Embed Size (px)
Citation preview

Yongbaek Kim, DVM, PhD. Dipl. ACVP
Seoul National University, College of Vet. Medicine,
Laboratory of Clinical Pathology
Clinical Pathology for
Diagnosis of Equine Diseases

Clinical Pathology
Hematology (complete blood count, CBC)
Cellular components : RBC, WBC, Platelets
Proteins
Clinical Chemistry
Enzymology
Biomarkers
Fluid Analysis
Urinalysis
Abdominal and thoracic, CSF, Joint
Cytology
Mass
Tracheal and bronchial washing

Blood Sampling: Indications
Diagnosis of clinical disease
Infectious, parasitic
Specific organ dysfunction
Routine management
Routine neonatal foal examinations
Performance horse monitoring
Preanesthetic checks
Prepurchase examinations
Insurance examinations
Immunoglobulin G [IgG] tests for neonatal foals
Import/export examinations

Blood Sampling and Testing
Blood Testing
Complete Blood Count
Clinical Chemistry
Coagulation Tests
EDTA Heparin Serum Citrate

Blood Sampling
Accurately label with the horse's and owner's names
and the date of collection
Analyses should be performed as soon as possible
Some delay is inevitable
Prudent to carry samples in an insulated 'cool bin' (12 to
20°C) to avoid the deleterious effects of excessive
temperature fluctuations that may occur in a vehicle

Blood Sampling
Whole blood samples
Should not be refrigerated: results in hemolysis rendering
hematological tests and many serum enzyme analyses
inaccurate
Ideally, serum should be separated from clotted
samples as soon as practical
Centrifugation or simple standing and pipetting may be
used
Serum separation tubes
Once separated, serum or plasma may be refrigerated or
frozen for storage purposes

Blood Profiles
Profile type Profile content
36 hours Hematology, serum proteins, fibrinogen, PV, SAA, serum IgG
Weanling and
yearling
Hematology, serum proteins and electrophoresis, fibrinogen,
SAP,
serum calcium and phosphate, urine phosphate fractional
clearance ratios
Training horse Hematology, serum proteins and electrophoresis, PV,
fibrinogen, SAA, AST, CK, urine phosphate fractional
clearance ratios
Mature horse Hematology, serum proteins and electrophoresis, fibrinogen,
PV, SAA, AST, CK, GLDH, LD, SAP, IAP, GGT, urea,
creatinine
Basic Screen Hematology, Serum proteins, fibrinogen, AST, CK, GGT, SAP,
urea, creatinine AST Aspartate aminotransferase, CK Creatine kinase, GGT L-gamma glutamyl transferase,
GLDH Glutamate dehydrogenase, IAP Intestinal alkaline phosphatase, LD Lactate dehydrogenase,
PV Plasma viscosity, SAA Serum amyloid A, SAP Serum alkaline phosphatase

Blood Profiles
Profile type Profile content
Inflammatory
profile
Hematology, serum proteins, PV, fibrinogen, SAA
Liver profile Hematology, serum proteins and electrophoresis, fibrinogen,
PV, SAA, AST, GLDH, LD, SAP, IAP
Renal Hematology, Serum proteins, fibrinogen, Urea, Creatinine, Ca,
PO4
Muscle Hematology, AST, CK, Urea, Creatinine
Intestinal profile
Hematology, serum proteins and electrophoresis, fibrinogen,
PV, SAA, SAP, IAP
Electrolytes Na, K, Cl, Ca, PO4, Mg
Endocrine ACTH, insulin, Glucose, Triglycerides
AST Aspartate aminotransferase, CK Creatine kinase, GGT L-gamma glutamyl transferase,
GLDH Glutamate dehydrogenase, IAP Intestinal alkaline phosphatase, LD Lactate dehydrogenase,
PV Plasma viscosity, SAA Serum amyloid A, SAP Serum alkaline phosphatase

Complete Blood Count (CBC)
Hematology analyzer
•Cell counts
•Hemoglobin
•Cell parameters
Microhematocrit tube
•Packed cell volume
•Total plasma protein
•+/- fibrinogen
Blood smear
•WBC differential
•Confirm platelet
count
•Cell morphology
+/- Reticulocyte count
•Some hematology
analyzers can perform
•Only needed in anemic
patients

Erythrogram Hemoglobin** Red cell count** Hct MCV** MCH MCHC RDW Morphology
**Directly measured, all others calculated
Platelets Count** MPV** PDW Morphology
Leukogram TNCC (WBC count)** (Differential cell count) Morphology
Protein Total protein** Albumin** Globulin
Complete Blood Count (CBC)

Complete Blood Count (CBC)
Diseases Blood tests
Anemia Low red blood cell count, packed cell volume
and hemoglobin level
Hemoconcentration
/dehydration
Raised red blood cell count, packed cell
volume and hemoglobin level
Bacterial infections High white blood cell count and neutrophilia
Viral infections Low white blood cell count and neutropenia
during the acute phase
Parasitic or allergic
conditions
Eosinophilia in some cases

ANEMIA
Regenerative anemia
Acute blood loss, hemolytic anemia, and mild/moderate
intestinal parasitism
Reticulocytes: increased (some automated machine)
Macrocytic anemia
Non-regenerative anemia
Generalized bone marrow suppression, chronic inflammation,
neoplasia, chronic renal disease, or iron deficiency
Positive direct antiglobulin (Coombs) test
Diagnostic of immune-mediated anemia: idiopathic immune-
mediated anemia, neonatal isoerythrolysis and equine
infectious anemia.

LEUKOCYTOSIS
Physiological leukocytosis Excitement or stress
Increased blood pressure, heart rate and splenic contraction
Associated with intense exercise, fear or excitement
Transient, return to normal in an hour
Pathological leukocytosis with neutrophilia Infectious and non-infectious inflammation
Circulating immature neutrophils (ie, metamyelocyte and 'band' neutrophils)
Severe acute bacterial infections or septicemic processes
Toxic band cells: neonatal septicemia and adult colitis or enterotoxaemia

LEUKOPENIA
Increased emigration to inflamed tissues
Sequestration to highly vascular organs: pneumonia
Sequestration to body cavities: suppurative peritonitis
or pleuritis
Destruction in the microcirculation
Reduced neutrophil production in bone marrow
suppression: viral infections
Endotoxin shock: acute strangulation, intussusception,
salmonellosis, neonatal bacteremia and septicemia

LYMPHOCYTOSIS
Chronic viral infections
Chronic immune stimulation
Lymphoid neoplasia
May be dramatically elevated (as high as 100 x 109/l) in
cases of generalized lymphoma
None of these conditions consistently produces a
lymphocytosis.

EOSINOPHILIA
Antigen-antibody response in tissues rich in mast
cells
Skin, lung, gastrointestinal tract and female genital tract
Parasitism
Eosinophilic leukemia with eosinophil counts as
high as 2-5 x 109/l (25% on differential leucocyte
count).

THROMBOCYTOPENIA
Increased platelet destruction: immune-mediated
Primary or secondary to other diseases including
infections, neoplasia and drug treatments
Increased platelet usage: hemorrhage or trauma
Transient and reversible thrombocytopenia
DIC: severe and prolonged thrombocytopenia
EDTA-related pseudothrombocytopenia
Clumping of the platelets
Examination of extremities of the blood film
Heparinized or citrated blood should give normal platelet
numbers.

BLOOD BIOCHEMISTRY
Proteins
Plasma viscosity
Plasma fibrinogen
Serum enzymes
Other biochemical tests
Electrolytes

Proteins
Total proteins
Albumin
Globulin
Inflammatory proteins

Proteins: Albumin
Hyperalbuminemia: hemoconcentration and dehydration
Hypoalbuminemia: kidney, intestine, and liver diseases
Protein losing enteropathy: most common
Acute: salmonellosis or cyathostomiasis during the larval
emergence phase
Chronic: heavy cyathostomiasis or mixed large and small
stronglye burden, or a progressive infiltrative lesion of the
intestinal mucosa
Renal failure
Pigment-induced nephropathy, glomerulonephritis and
neoplasia
Liver failure: reduced production of albumin
Confirmed by increased serum liver enzymes and bile acids

Proteins: Globulin
alpha (α), beta (β) and gamma (ϒ) globulin fractions
α2-globulin: acute phase tissue proteins
elevated in acute inflammation and parasitism
(especially cyathostomiasis)
β1-globulin elevated in large and mixed strongyle
larval migration
β2-globulin raised in horses with hepatopathy
fibrinogen levels difficult in heparinized plasma samples

Proteins: Globulin
ϒ-globulin raised in response to antibody production
chronic infection or inflammation
Dramatic β2- or ϒ-globulin monoclonal 'spikes' in
cases with lymphoma or plasma cell myeloma
Hypogammaglobulinemia in neonatal foals with failed
passive immunity transfer
collected between 18 and 36 hours of age

Proteins: INFLAMMATORY PROTEINS
Serum amyloid A
sensitive, rapidly reacting, acute phase protein
help to detect early responses to infection and monitor the response to treatment
rises within hours and peaks at two days
Plasma fibrinogen
acute phase protein in horses with tissue damage
more chronic inflammation (eg, internal abscessation, chronic parasitism or infections)
crudely by subtraction of protein levels between fresh paired serum and plasma samples
direct coagulometry on a citrated blood sample
peak by 10 days and returns to normal slowly

Proteins: INFLAMMATORY PROTEINS

MUSCLE ENZYMES: AST, CK
Aspartate aminotransferase or serum glutamic-oxaloacetic aminotransferase (SGOT)
Rise in acute hepatopathy or myopathy peak at around 24 to 48 hour
return to baseline by 10 to 21 days
Creatine kinase (CK; creatine phosphokinase, CPK)
In acute myopathy, peak at six to 12 hours and return to baseline by three to four days
Exercise-induced myopathy
Serum before, and two to three hours after, submaximal exercise
Viral infections: EHV-1
clinical signs such as fatigue and stiffness.

SERUM ENZYMES: AST, CK

Cytoplasmic (“leakage or hepatocellular enzymes”) Enzymes are released from damaged cells or upon cell
death (necrosis)
AST (Aspartate aminotranferase, SGOT)
SDH (Sorbitol dehydrogenase)
GLDH (Glutamate dehyrogenase) ***ALT in horse: limited activity in liver
Induced (“cholestatic”) Enzymes are produced by cells (increased synthesis of an
enzyme)
GGT (gamma-glutamyl tranferase): preferable
ALP (alkaline phosphatase, “alk phos”, AP)
Hepatic Enzymes

Liver specific High concentration in liver but low in other tissues
Primarily in central lobular region
Mitochondrial rather than cytosolic
Released only with irreversible cell injury
Stable for a month at ~20C
More sensitive than SDH for liver diseases Valuable for the diagnosis of acute liver injury in horses
Limited availability of the assay in US
Cytoplasmic Enzymes: GLDH

SDH: less than 12 hours
SDH < GLDH <AST
AST: several days
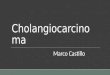
Hepatic Enzymes: Half-life
Reference Interval
SDH
AST & GLDH
2 10 6 4 8
Days after following severe Liver injury with recovery

Present in multiple tissues Relatively low in liver but liver ALP is found in serum Relatively high in intestine, but not in serum Bound to bile canalicular surface membranes
Serum ALP mainly from bone and liver Higher in growing horse: 100 fold greater than in adults Half life: about 3 days similar to GGT
Increased ALP by cholestasis Cholangitis, biliary cirrhosis, extrahepatic bile duct
obstruction
Hepatobiliary Enzymes: ALP

Most serum GGT activity originates from liver
Present high in liver, kidney, intestine and pancreas
Half life: about 3 days similar to ALP
Increased with cholestasis and biliary hyperplasia
GGT is more sensitive than ALP for cholestatic diseases
In horse with cholestasis: 9 fold increased GGT, 2-fold
in ALP
No significant difference in GGT activity pre and post
suckling colostrum
Hepatobiliary Enzymes: GGT

Hepatic diseases: Toxins
Pyrrolizidine alkaloids
Megalocytosis, periacinar necrosis, biliary hyperplasia,
periprotal fibrosis
Enzymes elevated before clinical signs
SDH, GLD may be within RI: chronic
Increased GGT and ALP

Hepatic diseases: Toxins
Mycotoxins (aflatoxins, fumonicin) Megalocytosis, centrilobular hepatocellular necrosis,
biliary hyperplasia
Increased SDH, GLD
Increased GGT and ALP: in chronic
Iron toxicosis Foals are more susceptible
Massive periacinar necrosis and deposition of iron in Kupffer cells
Ferrous fumarate or sulfate containing vitamin supplements
Increased SDH, GLD

Hepatic diseases: Infections
Tyzzer’s disease (Clostridium piliforme)
One to six week old foal- acute or peracute hepatitis
Death within hours or days
Multifocal to confluent centeral coagulation necrosis
with inflammatory cells
Filamentous bacteria within hepatocytes: Warthin starry
stain
Marked increase in SDH, moderate to marked
hyperbilirubinemia
Moderate increase in GGT; ALP is not increased

Hepatic diseases: Infections
Cholangiohepatitis
Ascending infection from the intestinal tract: Salmonella,
E.coli, Actinobacillus equuli, etc
Inflammation of biliary tract and adjacent liver
High GGT and ALP relative to SDH and GLD
Hyperglobulinemia in chronic (>3 weeks)
Cholelithiasis is frequent, possible due to decreased
biliary flow

Hepatic diseases: parasites
Parascaris equorum, strongyle larvae
Migrate through liver: hemorrhagic tract with
inflammatory cells (eosinophils), necrosis and fibrosis
Liver flukes (Fasciola hepatica)
Multifocal granuloma with eosinophilic and lymphocytic
inflammation
Elevated GLD and GGT three to five month post
infection

Renal Markers: Urea, Creatinine
Urea: By-product of protein metabolism
Increased by high protein diet or urea supplementation
Increased in fasting or prolonged excerecise:
catabolism
Decreased in protein poor diets or liver failure
Creatinine: By-product of muscle metabolism
Correlated with total muscle mass
Falsely increased in non-creatinine chromogens:
glucose, ketones, cephalosporin antibiotics
Falsely low in hyperbilirubinemia
BUN:creatinine ratio
Not useful to differentiate prerenal, renal, postrenal

Renal Markers: Electrolytes
Hyponatremia, hypochloremia, hyper- or
hypocalcemia, hypophosphatemia, hyper- or
hypokalemia, decreased or increased bicarbonate
Hypercalcemia: commonly in chronic renal failure
Hypocalcemia: commonly in acute renal failure

Renal diseases
ARF CRF Dehydration
Azotemia + + +
Urea/Creat >1:10 <1:10 Variable
USG 1.008 - 1.012 1.008 - 1.012 >1.035
Proteinuria + + _
Others Glycosuria Nonregenerative
anemia
Clinical signs
High FE HyperMg
Hyper Mg Hyperlipidemia
Enzymuria Hypoalbuminemia
Urine casts and
WBCs
Metabolic acidosis
Metabolic acidosis

Colic: Negative Prognostic Indicator
Adopted from Practical Guide to
Equine Colic, by Southwood

Thank you for your attention!!!