Embed Size (px)
Citation preview

Clinical Practice Groups

CPG ProgrammeTheory of Improvement
Care delivery problem:
• Variation in clinical practice and process, leads to worse patient outcomes at
higher system costs
Goal of the intervention:• To reduce unwarranted variation in clinical practice and process
Intervention:• Implementation of evidence based standardised clinical practice and
processes as core operating standard across RFL group of hospitalsRef: BMJ Qual Saf doi:10.1136/bmjqs-2014-003627
2

Reducing unwarranted variation through CPGs
Clinical Practice Groups (CPGs)
Quality Improvement
(QI)
New Model Content EPR
Reduce unwarranted
clinical variation
using standardised
pathways
Develop a continuous
improvement culture Implement a Group wide
EPR to digitise CPGs
Optimise patient
care, safety and
outcomes

Clinical Practice Groups in practice
CPG
Programme
manager
CPG
Programme
manager
Group Exec
Hospital Unit 1
Exec
Hospital Unit 2
Exec
Hospital Unit 3
Exec
Division 1
Group Board
Division 2
Division 3
Division 1
Division 2
Division 3
Division 1
Division 2
Division 3
Sh
are
d S
erv
ices
Gro
up
Clin
ical
Serv
ices
Shared Services support all hospital units
CP
Gs s
up
po
rt
all H
Us
CPG
Programme
manager
CPG
Programme
manager
CPG
chair
CPG
chair
CPG
chair
CPG
chair
4
CPG Implementation Group
Quality Strategy Board Digital Board
Change Board
Clinical Standard and
Innovation Committee
https://intermountainhealthcare.org

Activity analysis
Quality and outcome metrics
Performance Cost analysis
Pathway Prioritisation Matrix
5

Pathway Prioritisation: Admitted Patient Care: ICD Code Review:
Top 30 by Cost
ICD Code Cost
Patient
Encounters
Average
Encounter
Cost Beds ITU Theatres Radiology Pathology Endoscopy
£
# of
encounters £ LoS Days LoS Days
Cutting
Minutes
# of scans or
investig # of tests
# of
encounters
A419-SEPTICAEMIA, UNSPECIFIED 7,189,470 2,360 3,046 13,274 1,309 5,717 2,873 62,477 70
J181-LOBAR PNEUMONIA, UNSPECIFIED 6,457,347 2,979 2,168 12,259 1,088 550 2,305 49,692 51
S720-FRACTURE OF NECK OF FEMUR 5,237,450 1,075 4,872 6,943 193 38,883 1,220 18,468 -
N390-URINARY TRACT INFECTION, SITE NOT SPECIFIED 4,806,933 2,738 1,756 9,532 51 1,048 1,359 32,786 12
O701-SECOND DEGREE PERINEAL LACERATION DURING DELIVERY 4,452,665 1,165 3,822 767 - 1,339 31 5,822 -
O342-MATERNAL CARE DUE TO UTERINE SCAR FROM PREVIOUS SURGERY 4,451,990 693 6,424 571 - 25,275 49 4,482 -
I500-CONGESTIVE HEART FAILURE 4,255,506 1,775 2,397 8,389 120 109 1,283 39,600 19
N185-CHRONIC KIDNEY DISEASE, STAGE 5 3,890,897 2,049 1,899 3,017 241 40,033 1,076 22,517 7
J690-PNEUMONITIS DUE TO FOOD AND VOMIT 3,526,427 1,339 2,634 7,792 318 738 1,131 24,303 38
C509-MALIGNANT NEOPLASM, BREAST, UNSPECIFIED 3,353,782 2,598 1,291 1,098 6 46,746 679 9,128 5
O688-LABOUR AND DELIVERY COMPLICATED BY OTHER EVIDENCE OF FETAL S 3,216,820 513 6,271 470 1 11,204 57 8,143 -
Z369-ANTENATAL SCREENING, UNSPECIFIED 3,028,364 12,062 251 - - 1,009 4,509 30,665 -
J189-PNEUMONIA, UNSPECIFIED 2,949,607 1,566 1,884 5,599 205 180 972 23,645 14
N179-ACUTE RENAL FAILURE, UNSPECIFIED 2,916,570 1,265 2,306 5,089 276 1,288 1,141 29,332 11
O628-OTHER ABNORMALITIES OF FORCES OF LABOUR 2,811,162 441 6,375 - - 15,676 46 8,272 -
H269-CATARACT, UNSPECIFIED 2,607,599 3,131 833 602 - 61,763 6 69 1
O680-LABOUR AND DELIVERY COMPLICATED BY FETAL HEART RATE ANOMALY 2,554,656 409 6,246 269 2 10,325 50 5,978 -
C64X-MALIGNANT NEOPLASM OF KIDNEY, EXCEPT RENAL PELVIS 2,531,053 724 3,496 1,252 59 44,590 364 6,601 7
O700-FIRST DEGREE PERINEAL LACERATION DURING DELIVERY 2,498,164 659 3,791 253 - 1,241 28 3,137 -
I639-CEREBRAL INFARCTION, UNSPECIFIED 2,493,860 480 5,196 5,289 100 307 629 9,411 12
M179-GONARTHROSIS, UNSPECIFIED 2,450,092 623 3,933 2,796 125 50,436 654 5,966 1
O800-SPONTANEOUS VERTEX DELIVERY 2,289,215 586 3,907 491 - - 5 1,416 -
L031-CELLULITIS OF OTHER PARTS OF LIMB 2,040,823 1,668 1,224 2,695 14 1,896 580 12,674 6
C787-SECONDARY MALIGNANT NEOPLASM OF LIVER 2,003,680 783 2,559 1,262 311 22,804 618 7,054 12
I214-ACUTE SUBENDOCARDIAL MYOCARDIAL INFARCTION 1,948,776 723 2,695 2,676 126 135 749 12,892 6
O420-PREMATURE RUPTURE OF MEMBRANES, ONSET OF LABOUR WITHIN 24 HO 1,920,897 538 3,570 111 - 744 9 3,430 -
R296-TENDENCY TO FALL, NOT ELSEWHERE CLASSIFIED 1,899,828 1,280 1,484 4,283 - 50 584 9,038 7
I702-ATHEROSCLEROSIS OF ARTERIES OF EXTREMITIES 1,851,607 237 7,813 2,189 58 12,973 407 6,534 -
J440-CHRONIC OBSTRUCTIVE PULMONARY DISEASE WITH ACUTE LOWER RESPI 1,840,843 1,126 1,635 3,212 297 159 468 10,879 7
O321-MATERNAL CARE FOR BREECH PRESENTATION 1,828,425 301 6,075 244 - 8,567 34 2,519 -
• Top 30 Admitted Patient Care ICDs are 10% of Trust total costs
• Most of these encounters and those under linked ICDs have been corralled into the first two sets of
pathways
Key Clinical ProcessesHigh total cost, and review
total encounters, and av.
cost

CPG Pathways
7

Methodology
8
Agree scope of
service
• Clinical pathways
• Clinical guidelines
• Patient experience
• Current Value
stream map
Quality metrics
• Clinical outcomes
• Patient
experience
• Activity
• Performance
• Cost Data
• Patient Safety
Data analysis
• Pareto analysis
• Gap analysis
• Value
assessment
• Clinical
grouping s and
outcomes
• Pathway
selection
Improve
• Agree future
state
• Model future
state
• Test pathways
• Develop IT
data collection
systems for
pathways
Sustain
• Chart analysis
of CPG impact
• Continuous
monitoring of
performance
• Continuous
Improvement
• Benefits
realisation
Step 1
Define
Step 2
Measure
Step 3
Analyse
Step 4
Design
(test PDSA)
Step 5
Continuously improve/ sustain

Patient Co-Design
Experience-Based Co-Design
Patient and Family Centred Care
(PFCC)
• Feedback questionnaires using Survey
Monkey
• Patient Shadowing
• Patient co-design panels
https://www.pointofcarefoundation.org.uk/

Example: Pre-Operative Assessment:
POA at the Barnet & Chase Hospital Sites - Current value stream map
CPG version 0.6
GP makes
referral to
surgical
specialty
Patient
attends
OPA with
decision to
treat
Admission
books TCI
and POA
Nurse-led
appointment
Book
anaesthetic
appointment
Obs, swabs
Happy
to
proceed
?
Y
Document on
Cerner
N
Obs, swabs, ?ECG,
medical and
physical history,
bloods, peak flow,
blood glucose
Bloods
normal?
Y
N
Renal impairment –
A&E
IV irons
Referral to anti-coag
Rebook for another
F2F appt
Happy
to
proceed
?
Y
N
Document on
Cerner
Further
investigation
s requested
More
information
required
from GP,
records etc.
Risk vs
benefits
discussion
Happy
to
proceed
?
N
Y
Document on
Cerner
Happy
to
proceed
?
N
Y
Document on
Cerner
Patient
happy
to
proceed
?
N
Y
Document on
Cerner
Document
on Cerner
Document on
Cerner
Nurse-led
50% POA clinics
have
anaesthetic
cover
Clinical Algorithm
For appointment face to
face or telephone
assessment

Example: Pre-Operative Assessment
Brown Paper and Gateway Documents
Bespoke Clinical Workflow Views
Message Centre Pools
Worklist Reports
Discern Alerts
Powerforms
Patient Portal - Clipboards

Dashboard – CPG pathway measures
12
POA – Orders eligible for same day POA and triage not completed
Chase Farm Hospital
Improvement period 1
(additional support for go-live)Improvement period 2
(change in staffing resource)

Pathways: Approach to Financial Benefits
Cohort
Moments of Care
Current and Future
Income, Resources, and
Costs
Current and Future
Metrics and profiling
Decision to proceed
Business Units embed in
financial plans
Implement, monitor
CPG SAS
Pathway Lower GI
# of pathways 100
Total Annual Cohort size 7100
Future State
For # of
pathways
For Total
Cohort
Moment of care & Setting Total Total
Resource
Additional Detail Units OP FA F2F OP STT
Colonscopy
(Endo)
Virtual
colonoscop
y
CT
Abdomen/
Pelvis
Results
review
Unit
Cost Cost Cost
Clinical Income
# of moments of care 25 100 52 20 16 100
# of pathways 100 100 100 100 100 100
Direct Clinical Delivery Service
Pay
Consultant Hours 11 28 21 10 100 6,930 492,030
Senior Fellow Hours 34 - -
Nurse Endoscopist Hours 14 34 471 33,474
Nurse Hours 27 - -
Therapist Hours 27 - -
A&C - Navigator Hours 8 5 15 180 12,788
Non-Pay
Drugs £ 100 3 300 21,300
Hotel £ 1 - -
Outsourced £ 1 - -
Clinical Non Pay £ 100 8 800 56,800
Clinical Support Services
Radiology Virtual colonoscopy Count 20 107 2,133 151,475
CT Abdomen/Pelvis Count 16 93 1,493 106,031
Pathology Biopsy Count 42 60 2,496 177,216
Other Pathology Days 100 8 800 56,800
Ward - Surgical Days 250 - -
POA Count 69 - -
Endoscopy Hours 35 300 10,400 738,400
Total Cost per 100 Pathways 1,163 4,768 15,447 2,133 1,493 1,000 26,004 1,846,314
Cost per moment of care 47 48 297 107 93 10
# of moments of care (Total 1,775 7,100 3,692 1,420 1,136 7,100
Annual Total Cost (Total Cohort) 82,538 338,500 1,096,770 151,475 106,031 71,000 1,846,314 -
Future StateCPG SAS
Pathway Elective Knee
# of pathways 100
Total Annual Cohort size 7100
Current State
For # of
pathways
For Total
Cohort
Moment of care & Setting Total Total
Resource
Additional Detail Units OP FA F2F OP STT
Colonscopy
(Endo)
Virtual
colonoscop
y
CT
Abdomen/
Pelvis
Results
review
Unit
Cost Cost Cost
Clinical Income
# of moments of care 100 100 52 20 16 100
# of pathways 100 100 100 100 100 100
Direct Clinical Delivery Service
Pay
Consultant Hours 42 28 10 100 7,973 566,107
Senior Fellow Hours 34 - -
Nurse Endoscopist Hours 7 34 236 16,737
Nurse Hours 27 - -
Therapist Hours 27 - -
A&C - Navigator Hours 30 15 450 31,950
Non-Pay
Drugs £ 100 3 300 21,300
Hotel £ 1 - -
Outsourced £ 1 - -
Clinical Non Pay £ 100 8 800 56,800
Clinical Support Services
Radiology Virtual colonoscopy Count 20 107 2,133 151,475
CT Abdomen/Pelvis Count 16 93 1,493 106,031
Pathology Biopsy Count 42 60 2,496 177,216
Pathology Other Days 100 8 800 56,800
Ward - Surgical Days 250 - -
POA Count 69 - -
Endoscopy Hours 35 300 10,400 738,400
Total Cost per 100 Pathways 6,550 - 15,905 2,133 1,493 1,000 27,082 1,922,816
Cost per moment of care 66 - 306 107 93 10
# of moments of care (Total 7,100 7,100 3,692 1,420 1,136 7,100
Annual Total Cost (Total Cohort) 465,050 - 1,129,260 151,475 106,031 71,000 1,922,816 -
Moments of care R
e
s
o
u
r
c
e
Current State
C
o
s
t
sCosts and
Income
Governance: Financial Benefits Realisation Group Chaired By CFO broke
this summary arrow into 12 steps and applied RAPID Decision Tool

• Pathways:• Complexity
• Multiple people/services
responsible for parts of the
pathway
• Costs:• Strong modelling assumptions
• Sticky costs: fixed versus variable
• GL Structure not fit pathways
• Patient encounters not easily
linked to pathways
• Complexity of costs
Key risks
• Internal:• IT analytics and systems not set
up for pathway analysis
• Multiple potential owners of
change
• Focus on short term hard cash
out not long term reorganisation
• Service Line profitability may be
differentially affected
• External:• Distribution of benefits across
the health economy
• Inability to control the whole
pathway

Board Goal: 20 Million cost reduction through CPGs
CPG Pathways embedded, monitored and digitised
15
Pathway A (‘Current state’)
◼ Patient seen in OP with a decision to list for surgery (variation in conversion)
◼ Average length of inpatient stay ~4 days
◼ Full hip precautions being applied to all THR patients
◼ Variation in follow-up procedures by consultant
Pathway B (‘Future state’)
◼ Standardised means of listing patients for surgery
◼ Anaesthetic protocol now spinal +/- sedation
◼ Structured phases of recovery during inpatient stay – built into digital pathway
◼ Hip precautions no longer in place following literature review
◼ Discharge summary completed at phase 2 to remove delays
◼ Virtual follow-up clinics being developed
Key measures to deliver benefit realisation
Length of stay PROMS outcomes (patient experience)
RTT performance NJR outcomes (Clinical effectiveness)
Key enablers to realise benefits
Adoption of digitised pathway, Clinical agreement re. no hip precautions, no stockings, spinal anaesthetic,
physio resource to support early mobilisation
Aim
Excellence in clinical outcomes whilst offering value to the tax payer with an average length of stay of 3
days or less
Income implications
◼ Reduction in OP attendances although expect to be populated with existing unmet demand
◼ Expect average IP spell income remains the same
CPG: Elective joint replacement, SaS CPG Chair: Lila Dinner
CPG Pathway Lead; Philip Ahrens
CPG Programme Manager: Helen Wark / Rachel Luker
Risks / Barriers
▪ Potential Risks:
Lack of adoption from all staff with newly designed pathway – some areas not yet agreed complete clinical
consensus
▪ Potential Barriers:
Long waiting times for many orthopaedic procedures, physio resource to support regular mobilisation
Critical Milestones Time line
Current state pathway mapped Sept 17 - Nov ’17
Literature reviews, shared learning with other providers Jan ‘18 – Jul ‘18
Agree key measures and understand current performance May ‘18 – Jul ‘18
Digitisation design sessions Feb ‘18 - May ’18
Joint schools harmonised Mar ’18 - Jul ’18
Agreement re. hip precautions and f/up protocol Sept ’18
Patient co-design event Oct ‘18
Digitisation training and launch Oct ‘18 – Nov ‘18
Benefits
◼ Activity/volumes
Moving activity to cold elective site – CFH,
increased efficiency for IP and OP
◼ Patient and Clinical Outcomes
Reduced LoS, improved patient experience
◼ Performance
Improved RTT, PROMS and NJR performance
◼ Cost
Reduced LoS with less resource input

Step 1
Decide the patient cohort
In determining the scope of the elective joint pathway, the
cohort of patients was defined by the pathway team:
• Patients over the age of 50
• Who are suitable for Chase Farm Hospital, and
• Having total hip replacements or a total knee
replacement
Chase Farm theatres elective hip patient population
Barbara’s story
Barbara is 81 years old, lives in East
Barnet and is typical of the patient
cohort for this pathway. She visited her
local GP in late 2018 and was referred
to an outpatient clinic at Barnet
Hospital to discuss a right total hip
replacement

Step 2Decide the moments of
care that make up Pathway A and B
Each pathway that the team has mapped (current state /
pathway A and future state / pathway B) can be broken
down into moments of care, that require some resource
Pathway A
Pathway B
Barbara’s story
Barbara’s first ‘moment of care’ in
the pathway was when she
attended Barnet Hospital to see
a consultant on 14 January 2019,
where she and her consultant
decided she would have a right
total hip replacement

Moments of care summary
-
1,000
2,000
3,000
4,000
Pathway A Pathway B
RFH 1,193 1,060
CFH 2,426 2,156
Nu
mb
er
of
OP
ap
po
intm
en
ts
Decrease in OP appointments
3,618
804 804 804
3,216
804 804 804
OP IP DI Therapy
Moments of care
Changes in moments of care
Pathway A Pathway B
Reducing the number of pre and post follow up appointments will reduce the moments of
care needed in the pathway. The reduction in outpatient appointments is due to
• No pre-operative OP follow up appointments following imaging
• Post-operative OP follow up appointments reducing from median of 1.5 to 1.0
The number of moments care along the rest of the pathway remain the same.
Imaging

Step 3
Decide the clinical and non-
clinical resources needed to
deliver the moments of care
in Pathways A and B
For example, in pathways A and B, all patients are
invited to attend Joint School before their
operation. This ‘moment of care’ needs the resource
of the staff members who run the session:
Barbara went to Joint School
at Chase Farm Hospital on 2
April 2019 and said:
“It was useful and informative. I have had my knee
done before and when I woke up shivering I felt
worried because I thought there was something
wrong with me, but [at joint school] they explained
that this is how your body warms up after surgery,
so I wasn’t worried this time”
Barbara’s story
Resource required Time required
per week
Cost (in A and B) per
annum
Anaesthetist 15 minutes £3.4k
Nurse 90 minutes £5.0k
Therapist 90 minutes £5.0k
TOTAL £13.4k

Step 4Decide the income and cost for
Pathway A (based on current
encounter data set)
Pathways A and B can then be looked at in terms of
cost and income. For example, in Pathway B there
are fewer outpatient appointments before surgery,
therefore both cost and income will be impacted:Step 5
Decide the cost of resources for
Pathway B and estimate income
Barbara only had to attend one
outpatient appointment before
her operation, and had had an
x-ray on the same day. She also
walked round to pre-operative
assessment at Barnet Hospital,
was triaged same day and then
returned on 5 March 2019 for a
face to face assessment
Average no. of pre-operative outpatient appointments per
patient (hips and knees) Apr 2016 – Mar 2019
Barbara’s story
Pathway
A
Pathway
B Variance
Total number of pre-op follow up
appointments 402 - - 402
Percentage of total OP
appointments 11% 0% -11%
Total income 28,927 - - 28,927
Total cost 10,050 - - 10,050

Step 6
Decide the contribution of Pathway A and
estimate the contribution of Pathway B
Once total income and cost per pathway are
understood, contribution (the difference
between the two as a percentage of income)
can be calculated.
Pathway A contribution = 45%
Estimated Pathway B contribution = 51%
Change in contribution is due to lower length
of stay. Time, resources and experience in
theatre will remain unchanged, so contribution
of moment of care in theatre is unchanged.
• Barbara had her operation (right total hip
replacement) at Chase Farm Hospital
on 16 April 2019
• Barbara arrived on the ward at 6.30pm
that evening and the first nursing
checklist within the elective hip care
pathway an hour later
• Barbara was first mobilised by a
physiotherapist at 9.30am the following
morning, and the first physio checklist
was also completed
Barbara’s story

Step 7
Decide the financial and non-financial
measures describing the benefits and
include in measurement plans
The primary outcome measure in the elective
hip and knee pathway is length of stay, this
describes a key outcome and is captured in the
measurement plan for the pathway.
Step 8
Decide the expected change in financial profile from
Pathway A to Pathway B from expected changes in
measures
Change in average length of stayLength of stay (elective hip)
Apr 2016 – Mar 2019Hip Knee
Before go-live (Apr-
Oct 2018)4.5 days 4.0 days
Since go-live (Nov 2018-Mar 2019)
3.7 days 3.6 days
Change so far 0.8 days 0.4 days

Dashboard – CPG pathway measures
23
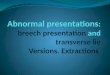
Elective hip - Variation in length of stay by consultant (anon.) at Chase Farm Hospital

• After spending three nights at Chase Farm Hospital,
Barbara’s final nursing and physiotherapy checklists
were completed and she was confirmed ready for
discharge on 19 April 2019
• Barbara’s length of stay was 3.14 days
• Barbara’s GP discharge letter confirmed a follow up
outpatient appointment 6 weeks post-discharge, as her
final moment of care on the pathway
Barbara’s story
2,600 2,700 2,800 2,900 3,000 3,100 3,200 3,300
4.6 4.5 4.4 4.3 4.2 4.1 4.0 3.9 3.8 3.7 3.6 3.5 3.4 3.3 3.2 3.1 3.0
LOS (Days)
Cost and length of stay (LOS)
Cost (£k)
LOS
(Days) Cost (£k)
Pathway A 4.6 3,192
Pathway B 3.0 2,835 - 358
Reducing length of stay (LOS)
will result in a reduction in cost.
This will release both consultant
time and beds in the surgical ward
Cost reduces with
length of stay

Summary of financial benefits realisationDeciding Factor for
Change
Effect of
Change CPG Benefits
CPG
Benefits
£k
Reduced Length of
Stay
Reducing LOS
from 4.6 to 3.0
days
Ward LOS -
Reduction
358-
No follow up
appointment after
imaging
Removal of
staff costs as
patient has one
less OP
appointment
F2F Follow ups -
Reduction in Vol
10-
Reduced Follow up
appointments
Reduction in
the number of
follow up
appointments
after being
discharged
F2F Follow ups -
Reduction in Vol
9-
Income Associated
income with
cost saving
measures
Income Redt'n -
Standardisation
Methodology
across sites
58
319-
This table shows the key drivers of
change and the financial impact of
the change.
• The biggest financial gain can be
achieved by reducing length of
stay from 4.6 to 3.0 days for
elective hip and knee patients.
• Further cost reduction comes
from reducing outpatient
appointments
Pathway: Elective Hip & KneePathway A
£KPathway B
£KDiff£k
Diff (%)
Income 6,172 6,114 (58) (1%)Expenditure 3,377 3,000 (377) (11%)Contribution 2,795 3,114 319 11%Contribution % 45% 51%
This summary of income and
expenditure in pathway A and
pathway B demonstrates an
opportunity to remove £377k cost
from the pathway which can free
up capacity
Income Expenditure Contribution
Pathway A 7,677 4,200 3,476
Pathway B 7,605 3,732 3,873
(72) (469) 397
Average per patient (£)Similarly looking at the average
cost per patient, we can see
opportunity to remove further cost
from both the hip and knee pathways

Step 9
Whether to
proceed with
the financial
case
(“Gateway
review”)
Step 10
Decide the ownership
of the realisation of
expected benefits
within the business
units and pathway
development team
Step 11
Decide the infrastructure
that is appropriate to
deliver, monitor and report
on the financial effects
within the business units
and pathway development
team
Step 12
Decide on
reconciliation
between the
business unit
and pathway
development
team benefits
realisation
• After Barbara had gone home, the ward team at
Chase Farm did their weekly dashboard
review to see all of the patients who had a
length of stay longer than 3 days
• The team then reviewed these patients’ records,
including Barbara’s, to understand and record
the drivers behind a longer length of stay,
and to take action accordingly
Barbara’s story