Embed Size (px)
Citation preview
0
Clinical Policy Title: Acupuncture
Clinical Policy Number: 03.02.03
Effective Date: April 1, 2015
Initial Review Date: January 21, 2015
Most Recent Review Date: March 15, 2017
Next Review Date: March 2018
Related policies:
None.
ABOUT THIS POLICY: AmeriHealth Caritas Pennsylvania has developed clinical policies to assist with making coverage determinations. AmeriHealth Caritas Pennsylvania’s clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by AmeriHealth Caritas Pennsylvania when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. AmeriHealth Caritas Pennsylvania’s clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. AmeriHealth Caritas Pennsylvania’s clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, AmeriHealth Caritas Pennsylvania will update its clinical policies as necessary. AmeriHealth Caritas Pennsylvania’s clinical policies are not guarantees of payment.
Coverage policy
AmeriHealth Caritas Pennsylvania considers the use of acupuncture to be clinically proven and,
therefore, medically necessary when all of the following criteria are met:
Patient is age 18 years or older.
Patient needs treatment for one of the following medical conditions:
- Postoperative-related nausea and vomiting.
- Chemotherapy-induced nausea and vomiting (CINV).
- Chronic non-specific low back pain (CNSLBP) (i.e., more than three months).
- Chronic migraine.
- Chronic pain caused by osteoarthritis (OA) of the knee.
As adjunctive treatment when either:
- Other standard treatment options inadequately control symptoms.
- Patient refuses treatment or experiences adverse effects from such treatment.
When performed by a qualified practitioner who is both:
- Appropriately trained and licensed in acupuncture.
Policy contains:
Chronic non-specific low back
pain (CNSLBP).
Chronic migraine.
Knee osteoarthritis (OA).
Nausea and vomiting.
1
- Credentialed by AmeriHealth Caritas Pennsylvania.
Limitations:
All other uses of acupuncture are not medically necessary. Please note:
Maintenance treatment, where the member’s symptoms are neither regressing nor
improving, is not medically necessary.
Treatments beyond five visits without meaningful improvement in symptoms require review
by a Medical Director.
For Medicare members only:
AmeriHealth Caritas Pennsylvania considers the use of acupuncture to be investigational and, therefore,
not medically necessary.
Alternative covered services:
Standard medical management of chronic pain syndromes or nausea and vomiting due to
chemotherapy or anesthesia.
Background
According to the National Center for Complementary and Integrative Health (NCCIH), acupuncture is one
of the practices of traditional Chinese medicine (TCM) (NCCIH, 2014). According to TCM, energy known
as “qi” flows throughout the body along patterns known as meridians. Disturbances in the flow of “qi”
are thought to result in disease. Acupuncture is based on the belief that stimulating specific points on
the body corrects imbalances in the flow of “qi.” The technology has four components:
Acupuncture needle(s).
Target location defined by TCM.
Depth of needle insertion.
Stimulation of the inserted needle.
Traditional acupuncture uses thin needles, but it may also apply manual pressure, electrical stimulation,
magnets, low-power lasers, heat, and ultrasound. The U.S. Food and Drug Administration (FDA)
regulates acupuncture needles as Class II medical devices with special controls. Acupuncture needles
must be labeled for single use only, biocompatible and sterile, and be administered by qualified
practitioners only (21CFR880.5580).
The professional credentials of an acupuncture practitioner can range from none to licensed medical
doctor. Licensure laws and scope-of-practice guidelines regulating acupuncture practitioners vary by
state. Currently, 43 states and the District of Columbia require the passage of the National Certification
2
Commission for Acupuncture and Oriental Medicine (NCCAOM) examinations, or NCCAOM certification
as a prerequisite for licensure (NCCAOM, 2015). Board certification in medical acupuncture is granted by
the American Board of Medical Acupuncture (ABMA) (ABMA, 2015). Certification entails (ABMA, 2015):
Meeting minimum general requirements.
Meeting education and training requirements.
Meeting experience requirements.
Successfully passing the ABMA examination.
Searches
AmeriHealth Caritas Pennsylvania searched PubMed and the databases of:
UK National Health Services Centre for Reviews and Dissemination.
Agency for Healthcare Research and Quality’s National Guideline Clearinghouse and other
evidence-based practice centers.
The Centers for Medicare & Medicaid Services (CMS).
We conducted searches on January 12, 2017. Search terms were: "acupuncture" (MeSH) and
"acupuncture therapy" (MeSH), as well as free text “acupuncture” for articles published in English.
We included:
Systematic reviews, which pool results from multiple studies to achieve larger sample sizes
and greater precision of effect estimation than in smaller primary studies. Systematic
reviews use predetermined transparent methods to minimize bias, effectively treating the
review as a scientific endeavor, and are thus rated highest in evidence-grading hierarchies.
Guidelines based on systematic reviews.
Economic analyses, such as cost-effectiveness, and benefit or utility studies (but not simple
cost studies), reporting both costs and outcomes — sometimes referred to as efficiency
studies — which also rank near the top of evidence hierarchies.
Findings
Given the substantial volume of literature on this topic, AmeriHealth Caritas Pennsylvania considered
only the most comprehensive systematic reviews of acupuncture published in the last five years. More
than 100 systematic reviews and meta-analyses were identified, the majority of which found evidence
for various clinical uses of acupuncture to be of low quality. Conflicting results were also evident.
An evidence map of acupuncture (not a formal systematic review) produced for the Veterans Health
Administration (VHA), which identified 183 systematic reviews published since 2005, found
inconsistency in the quality and findings of systematic reviews (Hempel, 2014). Inconsistency in results
appeared to be related to the selection of the comparator to which the treatment effects of
acupuncture were compared. Controls included no treatment, waiting list assignment, acupuncture as
3
add-on treatment to a treatment plan received by both treatment groups, placebo control (such as
sham acupuncture), and active controls, such as exercise and usual care. Typically, trials included a
placebo arm and a no-treatment arm to explore variations in the impact of the different types of
placebo. There is currently no universal standard for what constitutes an appropriate method or
procedure for a sham acupuncture control, and this may contribute to the discrepancy between
observed clinical effectiveness of acupuncture and the lack of rigorous research supporting these
observations for many indications (Hempel, 2014).
Therefore, this policy will focus on those indications for which there is high-quality and consistent
evidence demonstrating improvement in health outcomes with acupuncture; nine systematic reviews
are listed in the summary table. Eight evidence-based guidelines and two economic analyses pertaining
to the topics of these syntheses were identified.
There is sufficient evidence to support the use of acupuncture as adjunctive treatment for certain types
of chronic pain and nausea and vomiting. Included were individual syntheses for the following
indications:
Postoperative- and CINV.
CNSLBP.
Chronic migraine.
OA of the knee.
The benefits of acupuncture are limited mostly to immediate and short-term post-treatment periods in
patients ages 18 or older using sham or no-acupuncture controls. Evidence of its effectiveness over
other conventional treatment modalities is conflicting or of low quality. Evidence-based guidelines listed
in the references recommend acupuncture as an adjunct to standard treatment for the specific
indications in the summary table, when other treatment options inadequately control symptoms, or
when patients refuse treatment or experience adverse effects from such treatment. One guideline did
not recommend acupuncture for the management of OA of the knee (Jevsevar, 2013).
While acupuncture is generally a safe procedure, reporting of harms was poor across studies, so a
comparison of the rate of adverse events between acupuncture and other treatments cannot be made.
Where reported, adverse events were generally localized, minor, transient, and infrequent when
performed by an appropriately trained practitioner using clean technique and single-use needles. When
not delivered properly, acupuncture can cause serious adverse effects, including infections, punctured
organs, collapsed lungs, injury to the central nervous system, and even death (Ernst, 2011; NCCAM,
2015).
There is insufficient evidence to draw conclusions regarding the optimal frequency of
administration, duration of each session, number, depth of needle penetration, or needle
location.
4
There is insufficient evidence to support the cost-effectiveness of acupuncture for any
indication. The few cost-effectiveness analyses that have been conducted in the United
States found either a lack of effectiveness or sufficient rigor needed to further inform
practice (Kim, 2012; Pinto, 2012).
Policy updates:
We identified 26 new systematic reviews and meta-analyses and one new clinical practice guideline
published in the last year for this policy. Seven systematic reviews and meta-analyses reported
significant short-term or intermediate-term positive effects of acupuncture treatment for several
conditions, but significant study design flaws and small numbers of studies limited the validity of the
evidence included in these analyses (Feng, 2015; Zhou, 2015; Yuan, 2015; Law, 2015; Gutke, 2015; Dong,
2015; Chan, 2015). One clinical practice guideline stated acupuncture could be a non-pharmacologic
option for allergic rhinitis based on moderate evidence from two large randomized controlled trials
(RCTs) reporting improvement in symptoms and quality of life with acupuncture, but stopped short of
issuing a firm recommendation for its use (Seidman, 2015). The new information would not alter the
conclusions of the original policy. Therefore, no changes to the policy are warranted.
In 2017, we identified 15 new systematic reviews and meta-analyses and one new evidence-based
guideline for this policy. New evidence confirms previous policy findings of acupuncture’s safety and
efficacy in TTH (Linde, 2016a), migraine (Linde, 2016b), and palliation of CINV (Lau, 2016), as well as
insufficient demonstration of safety and efficacy in chronic pain syndromes (Qin, 2016), and post-
operative pain (Wu, 2016).
The results of several systematic reviews and meta-analyses suggested acupuncture had a limited
treatment effect on a number of new clinical indications, but the evidence of safety and efficacy was
inconclusive due to poor methodological quality, insufficient quantity, or conflicting findings (Cui, 2016;
del Pino-Sedeno, 2016; He, 2016; Kim, 2016; Lim, 2016; Mangese, 2016; Smith, 2016; Su, 2016; Van den
Heuvel, 2016; Yang, 2016). A guideline by the American College of Physicians on treatments (including
acupuncture) for major depressive disorder in adults issued strong evidence-based recommendations
for cognitive behavioral therapy and antidepressants, but made no specific recommendation for
acupuncture (Qaseem, 2016). The new information does not change the original findings. Therefore, no
policy changes are warranted.
Summary of clinical evidence:
Citation Content, Methods, Recommendations
Nausea and vomiting
Cheong (2013) Prevention and treatment of postoperative nausea and
Key points:
Systematic review and meta-analysis of 30 RCTs (n=1,276 patients [acupuncture], n=1,258 patients [no acupuncture or sham]).
Overall quality: three of low quality, nine of moderate quality, and four of high quality for Nei Guan acupuncture point (PC6)-only studies; six of low quality for PC6 + other acupoints; one of
5
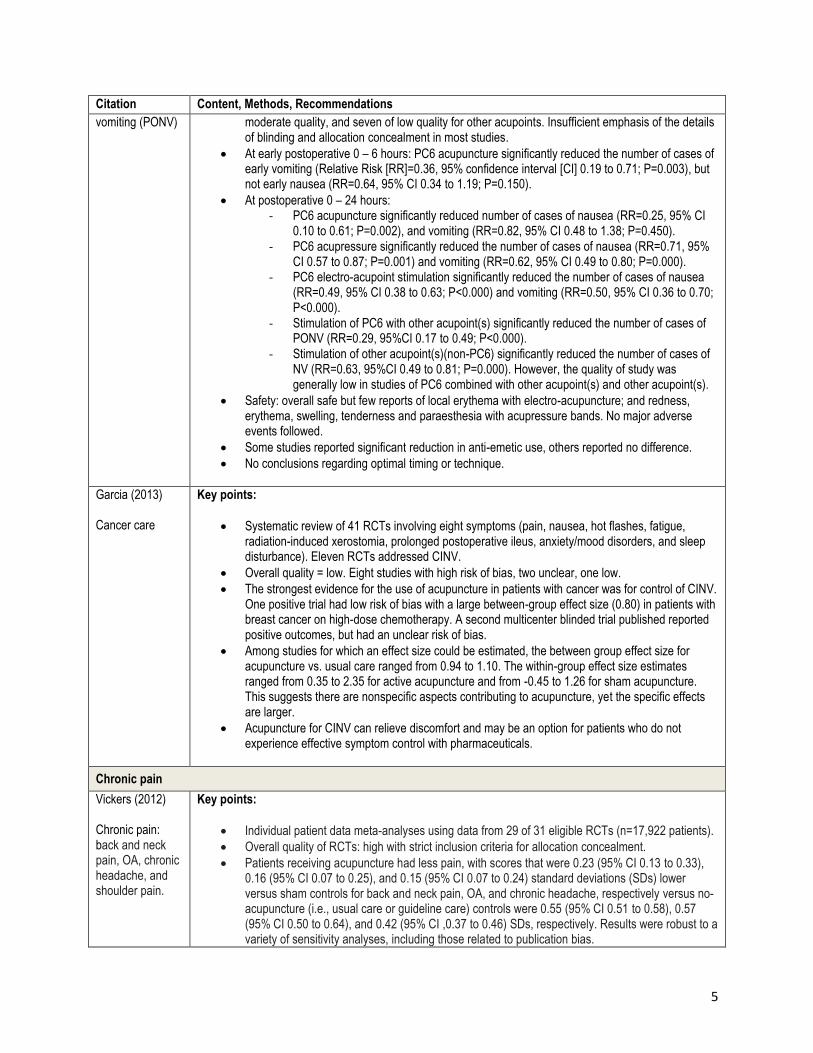
Citation Content, Methods, Recommendations
vomiting (PONV)
moderate quality, and seven of low quality for other acupoints. Insufficient emphasis of the details of blinding and allocation concealment in most studies.
At early postoperative 0 – 6 hours: PC6 acupuncture significantly reduced the number of cases of early vomiting (Relative Risk [RR]=0.36, 95% confidence interval [CI] 0.19 to 0.71; P=0.003), but not early nausea (RR=0.64, 95% CI 0.34 to 1.19; P=0.150).
At postoperative 0 – 24 hours: - PC6 acupuncture significantly reduced number of cases of nausea (RR=0.25, 95% CI
0.10 to 0.61; P=0.002), and vomiting (RR=0.82, 95% CI 0.48 to 1.38; P=0.450). - PC6 acupressure significantly reduced the number of cases of nausea (RR=0.71, 95%
CI 0.57 to 0.87; P=0.001) and vomiting (RR=0.62, 95% CI 0.49 to 0.80; P=0.000). - PC6 electro-acupoint stimulation significantly reduced the number of cases of nausea
(RR=0.49, 95% CI 0.38 to 0.63; P<0.000) and vomiting (RR=0.50, 95% CI 0.36 to 0.70; P<0.000).
- Stimulation of PC6 with other acupoint(s) significantly reduced the number of cases of PONV (RR=0.29, 95%CI 0.17 to 0.49; P<0.000).
- Stimulation of other acupoint(s)(non-PC6) significantly reduced the number of cases of NV (RR=0.63, 95%CI 0.49 to 0.81; P=0.000). However, the quality of study was generally low in studies of PC6 combined with other acupoint(s) and other acupoint(s).
Safety: overall safe but few reports of local erythema with electro-acupuncture; and redness, erythema, swelling, tenderness and paraesthesia with acupressure bands. No major adverse events followed.
Some studies reported significant reduction in anti-emetic use, others reported no difference.
No conclusions regarding optimal timing or technique.
Garcia (2013) Cancer care
Key points:
Systematic review of 41 RCTs involving eight symptoms (pain, nausea, hot flashes, fatigue, radiation-induced xerostomia, prolonged postoperative ileus, anxiety/mood disorders, and sleep disturbance). Eleven RCTs addressed CINV.
Overall quality = low. Eight studies with high risk of bias, two unclear, one low.
The strongest evidence for the use of acupuncture in patients with cancer was for control of CINV. One positive trial had low risk of bias with a large between-group effect size (0.80) in patients with breast cancer on high-dose chemotherapy. A second multicenter blinded trial published reported positive outcomes, but had an unclear risk of bias.
Among studies for which an effect size could be estimated, the between group effect size for acupuncture vs. usual care ranged from 0.94 to 1.10. The within-group effect size estimates ranged from 0.35 to 2.35 for active acupuncture and from -0.45 to 1.26 for sham acupuncture. This suggests there are nonspecific aspects contributing to acupuncture, yet the specific effects are larger.
Acupuncture for CINV can relieve discomfort and may be an option for patients who do not experience effective symptom control with pharmaceuticals.
Chronic pain
Vickers (2012) Chronic pain: back and neck pain, OA, chronic headache, and shoulder pain.
Key points:
Individual patient data meta-analyses using data from 29 of 31 eligible RCTs (n=17,922 patients).
Overall quality of RCTs: high with strict inclusion criteria for allocation concealment.
Patients receiving acupuncture had less pain, with scores that were 0.23 (95% CI 0.13 to 0.33), 0.16 (95% CI 0.07 to 0.25), and 0.15 (95% CI 0.07 to 0.24) standard deviations (SDs) lower versus sham controls for back and neck pain, OA, and chronic headache, respectively versus no-acupuncture (i.e., usual care or guideline care) controls were 0.55 (95% CI 0.51 to 0.58), 0.57 (95% CI 0.50 to 0.64), and 0.42 (95% CI ,0.37 to 0.46) SDs, respectively. Results were robust to a variety of sensitivity analyses, including those related to publication bias.
6
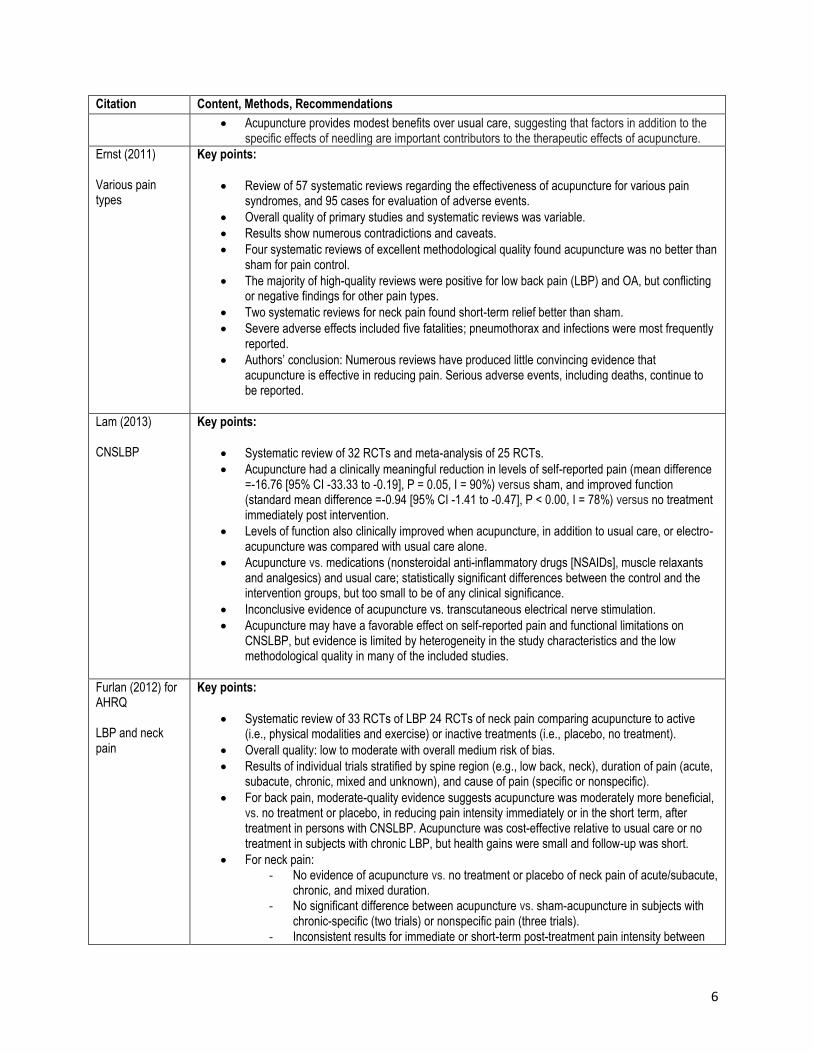
Citation Content, Methods, Recommendations
Acupuncture provides modest benefits over usual care, suggesting that factors in addition to the specific effects of needling are important contributors to the therapeutic effects of acupuncture.
Ernst (2011) Various pain types
Key points:
Review of 57 systematic reviews regarding the effectiveness of acupuncture for various pain syndromes, and 95 cases for evaluation of adverse events.
Overall quality of primary studies and systematic reviews was variable.
Results show numerous contradictions and caveats.
Four systematic reviews of excellent methodological quality found acupuncture was no better than sham for pain control.
The majority of high-quality reviews were positive for low back pain (LBP) and OA, but conflicting or negative findings for other pain types.
Two systematic reviews for neck pain found short-term relief better than sham.
Severe adverse effects included five fatalities; pneumothorax and infections were most frequently reported.
Authors’ conclusion: Numerous reviews have produced little convincing evidence that acupuncture is effective in reducing pain. Serious adverse events, including deaths, continue to be reported.
Lam (2013) CNSLBP
Key points:
Systematic review of 32 RCTs and meta-analysis of 25 RCTs.
Acupuncture had a clinically meaningful reduction in levels of self-reported pain (mean difference =-16.76 [95% CI -33.33 to -0.19], P = 0.05, I = 90%) versus sham, and improved function (standard mean difference =-0.94 [95% CI -1.41 to -0.47], P < 0.00, I = 78%) versus no treatment immediately post intervention.
Levels of function also clinically improved when acupuncture, in addition to usual care, or electro-acupuncture was compared with usual care alone.
Acupuncture vs. medications (nonsteroidal anti-inflammatory drugs [NSAIDs], muscle relaxants and analgesics) and usual care; statistically significant differences between the control and the intervention groups, but too small to be of any clinical significance.
Inconclusive evidence of acupuncture vs. transcutaneous electrical nerve stimulation.
Acupuncture may have a favorable effect on self-reported pain and functional limitations on CNSLBP, but evidence is limited by heterogeneity in the study characteristics and the low methodological quality in many of the included studies.
Furlan (2012) for AHRQ LBP and neck pain
Key points:
Systematic review of 33 RCTs of LBP 24 RCTs of neck pain comparing acupuncture to active (i.e., physical modalities and exercise) or inactive treatments (i.e., placebo, no treatment).
Overall quality: low to moderate with overall medium risk of bias.
Results of individual trials stratified by spine region (e.g., low back, neck), duration of pain (acute, subacute, chronic, mixed and unknown), and cause of pain (specific or nonspecific).
For back pain, moderate-quality evidence suggests acupuncture was moderately more beneficial, vs. no treatment or placebo, in reducing pain intensity immediately or in the short term, after treatment in persons with CNSLBP. Acupuncture was cost-effective relative to usual care or no treatment in subjects with chronic LBP, but health gains were small and follow-up was short.
For neck pain: - No evidence of acupuncture vs. no treatment or placebo of neck pain of acute/subacute,
chronic, and mixed duration. - No significant difference between acupuncture vs. sham-acupuncture in subjects with
chronic-specific (two trials) or nonspecific pain (three trials). - Inconsistent results for immediate or short-term post-treatment pain intensity between
7
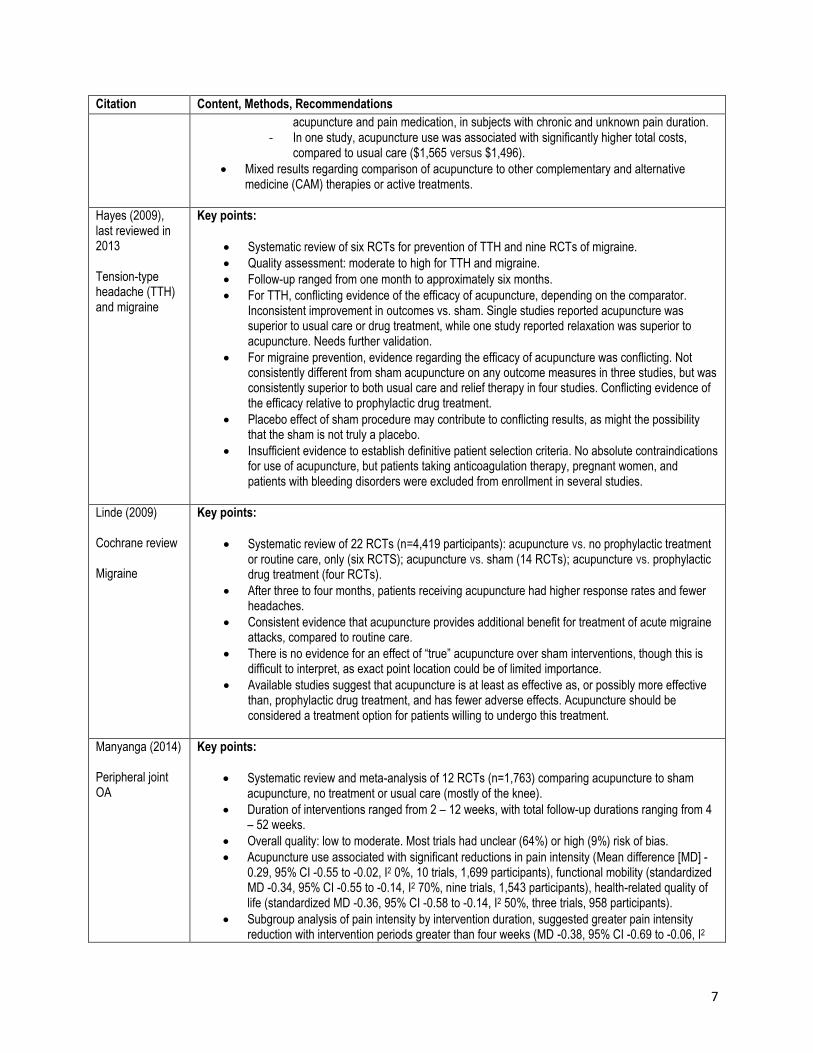
Citation Content, Methods, Recommendations
acupuncture and pain medication, in subjects with chronic and unknown pain duration. - In one study, acupuncture use was associated with significantly higher total costs,
compared to usual care ($1,565 versus $1,496).
Mixed results regarding comparison of acupuncture to other complementary and alternative medicine (CAM) therapies or active treatments.
Hayes (2009), last reviewed in 2013 Tension-type headache (TTH) and migraine
Key points:
Systematic review of six RCTs for prevention of TTH and nine RCTs of migraine.
Quality assessment: moderate to high for TTH and migraine.
Follow-up ranged from one month to approximately six months.
For TTH, conflicting evidence of the efficacy of acupuncture, depending on the comparator. Inconsistent improvement in outcomes vs. sham. Single studies reported acupuncture was superior to usual care or drug treatment, while one study reported relaxation was superior to acupuncture. Needs further validation.
For migraine prevention, evidence regarding the efficacy of acupuncture was conflicting. Not consistently different from sham acupuncture on any outcome measures in three studies, but was consistently superior to both usual care and relief therapy in four studies. Conflicting evidence of the efficacy relative to prophylactic drug treatment.
Placebo effect of sham procedure may contribute to conflicting results, as might the possibility that the sham is not truly a placebo.
Insufficient evidence to establish definitive patient selection criteria. No absolute contraindications for use of acupuncture, but patients taking anticoagulation therapy, pregnant women, and patients with bleeding disorders were excluded from enrollment in several studies.
Linde (2009) Cochrane review Migraine
Key points:
Systematic review of 22 RCTs (n=4,419 participants): acupuncture vs. no prophylactic treatment or routine care, only (six RCTS); acupuncture vs. sham (14 RCTs); acupuncture vs. prophylactic drug treatment (four RCTs).
After three to four months, patients receiving acupuncture had higher response rates and fewer headaches.
Consistent evidence that acupuncture provides additional benefit for treatment of acute migraine attacks, compared to routine care.
There is no evidence for an effect of “true” acupuncture over sham interventions, though this is difficult to interpret, as exact point location could be of limited importance.
Available studies suggest that acupuncture is at least as effective as, or possibly more effective than, prophylactic drug treatment, and has fewer adverse effects. Acupuncture should be considered a treatment option for patients willing to undergo this treatment.
Manyanga (2014) Peripheral joint OA
Key points:
Systematic review and meta-analysis of 12 RCTs (n=1,763) comparing acupuncture to sham acupuncture, no treatment or usual care (mostly of the knee).
Duration of interventions ranged from 2 – 12 weeks, with total follow-up durations ranging from 4 – 52 weeks.
Overall quality: low to moderate. Most trials had unclear (64%) or high (9%) risk of bias.
Acupuncture use associated with significant reductions in pain intensity (Mean difference [MD] -0.29, 95% CI -0.55 to -0.02, I2 0%, 10 trials, 1,699 participants), functional mobility (standardized MD -0.34, 95% CI -0.55 to -0.14, I2 70%, nine trials, 1,543 participants), health-related quality of life (standardized MD -0.36, 95% CI -0.58 to -0.14, I2 50%, three trials, 958 participants).
Subgroup analysis of pain intensity by intervention duration, suggested greater pain intensity reduction with intervention periods greater than four weeks (MD -0.38, 95% CI -0.69 to -0.06, I2
8
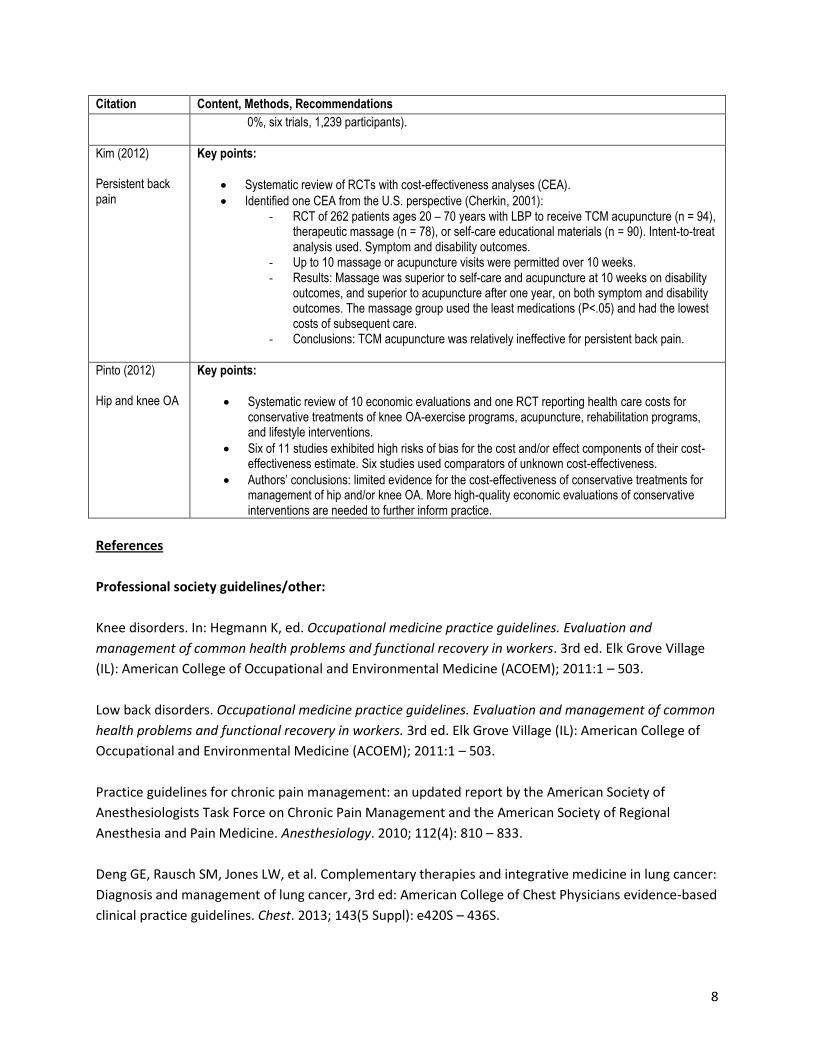
Citation Content, Methods, Recommendations
0%, six trials, 1,239 participants).
Kim (2012) Persistent back pain
Key points:
Systematic review of RCTs with cost-effectiveness analyses (CEA).
Identified one CEA from the U.S. perspective (Cherkin, 2001): - RCT of 262 patients ages 20 – 70 years with LBP to receive TCM acupuncture (n = 94),
therapeutic massage (n = 78), or self-care educational materials (n = 90). Intent-to-treat analysis used. Symptom and disability outcomes.
- Up to 10 massage or acupuncture visits were permitted over 10 weeks. - Results: Massage was superior to self-care and acupuncture at 10 weeks on disability
outcomes, and superior to acupuncture after one year, on both symptom and disability outcomes. The massage group used the least medications (P<.05) and had the lowest costs of subsequent care.
- Conclusions: TCM acupuncture was relatively ineffective for persistent back pain.
Pinto (2012) Hip and knee OA
Key points:
Systematic review of 10 economic evaluations and one RCT reporting health care costs for conservative treatments of knee OA-exercise programs, acupuncture, rehabilitation programs, and lifestyle interventions.
Six of 11 studies exhibited high risks of bias for the cost and/or effect components of their cost-effectiveness estimate. Six studies used comparators of unknown cost-effectiveness.
Authors’ conclusions: limited evidence for the cost-effectiveness of conservative treatments for management of hip and/or knee OA. More high-quality economic evaluations of conservative interventions are needed to further inform practice.
References
Professional society guidelines/other:
Knee disorders. In: Hegmann K, ed. Occupational medicine practice guidelines. Evaluation and
management of common health problems and functional recovery in workers. 3rd ed. Elk Grove Village
(IL): American College of Occupational and Environmental Medicine (ACOEM); 2011:1 – 503.
Low back disorders. Occupational medicine practice guidelines. Evaluation and management of common
health problems and functional recovery in workers. 3rd ed. Elk Grove Village (IL): American College of
Occupational and Environmental Medicine (ACOEM); 2011:1 – 503.
Practice guidelines for chronic pain management: an updated report by the American Society of
Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional
Anesthesia and Pain Medicine. Anesthesiology. 2010; 112(4): 810 – 833.
Deng GE, Rausch SM, Jones LW, et al. Complementary therapies and integrative medicine in lung cancer:
Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based
clinical practice guidelines. Chest. 2013; 143(5 Suppl): e420S – 436S.
9
Gan TJ, Diemunsch P, Habib AS, et al. Consensus guidelines for the management of postoperative
nausea and vomiting. Anesth Analg. 2014; 118(1): 85 – 113.
Headaches. Diagnosis and management of headaches in young people and adults. NICE clinical guideline
150. NICE website. http://www.nice.org.uk/guidance/cg150. Accessed January 10, 2017.
Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for
the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee.
Arthritis Care Res (Hoboken). 2012; 64(4): 465 – 474.
Jevsevar DS, Brown GA, Jones DL, et al. The American Academy of Orthopaedic Surgeons evidence-
based guideline on: treatment of osteoarthritis of the knee 2nd edition. J Bone Joint Surg Am. 2013;
95(20): 1885 – 1886.
Qaseem A, Barry MJ, Kansagara D. Nonpharmacologic Versus Pharmacologic Treatment of Adult Patients
With Major Depressive Disorder: A Clinical Practice Guideline From the American College of Physicians.
Ann Intern Med. 2016; 164(5): 350 – 359.
Seidman MD, Gurgel RK, Lin SY, et al. Clinical practice guideline: Allergic rhinitis. Otolaryngol Head Neck
Surg. 2015; 152(1 Suppl): S1 – 43.
Peer-reviewed references:
21CFR880.5580. Acupuncture needle.
Acupuncture: In Depth. National Center for Complementary and Integrative Health (NCCIH). NCCAM
website. http://nccam.nih.gov/health/acupuncture/introduction. Accessed January 10, 2017.
Chan YY, Lo WY, Yang SN, Chen YH, Lin JG. The benefit of combined acupuncture and antidepressant
medication for depression: A systematic review and meta-analysis. J Affect Disord. 2015; 176: 106 – 117.
Cheong KB, Zhang JP, Huang Y, Zhang ZJ. The effectiveness of acupuncture in prevention and treatment
of postoperative nausea and vomiting--a systematic review and meta-analysis. PLoS One. 2013; 8(12):
e82474.
Cherkin DC, Eisenberg D, Sherman KJ, et al. Randomized trial comparing traditional Chinese medical
acupuncture, therapeutic massage, and self-care education for chronic low back pain. Archives of
internal medicine. 2001; 161(8): 1081 – 1088.
Cui X, Zhou J, Qin Z, Liu Z. Acupuncture for Erectile Dysfunction: A Systematic Review. Biomed Res Int.
2016; 2016: 2171923.
10
del Pino-Sedeno T, Trujillo-Martin MM, Ruiz-Irastorza G, et al. Effectiveness of Nonpharmacologic
Interventions for Decreasing Fatigue in Adults With Systemic Lupus Erythematosus: A Systematic
Review. Arthritis Care Res (Hoboken). 2016; 68(1): 141 – 148.
Dong W, Goost H, Lin XB, et al. Treatments for shoulder impingement syndrome: a PRISMA systematic
review and network meta-analysis. Medicine (Baltimore). 2015; 94(10): e510.
Ernst E, Lee MS, Choi TY. Acupuncture: does it alleviate pain and are there serious risks? A review of
reviews. Pain. 2011; 152(4): 755 – 764.
Feng S, Han M, Fan Y, et al. Acupuncture for the treatment of allergic rhinitis: a systematic review and
meta-analysis. Am J Rhinol Allergy. 2015; 29(1): 57 – 62.
Furlan AD, Yazdi F, Tsertsvadze A, et al. A systematic review and meta-analysis of efficacy, cost-
effectiveness, and safety of selected complementary and alternative medicine for neck and low-back
pain. Evid Based Complement Alternat Med. 2012; 2012: 953139.
Garcia MK, McQuade J, Haddad R, et al. Systematic review of acupuncture in cancer care: a synthesis of
the evidence. J Clin Oncol. 2013; 31(7): 952 – 960.
Gutke A, Betten C, Degerskar K, Pousette S, Olsen MF. Treatments for pregnancy-related lumbopelvic
pain: a systematic review of physiotherapy modalities. Acta Obstet Gynecol Scand. 2015; 94(11): 1156 –
1167.
Hayes Inc., Hayes Medical Technology Report. Acupuncture for treatment of headache. Lansdale, Pa.
Hayes Inc.; 2009.
He M, Li X, Liu Y, et al. Electroacupuncture for Tinnitus: A Systematic Review. PLoS One. 2016; 11(3):
e0150600.
Hempel S, Taylor SL, Solloway MR, et al. Evidence Map of Acupuncture [Internet] VA-ESP Project #05-
226; 2013.
Hutchinson AJ, Ball S, Andrews JC, Jones GG. The effectiveness of acupuncture in treating chronic non-
specific low back pain: a systematic review of the literature. Journal of orthopaedic surgery and
research. 2012; 7: 36.
Kim KH, Lee MS, Kim TH, et al. Acupuncture and related interventions for symptoms of chronic kidney
disease. Cochrane Database Syst Rev. 2016; (6): Cd009440.
11
Kim SY, Lee H, Chae Y, Park HJ, Lee H. A systematic review of cost-effectiveness analyses alongside
randomized controlled trials of acupuncture. Acupuncture in medicine: journal of the British Medical
Acupuncture Society. 2012; 30(4):273 – 285.
Lam M, Galvin R, Curry P. Effectiveness of acupuncture for nonspecific chronic low back pain: a
systematic review and meta-analysis. Spine (Phila Pa 1976). 2013; 38(24): 2124 – 2138.
Lau CH, Wu X, Chung VC, et al. Acupuncture and Related Therapies for Symptom Management in
Palliative Cancer Care: Systematic Review and Meta-Analysis. Medicine (Baltimore). 2016; 95(9): e2901.
Law D, McDonough S, Bleakley C, Baxter GD, Tumilty S. Laser acupuncture for treating musculoskeletal
pain: a systematic review with meta-analysis. J Acupunct Meridian Stud. 2015; 8(1): 2 – 16.
Lee MS, Ernst E. Acupuncture for pain: an overview of Cochrane reviews. Chinese journal of integrative
medicine. 2011; 17(3):187 – 189.
Lim CE, Ng RW, Xu K, et al. Acupuncture for polycystic ovarian syndrome. Cochrane Database Syst Rev.
2016; (5): Cd007689.
Linde K, Allais G, Brinkhaus B, et al. Acupuncture for the prevention of tension-type headache. Cochrane
Database Syst Rev. 2016; 4: Cd007587.(a)
Linde K, Allais G, Brinkhaus B, et al. Acupuncture for the prevention of episodic migraine. Cochrane
Database Syst Rev. 2016; 6: Cd001218.(b)
Mangesi L, Zakarija-Grkovic I. Treatments for breast engorgement during lactation. Cochrane Database
Syst Rev. 2016; (6): Cd006946.
Manyanga T, Froese M, Zarychanski R, et al. Pain management with acupuncture in osteoarthritis: a
systematic review and meta-analysis. BMC Complement Altern Med. 2014; 14: 312.
National Certification Commission of Acupuncture and Oriental Medicine (NCCAOM). State licensure
requirements. 2015. Available at: http://www.nccaom.org/regulatory-affairs/state-licensure-map.
Accessed January 10, 2017.
Pennick V, Liddle SD. Interventions for preventing and treating pelvic and back pain in pregnancy. The
Cochrane database of systematic reviews. 2013; 8: Cd001139.
Pinto D, Robertson MC, Hansen P, Abbott JH. Cost-effectiveness of nonpharmacologic, nonsurgical
interventions for hip and/or knee osteoarthritis: systematic review. Value in health: the journal of the
International Society for Pharmacoeconomics and Outcomes Research. 2012; 15(1): 1 – 12.
12
Qin Z, Wu J, Zhou J, Liu Z. Systematic Review of Acupuncture for Chronic Prostatitis/Chronic Pelvic Pain
Syndrome. Medicine (Baltimore). 2016; 95(11): e3095.
Requirements for Certification in Medical Acupuncture. American Board of Medical Acupuncture
website. http://www.dabma.org/requirements.asp. Accessed January 10, 017.
Smith CA, Armour M, Zhu X, et al. Acupuncture for dysmenorrhoea. Cochrane Database Syst Rev. 2016;
4: Cd007854.
Su L, Meng L, Chen R, et al. Acupoint Application for Asthma Therapy in Adults: A Systematic Review and
Meta-Analysis of Randomized Controlled Trials. Forsch Komplementmed. 2016; 23(1): 16 – 21.
Van den Heuvel E, Goossens M, Vanderhaegen H, Sun HX, Buntinx F. Effect of acustimulation on nausea
and vomiting and on hyperemesis in pregnancy: a systematic review of Western and Chinese literature.
BMC Complement Altern Med. 2016; 16: 13.
Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture for chronic pain: individual patient data meta-
analysis. Arch Intern Med. 2012; 172(19): 1444 – 1453.
Wu MS, Chen KH, Chen IF, et al. The Efficacy of Acupuncture in Post-Operative Pain Management: A
Systematic Review and Meta-Analysis. PLoS One. 2016; 11(3): e0150367.
Yang A, Wu HM, Tang JL, et al. Acupuncture for stroke rehabilitation. Cochrane Database Syst Rev. 2016;
(8): Cd004131.
Yuan QL, Guo TM, Liu L, Sun F, Zhang YG. Traditional Chinese medicine for neck pain and low back pain:
a systematic review and meta-analysis. PLoS One. 2015; 10(2): e0117146.
Zhou J, Peng W, Xu M, Li W, Liu Z. The effectiveness and safety of acupuncture for patients with
Alzheimer disease: a systematic review and meta-analysis of randomized controlled trials. Medicine
(Baltimore). 2015; 94(22): e933.
CMS National Coverage Determinations (NCDs):
30.3 Acupuncture. CMS website. http://www.cms.gov/medicare-coverage-database/details/ncd-
details.aspx?NCDId=11&ver=1. Accessed January 10, 2017.
30.3.1 Acupuncture for Fibromyalgia. CMS website. http://www.cms.gov/medicare-coverage-
database/details/ncd-details.aspx?NCDId=283&ver=1. Accessed January 10, 2017.
30.3.2 Acupuncture for Osteoarthritis. CMS website. http://www.cms.gov/medicare-coverage-
database/details/ncd-details.aspx?NCDId=284&ver=1. Accessed January 10, 2017.
13
10.3 Inpatient Hospital Pain Rehabilitation Programs. CMS website. http://www.cms.gov/medicare-
coverage-database/details/ncd-details.aspx?NCDId=23&ver=1. Accessed January 10, 2017.
10.4 Outpatient Hospital Pain Rehabilitation Programs. CMS website. http://www.cms.gov/medicare-
coverage-database/details/ncd-details.aspx?NCDId=24&ver=1. Accessed January 10, 2017.
Local Coverage Determinations (LCDs):
No LCDs identified as of the writing of this policy.
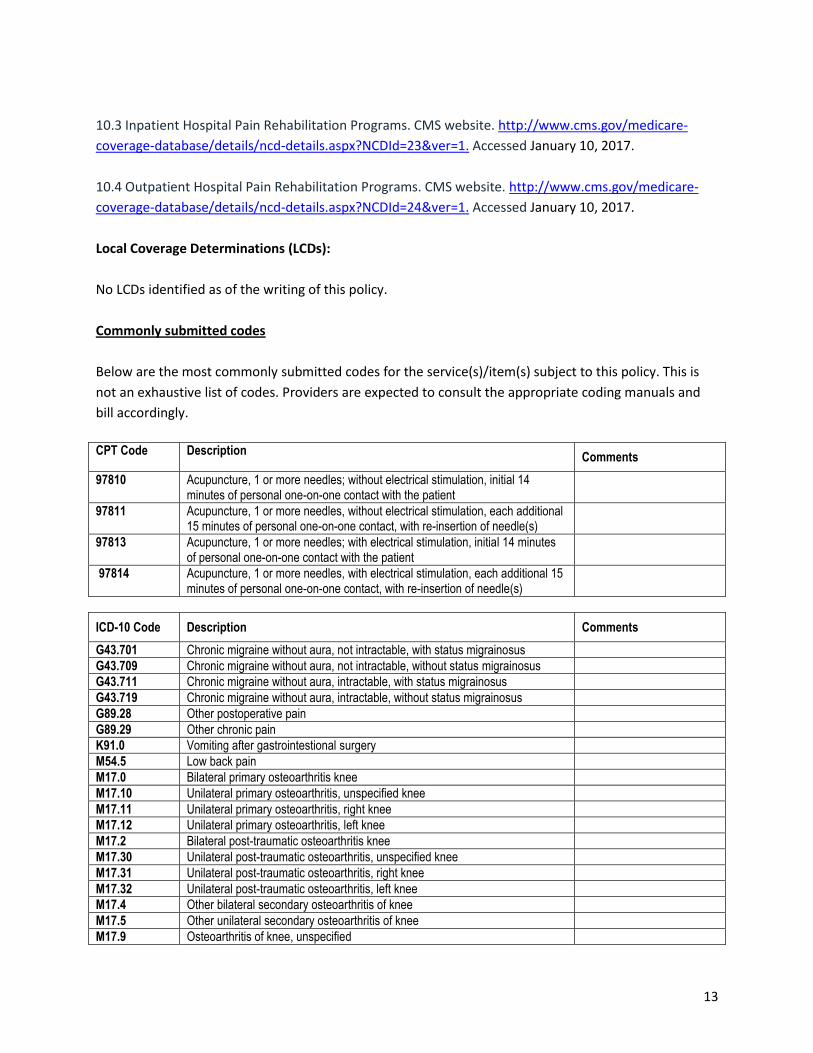
Commonly submitted codes
Below are the most commonly submitted codes for the service(s)/item(s) subject to this policy. This is
not an exhaustive list of codes. Providers are expected to consult the appropriate coding manuals and
bill accordingly.
CPT Code Description
Comments
97810 Acupuncture, 1 or more needles; without electrical stimulation, initial 14 minutes of personal one-on-one contact with the patient
97811 Acupuncture, 1 or more needles, without electrical stimulation, each additional 15 minutes of personal one-on-one contact, with re-insertion of needle(s)
97813 Acupuncture, 1 or more needles; with electrical stimulation, initial 14 minutes of personal one-on-one contact with the patient
97814 Acupuncture, 1 or more needles, with electrical stimulation, each additional 15 minutes of personal one-on-one contact, with re-insertion of needle(s)
ICD-10 Code Description Comments
G43.701 Chronic migraine without aura, not intractable, with status migrainosus
G43.709 Chronic migraine without aura, not intractable, without status migrainosus
G43.711 Chronic migraine without aura, intractable, with status migrainosus
G43.719 Chronic migraine without aura, intractable, without status migrainosus
G89.28 Other postoperative pain
G89.29 Other chronic pain
K91.0 Vomiting after gastrointestional surgery
M54.5 Low back pain
M17.0 Bilateral primary osteoarthritis knee
M17.10 Unilateral primary osteoarthritis, unspecified knee
M17.11 Unilateral primary osteoarthritis, right knee
M17.12 Unilateral primary osteoarthritis, left knee
M17.2 Bilateral post-traumatic osteoarthritis knee
M17.30 Unilateral post-traumatic osteoarthritis, unspecified knee
M17.31 Unilateral post-traumatic osteoarthritis, right knee
M17.32 Unilateral post-traumatic osteoarthritis, left knee
M17.4 Other bilateral secondary osteoarthritis of knee
M17.5 Other unilateral secondary osteoarthritis of knee
M17.9 Osteoarthritis of knee, unspecified
14
R11.2 Nausea and vomiting Add I10 code for adverse effect of type of chemo
HCPCS Level II
Description Comments
N/A