Embed Size (px)
Citation preview

Bite to Left Leg. Walker, Hogan
University of Oklahoma Ilealth Sciencqs Center, Oklahoma City. OK
Sectibn of Emergency Medicine (JSW, DEH)
I
I
Clinical Pearls
Bite to the Left Leg James S. Walker, DO, David E. Hogan, DO
fhoio&aflhic critique: Phreb Petersen Photbgraphy Supervisor The pdiversity of Texas Health Science Center at San Antonio San An!onio, TX
Lawtenice €3. Stack. MD Joint Military Medical Centers Emelgqncy Medicine Residency Brooke Army Medical Center Wilfprd Hall Medical Center San Antonio. TX
Sectioil Eiditor:
17. 1994 Rec-’. .LA. 11 _... Re\ d: October 19, 1993 Acc 3er 30. 1991
A d it: Funding for these edu :rials has been
health cak professionals.
Keywrkds: wound: spider bite; Loxmdef rccfusa; IomsceIisrn; necrotic arachnidism 4”
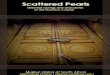
I FIGURE 1. T h e “bite” on the initial ED visit
Chief complaint: Bite to the left leg.
History of present illness: A 19-year-old man presents with the com- plaint of “something bit me” 24 hours ago on the posterior aspect of the left calf. A minor “stinging or sticking” sensation was felt shortly after putting on his jeans, which had been left on the bedroom floor overnight. He was not able to visualize or identify what had caused this skin irritation. He remained asymptomatic until eight hours later, when the involved area of skin began to itch as well as hurt. Worsening pain prompted this ED visit. He has no other complaint. He is healthy and takes no medication. Immunizations are current. He denies to- bacco, alcohol, and illicit drug use.
Physical examination: The patient is alert and in mild discomfort. Vital signs are normal. The examination is normal except for the lesion of the left calf (Fig. 1). The lesion is 2 x 2 cm with two areas of ecchymosis with circumferential pallor.
Initial management: The patient was diagnosed as having an insect bite, was prescribed diphenhydramine (50 mg) four times a day, and was instructed to return to the ED in four to five days if there was no improvement. (The patierit course appears 011 page 231 .)

Bite to Left Leg, Wa(ker, Hogan 23 1
Clinical Pearls (cont . from page 223)
Patient course: The patient returns to the ED four days later because the skin lesion is getting worse. The patient adamantly states that he took the diphenhydra- mine as prescribed. The patient also reports that he has developed “flu symptoms” over the past 96 hours and feels weak. is fatigued, and has a headache. He reports having a low-grade fever and chills over the last few days.
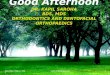
Physical examination on the return visit is normal except for a fever of 37.9”C and tachycardia of 110 beatslmin. The lesion of the left calf has become an 8 x 5-cm necrotic ulcer (Figs. 2 and 3). The ulcer is
indurated with serpiginous edges and circumferential erythema. A black eschar (2 X 2 cm) is noted superi- orly. The base of the ulcer is exudative with scattered pockets of subcutaneous fat protruding from the floor. There is no active bleeding. There is no sign of lym- phangitis, cellulitis, or localized infection. There is no reactive lymph node in the popIiteaI fossa or left in- guinal region.
A complete blood count (CBC) reveals a WBC count of 17.2 10y/L, a hemoglobin level of 102 g/L (10.2 g/ dL), a hematocrit of 31.0%, and a platelet count of 96 10y/L. The urinalysis is normal.
(The correct dingnosis m7d discussion appear 017 page 234.)
I FIGURES 2 and 3. The patient’s leg on the return visit. An S X 5-cm ulcer is seen

234 ACADEMIC EMERGENCY MEDICINE MAR 1995 VOL 2/NO 3
CliniCtZl PeUrts (cont. from page 231)
Diagnosis: Necrotic ulcer from a brown recluse spider (Loxosceles reclusa) bite (cutaneous and systemic loxos- celism).
Discussion In many parts of the United States, the brown re-
cluse, or fiddle back, spider is becoming one of the most feared animal envenomations by the lay public due to its disfiguring localized effects. Furthermore, this fear has been propagated by media coverage of a few sen- sational cases. The media are quick to point out that the fiddle back spider is a much greater public health menace than is the infamous black widow spider or any other arachnid. Accordingly, many patients will express their concern that they may have been bitten by such a spider.
The spider, Loxosceles reclusa, acquired its common names of brown recluse, fiddle back, or violin spider by virtue of its appearance, its habitat, and its de- meanor. The spider obtained its name of “violin” or “fiddle back” from the characteristic fiddle- or violin- like marking on the dorsal surface of the cephalothorax. The body portion of the violin is always toward the head of spider and the neck of the violin points to the posterior. The abdomen of the spider has no distin- guishing mark. The color of the body (abdomen and cephalothorax) varies from a light or dark brown to a dark shade of gray. The legs are usually darker than the body. These spiders vary in size from 2 cm to 5 cm, inclusive of leg length (Fig. 4).
The spiders are often found in a “country” setting in addition to the buildings of man. In the rural habitat,
I FIGURE 4. A brown recluse (Loxosceks reclusa) spider.
the spiders are found around and under woodpiles and rock piles. However, abandoned buildings, barns, and grain bins tend to be their most preferred abodes. In the urban setting, areas of the home that have low activity levels tend to be chosen. Closets, attics, and garages are favorite homesites in the “urban” setting. These spiders are not aggressive and are easily fright- ened. The spiders will not attack unless they are trapped or threatened. They are nocturnal and hunt moths, flies, beetles, and other spiders for a food source. The spi- ders’ activity cycles peak from April to October. They hibernate during the fall and winter.’.2
Clinical Presentation Loxosceles envenomations can be divided into lo-
calized (cutaneous) and systemic manifestations. As with any type of envenomation, the patient commonly pre- sents with predominantly localized rather than systemic symptoms. Also, systemic reactions do not necessarily correlate with the severity of the cutaneous lesions.
Localized Manifestations The spectrum of events associated with the local
effects of a brown recluse spider bite is called cutaneous loxoscelism. It is important to understand the chron- ologic appearance of the evolving necrotic bite to be able to diagnose the skin lesion at various stages of development (Fig. 5 ) . Initially, the patient may notice only transient irritation of the skin. Accordingly, few patients are able to catch or identify the arthropod re- sponsible for the bite. In fact, it has been suggested that many Loxosceles bites are never brought to the attention of the physician due to their minor n a t ~ r e . ~ . ~ After two to eight hours, the affected area becomes an indurated, erythematous papule. This papule eventu- ally turns white from the localized thrombosis, vaso- constriction, and subsequent infarction of the tissue. The skin lesion then turns ecchymotic as necrosis de- velops and becomes more evident with the development of a hemorrhagic vesicle. The time frame from the onset of the bite to the formation of the hemorrhagic vesicle is usually two to five days. The vesicle subsequently ruptures and forms a black eschar or crust. When the crust sloughs, it has a necrotic ulcer, which can extend through the subcutaneous fat and expose muscles and fascia1 planes. These ulcers can be quite large (up to 25 cm) and disfiguring. Secondary bacterial infection is a clinical concern.

~ ~~~~~ ~~
Bite to Left Leg, Walker, Hogan 235
Systemic Manifestations Significant systemic manifestations are known as
“viscerocutaneous” loxoscelism, or, simply, systemic lox~scelism.~ The clinical spectrum ranges from fever, chills, malaise, arthralgias, nausea and vomiting, and scarlatiniform rash to hemolytic anemia, renal failure, and disseminated intravascular coagulation (DIC) with fibrinolysis.
Systemic loxoscelism is reported to develop in fewer than 10% of cutaneous cases.’ There is a higher fre- quency of systemic symptoms in children than adults.‘ At times the systemic manifestations may develop be- fore the cutaneous lesion becomes clearly apparent, resulting in difficulty in diagnosis. Acute onset of fever, usually within 24 hours of envenomation, followed by the development of a generalized rash and constitu- tional symptoms may herald the syndrome. A hemolytic anemia may develop, progressing to thrombocytopenia and DIC. Renal failure may occur from hemoglobin- uria. The hemolytic process usually resolves within a week when complications are supported. However, death may result from renal failure, DIC, or other organ fail- ure.
Laboratory Diagnosis GeneraHy, the diagnosis is established clinically” with
special emphasis being placed upon the physical ap- pearance of the necrotic lesion. N o specific laboratory assay is commercially available nor are laboratory val- ues uniformly consistent with Loxosceles envenoma- tion. A passive hemagglutination inhibition test has been used in animal models’ but has not been verified in humans. Although not diagnostically useful, many lab- oratory abnormalities can be associated with systemic loxoscelism. Elevated WBC counts are commonly noted. A Coombs-positive hemolytic anemia is sometimes pre- sent. Thrombocytopenia, elevated fibrin split products, and diminished fibrinogen levels are associated with DIC. As noted above, .hemoglobinuria and proteinuria may be present.
Differential Diagnosis
Without confirmatory laboratory tests, it is impor- tant that the clinician recognize lesions that could be confused with loxoscelism. The following medical con- ditions have been misdiagnosed as being a “brown recluse spider bite”: 1) erythema chronicum migrans, 2) pyoderma gangrenosum, 3) erythema nodosum, 4) periarteritis nodosa, 5 ) sporotrichosis, 6) purpura ful- rninans, 7) diabetic ulcer, 8) poison ivy, 9) toxic epi- dermal necrolysis, 10) erythema multiforme, 11) in- fected herpes simplex, and 12) tularemia (ulceroglandular).X It also is noteworthy that a number
Erythematous papule (2-8 hours)
1
1
.1
4
J
White vasoconstriction (8-72 hours)
Ecchymosis (24-72 hours)
Hemorrhagic vesicle (48-96 hours)
Eschar (4-7 days)
Ulcer (4 days-several months)
FIGURE 5. Flow diagram showing the sequential evolution of cu- taneous loxoscelism.
of spiders in the United States are venomous and cause necrotic ulcers that may be mistaken for a brown recluse spider bite.
Treatment There is currently no “standard of care” for treating
patients for cutaneous loxoscelism. Although many cli- nicians have management strategies, few of them are grounded scientifically using double-blinded experi- mental designs. Management may be more appropri- ately called “therapeutic art forms.”
Most Loxosceles envenomations resolve without specific therapy within a few weeks to months. Benign neglect and wound care have been used in many cases with successful results.’ However, despite good local wound care and antibiotics, some patients develop sig- nificant ulcers. “’
Antibiotics are commonly used due to the angry appearance of the lesions. The inflammatory reaction associated with the bite makes it difficult to diagnose true cellulitis. Because of this difficult distinction, many clinicians use antibiotics as part of the usual treatment of Loxosceles envenomation, but benefit has not been clearly shown. Antihistamines have been used and are somewhat helpful in decreasing the itch and pain as- sociated with the lesion, probably via their sedative action.
Steroid use by injection into the lesion as well as oral or systemic administration have been suggested.. However, animal studies have shown that intralesional injections of steroids increase intralesional pressure, prolong vasoconstriction, and fail to neutralize the venom.’’-’3
Dapsone therapy has been studied and there are

~ ~~ ~
236 ACADEMIC EMERGENCY MEDICINE MAR 1995 VOL 2/NO 3
indications of some benefit.* Dapsone is a leukocyte inhibitor that can cause hemolysis in glucose-6-phos- phate-dehydrogenase (G6PD)-deficient patients and can produce methemoglobinemia. Screening for G6PD de- ficiency and monitoring hematocrits and systemic symp- toms are recommended during dapsone therapy. A dose of dapsone, 100 mg PO bid, given until the lesion heals or the erythema subsides has been suggested.*
Surgical excision of the lesion has been done but has no clear benefit. l 4 Electroshock therapy has been suggested for a number of envenomations, including Loxosceles, but has no scientific support. Stun-gun electroshock therapy was less effective than dapsone therapy for early brown recluse spider venom-induced necrotic skin lesions in a guinea pig m0de1.l~
Hyperbaric O2 (HBO) therapy has been investi- gated in an animal model. Improvement in histologic appearance and wound healing was s ~ g g e s t e d . ’ ~ . ’ ~ A pilot study of 14 patients who had brown recluse spider bites suggested benefit with HBO therapy for cutaneous loxoscelism. l9
An antivenom for cutaneous loxoscelism has been developed at Vanderbilt University and has undergone some testing. It is not generally available but may be useful before the necrotic lesion develops. Direct in- jection of the cutaneous site with IgG polyvalent an- tibody to the sphingomyelinase activity of the venom has been investigated.*”
The preceding discussion on the treatment for known recluse spider bites is directed at the cutaneous expres- sion of the bite. Managing the systemic manifestations of loxoscelism requires evaluation for hemolytic ane- mia, hemoglobinuria, acute renal failure, and DIC. Sys- temic loxoscelism rarely can result in severe sequelae and death. A laboratory screen consisting of a CBC and urinalysis for individuals with systemic symptoms is use- ful. Patients with normal laboratory findings can be treated on an outpatient basis with clinical assessment and a repeat screening laboratory follow-up within 24 - 48 hours.
The patient who develops any manifestation of sys- temic loxoscelism requires hospitalization and consid- eration for intensive care unit admission. Inpatient management should focus on conventional therapy for the given sequelae. The use of IV steroids in this setting has been reported but is controversial.
Clinical Pearls 1. The diagnosis of loxoscelism, whether localized or
systemic, is established clinically. There is no com- mercially available diagnostic test.
2. The primary manifestations of localized envenoma- tion are pain, lymphangitis, infectionlcellulitis, and necrotic ulcers.
3. Significant systemic manifestations of loxoscelism are hemolytic anemia, hemoglobinuria, renal failure, DIC, and death.
4. There is currently no “standard of care” for managing cutaneous loxoscelkm. Many treatment modalities are used but none are scientifically founded. The authors of this article recommend the use of dapsone.
5. The treatment for systemic loxoscelism is supportive care. The use of steroids in this setting is controversial.
Photograph Critique (by Phred Petersen) The value of color photographs is demonstrated in
this case as the pallor and ecchymosis described in the text are nicely seen. Suggestions to improve this series of photographs include: 1) Maintain constant viewpoint and magnification. Keeping a constant viewpoint throughout the series of photographs would make changes in the size and shape of the lesion easier to appreciate. Maintaining constant magnification could be accom- plished by taking all photographs at a specific magni- fication ratio (i.e., 1 : lO) as marked on the barrel of the lens. Including anatomic landmarks in the photograph would make the location of the lesion more apparent. 2) Placement of the light source to one side of the camera rather than on the lens axis would better dem- onstrate any elevation or relief of the lesion. 3) Inclu- sion of a scale at the plane of injury would make a series of photographs at a constant magnification possible, especially if the course of the disease necessitates a change in the magnification of the lens.
REFERENCES 1.
2.
3.
4.
5.
6. 7.
8.
9.
10.
Stewart CE. Bites and stings: arthropods. In: Stewart CE. En- vironmental Emergencies. Baltimore: Williams & Wilkins, 1990,
Rees RS, Campbell DS. Spider bites. In: Auerbach PS, Geehr EC (eds). Management of Wilderness and Environmental Emer- gencies (2nd ed). St. Louis: C. V. Mosby, 1986, pp 543-68. Wasserman GS, Siege1 C. Loxoscelism (brown recluse spider bite): a review of the literature. Clin Toxicol. 1979; 14:353-8. Berger RS. The unremarkable brown recluse spider bite. JAMA.
Ginsberg CM, Weinberg AG. Hemolytic anemia and multiorgan failure associated with localized cutaneous lesion. J Pediatr. 1988;
Prince GE. Arachnidism in children. J Pediatr. 1956; 49:101-8. Barrett SM, Romine-Jenkins M, Blick KE. Passive hemagglu- tination inhibition test for diagnosis of brown recluse spider bite envenomation. Clin Chem. 1993; 39:2104- 7. Russell FE, Gertsch WJ. Letter to the editor. Toxicon. 1983;
Duffey PH, Linbacher HP. Brown spider bites. Ariz Med. 1971;
Timchuk LD, Luchko AS, Palamarchok VN, et al. Hyperbaric oxygen in complex treatment of acute poisoning. In: Yefuny SN (ed). Proceedings of the 7th International Congress on Hyper- baric Medicine. Moscow: USSR Academy of Sciences, 1981, p 333.
pp 163 - 5 .
1973; 225: 1109- I l .
112:496-9.
21:337 - 9.
28:89 - 95.

Bite to Left Leg, Walker, Hogan 237
11. Rees RS, Shack RB, Withers E, Madden J, Franklin J , Lynch JB. Management of the brown recluse spider bite. Plast Reconstr Surg. 1981; 68:768- 73.
12. Rees RS. King LE. Treatment of brown recluse spider bites. J Am Acad Dermatol. 1986; 14:691-2.
13. Erickson T. Hryhorczuk DO. Brown recluse spider bites in an urban wilderness. J Wilder Med. 1990; 11258 - 64.
14. Rees RS, Altenbern DP, Lynch JB, King LE Jr. Brown recluse spider bite: a comparison of early surgical excision and dapsone and delayed surgical excision. Ann Surg. 1985; 20:2126- 30.
15. Osborn CD. Treatment of spider bites by high voltage direct current. 1 Okla State Med Assoc. 1991; 841257-60.
16. Barrett SM, Walker .IS, Romine-Jenkins M. Electrotherapy for venomous bites from snakes and spiders. J Okla State Med Assoc.
’
1992; 85:533-5.
17. Barrett SM. Romine-Jenkins M, Fisher DE. Dapsone or electric shock therapy of brown recluse spider envenomation? Ann Emerg Med. 1994; 24:21-5.
18. Strain GM, Snider TG, Tedford BL, Cohn GH. Hyperbaric oxy- gen effects on brown recluse spider (Loxosceles reclusa) enven- omation in rabbits. Toxicon. 1991; 291989- 96.
19. Maynor ML, Abt JL, Osborne PD. Brown recluse spider bites: beneficial effects of hyperbaric oxygen. J Hyperbaric Med. 1992; 7189- 102.
20. Rees RS. Campbell C, Rieger E, King LE. The diagnosis and treatment of brown recluse spider bites. Ann Emerg Med. 1987; 161945 - 9.