Embed Size (px)
Citation preview

Clinical significance of increased tricuspid valve incompetencefollowing implantation of ventricular leads
Giselle A. Baquero & Pradeep Yadav & Joshua B. Skibba & Javier E. Banchs &
Latoya N. Linton-Frazier & Eugene J. Lengerich & Soraya M. Samii & Erica Penny-Peterson &
Deborah L. Wolbrette & Jerry C. Luck & Gerald V. Naccarelli & Mario D. Gonzalez
Received: 29 May 2013 /Accepted: 13 August 2013 /Published online: 11 September 2013# Springer Science+Business Media New York 2013
AbstractPurpose Cardiac rhythm management devices (CRMD) re-quire a ventricular lead to be placed across the tricuspid valve.Tricuspid regurgitation (TR) is an under-recognized clinicalcomplication of lead implantation and its clinical significanceis unknown. We studied the incidence of hospitalizations forcongestive heart failure (CHF) exacerbation among patientswith worsening TR after ventricular lead implantation.Methods We reviewed 148 patients (age 68±15) that receiveda CRMD. TR and pulmonary artery systolic pressure (PASP)measured by Doppler echocardiography before and afterCRMD implantation were analyzed. Hospitalizations forCHF exacerbation post-implantation were counted.Results Follow-up was 32±14 months. Ninety-nine (67 %)patients had no change, 24 (16 %) slight, and 9 (6 %) signif-icant increase in TR after CRMD implantation, while 13 (9%)patients had slight and 3 (2 %) significant improvement.Patients with a significant increase in TR had higher incidenceof hospitalizations (1.7±0.5) compared to patients with slight(0.8±1; p =0.006) or no increase (0.5±1; p =0.0002) in TR.Patients with significant increase in TR had a greater changein PASP (25 mmHg; p =0.002) after device implantationcompared to those with a slight (10 mmHg; p =0.002) or noincrease (0.7 mmHg; p =0.17).Conclusion Increased TR following CRMD implantation isrelatively common (33 %) and correlated with subsequent risk
of hospitalization for heart failure. A preventive strategy andclose monitoring for development or worsening of CHF afterCRMD implantation may help prevent hospital admissions.
Keywords Tricuspid regurgitation . Valve incompetence .
Cardiac rhythmmanagement devices . Ventricular leads
1 Introduction
Cardiac rhythm management devices (CRMD) require anendocardial ventricular lead to be placed across the tricuspidvalve. Tricuspid valve incompetence and regurgitation (TR)has been an under-recognized clinical complication of endo-cardial ventricular lead implantation, and its clinical signifi-cance is not fully known with some authors reporting it as arare phenomenon [1–4] and only a few recent studies account-ing its increased occurrence [5–9]. The incidence of hospital-izations for congestive heart failure (CHF) exacerbationamong patients that experienced worsening TR following aventricular lead implantation has not been reported. The pur-pose of this study was to evaluate the prevalence of TRfollowing the implantation of CRMD and its possible associ-ation with hospitalizations for CHF exacerbation.
2 Methods
After obtaining approval by the Penn State Hershey Institu-tional Review Board, we retrospectively reviewed 148 con-secutive patients who received a CRMD in our institution andhad transthoracic echocardiograms (TTEs) performed beforeand after device implantation. The following echocardio-graphic parameters were recorded: TR, pulmonary artery sys-tolic pressure (PASP), and ejection fraction (EF). The PASPwas calculated from the measured peak tricuspid valve jet
G. A. Baquero (*) : P. Yadav : J. B. Skibba : J. E. Banchs :L. N. Linton-Frazier : S. M. Samii : E. Penny-Peterson :D. L. Wolbrette : J. C. Luck :G. V. Naccarelli :M. D. GonzalezDepartment of Cardiology, Penn State College of Medicine, PennState Heart and Vascular Institute, Mail Code H047, 500 UniversityDrive, PO Box 850, Hershey, PA 17033, USAe-mail: [email protected]
E. J. LengerichDepartment of Public Health, Penn State College of Medicine,Hershey, PA, USA
J Interv Card Electrophysiol (2013) 38:197–202DOI 10.1007/s10840-013-9826-2

velocity adding an estimated right atrial pressure. The TR wasgraded according to the degree of severity proposed by theAmerican Society of Echocardiography as mild, moderate,and severe [10] and logged as reported by an expert echocar-diographer according to jet size on color Doppler, jet density,and contour by continuous wave Doppler and examination ofhepatic veins by pulsed wave Doppler. A scale of 0–4according to the grade of severity was used. The primaryend point of the study was to evaluate changes in the severityof TR after implantation of CRMD. Change in the severity ofTR was classified, corresponding with the changes in gradesof severity of TR, as follows: none (0), slight (1grade), andsignificant change (≥2 grade). The studies were performed inan accredited echocardiography laboratory by appropriatelytrained technicians and interpreted by board-certified expertechocardiographers blinded to the clinical history and devicetype. The secondary end point was hospitalizations for CHFexacerbation after device implantation. A detailed review ofthe electronic medical record pertaining to the patient’s sub-sequent inpatient and outpatient visits was performed foraccuracy. Change in pulmonary artery systolic pressure afterCRM implant was also evaluated. Baseline pulmonary hyper-tension was defined as PASP ≥35 mmHg before CRMD.
3 Statistical analysis
Continuous variables are presented as mean ± standard devi-ation. Comparison between groups was performed using aone-tailed paired Student’s t test and chi-square test for cate-gorical variables. A p value of <0.05 was considered statisti-cally significant.
4 Results
The study population consisted of 148 patients (age 68±15; 49women) that received a CRMD comprising implantablecardioverter defibrillators (ICD) (n=59; 40%), permanent pace-makers (PPM) (n=53; 36 %), and cardiac resynchronizationtherapy devices (CRT) (n =36; 24 %). All CRT devices wereCRT defibrillators. TTEs were performed before and after de-vice implantation. The average time elapsed between thesestudies was 29±15 months. Baseline TTE revealed an averageEF of 40±18 %, PASP of 40±15 mmHg, and TR of 1.1±0.7.Fifty patients (34 %) had trivial and two (1 %) had no TR atbaseline. Forty-nine (33 %) patients had preserved left ventric-ular systolic function. All patients were continued on optimalmedical therapy according to their underlying cardiac diagnosis,including beta-blockers (n=123; 83 %), angiotensin-convertingenzyme inhibitors/angiotensin receptor blockers (n =100;68 %), diuretics (n=85; 57 %) and/or digoxin (n=31; 21 %)after CRMD implantation (Table 1).
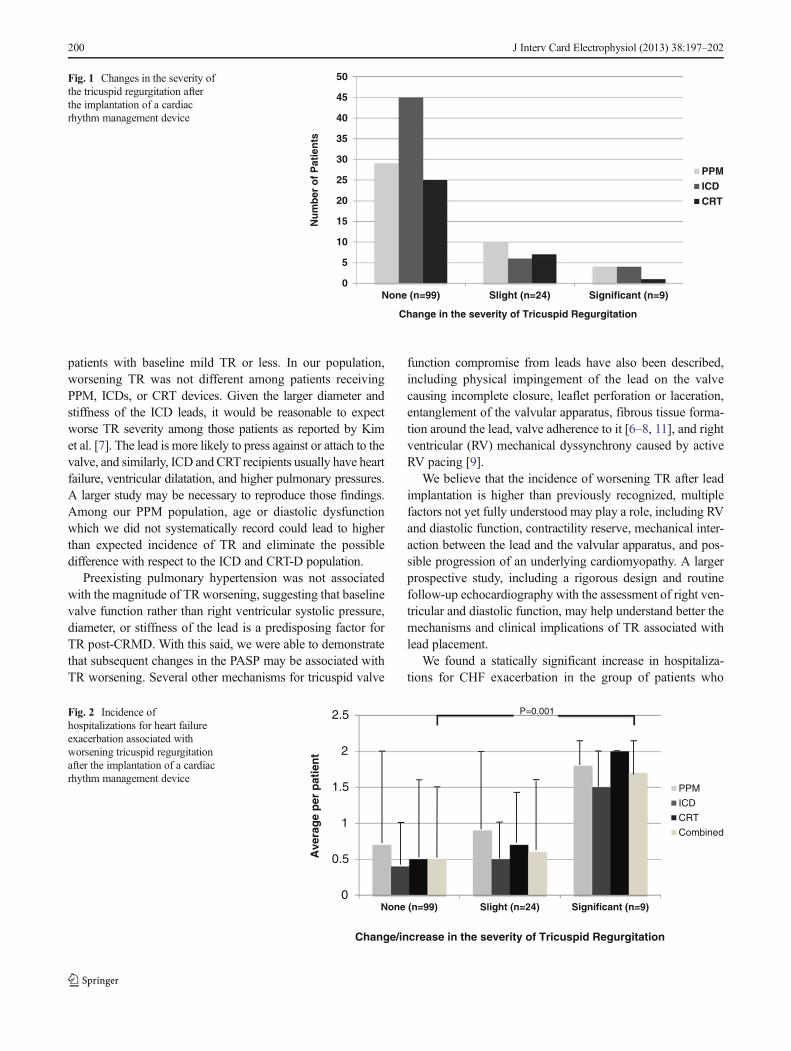
After a mean follow-up time of 32±14 months, 99 (67 %)patients had none, 24 (16 %) slight, and 9 (6 %) significantincrease in TR after device implantation (Table 2). Thirteen(9 %) patients had slight and three (2 %) significant improve-ment in TR after device implantation. One of the two patientsidentified as not having TR at baseline developed severe wors-ening in TR. None of the patients with trivial TR at baseline hadany degree of TR worsening after CRMD implantation. Eval-uation of increasing TR per type of device implanted revealedno difference between patients who received PPM, ICD, orCRT (ICD/CRT vs PPM, p =0.41; ICD vs PPM, p =0.42; ICDvs CRT, p =0.46; and CRT vs PPM, p =0.45) (Fig. 1).
A total of 81 hospital admissions for CHF exacerbation weredocumented, average 0.6±1 (0–5) per patient. Patients whoexperienced a significant increase in TR had higher incidenceof hospitalizations for CHF (1.7±0.5) compared to patients thathad a slight (0.8±1; p=0.006) or no increase (0.5±1; p=0.0002)in TR (Fig. 2). Patients with no change in TR had significantimprovement in EF (40±17 to 45±15 %; p=0.0003) in contrastto patients that experienced a slight (41±19 to 40±17 %;p=0.32) or significant increase in TR (43±12 to 36±13 %;p=0.07) (Table 2). There were 82 patients (55 %) with pulmo-nary hypertension at baseline. The mean PASP in this group was50±12 mmHg. A small improvement in PASP after CRMDimplantation (from 50±12 to 44±15 mmHg; p=0.001) wasnoted in this group. These patients had an average increase inthe severity of TR of 0.1±1.1 (from 1.3±0.7 to 1.5±0.9;p=0.07), not significantly different when compared to the in-crease in TR seen in patients with normal baseline PASP (0.3±0.7; p=0.001) (Table 2). Analysis of changes in PASP amongthe groups revealed that patients with a significant increase inTR had a statistically significant rise in PASP (Δ PASP25 mmHg; p =0.002) after device implantation, which wasalso present in those with slight worsening of TR (Δ PASP10mmHg; p =0.002). Individuals with no increase in TR had atrend towards lower PASP after CRMD (Δ PASP=0.7 mmHg;p =0.17).
5 Discussion
CRMD require an endocardial ventricular lead to be placedacross the tricuspid valve. Tricuspid valve incompetence andTR following CRMD has been an under-recognized andunderstudied clinical complication of endocardial ventricularlead implantation. The prevalence of this complication is notfully known with some authors asserting that the developmentof new or worsening TR after implantation of a CRMD is rare[1–4]. In a retrospective study of 20 patients using inferiorvena cava contrast reflux during systole as a marker of TR,Morgan et al. [1] reported no association between TR andventricular demand pacing. However, the study was limitedby lack of clinical information about the patients prior to PPM
198 J Interv Card Electrophysiol (2013) 38:197–202
implantation, small sample size, and prolonged amount oftime elapsed between the implantation date and post-implantation echocardiogram (mean 52 months). On the sameline, Kucukarslan et al. [2] after analyzing retrospective data
on 61 patients concluded that new or worsening TR is rareafter PPM implantation. Highlighted limitations of this reportincluded the small sample size and short period of timeelapsing from the implantation date to the follow-up echocar-diogram (mean 1±1 days). Leibowitz et al. [3] exposed sim-ilar findings in a small prospective study of 35 patients, andWebster et al. [4] with a larger sample of 123 pediatric patientsfound a minimal, but statistically significant change in TR,suggesting that there is little impact of transvenous leads onTR in growing children or patients with right-sided structuralheart disease.
Our findings suggest that worsening TR associated with theimplantation of CRMD is common with 25 % of our patientsdeveloping TR after the implantation of an endocardial ventric-ular lead, including 9 % acquiring moderate to severe TR, andconcur with other authors that have reported increased occur-rence of TR related to ventricular leads [5–9], includingPanigua et al. [5] who reported an increase in the prevalenceof moderate to severe TR in patients with transvenous PMcompared to an age- and sex-matched control group, Linet al. [6] who in 2005 presented 41 patients with severe TRdue to PPM or ICD lead placement requiring tricuspid valvesurgery, and Kim et al. [7] who assessed the effect of trans-tricuspid placement of PPM and ICD leads on TR in 248patients with echocardiograms before and after implant. Theyreported development of TR in 21.2 % and severe TR in 3.9 %of patients with initially normal tricuspid valves, concludingthat TRworsening was more commonwith ICDs than PPMs in
Table 1 Patient clinical characteristics
Patient characteristics
Patients 148
Age 68±15
Male/female 99/49
Baseline ejection fraction (%) 40±18
Pulmonary artery systolic pressure (mmHg) 40±15
Baseline TR
No TR (0) 2 (1.3 %)
Trivial TR (0.5) 50 (34 %)
Mild TR (1) 71 (48 %)
Moderate TR (2) 21 (14 %)
Severe TR (>3) 4 (2.7 %)
Average TR (0–4) 1.1±0.7
Medications
Beta-blocker 123 (83 %)
Acetyl cholinesterase inhibitors 100 (68 %)
Spironolactone/eplerenone 30 (20 %)
Vasodilators 28 (19 %)
Diuretics 85 (57 %)
Digoxin 31 (21 %)
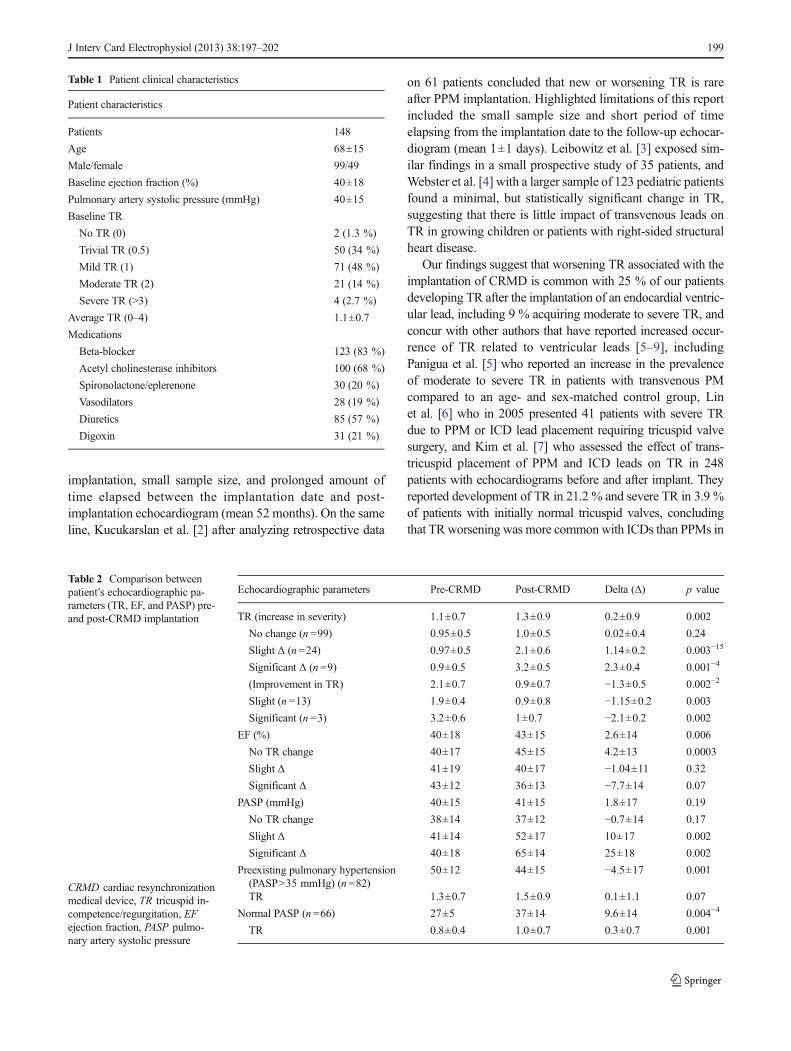
Table 2 Comparison betweenpatient’s echocardiographic pa-rameters (TR, EF, and PASP) pre-and post-CRMD implantation
CRMD cardiac resynchronizationmedical device, TR tricuspid in-competence/regurgitation, EFejection fraction, PASP pulmo-nary artery systolic pressure
Echocardiographic parameters Pre-CRMD Post-CRMD Delta (Δ) p value
TR (increase in severity) 1.1±0.7 1.3±0.9 0.2±0.9 0.002
No change (n =99) 0.95±0.5 1.0±0.5 0.02±0.4 0.24
Slight Δ (n =24) 0.97±0.5 2.1±0.6 1.14±0.2 0.003−15
Significant Δ (n =9) 0.9±0.5 3.2±0.5 2.3±0.4 0.001−4
(Improvement in TR) 2.1±0.7 0.9±0.7 −1.3±0.5 0.002−2
Slight (n =13) 1.9±0.4 0.9±0.8 −1.15±0.2 0.003
Significant (n =3) 3.2±0.6 1±0.7 −2.1±0.2 0.002
EF (%) 40±18 43±15 2.6±14 0.006
No TR change 40±17 45±15 4.2±13 0.0003
Slight Δ 41±19 40±17 −1.04±11 0.32
Significant Δ 43±12 36±13 −7.7±14 0.07
PASP (mmHg) 40±15 41±15 1.8±17 0.19
No TR change 38±14 37±12 −0.7±14 0.17
Slight Δ 41±14 52±17 10±17 0.002
Significant Δ 40±18 65±14 25±18 0.002
Preexisting pulmonary hypertension(PASP>35 mmHg) (n =82)
50±12 44±15 −4.5±17 0.001
TR 1.3±0.7 1.5±0.9 0.1±1.1 0.07
Normal PASP (n =66) 27±5 37±14 9.6±14 0.004−4
TR 0.8±0.4 1.0±0.7 0.3±0.7 0.001
J Interv Card Electrophysiol (2013) 38:197–202 199
patients with baseline mild TR or less. In our population,worsening TR was not different among patients receivingPPM, ICDs, or CRT devices. Given the larger diameter andstiffness of the ICD leads, it would be reasonable to expectworse TR severity among those patients as reported by Kimet al. [7]. The lead is more likely to press against or attach to thevalve, and similarly, ICD and CRT recipients usually have heartfailure, ventricular dilatation, and higher pulmonary pressures.A larger study may be necessary to reproduce those findings.Among our PPM population, age or diastolic dysfunctionwhich we did not systematically record could lead to higherthan expected incidence of TR and eliminate the possibledifference with respect to the ICD and CRT-D population.
Preexisting pulmonary hypertension was not associatedwith the magnitude of TR worsening, suggesting that baselinevalve function rather than right ventricular systolic pressure,diameter, or stiffness of the lead is a predisposing factor forTR post-CRMD. With this said, we were able to demonstratethat subsequent changes in the PASP may be associated withTR worsening. Several other mechanisms for tricuspid valve
function compromise from leads have also been described,including physical impingement of the lead on the valvecausing incomplete closure, leaflet perforation or laceration,entanglement of the valvular apparatus, fibrous tissue forma-tion around the lead, valve adherence to it [6–8, 11], and rightventricular (RV) mechanical dyssynchrony caused by activeRV pacing [9].
We believe that the incidence of worsening TR after leadimplantation is higher than previously recognized, multiplefactors not yet fully understood may play a role, including RVand diastolic function, contractility reserve, mechanical inter-action between the lead and the valvular apparatus, and pos-sible progression of an underlying cardiomyopathy. A largerprospective study, including a rigorous design and routinefollow-up echocardiography with the assessment of right ven-tricular and diastolic function, may help understand better themechanisms and clinical implications of TR associated withlead placement.
We found a statically significant increase in hospitaliza-tions for CHF exacerbation in the group of patients who
0
5
10
15
20
25
30
35
40
45
50
None (n=99) Slight (n=24) Significant (n=9)
PPMICDCRT
Nu
mb
er o
f P
atie
nts
Change in the severity of Tricuspid Regurgitation
Fig. 1 Changes in the severity ofthe tricuspid regurgitation afterthe implantation of a cardiacrhythm management device
0
0.5
1
1.5
2
2.5
None (n=99) Slight (n=24) Significant (n=9)
PPM
ICD
CRT
Combined
Ave
rag
e p
er p
atie
nt
Change/increase in the severity of Tricuspid Regurgitation
P=0.001Fig. 2 Incidence ofhospitalizations for heart failureexacerbation associated withworsening tricuspid regurgitationafter the implantation of a cardiacrhythm management device
200 J Interv Card Electrophysiol (2013) 38:197–202

experienced a significant increase in TR when compared tothe patients with a slight (1.7±0.5 vs 0.9±1; p =0.006) or noincrease in TR (1.7±0.5 vs 0.5±1; p =0.0002) after CRMDimplantation (Fig. 2). This cohort is the first report on theincidence of hospitalizations for CHF exacerbation amongpatients with worsening of TR after implantation of CRMD.Based on our findings, it may be important to consider closerfollow-up of these patients given their increased risk of sub-sequent hospitalization. It seems logical that mechanical in-terference with the closure of the tricuspid valve leaflets is themechanism for worsening TR, and baseline elevated pulmo-nary pressures predispose to more severe TR. Nevertheless,cardiac disease, either conduction disease or myopathy, isinherent of the patient population who has indications forCRMD. We speculate that the worsening TR documented inthese patients could also be, to some degree, a result of thenatural progression of the cardiovascular disease that led to theCRMD indication on the first place. This may be particularlytrue for the CHF patients which represent 51 % of our studypopulation, and it is supported by the finding that PASPincreased in patients with worsening TR in contrast to thosewith no change in TR which not only showed a trend towardsreduction in PASP, but a modest improvement in EF. Surpris-ingly, there was a small subset of 16 patients (11 %) thatdemonstrated improvement in the severity of the TR afterreceiving a CRMD (Table 2). Themechanism of improvementin TR among those patients is no entirely clear, but wespeculate that it may be related to hemodynamic improve-ments derived from either restoration of AV synchrony withpacing or simultaneous diuresis and optimization of medicaltherapy at the time of CRM implant.
Our findings seem to suggest that patients who receiveCRMD frequently are at a vulnerable time in the progressionof their cardiovascular disease. Many of these patients maybenefit from preventive or early heart failure interventions,including sodium restriction, daily weight monitoring, closeclinical follow-up, and possibly up-titration of pharmacologi-cal therapy. Results intriguing that CRT recipients had nodifference in development of worsening TR when comparedto patients who received PPMs or ICDs since the improvementin CHF derived from CRT could be expected to reduce PASPand the severity of TR. One possible explanation is the variableseverity of CHF in our CRT patients as well as the variableresponse that individuals may experience after CRT. Anotherexplanation is the small representation of CRT (36 patients).
6 Limitations
The study is based on a retrospective analysis of 148 patients;therefore, a larger prospective clinical study may be needed tofully understand TR after CRMD implantation. A larger num-ber of patients from our institution could not be included as they
were lacking appropriate post-CRMD implantation echocardio-graphic studies. A selection bias is possible in our population,since patients with symptoms or worse functional status aremore likely to have follow-up studies. This may bias ourfindings to a higher prevalence of worsening TR after CRMDimplantation. Significant intra-observer and inter-observer var-iability is observed among readers of echocardiography studies,and this could represent an unmeasured cofounder.
7 Conclusion
Increased TR following a CRMD implantation is relativelycommon (33 out of 148 implants, 22 %) and correlated withsubsequent risk of hospitalization for heart failure. Lead-related valve incompetence and preexisting valve incompe-tence, rather than pulmonary hypertension or device type,contribute to worsening TR after CRMD implantation. Apreventive strategy and close monitoring for the developmentor worsening of CHF after CRMD implantation may helpprevent hospital admissions.
References
1. Morgan, D. E., Norman, R., West, R. O., & Burggraf, G. (1986).Echocardiographic assessment of tricuspid regurgitation during ven-tricular demand pacing. The American Journal of Cardiology,58(10), 1025–1029.
2. Kucukarslan, N., Kirilmaz, A., Ulusoy, E., Yokusoglu, M.,Gramatnikovski, N., Ozal, E., & Tatar, H. (2006). Tricuspid insuffi-ciency does not increase early after permanent implantation of pace-maker leads. Journal of Cardiac Surgery, 21(4), 391–394.
3. Leibowitz, D. W., Rosenheck, S., Pollak, A., Geist, M., & Gilon, D.(2000). Transvenous pacemaker leads do not worsen tricuspid regur-gitation: a prospective echocardiographic study. Cardiology, 93(1–2),74–77.
4. Webster, G., Margossian, R., Alexander, M. E., Cecchin, F.,Triedman, J. K., Walsh, E. P., & Berul, C. I. (2008). Impact oftransvenous ventricular pacing leads on tricuspid regurgitation inpediatric and congenital heart disease patients. Journal ofInterventional Cardiac Electrophysiology, 21(1), 65–68.
5. Paniagua, D., Aldrich, H. R., Lieberman, E. H., Lamas, G. A., &Agatston, A. S. (1998). Increased prevalence of significant tricuspidregurgitation in patients with transvenous pacemakers leads. TheAmerican Journal of Cardiology, 82(9), 1130–1132. A9.
6. Lin, G., Nishimura, R. A., Connolly, H. M., Dearani, J. A., Sundt, T.M., 3rd, & Hayes, D. L. (2005). Severe symptomatic tricuspid valveregurgitation due to permanent pacemaker or implantablecardioverter-defibrillator leads. Journal of the American College ofCardiology, 45(10), 1672–1675.
7. Kim, J. B., Spevack, D. M., Tunick, P. A., Bullinga, J. R., Kronzon, I.,Chinitz, L. A., & Reynolds, H. R. (2008). The effect of transvenouspacemaker and implantable cardioverter defibrillator lead placementon tricuspid valve function: an observational study. Journal of theAmerican Society of Echocardiography, 21(3), 284–287.
8. Klutstein, M., Balkin, J., Butnaru, A., Ilan, M., Lahad, A., &Rosenmann, D. (2009). Tricuspid incompetence following permanent
J Interv Card Electrophysiol (2013) 38:197–202 201

pacemaker implantation. Pacing and Clinical Electrophysiology,32(Suppl 1), S135–S137.
9. Vaturi, M., Kusniec, J., Shapira, Y., Nevzorov, R., Yedidya, I.,Weisenberg, D., Monakier, D., Strasberg, B., & Sagie, A. (2010).Right ventricular pacing increases tricuspid regurgitation grade re-gardless of the mechanical interference to the valve by the electrode.European Journal of Echocardiography, 11(6), 550–553.
10. Zoghbi, W. A., Enriquez-Sarano, M., Foster, E., Grayburn, P. A.,Kraft, C. D., Levine, R. A., Nihoyannopoulos, P., Otto, C. M.,
Quinones, M. A., Rakowski, H., Stewart, W. J., Waggoner, A.,Weissman, N. J., & American Society of Echocardiography. (2003).Recommendations for evaluation of the severity of native valvularregurgitation with two-dimensional and Doppler echocardiography.Journal of the American Society of Echocardiography, 16(7), 777–802.
11. Robboy, S. J., Harthorne, J. W., Leinbach, R. C., Sanders, C. A., &Austen, W. G. (1969). Autopsy findings with permanent pervenouspacemakers. Circulation, 39(4), 495–501.
202 J Interv Card Electrophysiol (2013) 38:197–202