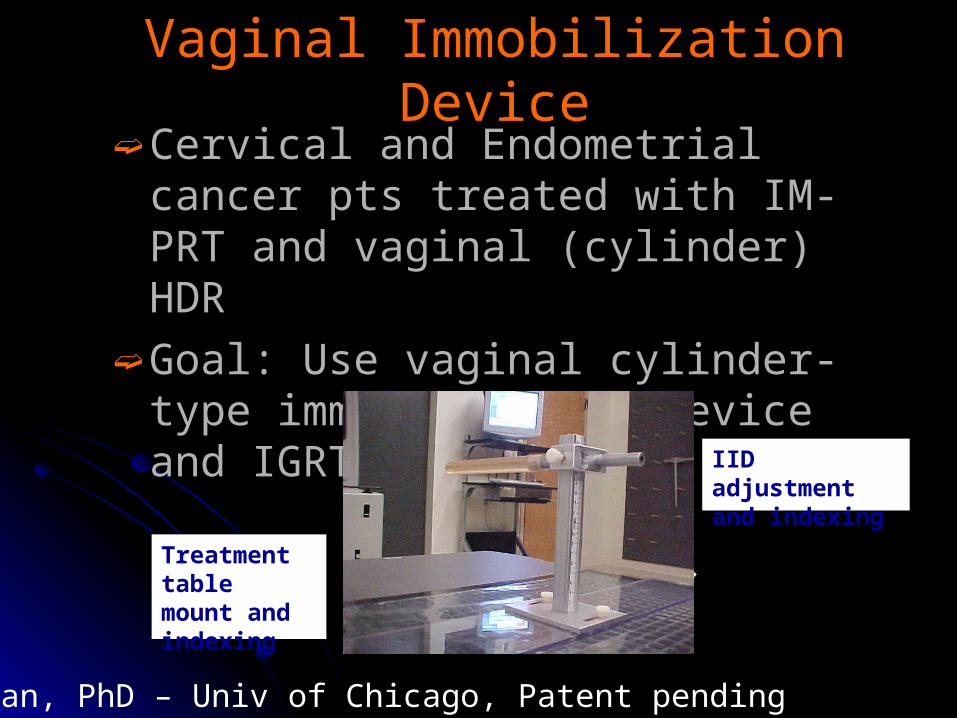
Vaginal Immobilization DeviceVaginal Immobilization Device➫ Cervical and Endometrial cancer pts
treated with IM-PRT and vaginal (cylinder) HDR
➫ Goal: Use vaginal cylinder-type immobilization device and IGRT
B Aydogan, PhD – Univ of Chicago, Patent pending
Treatment table mount and indexing
IID adjustment and indexing
Adaptive approach in Gynecologic Adaptive approach in Gynecologic IMRTIMRT
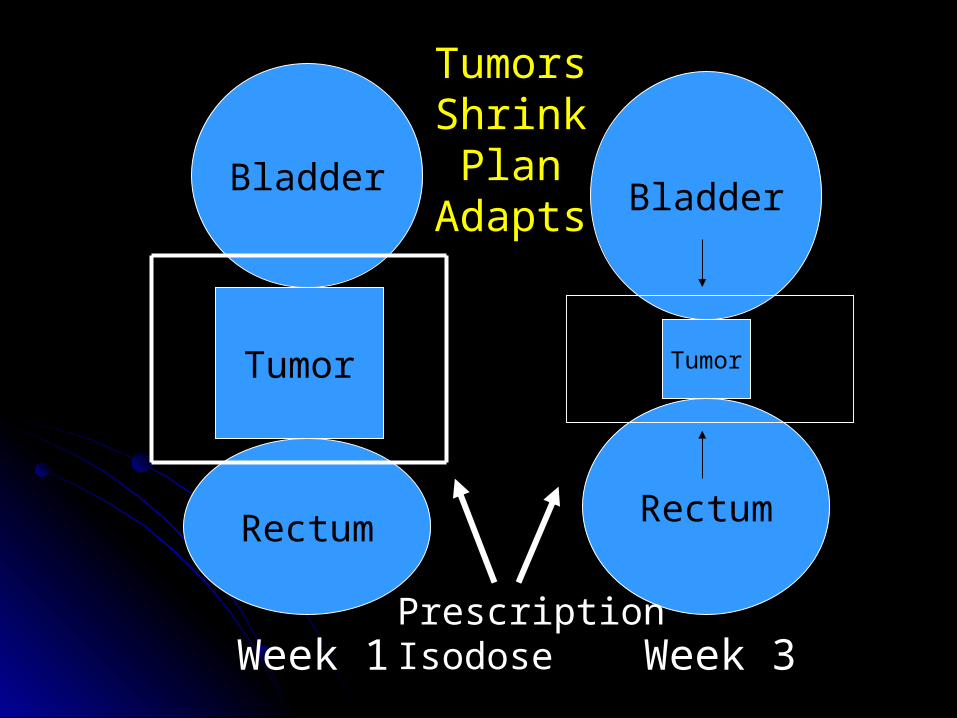
➫Many cervical tumors rapidly shrink during RT (especially with concomitant chemotherapy)
➫Tight margins (CTV-to-PTV expansions) early on may be too large by the end of treatment
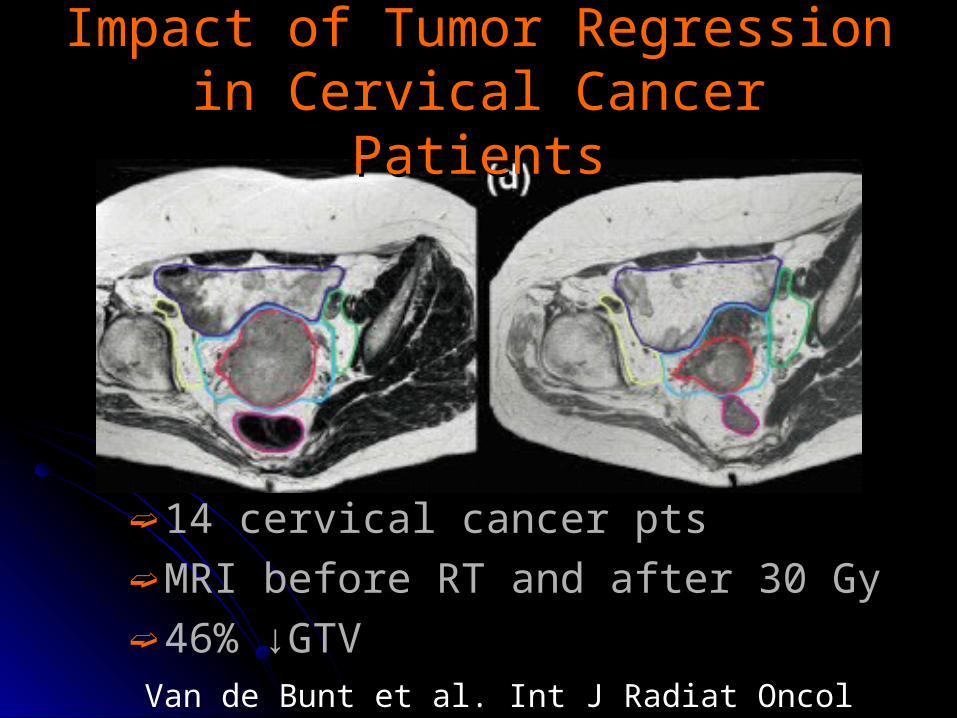
➫ 14 cervical cancer pts➫ MRI before RT and after 30 Gy➫ 46% ↓GTV
Impact of Tumor Regression in Impact of Tumor Regression in Cervical Cancer PatientsCervical Cancer Patients
Van de Bunt et al. Int J Radiat Oncol Biol Phys 64(1):189-96, 2006.
Bladder
Rectum
Tumor
Bladder
Tumor
Rectum
PrescriptionIsodoseWeek 1 Week 3
TumorsShrinkPlan
Adapts
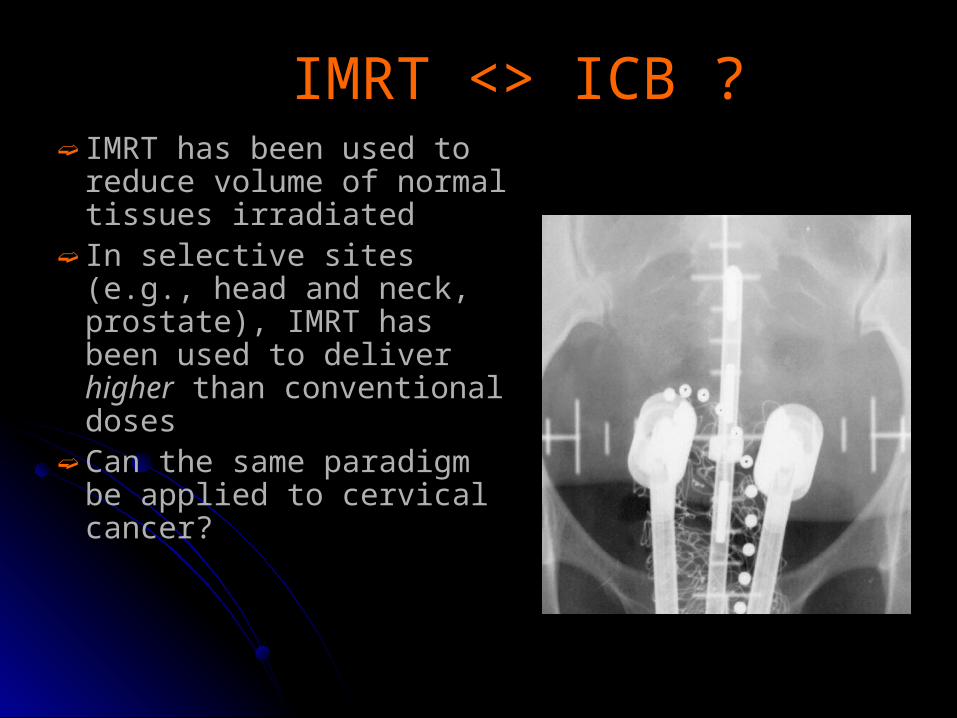
IMRT <> ICB ?IMRT <> ICB ?➫ IMRT has been used to
reduce volume of normal tissues irradiated
➫ In selective sites (e.g., head and neck, prostate), IMRT has been used to deliver higher than conventional doses
➫ Can the same paradigm be applied to cervical cancer?
ApproachesApproaches
➫ SRS Boost☣ Molla et al. Int J Radiat Oncol Biol Phys 62:
118-24, 2005.
➫ Vaginal Immobilization Device☣ Aydogan B. Int J Radiat Oncol Biol Phys
65:266-73, 2006.
➫ SIB☣ Guerrero M, et al. Int J Radiat Oncol Biol Phys
62(3):933-39, 2005.
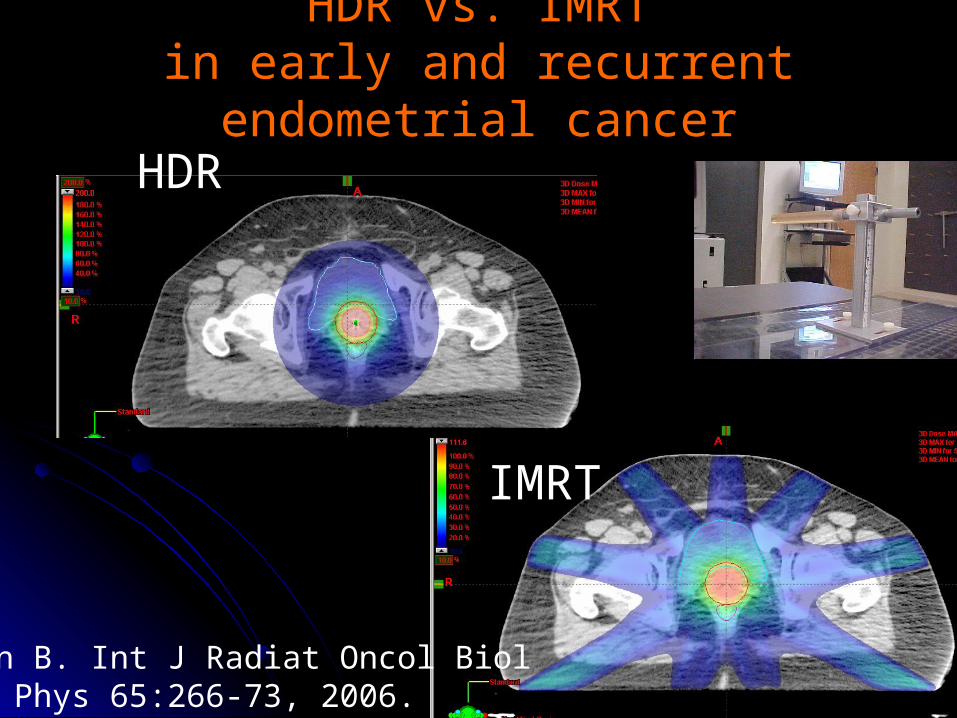
HDR vs. IMRTHDR vs. IMRTin early and recurrent endometrial cancerin early and recurrent endometrial cancer
Aydogan B. Int J Radiat Oncol Biol Phys 65:266-73, 2006.
HDR
IMRT
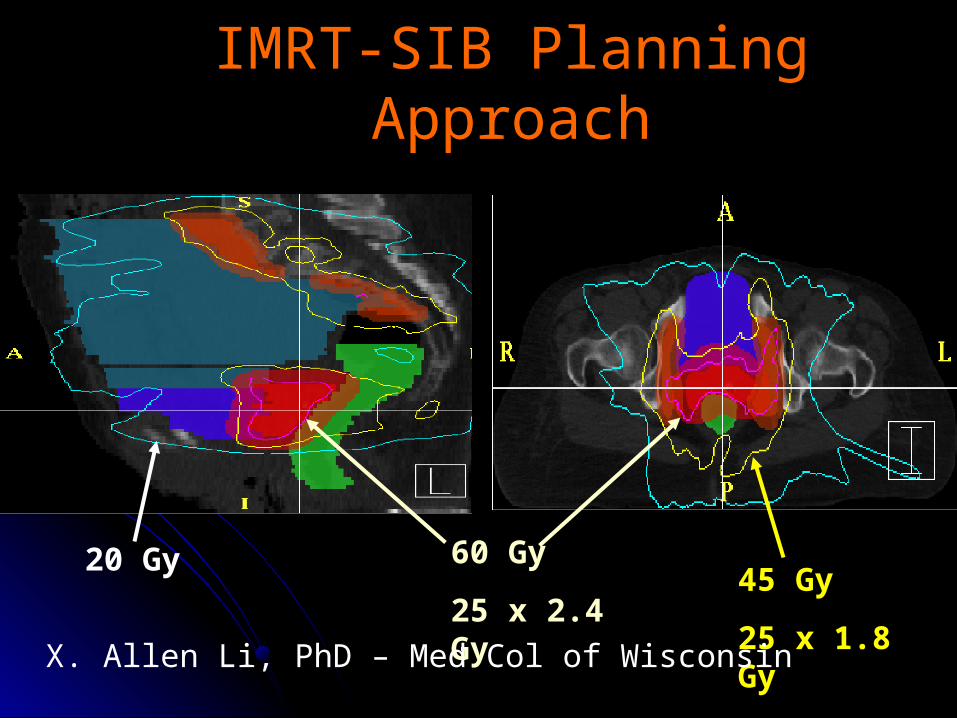
45 Gy
25 x 1.8 Gy
60 Gy
25 x 2.4 Gy
20 Gy
X. Allen Li, PhD – Med Col of Wisconsin
IMRT-SIB Planning IMRT-SIB Planning ApproachApproach
BMS-IMRTBMS-IMRT
➫Rationale☣CRT Improved tumor control and
survival ☣Increased toxicity in particular HT
ʚ Acute grade >2 HT is up to 50% more ʚ Acute grade >3 HT is up to 35% more
☣BMS-IMRT may reduce HT
Aydogan et al: IJROB, under review
ASTRO 2007 ARRO Poster # 2353
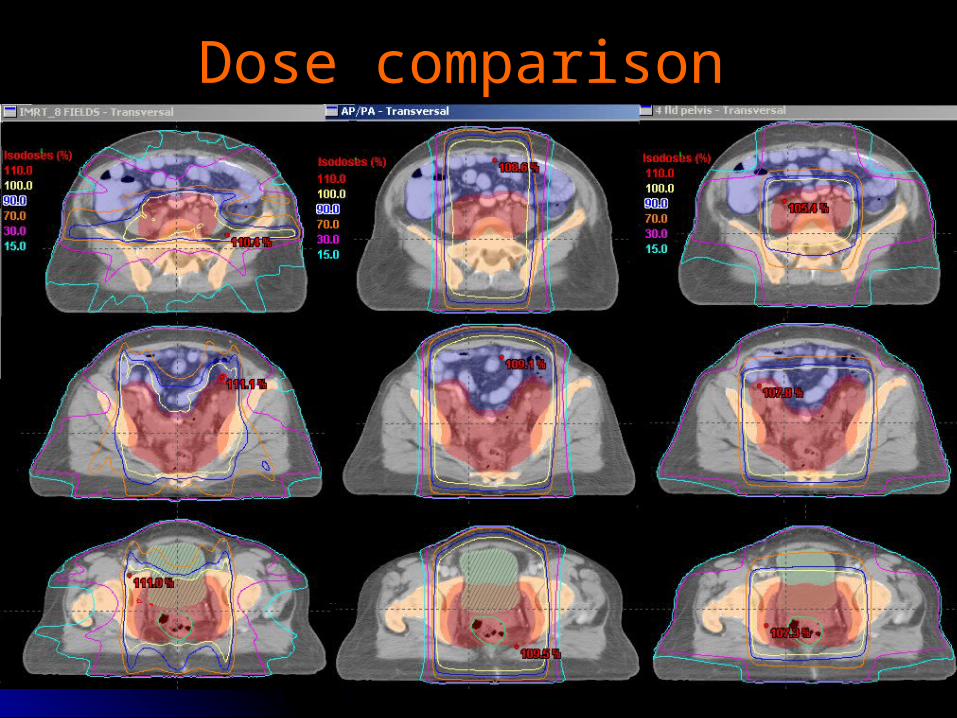
Dose comparison Dose comparison
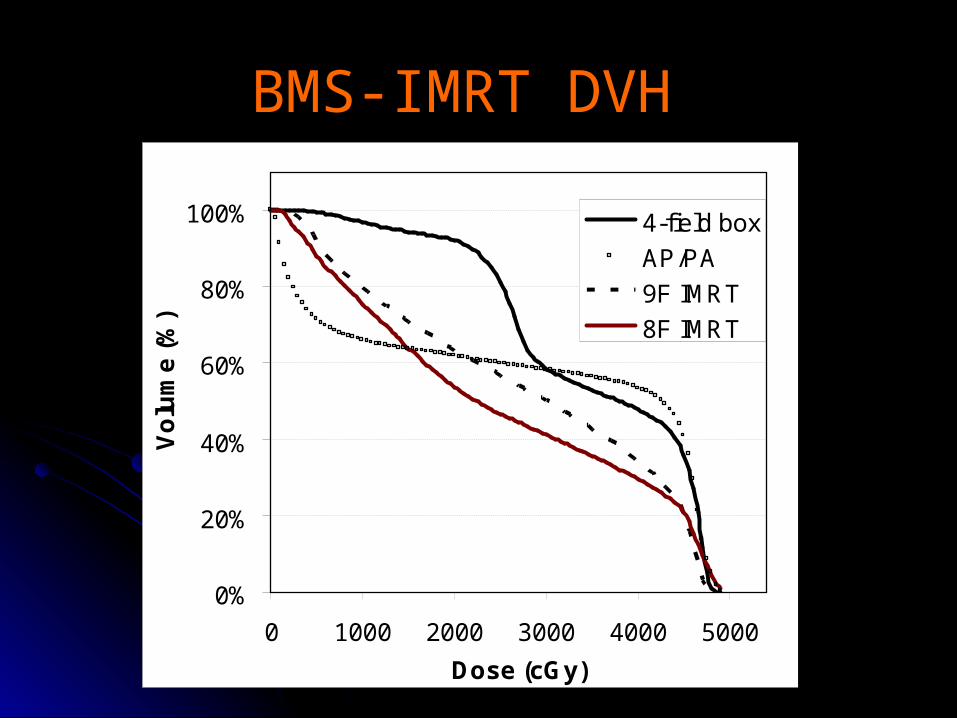
BMS-IMRT DVH BMS-IMRT DVH
0%
20%
40%
60%
80%
100%
0 1000 2000 3000 4000 5000
Dose (cGy)
Vo
lum
e (
%)
4-field box
AP/PA
9F IMRT
8F IMRT
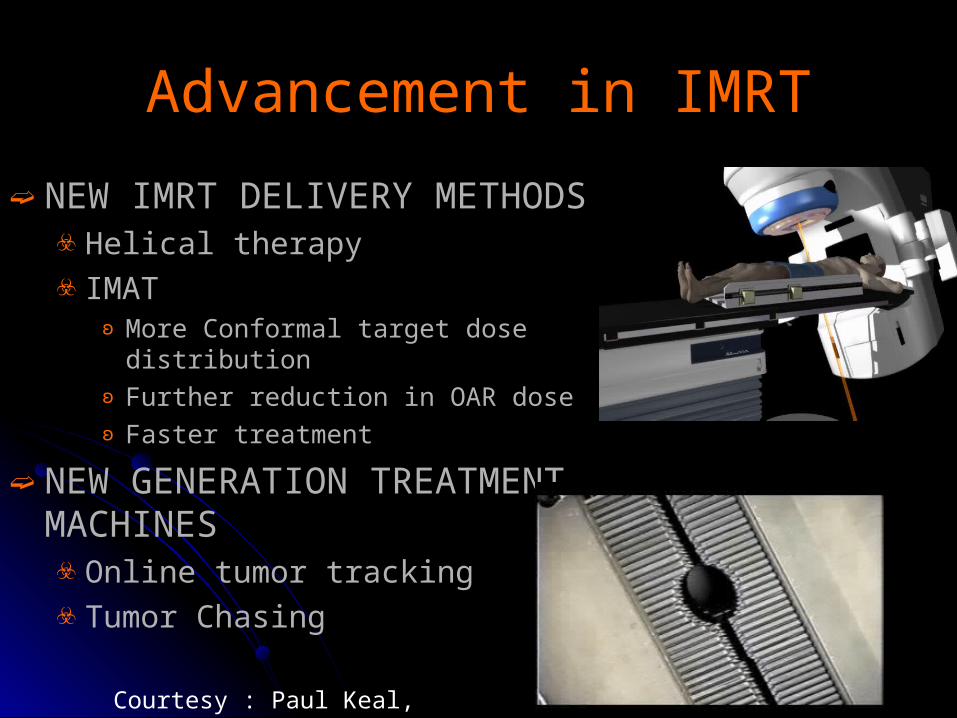
Advancement in IMRTAdvancement in IMRT
➫ NEW IMRT DELIVERY METHODS☣ Helical therapy☣ IMAT
ʚ More Conformal target dose distributionʚ Further reduction in OAR doseʚ Faster treatment
➫ NEW GENERATION TREATMENT MACHINES ☣ Online tumor tracking☣ Tumor Chasing
Courtesy : Paul Keal, Stanford Unv.
SummarySummary
➫ IMRT treatment planning is a multi-step process
➫ Careful consideration throughout the entire process is necessary to ensure that an optimal plan is achieved
➫ Decisions made at the time of simulation, target and tissue delineation, planning and the delivery/verification process itself impact the overall plan
SUMMARYSUMMARY➫ IGRT
☣Changing the way we do IMRTʚ Marginsʚ Biological targetingʚ Intrafraction vs. interfraction ʚ Organ management
٩ Gating , IID
ʚ Adaptation
☣Requires more resources and careful planning
THANKSTHANKS
➫John Roeske, PhD, Loyola University➫Arno J Mundt, MD, UCSD➫Loren K Mell, MD, Unv. of Chicago➫Brett Smith,MS, Unv. ofChicago➫Hanifi Tiryaki, PhD, Unv. of Illinois at Chicago
➫Joel Wilkie, PhD, Unv. of Chicago





























