Embed Size (px)
Citation preview

Resuscitation (2008) 76, 198—206
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate / resusc i ta t ion
CLINICAL PAPER
C.A.U.S.E.: Cardiac arrest ultra-sound exam—–A better approach to managing patients in primarynon-arrhythmogenic cardiac arrest!
Caleb Hernandeza, Klaus Shulera, Hashibul Hannana, Chionesu Sonyikaa,Antonios Likourezosa,!, John Marshall a,b
a Department of Emergency Medicine, Maimonides Medical Center, 4802 Tenth Avenue, Brooklyn, NY 11219, United Statesb Mount Sinai School of Medicine, One Gustave L. Levy Place, New York, NY 10029, United States
Received 23 February 2007; received in revised form 21 June 2007; accepted 25 June 2007
KEYWORDSAdvanced life support(ALS);Cardiac arrest;Cardiac tamponade;Hypovolemia;Pulmonary embolism;Pulseless electricalactivity (PEA);Tensionpneumothorax;Ultrasound
Summary Cardiac arrest is a condition frequently encountered by physicians in the hospitalsetting including the Emergency Department, Intensive Care Unit and medical/surgical wards.
This paper reviews the current literature involving the use of ultrasound in resuscitation andproposes an algorithmic approach for the use of ultrasound during cardiac arrest. At presentthere is the need for a means of differentiating between various causes of cardiac arrest, whichare not a direct result of a primary ventricular arrhythmia. Identifying the cause of pulselesselectrical activity or asystole is important as the underlying cause is what guides managementin such cases. This approach, incorporating ultrasound to manage cardiac arrest aids in thediagnosis of the most common and easily reversible causes of cardiac arrest not caused byprimary ventricular arrhythmia, namely; severe hypovolemia, tension pneumothorax, cardiactamponade, and massive pulmonary embolus. These four conditions are addressed in this paperusing four accepted emergency ultrasound applications to be performed during resuscitation ofa cardiac arrest patient with the aim of determining the underlying cause of a cardiac arrest.Identifying the underlying cause of cardiac arrest represents the one of the greatest challengesof managing patients with asystole or PEA and accurate determination has the potential toimprove management by guiding therapeutic decisions.
We include several clinical images demonstrating examples of cardiac tamponade, massivepulmonary embolus, and severe hypovolemia secondary to abdominal aortic aneurysm.
In conclusion, this protocol has the potential to reduce the time required to determine theetiology of a cardiac arrest and thus decrease the time between arrest and appropriate therapy.© 2007 Elsevier Ireland Ltd. All rights reserved.
! A Spanish translated version of the summary of this article appears as Appendix in the final online version at10.1016/j.resuscitation.2007.06.033.
! Corresponding author. Tel.: +1 718 283 6896; fax: +1 718 635 7274.E-mail address: [email protected] (A. Likourezos).
0300-9572/$ — see front matter © 2007 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.resuscitation.2007.06.033

C.A.U.S.E. in primary non-arrhythmogenic cardiac arrest 199
Introduction
Cardiac arrest is a condition frequently encountered byphysicians in the hospital setting including the Emer-gency Department, Intensive Care Unit and medical/surgicalwards. Since the implementation of preventative healthpolicy and ACLS, deaths from ventricular fibrillation andventricular tachycardia have decreased significantly, how-ever the prevalence of pulseless electrical activity (PEA) andasystole have increased.1 Unlike ventricular fibrillation andpulseless ventricular tachycardia where the pattern/rhythmof electrical activity is the focus of treatment rather thanthe underlying cause, PEA and asystole are corrected byaddressing the underlying cause.2 The importance of identi-fying a reversible underlying cause in these forms of cardiacarrest is of such importance that almost half of the ACLSfor experienced practitioners manual is dedicated to thistopic and its practical application.2 Hughes et al. provideda list of the etiologies of PEA in the order of frequency andease of reversal.3 He lists the top five conditions as hypoxia,hypovolemia, tension pneumothorax, pericardial tampon-ade, and pulmonary emboli. These conditions are potentiallyreversible, but the treatment is often invasive and may bedeadly if mistakenly applied to the wrong etiology.4 For thisreason accurate and timely diagnosis of the underlying causeis crucial. Currently the AHA recommends using physicalsigns and the patient’s history to guide the management ofPEA and asystole.2 However, physical examination can beunreliable and many physicians may withhold therapy for afear of causing harm if uncertain of the cause of cardiacarrest.4
Ultrasound is a diagnostic tool with increasing applica-tions and use in emergency situations.5 Levitt et al. haveobserved that emergency physicians had increased con-fidence in clinical decision-making when presented withdiagnostic ultrasonographic images of medical conditionsversus clinical impression and physical examination alone.6
Ultrasound examination has the potential to bring increaseddiagnostic clarity to clinical decision-making and aid in theidentification of a reversible cause for PEA or asystole.Recently many studies and case reports have examined theapplication of emergency ultrasound to cardiac arrest.6—15
Niendorff et al. observed that it was feasible for trainedemergency sonographers to obtain diagnostic images duringresuscitation of cardiac arrest patients and that obtainingsonographic images did not interfere with the resuscita-tion process.15 Other investigators have also made thisobservation.7,14,15 Many of these investigators have studiedthe application of ultrasound to one, or a few, causes of PEAand cardiac arrest; however a protocol that addresses themost common cardiac and pulmonary causes of PEA has notbeen developed.6—15
There remains a need for an organized and structuredapproach to non-arrhythmogenic cardiac arrest with suffi-cient diagnostic accuracy to justify appropriate aggressivelife-saving therapy. An effective protocol for emergencyultrasound evaluation in cardiac arrest patients wouldaddress the most likely and reversible causes; severe hypo-volemia, tension pneumothorax, cardiac tamponade, andpulmonary embolus. There is a body of literature support-ing the use of ultrasound as an accurate diagnostic aid inthe four above-mentioned conditions. The purpose of this
paper is twofold; first, to review the literature involvingultrasound and resuscitative conditions. Second, to proposea goal oriented approach to the cardiac arrest patient thatincorporates the use of ultrasound to address the most com-mon reversible causes of non-arrhythmia cardiac arrest. Thename of this new test is C.A.U.S.E., an acronym for cardiacarrest ultra sound examination, and whose name has theadded benefit of reminding the practitioner that the pri-mary goal of their effort in PEA or asystole should be toidentify and address the underlying cause. The protocol alsoserves to organize a process that can at times be chaoticand disorganized. Past studies have shown that increasedorganization during resuscitation increases the likelihoodof survival.16,17 A similar organizational protocol has beenused for the treatment of ventricular arrhythmias usingthree-lead electrocardiogram as a diagnostic tool with greatsuccess.1,2
Sonographic applications for cardiac arrest
Ultrasound has been used as an effective diagnostic tool dur-ing cardiac arrest and has identified causes of PEA. Theseinclude cardiac tamponade, severe hypovolemia, pulmonaryembolus, tension pneumothorax, and true asystole.
Cardiac tamponade
The use of ultrasound is widely accepted in the diagnosis ofcardiac tamponade in the form of identifying a pericardialeffusion during the FAST screening examination for trauma.Cardiac tamponade is more accurately identified by visual-izing pericardial effusion and right chamber collapse witheither of the parasternal views or the subxyphoid/costalview.14,15,18
Ultrasound is also highly accurate in diagnosing thiscondition. Mandavia et al., demonstrated that emergencyphysicians could diagnose the presence of pericardial effu-sion accurately when compared to a cardiologist with anoverall sensitivity of 96%, specificity of 98% and overall accu-racy of 97.5%.18
Currently the AHA recommends identifying neck veindistention and absence of pulse with CPR as diagnostic cri-teria for tamponade. However these features are sharedby tension pneumothorax as well. During cardiac arrest sit-uations it could be difficult to differentiate between thetwo conditions, as unequal breath sounds are difficult toappreciate in noisy or chaotic environments (i.e. emer-gency departments). Regularly using ultrasound to identifycardiac tamponade would add a greater level of accuracyto the determination of this cause for cardiac arrest andmay prevent the use of inappropriate therapy. Therapyfor cardiac tamponade is invasive (i.e. pericardiocentesisor open thoracotomy). Having a test that is available inreal time with greater accuracy than a physical examina-tion would be useful to physicians managing a patient incardiac arrest and reduce concerns of making a diagnos-tic and therapeutic error. Physical examination and historyremain important factors in medical decision-making, andtheir importance should not be neglected. There are caveatsthat should always be remembered when interpreting sono-graphic findings. For example patients in chronic renal

200 C. Hernandez et al.
Figure 1 Subxyphoid emergency ultrasound image of apatient with cardiac tamponade as a cause of PEA. Notice thepericardial effusion and right atrial collapse.
failure may have long standing pericardial effusions thatmay be unrelated to the cause of cardiac arrest (i.e.hyperkalemia), or patients who have trauma to the chestmay have minimal pericardial effusion but demonstrateclinical signs of tamponade. The characteristic emergencyultrasound image of cardiac tamponade is depicted above(Figure 1).
Hypovolemia
Hypovolemia is suggested by flattened right and left ventri-cles in the subxyphoid or long axis views of the heart,9,15
or by measuring left ventricular end-diastolic area from theshort axis parasternal view.19 Brown et al. reviewed liter-ature on the use of sonography to monitor hemodynamicstatus.19 He observed that left ventricular end-diastolic vol-ume correlated extremely well with blood loss (r = 0.96)and could significantly detect small changes in intravascu-lar volume by as little as 1.75 mL/kg in human subjectsand 5 mL/kg in pigs demonstrating that ultrasounds areuseful as an accurate tool to determine volume statusnoninvasively. Hendrickson et al. reports a case where ultra-
sound was used to diagnose hypotension as the cause ofPEA.9 He describes a patient with the characteristic signsof hypovolemia on cardiac sonogram and was found tohave a ruptured abdominal aortic aneurysm. The use ofultrasound in this case affected the patient’s care signifi-cantly.
Ultrasound of the inferior vena cava (IVC) can be a valu-able adjunct to cardiac imaging in the setting of cardiacarrest. IVC is measured in the sub-xiphiod space in the longaxis, using the liver as an acoustic window. There have beensome studies that have linked the IVC diameter to volumestatus and right ventricular pressure,20,21 demonstrating asensitivity and specificity of 88 and 81%, respectively,20 anda high degree of correlation between blood loss and IVCdiameter at r = 0.83.21 However, most of these studies wereperformed on patients with spontaneous respiration whichis not likely to be the case in the setting of cardiac arrestwhere positive pressure ventilation is routine. The authorsrecommend that in the setting of cardiac arrest a flat (IVCdiameter <5 mm) or collapsed IVC represents hypovolemiaand should prompt aggressive fluid resuscitation. On theother hand, a dilated IVC (IVC diameter >20 mm) in the set-ting of a cardiac arrest would be more consistent with pumpfailure from congestive heart failure, cardiac tamponadeor pulmonary embolism or may be as a result of cardiacarrest itself. In any case echocardiographic findings shouldbe correlated with clinical impression for a more educatedresuscitative plan.
Ultrasound to diagnose hypovolemia in the presence ofPEA adds increased diagnostic clarity, speed and accuracy,and may decrease the use of unnecessary, time-wastingand potentially harmful empiric therapy (i.e. thrombolyt-ics for suspected massive PE in the setting of true aorticaneurysm rupture). A characteristic emergency ultrasoundimage of the heart in hypovolemia may be viewed bel-low (Figure 2). There is also an ultrasound of imagedemonstrating the cause of this hypovolemia in the samepatient as Picture 2, a ruptured abdominal aortic aneurysm(Figure 3).
Figure 2 Subxyphoid emergency ultrasound image of apatient with hypovolemia as the cause of PEA. Patient wasactively being resuscitated with two large bore central venouscatheters at time of image acquisition.

C.A.U.S.E. in primary non-arrhythmogenic cardiac arrest 201
Figure 3 Sonographic evaluation of the aorta in a patientfrom Figure 2. This abdominal aortic aneurysm was identifiedas the cause of this patient’s hypovolemia and PEA.
Pulmonary embolus
Pulmonary embolus has been observed to be the direct causeof almost 5% of cardiac arrests, with PEA being the initialdiagnostic rhythm in 63% and asystole in another 32% ofthese cases.22 It has also been observed that in patientspresenting with cardiac arrest as a consequence of acutepulmonary emboli, thrombolytic therapy resulted in a sig-nificantly higher return of spontaneous circulation whencompared to similar patients who did not receive throm-bolytic therapy, 81% versus 43%, respectively.22 Thereforehaving a diagnostic tool with the potential of directingthrombolytic therapy in patients in cardiac arrest as a con-sequence of pulmonary emboli has the potential to greatlyimpact outcomes in this patient population.
Pulmonary embolus is identified sonographically by thefinding of an engorged right ventricle with a flattened leftventricle.4,7,15 There are a few reports of the use of car-diac ultrasound in the setting of cardiac arrest. MacCarthyet al. described a case where a 25-year-old woman experi-enced cardiac arrest due to massive pulmonary embolus.4
The above findings were recognized on cardiac ultrasoundand the patient was given appropriate management, leadingto the eventual discharge of the patient from the hospi-tal. Similarly Tovar et al. describes a similar case wheretransthoracic ultrasound was used to diagnose pulmonaryembolism in a 61-year-old man.7 In this case embolectomywas performed and the patient was discharged form thehospital to live a normal life. Both of these case reportsillustrate that sonographic diagnosis of massive pulmonaryemboli allow physicians the confidence to employ aggressivelife-saving therapy that may have not been used or reluc-tantly used in the face of diagnostic uncertainty, due to thefear of potential catastrophic negative outcome.
The use of transthoracic ultrasound to diagnose pul-monary emboli has been studied as well in patients notexperiencing cardiac arrest. Nazeyrollas et al. performeda prospective study in 70 patients with suspected acutepulmonary emboli, he found that right sided enlargementin this patient population demonstrated a sensitivity of0.70 and a specificity of 0.86 for diagnosing acute pul-monary emboli when a threshold of 25 mm was used.23
Miniati et al. performed a prospective study in 110 consec-utive patients with suspected pulmonary emboli; he foundthat echocardiographic criteria for PE demonstrated a sen-sitivity of 56% and specificity of 90%.24 Similarly Jacksonet al. evaluated patients prospectively with suspected pul-monary emboli and found that ultrasound had a sensitivityof 0.41 and specificity of 0.91.25 Torbicki and Pruszczykreviewed the available literature on the use of ultrasoundto diagnose acute pulmonary emboli and found that car-diac ultrasound has specificity between 81 and 94%, witha positive predictive value of 71—86%.26 These data allindicate that ultrasound has poor to moderate sensitivityas a routine screening test in all patients with suspectedpulmonary emboli. However cardiac ultrasound has demon-strated good to excellent specificity at detecting acutepulmonary emboli, which may be more important and appro-priate in the setting of cardiac arrest, where the need forspecific therapy must be justified.
After reviewing the available literature on the useof echocardiography in the diagnosis of acute pulmonaryemboli Lebowitz recommended that ultrasound had thepotential to make the greatest clinical impact in patientswith central hemodynamically significant pulmonary emboli(i.e. those capable of causing cardiac arrest) versus themajority of patients with small peripheral pulmonaryemboli.27 This recommendation is logical as echocardio-graphic findings of pulmonary embolus begin to be evidentafter acute obstruction of more than 30% of the pul-monary arterial bed.26 Ultrasound therefore appears to bean excellent bedside test for detecting the presence of largepulmonary emboli capable of causing cardiac arrest.
A characteristic four-chamber apical view of the heartof a patient with massive pulmonary embolus is demon-strated below (Figure 4). A CT-scan image of the samepatient demonstrating a large saddle pulmonary embolus ispresented as well (Figure 5).
Tension pneumothorax
Tension pneumothorax is identified sonographically byabsence of ‘‘sliding sign’’ between the visceral and pari-etal pleura when viewed anteromedially at the level ofthe second intercostal interspace and the mid clavicu-lar line. This approach was used by Knudtson et al. intrauma patients 28 and provides the ability to diagnosepneumothorax in as little as 30 s with a sensitivity of92.3%, specificity of 99.6%, and positive predictive valueof 92.3% and accuracy of 99.3%.28 Other studies haveachieved equally impressive accuracies using ultrasound forthe detection of pneumothorax.29,30 This high level of accu-racy in both ruling pneumothorax in or out could greatly aidphysicians in managing cardiac arrest. A protocol address-ing the pulseless patient should address pneumothorax, as it

202 C. Hernandez et al.
Figure 4 Four-chamber apical view of the heart in patientwith suspected pulmonary embolus. Notice the massive enlarge-ment of both right chambers when compared to the left side ofthe heart.
Figure 5 CT angiogram of the chest in a patient from Figure 4,obtained 1 h after initial ultrasound image. Notice the largesaddle pulmonary embolus. As a result of interventions startedafter initial emergency ultrasound patient survived and was dis-charged from the hospital.
Figure 6 Diagram comparing relative sizes of the cardiac chambers (apical four-chamber view) in cardiac tamponade, pulmonaryembolus, and hypovolemia to that of a normal heart. Please note that this diagram represents images obtained with normalemergency room probe setting, if using cardiac setting the diagram is flipped to its mirror image. Please see Figure 4 for anexample.

C.A.U.S.E. in primary non-arrhythmogenic cardiac arrest 203
is a common problem and readily reversible. Ultrasound hasbeen demonstrated to be a highly accurate diagnostic aid forpneumothorax, and could be of great use in a cardiac arrestsituation where ambient noise may affect the accuracy ofauscultation via stethoscope. Furthermore the high degreeof accuracy afforded by ultrasound assists in differentiat-ing between cardiac tamponade and tension pneumothorax,both of which present with similar clinical features.
True asystole
Ultrasound has also been useful in distinguishing true asys-tole from other types of cardiac arrest. Cardiac standstillor true asystole is identified by complete absence of anymotion in the heart including the valves, atria or ventricles31 and is often seen in association with severe spontaneousecho contrast. Blaivas et al. observed that cardiac stand-still in the emergency department had a positive predictivevalue of 100% for death in the emergency department.13
Salen et al. made similar observations in his study.31 Salenobserved that none of the patients with absence of car-diac kinetic activity on sonogram had spontaneous return ofcirculation. However, evidence of kinetic activity on sono-graphic evaluation of the heart was associated with returnof spontaneous circulation. This knowledge may be usefulfor physicians, allowing them to make decisions regardingthe value of continued resuscitative efforts. There appearsto be justification for terminating resuscitative efforts ifno cardiac motion is detected on cardiac ultrasound afteradequate resuscitative efforts were employed.
C.A.U.S.E.
C.A.U.S.E. is a new approach developed by the authors. TheC.A.U.S.E. protocol addresses four leading causes of cardiacarrest and achieves this by using two sonographic perspec-tives of the thorax; a four-chamber view of the heart andpericardium and anteromedial views of the lung and pleuraat the level of the second intercostal space at the midclavic-ular line bilaterally. The four-chamber view of the heart andpericardium is attained using either the subcostal, paraster-nal or apical thoracic windows. This allows the individualperforming the examination to select the most adequateview depending on the patients’ anatomy. The authors rec-ommend beginning with the subcostal view first as this viewmakes it possible for the practitioner to evaluate the heartwithout interrupting chest compression.9 If this view is notpossible then the apical or parasternal approaches may beused during coordinated pulse checks lead by the resus-citation team leader. A four-chamber view is used in thisprotocol as it allows for ease of comparison between thedifferent chambers in the heart, facilitating the diagnosis ofhypovolemia, massive PE, and cardiac tamponade (Figure 6).Pneumothorax is diagnosed by identifying the lack of slid-ing sign and comet-tail artifact while looking in the sagitalplane at the second intercostal space of the midclavicu-lar line (Figure 7). For both the cardiac and lung views itis recommended to use a 2.5—5.0 phased array transducerprobe. This allows the examiner to use the same probefor both lung, heart and if needed abdominal exam. Thistype of probe was used by Knudtson in his study involving
Figure 7 Diagram demonstrating ultrasound findingsobserved in pneumothorax and comparing these to findings ofnormal lung.
ultrasound for the use of identifying pneumothorax as anaddition to the FAST exam, and it yielded very a high accu-racy in detecting pneumothorax,28 yet still remained usefulin identifying the heart and abdominal organs. The proto-col is best described in diagram form (Figure 8). Pulselesspatients are treated with standard resuscitative protocol.After the monitor is attached patients are divided intotwo groups: arrhythmogenic (i.e. ventricular fibrillation andventricular tachycardia) and non-arrhythmogenic (i.e. mas-sive PE, hypovolemia, tension pneumothorax, etc.) cardiacarrest. Arrhythmogenic patients are treated with electri-cal cardioversion, but non-arrhythmogenic patients are thenexamined with the C.A.U.S.E. protocol to exclude readilyreversible causes for the cessation of the circulation.
The cardiac view is the first performed as this gives thepotential to diagnose one of the three conditions in a singleview (massive PE, cardiac tamponade, and hypovolemia),and this view takes the least time, meaning less interferencewith resuscitation as possible. If the results of the cardiacview are inconclusive the pulmonary views are attemptedas these use approximately 30 s per side and diagnose onlyone condition, pneumothorax. If these studies are negativealternate causes of the arrest are considered as described by

204 C. Hernandez et al.
Figure 8 Flow diagram demonstrating use of C.A.U.S.E. protocol in patients with cardiac arrest.
Figure 9 Characteristic image of IVC diameter in a patientwithout hypovolemia.
Figure 10 Characteristic image of IVC diameter in a patientwith hypovolemia.
C.A.U.S.E. in primary non-arrhythmogenic cardiac arrest 205
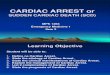
Figure 11 High quality subcostal image using newer bedsideultrasound equipment, demonstrating enlarged right ventricleand collapsed left ventricle in a patient with confirmed pul-monary embolism. Compare quality of newer machines withimage from Figure 4.
Hughes in order of frequency and ease of reversibility (i.e.electrolyte and metabolic disturbance, massive hypother-mia, massive myocardial infarction, and drugs or toxins).3
If one encounters an abnormal image on examination of thefour chambers of the heart, one may attempt further con-firmatory views with the ultrasound to make the diagnosismore clear (i.e. the finding of collapsed right and left ven-tricles should be followed by sonographic evaluation of theIVC and abdominal aorta) (Figures 9 and 10).
Conclusion
Ultrasound is currently the only radiographic modality withthe potential to guide management in real time, at thebedside, during cardiac arrest without interfering withresuscitation. This literature review justifies the need forfurther study of ultrasound in the setting of cardiac arrestand also demonstrates that implementation of sonographyinto patient-care provides substantial potential benefits topatients and clinicians alike. As technology and trainingimprove it will become easier to incorporate ultrasound intothe care of patients in need of resuscitation (Figure 11). Thereviewers included a proposed protocol to add organizationand structure to a clinical scenario that has the potentialfor chaos. The protocol is an attempt to incorporate themost clinically relevant information in the literature on theapplications of ultrasound use for cardiac arrest in an orga-nized manner for clinical application. The hope is that thisprotocol will foster future study in the area of sonographicdiagnosis during cardiac arrest, and eventually reduce thetime required for emergency providers to determine the eti-ology of a cardiac arrest and thus decrease the time betweenarrest and appropriate therapy.
Conflict of interest
None.
References
1. Parish DC, Dinesh Chandra KM, Dane FC. Success changes theproblem: why ventricular fibrillation is declining, why pulse-less electrical activity is emerging, and what to do about it.Resuscitation 2003;58:31—5.
2. Cummins RO, editor. ACLS provider manual, 2001. Dalas, TX:American Heart Association; 2002. p. 97—8.
3. Hughes S, McQuillan PJ. Sequential recall of causes of electro-mechanical dissociation (EMD). Resuscitation 1998;37:51.
4. MacCarthy P, Worrall A, McCCarthy G, Davies J. The use oftransthoracic echocardiogram to guide thrombolytic therapyduring cardiac arrest due to massive pulmonary embolism.Emerg Med J 2002;19:178—9.
5. Legome E, Pancu D. Future applications for emergency ultra-sound. Emerg Med Clin North Am 2004;22:817—27.
6. Levitt MA, Jan BA. The effect of real time 2D-echocardiographyon medical decisionmaking in the emergency department. JEmerg Med 2002;22:229—33.
7. Tovar EA, Borsari A, Kunelis CT, Song M. Diagnosis of fulmi-nant pulmonary embolism by transthoracic echocardiogram. TexHeart Inst J 1997;24:68—70.
8. Knowles P. Transthoracic echocardiography during cardiacarrest due to massive pulmonary embolism. Emerg Med J2003;20:395—6.
9. Hendrickson RG, Dean AJ, Costantino TG. A novel use ofultrasound in pulseless electrical activity: the diagnosis ofan acute abdominal aortic aneurysm rupture. J Emerg Med2001;21:141—4.
10. Hilty WM, Hudson PA, Levitt MA, Hall BJ. Real-time ultrasound-guided femoral veincatheterization during cardiopulmonaryresuscitation. Ann Emerg Med 1997;29:331—7.
11. Bocka JJ, Overton DT, Hauser A. Electromechanical dissociationin human beings: an echocardiographic evaluation. Ann EmergMed 1988;17:450—2.
12. Varriale P, Maldonado J. Echocardiographic observations dur-ing inhospital cardiopulmonary resuscitation. Crit Care Med1997;25:1717—20.
13. Blaivas M, Fox JC. Outcome in cardiac arrest patients found tohave cardiac standstill on the bedside emergency departmentechocardiogram. Acad Emerg Med 2001;8:616—21.
14. Tayal VS, Kline JA. Emergency echocardiography to detectpericardial effusion in patients in PEA and near-PEA states.Resuscitation 2003;59:315—8.
15. Niendorff DF, Rassias AJ, Palac R, et al. Rapid cardiac ultra-sound of inpatients suffering PEA arrest preformed by nonexpertsonographers. Resuscitation 2005;67:81—7.
16. Weng TI, Huang CH, Ma MH, et al. Improving the rate of return ofspontaneous circulation for out-of-hospital cardiac arrests witha formal, structured emergency resuscitation team. Resuscita-tion 2004;60:137—42.
17. Andreasson AC, Herlitz J, Bang A, et al. Characteristics andoutcome among patients with a suspected in-hospital cardiacarrest. Resuscitation 1998;39:23—31.
18. Mandavia DP, Hoffner RJ, Mahaney K, Henderson SO. Bedsideechocardiography by emergency physicians. Ann Emerg Med2001;38:377—82.
19. Brown JM. Use of echocardiography for hemodynamic monitor-ing. Crit Care Med 2002;30:1361—4.
20. Kircher B, Himelman R, Schiller N. Noninvasive estimation ofright atrial pressure from the inspiratory collapse of the IVC.Am J Cardiol 1990;66:493—6.
21. Lyon M, Blaivas M, Brannam L. Sonographic measurement of theinferior vena cava as a marker of blood loss. Am J Emerg Med2005;23:45—50.
22. Kurkciyan I, Meron G, Sterz F, et al. Pulmonary embolism as acause of cardiac arrest. Arch Inter Med 2000;160(10):1529—35.

206 C. Hernandez et al.
23. Nazeyrollas P, Metz D, Maillier B, et al. Transthoracicechocardiography and diagnosis of acute pulmonary embolism.Change in the diagnostic value with respect to thresh-olds of classification. Arch Mal Coeur Vaiss 1997;90(4):463—9.
24. Miniati M, Monti S, Pratali L, et al. Value of transthoracicechocardiography in the diagnosis of pulmonary embolism:results of a prospective study in unselected patients. Am J Med2001;110(7):528—35.
25. Jackson RE, Rudoni RR, Hauser AM, Pacaul RG, Hussey ME.Prospective evaluation of two-dimesional transhtoracicechocardiography in emergency department patientswith suspected pulmonary embolism. Acad Emerg Med2000;7(9):994—8.
26. Torbicki A, Pruszczyk P. The role of echocardiography in sus-pected and established PE. Semin Vasc Med 2001;1(2):165—74.
27. Leibowitz D. Role of echocardiography in the diagnosis andtreatment of acute pulmonary thrmboembolism. J Am SocEchocardiogr 2001;14(9):921—6.
28. Knudtson JL, Dort JM, Helmer SD, Smith RS. Surgeon-preformedultrasound for pneumothorax in the trauma suite. J Trauma2004;56:527—30.
29. Dulchavsky SA, Schwarz KL, Kirkpatrick AW, et al. Prospectiveevaluation of thoracic ultrasound in the detection of pneumoth-orax. J Trauma 2001;50:201—5.
30. Kirkpatrick W, Sirois M, Laupland KB, et al. Hand-held tho-racic sonography for detecting post-traumatic pneumothoraces:the extended focused assessment with sonography for trauma(EFAST). J Trauma 2004;57:288—95.
31. Salen P, Melniker L, Chooljian C, et al. Does the presence orabsence of sonographically identified cardiac activity predictresuscitation outcomes of cardiac arrest patients? Am J EmergMed 2005;23:459—62.