Embed Size (px)
Citation preview

DOI: 10.1161/CIRCULATIONAHA.114.010376
1
Clinical Profile and Influences on Outcomes in Patients Hospitalized for
Acute Pericarditis
Running title: Kytö et al.; Clinical Profile and Acute Pericarditis
Ville Kytö, MD, PhD, MsocSc1; Jussi Sipilä, MD2; Päivi Rautava, MD, PhD3
1Heart Center, Clinical Neurosciences; 2Neurology; 3Clinical Research Center,
Turku University Hospital, Turku, Finland
Address for Correspondence:
Ville Kytö, MD, PhD
Heart Center
Turku University Hospital
POB 52, FI-20521 Turku, Finland
Tel: +358405383511
Fax: +35823137206
E-mail: [email protected]
Journal Subject Codes: Hypertension:[114] Pericardial disease, Etiology:[8] Epidemiology
Ville Kytö, MD, PhD, MsocSc1; Jussi Sipilä, MD2; Päivi Rautava, MD,D,D, PPPhDhDhD333
11HeHeHeara t CeCeCennter, Clinical Neurosciences;;; 22NeNN urology; 3Clinicalall RRRese earch Center,
TuTuTurkrkrkuu u UnUnUnivivi eersiiitytyty HHHosspipipittal,,, TTTururrkukuku, , FFiFinlnllanand d d
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
2
Abstract
Background—The clinical profile with regard to gender and the influences on outcomes in
patients who have been hospitalized for acute pericarditis are largely uncharacterized.
Methods and Results—We studied all patients aged 16 years admitted to hospital due to acute
pericarditis (post-pericardiotomy and myocardial infarction associated pericarditis were
excluded). Data were collected from a Finnish national registry including data on all
cardiovascular admissions (670,409) during 9.5 years in 29 hospitals nationwide. During the
study period there were 1,361 admissions for acute pericarditis. Pericarditis patients were more
likely to be male (64.9% of patients) than female (35.1%) with age-adjusted likelihood ratio of
1.85 (95% confidence interval (CI) 1.65-2.06, p<0.0001) for male sex. Standardized incidence
rate of hospitalizations for acute pericarditis was 3.32 per 100.000 person-years. Men aged 16-
65 were at higher risk for pericarditis (relative risk (RR) 2.02; CI 1.81-2.26; p<0.0001) than
women in general admitted population with highest risk-difference among young adults. Acute
pericarditis caused 0.20% (CI 0.19-0.22%) of all cardiovascular admissions. Proportion of
caused admissions declined by estimated 51% per 10-year increase in age. In-hospital mortality
rate for acute pericarditis was 1.1% (CI 0.6-1.8%). Mortality increased with age (HR 3.26; CI
1.78-5.95; per 10-year increase in age; p=0.0001) and severe co-infection (pneumonia or
septicemia) (HR 13.46; CI 2.26-80.01; p<0.005) but was not associated with sex in multivariate
analysis.
Conclusions—Patients hospitalized for acute pericarditis are more commonly men. Increasing
age and severe co-infection are associated with greater in-hospital mortality in hospitalized acute
pericarditis patients.
Key words: pericardial disease, pericarditis, sex, aging, epidemiology
ate of hospitalizations for acute pericarditis was 3.32 per 100.000 person years. MMenen aageg dd 1616
65 were at higher risk for pericarditis (rela tive risk (RR) 2.02; CI 1.81-2.26; p<00...000000 11)1) tthahhannn
women in general admitted population with highest risk-difference among young adults. Acute
pericaarditis ccaua sesed d 0.20% (CI 0.19-0.22%) of alll cara diovascular admissssioions. Proportion of Proportion of
cacaausuuseeded admdmisisi sionons s dedeclclinineded by y esestit mamatet d d 5151% % peperr r 110- yeyearar iincreeaasasee inn aagege. Inn-hhosospipitaal momortallitity
aateee ffor acute ppererricccarrdidditiiss wawaass 11.1%1%% ((CCCI 00.6--1..8%))). MMorororttatalilittyty iincnccreeasededd wwwitith h h aagage e (H(H(HR R R 333.262626; CICICI
1.1.787878-5-5- .9.95;; pppererer 11000-yyeyeararr inncncreeaasa e e e inin aaagegge; ; ; pp=p=0.0.000000101 (p(ppneneeumumonononia orr r )) aannd d seeeveverrere cco-o--innnfefectctioionn
eptpticiceemiaia)) (H(HR R 133 4.46;6; CCI I 2.2626 8-80.0 01;; p<p<0.0 00005)5) but wwasas nonot t asa soociciatateded wwiti h h sesex x ini mmulu titivavaririatte e
analysy is.
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
3
Acute pericarditis is an inflammatory disease of pericardium triggered commonly by viral
infections in developed countries, while tuberculosis is the most common cause in developing
countries 1, 2. Experimental studies have found males to be at higher risk for acute viral heart
disease 3, 4, but clinical studies have reported conflicting results on sex distribution of acute
pericarditis patients 5-7. It is commonly thought that there is no specific sex predisposition to
pericarditis 8. Murine studies have also found the susceptibility for viral heart disease to be
significantly age-dependent with highest sensitivity at adolescence or young adulthood 9. Mean
age of acute pericarditis patients in clinical series has ranged from 41 to 60 years 5, 10-12, but sex
associated differences in age have not been reported. Prognosis of viral/idiopathic pericarditis is
good 12, but purulent and tuberculosis pericarditis have high mortality 13. Female sex has been
associated with complications after acute pericarditis14, but this little is known about the effect of
age. We studied the associations of age- and sex- with occurrence of acute pericarditis in all-
comer adult patients using a multihospital, nationwide setting.
Methods
Study patients and data collection
Patients aged 16 years admitted to hospital due to acute pericarditis during a 9.5 year period
were studied. Postpericardiotomy syndromes and post infarction pericarditis were excluded. Data
of all cardiovascular hospital admissions (n=670,409) between May 1st, 2000 and October 31st,
2009 in 29 hospitals were retrospectively collected from the Finnish Hospital Discharge Register
(FHDR), a nationwide maintained by the Finnish National Institute for Health and Welfare
database containing hospital discharge data of all hospital admissions in Finland. Patients aged
16 years with acute pericarditis as the primary cause of admission (ICD-10 codes I01.0 and I30)
good 12, but purulent and tuberculosis pericarditis have high mortality 13. Femalee sexexx hhhasasas bbbeeeeeenn
associated with complications after acute pericarditis14, but this little is known about the effect ofkk
agge.e.e. WeWeWe ssstututudidd eddd ttthhehe associations of age- and sex-x-x- wwwith occurrencecee of f acacacuutute pericarditis in all-
coommemer adult paatiitienenentss uuusisingngng aa mmmulultitiihohohosspppittaal, nnnatttionnwwiidee sseettttinini gg.g.
Methods
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.114.010376
4
were identified. Co-morbidities and potential etiologies were detected from hospital discharge
diagnoses. Study population was mainly Caucasians. Differences in incidence rate were
estimated using age- and sex-matched population data of Finland from the study period
(39,523,746 person-years) obtained from Statistics Finland.
Hospital organization in Finland consists of three main levels: 5 university
hospitals represent the highest level of hierarchy, followed by 16 central hospitals with coronary
angiolaboratory and intensive care units, and smaller regional hospitals. Treatment of acute
cardiovascular patients occurs mainly in university and central hospitals. This study included
data from all university and central hospitals and 8 large regional hospitals located across the
country. The study was conducted according to the National Institute for Health and Welfare
permission (THL/1576/5.05.00/2010).
Statistical analysis
Data was analyzed with Poisson regression models. In the Poisson model of incidence rate, the
logarithm of population was used as an offset and in the model for the proportion of
cardiovascular admissions, the logarithm of total cardiovascular admissions was used as an
offset. Sex-differences in dichotomous variables were estimated by modified Poisson regression
with robust error variances15. In-hospital mortality during admission for acute pericarditis was
studied using Cox-regression model stratified by study year with exact method for failure time
ties. Multivariate mortality model included patient characteristics associated with mortality at the
level of p<0.1 in univariate analysis. Variables displayed in Table 1 in addition to gender and
age were considered as potential predictors of in-hospital mortality. Scale variables are presented
as mean±standard deviation or median with interquartile range (IQR) as appropriate. Total
incidence rates were standardized with US 2000 standard population by using a direct method.
country. The study was conducted according to the National Institute for Health h aaand dd WeWeWelflflfararareee
permission (THL/1576/5.05.00/2010).
Sttatatatisisistititicacaalll anananalysysysiisis
DDattata was analylyzzeeddd wiwiithth PPPoioioisssssoonon rrregegegreressssiion momodells. Innn tththee PoPooisisssosonn momoodeeel l ofofof iiincncidididenenncecee rrataate,e, thhhe
oogagagariririthththm m ofofof ppopoppulullatatioioon n wawas ususu ededed aaasss anann oooffffffsssetet f aaandndnd iinnn ththhe e momomodededel ll ffofor rr thththee prrropopoorortititiononn ooofff
cardiovascullararar aaadmdmmisisi sisis onoo s,s,, ttheheh lllogogogararariti hmhmhm ooof f f totootatata ll cacacardrdr iooovavavascscsculululararar aadmdmdmisisissisis onononsss wawawas s s usususededd as an
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
5
Categorical variables are presented as counts, percentages or relative risks (RR) with 95%
confidence intervals (CI) as appropriate. Confidence intervals were calculated using Poisson
distribution. P-values <.05 were considered statistically significant. The SAS system version 9.3
(SAS Institute Inc, Cary, NC, USA) was used for statistical analyses.
Results
Frequency
The study period included 1361 hospital admissions with acute pericarditis as primary diagnosis.
Pericarditis patient was more likely to be male (64.9% of patients; CI 60.7-69.3%) than female
(35.1%; CI 32.0-38.4%) with age-adjusted likelihood ratio of 1.85 (CI 1.65-2.06, p<0.0001) for
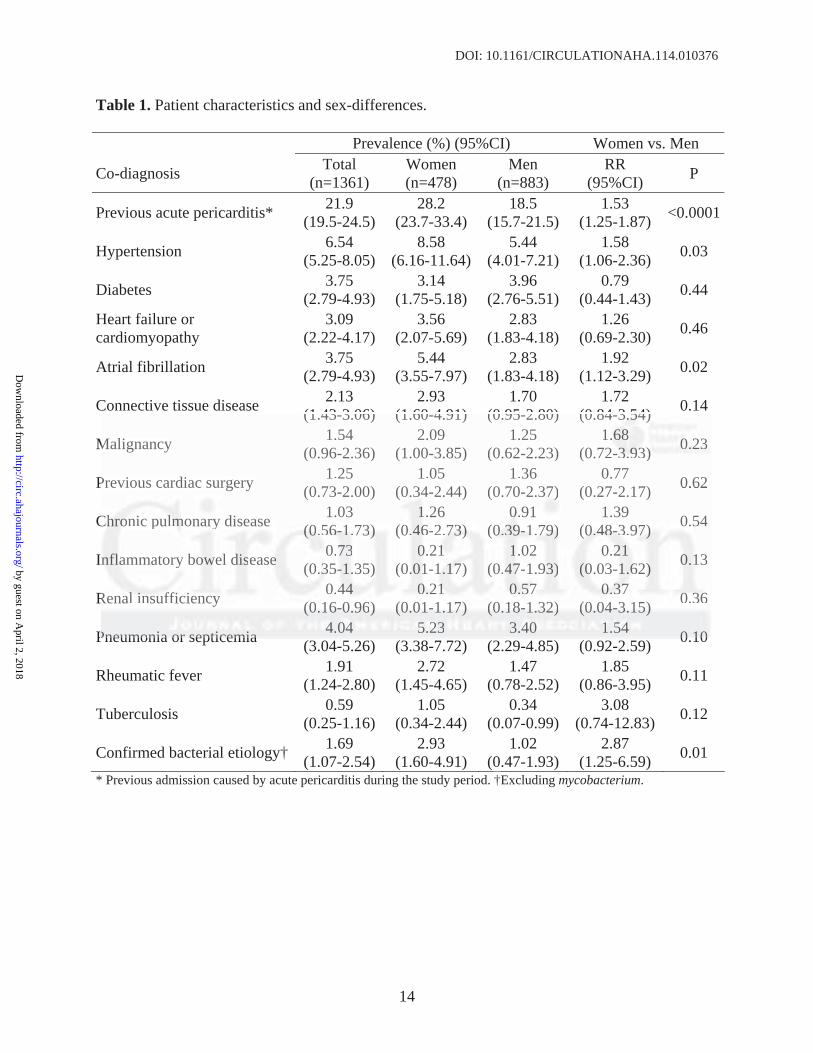
male sex. Prevalence of potential etiological co-morbidities was similar between men and
women, but previous acute pericarditis was more common among women (Table 1). In addition,
bacterial etiology was confirmed more commonly in women. Acute pericarditis patient was
most commonly aged 50-59 years with median age of 52 years (range 16-93, IQR 35-63 years)
(Figure 1A). Male patients were significantly younger than female patients (mean 45.9±18.3 vs.
56.2±17.3 years, p<0.0001). Age distribution varied significantly by sex, as proportion of male
patients was notably higher in patients aged 16-65 years (Figure 1B). Median duration of
admission for acute pericarditis was 5 days (IQR 3-8). Women were treated longer than men
(7.5±6.9 vs. 6.1±5.1 days, age-adjusted p<0.0001). Admission lengthened by estimated 10% per
10-year increase in age (RR 1.10; CI 1.09-1.12, p<0.0001).
Acute pericarditis as cause of hospital admission
Acute pericarditis caused 4 % of all cardiovascular admissions among adults aged 16-20 years,
but the proportion decreased by estimated 51% (RR 0.49; 95% 0.48-0.51, p<0.0001) per 10-year
35.1%; CI 32.0-38.4%) with age-adjusted likelihood ratio of 1.85 (CI 1.65-2.06,6,, p<0<0< .0.0.00000001)1)1) fforo
male sex. Prevalence of potential etiological co-morbidities was similar between men and
wowomememenn,n, bbbututut ppprevivivioouous acute pericarditis was morrre ee cooommon amonggg womommeenen (Table 1). In addition,
bbaactcttere ial etioloogygyy wwwasas conononfififirmrmrmeded mmmoororeee cccommmmooonlyyy iinn wowowomemeen.. AAccuutute e pepeerriicacardrdrdiititisis pppatattieieiennnt wwwasass
momooststst cccomomo momomonlnly y y agggeded 500-0-595 yyyeaaarsrsrs wwwitithh h mememeddidianann agagge e ofoff 55222 yeyeyeararrsss (r(r(rananngegeg 166-6-93933, , , IQIQIQRR R 33535-6663 yeyeaaars)s)s)
Figure 1A).). MMMalaleee papapatitit enee tstss wwwererre e e sisis gngng iffficici ananantltltly y y yoyoyoununungegeger thththananan fffemememalaa e e e papapatitiienenentststs (m(mmeaeaean n n 454545.9±18.3 vs..
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.114.010376
6
increase in age to 0.02 % in patients aged 85 years or older (Figure 2). Overall, 0.20% (CI 0.19-
0.22%) of cardiovascular admissions were caused by acute pericarditis. In men, pericarditis
caused 0.24% (CI 0.22-0.25%) of admissions while this proportion was 0.16% (CI 0.15-0.18%)
in women. Men aged 16-35 were more likely to have acute pericarditis as the cause of admission
than women, while opposite was true for patients aged 46-75 (Figure 2B).
Incidence rate
Overall incidence rate of acute pericarditis was similar in population aged 16-49 years, but
increased in older population (Figure 3A). Incidence rate among men was 4.52 (CI 4.22-4.83)
per 100,00 person-years, with declining trend between 16-45 years followed by re-increase in
older population segments (Figure 3B). Among women, standardized incidence rate of acute
pericarditis was 2.11 (CI 1.91-2.32) per 100,000. Incidence was lowest among young women,
followed by gradual increase with age with peak in population aged 65-74 years. Young (16-35
year old) men had highest incidence of acute pericarditis compared to young women (incidence
rate ratio 4.65; CI 3.52-6.14, p<0.0001). Sex-difference in incidence rate was reduced with
increasing age, and in population aged 66 years rate for acute pericarditis was similar in both
sexes (Figure 4). Total standardized incidence rate of acute pericarditis was 3.32 (CI 3.14-3.50) /
100,000 person-years. Incidence rate of acute pericarditis was 2.02 (CI 1.81-2.26; p<0.0001)
times higher among men compared to women in total population (Figure 4).
In-hospital mortality
In-hospital mortality rate for acute pericarditis was 1.10% (CI 0.61-1.82). Female sex was
associated with increased mortality in univariate analysis, but was not an independent predictor
of death in multivariate model (Table 2). Mortality increased significantly with age in both
univariate and multivariate analysis (Table 2). Strongest predictor of in-hospital mortality in
older population segments (Figure 3B). Among women, standardized incidencee rrratatte ee ofofof aaacucucutetete
pericarditis was 2.11 (CI 1.91-2.32) per 100,000. Incidence was lowest among young women,
foolllllowowowededed bbby y y gggradadduauaual l increase with age with peak k k inin population agggedee 665-5-5-77474 years. Young (16-35
yyearrar old) men n hahahad hiiighghg eesesttt ininincicicidedencncnceee ooff aaacuttee pppericacaardiittisiss ccomomompapareredd toto yyoououngngng wwomommenenn (((inini cicicideedencncce
aatetete rrratatatioio 444.6.6.655;5; CCCI 3.3.52522-666.1.14, ppp<<<000.00000001011).). SSSexexex-dddififi fefeferereenccce ininin iiincnccididi eeencncce e e raraateee wwaasas rrrededucucuceded wwititi h h
ncreasing agegege,, ananand d d inini pppopopulululatatatiooon n n agaggedede 666666 yyyeaeaearsrss rrratatate e fofofor rr acacacututute e e pepp ririricacacardrdrditititisiss wwasasas sssimimimilili ara in both
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
7
acute pericarditis was severe co-infection (pneumonia or septicemia). Co-morbidities listed in
Table 1, but not in Table 2 were not associated with in-hospital mortality in univariate analysis.
Discussion
This nationwide multi-hospital study describes age- and sex- associated occurrence of acute
pericarditis at the population level. Previous studies have reported conflicting results on effect of
sex on risk of pericarditis 5-7. Recent randomized trial of 240 acute pericarditis patients found
60% of patients to be male6, while previous studies have reported higher male prominence7, but
also female prominence5. We found 65% of 1361 patients to be male and the age-adjusted
likelihood of acute pericarditis patient to be a male was 1.9. Furthermore, the incidence rate of
acute pericarditis in general adult population was two-fold among men compared to women.
Etiology of acute pericarditis is idiopathic in majority of cases but with an immune-
mediated process probably triggered by a viral infection in many cases 16, 17. Reasons of sex-
differences in pericardial inflammation are unknown, but experimental viral studies of
myocardial inflammation have suggested that although genetic differences have some effect, sex
hormones are major contributors for sex predisposition 3, 18. Testosterone appears to play a
major role in development of myocarditis, as exogenous testosterone increases viral replication
and inflammation in the heart and gonadectomy inhibits cardiac inflammation in experimental
viral myocarditis 19, 20. Mechanisms of testosterone action include inhibition of anti-
inflammatory cells 19, commitment to Th1 type immune response 21, and increasing viral binding
to myocytes 20. In accordance with testosterone-effect, we found the risk for pericarditis to be
significantly higher among young men compared to women. Although occurrence of acute
pericarditis in men declined with age after teenage years, there was a re-increase in occurrence
ikelihood of acute pericarditis patient to be a male was 1.9. Furthermore, the inccidiidenee cecee rrratatateee ofof
acute pericarditis in general adult population was two-fold among men compared to women.
EtEtEtioioiololologyy ooofff aacute pericarditis is idiopathihiicc c innn majority of cccasaa ess bbbuutut with an immune-f
mmeddidiated procecessss ppproobabab blblbly y trtrrigigiggegerrered d d bbyy a viirraal infffeecctiononon iin n mmamanynyy cccasasesess 166, 177. RReReasassononnss ofofo sssexex--
didifffffferererenenencecesss ininin ppeericccarardddiaalal iinfnfflalal mmmmmmatatatioionnn ararareee unununknknk owowown,n, bbututut eeexpxpxperere imimmenenentatalll vviviraralll ststtududu ieieiesss offf
myocardial iinfnfnflalaammmmmmatattioioion hahahavevv sssugugu gegegestttededed ttthahahatt t alala ththhouououghghg gggeneneneteteticicc dddifi fefeferererencncnceseses hhhavavveee sososomemem effect, sexxx
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.114.010376
8
after 45 years of age. This may suggest that interaction of testosterone with susceptibility to
pericarditis may not be linear or that unrecognized etiology of pericarditis varies by age.
Female sex hormones also affect the risk for cardiac inflammation. Progesterone
aggravates cardiac inflammation 22 while oestrogen has inhibitory effects by favouring inhibiting
pro-inflammatory T-cells 23, stimulating inhibitory T cells 24 and favouring Th2 type immune
response 21. Accordingly, we found the incidence of pericarditis in women to be highest at
postmenopausal period when estrogenic levels are low. In addition to viral infections, systemic
connective tissue diseases are potential causes of acute pericarditis 25. In line with previous
studies 6, 7, connective tissue disease was diagnosed in 2 % of our patients. Women have a
general higher tendency for connective tissue diseases associated with pericarditis, e.g, systemic
lupus erythematosus and rheumatoid arthritis 26, but we found no sex difference in prevalence
among acute pericarditis patients. Systemic autoimmune diseases are however a diagnostic
challenge 27 and autoimmune processes begin earlier than classical clinical symptoms are
diagnosed 28.
Few studies have reported on epidemiology of pericarditis. Pericarditis is found in 4.4 %
of emergency room chest-pain patients 29 and in 1.7% of patients with ST-segment elevation 30 of
whom myocardial infarction is ruled out. We found acute pericarditis to be a significant cause of
cardiovascular admissions among young adults, but with increasing general morbidity the
proportion deceased logarithmically with aging. Pericarditis was a more likely cause of
admission to men at younger age-groups, but to women at ages of 46-75. Overall, pericarditis
caused 0.2% of hospital admissions, which compares to previous estimate of acute pericarditis
causing 0.1% of all hospital admissions 1. Swedish registry study found incidence rate of 18.0
per 100,000 for pericarditis in general population 31 while clinical study conducted in Italian
general higher tendency for connective tissue diseases associated with pericardititiiss, eee.ggg,, sysysystststememe ic
upus erythematosus and rheumatoid arthritis 26, but we found no sex difference in prevalence
ammononongg g acacutututee ppeririicacacardr itis patients. Systemic autoooiimimmmune diseases s ara e hohohowwwever a diagnostic
hchhalalllel nge 277 andndd auuutoioiimmmmmununneee pprprococcesesssesees bbeggiinn earrllieeer thhhaanan ccclaaassssiciccaall ccliliininn ccacal l sysysympmptototommsms aareree
didiagagagnononosesedd 28288.
Few ststtudududieiees s s hahahaveveve rrepepeporoo teteed d d ononon eepipipidededemimimiololologogogy yy ofofo pepepeririicacacardrdditititisisi . PePePeririricacacardrdrdititisss iiisss fofofoununu d in 4.4 %%
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
9
urban metropoly area reported incidence rate of 27.7 per 100,000 11. In retired US military
personnel, the incidence rate of pericarditis is 7.4 / 100,000 32. We found an incidence rate of 3.3.
per 100,000, reflecting the fact that we included only patients with acute pericarditis admitted to
hospital and excluded pericardiotomy and myocardial infarction caused disease. Since
overdiagnosis of pericarditis is common14, we maximized the accuracy of real-life diagnosis by
including patients that had been examined and diagnosed at the hospital ward. This, in addition
to the fact that our data collection did not cover all of the smallest regional hospitals that treat
cardiac patients, may result in underestimation of the absolute incidence rate of acute
pericarditis.
Presentation of pericarditis varies from chest pain to classical symptoms of cardiac
tamponade. Prodromal syndrome of fever, myalgia, and malaise is common33. Main findings
include ST-level changes in ECG, elevation of circulating inflammatory markers, friction rub in
cardiac ausculation, fever, and pericardial effusion in echocardiography2, 33, 34. In clinical
practice, and in the current study, diagnosis is based on combination of these findings, exclusion
of acute coronary syndromes when appropriate, and clinical judgment. Diagnosis of even life
threatening pericarditis is however a challenging task as demonstrated by study on unrecognized
causes of death in intensive care unit 35.
This study has some limitations. Major limitation is the retrospective nature of
observational registry data. Thus, diagnoses were made by treating physicians, which may have
affected the included patient population and accuracy of co-morbidity data. In addition, as we
included only hospitalized patients our results may underrepresent patients with low-risk features
that may be treated without admissions 14. Although we report on potential etiological co-
morbidities, the nature of our data does not allow describing on detailed etiological studies. Also,
Presentation of pericarditis varies from chest pain to classical symptoms ooof f cacc rdrdrdiaiaiacc c
amponade. Prodromal syndrome of fever, myalgia, and malaise is common33. Main findings
nnclclludududeee STSTST-l-l-leeevelel ccchahah nges in ECG, elevation of cicicircrcuulating inflammmamm tooryryry mmarkers, friction rub in
caardddiai c auscullatatioii nnn, fffeeeveerer, ananand dd peperirir ccacarrddiiaal efefffuuusioonn iin ececechohoccacardrdioiooggrrapaphyhyh 22,, 33,, 343434.. InIn ccclililininiicacac l ll
prpracacactititicecec ,, , anannd d d inin ttthehee ccuruurrereentnt stututudydydy, dididiagagnononosisisis s s iss babab ssseddd oonon cccomomombibibinananatitiononon ooff ththhesesse ee fififindnddininingsgs,,, exxxclcluuusiioon
of acute corononnarararyyy sysysyndnddroror mememes s s whwhhenene aaappppprororoprprpriaiaiatetete, , ananand d clc ininnicicicalalal jjjudududgmgmgmenenent.t.t DDDiaiaiagngng osososisisis ooof f f eve en life
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
10
since prevalence of tuberculosis in Northern Europe is very low, our results may not be
applicable world-wide.
Prognosis of acute pericarditis is usually good. Although mortality in idiopathic / viral
pericarditis is low, purulent pericarditis is always fatal if untreated and carries a mortality of c.a.
40 % even when treated13, 36. Purulent pericarditis is commonly a complication of intra-thoracic
infection or a consequence of haematological bacterial spread13. Accordingly, we found
pneumonia and septicaemia to be strong predictors of in-hospital mortality. Female sex has been
associated with complications in acute pericarditis14. We found female sex to be associated with
mortality in univariate analysis, but not in multivariate analysis. Increasing age was however an
independent predictor of death.
In conclusion, men have a two-fold incidence rate of acute pericarditis compared to
women with highest difference among young adults. Increasing age and severe co-infection
predict in-hospital mortality in acute pericarditis, but sex does not appear to be an independent
risk factor for death.
Funding Sources: This study was funded by the Clinical Research Foundation of Turku
University Hospital.
Conflict of Interest Disclosures: None.
References: 1. Lange RA and Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004;351:2195-2202.
2. Imazio M, Spodick DH, Brucato A, Trinchero R and Adler Y. Controversial issues in the management of pericardial diseases. Circulation. 2010;121:916-928. 3. Huber SA, Job LP and Auld KR. Influence of sex hormones on Coxsackie B-3 virus infection
ndependent predictor of death.
In conclusion, men have a two-fold incidence rate of acute pericarditis compared to
wowomememennn wiwiwiththth hhhigghehehestst difference among young addduuulttss. Increasing aagegg aandndnd ssevere co-infection
predddici t in-hosspipiittatall momoorrtalalalititity y ininin aacucuutetee ppererricarrrdiiitis, buuut sssexexx ddoeoeoes s nnoott apppepeeaarr ttooo bebbe aan nn ininndededepeeendndndenenentt r
iisksksk fffacacactotorr fofoforr dedeeatatth.h.
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
11
in Balb/c mice. Cell Immunol. 1982;67:173-179.
4. Li Z, Yue Y and Xiong S. Distinct Th17 inductions contribute to the gender bias in CVB3-induced myocarditis. Cardiovasc Pathol. 2013;22:373-382.
5. Imazio M, Bobbio M, Cecchi E, Demarie D, Demichelis B, Pomari F, Moratti M, Gaschino G, Giammaria M, Ghisio A, Belli R and Trinchero R. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation. 2005;112:2012-2016. 6. Imazio M, Brucato A, Cemin R, Ferrua S, Maggiolini S, Beqaraj F, Demarie D, Forno D, Ferro S, Maestroni S, Belli R, Trinchero R, Spodick DH, Adler Y and Investigators I. A randomized trial of colchicine for acute pericarditis. N Engl J Med. 2013;369:1522-1528. 7. Zayas R, Anguita M, Torres F, Gimenez D, Bergillos F, Ruiz M, Ciudad M, Gallardo A and Valles F. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75:378-382.
8. Imazio M and Brucato A. Management of pericarditis in women. Womens Health (Lond Engl). 2012;8:341-348. 9. Lyden D, Olszewski J and Huber S. Variation in susceptibility of Balb/c mice to coxsackievirus group B type 3-induced myocarditis with age. Cell Immunol. 1987;105:332-339. 10. Permanyer-Miralda G, Sagrista-Sauleda J and Soler-Soler J. Primary acute pericardial disease: a prospective series of 231 consecutive patients. Am J Cardiol. 1985;56:623-630. 11. Imazio M, Cecchi E, Demichelis B, Chinaglia A, Ierna S, Demarie D, Ghisio A, Pomari F, Belli R and Trinchero R. Myopericarditis versus viral or idiopathic acute pericarditis. Heart. 2008;94:498-501.
12. Imazio M, Brucato A, Barbieri A, Ferroni F, Maestroni S, Ligabue G, Chinaglia A, Cumetti D, Della Casa G, Bonomi F, Mantovani F, Di Corato P, Lugli R, Faletti R, Leuzzi S, Bonamini R, Modena MG and Belli R. Good prognosis for pericarditis with and without myocardial involvement: results from a multicenter, prospective cohort study. Circulation. 2013;128:42-49. 13. Pankuweit S, Ristic AD, Seferovic PM and Maisch B. Bacterial pericarditis: diagnosis and management. Am J Cardiovasc Drugs. 2005;5:103-112.
14. Imazio M, Cecchi E, Demichelis B, Ierna S, Demarie D, Ghisio A, Pomari F, Coda L, Belli R and Trinchero R. Indicators of poor prognosis of acute pericarditis. Circulation. 2007;115:2739-2744. 15. Zou G. A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159:702-706.
8. Imazio M and Brucato A. Management of pericarditis in women. Womens Heaeaaltth hh (L(L(Lononnd d d EnEEnglgl))2012;8:341-348.
9. Lydyden D,, OlO szewski J and Huber S. Variation in susceptibility of Balb/c mice to cooxsxsxsacacckikikieveveviririruuus gggrororoupu B type 3-induced myocardididittisss with age. Ceellllll Immmmmuununol. 1987;105:332-339.
1100. PPermanyer-r-MiMiM raraldldlda G,GG, SSSagagagririststta-a-a SaSaaululledaa J anddd SSSoleeer-r--SoSoleler r J.J PPririmamaryry aacucucutetete ppererericiccarardidid alalal dididiseeeasa e: a prorospeeectttivee seeerieess s oofof 223131 cccoonnsssecuuttivvve ppattieientntnts.s.s. AmAmAm J CCCaarrdiolll. 191988585;5;56:6626233-3-6663000.
11. ImImazioio MM, , CeC cccchihi E, DeD mimichchelelisi B, ChChininagaglilia A, IIerernana SS, , DeDemamaririee D, GGhihisisio o A, PPommararii F, Belli R and TrTrrinininchchherereroo R.RR MMMyoyoyopepeeririricacaardrditititisiss vvvererersusususs vvviriri alala oorr r ididdioioiopapapathththiccc aaacucucutetete ppperere icccararardididititit s.s.s Heart. 20200808;9;94:4:494988-505011
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
12
16. Pankuweit S, Stein A, Karatolios K, Richter A, Ruppert V and Maisch B. Viral genomes in the pericardial fluid and in peri- and epicardial biopsies from a German cohort of patients with large to moderate pericardial effusions. Heart Fail Rev. 2013;18:329-336. 17. Imazio M, Brucato A, Maestroni S, Cumetti D, Belli R, Trinchero R and Adler Y. Risk of constrictive pericarditis after acute pericarditis. Circulation. 2011;124:1270-1275. 18. Fairweather D, Cooper LT, Jr. and Blauwet LA. Sex and gender differences in myocarditis and dilated cardiomyopathy. Curr Probl Cardiol. 2013;38:7-46. 19. Frisancho-Kiss S, Coronado MJ, Frisancho JA, Lau VM, Rose NR, Klein SL and Fairweather D. Gonadectomy of male BALB/c mice increases Tim-3(+) alternatively activated M2 macrophages, Tim-3(+) T cells, Th2 cells and Treg in the heart during acute coxsackievirus-induced myocarditis. Brain Behav Immun. 2009;23:649-657. 20. Lyden DC, Olszewski J, Feran M, Job LP and Huber SA. Coxsackievirus B-3-induced myocarditis. Effect of sex steroids on viremia and infectivity of cardiocytes. Am J Pathol. 1987;126:432-438. 21. Huber SA and Pfaeffle B. Differential Th1 and Th2 cell responses in male and female BALB/c mice infected with coxsackievirus group B type 3. J Virol. 1994;68:5126-5132. 22. Lyden DC and Huber SA. Aggravation of coxsackievirus, group B, type 3-induced myocarditis and increase in cellular immunity to myocyte antigens in pregnant Balb/c mice and animals treated with progesterone. Cell Immunol. 1984;87:462-472. 23. Li Z, Yue Y and Xiong S. Distinct Th17 inductions contribute to the gender bias in CVB3-induced myocarditis. Cardiovasc Pathol. 2013;22:373-382. 24. McCarthy RE, 3rd, Boehmer JP, Hruban RH, Hutchins GM, Kasper EK, Hare JM and Baughman KL. Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N Engl J Med. 2000;342:690-695. 25. Imazio M. Pericardial involvement in systemic inflammatory diseases. Heart. 2011;97:1882-1892.
26. Tedeschi SK, Bermas B and Costenbader KH. Sexual disparities in the incidence and course of SLE and RA. Clin Immunol. 2013;149:211-218.
27. Schirmer M, Duftner C and Dejaco C. Challenges in the diagnosis of chronic immune-mediated rheumatic diseases. Discov Med. 2013;15:160-165.
28. Arbuckle MR, McClain MT, Rubertone MV, Scofield RH, Dennis GJ, James JA and Harley JB. Development of autoantibodies before the clinical onset of systemic lupus erythematosus. NEngl J Med. 2003;349:1526-1533.
1987;126:432-438.
21. Huber SA and Pfaeffle B. Differential Th1 and Th2 cell responses in male andndd fffemememalalaleee BALB/c mice infected with coxsackievirus group B type 3. J Virol. 1994;68:5126-5132.
222. . LyLyLydededennn DCDCDC aandndnd HHuber SA. Aggravation of coooxsxx aackievirus, grouououp B,B,B tttyype 3-induced mymymyooocarditiis aaand d ininincrcreaeaaseses iiin n n cecelllllululularara iimmmmununitity y y toto mymym ocytytyteee anana tigegegensnsn iin n prprpregee nanantntt BBBalalb/b/c c mimim cecee aaandn annimmmals treateed d wiwiw thth ppproroogegegesststerereronone.e.e. CeCeC lll IImmmmunnol. 11998444;8;8;87:7:4646462-2-447472.2.
2333. LiLiLi ZZZ,, , YuYuYueee Y Y annnd d XXXioonongg SS.S. DDDisisistititinncnct t ThThTh171717 indndnduucctitiiononns cococonnntririibubub tete ttto o o ththhe e gegeg nndnderere bbbiaiaiass innn CCCVBVBB33--nduducecedd mymyoccarardititis.s. CCardrdioovavascsc PPatholl. . 20201313;2;22:2 3773-3-38382.2.
2424 McMcCaCartrthyhy RREE 33rdrd BoBoehehmemerr JPJP HrHrububanan RRHH HuHutctchihinsns GGMM KKasaspeperr EKEK HaHarere JJMM anandd
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
13
29. Launbjerg J, Fruergaard P, Hesse B, Jorgensen F, Elsborg L and Petri A. Long-term risk of death, cardiac events and recurrent chest pain in patients with acute chest pain of different origin. Cardiology. 1996;87:60-66. 30. Brady WJ, Perron AD, Martin ML, Beagle C and Aufderheide TP. Cause of ST segment abnormality in ED chest pain patients. Am J Emerg Med. 2001;19:25-28. 31. Elfstrom P, Hamsten A, Montgomery SM, Ekbom A and Ludvigsson JF. Cardiomyopathy, pericarditis and myocarditis in a population-based cohort of inpatients with coeliac disease. JIntern Med. 2007;262:545-554. 32. Lin AH, Phan HA, Barthel RV, Maisel AS, Crum-Cianflone NF, Maves RC and Nayak KR. Myopericarditis and pericarditis in the deployed military member: a retrospective series. MilMed. 2013;178:18-20. 33. Maisch B, Seferovic PM, Ristic AD, Erbel R, Rienmuller R, Adler Y, Tomkowski WZ, Thiene G, Yacoub MH, Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur Heart J. 2004;25:587-610. 34. Seferovic PM, Ristic AD, Maksimovic R, Simeunovic DS, Milinkovic I, Seferovic Mitrovic JP, Kanjuh V, Pankuweit S and Maisch B. Pericardial syndromes: an update after the ESC guidelines 2004. Heart Fail Rev. 2013;18:255-266. 35. Combes A, Mokhtari M, Couvelard A, Trouillet JL, Baudot J, Henin D, Gibert C and Chastre J. Clinical and autopsy diagnoses in the intensive care unit: a prospective study. Arch Intern Med. 2004;164:389-392. 36. Sagrista-Sauleda J, Barrabes JA, Permanyer-Miralda G and Soler-Soler J. Purulent pericarditis: review of a 20-year experience in a general hospital. J Am Coll Cardiol. 1993;22:1661-1665.
he European Society of Cardiology. Guidelines on the diagnosis and managemennt t ofofof ppperericicarardidialdiseases executive summary; The Task force on the diagnosis and management oofof ppperericiccararardididialaal diseases of the European society of cardiology. Eur Heart J. 2004;25:587-610. JJ
34. SeS ferovic PM,, Ristic AD, Maksimovic R, Simeunovic DS, Milinkovic I, Seferovic MitrovicJPP,, KaKaKanjnjnjuhuhuh VVV, PaPaanknknkuuweit S and Maisch B. Pericacacardrdiial syndromes:s:: an upupupdddate after the ESC guguuididdelelini es 2200004.4. HeHeH arartt t FaFaailili RRevevv.. 20202 1313;1;1; 8:8:25255-5-26266.6.
35355. CCoC mbess AA, MoMoMokhtttarrri MM, CCCouvu elellarardd AA, TTTroouilllleett JLJLL, BaBaBaududdot JJ, Henninn n DD,, GGGibiberttt CCC aaanddd ChhhaasstreJ.. CCCliliinininicacall ananandd auauutooopspsyyy ddidiaagnononoseseesss ininin ththhee ininintetetensnssivivive e caaareree uunininit:t:t: aa ppproroospsppecece titiiveee sstututudydydy.. ArArArccch IIInttterernnnMeedd. 20200404;1; 644:3: 899-3-3992.
3636 SaSagrgrisistata S-Sauauleledada JJ BaBarrrrababeses JJAA PPerermamanynyeerr-MiMiraraldldaa GG anandd SoSolelerr-SoSolelerr JJ PPururululenentt
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.114.010376
14
Table 1. Patient characteristics and sex-differences.
Prevalence (%) (95%CI) Women vs. Men
Co-diagnosis Total (n=1361)
Women (n=478)
Men (n=883)
RR (95%CI) P
Previous acute pericarditis* 21.9 (19.5-24.5)
28.2 (23.7-33.4)
18.5 (15.7-21.5)
1.53 (1.25-1.87) <0.0001
Hypertension 6.54 (5.25-8.05)
8.58 (6.16-11.64)
5.44 (4.01-7.21)
1.58 (1.06-2.36) 0.03
Diabetes 3.75 (2.79-4.93)
3.14 (1.75-5.18)
3.96 (2.76-5.51)
0.79 (0.44-1.43) 0.44
Heart failure or cardiomyopathy
3.09 (2.22-4.17)
3.56 (2.07-5.69)
2.83 (1.83-4.18)
1.26 (0.69-2.30) 0.46
Atrial fibrillation 3.75 (2.79-4.93)
5.44 (3.55-7.97)
2.83 (1.83-4.18)
1.92 (1.12-3.29) 0.02
Connective tissue disease 2.13 (1.43-3.06)
2.93 (1.60-4.91)
1.70 (0.95-2.80)
1.72 (0.84-3.54) 0.14
Malignancy 1.54 (0.96-2.36)
2.09 (1.00-3.85)
1.25 (0.62-2.23)
1.68 (0.72-3.93) 0.23
Previous cardiac surgery 1.25 (0.73-2.00)
1.05 (0.34-2.44)
1.36 (0.70-2.37)
0.77 (0.27-2.17) 0.62
Chronic pulmonary disease 1.03 (0.56-1.73)
1.26 (0.46-2.73)
0.91 (0.39-1.79)
1.39 (0.48-3.97) 0.54
Inflammatory bowel disease 0.73 (0.35-1.35)
0.21 (0.01-1.17)
1.02 (0.47-1.93)
0.21 (0.03-1.62) 0.13
Renal insufficiency 0.44 (0.16-0.96)
0.21 (0.01-1.17)
0.57 (0.18-1.32)
0.37 (0.04-3.15) 0.36
Pneumonia or septicemia 4.04 (3.04-5.26)
5.23 (3.38-7.72)
3.40 (2.29-4.85)
1.54 (0.92-2.59) 0.10
Rheumatic fever 1.91 (1.24-2.80)
2.72 (1.45-4.65)
1.47 (0.78-2.52)
1.85 (0.86-3.95) 0.11
Tuberculosis 0.59 (0.25-1.16)
1.05 (0.34-2.44)
0.34 (0.07-0.99)
3.08 (0.74-12.83) 0.12
Confirmed bacterial etiology† 1.69 (1.07-2.54)
2.93 (1.60-4.91)
1.02 (0.47-1.93)
2.87 (1.25-6.59) 0.01
* Previous admission caused by acute pericarditis during the study period. †Excluding mycobacterium.
(1.43-3.06) (1.60-4.91) (0.95-2.80) (0.84-3.3..54545 ) )
Malignancy 1.54 (0.96-2.36)
2.09 (1.00-3.85)
1.25 (0.62-2.23)
1.1.686868 (0.72-2-333.99393) )) 0.0.0 23232
Previous cardiac surgery 1.25 (0.73-2.00)
1.05 (00.34-2.44)
1.36 (0.70-2.3737)))
0.77 (0.27-2.17) 0.62
ChChhroooninic c puulmlmlmonnarary y did seseasase e 1.03 (0(0(0.5.5. 6-6-6 1.1.1 73733)))
11.26 (0( ..466-2.2.737373)))
0.0.0 91 (0(00 33.39-9-9-1.1.1 797979)))
1.39 (0(0(0.4.4.48-8-8-3.3.3 97977))) 0.0 545
nnnfllaaammatoryry bowowowel dddisseasesee 0.0 7373 (0( .3.335-5--1..35))
000.2111 (0( ..011-1.1..171717))
1..0202 (0.44777-1.993)))
0.0 22121 (000.003-11.66262)) 000.113
Renanalll iininsusufffficcieiency y 0.0 444444 (0(0(0 1.1.16-6-6 00.0.969696)))
00.0.212121 (0(0(0 0.0.01-1-1 11.1.171717)))
00.0.575757 (0(0(0 1.1.18-8-8 11.1.323232)))
0.0.0.373737 (0(0(0 0.0.04-4-4 33.3.151515))) 00.0.363636
PnPneueumomoniniaa oror ssepeptiticecemimiaa 44.4 040404 555.2232 3.3 404040 11.1 545454 00 1010
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.114.010376
15
Table 2. Predictors of in-hospital mortality. Results of both univariate and multivariate Cox-analysis. See methods for details.
Univariate analysis Multivariate analysis HR (95%CI) p HR (95%CI) p
Female sex 3.66 (1.11 - 12.05) 0.03 1.23
(0.32 - 4.74) 0.76
Age / 10-year increase 3.61 (1.94 - 6.72) <0.0001 3.26
(1.78 - 5.95) 0.0001
Septicemia or pneumonia 8.53 (2.27 - 32.06) 0.0008 13.46
(2.26 – 80.01) 0.003
Heart failure or cardiomyopathy 4.54 (0.88 - 23.15) 0.07 1.54
(0.22 - 10.61) 0.66
Figure Legends:
Figure 1. Frequency of acute pericarditis. Age-distribution of all pericarditis patients (A) and by
sex (from total number of patients) (B). Error bars represent upper limits of 95% confidence
intervals. *** p<0.0005
Figure 2. Cardiovascular admissions caused by acute pericarditis. Proportion of all
cardiovascular admissions (A) and by sex (B). Error bars represent upper limits of 95%
confidence intervals. *** p<0.0005, ** p<0.005, *p<0.05. Please note logarithmic y-axis.
Figure 3. Incidence rate of acute pericarditis in general population. Total (A) and sex-specific
(B) incidence rates (per 100,000 person-years) by age. Error bars represent upper limits of 95%
confidence intervals. *** p<0.0005, ** p<0.005.
Figure 4. Sex-associated incidence rate ratio of acute pericarditis by age in general population.
Ratio is calculated as men vs. women and adjusted for study year. Error bars represent 95%
confidence intervals.
Figure 1. Frequency of acute pericarditis. Age-distribution of all pericarditis pattiei tnts (A(A)) andd bby
ex x (f(frorom m tootatal nunuumbmbm er of patients) (B). Error baarsrs rrrepresent upper limmititits s s of 95% confidence
nnnteterrvrvals. ****** ppp<0<0<0.0.0000000555
FiFigugureree 222. CCaCardrdioioi vavascscullularar aadmmisisissisisionons caausususededed bbby y acac tututee pepee iriricaca drdrditisis.. PPrPropoporortitionon ooof ff alall l
cacardrdioiovavascsculullarar aadmdmd isiissisiononss (A(A(A)) aandndd bbby y sesexx (B(B).)). EEErrrroror bbbararss rereprpresesenentt upuppeperr lilimimitstts ooff f 959595%%
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

Figure 1
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

Figure 2
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

Figure 3
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

Figure 4
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from

Ville Kytö, Jussi Sipilä and Päivi RautavaClinical Profile and Influences on Outcomes in Patients Hospitalized for Acute Pericarditis
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2014 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online September 9, 2014;Circulation.
http://circ.ahajournals.org/content/early/2014/09/09/CIRCULATIONAHA.114.010376World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on April 2, 2018
http://circ.ahajournals.org/D
ownloaded from





























