Embed Size (px)
Citation preview

Clinical Performance of Parathyroid HormoneImmunometric Assays
PAl c. KAO, Ph.D., Section of Clinical Biochemistry; JON A. van HEERDEN, M.B.,Ch.B.,CLIVE S. GRANT, M.D., Division ofGastroenterologic and General Surgery;GEORGE G. KLEE, M.D., Ph.D., Section ofMetabolic and Hematologic Biochemistry;SUNDEEP KHOSLA, M.D., Division ofEndocrinology/Metabolism and Internal Medicine
Three immunometric assays of parathyroid hormone (PTH)-a commercial immunoradiometricassay, an in-house immunoradiometric assay, and an immunochemiluminometric assay-were evaluated in 50 patients with surgically proven primary hyperparathyroidism. Of these patients, 43 hadincreased values with the commercial assay (sensitivity, 86%), whereas 45 patients had increasedconcentrations with both the in-house immunoradiometric and the in-house immunochemiluminometric assays (sensitivities, 90%). Because of the results of this comparison study, we confidently chose theimmunochemiluminometric assay as our routine assay; this assay was evaluated retrospectively in 361patients with surgically proven primary hyperparathyroidism. In 45 patients, PTH values were belowthe upper limit of normal (sensitivity, 88%). The results indicate that the sensitivities of currentimmunometric assays are approximately 90%. Twenty patients who had hypercalcemia associatedwith malignant involvement were assessed with the immunochemiluminometric assay. Of these 20patients, 19 had subnormal PTH values, and 1 had a value within the normal range. In contrast, in thepast, PTH values determined with radioimmunoassays have often been in the normal range for suchpatients. Thus, an immunometric PTH assay is superior to a radioimmunoassay in the differentialdiagnosis of hypercalcemia associated with malignant disease.
Parathyroid hormone (PTH) is a single-chain polypeptide of84 amino acid residues. Its major function is to maintain theserum total calcium concentration within a narrow range (8.9to 10.1 mg/dl). PTH increases the renal reabsorption ofcalcium and decreases the renal reabsorption of phosphate.A low renal phosphate concentration increases the synthesisof 1,25-dihydroxyvitamin D, an active hormone that stimulates calcium absorption in the intestine. Thus, the neteffects of PTH are to increase the serum concentration ofcalcium and to decrease that of phosphate.!?
Intact (l-84)PTH has a short biologic half-life (2 to 5minutes). It is rapidly degraded initially between aminoacids 34 and 35 into an amino (N)-tenninal (1-34) peptidefragment and a carboxyl (C)-terminal (35-84) peptide frag-
Address reprint requests to Dr. P. C. Kao, Section of ClinicalBiochemistry, Mayo Clinic, Rochester, MN 55905.
ment. The N-tenninal fragment is biologically as active asintact PTH, also has a short half-life (less than 5 minutes),and is rapidly degraded in the bloodstream. The C-tenninalpeptide is biologically inactive; however, in comparisonwith the N-tenninal fragment, it has a longer half-life (25 to~O minutes). In the circulation, the concentration of the Cterminal fragment is about lO-fold that of intact PTH, andthe concentration of the N-tenninal fragment is very low(virtually undetectablej.':'? Many assays, such as the Nterminal, midregion (44-68), and C-terminal PTH radioimmunoassays (RIAs), have been developed to measure various fragments of PTH. An ideal PTH assay should be usefulin the differential diagnosis of hypercalcemia caused byeither primary hyperparathyroidism or malignant disease. Intheory, serum PTH values would be increased above thenormal range in patients with primary hyperparathyroidismor increased in comparison with the level present before the
Mayo Clin Proc 67:637-645, 1992 637

638 PARATHYROID HORMONE IMMUNOMETRlC ASSAYS
disease developed. Hypercalcemia in patients with malignant involvement is caused by PTH-related peptide or otherfactors, and PTH concentrations in these patients would besuppressed.!':"
In a previous survey of RIAs, aliquots of serum from 14patients with primary hyperparathyroidism and from 20 withhypercalcemia associated with malignant disease were sentto five laboratories. The sensitivities of the RIAs for detecting primary hyperparathyroidism varied; the range was 57 to100%.14 In general, the sensitivities of C-terminal andmidregion assays ranged from 93 to 100%, except for one Cterminal assay with a sensitivity of 57%. The sensitivity ofan N-terminal assay, however, was only in the 70% range.Theoretically, because the N-terminal assay measured thebiologically active N-terminal fragment and also the intactPTH, it should be more accurate than the C-terminal ormidregion assay; however, for detecting primary hyperparathyroidism, the midregion and C-terminal RIAs outperformed the N-terminal RIA. One explanation may be thatthe very low to undetectable concentrations of N-terminalfragment allow the N-terminal RIA to measure only intact'PTH, which is at very low concentrations (picomoles/liter)and difficult to measure accurately by RIA. Thus, accuracyis a relative term; it is dominated by the analytic sensitivityof an assay and the concentration of an analyte present in aspecimen.
In the differential diagnosis of hypercalcemia, one of the .major deficiencies of all RIAs was that none showed suppressed PTH values in patients with hypercalcemia associated with malignant involvement. Typically, the assaysrevealed that these patients had PTH values within or evenslightly above the normal range, except for one assay thatapplied immunoextraction of N-terminal fragments and intact PTH from large volumes of specimens before determination by a midregion RIA.'5 This assay disclosed suppressed PTH levels in patients with malignant involvement;however, the sensitivity of this immunoextraction midregionassay for detecting primary hyperparathyroidism was lowerthan that of direct midregion RIA without extraction. Nonetheless, this concept of extraction provided a possible meansof measuring intact PTH in the clinical laboratory.
The high sensitivity (93 to 100%) of C-terminal or midregion PTH assays" was determined in a relatively smallnumber of patients (approximately 20) with surgicallyproven primary hyperparathyroidism. When the number ofpatients increased, the sensitivity decreased. Clearly, thetrue sensitivity of a PTH assay could be better determinedonly with a larger number of patients. One of our midregionassays, which had a sensitivity of 93% in a small number ofpatients," was further evaluated in a large number of patients(N = 1,061) with surgically proven primary hyperparathyroidism in a retrospective study during a 6-year period. The
Mayo CIiDProc, July 1992, Vol 67
sensitivity of the assay decreased to 86%. This percentagemay indeed be the true sensitivity of a PTH RIA. ' 6
Although a low concentration of PTH cannot be accurately detected by RIAs, the new technique of immunometricassay can detect subnormal levels (less than 1 pmol/liter) ofintact PTH. This "sandwich" assay uses one antibody ascapture antibody (generally, against C-terminal PTH) immobilized in solid phase to capture or to bind any PTH moleculethat has a C-terminal sequence. A second antibody as signalantibody (generally, against N-terminal PTH) is labeled witheither radioisotope or acridinium ester to bind the N-terminalportion of a PTH molecule to solid phase by captured antibody. After washing to remove the "free" (nonbound) signalantibody, the amount of signal antibody linked to the solidphase is measured. It is proportional to the amount of intactPTH present in a specimen. The assay is an immunoradiometric assay (IRMA)'7,'8 or an immunochemiluminometricassay (lCMA),'9,20 depending on whether radioisotope- oracridinium ester-labeled signal antibody is used.
Analytically, immunometric assays are superior to RIAs;they are easier to perform and can detect subnormal concentrations of intact PTH;17,18 currently, however, informationon the sensitivity of immunometric assays for detecting primary hyperparathyroidism is limited. Two recent publications reported that the sensitivity of a commercial IRMA(Allegro intact 'PTH assay) was 90% by estimation" and72% by examination of 29 patients."
In the current analysis, we studied the performance of ourimmunometric assay for detecting patients with primaryhyperparathyroidism and for determining the differentialdiagnosis in patients with hypercalcemia associated withmalignant disease. To determine the usefulness of ICMA,we first compared the results of three immunometric PTHassays-a commercially available IRMA (Allegro), anin-house IRMA. and an in-house ICMA-in 50 patients withsurgically proven primary hyperparathyroidism. The comparison study convinced us to choose ICMA as our routineassay. Next, we determined, retrospectively, the sensitivityof our ICMA in 361 patients with surgically proven primary hyperparathyroidism by reviewing a monthly tissueregistration list. To compare the performance of the PTHICMA and the PTH-related peptide RIA for determining thedifferential diagnosis in 20 patients with hypercalcemia associated with malignant disease, we measured PTH concentrations with ICMA and concentrations of PTH-relatedpeptide in the same patients. Finally, to detect intact PTHconcentrations in patients with chronic renal failure in whomparathyroidectomy was necessary, we determined PTHconcentrations by ICMA in 16 patients with chronic renalfailure who were receiving hemodialysis therapy and whorequired parathyroidectomy because of secondary hyperparathyroidism.

Mayo Clio Proc, July 1992, Vol 67
METHODSCommercial IRMA Reagent Kit.-The Allegro intact PTHassay was purchased from Nichols Institute Diagnostics (SanJuan Capistrano, California). The antiserum of this kit wasfrom goats immunized with partially purified human parathyroid hormone (hPTH) isolated from human parathyroidadenomas. N-terminal and C-terminal antibodies wereimmunopurified from the same antiserum with (1-34)hPTHand (39-84)hPTH affinity columns, respectively. The Nterminal (signal) antibody was labeled with 1251, and the Cterminal (capture) antibody was immobilized on polystyrenebeads. Specimen, signal antibody, and capture-antibodybead were added together for a 22-hour incubation at roomtemperature. The normal range suggested by the manufacturer of the kit was from 10 to 60 ng/liter."
In-House IRMA.-N-terminal antiserum was obtainedfrom goat A immunized with (l-44)hPTH conjugated tobovine serum albumin as carrier protein. We used (144)hPTH instead of (1-34)hPTH as antigen because no useful antiserum had been obtained previously with (1-·34)hPTH conjugated to various carrier proteins and injectedinto different animals. The (1-44)antiserum from goat A wasfurther immunopurified with a (1-34)hPTH-Sepharose 4Baffinity column. The (1-34)hPTH antibodies absorbed onthe affinity column were eluted from the column, lyophilized, and labeled with 1251 by the iodogen method. Theywere used as signal antibodies. The detailed immunizationmethod and schedule have been described previously."
Midregion antiserum was obtained from goat B immunized with (44-68)hPTH conjugated to bovine serum albumin. The antiserum was immunopurified with a midregion(44-68)hPTH affinity column. The N-terminal antiserumfrom goat A was also affinity purified, this time with a (144)hPTH affinity column. These affinity-purified,midregion (44-68), and N-terminal (1-44) antibodies (0.5 ~g
each) were immobilized on polystyrene beads by adsorption.Thus, our method detected both intact PTH and N-terminalfragments of PTH up to 44 residues rather than intact PTHonly.
For the assay, 200 ~l of ethylenediaminetetraacetic acidtreated plasma and 100 ul of signal antibody that contained200,000 cpm were incubated overnight at room temperature.Beads coated with immobilized capture antibody were thenadded and incubated for an additional 3 hours, after whichthey were washed. The rationale for delaying the addition ofcapture-antibody bead is to complete the binding ofPTH andsignal antibody first and then draw the complex to the bead.If the capture-antibody bead binds PTH first, because ofstereohindrance, the signal antibody may take longer to bindor binding may be difficult. The radioactivity on the beadswas counted in a gamma counter. (1-84)hPTH from Peninsula Laboratories, Inc. (Belmont, California) was used as
PARATHYROID HORMONE IMMUNOMETRIC ASSAYS 639
standard in a range of 0.09 to 106 pmol/liter. The normalrange of our in-house IRMA was 1.0 to 5.0 pmol/liter (N =61).
In-House ICMA.-The procedure for the ICMA wasidentical to that for our in-house IRMA. Both assays usedthe same beads coated with immunopurified (1-44)hPTHand (44-68)hPTH antibodies. The only difference was thesignal antibody. Instead of 1251-labeled (l-34)hPTH antibody, acridinium ester-labeled (1-34)hPTH immunopurifiedsheep antibody (Ciba Coming Diagnostics, East Walpole,Massachusetts) was used. After the same incubation andwashing procedure as described for the IRMA, chemiluminescent light was measured in a luminometer (Ciba Coming Magic Lite Analyzer II, Ciba Coming Diagnostics). Thenormal range of this assay was 1.0 to 5.0 pmol/liter (N =262). With the addition of (44-68)hPTH up to a concentration of 352 pmol/liter and of (53-84)hPTH up to 2,847 pmol!liter in specimens, no significant inhibition of recovery ofintact PTH was noted. The assay correlated well with ourbioassay for measuring various clinical specimens (N =102,r =0.81, slope =0.73, intercept =1.92).24
Parathyroid Hormone-Related Peptide.-Plasma PTHrelated peptide was measured with an extraction RIA (asdescribed previously)." In brief, 1.0 ml of ethylenediaminetetraacetic acid-treated plasma was extracted with a C-2cartridge, eluted, lyophilized, reconstituted, and assayed by a(1-34)PTH-related peptide RIA (Peninsula Laboratories,Inc.). The normal range was 2.0 to 5.0 pmol/liter (N =48).
Study Subjects. Primary HyperparathyroidismWith use of surgical and tissue registration lists, we retrospectively reviewed the PTH values of a total of 361 patientstreated for surgically proven primary hyperparathyroidism atour institution.
Hypercalcemia Associated With Malignant Disease.In the 20 patients with hypercalcemia associated with malignant disease, the conditions were as follows: squamous cellcarcinoma in 4 (lung in 2 and genital vulva in 2), renal cellcarcinoma in 4, malignant lymphoma in 4, multiple myeloma in 4, and small cell carcinoma of the lung, islet cellcarcinoma, papillary adenocarcinoma, and paraganglioma in1 each. All specimens were routine.
Chronic Renal Failure.-With use of surgical and tissueregistration lists, we studied the findings in 16 patients withchronic renal failure who required parathyroidectomy because of secondary or tertiary hyperparathyroidism.
RESULTSComparison of the Three Immunometric Assays.-Of the50 patients with surgically proven primary hyperparathyroidism, 7 had normal PTH values by the Allegro commercial assay, and 5 had normal results by both our in-houseIRMA and our ICMA (Fig. 1). The sensitivity for detection

640 PARATHYROID HORMONE IMMUNOMETRIC ASSAYS Mayo CIiDProc, July 1992, Vol 67
30 l- • 300I .:•25 I- 250-: •••20 I- ". •• • 200
15 I-.~ -r ••
tX- •• 150:::::: lie0 :::::
10 I- - ~• 120 0>E 9
.. ea· 110 c::I-a. :fi: .. .. 1008 I- -# ... II
A... 90 l-
I- 7 l- •• 5? 80 a.a. 6
~. •:fit 70
5
•60
4 50
3 40
23020
1 100 0
Mayo Mayo AllegroleMA IRMA IRMA
Fig. 1. Comparison of results with three immunometric assays-in-house immunochemiluminometrlc assay (Mayo leMA), in-house imrnunoradiornetric assay (Mayo IRMA), andcommercial immunoradiometric assay (Allegro IRMA)-in 50 patients with surgicallyproven primary hyperparathyroidism. Results were within normal range in five patientswith Mayo ICMA and IRMA and in seven patients with the Allegro assay. Correlation coefficients were as follows: Allegro IRMA versus Mayo IRMA, r = 0.949; Allegro IRMAversus Mayo ICMA, r = 0.959; Mayo IRMA versus Mayo ICMA, r = 0.946. PTH =parathyroid hormone; shaded areas = normal ranges.
of primary hyperparathyroidism was 86% (43 of 50 patients)for the Allegro assay and 90% (45 of 50) for the in-houseIRMA and ICMA. Other than the slight variance in sensitivity, the three assays correlated well (r value range, 0.946 to0.959). Because of these data, we confidently used ICMA asour routine assay.
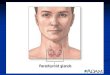
leMA in Primary Hyperparathyroidism.-In the retrospective study of 361 patients (including the patients described in the preceding paragraph) with surgically provenprimary hyperparathyroidism, 45 (12%) had normal PTHvalues (less than 5 pmol/liter) (Fig. 2). The sensitivity ofthe ICMA for detecting primary hyperparathyroidism was88%.
Among the 361 patients, the PTH values were between 5and 8 pmol/liter in 142 patients (39%), from 9 to 10 pmol/liter in 70 (19%), and between 11 and 15 pmol/liter in 65(18%) (Fig. 2). Thus, patients with surgically proven primary hyperparathyroidism did not have impressively increased PTH levels; approximately 50% of the values wereless than 8 pmol/liter, 71% were less than 10 pmol/liter,and almost 90% were less than 15 pmol/liter. In these361 patients, the median PTH value was 7.7 pmol/liter
(mean ± SO, 9.2 ± 6), and the values ranged from 2.1 to 74pmol/liter.
Hypercalcemia was confirmed by more than one determination (usually three) of the total serum calcium concentration. The median value concurrently measured with the PTHassay was 11.1 mg/dl (mean ±SO, 11.1 ±0.7), and the valuesranged from 9.7 to 16.7 mg/dl. In 5 of the 361 patients, theconcurrently measured total calcium value was less than10.1 mg/dl; however, hypercalcemia was verified in all patients preoperatively.
The serum phosphate value also was measured concurrently with the PTH value in this group of patients; 41% hadserum phosphate concentrations of less than 2.5 mg/dl (normal, 2.5 to 4.5, expressed as concentration of phosphorus inmilligrams per deciliter). The values, however, were lessthan 3.0 mg/dl in 80% ofthe patients and less than 3.5 mg/dlin 98% (Fig. 3). The serum phosphate value ranged from 1.2to 4.1 mg/dl; the median value was 2.7 mg/dl (mean ± SO,2.7 ± 0.5).
The serum creatinine values in this group ranged from 0.3to 1.9 mg/dl; the median value was 0.9 mg/dl (mean ± SO,0.97 ± 0.2). The correlation coefficients of calcium, phos-
Mayo Clio Proc, July 1992, Vol 67 PARATHYROID HORMONE IMMUNOMETRIC ASSAYS 641
Cumulative %I 100%I ll9%I 71%I---52%-----i~12%--i
60
~ 50:r::
i 40
'1:
~30"iii 20
E::> 10Z
3 4 5 6 7 6 9 10 11 12 13 14 15 16 20 25 35 75
ICMAPTH, pmol/l
Cumulative %I 100%I 88%I llO'll.I 41%
70
E: 80X
~50
'C: 40Q.
~ 30
~ 20E~
Z 10
1.7 1.9 2.1 2.3 2.5 2.7 2.9 3.1 3.3 3.5 4.1
Serum phosphorus, mg/dl
Fig. 2. Distribution of parathyroid hormone (PTH) concentrations(as determined with immunochemiluminometric assay [leMA]) in361 patients with surgically proven primary hyperparathyroidism(HPT).
Fig. 3.. Distribution of serum phosphate, measured as.concentrationsof phosphorus, in 361patientswithsurgically provenprimaryhyperparathyroidism (HPT).
Fig.4. Comparison of parathyroid hormone (PTH) andparathyroidhormone-related peptide (PTHrP) values in 20 patients who hadhypercalcemia associated withmalignant disease. Shaded areas =normalranges.
mg/dl; the median value was 10.5 mg/dl (mean ±SD, 10.5 ±0.8).
PTH With ICMA Versus Calcium Value ofPatients.We plotted the PTH concentration, determined with ICMA,against the total serum calcium concentration of three groupsof patients: (l) those with surgically proven primary hyperparathyroidism, (2) those with secondary and tertiary hyperparathyroidism of chronic renal failure, and (3) those with
,....------,100
•• '=
'0Y E
Q.10 a..-...
::I:5 Ii:
2
10.0
5.0
'='0EQ. 1.0
If-n,
..••••
0.1 ...
phate, and creatinine concentrations with PTH values thatwere determined with ICMA were 0.435, 0.337, and 0.310,respectively.
Hypercalcemia Associated With Malignant Disease.Of the 20 patients who had hypercalcemia associated withmalignant disease, 19 had PTH concentrations, as determined with ICMA, below the lower limit of normal (1.0pmolJliter) (Fig. 4 Left). The median value was 0.2 pmollliter (mean ± SD, 0.5 ± 0.7). The PTH-related peptidevalue was increased in 9 of the 20 patients, normal in 5, andbelow normal in 6 (normal, 2 to 5 pmollliter) (Fig. 4 Right).The median value was 4.2 pmol/liter (mean ± SD, 7.4 ±7.5).
The total serum calcium concentration in these patientsranged from 11.3 to 17.1 mg/dl. The median value was 12.6mg/dl (mean ± SD, 12.8 ± 1.2).
Chronic Renal Failure.-In the 16 patients with chronicrenal failure in whom parathyroidectomy was necessarybecause of secondary or tertiary hyperparathyroidism, thePTH levels, as determined with ICMA, ranged from 11 to 94pmol/liter; the median value was 38 pmolJliter (mean ± SD,42 ± 22). Of these 16 patients, 14 had PTH levels that werehigher than the levels in most of the patients with primaryhyperparathyroidism (Fig. 5). In the other two patients, thePTH values were 11 and 19 pmol/liter. All 16 patients hadsubstantially increased creatinine and serum phosphate concentrations. The creatinine values ranged from 2.2 to 15.0mg/dl (mean ± SD, 9.0 ± 3.8), and the serum phosphatevalues ranged from 4 to 11 mg/dl (mean ± SD, 6.3 ± 2). Thetotal serum calcium concentrations ranged from 8.6 to 11.6

642 PARATHYROID HORMONE IMMUNOMETRIC ASSAYS Mayo Clio Proc, July 1992, Vol 67
1810 11 12 13 14 15 16 17
Serum Ca, mg/dl9
o8
1° HPT
•• •
::::::: • •0 • •E •c.. •J: 15
h:E:3
10"-CD
en
5
Fig. 5. Parathyroid hormone (PTll) concentrations plotted against total serum calcium(Ca) valuesin 361 patientswith surgically proven primaryhyperparathyroidism (10 HPT)(e), 20 patients withhypercalcemia associated with malignantdisease(.), and 16patientswithchronic renal failure (.a.).
hypercalcemia associated with malignant disease (Fig. 5).The results show a clear separation of the first and thirdgroups of patients.
DISCUSSIONThe performance of the three immunometric assays wascomparable (r = 0.946 to 0.959), although both in-houseassays (ICMA and IRMA) had a slightly greater sensitivity(90%) than the commercial assay (86%) for detecting increased PTH values in the group of 50 patients with surgically proven primary hyperparathyroidism. This observation indicates that the variability of PTH measurement byimmunometric assays might be smaller than that of RIA andthat ICMA is a useful PTH assay. We chose the ICMA asour routine PTH assay because (1) it seemed to be moresensitive, or at least was not less sensitive, than IRMA assaysand (2) the nonradioisotope acridinium ester used for labeling was much less harmful and had a substantially longerreagent shelf life than did 1251.
After 2 years of use of the ICMA as our routine PTHassay, its sensitivity, as determined retrospectively in 361patients with surgically proven primary hyperparathyroidism, was 88%. The newly developed imrnunometricassay was only slightly more sensitive than the old C-terminal RIA, which had a sensitivity of 86%, as determined in1,061 patients with surgically proven primary hyperparathyroidism." In these patients, the median PTH value, as determined by C-terminal RIA, was 78 ul eq/ml (normal, lessthan 50); the biologically inactive C-terminal fragment wasnot impressively increased either.
For the differential diagnosis of hypercalcemia associatedwith malignant disease versus primary hyperparathyroidism,immunometric PTH assays are clearly superior to RIAs. Ofthe 20 patients with hypercalcemia caused by malignantinvolvement, 19 had PTH concentrations, as determinedwith ICMA, below the normal range. RIAs usually gavePTH values within the normal range in patients with hypercalcemia associated with malignant tumors." In the same

Mayo CIiDProc, July 1992, Vol 67
patients, a PTH-related peptide assay showed increased values in only 9 of these 20 patients (45%). Currently, PTHrelated peptide assays are in an early stage of clinical application. The four PTH-related peptide assays with publisheddescriptions are two extraction RIAs, one IRMA, and onedirect RIA. Their overall sensitivity for detecting hypercalcemia associated with malignant lesions is approximately 50to 70%.25-28
Sensitivity is the standard term used to describe the utilityof an assay. A 90% sensitivity indicates that the assay willdetect a PTH value above the normal range in 90% of patients with disease. Alternatively, it indicates that 10% ofpatients with disease will have values that overlap the normal range. Clinically, this overlap can impair our ability todiagnose primary hyperparathyroidism and lead to additional, sometimes unnecessary, tests to exclude the causes ofhypercalcemia. With the use of superior immunometricassays for PTH, we had hoped that this overlap of PTHvalues between patients with primary hyperparathyroidismand normal subjects would be eliminated. The immunometric PTH assays, however, did not seem to have a substantially improved sensitivity in comparison with that of the oldRIAs. Two recent publications'"-" reported that the sensitivity of the same commercial PTH assay was 90% by estimation and 72% by determination in 29 patients. Our reportconfirms their finding that considerable overlap in PTH values still exists between patients with primary hyperparathyroidism and normal subjects, even with the use of immunometric assays.
In one of these reports," the same group of 29 patientswas tested with a homogeneous midregion RIA; surprisingly, the sensitivity for hyperparathyroidism was 100%.Reagents for the homogeneous assay were (44-68)hPTHprepared tracer, (44-68)hPTH standard, and a midregionPTH antibody. With this homogeneous midregion RIA,however, one of the normal subjects had a considerablyincreased PTH value and, as in other RIAs, PTH concentrations in patients with hypercalcemia associated with malignant disease were not totally suppressed; they were withinthe normal range instead of below the normal range, as foundwith immunometric assays. The investigators believed thatthe midmolecule PTH may be directly released from parathyroid tumors into the circulation; thus, the midmoleculePTH values are increased in patients with hyperparathyroidism." An alternative possibility, however, is that degradation of intact PTH is increased in the circulation as anadaptive mechanism induced by hypercalcemia." In ourexperience with a similar midregion RIA, the sensitivity ofour homogeneous midregion assay was not better than thatof the regular C-terminal PTH RIAs, The sensitivity of thehomogeneous midregion RIA needs to be tested further in alarge group of patients with surgically proven primary
PARATIIYROID HORMONE IMMUNOMETRIC ASSAYS 643
hyperparathyroidism to confirm its value in the diagnosis ofprimary hyperparathyroidism.
The problem of overlap of results between patients withdisease and normal subjects exists in many other hormonalmeasurements and is not unique to primary hyperparathyroidism. For example, not all patients with pituitary Cushing's disease have increased concentrations of adrenocorticotropic hormone (corticotropin). When these values areincreased, they may also be due to secretion of immunoreactive corticotropin by a nonpituitary tumor ("ectopic ACTHsyndrome"). Rather than relying only on the corticotropinmeasurement, clinicians often rely on dynamic tests, such asthe dexamethasone suppression test and stimulation of corticotropin-releasing hormone, in conjunction with sampling ofthe petrosal sinus to distinguish patients with pituitary Cushing's disease from those with ectopic production of corticotropin.v" In contrast, currently no diagnostically dynamic test is available for primary hyperparathyroidism.Both ethylenediaminetetraacetic acid stimulation of secretion of PTH and infusion of calcium to suppress secretion ofPTH have been used only in experimental animals and human volunteers, but they have not been accepted for routineclinical practice. The lack of clinical use has been primarilydue to the cumbersomeness of the ethylenediaminetetraacetic acid procedure and the concern about inducingfurther severe hypercalcemia after infusion of calcium inpatients with existing hypercalcemia.
In addition to its effect on serum calcium concentration,PTH has important effects on serum phosphate levels. Itdecreases the renal tubular reabsorption of phosphate. Thus,in hyperparathyroidism, the serum phosphate concentrationshould be low. Superficially, measurement of serum phosphate did not help in the interpretation of primary hyperparathyroidism because only 41% of the patients with primary hyperparathyroidism had serum phosphate values below the normal range (2.5 to 4.5 mg/dl), and 59% had valueswithin the normal range; however, 80% of the results wereless than 3.0 mg/dl, and 98% were less than 3.5 mg/dl. Thesepercentages of distribution of serum phosphate concentrations were repeatedly confirmed in two previous studies'<"and in the current study in a total of 1,520 patients withsurgically proven primary hyperparathyroidism. Serumphosphate, however, is not a specific marker. Transienthypophosphatemia can result from the use of phosphatebinders, such as aluminum hydroxide and antacid gel.
Patients with chronic renal failure have increased serumphosphate values because of impaired renal tubular excretion of phosphate. High renal phosphate concentrationsinhibit the synthesis of 1,25-dihydroxyvitamin D, decreaseintestinal absorption of calcium, and cause oversecretion ofPTH. Secondary and tertiary hyperparathyroidism will thendevelop. These patients, however, can be identified by the

644 PARATHYROID HORMONE IMMUNOMETRIC ASSAYS
increased serum creatinine values (as shown in the 16 patients with chronic renal failure in the current study). Theincreased phosphate and PTH values in such patients will notinterfere with the usefulness of the serum phosphate concentration in the interpretation of primary hyperparathyroidism.Seldom, patients with primary hyperparathyroidism haveserum creatinine concentrations of more than 2 mg/dl, andpatients with secondary and tertiary hyperparathyroidismhave serum creatinine values of less than 2 mg/dl. Therefore, routinely in our PTH assay, we concurrently measureserum PTH, total calcium, phosphate, and creatinine concentrations to facilitate the interpretation.
Analytically, immunometric assays can detect subnormalconcentrations of intact PTH, whereas RIAs cannot. Thisinability of the RIA can be explained by two major differences: the amount of signal and the nature of the two assays.Generally, 10,000 counts of signal per tube are used in RIA,but a quarter million counts of signal per tube are used inimmunometric assays because the antigen is labeled in RIA.The small molecule (9,500 daltons) of PTH cannot be labeled with a large amount of radioisotope without damagingits immunoaffinity. In immunometric assays, the signal islabeled on the antibody, which is considerably larger(140,000 daltons) and can incorporate larger amounts oflabel than PTH. The large amount of signal per assay tubeimproves analytic accuracy. RIA is a reverse-direction assay; it measures suppression of total counts bound with anincreasing concentration of PTH. The most reliable portionof the RIA suppression curve is between 20 and 80%. Anyspecimen with less than 20% suppression is reported as lessthan a certain amount of PTH, which produces 20% of thesuppression. RIA has no ability to determine subnormallevels of PTH. In contrast, the immunometric assay is aforward-direction assay; the signal increases with the increase in PTH concentration. For example, in ICMAs, theincreases in signal over the background of 0.1, 0.4, 0.8, and1.5 pmol/liter of PTH doses are 25%, 60%, 110%, and260%, respectively. The large increments allow completeconfidence in the reporting of subnormal levels (less than 1.0pmollliter) of PTH. In both IRMAs, the percentages ofincrement are smaller than those of ICMA. For example, 1.5pmollliter is associated with an increment of 130% abovebackground in IRMA instead of 260%. The smaller increments in IRMA may explain why ICMA is more sensitivethan IRMA for detecting small doses of intact PTH.
CONCLUSIONThe newly developed ICMA for PTH is technically an important improvement that enables us to measure, in levels of0.1 pmol/liter, biologically active PTH molecules withoutinterference from biologically inert C-terminal fragments.This ability substantially improves the differential diagnosis
Mayo elin Proc, July 1992, Vol 67
of primary hyperparathyroidism and hypercalcemia associated with malignant disease. PTH values were suppressed tosubnormal in most patients who had hypercalcemia associated with malignant involvement. The sensitivity for detecting primary hyperparathyroidism (90%) is only slightlyimproved over that of RIA (86%).
ACKNOWLEDGMENTWe are indebted to our associates in the endocrine laboratories and the tissue registry office. Their efforts made thiswork possible.
REFERENCES1. Potts JT Jr, Kronenberg HM, Rosenblatt M: Parathyroid
hormone: chemistry, biosynthesis, and mode of action. AdvProtein Chern 35:323-396, 1982
2. Nissenson RA, Abbott SR, Teitelbaum AP, Clark OR, Arnaud CD: Endogenous biologically active human parathyroid hormone: measurement by a guanyl nucleotide-amplified renal adenylate cyclase assay. J Clin Endocrinol Metab52:840-846, 1981
3. Cohn DV, MacGregor RR, Chu LLH, Kimmel JR, HamiltonJW: Calcemic fraction-A: biosynthetic peptide precursor ofparathyroid hormone. Proc Nat! Acad Sci USA 69:15211525, 1972
- 4. Brown EM: PTH secretion in vivo and in vitro: regulation bycalcium and other secretagogues. Miner Electrolyte Metab8:130-150,1982
5. Cohn DV, Macfrregor RR: The biosynthesis, intracellularprocessing, and secretion of parathormone. Endocr Rev 2:126, 1981
6. Portale AA, Booth BE, Tsai HC, Morris RC Jr: Reducedplasma concentration of 1,25-dihydroxyvitamin D in childrenwith moderate renal insufficiency. Kidney Int 21:627-632,1982
7. MacGregor RR, Cohn DV, Hamilton JW: The content ofcarboxyl-terminal fragments of parathormone in extracts offresh bovine parathyroids. Endocrinology 112:1019-1025,1983
8. Bringhurst FR, Segre GV, Lampman GW, Potts JT Jr: Metabolism of parathyroid hormone by Kupffer cells: analysisby reverse-phase high-performance liquid chromatography.Biochemistry 21:4252-4258,1982
9. Botti RE Jr, Heath E, Frelinger AL, Chuang J, Roos BA, ZullJE: Specific cleavage of bovine parathyroid hormone catalyzed by an endopeptidase from bovine kidney. J BioI Chern256:11483-11488,1981
10. Hamilton JW, Jilka RL, MacGregor RR: Cleavage of parathyroid hormone to the 1-34 and 35-84 fragments by cathepsin D-like activity in bovine parathyroid gland extracts.Endocrinology 113:285-292, 1983
11. Marx SJ, Sharp ME, Krudy A, Rosenblatt M, Mallette LE:Radioimmunoassay for the middle region of human parathyroid hormone: studies with a radioiodinated synthetic peptide. J Clin Endocrinol Metab 53:76-84,1981
12. Mallette LE, Tuma SN, Berger RE, Kirkland JL: Radioimmunoassay for the middle region of human parathyroid hormone using an homologous antiserum with a carboxy-terminal fragment of bovine parathyroid hormone as

Mayo Clin Proc, July 1992, Vol 67
radioligand. J Clin Endocrinol Metab 54:1017-1024,1982
13. Arnaud CD, Kolb FO: The calciotropic hormones & metabolic bone disease. In Basic & Clinical Endocrinology. Second edition. Edited by FS Greenspan, PH Forsham. LosAltos, California, Lange Medical Publications, 1986, pp 202271
14. Lufkin EG, Kao PC, Heath H Ill: Parathyroid hormoneradioimmunoassays in the differential diagnosis of hypercalcemia due to primary hyperparathyroidism or malignancy.Ann Intern Med 106:559-561, 1987
15. Lindall AW, Elting J, Ells J, Roos BA: Estimation ofbiologically active intact parathyroid hormone in normal and hyperparathyroid sera by sequential N-terminal immunoextractionand midregion radioimmunoassay. J Clin Endocrinol Metab57:1007-1014,1983
16. Kao PC: Parathyroid hormone. In-Service Training andContinuing Education, American Association for ClinicalChemistry 9:5-17, October 1990
17. Nussbaum SR, Zahradnik RJ, Lavigne JR, Brennan GL,Nozawa-Ung K, Kim LY, Keutmann HT, Wang C-A, PottsJT Jr, Segre GV: Highly sensitive two-site immunoradiometric assay of parathyrin, and its clinical utility in evaluatingpatients with hypercalcemia. Clin Chern 33:1364-1367,1987
18. Blind E,Schmidt-Gayk H, Armbruster FP, Stadler A: Measurement of intact human parathyrin by an extracting two-siteimmunoradiometric assay. Clin Chern 33:1376-1381,1987
19. Brown RC, Aston JP, S1.John A, Woodhead JS: Comparisonof poly- and monoclonal antibodies as labels in a two-siteimmunochemiluminometric assay for intact parathyroidhormone. J Immunol Methods 109:139-144, 1988
20. Bohler U, Blind E, Vogel G, Hitzler W, Fientje D, SchmidtGayk H: Two-site immunochemiluminometric assay of intact human parathyrin in serum with use of a tracer peptidepurified by reversed-phase high-performance liquid chromatography. Clin Chern 35:215-222,1989
21. Nussbaum S: Immunometric assays of parathyrin in thediagnosis of hypercalcemic individuals (editorial). ClinChern 37:142-143,1991
22. Endres DB, Villanueva R, Sharp CF Jr, Singer FR: Immunochemiluminometric and immunoradiometric determinationsof intact and total immunoreactive parathyrin: performance
PARATHYROID HORMONE IMMUNOMETRIC ASSAYS 645
in the differential diagnosis of hypercalcemia and hypoparathyroidism. Clin Chern 37:162-168, 1991
23. Klee GG, Preissner CM, Schloegel IW, Kao PC: Bioassay ofparathyrin: analytical characteristics and clinical performance in patients with hypercalcemia. Clin Chern 34:482488, 1988
24. Klee GG, Preissner CM, Schryver PG, Taylor RL, Kao PC:Multisite immunochemiluminometric assay for simultaneously measuring whole-molecule and amino-terminal fragments of human parathyrin. Clin Chern 38:628-635,1992
25. Kao PC, Klee GG, Taylor RL, Heath H Ill: Parathyroidhormone-related peptide in plasma of patients with hypercalcemia and malignant lesions. Mayo Clin Proc 65: 1399-1407,1990
26. Budayr AA, Nissenson RA, Klein RF, Pun KK, Clark OH,Diep D, Arnaud CD, Strewler GJ: Increased serum levels ofaparathyroid hormone-like protein in malignancy-associatedhypercalcemia. Ann Intern Med 111:807-812, 1989
27. Burtis WJ, Brady TG, Orloff n, Ersbak JB, Warrell RP Jr,Olson BR, Wu TL, Mitnick ME, Broadus AB, Stewart AF:Immunochemical characterization of circulating parathyroidhormone-related protein in patients with humoral hypercalcemia of cancer. N Engl J Med 322:1106-1112,1990
28. Henderson JE, Shustik C, Kremer R, Rabbani SA, HendyGN, Goltzman D: Circulating concentrations of parathyroidhormone-like peptide in malignancy and in hyperparathyroidism. J Bone Miner Res 5:105-113,1990
29. Chrousos GP, Schulte HM, Oldfield EH, Gold PW, CutlerGB Jr, Loriaux DL: The corticotropin-releasing factor stimulation test: an aid in the evaluation of patients with Cushing'ssyndrome. N Engl J Med 310:622-626, 1984
30. Nieman LK, Chrousos GP, Oldfield EH, Avgerinos PC, Cutler GB Jr, Loriaux DL: The ovine corticotropin-releasinghormone stimulation test and the dexamethasone suppressiontest in the differential diagnosis of Cushing's syndrome. AnnIntern Med 105:862-867,1986
31. Young WF Jr, Zinsmeister AR, Twomey CK, Kao PC, JiangN-S, Carpenter PC: Ovine corticotropin releasing hormonestimulation test: normal value study. Mayo Clin Proc65:943-948, 1990
32. Kao PC, Jiang N-S, Klee 00, Purnell DC: Development andvalidation of a new radioimmunoassay for parathyrin (PTH).Clin Chern 28:69-74,1982














![4. PARATHYROID HORMONE.ppt [Read-Only]ocw.usu.ac.id/.../mk_end_slide_parathyroid_hormone.pdf · Parathyroid Hormone (PTH) Peptide hormone secreted by parathyroid glands, which are](https://img.pdfslide.us/doc/110x75/5fd9a3fa6d8805309b4bc740/4-parathyroid-read-onlyocwusuacidmkendslideparathyroidhormonepdf.jpg)