Embed Size (px)
Citation preview

CLINICAL PROGRESS
Pathophysiology of Card'iac Pain
By RIcHARD GORLIN, M.D.
ANGINA pectoris can be no better de-scribed than in Heberden's original dis-
cussion some 160 years ago.' Despite theenduring quality of his description, Heber-den had no idea of the cause of anginapectoris, although he did appreciate its morbidquality. In the same era, Jenner, Parry, andBurns were among the first clinicians toassociate angina pectoris with anatomicdisease of the coronary arteries. This notionlost favor somewhat during the latter halfof the nineteenth century when anginalpain was thought to originate in spasm ofthe coronary arteries or in disease of theaortic wall itself.2 The twentieth centurywitnessed the observations of Herrick,3 Mac-Kenzie,4 Levine,5 Keefer and Resnik,6 andBlumg-art, Schlesinger, and Davis,7 culmi-nating in the theory that angina pectoriscame about as the result of myocardial ische-mia, usually in the presence of intraluminalcoronary artery disease or disease causingcardiac hypertrophy, and elicited by disturb-ance of the balance between coronaryoxygen supply and myocardial oxygen de-mand.The purpose of this report is to indicate
what new facts may be added to thesemasterful disser;tations. The discussion isdivided into three parts: mechanism of painexcitation within the heart; myocardio-neu-ronal reception and transmission of pain
impulses; clinico-physiologic factors in thedevelopment of angina pectoris.
Mechanism of Pain Excitationwithin the Heart
Myocardial IschemiaThe "ischemia" theory of angina pectoris
has been based in large measure on theresults of retrospective observations, i.e., thatthe coronary arteries are narrowed or oc-cluded; regions of myocardium served bythese vessels are often necrotic or scarred,and that clinical factors favoring cardiacanoxemia precipitate or aggravate angina.
SPONTANEOUSANGINA
REST
1.0
.9
.7
LACTATE .6
mM/ L.s
NOANGINA
REST ISOPROTERENOL
VENOUS OARTERIAIL*
qSN. //CAD 'K _
ISOPROTERENOL
From the Medical Clinics, Peter Bent BrighamHospital and Harvard Medical School, Boston, Massa-chusetts.
Supported by grants from the U. S. Public HealthService (NIH H-2637 and HE 08591-01, Peter BentBrigham Hospital, GRS 9831-6, and Warner ChilcottLaboratories.
138
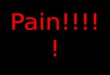
Figure 1
Myocardial lactate metabolism in coronary heart dis-ease. Arteriocoronary venous lactate difference in asubject with rheumatic heart disease and normalcoronary arteries (N) (solid lines); and a subject withtotally occluded right coronary artery and major ste-nosis of both branches of the left coronary artery(CAD, coronary artery disease) (broken lines).
Circulation, Volume XXXII, July 1965
ol
REST
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

PATHOPHYSIOLOGY OF CARDIAC PAIN
During the last few years, our laboratoryhas been able to document directly theoccurrence of ischemia of the heart in as-sociation with angina pectoris. This wasaccomplished by placing a catheter in thecoronary sinus, and by sampling oxygen andlactic acid concentration of coronary venousblood draining the left ventricular myocar-dium, and then comparing it with theconcentration of arterial blood drawn simul-taneously. The heart is a curious organ, andcompletely different from skeletal muscle inthat, normally, it is totally aerobic, i.e., thereis hardly ever breakdown of glucose orglycogen to lactic acid under normal or evenstressful conditions. In fact, the normal heartextracts lactate from the blood and convertsthis to pyruvate. In figure 1 is shown lactatearteriovenous difference at rest and againwhen the heart is challenged by infusion ofa powerful catecholamine, isoproterenol. Inthe heart with the normal coronary arteries,extraction of lactate occurred both at restand while the heart was stimulated byisoproterenol. In the patient with angiograph-ically proved severe coronary artery disease,however, while at rest there was lactateextraction, with "spontaneous" angina pec-toris and again with isoproterenol infusionthere was reversal of extraction, so thatactual production of lactate, or evidence forglycolysis in excess of oxidation, occurred.When myocardial arteriovenous sampling oflactate has been performed at the time ofan anginal attack, markedly reduced extrac-tion (0 to 5 per cent) or actual productionof lactate has been observed in 90 per centof observations.8 On the other hand, lactateproduction was seen not infrequently in thecomplete absence of clinical pain in subjectswith established angina pectoris. It is highlyunlikely, therefore, that lactic acid itself isthe primary cause of pain. However, lactateproduction is unique as a biochemicaldiagnostic test for myocardial ischemia, andin fact, it can serve as a functional indicatorof the adequacy of any given degree ordistribution of coronary arterial disease.
Because of the spotty nature of coronaryCirculation, Volume XXXII, July 1965
artery lesions, myocardial ischemia may oc-cur only in certain zones of muscle and onlywith provocation. Two principles are essen-tial in laboratory diagnosis: the first is thatmyocardial ischemia must be provoked duringthe laboratory study by simulating thoseclinical conditions that lead to ischemia orpain, or both; the second is that samplingmust be done at multiple sites in thecoronary sinus to detect the different venousdrainages from the anterolateral and infero-posterior walls of the heart. For example,lactate production sampled far out in thegreat cardiac vein can be diluted by venousdrainage from other nonischemic areas, andtherefore be undetected when sampling isobtained farther down the coronary sinus(table 1). The site of ischemia can be small,and yet result in angina pectoris. Also, asshown in table 1, the site of lactate productiondid not always match the demonstrated siteof coronary disease. This discrepancy be-tween locale of arterial disease and region ofaffected myocardium could have been pre-dicted from the concept of "infarction at adistance" propounded by Blumgart, Schle-singer, and Davis.7 If deliberately and dili-gently sought for by multiple site samplingsduring stressful challenge to the heart, lactateproduction will almost always be elicited inthe anginal subject.
It is also significant that but for a raresubject (5 per cent of the series), cardiacpain and lactate production always occurredin the presence of organic disease-eithercoronary artery disease or disease resultingin left ventricular hypertrophy. Due to thetype of cases referred to our laboratory forstudy, aortic stenosis or insufficiency was thelesion most commonly leading to left ventric-ular hypertrophy. A small number of casesof hypertrophic subaortic stenosis or idio-pathic hypertrophy constituted the re-mainder. Approximately 40 per cent of theaortic valve disease cases and all the otherhypertrophic disorders had normal coronaryarteries cineangiographically.9 The occurrenceof angina and cardiac lactate production inthese latter groups, supports the concept that
139
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

o) io cq -q06 016
-40666
+
4 -4-4)0 0
N
0 14
14)
0o4)0
,. -S -.Ct Q
-B 04-UA "d -'-I
40 4
X '1 O
b-O
-40-~~~~~~~~~~-
Cd ~~~~~C)
0--
00CoI
00
10 0t-tU
C)0
0) +
0 0
+ +
P0
C13'N0'-4P.,
4)i
9
E
",, .)0-4, Zra.
_t Q
4)444
So
4)JC4
1=1.
P44) 4)
4) 44
o0
04
._
004)
+0o ±+
t4- CD in~r-- o C'l
I +
Circulation, Volume XXXII, July 1965
140 GORLIN
Cd
e 0
CS
q)Cd
0*_
0
0
OC4 S)
-Q,CA00.4$-t,
Cd
00C)
0S =
400004)J0
00C',
044
-4)C)
00
1.0
4)
o c
00C0
Q
4)
>4C)
41)
On
-4
CZ
0
0a)' 4.0
IN
I_0
40
;40z
II
II
II
o o
C: m.6 6
oolo
Ci
.X N
_.4)
0
.; 0
.0 Q1.4
Q 4
C.)Q
00,4)-
*44 .5
;>0U
044="0).= .tH >40*
0t Q
0.,
0t * ^
01 4
:>40
4) 4-)
0 S55
0 Q.;; U;
^44.44)
4).44
a 00* +v.
4)0
4q
44444
4-
co
44
0-O
co
44 44
4) -4e444._
-S X *
o
to4) .5
'
0
0 +
F-
E* 14)44)r34)
COD
.-
0
*.
Ctz
0
u
r_"
Q-)
46)4)."
"-.4+46
C) iO C300
100+
I_ g 0-
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

PATHOPHYSIOLOGY OF CARDIAC PAIN
angina anid myocardial ischeemia can occtur\vithout coroniary disease,"' presumably be-cauise hlypertroplty has ouitstripped its vas-cuilar siupply.Coronary Spasm
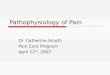
Seventy-five years ago, Latham and Gaird-ner advocated that spasm of tlhe coronaryarteries wvas the instigator of anginial pain.This idea received clinical support becausetlhe characteristically precipitouis and violentaniginal attack cotuld be relieved quickly bythe administration of smooth-muscle relaxants(niitroglycerini) and by carotid sinus pressure.'"The "spasm" theory has also been suip-ported by various angiographic labora-tories, which have docuimented the transientniarrowing and occasional actual occlusion ofcoronary vessels. Figure 2 shloxvs an exampleof suich spasm. However, there has been aniinconstant associatioii of symptoms of anykincd with the observed spasm. In a numberof instances, the spasm has been attributedto direct stimulation by the tip of the anigio-graphic catheter. In our experience, recordedsequences of spasm were totally unrecognizedby the patient, and occasioned no alterationwhatever in cardiac fuinction. Certainly, sys-
Settcliv. RighI Co#onfry Ingecti.n
FIRST
r
SECOND
THIRD
Figure 2
Evidetnce for coronar-y spasm. Single frames have
been taken fron? three successive selective injectionsof right coronary artery to illustrate the progressivedevelopment of a zone of narrowing. This subsequent-ly disappeared. The patient experienced no sensationwchatever and the electrocardiogram teas unchanged.
Circulation, Volumne XXXII, July 1965
Clinical State P.i. F.** Angina P.t.is at1 Iest P.i. F..wcl -eSt du,ation: mnin 2 min post tNG
0 2 4 o.3 mg w6ling.olly
Rate40
A,ta,mal
Blood P...
.m Hg
tV *dpmm Hg
C.di 1.4.2
Ejeclieo. 127 122
m ./s-X'|7 o
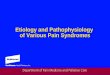
Figure 3
5poitanecons angina pectoris and sylstemic vasocon-striction. Patient developed anginal pain as his bloodpressture began to rise. Pain was relieved wheni. pres-sulre wcas lotwere(l bIy sublingial niitroglylcerin.
teinic arterial spasm per se can elicit severepain; however, coronary spasImi cain occuir vithor witbout causing pain. Pain associated witlhspasm may depend on- wvhether the changein caliber of the vessel is oceluisive enioughto initiate isehemia of the myocardiumdoxvnstream. Thus, in sutmmary, spasmn hasbeen morphologically demonstrated to occurirrespective of the presence of coronarysclerosis; and it can occur without incitingpain. The precise relationship, if any, of suchspasm to clinical angina pectoris is stilluinsettled.
Acute Left Ventricular Failure
In a study of patients xvith coronary lheartdisease, Muller and lB0rvikl'2 described a risein pulmonary capillary pressiure duiring exer-cise that preceded the onlset of anoginal pain.Both the rise in pressure and the occurrenceof pain vere abolisheld b)y prior uise ofnitroglycerini. They suggested that the occuir-rence of pain might be related to suiddeincongestion of the heart or lunigs. Sueh a clhainof events has been uncommoni in our experi-ence. In at least 30 examples of stress-indulcecdangina, an increase in left ventricular end-diastolic pressure was observed in only oneinstance. Here, left ventricular systolic pres-sure had risen remarkably because of thepresence of severe aortic valvular disease. XVe
141
190170
14 5
7 4
I
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

GORLIN
have observed eight instances of "sponta-neous* angina unrelated to any deliberatelaboratory stress. Left ventricular end diastolicpressure rose on three occasions. In each,systolic blood pressure had risen considerably.Figure 3 shows the sequence in a patientwith coronary disease with fixed heart ratedue to complete heart block and controlledby an internal pacemaker. Left ventricularsystolic pressure rose progressively, as well asend-diastolic pressure, and soon the patientcomplained of angina. Reciprocally, the car-diac output and mean ejection rate declined,indicating peripheral vasoconstriction as wellas acute heart failure. A significant featureof the unprovoked anginal attack often ap-pears to be acute vasoconstriction with acutehypertension and sometimes a rise in ventric-ular end-diastolic pressure. Cardiac perfor-mance can be profoundly affected bysystemic vasoconstriction when the heart isdiseased. In another patient, however, anginadeveloped on two occasions at two completelydifferent values of left ventricular systolic andend-diastolic pressure.8 Pain and failure ofcardiac function are probably both dependenton myocardial ischemia, in part abetted bythe obligatory pumping of the heart againsthypertensive pressure; but pain and failureare not necessarily dependent on each other.It would seem unlikely that pain is due toheart failure per se.
Free Branching Sensory Receptors Dead
I~~I~~~ ~~~ ~~~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Increased \K n Kinins or PPS
[H ][ K ]
? Activation by Kallikrein
By-products of Ischemic Muscle
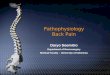
Figure 4
Pain generation within cardiac muscle.
Myocardio-Neuronal Reception andTransmission of Pain Impulses
It is unclear how the pain signal is initiated,but some factors are known. There are twonetworks of sensory fibers in the heart: theperivascular network encircling the coronaryarteries and the paravascular fibers, runningalongside the vessels and terminating be-tween the muscle fibers in free-branching,unmyelinated and nonspecific nerve endings.13These endings are not so numerous in mus-cle as in other structures.The present concept of pain (fig. 4)
holds that with ischemia, various pain-produc-ing substances or substances akin to oridentical with the plasma kinins, are activated,possibly by kallikrein released from ischemicor inflamed tissue.'4 Concentration of suchsubstances is intensified by stagnation ofblood flow, and their action to produce painis augmented by heightened local concentra-tion of H+ or K+-15-a likely interstitialconsequence of cellular hypoxia. Apparently,these agents affect the free-branching ter-minals, and pain is registered in proportionto the intensity of chemical stimulation andto the number of receptors sending signals(size of total area of ischemia produced aswell as the number of live receptors, i.e.,loss with prior infarction).
This theory does not answer three discrep-ancies: (1) pain is uncommon with acutemyocarditis as opposed to myocardial ische-mia, and inflammation is notorious inreleasing pain-producing substances; (2) gen-eralized ischemia of the heart as a wholemay not necessarily cause pain, and yet asmall area of ischemia may result in majordiscomfort; (3) similar degrees of chemicalischemia (seen in the same patient) mayor may not initiate pain.Once the receptors have initiated the
signals, this information flows to the centralnervous system through the eighth cervicaland first four thoracic ganglia. In so doing,these impulses must utilize the same pathwaysas impulses bringing information from otherorgan systems. In addition, there is segmen-tal "overflow" both along the ganglionic chain
Circulation, Volume XXXII, July 1965
142
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

PATHOPHYSIOLOGY OF CARDIAC PAIN
and within the lateral ascending pathwaysof the spinal cord. For these reasons, in-formation coming from the heart cannot neces-sarily be distinguished as such, but may beexpressed solely via a somatic referral-aprojection onto that part of the body surfacesupplied by that particular spinal cord seg-ment. Here again, the intensity of stimulifrom the heart can be amplified or diminisheddepending on what other traffic is in thissegment of the nervous system. For instance,impulses from another organ such as adiseased gallbladder (or hiatus hernia) mayordinarily be below the threshold of consciousrecognition, but the summation effect ofsubliminal stimuli from the gallbladder andheart may elevate angina to conscious aware-ness and make perception of pain more likelywith minimal degrees of cardiac ischemia. Ihave also observed that patients with partic-ularly crippling angina pectoris almost al-ways have some other pain-producingsyndrome such as cervical spine disease,costochondritis, or a gastrointestinal disorder.A 68-year-old patient was seen who had a
10-year history of relatively infrequent attacks ofangina pectoris. For 1 week, substernal painhad increased in frequency and intensity, particu-larly after meals, and waking the patient fromsleep. Electrocardiogram showed ST-segment de-pression over the left precordium. The patient washospitalized for presumed preinfarctional angina.After 4 days there was a sudden increase in pain,with a shift in location for the first time to theepigastrium. He developed chills and fever to103 F. and subsequently became icteric with arise in serum SGOT and LDH; within 48 hoursall symptoms and signs of biliary tract obstructionreceded; the anginal syndrome and ST changeson the electrocardiogram subsided within 3 days.Gallstones were subsequently demonstrated andhis gallbladder was removed surgically. Anginahas returned to its former mild tempo.
Thus, previously stabilized angina can beso increased in intensity and frequency byanother disease, i.e., cholelithiasis, as to sug-gest the preinfarctional state. Complete re-mission resulted once the offending conditionis corrected.
Finally, the information reaching the brainmust be sorted and identified, allowing ampleCirculation, Volume XXXII, July 1965
opportunity for reinterpretation. Indeed, thewell-worn pathway of impulses streamingfrom the heart, as proposed by MacKenzie4can become part of a conditioned andeasily provoked reflex. Is the load on theheart necessarily different in the morningwhile the patient is shaving or when rushingfor a bus so that angina should be morefrequent at such times than during similaractivities later in the day? It is probablethat conditioning of a reflex response playssome role here. It is not that ischemia doesnot occur on other occasions, but rather thatunder certain given circumstances, cardiacischemia is more specifically directed to thepatient's conscious level. Thus pain awarenessis not only a function of the occurrence ofischemia, but also of neuronal receptor stimu-lation, density, and intensity of sensorytraffic, and finally its reception and interpre-tation by the brain itself.
Clinicophysiologic Factors in Developmentof Angina Pectoris
Anginal pain is not an automatic by-product of cardiac ischemia. Nevertheless,angina does fall into certain well-knownpatterns and has a predisposing background.
Predisposing BackgroundReduction in arterial oxygen content or
capacity as with chronic anemia by reducingoxygen transport per milliliter of coronaryflow, potentiates angina; and, although ex-tremely rare, it is reported that severe enoughanemia has caused angina in the absence ofmorphologic coronary disease.16 Cardiac ac-tivity and metabolism can be chronicallyheightened as in thyrotoxicosis, valvularheart disease, arteriovenous fistula, and pul-monary or systemic hypertension. These factorscan so burden the oxygen transport system asto bring borderline areas of myocardiumcloser to frank ischemia. Polycythemia canaugment a tendency to angina. Finally,changes in blood lipids can result in sludgingor clumping of cells, or possibly inhibitionof oxygen diffusion through the capillarieswith intensification of already existing ische-mic symptoms. Whether these latter factors
143
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

GORLIN
10.
08.
Lactate06.
mM/L
04.
021
U'Venous o
Arterial
uI Il
Rest Exercise
Figure 5Change in cardiac lactate arteriovenous difference in-duced by exercise. Patient had total occlusion of theleft anterior descending artery, the rest being normal.Angina and ST depression were induced by effort.Simultaneously, lactate extraction at rest changed tolactate production during exercise.
are operative in the absence of morphologiccoronary disease is unknown.
Angina of Effort
This is readily understood. During exercise,increased mechanical work is expected of aheart in which energy supply to certain areasof the myocardium may be inadequateunder stress. Exercise may evoke a poormechanical performance* as documented byreversed splitting of the second sound,17 byinadequate elevation in cardiac output andin mean ejection rate,'8 and by an occasional,abnormal increase in left ventricular end-diastolic pressure (fig. 3). In addition, elec-trocardiographic changes are common andcardiac lactic acid production is almostalways the rule with leg exercise (fig. 5).Occasionally, only special types of effort maycause pain such as use of the arms as inlifting or pushing. All these abnormalitiesmay occur with effort, but without pain, evenin the patient with established effort angina.
*It is the author's belief that many patients withcoronary heart disease have subliminal cardiac failure.Not only are there measurable deficiencies in theresponse of cardiac output to stress, but some patientsexhibit moderate salt and water retention long beforeovert effort dyspnea or pedal edema occurs. This canbe detected by the response to mercurial diuresis,which often will result in a surprising weight loss of5 to 10 lb. as compared to a normal of about 3 lb.
Angina with TachyeardiaTachycardia reduces coronary artery filling
time in diastole as well as augmenting car-diac oxygen requirement.'9 This sets thestage for selective myocardial ischemia be-yond a stenotic coronary artery.
Spontaneous AnginaAlthough angina at rest may occur without
discernible hemodynamic change,4 Sir Thom-as Lewis pointed out that blood pressure orpulse increases in most patients at the time ofan attack. This has been true of the majority ofpatients observed in our laboratory during anattack of "spontaneous" or unprovoked pain.The patients are usually tense, nervous, orfearful. The rise in pulse or blood pressure,
p 153/78P 54
105 -
CPM
104
CPM
CORONARYRESISTANCE
d.s.c-. .103
LACTATE A-V
mmM/L
/11086
130/7365
30 60 90 120 150 1i0
TIME - SEC
CONTROLb 05
71 .Ir/100 m 1 0n104-
30 60 90 120 )so too
TIME - SEC
76
+ .12
PAIN
TN
30 60 90 120 lSO ISO
lO! 51
.04 +.12
Figure 6
Change in coronary blood flow during spontaneousanginal attack. CPM, counts per minute; BP, bloodpressure; P, pulse; TNG, nitroglycerin. A controlcoronary flow measured prior to the attack is shown(semilogarithmic plot, lower left), and is higher de-spite a lesser mechanical workload on the left ventriclewhen compared to flow during the attack (semi-logarithmic plot, lower right). Lactate arteriovenousdifferences across the heart were positive (normal) atrest and upon recovery from pain. The reversed(negative) arteriovenous difference in quotation markshad been obtained during a separate but similar an-ginal episode in this patient.
Circulation, Volume XXXII, July 1965
144
FAI N TNG
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

PATHOPHYSIOLOGY OF CARDIAC PAIN
of itself, would not seem to be enough of amechanical load to precipitate angina throughdemand-energy imbalance alone (fig. 3).On the other hand, these changes mayrepresent signs of generalized sympathet-ic nervous discharge involving vasoconstric-tion through vascular beds as well as directinotropic and chronotropic stimulation tothe heart.
Figure 6 represents a fortuitous set ofobservations made during a spontaneousanginal attack in a patient with severe,diffuse narrowing of the left anterior de-scending coronary artery. The figure shows acontinuous krypton-85 left coronary bloodflow determination initiated from a subostialposition approximately 1 minute prior to thetime that the patient began to complain ofwhat was for her a typical attack of anginawith severe substernal chest pain (byhistory the patient's pain had no apparentpredictable provocation). It was noted thatshe developed hypertension of 180/110 froma nearly normal blood pressure, a relativetachycardia of 86 from a slow heart rate,and change in T waves of lead III. Theportion of coronary flow curve recordedduring the time of pain, yielded a value of51 ml./100 Gm./min. This was significantlylower than a control value for coronaryflow (71 ml./100 Gm./min.) in this patientmeasured at an earlier time in the studywhen hemodynamics were normal and cardiacoxygen demand was presumably much less.This patient then had a reduced coronary flowin the presence of increased cardiac workdue to acute hypertension. Coronary vascu-lar resistance was increased during the attackindicating that there must have been markedcoronary artery or arteriolar constriction.Nitroglycerin, given sublingually, resulted inan almost immediate increase in coronaryflow to 88 ml./100 Gm./min., and thereafterrelief of pain and return of pulse, bloodpressure, and T wave to baseline. This caserepresents documentation of a severe vaso-constrictor (or less likely arterio-spastic)episode occurring as part of a generalizedsympathetic constrictor discharge. This mayCirculation, Volume XXXII, July 1965
supply an important clue to the nature ofmany so-called spontaneous anginal attacks.It is probable that such phenomena occurfrequently with sympathetic nervous dischargein all kinds of people (fig. 3). When thisoccurs in a patient with obstructive coronaryartery disease and lowered pre-arteriolararterial pressure, such arteriolar vasoconstric-tion may readily precipitate myocardialischemia. It is well known that coronaryvasoconstriction when produced by ergot andPitressin can precipitate angina pectoris, andnorepinephrine administered intravenouslymay cause coronary vasoconstriction.20 Oneof the important roles of both the long-actingand short-acting nitrites may be in the pre-vention or mitigation of such constrictorepisodes.
Angina of Emotion
It seems most likely that this form ofangina has a dual origin similar to that of"spontaneous" angina. Undoubtedly, withsympathetic stimulation an increased bloodpressure, heart rate, and vigor of contractionaugment the cardiac need for oxygen. To thismay be added the possible further aggravationof ischemia by participation of the coronarysystem in systemic vasoconstriction. The verysame response pattern to emotion may takeplace in any individual. Only if there is under-lying segmental vascular disease and antece-dent drop in line pressure will superimposedconstriction seriously impair segmental coro-nary flow.
Angina of DeglutitionThis is poorly understood. Occasionally, if
this symptom is outstanding, it may serveas a clue to the presence of an associateddisease in the gastrointestinal tract, such ascholelithiasis or hiatus hernia, working throughthe summation phenomenon discussed earlier.More often, however, angina with eating isusually a sign of advanced coronary diseaseor of the pre-infarctional state. The few studiesof hemodynamics during eating have failed toindicate major changes either in blood pres-sure or in cardiac output, and heart rate doesnot rise much above 110. Perhaps unrecog-
145
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

GORLIN
nized visceral coronary reflexes or alterationsin the chemical constituents of the blood maybe important in angina of eating.
Angina with Cold WindThis symptom is virtually characteristic for
angina related to coronary heart disease, andis less commonly seen when other diseaseunderlies the anginal state. Its mechanism isunclear. Freedburg and co-workers21 demon-strated that anginal pain and electrocardio-graphic abnormalities following exercise weremore readily elicited if the subject were ina cold as opposed to a warm room, or heldice cuLbes in his hands. Murray22 has shownthat a blast of cold air can cause electro-cardiographic changes in some subjects withcoronary disease. He has recently demon-strated in the dog that cold air triggersa marked vasoconstrictor reflex in the system-ic and possibly the pulmonary vasculaturewhich can be blocked by local anesthesiato the pulmonary airway.23 Perhaps similarto observations reported during "spontaneous"angina, hypertension and concurrent coro-nary vasoconstriction result from exposure tocold air.
Nocturnal AnginaThis form of angina was once considered
solely a late and quite serious manifestationof myocardial ischemia. We now know thatthis can be the presenting manifestation ofangina even preceding angina of effort. Itsmechanism is unclear, but three possibilitiesseem reasonable: (1) nocturnal angina maypoint to early heart failure and be asymptom equivalent to paroxysmal nocturnaldyspnea; (2) nocturnal angina may be dueto fall in blood pressure at night with inade-quate perfusion of the myocardium be-yond a stenosed coronary artery; and (3)nocturnal angina may be due to sympatheticdischarge as in "spontaneous" angina, andmay be brought about as a reaction to adream.Angina can also occur with idiosyncrasy
to tobacco, coffee, drugs, etc. The reasonsare as yet unclarified.
Amelioration of Angina PectorisAngina pectoris can be mitigated in
various ways.1. Morphologic: Total infarction may de-
stroy the nerve receptors of an ischemic regionor new anastomotic collateral ingrowths mayeventually revascularize a region formerlyischemic. The development of heart failuremay alleviate angina as well. This is usuallyattributed to lessened physical activity, butit may involve, to a greater degree, themode or vigor of contraction of the heartplus a more sluggish mechanical response ofthe failing heart to environmental stress. (Inthis connection an occasional patient willsuffer aggravation of angina pectoris upondevelopment of heart failure with relief byspecific therapy of failure.)
2. Physiologic: Cessation of physical effortor control of emotional tension can alleviateangina. Carotid sinus pressure usually stopsan anginal attack for reasons unknown. Therelief is too rapid to be due solely to slowingof the pulse, and may involve inhibition ofsympathetic constrictor activity.
3. Pharmacologic: Smooth muscle relaxantscan relieve angina. The caliber of largearteries can be visibly increased by nitrites,but this implies nothing about total bloodflow along the vessel. It may well be thatdistribution of blood flow may be improvedthrough dilatation of collateral vessels. Ifsevere arteriolar constriction or spasm oc-curs, as in "sponitaneous" angina (fig. 6),the nitrites can effect dilatation and thereforerelief of ischemia. The fact that relief ofpain cannot alwyas be attributed to relief ofischemia is illustrated in the relief of painwith monamine oxidase inhibitors. Patients onsuch agents often obtain pain relief, butcontinue to show gross alterations in electro-cardiographic response to exercise, and theyoccasionally develop frank myocardial infarc-tion without pain. This indicates how paintransmission or perception can be dramati-cally diminished without change in the under-lying pathologic process.
Czrculaiion, Voiume XXXII, July 1965
146
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

PATHOPHYSIOLOGY OF CARDIAC PAIN
General Formulation ConcerningAngina Pectoris (Fig. 7)
Almost invariably angina pectoris occursin the presence of obstructive coronary arterydisease or of myocardial hypertrophy. Ische-mia can be precipitated by any set of circum-stances which disturbs the balance betweenoxygen supply and oxygen demand. Oxygendemand can be chronically augmented byany disease process chronically increasingcardiac activity. This demand can be acutely
Figure 7
This figure encompasses those factors believed toenter into the production of angina pectoris. A partial-ly obstructing atherosclerotic plaque is depicted in
one vessel and not in another. PPS, pain-producingsubstances; PF, arterial pressure; P2. postobstructionarterial pressure; P3. arteriolar pressure. Because P2is less than P1. the superimposition of sympatheticallymediated arteriolar constriction (or arterial spasm)will act to reduce Ps further, and therefore reducesegmental flow. Thus, regional ischemia can readilybe induced. Also effective are autonomic impulses in-creasing inotropic or chronotropic activity of theheart (and particularly in the ischemic zone). Theinduction of ischemia releases pain-producing sub-stances (PPS), stimulating unmyelinated, free-branch-ing nerve endings. This sensory information passesvia a paravascular network to the autonomic gangliathrough a series of synapses to the brain. Theseimpulses are also integrated with sensory impulsesarising from other nearby organs.
Circulation, Volume XXXII, July 1965
increased by any stress which acutely in-creases cardiac pressure, contraction, or rate.Emotion, through autonomic stimuli to theheart, can even be more detrimental thaneffort in provoking ischemia. Conversely, ther-eserve mechanism of oxygen supply canbe chronically compromised by disease pro-cesses chronically affecting oxygen transport(anemia). Oxygen supply can be acutelycompromised by reduction in perfusion pres-sure or time and, more important, by acutecoronary vasoconstriction (or coronary spasmif it occurs clinically). Acting as a resistancein series with arterial obstruction, constric-tion can readily induce ischemia in thediseased heart. Thus, the potential exists forischemia to occur with varying degrees ofmorphologic coronary disease, dependingsolely on what other influences play uponthe heart. For example, severe coronarydisease may be decompensated by even amild anemia or mild physical effort. By con-trast, a single moderate coronary stenosis canbe made highly significant by the simultaneouseffect of increased cardiac effort and coro-nary vasoconstriction. Special emphasis mustbe given to reflexes from the central nervoussystem in changing cardiac activity. Theresponse to an emotional stress or to externalstimuli, such as environmental cold, mayinvolve acute hypertension, tachycardia, andaugmented vigor of contraction. Such stimu-lation may be poorly tolerated in the damagedand potentially ischemic heart. In addition,active coronary vasoconstriction, an "inap-propriate" sympathetic nervous system re-sponse, may be a major factor in many attacksof angina. Vasoconstriction further com-promises coronary supply in areas distal toarterial obstruction or narrowing, particularlyunder circumstances demanding augmentedcardiac performance.The interplay of all these factors may well
explain some hitherto confusing aspects ofclinical angina. The occurrence of ischemiais not necessarily a good yardstick for thesignificance of morphologic coronary disease.Not only is there the anatomic variable ofcollateral flow, but there is the functional
147
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

GORLIN
variable of load on the heart and antagonisticreflexes to modify the ischemic resultant ofany given degree of coronary disease.Once ischemia occurs, it may be recog-
nized biochemically as cardiac lactate produc-tion, and is often associated with ab-normalities in the electrocardiogram and incardiac performance. Ischemia releases chemi-cal by-products, of the polypeptide variety,which act on nonspecific nerve endings in theheart. This stimulus is returned to the spinalcord, sorted, and sent to the cerebral cortexfor further analysis. Whether ischemia actuallyresults in pain or causes more pain thanseems appropriate, will depend on the amountof pain substances produced, on the numberof intact receptors stimulated, on reception,and finally on the competition and augmenta-tion within the nervous system frominformation originating in other organs or fromconditioned pathways developed from priorpsychic experiences.
AcknowledgmentThe author acknowledges the invaluable contribu-
tions to these studies of Drs. Michael D. Klein, Fran-cis J. Lane, Michael V. Herman, Jay M. Sullivan,William C. Elliott, and Lawrence S. Cohen.
References1. HEBERDEN, W.: Commentarii de Morborum, His-
toria et Curatione. A. Londini, T. Payne, 1802.2. FOTHERGILL, J. M.: The Heart and its Diseases.
Philadelphia, Lindsay & Blakiston, 1879.3. HERRICK, J. B., AND NUZUM, F. R.: Angina
pectoris. J.A.M.A. 70: 67, 1918.4. MACKENZIE, Sm JAMES: Angina Pectoris. London,
H. Frowde & Hodder & Stoughton, 1923.5. LEVINE, S. A.: Angina pectoris (some clinical
considerations). J.A.M.A. 79: 928, 1922.6. KEEFER, C. S., AND RESNIK, W. H.: Angina pec-
toris: A syndrome caused by anoxemia of themyocardium. Arch. Int. Med. 41: 669, 1928.
7. BLUMGART, H. L., SCHLESINGER, M. J., ANDDAVIS, D.: Studies on the relation of theclinical manifestations of angina pectoris,coronary thrombosis and myocardial infarctionto the pathological findings. Am. Heart J. 19:1, 1940.
8. COHEN, L. S., ELLIOTT, W. C., ROLETT, E. L.,AND GORLIN, R.: Hemodynamic studies dur-ing angina pectoris. Circulation 31: 409, 1965.
9. ELLIOTT, W. C., COHEN, L. S., KLEIN, M. D.,LANE, F. J., AND GORLIN, R.: Selective cine-
arteriographic study of angina pectoris in val-vular heart disease. Circulation 30: 73, 1964.
10. ZOLL, P., WESSLEiR, S., AND BLUMGART, H. L.:Angina pectoris: Clinical and pathologicalcorrelation. Am. J. Med. 11: 331, 1951.
11. LowN, B., AND LEVINE, S. A.: The carotid sinus:Clinical value of its stimulation. Circulation23: 766, 1961.
12. MULLER, O., AND R0RvIN, K.: Hemodynamicconsequences of coronary heart disease withobservations during anginal pain and on theeffect of nitroglycerin. Brit. Heart J. 20: 302,1958.
13. LIM, R. K. S., LwU, C. N., GUZMAN, F., ANDBRAUN, C.: Visceral receptors concerned invisceral pain and the pseudaffective responseto intra-arterial injection of bradykinin andother algesic agents. J. Comp. Neurol. 118:269, 1962.
14. GUZMAN, F., BRAUN, C., AND LIM, R. K. S.: Vis-ceral pain and the pseudaffective response tointra-arterial injection of bradykinin and otheralgesic agents. Arch. Int. Pharmacodyn. 136:353, 1962.
15. EDERY, H., AND LEWIS, G. P.: Effect of pH onthe formation and inactivation of plasma kin-ins in blood. J. Physiol. 160: 20 P, 1962.
16. WILLIUS, F. A., AND GRIFFIN, H. Z.: The anginalsyndrome in pemicious anemia. Am. J. M.Sc. 174: 30, 1927.
17. YURCHAK, P. M., AND GOBLIN, R.: Paradoxicalsplitting of the second heart sound in coronaryheart disease. New England J. Med. 260:741, 1963.
18. MESSER, J. V., LEVINE, H. J., WAGMAN, R. J.,AND GORLIN, R.: Effect of exercise on cardiacperformance in human subjects with coronaryheart disease. Circulation 28: 404, 1963.
19. GORLIN, R.: Studies on the regulation of thecoronary circulation in man. I. Atropine in-duced changes in cardiac rate. Am. J. Med.25: 37, 1958.
20. YURCHAK, P. M., ROLETT, E. L., COHEN, L. S.,AND GORLIN, R.: Effects of norepinephrine onthe coronary circulation. Circulation 30: 180,1964.
21. FREEDBURG, A. S., SPIEGL, E. D., AND RISEMAN,J. E. F.: Effect of external heat and cold onpatients with angina pectoris: Evidence forthe existence of a reflex factor. Am. Heart J.27: 611, 1944.
22. MURRAY, M. J.: Effect of inspiration of cold airon electrocardiogram of normal dogs andnormal humans with angina pectoris. Circula-tion 26: 765, 1962.
23. MURRAY, M. J.: The effect of inhalation of coldair on the circulation in dogs. Am. J. Cardiol.15: 141, 1965.
Circulation, Volume XXXII, July 1965
148
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from

RICHARD GORLINPathophysiology of Cardiac Pain
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1965 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.32.1.138
1965;32:138-148Circulation.
http://circ.ahajournals.org/content/32/1/138.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 4, 2017
http://circ.ahajournals.org/D
ownloaded from