Embed Size (px)
Citation preview

Clinical Pathological Case Conference -
AnswerKristin Remus, D.O.Chief ResidentNYU School of Medicine, Internal MedicineAugust 8, 2008

Radiology
Review of Radiology showed the following Normal Chest x-ray Lung nodule on Chest CT Normal Abdominal CT




A diagnostic test was performed:
Endoscopy and Colonoscopy with biopsies





Further Studies
Stool contained Strongyloides Stercoralis larva
Endoscopic studies did not show stigmata of recent bleeding
Lab tests HIV negative Lymph node biopsy was not performed The patient had been offered screening
colonoscopy 1 year prior and declined. Biopsies negative for H. pylori

Additional Lab Results
Iron ug/dL 70 (42-146)
TIBC ug/dL 189 (250-450)
Ferritin ng/mL 186.7 (22-322)
Retic % 3.77 (0.5-1.55)Retic Index 2%
PSA ng/mL 0.44 (0-4)CEA ng/mL <0.5 (<=5)CA-125 U/mL 14.2 (<=35)AFP ng/mL 1.5 (0-10)Serum ACE U/L 19 (9-67)Serum immunofixation – faint bands in IgG, IgM, and Kappa are present against a dense, polyclonal background.
Purkinje Cell Ab - negativeHu immunoreactivity – negativeAnti-ganglioside IgM <1:800Anti-ganglioside IgG <1:100

Strongyloides Stercoralis
Tropical Asia, Africa, Latin America, Southern US, Eastern Europe
May persist asymptomatically in host for up to 65 years
Risk factors for clinical manifestation Chronic disease – Diabetes, Kidney Disease, Alcoholism Immunosuppression Hematologic malignancies Malnutrition HTLV-1 infection
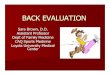
Diagnosis Parasite found in feces, sputum, duodenal aspiration, CSF,
tissue biopsy

infective larvae
SOIL
FECES
parthenogenesis
Strongyloides Life Cycle

Strongyloides Stercoralis Clinical Presentation
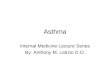
Skin larva currens
GI tract Cramps, diarrhea Malabsorption Rarely massive
hemorrhage Immunosuppressed
Fever Lungs
larvae in sputum
Many fatalities reportedCutaneous larva currens, “racing larva”

Stronglyoides Infection Immunosuppresion
Steroids may mimic endogenous parasitic-derived regulatory hormone
More eggs produced in the presence of exogenous steroids Hyperinfection
Disseminated infection Treatment
oral Ivermectin 200 ug/kg daily x 2 days, Albendazole as alternative
Prevention CDC recommends oral Ivermectin 200 ug/kg daily x 2 days
for prevention in immunosuppressed In a least one study, Thiabendazole was no more effective
than placebo

Chronic Acquired Demyelinating Polyneuropathy (CADP) A group of peripheral nerve disorders
Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) is a type of CADP
Peak incidence 40 to 60 years, male predominance
Pathophysiology unclear

CIDP Diagnostic Features
Symmetric proximal and distal muscle weakness +/- sensory loss Loss of deep tendon reflexes Progressive or relapsing Time course at least 2 months Diagnosis
Cerebral spinal fluid Albuminocytologic disassocation
Nerve conduction studies Biopsy

Concurrent Illness Variants of CIDP Several systemic disorders can occur with
CIDP HIV, Hep C Lymphoma, Myeloma, MGUS Inflammatory Bowel Disease Connective Tissue Diseases Diabetes Mellitus, Thyrotoxicosis Nephrotic Syndrome
Obligation to search for underlying cause

CIDP Clinical Course
Therapy IV Immunoglobulin (IVIg)
Repeated infusions, usually 1 course/month Corticosteroids
Starting dose 100 mg Prednisone per day Tapered with clinical improvement
Plasmapheresis Progression with IV IgG or Prednisone
Immunosuppressives Mycophenolate mofetil, Cyclosporine, Methotrexate

Acquired Ichthyosis
Acquired or Genetic Acquired usually due to drugs or systemic
disease Rhomboid, or fish-like, scales on the skin Symmetric, ranges in severity Primarily affects trunk, limbs, and extensor
surfaces Absence of inflammatory infiltrate with
hyperkeratosis is present on skin biopsy

Acquired Icthyosis Most commonly associated with Hodgkin’s Disease
or and non-Hodgkin’s lymphoma Also seen with
Transitional cell carcinoma, leiomyosarcoma, Kaposi’s Sarcoma, HCC, breast, lung, ovarian cancers
Dermatomyositis AIDS, HTLV-1 Sarcoidosis Thyroid disease Malnutrition/Malabsorption Cholesterol-lowering drugs such as Statins and Niacin
No report of association with Strongyloides Obligation to look for underlying cause

Final Diagnosis
Strongyloides Stercoralis
invading stomach Chronic Active Gastritis Innumerable sessile colonic
Polyps with tubulovillous adenoma and eosinophilic infiltrate

Acquired CIDP
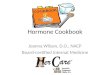
Proposed Pathogenesis
Acquired Icthyosis
?
Chronic Illness,Malnutrition
High DoseSteroids
AcquiredStrongyloides infection
GI BleedingGastritisAnemia
? Malabsorption
Disseminated Infection
? Polyp growth
Unknown disease process?

Follow Up
The patient was seen in Neurology clinic 3 weeks ago.
His symptoms have dramatically improved. The rash is also improving. He has had no further evidence of GI
bleeding. He will likely begin Azathioprine for his CIDP
once the Strongyloides infection is fully resolved.

Thank you!Dr. Martin BlaserDr. Charles Hazzi Dr. Herman YeeDr. Michael MacariDr. Emma RobinsonDr. Jonathan Ralston Dr. Philip TiernoDr. Gerald VillaneuvaDr. Malini SahuDr. Christina Yoon