Embed Size (px)
Citation preview
665
CLINICAL SECTIONCLINICO-PATHOLOGICAL CONFERENCE-No. 9*
A Case of Obstructive Jaundice
AA
'VV,
44
NID
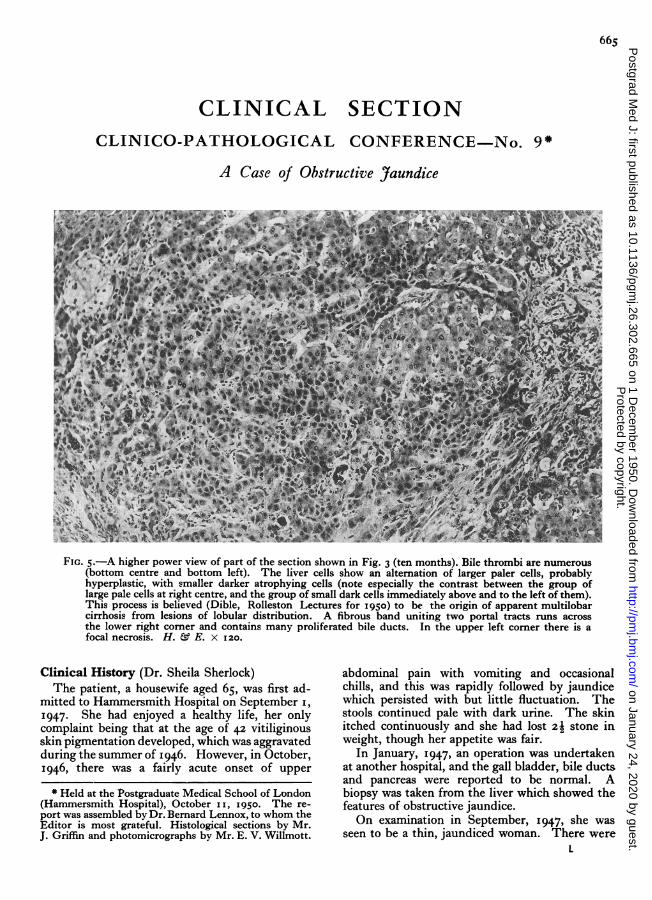
FIG. 5.-A higher power view of part of the section shown in Fig. 3 (ten months). Bile thrombi are numerous(bottom centre and bottom left). The liver cells show an altemation of larger paler cells, probablyhyperplastic, with smaller darker atrophying cells (note especially the contrast between the group oflarge pale cells at right centre, and the group of small dark cells immediately above and to the left of them).This process is believed (Dible, Rolleston Lectures for 1950) to be the origin of apparent multilobarcirrhosis from lesions of lobular distribution. A fibrous band uniting two portal tracts runs acrossthe lower right comer and contains many proliferated bile ducts. In the upper left comer there is afocal necrosis. H. & E. x 120.
Clinical History (Dr. Sheila Sherlock)The patient, a housewife aged 65, was first ad-
mitted to Hammersmith Hospital on September i,1947. She had enjoyed a healthy life, her onlycomplaint being that at the age of 42 vitiliginousskin pigmentation developed, which was aggravatedduring the summer of I946. However, in October,I946, there was a fairly acute onset of upper
* Held at the Postgraduate Medical School of London(Hammersmith Hospital), October i i, I950. The re-port was assembled by Dr. Bernard Lennox, to whom theEditor is most grateful. Histological sections by Mr.J. Griffin and photomicrographs by Mr. E. V. Willmott.
abdominal pain with vomiting and occasionalchills, and this was rapidly followed by jaundicewhich persisted with but little fluctuation. Thestools continued pale with dark urine. The skinitched continuously and she had lost 2j stone inweight, though her appetite was fair.
In January, 1947, an operation was undertakenat another hospital, and the gall bladder, bile ductsand pancreas were reported to be normal. Abiopsy was taken from the liver which showed thefeatures of obstructive jaundice.On examination in September, 1947, she was
seen to be a thin, jaundiced woman. There wereL
Protected by copyright.
on January 24, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.302.665 on 1 Decem
ber 1950. Dow
nloaded from
666 POSTGRADUATE MEDICAL JOURNAL December 1950
scratch marks on the skin; the forearms, neck andtrunk showed alternating patches of light and darkskin and this was interpreted as vitiligo. Theblood pressure was I26/78. The liver was enlargedto the umbilicus, the edge was firm and the surfacesmooth. The spleen was just palpable. Ascitescould not be clinically detected. Rectal examina-tion demonstrated piles. Urine showed per-sistent absence of urobilin; bile pigments werepresent. The faeces were always acholic. Bio-chemical investigations during the course of theillness are shown in the table.
Haematological examination showed haemo-globin 13.4 g. per cent., red blood corpuscles were4,ooo,ooo per c.mm., white blood count 8,ooo perc.mm., prothrombin time 85 per cent. of normal,and the erythrocyte sedimentation rate was 105mm. in an hour. Radiologically the wrist boneswere normally calcified. A biopsy of the skinshowed some excess pigment in the deeper layersbut was otherwise normal. An aspiration liverbiopsy was pe'rforimed and during this a littleascitic fluid was aspirated. Hepatic sectionsshowed considerable biliary cirrhosis.
Clinical and biochemical findings and thehepatic histologyall suggested obstructive jaundice,and a further laparotomy was considered'necessary.This operation was performed by Professor IanAird on October 7, 1947. The liver was con-siderably enlarged and the portal venous radicleswere congested. A firm mass was felt high up inthe portal fissures in the region of the left hepaticduct. The gall bladder was empty; there was noapparent biliary obstruction and the common bileduct was not opened.The post-operative course was complicated by a
biliary fistula which drained for seven weeks butwhich did not influence the depth of the jaundice.On December 4, I947, the patient was wellenough to go to a convalescent home.
In April, I948, there was a 'further short ad-mission for the drainage of an abscess in thelaparotomy scar. The pus in this abscess was
bacteriologically sterile. The jaundice continuedunchanged. From September, I948, to June,1950, the patient was under the care of her generalpractitioner, Dr. Dudley-Dunn of Highgate, andalso attended fairly regularly at the hospital out-patient department. In September, 1948, she wasstill tired and weak and complained of itching. Shealso had pain in the epigastrium two hours aftermeals which was relieved by alkalies. A new de-velopment was pain in the chest and shoulders.On examination a fresh clinical sign was the pre-sence of xanthomas under the eyelids. A bariummeal at this time was non-contributory. InDecember, 1949, she was still very weak withepigastric pain and backache. The itching, how-ever, had considerably abated. Over the past sixmonths she had had occasional epistaxes. Avascular spider had developed on the right handand ascites could now be detected clinically. Shewas treated with vitamin K by mouth and with alow fat, high protein diet.The patient was admitted to hospital for the
third time on June i6, 1950. She complained ofgeneralized body pains, repeated epistaxes, swellingof the ankles of one month's duration and, veryrecently, had had some diarrhoea. Her eyesightwas blurred and she complained of seeing yellow;her appetite remained good. Examination showedthat she was dyspnoeic at rest; there were spiderangiomata over the face, arms and neck, and ahaematoma over one finger; kyphoscoliosis haddeveloped. The pulse rate was go and the bloodpressure was I05/55. A systolic murmur could beheard maximally over the fourth left interspace.The liver was still greatly enlarged and firm. Thespleen could be felt 4 cm. below the left costalmargin. There was gross ascites. The rectal pileshad prolapsed. There was oedema of sacrum andankles. Urine showed, as before, excess bile pig-ments and absence of urobilin. X-rays nowshowed generalized osteoporosis with multiplefractures of the ribs and also probably of the pubicramus. The serum calcium was 9.2 mg. per ioo
BIOCHEMICAL INVESTIGATIONS
July Sept. Sept. Dec. June1I 947 1947 1948 I 949 I950
Bilirubin (mg./ioo ml. serum) . . *. 7.4 8.6 9.4 9.9 io.6
Alkaline phosphatase (units/ioo ml. serum) .. .. 59 75 74 121 54
Total cholesterol (mg./ioo ml. serum) ..l.864 568 398 104 i 19
Albumen (g./ioo ml. serum) .. .. .. .. 3.8 - 3.1 2.7 2.1
Thymol turbidity (units) .. .. .. .. 3.8 3.3 4.0 4.7
Colloidal gold reaction 5.. .. .. .. - 5 4
Protected by copyright.
on January 24, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.302.665 on 1 Decem
ber 1950. Dow
nloaded from

Decemoer 1950 Clinical Sectio? 667
A,\~ z.,
FIG. i.-From the mass in the portal fissure, showingscirrhous carcinoma with invasion of a small nerve.H. E. x II5.
FIG. 3.-Liver in the tenth month of disease (surgicalbiopsy), showing advancing cirrhosis, with broadbands of fibrous tissue uniting many portal tracts,but with preservation of much of the originallobular structure. H. & E. X 25.
ml. and the serum phosphate was i.8 mg. perIOO ml. An electrocardiogram showed the QTcat the upper limit of normal. It was thought thatthe generalized pains were related to the skeletallesions. The patient was treated with a high pro-tein, low fat diet, and it was now possible to givethe vitamin K intramuscularly. In spite of this,on June 26 the patient had a haematemesis andbecame unconscious. A further small haema-temesis occurred on June 27 and the circulatoryfindings of severe anaemia and liver failure wereshown, viz. jugular venous pressure +2 cm. abovethe sternal angle, blood pressure I15/60, an apicalmurmur with presystolic rhythm, the hands werewarm. The haemoglobin was 9.3 g. per cent. and
aq:,
FIG. 2.-Liver in the fourth month of disease (surgicalbiopsy), showing an early stage in biliary cirrhosis,with enlargement of the portal tracts only. H. &E. x go.
V,V'4ifi
FIG. 4. Liver at post-mortem, showing frank multi-lobular' cirrhosis with complete loss of normallobular architecture. H. & E. x 25.
the blood urea concentration 28 mg. per ioo ml.On June 28 there was a further haematemesis withmelaena. Blood pressure fell to 95/50 and thepatient went into deep coma. In spite of the liverfailure the fasting blood glucose was I29 mg. perIOO ml. On June 29 the blood urea concentrationwas 28 mg. per ioo ml. and the non-proteinnitrogen 64 mg. per ioo ml., indicating thataminoacids were probably increased in the blood,presumably as a result of liver failure. On June30 the haemoglobin was 7 3 g. per cent. On thenext day the patient was much more conscious,and on July 2 two pints of blood were given slowly.This raised the haemaglobin to 9.9 g. per cent.On July 7, however, the patient passed bright red
Protected by copyright.
on January 24, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.302.665 on 1 Decem
ber 1950. Dow
nloaded from
668 POSTGRADUATE MEDICAL JOURNAL December 1950
' A
BW~~~ :$..:x^**.i..
-:-...'-
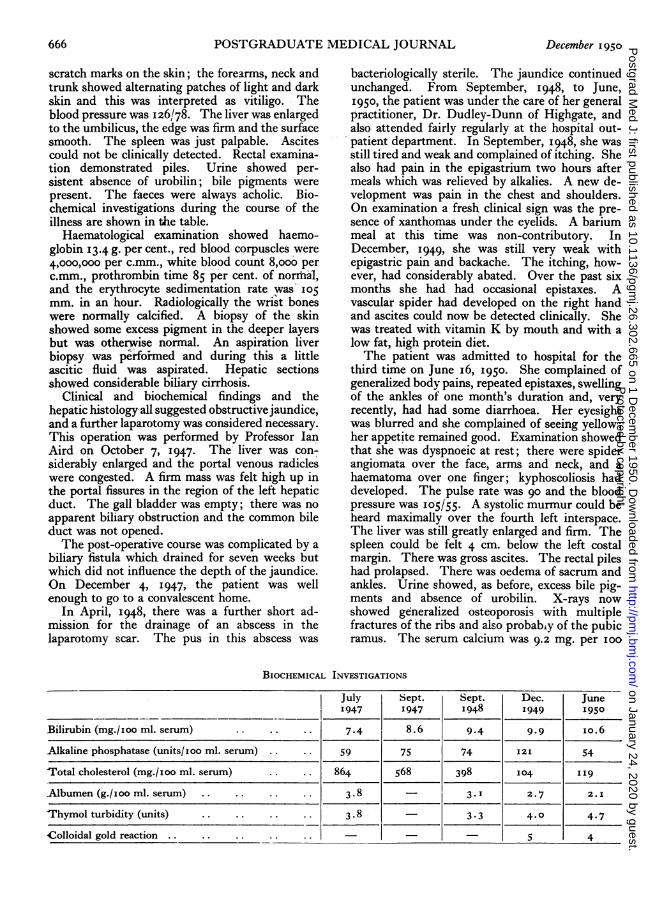
FIG. 6.-Leucocytic thrombi in the lungs. H. E.X 230.
blood per rectum and in spite of the transfusion ofa further two pints of blood, died on July 9.The clinical diagnosis was obstructive jaundice,
probably of primary intrahepatic type, with ter-minal liver failure and gastrointestinal haemor-rhage. Osteomalacia and multiple fractures wereassociated.
Autopsy Findings (Prof. Dible)At post-mortem the body was that of an old
woman with deep greenish jaundice. The legswere oedematous and the abdomen distended.There were effusions in the abdominal and bothpleural cavities and the pericardial sac. The heartwas rather atrophic. The lungs were somewhatcollapsed, but otherwise apparently normal.The chief lesion was found in the liver, which
was of approximately normal weight, but finelygranular, deep-green in colour and tough whencut. The main bile ducts within the liver weremarkedly distended with thin watery light-coloured fluid. At the junction of the two hepaticducts there was a mass of cicatricial tissue whichoccluded both ducts. Below this the common bileduct was of normal diameter and was not bilestained. There was no obvious obstruction to thepancreatic duct. The gall-bladder was normal inappearance and contained brown, thick mucin.The cystic duct was lost in cicatricial tissue andits opening could not be identified.
Histologically the obstruction to the hepaticducts was due to a scirrhous adeno-carcinomaarising in this situation (Fig. i). The variousbiopsies of the liver which had been taken at thefourth and tenth month of the disease and thefinal picture of the liver at post-mortem gave agood illustration of the progress of a biliary cirr-
.. ....*...*.8.F
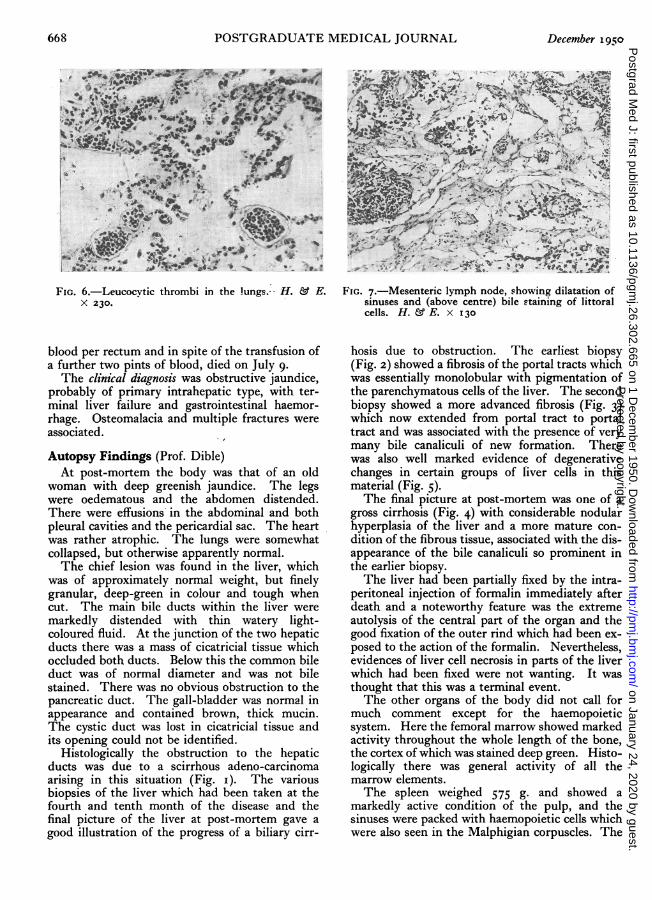
FIG. 7.-Mesenteric lymph node, showing dilatation ofsinuses and (above centre) bile staining of littoralcells. H. & E. x 130
hosis due to obstruction. The earliest biopsy(Fig. 2) showed a fibrosis of the portal tracts whichwas essentially monolobular with pigmentation ofthe parenchymatous cells of the liver. The secondbiopsy showed a more advanced fibrosis (Fig. 3)which now extended from portal tract to portaltract and was associated with the presence of verymany bile canaliculi of new formation. Therewas also well marked evidence of degenerativechanges in certain groups of liver cells in thismaterial (Fig. 5).The final picture at post-mortem was one of a
gross cirrhosis (Fig. 4) with considerable nodularhyperplasia of the liver and a more mature con-dition of the fibrous tissue, associated with the dis-appearance of the bile canaliculi so prominent inthe earlier biopsy.The liver had been partially fixed by the intra-
peritoneal injection of formalin immediately afterdeath and a noteworthy feature was the extremeautolysis of the central part of the organ and thegood fixation of the outer rind which had been ex-posed to the action of the formalin. Nevertheless,evidences of liver cell necrosis in parts of the liverwhich had been fixed were not wanting. It wasthought that this was a terminal event.The other organs of the body did not call for
much comment except for the haemopoieticsystem. Here the femoral marrow showed markedactivity throughout the whole length of the bone,the cortex of which was stained deep green. Histo-logically there was general activity of all themarrow elements.The spleen weighed 575 g. and showed a
markedly active condition of the pulp, and thesinuses were packed with haemopoietic cells whichwere also seen in the Malphigian corpuscles. The
Protected by copyright.
on January 24, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.302.665 on 1 Decem
ber 1950. Dow
nloaded from

December I950 Clinical Section 669
00E a,.-E -0
2- -- QO °
?-1004 - 700 -:
CC
0)
0 _-c
COLODL 0L
Tkm1ibd 0ui 10700 I I I '
OCT FEB JUNE OCT .FEB J)UNE OCT FEB JUNE OCT FEB JIUNE1946 1947 1948 1949 1950
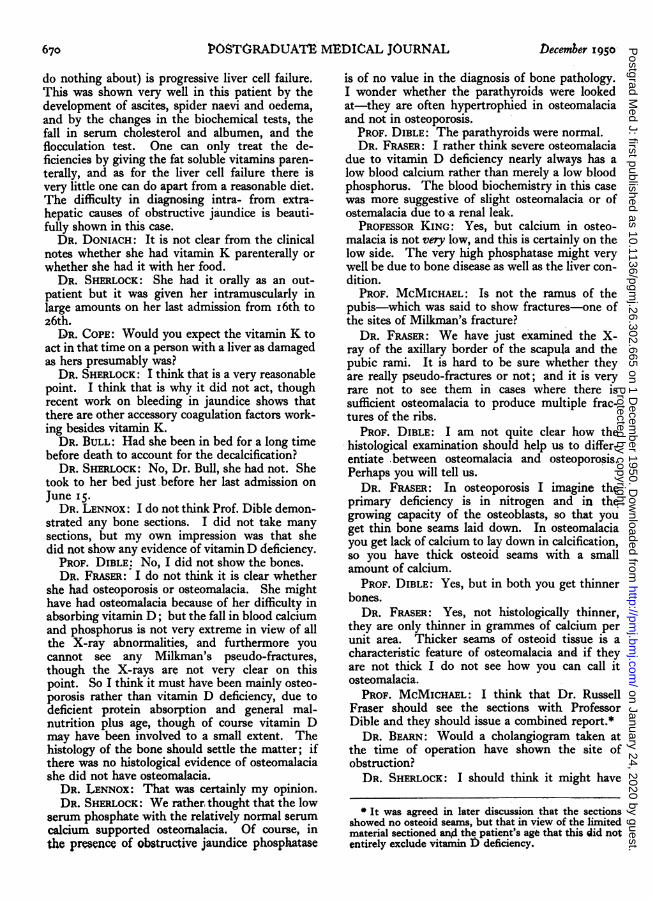
FIG. 8. -Showing clinical and biochemical landmarks.-
lung capillaries were stuffed with polymorphs(Fig. 6) and leucocytic thrombi were present inmany of the smaller pulmonary veins. The ap-pearance almost suggested a leukaemoid state, buta blood film made four days before death showedonly marked polymorphonuclear leukocytosis.An incidental finding was very extensive cal-
cification of almost all the mesenteric lymph glands.A single gland which was not affected showed anextreme degree of dilatation of the lymph-sinuseswhich were, as elsewhere, filled with pigment-containing phagocytes.The kidneys, which to the naked eye were
heavily bile-stained, showed only-moderate auto-lysis of the epithelium of the proximal convoluted-tubule and surprisingly little bile staining.
There were fractures of several ribs, the bonescut more readily than is usual, but their structureappeared normal to the naked eye.Summary. Intra-hepatic carcinoma of the main
bile ducts, producing advanced biliary cirrhosis.
DiscussionDR. Sherlock: This patient showed all the
features of obstructive jaundice; she had per-sistent jaundice over a long period, pruritis anddark urine with yellow or pale stools. Thedifficulty lay in making up one's mind whetherthe obstruction was intra- or extra-hepatic, and inthis particular instance we had nothing to helpus, The dinic.l findings would have passed for
.either condition: The biochemistry. was, as yousee, quite unhelpful, and it is useless to do liver,biopsies in these patients because they will onlytell you what is happening inside the liver and giveno clue as to the state of the bile ducts. So wemust rely on the surgeons. This patient had twolaparotomies and the surgeons, understand-ably, failed to find the obstruction which was highup. in the portal fissure, probably arising at thejunction of the three main ducts. *We were.alsoprevented from making a correct diagnosis by.thepersistence and duration of her illness., It is mostunusual for patients with carcinomatous jaundiceto survive as long as four years with a good,appetite and weight fairly well maintained.
The pathology of the tumour is, of course,interesting. This is not a common tumour; only45 cases .have been recorded of primary tumour inthis site and they are not usually as scirrhous, theyare usually -more cellular. Well, what are the.effects of long continued obstructive jaundice ofthis kind? The first things to be guarded againstare deficiencies in the fat soluble vitamins. Thispatient demonstrated defects. in vitamin K andvitamin D. Vitamin K deficiency was demon-strated by her bleedings, but I should mention thatvitamin K was-not.the complete answer becauseshe continued to bleed after being given vitaminK. Vitamin D deficiency was shown by her osteo-porosis, multiple fractures and bone pains. Well,then? the other thing one must expect (but can
Protected by copyright.
on January 24, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.302.665 on 1 Decem
ber 1950. Dow
nloaded from
6OSTOYTRADUAlt MEDICAL JOURNAL
do nothing about) is progressive liver cell failure.This was shown very well in this patient by thedevelopment of ascites, spider naevi and oedema,and by the changes in the biochemical tests, thefall in serum cholesterol and albumen, and theflocculation test. One can only treat the de-ficiencies by giving the fat soluble vitamins paren-terally, and as for the liver cell failure there isvery little one can do apart from a reasonable diet.The difficulty in diagnosing intra- from extra-hepatic causes of obstructive jaundice is beauti-fully shown in this case.
DR. DONIACH: It is not clear from the clinicalnotes whether she had vitamin K parenterally orwhether she had it with her food.
DR. SHERLOCK: She had it orally as an out-patient but it was given her intramuscularly inlarge amounts on her last admission from i6th toz6th.
DR. COPE: Would you expect the vitamin K toact in that time on a person with a liver as damagedas hers presumably was?
DR. SHERLOCK: I think that is a very reasonablepoint. I think that is why it did not act, thoughrecent work on bleeding in jaundice shows thatthere are other accessory coagulation factors work-ing besides vitamin K.
DR. BULL: Had she been in bed for a long timebefore death to account for the decalcification?
DR. SHERLOCK: No, Dr. Bull, she had not. Shetook to her bed just before her last admission onJune I5.
DR. LENNOX: I do not think Prof. Dible demon-strated any bone sections. I did not take manysections, but my own impression was that shedid not show any evidence of vitaminD deficiency.
PROF. DIBLE: No, I did not show the bones.DR. FRASER: I do not think it is clear whether
she had osteoporosis or osteomalacia. She mighthave had osteomalacia because of her difficulty inabsorbing vitamin D; but the fall in blood calciumand phosphorus is not very extreme in view of allthe X-ray abnormalities, and furthermore youcannot see any Milkman's pseudo-fractures,though the X-rays are not very clear on thispoint. So I think it must have been mainly osteo-porosis rather than vitamin D deficiency, due todeficient protein absorption and general mal-nutrition plus age, though of course vitamin Dmay have been involved to a small extent. Thehistology of the bone should settle the matter; ifthere was no histological evidence of osteomalaciashe did not have osteomalacia.
DR. LENNOX: That was certainly my opinion.DR. SHERLOCK: We rather thought that the low
serum phosphate with the relatively normal serumcalcium supported osteomalacia. Of course, inthe presence of obstructive jaundice phosphatase
is of no value in the diagnosis of bone pathology.I wonder whether the parathyroids were lookedat-they are often hypertrophied in osteomalaciaand not in osteoporosis.
PROF. DIBLE: The parathyroids were normal.DR. FRASER: I rather think severe osteomalacia
due to vitamin D deficiency nearly always has alow blood calcium rather than merely a low bloodphosphorus. The blood biochemistry in this casewas more suggestive of slight osteomalacia or ofostemalacia due to a renal leak.
PROFESSOR KING: Yes, but calcium in osteo-malacia is not very low, and this is certainly on thelow side. The very high phosphatase might verywell be due to bone disease as well as the liver con-dition.
PROF. McMIcHAEL: Is not the ramus of thepubis-which was said to show fractures-one ofthe sites of Milkman's fracture?
DR. FRASER: We have just examined the X-ray of the axillary border of the scapula and thepubic rami. It is hard to be sure whether theyare really pseudo-fractures or not; and it is veryrare not to see them in cases where there issufficient osteomalacia to produce multiple frac-tures of the ribs.
PROF. DIBLE: I am not quite clear how thehistological examination should help us to differ-entiate between osteomalacia and osteoporosis.Perhaps you will tell us.
DR. FRASER: In osteoporosis I imagine theprimary deficiency is in nitrogen and in thegrowing capacity of the osteoblasts, so that youget thin bone seams laid down. In osteomalaciayou get lack of calcium to lay down in calcification,so you have thick osteoid seams with a smallamount of calcium.
PROF. DIBLE: Yes, but in both you get thinnerbones.
DR. FRASER: Yes, not histologically thinner,they are only thinner in grammes of calcium perunit area. Thicker seams of osteoid tissue is acharacteristic feature of osteomalacia and if theyare not thick I do not see how you can call itosteomalacia.
PROF. MCMICHAEL: I think that Dr. RussellFraser should see the sections with ProfessorDible and they should issue a combined report.*DR. BEARN: Would a cholangiogram taken at
the time of operation have shown the site ofobstruction?
DR. SHERLOCK: I should think it might have
It was agreed in later discussion that the sectionsshowed no osteoid seams, but that in view of the limitedmaterial sectioned and the patient's age that this did notentirely exclude vitamin 1) deficiency.
670 December 1950,P
rotected by copyright. on January 24, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.665 on 1 D
ecember 1950. D
ownloaded from
Clinical Section
done so. We should have seen a block distally. Itis an important point.
DR. HARRISON: Did Dr. Sherlock say thatonly 45 cases of intra-hepatic carcinoma of the bileducts have been reported?
DR. SHERLOCK: I thought so. I have notsearched the literature very extensively however.
DR. HARRISON: I can show her two cases fromrecords in this hospital.
DR. FRASER: On that same point, may I ask ifany of these recorded cases were diagnosed ortreated ante-mortem, or had surgical treatment?
DR. SHERLOCK: I do not think so. They are allautopsy reports.
PROF. MCMICHAEL: Could we have a surgicalopinion on this?MR. SHACKMAN: I think we have tried to treat
such conditions surgically. f have, for instance,helped Professor Aird to anastomose an intra-hepatic bile duct to the intestinal tract, and it wastemporarily successful.
DR. SHERLOCK: I think perhaps r have beenmisunderstood about the rarity of, the condition.I mean the rarity of carcinoma of the junction ofthe two hepatic ducts and the common bile duct,not of those lower down, which are relativelycommon. It is the high ones which are rare.MR. SHACKMAN: r was referring to high ob-
structions. Those which are lower down are, ofcourse, more amenable to surgical resection. Thehigher they are the harder it is to get at them.
DR. LENNOX: I suppose your point is, Dr.Sherlock, that if they are lower down they areeasier to recognize, and if they are higher up theydo not cause obstructive jaundice because onelobe or the other would continue to secrete; it isthe ones at the level which produce the precisepicture seen in this case which are rare.
DR. SHERLOCK: Yes, just so.PROF. DIBLE: Why is it that the bilirubin
reaches a certain level and stays there? Whydoesn't it go on rising all the time in completeobstruction?
PROF. KING: I think it has gone up to 36 inthis hospital, hasn't it, Dr. Sherlock? In mostcases of obstructive jaundice it spills out into theurine after it has reached a certain high level inthe blood.
DR. SHERLOCK: Yes, but this is a very goodexample of one which did not ever reach a highlevel. We have records for over three years andher serum bilirubin remained at a moderate level.It is a matter of the attainment of a state in whichformation balances excretion. There is a de-creased formation of bilirubin which is almostbalanced by the output in the urine.
DR. LENNOX: Could I ask another rathertheoretical question? What makes the liver in a
case like this' hyperplase,' if I might coin a word?If you take out three-quarters of the thyroid youget production of thyrotropic hormone and thatmakes the remaining thyroid grow. Here you havegot continuous destruction of liver tissue for yearsand it is continuously being replaced. Has anyoneany idea what makes it do this?
DR. HARRISON: G. R. Cameron did some workon that in the 'thirties with Karunaratne.
DR. FRASER: It is often said to be the result ofdirect stimulation by necrotic liver tissue.
DR. DONIACH: I suppose that the regenerationof the liver might be regarded as a response to theresultant additional load of work caused by thelessened total volume of liver tissue-a ' work '
hypertrophy, comparable with that seen in thekidney submitted to an extra load.
DR. HOMER SMITH: I want to say that I openmy mouth in this conference just as a student.But there are three questions that r would like toask. The first that I would like to ask Dr. Sherlockis about seeing yellow. This patient was said to beseeing yellow. Now r would like to know if shewas asked any leading questions about that?
DR. SHERLOCK: Yes, Dr. Homer Smith, it wasin answer to a leading question. I always askthat question and it was the first time I haveheard that answer.
DR. HOMER SMITH: I thought so. The secondquestion I want to ask is if you have any ideasabout the origin of these vascular spiders. Mythird question-but before I ask that and getthrown out, I would like to comment on thepreservation of the tissue in the superficial layer ofthe liver. Recent physiological studies indicatethat all cells are constantly engaged in doing meta-bolic work in order to maintain their integrity,which requires oxygen consumption. I wonder ifthe injection of oxygen into tissues, the abdominalcavity or into any space where it would be re-tained temporarily has ever been tried as a meansof preserving tissues against autolysis.Now I come to my other question. I would
hesitate to disagree with the diagnosis because Iwould be overruled here by at least IOO to I, butmay I ask if the diagnosis of carcinoma can beaccepted with certainty? Is there a possibility ofascending infection, perhaps from the allegedmesenteric tuberculosis? Might it have been theprimary factor in the obstruction and the car-cinoma entirely accidental or coincidental, orperhaps even secondary to the cell changes?
DR. SHERLOCK: Shall I deal with the spidersfirst? The vascular spider is said to be due toostrogen effects. The liver cells fail to detoxicateoestrogen and you get an oestrogen effect on theskin- vessels, Now that is by noQ means certain,
December I1950 671P
rotected by copyright. on January 24, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.665 on 1 D
ecember 1950. D
ownloaded from
672 POSTORADUATE MEDICAL JOURNAL December I950
because studies of patients with cirrhosis haveshown that the urinary excretion of oestrogen maynot be particularly abnormal. Of course, thatdoes not mean that the blood oestrogen is notraised. Anyhow that is the accepted explanation atthe moment, though not a very good one.
PROF. DIBLE: The last question is a little com-plex and I am not sure that r remember all theimplications. First of all it was a carcinoma, thereis no doubt about that. They were carcinomacells, although the glands looked very well de-veloped, there was plenty of penetration and in-vasion of the perivascular and lymphatic channels.Secondly, could there be any relation between thecarcinoma and the abdominal tuberculosis? Iwould say directly no, because abdominal tuber-culosis is an extremely common condition and onethat is met with often in the post-mortem room,perhaps not so often now as previously, but it isstill a common enough condition and r do notthink such a correlation has ever been demon-strated all this time. At the same time the pre-sence of abdominal tuberculosis does raise certainpoints in the case which have been runningthrough my mind, and one of them is that pre-sumably in the mechanism of the absorption offat the lacteals must have been obstructed by these
necrotic glands. One knows that the lymphaticnetwork is so extensive that there must have beenplenty of by-paths; at the same time it is possiblethat the .absorption of neutral fat, may .have.been interfered with and that the alternativemechanism.may have been over-active. So thatalthough I cannot.see all the way along the routeI am trying to travel, it is possible that the,par-ticipation of the liver in fatty acid absorption mayhave been over-active and that that may have ledto some pathological condition in the liver a longway back which may have expressed itself as acarcinoma of the ducts.
DR. SHERLOCK: If that is so it is queer that wedo not have some fatty change in the liver. Mostof the steatorrhoeas and chronic diarrhoeas whichwe have seen showed fatty change.in the liver,andwe have related that to an increased portal veinabsorption of fat.A STUDENT: Is it not possible that the obstruc-
tion was primary and that led.to cirrhosis of theliver and then to carcinoma?
PROF. MCMICHAEL: I think this is not the typeof carcinoma which complicates cirrhosis of theliver. This cancer must have been primary an.dthe cause of the obstruction, that is the obviousinterpretatior.
H. K. LEWIS& Co. Ltd. Medical Lending LibraryMedical Pu blishers ANNUAL SUBSCRIPTION from ONE GUINEAand Booksellers For the CONVENIENCE of POST-GRADUATE STUDENTS SHORT
Catalogues on request State interests PERIOD SUBSCRIPTIONS ARE ARRANGED - for 3 or 6 months
1 36 GOWE R STR E ET Detailed Prospectus .on applicationLONDON, W .C 1 The Library Catalogue revised to December, 1949, containingclassified index of authors and subjects in preparation.
(Adjoining University College and Hospital) BI-Monthly List of New Bog" and New EdItIorsTrdhme: EUSton 4282 (7 lines) sent post free on requestTsIeeremss: Publicavit, Westcent, LondonBusines hours:9 am.to 5p.m. Saturdays: I p.m. NEW BOOKS ADDED IMMEDIATELY UPON PUBLICATION
Protected by copyright.
on January 24, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.302.665 on 1 Decem
ber 1950. Dow
nloaded from





























