Embed Size (px)
Citation preview

Accepted Manuscript
Clinical Outcomes of Erythropoietin Use in Heart Failure Patients with Anemia ofChronic Kidney Disease
Cynthia Jackevicius, BScPhm, PharmD, MSc, BCPS Cindy Shutieng Fan, PharmDAlberta Warner, MD
PII: S1071-9164(14)00064-5
DOI: 10.1016/j.cardfail.2014.02.001
Reference: YJCAF 3258
To appear in: Journal of Cardiac Failure
Received Date: 18 July 2013
Revised Date: 5 February 2014
Accepted Date: 6 February 2014
Please cite this article as: Jackevicius C, Fan CS, Warner A, Clinical Outcomes of Erythropoietin Use inHeart Failure Patients with Anemia of Chronic Kidney Disease, Journal of Cardiac Failure (2014), doi:10.1016/j.cardfail.2014.02.001.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Clinical Outcomes of Erythropoietin Use in Heart Failure Patients with Anemia of Chronic
Kidney Disease
Cynthia Jackevicius, BScPhm, PharmD, MSc, BCPS,1-5 Cindy Shutieng Fan, PharmD,1,2
Alberta Warner, MD2,6
1College of Pharmacy, Western University of Health Sciences, 2VA Greater Los Angeles
Healthcare System, 3Institute for Clinical Evaluative Sciences, 4Institute for Health Policy,
Management and Evaluation, 5University Health Network, 6Department of Medicine, Division of
Cardiology, UCLA
Address for correspondence:
Cynthia Jackevicius, BScPhm, PharmD, MSc, FCSHP, BCPS, AQ Cardiology
Professor, College of Pharmacy, Western University of Health Sciences
309 E. Second St., Pomona CA 91766;
Phone: 909-469-5527; Fax: 909-469-5539; [email protected]
Running title: Outcomes of EPO in CRAS
This study was funded by the American College of Clinical Pharmacy Watson Anemia
Investigator Development Research Award.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
Abstract
Background: Anemia and chronic kidney disease are common disorders in heart failure (HF)
patients, and are associated with increased morbidity and mortality. This study assesses clinical
outcomes associated with erythropoietin (EPO) treatment in this cardio-renal-anemia syndrome
(CRAS) population.
Methods and Results: This is a retrospective cohort study of VA patients with CRAS from
January 2003 to December 2006. The primary outcome was a composite of death, acute coronary
syndromes, HF and stroke. Multiple Cox regression modeling was used to evaluate the outcome
in patients prescribed (n=213) and not prescribed EPO (n=1845). Adjusted incidence of mortality
was statistically significantly higher in EPO than non-EPO users (33.8% vs. 19.7%;HR:1.40
95%CI1.06-1.85, p=0.02). The unadjusted composite of cardiovascular events/death was higher
in the EPO group, but not statistically significant when adjusted for confounders (p=0.12). Crude
ACS events were documented in 18.8% and 10.8% patients (p=0.001), and stroke events
occurred in 22.5% and 18.3% patients (p=0.14) in EPO and non-EPO groups, respectively.
Conclusions: We found that in CRAS patients, EPO use was associated with increased risk of
mortality and a trend towards increased cardiovascular events. Therefore, clinicians considering
EPO use in CRAS patients should assess whether any potential benefits outweigh the risks of
use.
Key Words: cardiac, health policy, outcome research

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
Introduction
Despite advances in therapy, heart failure (HF), a common and progressive condition,
continues to be associated with a substantial increase in morbidity and mortality.1-3 The majority
of patients with HF also have comorbidities, such as, hypertension, diabetes, dyslipidemia and
coronary artery disease. Treatment used for HF and these comorbidities may contribute to the
development of chronic kidney disease (CKD) if cardiac output is decreased, with such patients
progressing to end-stage renal disease.4 Depending on the severity, both HF and CKD can
complicate management of the other condition.
Anemia is also a common complication that is observed in both CKD and HF.1-3,5 The
prevalence of anemia in HF patients range from 7-70% depending on the patient cohort, and
increases as HF severity worsens.2,4-8 In the OPTIMIZE-HF registry, 51.2% of patients
hospitalized for HF had hemoglobin levels of <12.1g/dl, of which 25% were moderately to
severely anemic.9 In retrospective HF studies,3 reduced hemoglobin levels have been associated
with increased hospitalization, HF severity, decreased functional status, worsened symptoms and
mortality, while prospective studies have shown less promising results.1-5,8,10-12
HF, CKD and anemia often occur concurrently and are coined the cardio-renal-anemia
syndrome (CRAS) which significantly increases in-hospital mortality when compared to HF
alone.13 Although each condition amplifies the risk of the other, individuals with all 3 risk factors
are at particularly high risk for adverse cardiovascular (CV) events. Data regarding the effects of
erythropoietic stimulating agents (ESA) to correct anemia in CRAS patients is limited. Older
evidence in dialysis patients with underlying cardiac disease (ischemic heart disease or HF) and
anemia found increased mortality associated with ESA use.14 Smaller, single center studies have
shown that ESA’s effect of raising hemoglobin levels in anemic HF patients translated into

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
benefits on hospitalization rates, functional class, quality of life and exercise capacity, thus
improving HF and CKD.3,15,16 However, more recent studies in anemic CKD patients have
incidentally shown that ESA targeting higher hemoglobin levels were associated with increased
risk of all-cause mortality, adverse CV events and increased stroke events.12,17-19 Subsequently,
the US Food and Drug Administration modified the recommended dosing for ESA in an attempt
to prevent these adverse CV events.20 Furthermore, increased thrombotic events have been
reported in anemic HF patients without CKD with use of ESA.12 Given recent concerns in
isolated HF and CKD populations, more evidence about the potential negative outcomes
associated with treatment of anemia of CKD in HF patients is crucial in determining safe and
appropriate therapy. The aim of this study was to determine the CV clinical outcomes and
mortality associated with use of erythropoietin (EPO) in patients with CRAS.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
Methods
Study Design and Data Sources. We conducted a retrospective cohort study using
administrative and clinical data from Veterans Affairs Greater Los Angeles Healthcare System.
Our administrative databases have been successfully used for utilization and outcomes research
by other investigators.21 For the mortality outcome, we used the VA vital status file, which has
high sensitivity and accuracy when compared with the National Death Index. The study was
approved by institutional review committees at Veterans Affairs Greater Los Angeles Healthcare
System and Western University of Health Sciences.
Population. Patients from Veterans Affairs Greater Los Angeles from January 1, 2003 to
December 31, 2006 were included if they met the following three criteria: 1) ≥1 principal
or secondary diagnosis of HF or cardiomyopathy based on diagnoses from hospitalizations
and ambulatory visits using International Classification of Diseases, 9th Revision, Clinical
Modification [ICD-9-CM] codes 425.x (cardiomyopathy) and 428.x (HF); AND 2)
subsequent to the HF diagnosis, a diagnosis of CKD, as defined by an estimated glomerular
filtration rate <60 mL/min/1.73 m2 body surface area in 2 measurements over at least a 3
month period according to the NKF-K/DOQI guideline definition of CKD. Estimated
glomerular filtration rate is automatically calculated by our laboratory based on the four
variable Modification of Diet in Renal Disease equation;22 AND 3) subsequent to the HF
and CKD diagnoses, a diagnosis of anemia, as defined by the NKF-K/DOQI anemia
guidelines. The 2006 NKF-K/DOQI guidelines for the definition of anemia were used
(hemoglobin < 12 g/dL for adult males and postmenopausal females and hemoglobin < 11
g/dL for premenopausal females) as these guidelines cover the majority of our study
period.23 The index date was defined as the date when the patient had all three diagnoses of

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
interest to classify them as having the CRAS diagnosis. Patients were excluded if they had
one or more of the following: died before hospital discharge; received cardiac
transplantation; a diagnosis of anemia based on an episode of recognized acute blood loss,
such as trauma or upper gastrointestinal bleed, which may have accounted for a temporarily
low hemoglobin unrelated to anemia of CKD; documented hypersensitivity reaction to
EPO; or no records of their clinical status. Patient data for demographics, medications,
comorbidities and laboratory values was obtained from the electronic medical records and
linked using a unique encrypted scrambled patient identification number per patient.
Study Group. The exposure group was defined as prescription of EPO therapy (erythropoietin
was only ESA available) after CRAS diagnosis. According to institutional protocol, all EPO
prescriptions need to be approved by the Nephrology Service.
Control. The control group included patients who did not receive EPO therapy after CRAS
diagnosis.
Outcomes. The primary outcome in this study was to determine the composite of death, acute
coronary syndrome (ACS), HF and stroke. The secondary outcome was total mortality.
Statistical analysis. The characteristics of the population were described using mean ± standard
deviation as appropriate for continuous data and proportions for categorical data. The differences
in baseline characteristics between EPO and non-EPO were compared using the t-test for
continuous data and Chi-square test for categorical data. Crude (unadjusted) event rates are
reported and compared using Chi-square test. We then constructed a multivariate Cox regression
model, retaining all covariates with a p-value <0.15 in a backward stepwise regression, as well as
including variables of clinical importance to the outcome of interest. In the backward variable
screening, we deliberately chose to retain a variable in the model even if it was only moderately

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
significant. Imputation was used to fill in values for the one variable, ejection fraction (EF), with
missing values in order to retain all observations in the multivariate analysis. EF was then used
as a dichotomous variable (≤50% or >50%) due to the required imputation. The covariates
considered in the models were demographics (age, sex), baseline laboratory values for estimated
glomerular filtration rate, serum creatinine, blood urea nitrogen, hemoglobin, systolic blood
pressure and diastolic blood pressure, EF >50%, comorbidities [coronary artery disease,
cerebrovascular disease, atrial fibrillation, diabetes, hypertension, hyperlipidemia, chronic
obstructive pulmonary disease, malignancy], concomitant medications [angiotensin-converting
enzyme inhibitor, angiotensin receptor blocker, aspirin, beta-blocker, digoxin, diuretic,
hydralazine/nitrates, aldosterone antagonist, iron (oral or intravenous), warfarin, clopidogrel,
statin], use of dialysis, history of renal clinic appointment and participation in a specialty HF
clinic, all documented within 1 year prior to the index date. Hazard ratios and 95% confidence
intervals for the adjusted models are reported. All data were analyzed using SAS® version 9.2
(SAS Institute, Cary, NC). A p-value of <0.05 was considered statistically significant.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
Results
Of a total of 2058 patients with CRAS, 213 (10.3%) were prescribed EPO and 1845
(89.7%) did not receive EPO therapy. Median follow-up was 17.6 months (maximum 44.2
months). There were a number of significant differences in baseline characteristics of those
prescribed and not prescribed EPO (Table 1). There were significant differences between groups
for baseline parameters of renal function (estimated glomerular filtration rate, serum creatinine,
blood urea nitrogen) (p<0.0001), attributed to a more advanced disease process in the EPO-
treated group. Baseline hemoglobin/hematocrit was lower in those treated with EPO (p<0.0001).
Comorbidities were similar between groups except for hypertension and malignancy
which were higher in the EPO group (p=0.02, p=0.04, respectively). Use of aspirin, angiotensin
receptor blockers, iron supplements and hydralazine/nitrates was higher in the EPO group
(p=0.02, p=0.03, p<0.0001, <0.0001, respectively). History of renal clinic appointment and
dialysis were also higher in the EPO group (p<0.0001, p<0.01, respectively).
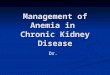
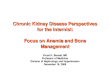
Unadjusted incidence of CV events and death was statistically significantly higher in the
EPO group (HR 1.19 95% CI 1.00-1.41, p=0.04). Unadjusted mortality was also significantly
higher in the EPO than the non-EPO group (33.8% and 19.7%, respectively; HR=1.62 95% CI
1.26-2.09, p<0.001). ACS events were documented more often (18.8% and 10.8%) in EPO than
non-EPO patients (p=0.001). All-cause hospitalizations were significantly higher in EPO than
non-EPO patients (p<0.001). There was a trend towards a higher proportion of patients receiving
EPO being hospitalized for HF (47.9% vs. 41.2%, p=0.07) as well as towards an increase in
stroke events in 22.5% and 18.3% (p=0.14). (Table 2, Figures 1 and 2)
The adjusted incidence of the composite of CV events and death was numerically higher
in the EPO group, but no longer statistically significant (HR=1.16 95% CI 0.96-1.40, p=0.12).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
(Table 3) Increased age, blood urea nitrogen, hemoglobin < 10g/dL, EF≤50%, comorbidities
[coronary artery disease, cerebrovascular disease, atrial fibrillation, chronic obstructive
pulmonary disease], and medications [aspirin, diuretic, and hydralazine/nitrates] contributed to
increased trend of CV events/death while history of hypertension was associated with reduced
composite events. Even after adjusting for other confounding factors, incidence of mortality
remained higher in the EPO group (HR=1.40 95% CI 1.06-1.85, p=0.02). (Table 4) Other
variables contributing to increased death were increasing age, increasing blood urea nitrogen,
hemoglobin < 10g/dL, EF≤50%, comorbidities [chronic obstructive pulmonary disease and
cancer], while higher systolic blood pressure, history of hypertension and medications [beta
blockers and statins] were associated with reduced mortality. Results were consistent using
propensity score-adjusted models for both mortality (HR for EPO exposure: 1.88 [1.37-2.60],
p<0.0001) and the composite endpoint (HR for EPO exposure: 1.05 [0.84-1.32], p=0.65).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
Discussion
Our study found that patients receiving EPO, as compared with non-EPO users, had a
higher risk of death. Possible explanations for the increased mortality rate in our study could be
that the EPO group consisted of sicker patients with worse renal function and anemia, along with
significantly more patients with cancer and hypertension. However, the increased risk remained
even after adjusting for numerous confounding variables. While several early, uncontrolled,
open label studies found favorable improvements in functional class, EF, hemoglobin and HF
hospitalizations in CRAS patients,1,,15,16 our results are more consistent with other recent studies
that show concerning increases in death, CV and thrombotic events with ESA.12,14 Despite more
recent attention, these concerns date as far back as 1998, with the large NHCT study which
randomized 1,223 patients with HF or ischemic heart disease undergoing hemodialysis to receive
epoetin alfa to achieve either a hematocrit of 45% or 30%. Similar to our study, this trial found a
significant increase in death in the EPO group in this CRAS population, and was stopped early
due to safety concerns.14 Trend towards increased death rates were also found in the CREATE
and CHOIR studies of anemic CKD patients without HF treated with EPO, while a meta-analysis
of ESAs in anemic HF patients showed no difference in mortality.17,24,25
We also observed an increasing trend toward CV events, ACS, and HF hospitalizations.
In a similar CRAS population, the NHCT study found an increase in nonfatal myocardial
infarction (MI) and thrombosis in the higher hematocrit group (39% vs. 29%, p=0.001).14 In
other populations, increased CV events have also been reported. In anemic HF patients in RED-
HF, increased thromboembolic events were reported with darbepoetin (13.5% vs 10.0%,
p=0.01), while they failed to find a reduction in their primary outcome of death and
hospitalization for worsening HF.12,26 There have been mixed findings in the anemic CKD

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
population. In the CHOIR trial, darbepoetin was associated with a 34% (p=0.03) increased
composite of death, HF hospitalizations, MI and stroke in anemic CKD patients.17 However,
other studies evaluating anemic, CKD patients observed no increase in CV events. In CREATE
and TREAT, both of which assessed the optimal hemoglobin target in anemic patients with
CKD, there were no significant difference between groups in reduction of CV events.18,24
However, TREAT did find a higher incidence of venous (2.0% vs 1.1%, p=0.02) and arterial
(8.9% vs 7.1%, p=0.04) thromboembolic events with darbepoetin compared with placebo.
The increased risk of stroke has been a recent concern in patients receiving ESA. In our
study, there was a trend towards increased stroke in the EPO group. Although our finding was
not statistically significant, it is consistent with several large trials of ESAs in treating anemia, all
suggesting increasing thrombogenicity concerns when targeting higher hemoglobin or hematocrit
levels.12,14,17,21 Most prominent was the TREAT trial, in which the annualized event rate for
stroke was nearly doubled with darbepoetin alfa (2.1% vs 1.1% in placebo).18
It has been postulated that raising hemoglobin levels may contribute to elevated blood
pressure and vascular thrombosis.7 By elevating hemoglobin, ESA increases platelet
adhesiveness and viscosity, possibly explaining the increased risk of thrombotic and stroke
events in some studies.7,17,24,27 This increased viscosity of the blood from ESA can also
exacerbate uncontrolled hypertension, leading to increased cardiovascular risk.7,27 Although
there are differences between darbepoetin and EPO, with the more potent darbepoetin having a
longer half-life and more efficient iron utilization, increased CV events and death have been
shown with both agents, raising similar concerns.28,29 Without head to head trials between
darbepoetin and EPO, it would be difficult to distinguish which agent has more concerns.
Although the 2009 ACC HF guidelines offer no recommendations for treatment of

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
anemia, separate guidelines exist for anemia of CKD in using ESA to raise hemoglobin
levels.23,30 Neither guideline excludes the use of ESA in patients who have HF along with anemia
of CKD, and so its benefits have been extrapolated for use in the CRAS population. Given the
concerns that our study and others have raised in using ESA to elevate hemoglobin levels,
current HF guidelines should address this topic.
Our study has its limitations. Since this study is retrospective, missing data may be
possible as we rely on data from patient care records. However, since the main study variables
are commonly required for routine medical care, most were available for our use. In addition,
there is no reason to expect missing data to differ systematically between groups. EF values were
missing for some patients in both groups. By including primary and secondary diagnoses in our
diagnostic criteria for capturing HF, we hoped to capture the majority of eligible patients. It is
possible that we may have missed patients with milder forms of HF, but they would be less likely
to have CKD and anemia as the severity of HF is correlated with the development of CKD and
anemia. Although we had unequal baseline characteristics of EPO users and nonusers,
imbalances were adjusted for in the multivariate model. There is still the possibility of residual
confounding. Our ability to document iron supplement use from over-the-counter acquisition is
limited within the VA pharmacy prescription claims system. Therefore, we recognize this
limitation and did not focus on iron use in this study. Although we did not record treated BP or
Hb values, or EPO dose or duration in order to evaluate their impact on outcomes, others have
shown higher dose ESA therapy is associated with higher CV events and mortality regardless of
Hb achieved.14,17,18,19,27,31 Our population was primarily comprised of men, which reduces the
generalizability of our findings to women with HF. Although women and men both have a poor
prognosis after HF diagnosis, median survival for women is 1.5 years longer than for men.32,33

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
However, women with preserved ejection HF have more HF hospitalizations, greater functional
capacity impairment and lower quality of life than men.34,35 Whether women respond differently
to EPO therapy than men is currently unknown. Despite these limitations, our study combines
administrative and clinical data to further address the knowledge gap regarding ESA use in
patients with anemia, HF and CKD, and complements the concerns of the larger body of
evidence in CKD/anemia and HF/anemia-specific populations.
Our findings do not support the use of EPO in patients with CRAS since it was associated
with increased risk of mortality, along with an increased trend in CV events and stroke. Our
study conclusion is concordant with other studies showing negative clinical outcomes with use of
ESA agents in CRAS, CKD and HF populations. Future studies are needed to explore the safety
of ESAs in CRAS patients. Caution is warranted in the use of EPO in CRAS patients, given the
increased risk of mortality and a trend toward increasing CV events from multiple studies.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
Disclosures
This article is not being considered for publication elsewhere, and contents of the paper have not
been previously published. All authors have read and approved the manuscript, with no
conflicts of interest to disclose. This study was funded by the American College of Clinical
Pharmacy Watson Anemia Investigator Development Research Award.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
Acknowledgements
We would like to acknowledge Mindy Chou, PharmD, for assistance with data management,
Carol Collier for data extraction, and Jeffrey Gornbein, PhD, who was a paid statistical
consultant.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
References
1. Herzog CA, Muster HA, Li S, Collins A. Impact of congestive heart failure, chronic kidney
disease, and anemia on survival in the Medicare population. J Card Fail 2004;10(6):467-72.
2. Groenveld HF, Januzzi JL, Damman K, Wijngaarden JV, Hillege HL, Veldhuisen DJ, et al.
Anemia and mortality in heart failure patients: a systematic review and meta-analysis. J Am
Coll Cardiol 2008;52(10):818-27.
3. Ponikowski P, Anker SD, Szachniewicz J, Okonko D, Ledwidge M, Zymlinski R, et al.
Effect of darbepoetin alfa on exercise tolerance in anemic patients with symptomatic chronic
heart failure: a randomized, double-blind, placebo-controlled trial. J Am Coll Cardiol
2007;49(7):753-62.
4. Kazory A, Ross EA. Anemia: the point of convergence or divergence for kidney disease and
heart failure? J Am Coll Cardiol 2009;53(8):639-47.
5. Go AS, Yang J, Ackerson LM, Lepper K, Robbins S, Massie BM, et al. Hemoglobin level,
chronic kidney disease, and the risks of death and hospitalization in adults with chronic heart
failure: the anemia in chronic heart failure: outcomes and resource utilization (ANCHOR)
study. Circulation 2006;113:2713-23.
6. Silverberg DS, Wexler D, Iaina A, Schwartz D. Anaemia management in cardio renal
disease. J Ren Care 2010;36(Suppl 1): 86-96.
7. Anand IS. Anemia and chronic heart failure: implications and treatment options. J Am Coll
Cardiol 2008;52(7):501-11.
8. Blecker S, Paul M, Taksler G, Ogedegbe G, Katz S. Heart failure – associated
hospitalizations in the united states. J Am Coll Cardiol 2013;61(12):1259-67.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
9. Young JB, Abraham WT, Albert NM, Gattis SW, Gheorghiade M, Greenberg BH, et al.
Relation of low hemoglobin and anemia to morbidity and mortality in patients hospitalized
with heart failure (insight from the OPTIMIZE-HF registry). Am J Cardiol 2008;101:223-30.
10. Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, Borenstein J. Anemia is
associated with worse symptoms, greater impairment in functional capacity and a significant
increase in mortality in patients with advanced heart failure. J Am Coll Cardiol 2002;
39(11):1780-86.
11. Maurer MS, Teruya S, Chakraborty B, Helmke S, Mancini D. Treating anemia in older adults
with heart failure with a preserved ejection fraction with epoetin alfa: Single-blind
randomized clinical trial of safety and efficacy. Circ Heart Fail 2013:6:254-263.
12. Swedberg K, Young JB, Anand IS, Cheng S, Desai AS, Diaz R, et al. Treatment of anemia
with darbepoetin alfa in systolic heart failure. N Engl J Med 2013;368:1210-19.
13. Luthi JC, Flanders WD, Burnier M, Burnand B, McClellan WM. Anemia and chronic kidney
disease are associated with poor outcomes in heart failure patients. BMC Nephrol 2006;7:3.
14. Besarab A, Bolton WK, Browne JK, Egrie JC, Nissenson AR, Okamoto DM, et al. The
effects of normal as compared with low hematocrit values in patients with cardiac disease
who are receiving hemodialysis and epoetin. N Engl J Med 1998;339:584-90.
15. Silverberg DS, Wexler D, Blum M, Keren G, Sheps D, Leibovitch E, et al. The use of
subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe,
resistant congestive heart failure improves cardiac and renal function and functional cardiac
class, and markedly reduces hospitalizations. J Am Coll Cardiol 2000;35:1737-44.
16. Silverberg DS, Wexler D, Sheps D, Blum M, Keren G, Baruch R, et al. The effect of
correction of mild anemia in severe, resistant congestive heart failure using subcutaneous

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
erythropoietin and intravenous iron: a randomized controlled study. J Am Coll Cardiol
2001;37:1775-80.
17. Singh AK, Szczech L, Tang KL, Barnhart H, Sapp S, Wolfson M, et al. Correction of anemia
with epoetin alfa in chronic kidney disease. N Engl J Med 2006;355:2085-98.
18. Pfeffer MA, Burdman EA, Chen CY, Cooper ME, Zeeuw DD, Eckardt KU, et al. A trial of
darbepoetin alfa in type 2 diabetes and chronic kidney disease. N Engl J Med
2009;361:2019-32.
19. McCullough PA, Barnhart HX, Inrig JK, Reddan D, Sapp S, Patel UD, et al. Cardiovascular
toxicity of epoetin-alfa in patients with chronic kidney disease. Am J Nephrol 2013; 37:549-
558.
20. US Food and Drug Administration. FDA drug safety communication: modified dosing
recommendations to improve the safe use of erythropoiesis-stimulating agents in chronic
kidney disease. June 24, 2011. Available at:
http://www.fda.gov/Drugs/DrugSafety/ucm259639.htm. Accessed January 13, 2013.
21. Cowper DC, Hynes DM, Kubal JD, Murphy PA. Using administrative databases for
outcomes research: select examples from VA health services research and development. J
Med Syst 1999;23:249-59.
22. Levey AS, Greene T, Kusek JW, Beck GJ. A simplified equation to predict glomerular
filtration rate from serum creatinine. J Am Soc Nephrol 2000;11:155A.
23. NKF K/DOQI Clinical practice guidelines and clinical practice recommendations for anemia
in chronic kidney disease in adults. Am J Kidney Dis 2006;47(5 Suppl 3):S17-57.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
24. Drueke TB, Locatelli F, Clyne N, Eckardt KU, Macdougall IC, Tsakiris D, et al.
Normalization of hemoglobin level in patients with chronic kidney disease and anemia. N
Engl J Med 2006;355:2071-84.
25. Desai A, Lewis E, Solomon S, McMurray J, Pfeffer M. Impact of erythropoiesis-stimulating
agents on morbidity and mortality in patients with heart failure: an updated, post-TREAT
meta-analysis. Eur J Heart Fail 2010;12:936-42.
26. Kleijn L, Westenbrink BD, Meer P. Erythropoietin and heart failure: the end of a promise?
Eur J Heart Fail 2013;15:479-481.
27. Vaziri ND, Zhou XJ. Potential mechanisms of adverse outcomes in trials of anemia
correction with erythropoietin in chronic kidney disease. Nephrol Dial Transplant 2009;
24:1082-88.
28. Shoji S, Inaba M, Tomosugi N, Okuno S, Ichii M, Yamakawa T, et al. Greater potency of
darbepoetin-α than erythropoietin in suppression of serum hepcidin-25 and utilization of iron
for erythropoiesis in hemodialysis patients. Euro J Haem 2013;90:237-44.
29. Singh AK Does TREAT give the boot to ESAs in the treatment of CKD anemia? J Am Soc
Nephrol 2010; 21:2-6.
30. Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, et al. 2009
Focused Update: ACCF/AHA guidelines for the diagnosis and management of heart failure
in adults: a report of the American College of Cardiology Foundation/American Heart
Association Task Force on Practice Guidelines. Circulation 2009;119:1977-2016.
31. Unger EF, Thompson AM, Blank MJ, Temple R. Erythropoiesis-Stimulating Agents – Time
for a Reevaluation. N Engl J Med 2010;362:189-92.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
32. Levy D, Kenchaiah S, Larson MG, et al. Long-term trends in the incidence of and survival
with heart failure. N Engl J Med 2002;347:1397-402.
33. Frazier CG, Alexander KP, Newby LK, et al. Associations of gender and etiology with
outcomes in heart failure with systolic dysfunction: a pooled analysis of 5 randomized
control trials. J Am Coll Cardiol 2007;49:1450-8.
34. Hsich EM, Pina IL. Heart failure in women, a need for prospective data. J Am Coll Cardiol
2009;54:491-8
35. Deswal A, Bozkurt B. Comparison of morbidity in women versus men with heart failure and
preserved ejection fraction. Am J Cardiol 2006;97:1228-31.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21
Table 1. Patient Baseline Characteristics
Characteristic EPO
(n=213)
Control
(n=1845) P-Value
Age (mean±SD , yr) 71.9±12 73.2±11 0.15
Sex (% M) 97.2 96.2 <0.45
SCr (mean±SD, g/dL) 3.2±2.4 2.1±1.7 <0.0001
eGFR (mean±SD, mL/min) 31.7±15 43.4±13 <0.0001
BUN (mean±SD, g/dL) 44.1±20 32.2±17 <0.0001
Hgb (mean±SD, g/dL) 10.5±1 11.1±0.89 <0.0001
Hct (mean±SD, g/dL) 33±5 35±4 <0.0001
SBP (mean±SD, mmHg) 133±23 128±22 <0.01
DBP (mean±SD, mmHg) 68±13 68±13 0.98
EF (mean±SD, %) 50.4±15 47.3±17 0.052
Comorbidities (%)
Hypertension 76.1 68.3 0.02
Diabetes 53.1 47.2 0.11
CAD 37.6 37.6 0.99
Cerebrovascular disease 14.6 13.7 0.75
Atrial fibrilllation 17.4 18.2 0.85
COPD 34.2 28.9 0.11
Cancer 32.4 25.9 0.04
Dialysis 5.2 1.1 <0.01
Renal Clinic (%) 69.5 36.9 <0.0001

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
22
Medications (%)
ASA 31.0 23.5 0.02
ACEI 32.9 39.1 0.08
ARB 17.4 12.0 0.03
Beta-blocker 54.0 47.4 0.07
Digoxin 7.0 10.5 0.12
Diuretic 50.2 46.4 0.29
Iron 5.6 0.16 <0.0001
Hydralazine/nitrates 10.8 3.1 <0.0001
Statin 48.4 42.6 0.12
Aldosterone
antagonist
8.5 9.3 0.70
eGFR = estimated glomerular filtrate rate; BUN = blood urea nitrogen; Hgb = Hemoglobin; EF = ejection fraction; CAD = coronary artery disease; COPD = chronic obstructive pulmonary disease; ASA = aspirin; ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; EPO = erythropoietin; SBP = systolic blood pressure; DBP = diastolic blood pressure

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
23
Table 2. Unadjusted (Crude) Clinical Outcomes of Death and Cardiovascular Events
EPO Treatment (n=213) Control (n=1846)
Event n (%) n % P-value
Death 72 33.8 363 19.7 <0.0001
Stroke 48 22.5 338 18.3 0.14
ACS 40 18.8 199 10.8 0.001
HF 102 47.9 761 41.2 0.07
All-cause
hospitalization
133 62.4 929 50.4 <0.001
ACS = acute coronary syndromes; EPO = erythropoietin; HF = heart failure hospitalizations

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
24
Table 3. Adjusted Risk of Cardiovascular Events/Death
Variable HR (95% CI) P-value
EPO (Unadjusted) 1.19 (1.00-1.41) 0.04
EPO (Adjusted) 1.16 (0.96-1.40) 0.12
Age (per year) 1.01 (1.002-1.01) <0.01
eGFR (per unit) 1.00 (0.99-1.01) 0.86
BUN (per unit) 1.003 (1.001-1.006) 0.047
Hgb <10g/dL 1.47 (1.25-1.75) <0.0001
SBP (per mmHg) 1.00 (1.00 – 1.00) 0.90
DBP (per mmHg) 1.00 (1.00 – 1.01) 0.66
EF ≤50% 1.02 (1.01-1.02) <0.0001
Hypertension 0.85 (0.75-0.97) 0.02
Diabetes 0.97 (0.86 – 1.09) 0.61
CAD 1.19 (1.04-1.36) 0.01
Cerebrovascular disease 2.03 (1.75-2.35) <0.0001
Atrial fibrillation 1.30 (1.12-1.50) <0.001
COPD 1.59 (1.41-1.80) <0.0001
Cancer 1.12 (0.98 – 1.27) 0.09
Dialysis 1.39 (0.88 – 2.19) 0.16
ASA 1.23 (1.08-1.41) <0.01
ACEI 1.12 (0.99-1.26) 0.07
Beta-Blocker 1.07 (0.94 – 1.21) 0.30
Digoxin 1.16 (0.96-1.39) 0.14

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
25
Diuretic 1.35 (1.19-1.53) <0.0001
Hydralazine/nitrates 1.21 (1.06-1.37) <0.01
Aldosterone antagonist 1.16 (0.96-1.40) 0.12
Statin 0.94 (0.83 – 1.06) 0.32
eGFR = estimated glomerular filtrate rate; BUN = blood urea nitrogen; Hgb = Hemoglobin; EF = ejection fraction; CAD = coronary artery disease; COPD = chronic obstructive pulmonary disease; ASA = aspirin; ACEI = angiotensin converting enzyme inhibitor; EPO = erythropoietin; SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = hazard ratio; CI = confidence interval

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
26
Table 4. Adjusted Risk of Mortality Variable HR (95% CI) P-value
EPO (Unadjusted) 1.62 (1.26-2.09) <0.001
EPO (Adjusted) 1.40 (1.06-1.85) 0.02
Age (per year) 1.02 (1.01-1.03) <0.001
eGFR (per unit) 1.00 (0.99-1.00) 0.32
BUN (per unit) 1.01 (1.002-1.013) <0.01
Hgb <10g/dL 1.72 (1.34-2.20) <0.0001
SBP (per mmHg) 0.99 (0.99-1.00) 0.03
DBP (per mmHg) 1.01 (1.00-1.02) 0.07
EF ≤50% 1.39 (1.10-1.75) <0.01
Hypertension 0.72 (0.58-0.88) <0.01
Diabetes 0.89 (0.72-1.10) 0.27
CAD 1.05 (0.84-1.31) 0.68
Atrial fibrillation 1.20 (0.95-1.51) 0.13
COPD 1.88 (1.54-2.30) <0.0001
Cancer 1.50 (1.23-1.84) <0.0001
Dialysis 1.08 (0.56-2.10) 0.82
ACEI 0.89 (0.72-1.10) 0.29
Beta-Blocker 0.77 (0.62-0.95) 0.01
Digoxin 1.28 (0.95-1.73) 0.11
Aldosterone antagonist 0.93 (0.66-1.30) 0.67
Statin 0.76 (0.61-0.93) <0.01
eGFR = estimated glomerular filtrate rate; BUN = blood urea nitrogen; Hgb = Hemoglobin; EF = ejection fraction; CAD = coronary artery disease; COPD = chronic obstructive pulmonary disease; ASA = aspirin; ACEI = angiotensin converting enzyme inhibitor; EPO = erythropoietin; SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = hazard ratio; CI = confidence interval

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Figure 1: All-Cause Mortality – Monthly percentage of unadjusted and adjusted rates of all-cause mortality in CRAS patients
receiving EPO or no EPO

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
Figure 2: Composite of Cardiovascular Events/Death – Monthly percentage of unadjusted and adjusted rates of composite of
cardiovascular events/death in CRAS patients receiving EPO or no EPO
CRAS: Cardio-renal-anemia syndrome EPO= erythropoietin; HR= Hazard Ratio