Embed Size (px)
Citation preview
Clinical Outcomes, Quality of Life, and DiagnosticUncertainty in the First Year of PolymyalgiaRheumaticaANDREW HUTCHINGS,1 JANE HOLLYWOOD,2 DONNA L. LAMPING,1 COLIN T. PEASE,3
KUNTAL CHAKRAVARTY,4 BARBARA SILVERMAN,5 ERNEST H. S. CHOY,6 DAVID G. I. SCOTT,7
BRIAN L. HAZLEMAN,5 BRIAN BOURKE,8 NAGUI GENDI,9 AND BHASKAR DASGUPTA2
Objective. To evaluate the impact of polymyalgia rheumatica (PMR) on clinical outcomes and quality of life (QOL); therelationship between laboratory measures and clinical outcomes, and changes in QOL; and agreement between rheuma-tologists in confirming the initial diagnosis.Methods. We conducted a prospective study of 129 participants in 8 hospitals in England who met a modified version ofthe Jones and Hazleman criteria and had not started steroid therapy. The main outcome measures were response tosteroids after 3 weeks (minimum 50% improvement in proximal pain, morning stiffness <30 minutes, acute-phaseresponse not elevated), relapses, QOL as measured by the Short Form 36 and Health Assessment Questionnaire, anddiagnosis reassessment at 1 year.Results. At 3 weeks, 55% of participants failed to meet our definition of a complete response to steroid therapy. Bothphysical and mental QOL at presentation were substantially lower than general population norms and improved by 12.6(95% confidence interval [95% CI] 10.8, 14.4) and 11.2 (95% CI 8.5, 13.8) points, respectively, at 1 year. Proximal pain andlonger morning stiffness were significantly associated with lower physical QOL during followup, whereas erythrocytesedimentation rate was most strongly associated with lower mental QOL during followup. There was moderate agreementbetween clinicians in confirming the PMR diagnosis (kappa coefficients 0.49–0.65).Conclusion. PMR is a heterogeneous disease with a major impact on QOL. Ongoing monitoring should include diseaseactivity based on symptoms, emergence of alternative diagnoses, and early referral of atypical and severe cases.
KEY WORDS. Polymalgia rheumatica; Quality of life; Treatment outcome; Diagnosis.
INTRODUCTION
Polymyalgia rheumatica (PMR), a common inflammatorycondition of elderly persons, is characterized by proximalpain and morning stiffness, an acute-phase response, and a
rapid response to steroids. In the UK, the age-adjustedincidence of diagnosed PMR increased by 35% between1990 and 2001 (from 6.9 to 9.3 per 10,000 person-years)(1). Patients with PMR are rarely referred to secondary care
Supported by the NHS Executive Eastern Research andDevelopment (project grant HSR/0500/9).
1Andrew Hutchings, MSc, Donna L. Lamping, PhD: Lon-don School of Hygiene & Tropical Medicine, London, UK;2Jane Hollywood, BA, Bhaskar Dasgupta, MD, FRCP: Sou-thend University Hospital NHS Foundation Trust, Essex,UK; 3Colin T. Pease, MD, FRCP: Leeds Teaching HospitalsNHS Trust, Leeds, UK; 4Kuntal Chakravarty, FRCP: Bark-ing, Havering, and Redbridge Hospitals NHS Trust, Essex,UK; 5Barbara Silverman, FRCP, Brian L. Hazleman, FRCP:Cambridge University Hospitals NHS Foundation Trust,Cambridge, UK; 6Ernest H. S. Choy, MD, FRCP: King’s Col-lege London, London, UK; 7David G. I. Scott, MD, FRCP:Norfolk and Norwich University Hospital NHS Trust, Nor-wich, UK; 8Brian Bourke, FRCP: St George’s HealthcareNHS Trust, London, UK; 9Nagui Gendi, FRCP: Basildon andThurrock University Hospitals NHS Foundation Trust, Es-sex, UK.
Dr. Chakravarty has received speaking fees (less than$10,000) from Aventis and honoraria from Aventis andMerck Sharp and Dohme. Dr. Choy has received consultingfees and/or honoraria (less than $10,000 each) from Abbott,Allergan, Bristol-Myers Squibb, Chelsea Therapeutics,GlaxoSmithKline, Jazz Pharmaceuticals, Merrimack, MerckSharp and Dohme, Pfizer, Pierre Fabre, Schering-Plough,UCB, Celltech, and Wyeth. Dr. Bourke has given experttestimony in various medical negligence and personal in-jury litigation cases.
Address correspondence to Bhaskar Dasgupta, MD,FRCP, Consultant Rheumatologist and Honorary Professor,Essex University, Department of Rheumatology, SouthendUniversity Hospital NHS Foundation Trust, PrittlewellChase, Westcliff-on-sea, Essex SS0 0RY, UK. E-mail:[email protected].
Submitted for publication August 25, 2006; accepted inrevised form November 17, 2006.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 57, No. 5, June 15, 2007, pp 803–809DOI 10.1002/art.22777© 2007, American College of Rheumatology
ORIGINAL ARTICLE
803

(1) and PMR is a common indication for long-term steroiduse in the community (2).
There is uncertainty regarding diagnosis and outcomesin PMR. Initial features vary, e.g., PMR without an ele-vated erythrocyte sedimentation rate (ESR) (3), and com-mon mimicking conditions can present with the polymy-algic syndrome (4). There is no gold standard test andseveral diagnostic criteria have been used (5–8). This mayexplain the lack of agreement in PMR diagnoses betweenprimary care physicians and rheumatologists (9–11) andthe revision of diagnoses in 5–23% of patients with long-term followup (12–14).
A rapid resolution of symptoms with steroid therapy isconsidered a diagnostic hallmark (15). Lack of responsemay indicate an incorrect diagnosis (16). There is littleevidence on what constitutes a typical response and how itrelates to longer-term outcomes or revisions of the initialdiagnosis. A study of 27 patients proposed 3 categories ofdisease course: a rapid response without significant re-lapse, a rapid response requiring extended treatment, andincomplete resolution of symptoms requiring extendedsteroid treatment (17). Accurate disease assessment andpatient-based outcomes are critical to balance the benefitsversus serious adverse outcomes of steroid therapy (18).To date, no studies have considered the impact of PMR onquality of life (QOL). The goals of this study were 1) toevaluate the impact of PMR, particularly the initial re-sponse to steroid therapy, on clinical outcomes and QOLin the first year; 2) to examine the relationship betweenlaboratory measures and clinical outcomes, and changes inQOL; and 3) to evaluate agreement between rheumatolo-gists in confirming the initial diagnosis of PMR after 1 yearof followup.
PATIENTS AND METHODS
Participants were recruited from 8 rheumatology clinics inEngland. General practitioners agreed to refer suspectedPMR cases prior to steroid therapy. Eligibility criteria weretypical clinical features of PMR using a modified versionof the Jones and Hazleman criteria (6). These clinical fea-tures included primarily muscular shoulder and/or pelvicgirdle pain in the absence of true muscle weakness, morn-ing stiffness �30 minutes, ESR �30 mm/hour, and ab-sence of mimicking diseases. Ethical approval was re-ceived from the Trent Multicentre Research EthicsCommittee (reference MREC/00/4/041) and all relevantlocal research ethics committees. All participants pro-vided informed written consent. Exclusion criteria wereother connective tissue disorders; advanced osteoarthritisof the shoulder, hip, or knee; systemic infection; abnormallevels of serum creatine kinase or thyroid-stimulating hor-mone; clinical features of giant cell arteritis (GCA; head-aches, jaw claudication, visual symptoms, and scalp ten-derness); or prior steroid therapy.
Patients received conventional steroid therapy with 15mg oral prednisolone following a tapering schedule of 12.5mg at 3 weeks, 10 mg at 6 weeks, 9 mg at 3 months, 8 mgat 4 months, and a 1-mg reduction every 2 months. Devi-ations from the treatment schedule could be made at thediscretion of the clinician.
Clinical, demographic, and laboratory data, includingESR and C-reactive protein (CRP) level, were collectedbefore starting steroid treatment. We assessed QOL at base-line, 3 months, and 12 months using the modified HealthAssessment Questionnaire (HAQ) (19) and the physicalcomponent summary score (PCS) and mental componentsummary score (MCS) of the Short Form 36 Health Survey(SF-36) UK version 2 (20). Data on PMR symptoms, labo-ratory measures, and adverse events were collected at 3weeks, 6 weeks, 3 months, 6 months, and 12 months.
We examined the initial response based on 3 compo-nents (proximal pain, morning stiffness, and acute-phaseresponse) of the Jones and Hazleman criteria (6) at theweek 3 assessment. A complete response was defined asno pain or at least a 50% improvement in pain in theshoulders and pelvic girdle on a visual analog scale (VAS),morning stiffness no longer than 30 minutes, ESR nohigher than 30 mm/hour, and CRP level no higher than 10mg/dl. A relapse was defined as a return of PMR symptomsrequiring an increase in steroid dose or maintenance of thesteroid dose beyond a scheduled reduction.
After the 12-month followup, each clinician rated thelikelihood of PMR being the correct diagnosis using a5-point scale (where 1 � definitely PMR and 5 � definitelynot PMR). In the absence of any criteria for confirming aPMR diagnosis on followup, we relied on individual ex-pert judgment. Two authors (rater 1 and rater 2), blinded tothese ratings, independently reviewed all patients’ base-line and followup data and provided their own ratingsusing the same scale. A third author was substituted whereindependent raters would otherwise assess their own pa-tients (5 patients for rater 1, 3 patients for rater 2).
Statistical analysis. To evaluate agreement betweenrheumatologists in confirming the PMR diagnosis, we usedquadratic-weighted kappa coefficients (�w) to estimatechance-corrected agreement. Patients were considered un-likely to have had PMR if the clinician and/or both inde-pendent raters gave ratings of 4 or 5. Rates of crude agree-ment were estimated after dichotomizing the ratings (1–3 � likely PMR, 4–5 � unlikely PMR).
To examine the impact of changes in laboratory andclinical measures of disease activity on changes in QOLduring followup, we used general estimating equations, amultivariate regression technique for analyzing correlatedlongitudinal data with repeated measurements (21). Theindependent variables of interest were ESR, CRP level,duration of morning stiffness, and presence of proximalpain at the 3- and 12-month assessments. The impact ofeach independent variable on changes in the 3 QOL mea-sures was first evaluated separately using an exchangeablecorrelation structure with adjustment for the relevant base-line QOL score and potential confounding variables (age,sex, socioeconomic status [22], comorbidity index [23],ESR, CRP level, morning stiffness, and peripheral involve-ment [hand edema, pain, or restriction of active or passivemovements] at baseline). The 4 independent variables ofinterest were added manually to the model in a forwardstepwise manner using a threshold of P less than 0.05 forretention in the model. These analyses excluded partici-
804 Hutchings et al
pants considered unlikely to have had PMR by the 12-month followup assessment, although the impact of in-cluding these participants in the analyses was examined.
RESULTS
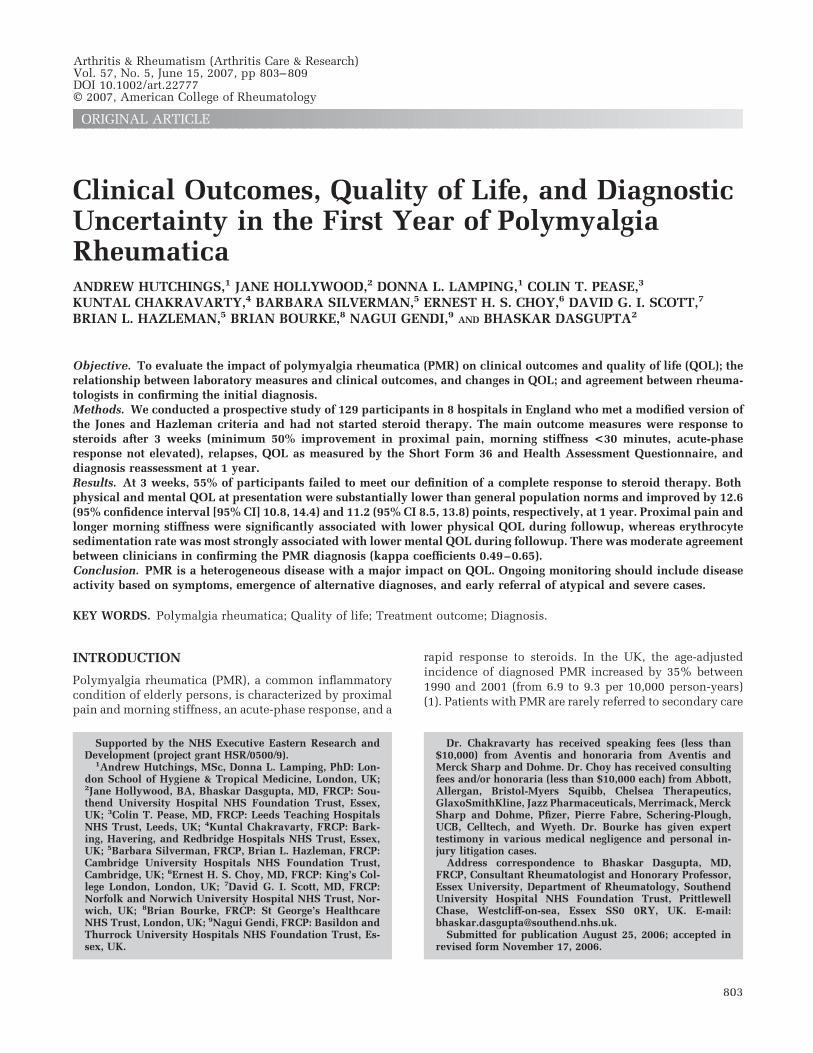
Between July 2001 and May 2003 we screened 249 patientswith suspected PMR, of whom 218 were referrals fromgeneral practice. We recruited 129 patients who met theeligibility criteria and provided informed, written consent(Figure 1). The mean age of patients was 70.9 years (range52–92 years), 77 (59.7%) were women, 3 (2.3%) werenonwhite, and the median duration of PMR symptoms atpresentation was 12 weeks (interquartile range 6–17).There were 43 (33%) patients with peripheral involvement(hand/wrist pain, joint involvement, or edema). Six pa-tients started treatment with prednisolone doses �15 mg(range 5–12.5 mg), 5 because of diabetes and 1 because ofpatient preference. Of the 87 excluded patients who failedto meet the Jones and Hazleman criteria (6), 4 were con-sidered to have PMR by the treating clinician duringscreening (1 had low ESR, 1 was initially diagnosed with
rheumatoid arthritis, and 2 had morning stiffness �30minutes).
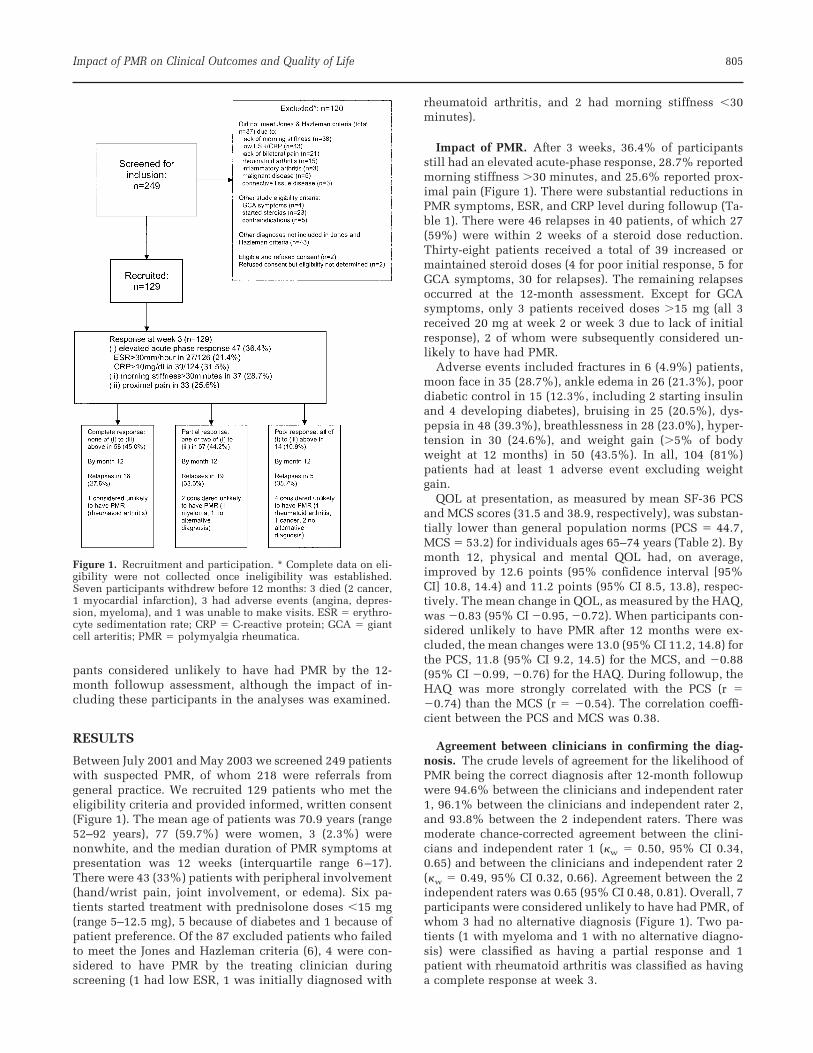
Impact of PMR. After 3 weeks, 36.4% of participantsstill had an elevated acute-phase response, 28.7% reportedmorning stiffness �30 minutes, and 25.6% reported prox-imal pain (Figure 1). There were substantial reductions inPMR symptoms, ESR, and CRP level during followup (Ta-ble 1). There were 46 relapses in 40 patients, of which 27(59%) were within 2 weeks of a steroid dose reduction.Thirty-eight patients received a total of 39 increased ormaintained steroid doses (4 for poor initial response, 5 forGCA symptoms, 30 for relapses). The remaining relapsesoccurred at the 12-month assessment. Except for GCAsymptoms, only 3 patients received doses �15 mg (all 3received 20 mg at week 2 or week 3 due to lack of initialresponse), 2 of whom were subsequently considered un-likely to have had PMR.
Adverse events included fractures in 6 (4.9%) patients,moon face in 35 (28.7%), ankle edema in 26 (21.3%), poordiabetic control in 15 (12.3%, including 2 starting insulinand 4 developing diabetes), bruising in 25 (20.5%), dys-pepsia in 48 (39.3%), breathlessness in 28 (23.0%), hyper-tension in 30 (24.6%), and weight gain (�5% of bodyweight at 12 months) in 50 (43.5%). In all, 104 (81%)patients had at least 1 adverse event excluding weightgain.
QOL at presentation, as measured by mean SF-36 PCSand MCS scores (31.5 and 38.9, respectively), was substan-tially lower than general population norms (PCS � 44.7,MCS � 53.2) for individuals ages 65–74 years (Table 2). Bymonth 12, physical and mental QOL had, on average,improved by 12.6 points (95% confidence interval [95%CI] 10.8, 14.4) and 11.2 points (95% CI 8.5, 13.8), respec-tively. The mean change in QOL, as measured by the HAQ,was �0.83 (95% CI �0.95, �0.72). When participants con-sidered unlikely to have PMR after 12 months were ex-cluded, the mean changes were 13.0 (95% CI 11.2, 14.8) forthe PCS, 11.8 (95% CI 9.2, 14.5) for the MCS, and �0.88(95% CI �0.99, �0.76) for the HAQ. During followup, theHAQ was more strongly correlated with the PCS (r ��0.74) than the MCS (r � �0.54). The correlation coeffi-cient between the PCS and MCS was 0.38.
Agreement between clinicians in confirming the diag-nosis. The crude levels of agreement for the likelihood ofPMR being the correct diagnosis after 12-month followupwere 94.6% between the clinicians and independent rater1, 96.1% between the clinicians and independent rater 2,and 93.8% between the 2 independent raters. There wasmoderate chance-corrected agreement between the clini-cians and independent rater 1 (�w � 0.50, 95% CI 0.34,0.65) and between the clinicians and independent rater 2(�w � 0.49, 95% CI 0.32, 0.66). Agreement between the 2independent raters was 0.65 (95% CI 0.48, 0.81). Overall, 7participants were considered unlikely to have had PMR, ofwhom 3 had no alternative diagnosis (Figure 1). Two pa-tients (1 with myeloma and 1 with no alternative diagno-sis) were classified as having a partial response and 1patient with rheumatoid arthritis was classified as havinga complete response at week 3.
Figure 1. Recruitment and participation. * Complete data on eli-gibility were not collected once ineligibility was established.Seven participants withdrew before 12 months: 3 died (2 cancer,1 myocardial infarction), 3 had adverse events (angina, depres-sion, myeloma), and 1 was unable to make visits. ESR � erythro-cyte sedimentation rate; CRP � C-reactive protein; GCA � giantcell arteritis; PMR � polymyalgia rheumatica.
Impact of PMR on Clinical Outcomes and Quality of Life 805
Tab
le1.
Dis
ease
acti
vity
inth
efi
rst
year
ofp
olym
yalg
iarh
eum
atic
a*
Bas
elin
e(n
�12
9)W
eek
3(n
�12
9)W
eek
6(n
�12
8)M
onth
3(n
�12
6)M
onth
6(n
�12
4)M
onth
12(n
�12
2)
ES
R,
mm
/hou
rM
edia
n(i
nte
rqu
arti
lera
nge
)61
(48–
81)
18(1
1–29
)18
(11–
26)
16(9
–27)
14(8
–25)
15(1
0–25
)M
ean
chan
gefr
omba
seli
ne
(95%
CI)
–�
43(�
46,�
39)
�45
(�49
,�41
)�
44(�
49,�
40)
�47
(�51
,�42
)�
45(�
50,�
41)
CR
Ple
vel,
mg/
dl
Med
ian
(in
terq
uar
tile
ran
ge)
48(2
2–84
)�
6(�
6–13
)�
6(�
6–12
)�
6(�
6–10
)�
6(�
6–7)
�6
(�6–
10)
Mea
nch
ange
from
base
lin
e(9
5%C
I)–
�48
(�55
,�40
)�
48(�
55,�
40)
�48
(�57
,�40
)�
51(�
59,�
43)
�50
(�58
,�42
)M
orn
ing
stif
fnes
s,m
inu
tes
Med
ian
(in
terq
uar
tile
ran
ge)
120
(60–
240)
0(0
–60)
0(0
–15)
0(0
–15)
0(0
–5)
0(0
–20)
Mea
nch
ange
from
base
lin
e(9
5%C
I)–
�16
9(�
215,
�12
3)�
167
(�21
8,�
116)
�18
5(�
230,
�13
9)�
185
(�24
1,�
129)
�17
7(�
234,
�11
9)S
hou
lder
gird
lep
ain
,n
o.(%
)12
7(9
8.5)
25(1
9.4)
16(1
2.6)
14(1
1.1)
19(1
5.5)
22(1
8.0)
Pel
vic
gird
lep
ain
,n
o.(%
)11
6(8
9.9)
18(1
4.0)
13(1
0.2)
15(1
1.9)
7(5
.7)
14(1
1.5)
Rel
apse
ator
pri
orto
asse
ssm
ent,
no.
(%)
–5
97
25C
um
ula
tive
no.
(%)
ofp
atie
nts
foll
owin
gst
eroi
dta
per
sch
edu
le†
128
(99.
2)12
2(9
5.3)
111
(88.
1)97
(78.
2)85
(69.
7)
Rea
son
sfo
rin
crea
sed
/mai
nta
ined
dos
eif
not
rela
pse
1la
ckof
resp
onse
‡3
lack
ofre
spon
se4
GC
Asy
mp
tom
s1
GC
Asy
mp
tom
s
*E
SR
�er
yth
rocy
tese
dim
enta
tion
rate
;95
%C
I�
95%
con
fid
ence
inte
rval
;C
RP
�C
-rea
ctiv
ep
rote
in;
GC
A�
gian
tce
llar
teri
tis.
†In
clu
des
pat
ien
tsab
leto
red
uce
ahea
dof
sch
edu
lew
ith
out
rela
pse
.‡
Pat
ien
tsu
bseq
uen
tly
dia
gnos
edas
hav
ing
can
cer
and
wit
hd
raw
nby
wee
k6.
806 Hutchings et al
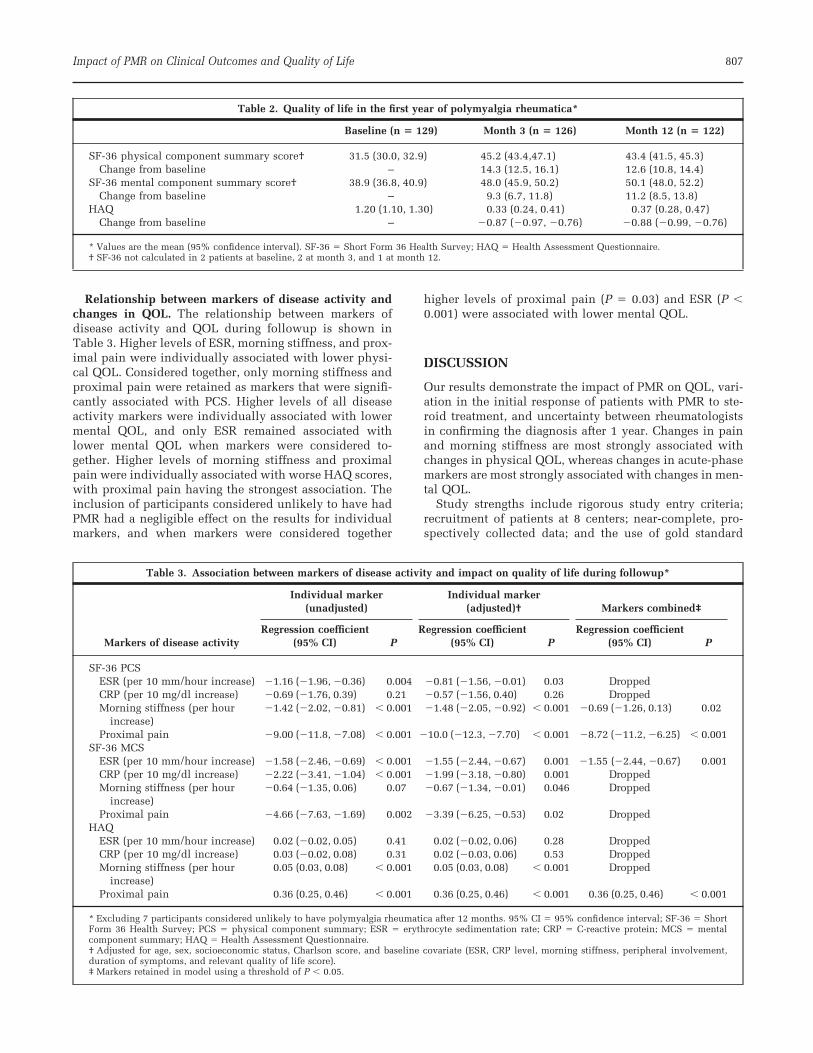
Relationship between markers of disease activity andchanges in QOL. The relationship between markers ofdisease activity and QOL during followup is shown inTable 3. Higher levels of ESR, morning stiffness, and prox-imal pain were individually associated with lower physi-cal QOL. Considered together, only morning stiffness andproximal pain were retained as markers that were signifi-cantly associated with PCS. Higher levels of all diseaseactivity markers were individually associated with lowermental QOL, and only ESR remained associated withlower mental QOL when markers were considered to-gether. Higher levels of morning stiffness and proximalpain were individually associated with worse HAQ scores,with proximal pain having the strongest association. Theinclusion of participants considered unlikely to have hadPMR had a negligible effect on the results for individualmarkers, and when markers were considered together
higher levels of proximal pain (P � 0.03) and ESR (P �0.001) were associated with lower mental QOL.
DISCUSSION
Our results demonstrate the impact of PMR on QOL, vari-ation in the initial response of patients with PMR to ste-roid treatment, and uncertainty between rheumatologistsin confirming the diagnosis after 1 year. Changes in painand morning stiffness are most strongly associated withchanges in physical QOL, whereas changes in acute-phasemarkers are most strongly associated with changes in men-tal QOL.
Study strengths include rigorous study entry criteria;recruitment of patients at 8 centers; near-complete, pro-spectively collected data; and the use of gold standard
Table 2. Quality of life in the first year of polymyalgia rheumatica*
Baseline (n � 129) Month 3 (n � 126) Month 12 (n � 122)
SF-36 physical component summary score† 31.5 (30.0, 32.9) 45.2 (43.4,47.1) 43.4 (41.5, 45.3)Change from baseline – 14.3 (12.5, 16.1) 12.6 (10.8, 14.4)
SF-36 mental component summary score† 38.9 (36.8, 40.9) 48.0 (45.9, 50.2) 50.1 (48.0, 52.2)Change from baseline – 9.3 (6.7, 11.8) 11.2 (8.5, 13.8)
HAQ 1.20 (1.10, 1.30) 0.33 (0.24, 0.41) 0.37 (0.28, 0.47)Change from baseline – �0.87 (�0.97, �0.76) �0.88 (�0.99, �0.76)
* Values are the mean (95% confidence interval). SF-36 � Short Form 36 Health Survey; HAQ � Health Assessment Questionnaire.† SF-36 not calculated in 2 patients at baseline, 2 at month 3, and 1 at month 12.
Table 3. Association between markers of disease activity and impact on quality of life during followup*
Markers of disease activity
Individual marker(unadjusted)
Individual marker(adjusted)† Markers combined‡
Regression coefficient(95% CI) P
Regression coefficient(95% CI) P
Regression coefficient(95% CI) P
SF-36 PCSESR (per 10 mm/hour increase) �1.16 (�1.96, �0.36) 0.004 �0.81 (�1.56, �0.01) 0.03 DroppedCRP (per 10 mg/dl increase) �0.69 (�1.76, 0.39) 0.21 �0.57 (�1.56, 0.40) 0.26 DroppedMorning stiffness (per hour
increase)�1.42 (�2.02, �0.81) � 0.001 �1.48 (�2.05, �0.92) � 0.001 �0.69 (�1.26, 0.13) 0.02
Proximal pain �9.00 (�11.8, �7.08) � 0.001 �10.0 (�12.3, �7.70) � 0.001 �8.72 (�11.2, �6.25) � 0.001SF-36 MCS
ESR (per 10 mm/hour increase) �1.58 (�2.46, �0.69) � 0.001 �1.55 (�2.44, �0.67) 0.001 �1.55 (�2.44, �0.67) 0.001CRP (per 10 mg/dl increase) �2.22 (�3.41, �1.04) � 0.001 �1.99 (�3.18, �0.80) 0.001 DroppedMorning stiffness (per hour
increase)�0.64 (�1.35, 0.06) 0.07 �0.67 (�1.34, �0.01) 0.046 Dropped
Proximal pain �4.66 (�7.63, �1.69) 0.002 �3.39 (�6.25, �0.53) 0.02 DroppedHAQ
ESR (per 10 mm/hour increase) 0.02 (�0.02, 0.05) 0.41 0.02 (�0.02, 0.06) 0.28 DroppedCRP (per 10 mg/dl increase) 0.03 (�0.02, 0.08) 0.31 0.02 (�0.03, 0.06) 0.53 DroppedMorning stiffness (per hour
increase)0.05 (0.03, 0.08) � 0.001 0.05 (0.03, 0.08) � 0.001 Dropped
Proximal pain 0.36 (0.25, 0.46) � 0.001 0.36 (0.25, 0.46) � 0.001 0.36 (0.25, 0.46) � 0.001
* Excluding 7 participants considered unlikely to have polymyalgia rheumatica after 12 months. 95% CI � 95% confidence interval; SF-36 � ShortForm 36 Health Survey; PCS � physical component summary; ESR � erythrocyte sedimentation rate; CRP � C-reactive protein; MCS � mentalcomponent summary; HAQ � Health Assessment Questionnaire.† Adjusted for age, sex, socioeconomic status, Charlson score, and baseline covariate (ESR, CRP level, morning stiffness, peripheral involvement,duration of symptoms, and relevant quality of life score).‡ Markers retained in model using a threshold of P � 0.05.
Impact of PMR on Clinical Outcomes and Quality of Life 807

measures to evaluate QOL. Patients were recruited beforestarting steroids and followed a standardized steroid treat-ment schedule.
The generalizability of our findings may be limited for 2reasons. First, the strict entry criteria excluded patientswithout elevated ESR. Second, the study was undertakenin secondary care where rheumatologists may see morecomplicated cases. A further limitation is the lack of acontrol group that did not receive steroids or did not havePMR, because it was ethically unacceptable to withholdtreatment for PMR or to administer steroids to those notrequiring them.
The classic PMR disease course of a rapid and completeresolution of symptoms was observed in only a minority ofparticipants. More than one-quarter of participants with acomplete response by 3 weeks had a relapse in the firstyear. The 14 participants with a poor response to steroidsat 3 weeks were a mixed group: 4 patients were subse-quently considered not to have PMR and the remainderexhibited a slow treatment response, 5 of whom subse-quently had a relapse. Caution in interpreting these resultsis required because the confirmation of the diagnosis at 12months was based on review of this initial response aswell as longer-term followup.
The apparently poor initial response in our participantsmay seem surprising but is not inconsistent with previousstudies. For example, CRP level remained elevated in 9 of20 patients with PMR after 1 week of receiving 15 mg ofprednisolone, and the mean ESR was 38 mm/hour (24). At2 weeks the mean duration of morning stiffness was 47minutes, mean ESR was 40 mm/hour, and there was amean reduction in VAS limb girdle pain score of 47% (25).At 1 month ESR was elevated in 13.2% of participants andCRP level was elevated in 41.9% (26). At 4 weeks the meanESR and CRP level were �30 mm/hour and 10 mg/liter,respectively, with VAS pain score decreasing from �70 to�20 on a 0–100 scale (27).
The disagreement between rheumatologists in confirm-ing the PMR diagnosis highlights uncertainty about therole of steroid response and later disease course as diag-nostic criteria for PMR. Although crude agreement washigh, the kappa coefficients indicated a gray area betweenpatients who follow a classic PMR disease course andthose who are given a confirmed alternative diagnosis thatwould explain a PMR-like presentation. We plan to ex-plore reasons for these differences in future work.
Existing criteria are based on clinical and laboratorymeasures at presentation and exclusions of other condi-tions. A response to steroid therapy is included in 2 sets ofcriteria (6,8) and is mentioned in 2 (5,7), but none providesa definition for this response. Findings from this studyhighlight the ubiquitous nonspecific responses to even 15mg of prednisolone in patients with an initial PMR diag-nosis.
Individuals with musculoskeletal conditions generallyhave low physical QOL, but not mental QOL, in compar-ison with other chronic conditions (28). Participants inthis study showed substantially reduced physical andmental QOL at presentation but considerable improve-ment in QOL after steroid therapy, despite �80% report-ing adverse events, which is higher than the rates of 65%
(18) and 36% (29) reported previously. The differencesmay be due to inclusion and recording of adverse eventsand duration of followup. Serious adverse events are alsomore likely to occur beyond 1 year when cumulative ste-roid doses are higher.
The finding that proximal pain and morning stiffness,but not ESR and CRP level, are associated with physicalQOL supports previous research that has demonstratedincreased inflammatory markers in the absence of clinicalsymptoms in patients with PMR (26). The relationship weobserved between elevated acute-phase markers of ESR orCRP level and poorer mental QOL is surprising, given thatthe acute-phase markers showed a stronger relationshipthan duration of morning stiffness, and that neither ESRnor CRP level showed a strong association with physicalQOL. The impaired mental QOL and depression com-monly seen in patients with PMR may therefore be relatedto the neurologic effects of circulating cytokines such asinterleukin-6, which is elevated in PMR and may havesignificant effects on the central nervous system (30,31).
The heterogeneity of the response to steroids and sub-sequent disease course indicates that PMR is similar toother chronic rheumatic and nonrheumatic conditions, inwhich treatment modalities and responses are influencedby many factors that include disease severity, comorbidity,and patient acceptability. This finding and the diagnosticuncertainty highlight the importance of a comprehensiveevaluation before starting steroids, careful ongoing moni-toring of the disease, and vigilance regarding alternativediagnoses. There is a need for clear guidelines on diagno-sis and management, with consideration of specialist re-ferral for patients with atypical presentation or incompleteresponse to low-dose steroids (32). Given the impact ofPMR on patients, disease monitoring and treatment shouldfocus on inflammatory symptoms and avoid using acute-phase markers alone. The relationship between acute-phase markers and mental QOL is intriguing and requiresfurther research on its pathogenesis and implications fortherapy.
AUTHOR CONTRIBUTIONS
Dr. Dasgupta had full access to all of the data in the study andtakes responsibility for the integrity of the data and the accuracyof the data analysis.Study design. Hutchings, Lamping, Pease, Chakravarty, Silver-man, Choy, Scott, Hazleman, Dasgupta.Acquisition of data. Hutchings, Hollywood, Lamping, Pease,Chakravarty, Silverman, Choy, Scott, Hazleman, Bourke, Gendi,Dasgupta.Analysis and interpretation of data. Hutchings, Hollywood,Lamping, Pease, Chakravarty, Silverman, Choy, Scott, Hazleman,Bourke, Gendi, Dasgupta.Manuscript preparation. Hutchings, Hollywood, Lamping, Pease,Chakravarty, Silverman, Choy, Scott, Hazleman, Bourke, Gendi,Dasgupta.Statistical analysis. Hutchings.
REFERENCES
1. Smeeth L, Cook C, Hall AJ. Incidence of diagnosed polymy-algia rheumatica and temporal arteritis in the United King-dom, 1990–2001. Ann Rheum Dis 2006;65:1093–8.
2. Walsh LJ, Wong CA, Pringle M, Tattersfield AE. Use of oral
808 Hutchings et al
corticosteroids in the community and the prevention of sec-ondary osteoporosis: a cross sectional study. BMJ 1996;313:344–6.
3. Helfgott SM, Kieval RI. Polymyalgia rheumatica in patientswith a normal erythrocyte sedimentation rate. ArthritisRheum 1996;39:304–7.
4. Brooks RC, McGee SR. Diagnostic dilemmas in polymyalgiarheumatica. Arch Intern Med 1997;157:162–8.
5. Bird HA, Esselinckx W, Dixon AS, Mowat AG, Wood PH. Anevaluation of criteria for polymyalgia rheumatica. AnnRheum Dis 1979;38:434–9.
6. Jones JG, Hazleman BL. Prognosis and management of poly-myalgia rheumatica. Ann Rheum Dis 1981;40:1–5.
7. Chuang TY, Hunder GG, Ilstrup DM, Kirkland LT. Polymyal-gia rheumatica: a 10-year epidemiologic and clinical study.Ann Intern Med 1982;97:672–80.
8. Healey LA. Long-term follow-up of polymyalgia rheumatica:evidence for synovitis. Semin Arthritis Rheum 1984;13:322–8.
9. Bahlas S, Ramos-Remus C, Davis P. Utilisation and costs ofinvestigations, and accuracy of diagnosis of polymyalgiarheumatica by family physicians. Clin Rheumatol 2000;19:278–80.
10. Blaauw AA, Schuwirth LW, van der Vleuten CP, Smits F, vander Linden S. Assessing clinical competence: recognition ofcase descriptions of rheumatic diseases by general practitio-ners. Br J Rheumatol 1995;34:375–9.
11. Gamez-Nava JI, Gonzalez-Lopez L, Davis P, Suarez-AlmazorME. Referral and diagnosis of common rheumatic diseases byprimary care physicians. Br J Rheumatol 1998;37:1215–9.
12. Pease CT, Haugeberg G, Morgan AW, Montague B, HensorEM, Bhatka BB. Diagnosing late onset rheumatoid arthritis,polymyalgia rheumatica, and temporal arteritis in patientspresenting with polymyalgic symptoms: a prospective long-term evaluation [published erratum appears in J Rheumatol2005;32:1043–6]. J Rheumatol 2005;32:1043–6.
13. Caporali R, Montecucco C, Epis O, Bobbio-Pallavicini F, MaioT, Cimmino MA. Presenting features of polymyalgia rheu-matica (PMR) and rheumatoid arthritis with PMR-like onset: aprospective study. Ann Rheum Dis 2001;60:1021–4.
14. Gonzalez-Gay MA, Garcia-Porrua C, Salvarani C, Olivieri I,Hunder GG. The spectrum of conditions mimicking polymy-algia rheumatica in Northwestern Spain. J Rheumatol 2000;27:2179–84.
15. Swannell AJ. Polymyalgia rheumatica and temporal arteritis:diagnosis and management [review]. BMJ 1997;314:1329–32.
16. Salvarani C, Cantini F, Boiardi L, Hunder GG. Polymyalgiarheumatica and giant-cell arteritis [review]. N Engl J Med2002;347:261–71.
17. Weyand CM, Fulbright JW, Evans JM, Hunder GG, Goronzy JJ.Corticosteroid requirements in polymyalgia rheumatica. ArchIntern Med 1999;159:577–84.
18. Gabriel SE, Sunku J, Salvarani C, O’Fallon WM, Hunder GG.Adverse outcomes of antiinflammatory therapy among pa-
tients with polymyalgia rheumatica. Arthritis Rheum 1997;40:1873–8.
19. Pincus T, Summey JA, Soraci SA Jr, Wallston KA, HummonNP. Assessment of patient satisfaction in activities of dailyliving using a modified Stanford Health Assessment Ques-tionnaire. Arthritis Rheum 1983;26:1346–53.
20. Jenkinson C, Stewart-Brown S, Petersen S, Paice C. Assess-ment of the SF-36 version 2 in the United Kingdom. J Epide-miol Community Health 1999;53:46–50.
21. Twisk JW. Applied longitudinal data analysis for epide-miology: a practical guide. Cambridge: Cambridge UniversityPress; 2003.
22. Office for National Statistics. The national statistics socio-economic classification user manual. London: Office for Na-tional Statistics; 2002.
23. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A newmethod for classifying prognostic comorbidity in longitudinalstudies: development and validation. J Chronic Dis 1987;40:373–83.
24. Schreiber S, Buyse M. The CRP initial response to treatmentas a prognostic factor in patients with polymyalgia rheu-matica. Clin Rheumatol 1995;14:315–8.
25. Di Munno O, Imbimbo B, Mazzantini M, Milani S, OcchipintiG, Pasero G. Deflazacort versus methylprednisolone in poly-myalgia rheumatica: clinical equivalence and relative antiin-flammatory potency of different treatment regimes. J Rheuma-tol 1995;22:1492–8.
26. Salvarani C, Cantini F, Niccoli L, Macchioni P, Consonni D,Bajocchi G, et al. Acute-phase reactants and the risk of re-lapse/recurrence in polymyalgia rheumatica: a prospectivefollowup study. Arthritis Rheum 2005;53:33–8.
27. Leeb BF, Bird HA, Nesher G, Andel I, Hueber W, Logar D, etal. EULAR response criteria for polymyalgia rheumatica: re-sults of an initiative of the European Collaborating Polymy-algia Rheumatica Group (subcommittee of ESCISIT). AnnRheum Dis 2003;62:1189–94.
28. Sprangers MA, de Regt EB, Andries F, van Agt HM, Bijl RV, deBoer JB, et al. Which chronic conditions are associated withbetter or poorer quality of life? J Clin Epidemiol 2000;53:895–907.
29. Kyle V, Hazleman BL. Treatment of polymyalgia rheumaticaand giant cell arteritis. II. Relation between steroid dose andsteroid associated side effects. Ann Rheum Dis 1989;48:662–6.
30. Dasgupta B, Panayi GS. Interleukin-6 in serum of patientswith polymyalgia rheumatica and giant cell arteritis. Br JRheumatol 1990;29:456–8.
31. Brebner K, Hayley S, Zacharko R, Merali Z, Anisman H.Synergistic effects of interleukin-1�, interleukin-6 and tumornecrosis factor-�: central monoamine, corticosterone and be-havioral variations. Neuropsychopharmacology 2000;22:566–80.
32. Dasgupta B, Hutchings A, Matteson EL. Polymyalgia rheu-matica: the mess we are now in and what we need to do aboutit [editorial]. Arthritis Rheum 2006;55:518–20.
Impact of PMR on Clinical Outcomes and Quality of Life 809