Embed Size (px)
Citation preview

Clinical outcomes of a specialised inpatient unit foradults with mild to severe intellectual disability andmental illnessjir_1213 60..69
Y. Lunsky,1,2 S. E. White,1 A. M. Palucka,1 J. Weiss,1,3 S. Bockus1 & T. Gofine4
1 Centre for Addiction and Mental Health,Toronto, Ontario, Canada2 University of Toronto,Toronto, Ontario, Canada3 York University,Toronto, Ontario, Canada4 Whitby Mental Health Centre,Whitby, Ontario, Canada
Abstract
Background Limitations of general psychiatric ser-vices have led to the development of specialisedpsychiatric programmes for patients with intellec-tual disability (ID) and mental health needs. Fewstudies have examined treatment outcomes ofspecialised inpatient units, and no studies haveexplored how the effects of intervention may differfor individuals at varying levels of cognitive ability.The present study examined clinical outcomes ofinpatients with mild ID in contrast to inpatientswith moderate to severe ID within the same service.Method Thirty-three patients (17 with mild ID and16 with moderate to severe ID) discharged between2006 and 2008 from a specialised inpatient unit inCanada for adults with ID and mental illness werestudied. In addition to examining change in scoreson clinical measures, outcomes with regard tolength of stay, diagnostic change, residential changeand re-admission to hospital were explored.Results Both groups demonstrated clinicalimprovement from admission to discharge.
However, only patients with mild ID demonstratedimprovements on the Global Assessment ofFunctioning.Conclusions This study is one of the first to con-sider outcomes of higher and lower functioningindividuals with ID on a specialised inpatient unit.Results suggest that outcomes may be different forthese groups, and some clinical measures may bemore sensitive to changes in patients with moresevere disabilities.
Keywords inpatient, intellectual disability, mentalhealth, psychiatric disorders
There has been increasing recognition that althoughmany individuals with intellectual disability (ID)access mainstream psychiatry services, a certainsubgroup of individuals requires and benefits fromspecialised inpatient care. Surprisingly, althoughmany papers have argued this, only a handful ofstudies have provided outcome data on such pro-grammes from around the world (see Chaplin 2006,2009 for review/critique). In our review of the lit-erature, fewer than 10 papers have been publishedin the past 15 years reporting outcomes of psychiat-ric inpatients served by specialised units for adultswith ID and mental illness. Earlier papers (e.g.,Reid et al. 1984; Day 1985; Ballinger et al. 1991;
Correspondence: Dr Yona Lunsky, Centre for Addiction andMental Health, Dual Diagnosis Program, 501 Queen St. West,Toronto, Ontario, Canada M5V2B4 (e-mail: [email protected]).
Journal of Intellectual Disability Research doi: 10.1111/j.1365-2788.2009.01213.x
volume 54 part 1 pp 60–69 january 201060
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

Hurst et al. 1994) were descriptive in nature anddid not include standardised outcome measures.More recent studies have provided pre- and post-treatment measures of client outcomes (van Minnenet al. 1997; Raitasuo et al. 1999; Tajuddin et al.2004; Xenitidis et al. 2004; Hall et al. 2006) andsome have included comparison groups (vanMinnen et al. 1997; Xenitidis et al. 2004; Hall et al.2006). Two additional studies of individuals in aspecialised day hospital setting also used pre- andpost-intervention measures (Carminati et al. 2005;Shedlack et al. 2005).
Raitasuo et al. (1999) followed 40 consecutiveinpatients admitted to a specialised unit in Finland,31 of whom (78%) were diagnosed with mild ID orborderline intellectual functioning. They offered‘need adapted treatment’, where treatment planswere individualised for each patient and caregiver.In addition to regular therapy meetings withpatient, caregivers and the inpatient team, patientsparticipated in occupational therapy, group therapy,adaptive daily living skill groups and pharmaco-therapy. Aftercare services were available to allpatients, with the option of re-admission for dete-rioration. With regard to outcome, patients’ scoreson the Brief Psychiatric Rating Scale reduced atdischarge and were maintained at 6-month follow-up. Caregiver ratings on a visual analogue scalesupported that they perceived patients to haveimproved from admission to discharge as well.
Hall et al. (2006) compared community-basedpatients to inpatients with mild ID and psychiatricdisorder at three points in time on a number ofclinical outcome measures assessing psychiatricsymptoms, risk, need and level of functioning. Theyfollowed inpatients at admission, discharge and 6
months post admission. Outcome data includedratings by caregivers, clients and hospital staff. The19 inpatients showed significant improvements overtime on the Global Assessment of Functioning(GAF), the Health of the Nation Outcome Scalesfor people with Learning Disabilities and theThreshold Assessment Grid (TAG). The unmetneeds of inpatients decreased over time accordingto staff and patient ratings on the CamberwellAssessment of Need for Adults with Developmentaland Intellectual Disabilities – short version, andaccording to staff, met needs increased followingtreatment.
Xenitidis et al. (2004) evaluated 33 individuals(29 with mild ID) admitted to a specialist inpatientunit over a 35-month period, using the PsychiatricAssessment Schedule for Adults with Developmen-tal Disabilities Checklist, the Disability AssessmentScale, the GAF and the TAG. Inpatients showedimprovement on each of the four measures atdischarge.
Tajuddin et al. (2004) conducted a retrospectiveanalysis on the 72 adults with ID treated in a spe-cialised inpatient unit over a 24-month period. Thisstudy included the largest subgroup of individualsin the moderate to severe range of all the studiesreviewed (41.7%). Reiss Screen for MaladaptiveBehavior total scores were significantly lower at dis-charge than at admission for the group. Seventy-sixper cent of individuals returned to their originalresidence. In the 2-year time period of the study,only 22% of individuals discharged werere-admitted to the unit.
Van Minnen et al. (1997) examined hospital-based and home-based treatment for clients withID and psychiatric disorder referred to their 48-bedinpatient unit. Patients were referred over a19-month period, and were assessed at admissionand at 7-week intervals over a 28-week period usingthe Reiss Screen, Psychopathology Inventory forMentally Retarded Adults and the Global RatingScale for Improvement. Although the authors com-pared scores on these measures between groups ateach time period and found that, overall, the groupswere equivalent in their ratings, they did notexamine whether either group improved signifi-cantly with treatment.
Each of the papers reviewed above argued thatsome type of specialised service was required toserve the most vulnerable of clients. Specialisedinpatient services may lead to fewer out of areaplacements, although treatment may require alonger length of stay (LOS) than what is seen inmainstream psychiatry (Sovner et al. 1995; Xenitidiset al. 2004). Although the benefits of specialisedinpatient programmes should apply across levels ofdisability, the outcome studies reviewed abovefocused primarily on individuals with mild disabil-ity. In the one reviewed study where lower function-ing individuals were included (Tajuddin et al.2004), their outcome was not analysed separatelyfrom other patients. Outcome research for people
61Journal of Intellectual Disability Research volume 54 part 1 january 2010
Y. Lunsky & A. M. Palucka • Outcomes of a specialised inpatient unit
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

with more severe disabilities using specialised ser-vices is especially important given that general inpa-tient services are most underutilised by this group(Chaplin 2009). Unfortunately, few studies havereported on the benefits of such units for thoseindividuals, or compared outcomes of those withmore severe to less severe ID.
In Ontario (Canada’s most populated province of11 million individuals), five inpatient units currentlyoperate within tertiary level mental healthcare facili-ties that are targeted specifically towards inpatientswith ID and mental health needs. These pro-grammes differ from other inpatient units in termsof the level of expertise in ID, as well as staffcomplement (high ratio and interdisciplinary), andtypes of individual and group therapy available (seeMorris 2005 for detailed summary of programmecharacteristics). To date, no studies have examinedclinical outcomes of patients in these units in aCanadian context.
The purpose of this paper is to describe the clini-cal presentation of all individuals discharged from aCanadian specialised dual diagnosis inpatient unitat the Centre for Addiction and Mental Health(CAMH) between 2006 and 2008, and to report onpatient outcomes in terms of symptom improve-ment, change of diagnosis, LOS, place of dischargeand re-admission rates. Because the unit admitsboth individuals with mild disabilities and thosewith more severe disabilities, a secondary purposeof this paper was to compare the outcomes of thesetwo groups.
Method
Description of the specialised unit
Opened in 1997, the dual diagnosis inpatient unit atthe CAMH is a 15-bed, locked unit. It has a capac-ity for 12 to 15 inpatients of both genders, aged 16
years and older, and is exclusively for patients withan ID and mental health problem. Inpatient admis-sion is offered as part of a continuum of care. Whenpossible, admissions to the unit are planned by wayof triage through a parallel interdisciplinary outpa-tient consultation service. Clients are typically con-sidered for admission when they are in need ofintensive interdisciplinary assessment and/or theirrecommended treatment cannot easily be completed
in the community. In addition, comorbid medicalconcerns may exist for individuals offered inpatientadmission, which require a high level of observationand clinical safety. The interdisciplinary clinicalteam is led by a psychiatrist, and includes psychol-ogy, social work, nursing, recreation therapy, behav-iour therapy and occupational therapy. Within 2
weeks of admission, the team conducts a clinicalplanning meeting, at which time, the AberrantBehavior Checklist (ABC) and the Reiss Screen forMaladaptive Behavior are completed by the primarynurse(s) who works most closely with the client.The psychiatrist, with team input, determines adiagnosis and GAF score. When it is evident to theteam that the patient has improved clinically and isready for discharge, he or she is re-assessed usingthe Reiss Screen, ABC and GAF, in the samemanner as admission, and ideally, by the sameraters.
While on the unit, patients receive interdiscipli-nary assessment and intervention, and there areoften significant changes made in the type anddosage of psychotropic medications. Psychosocialinterventions include relaxation training, angermanagement, counselling, recreation therapy, socialskills and community skills training, and can beadministered in a group or individual context. Car-egivers from community settings (family and paidstaff who will support the patient once discharged)meet regularly with the inpatient team to discusspatient progress and goals for discharge; the outpa-tient consultation programme assists with the tran-sition process and provides time limited post-discharge support in the community. On someoccasions, patients are assessed as ready for dis-charge, but because of a lack of available commu-nity placements, their reintegration into thecommunity can be delayed.
Participants
Thirty-seven inpatients were discharged from thespecialised dual diagnosis unit at the CAMHbetween January 2006 and December 2008. Fourpatients were discharged prematurely, and weretherefore excluded from analyses (see Fig. 1).Although there were some changes in staffing (pri-marily nursing staff) within that time frame, thenurse manager, psychiatrist, psychologist, behaviour
62Journal of Intellectual Disability Research volume 54 part 1 january 2010
Y. Lunsky & A. M. Palucka • Outcomes of a specialised inpatient unit
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

therapist, recreation therapist and occupationaltherapist were consistent. Characteristics of the finalsample (n = 33) are presented in Table 1. Upon dis-charge, 51.5% (n = 17) of the sample was assessedwith mild ID, 42.4% (n = 14) with moderate IDand 6.1% (n = 2) with severe ID.
Prior to admission, 19 patients (57.6%) lived ingroup homes, three (9.1%) resided in SupportedIndependent Living and five (15.2%) with family.Two patients (6.1%) lived alone, three (9.1%) inboarding homes or long-term care facilities and one(3.0%) in a correctional treatment facility for youth.At the time of admission, none of the patients weregainfully employed. Twenty-two patients (67.7%)had previously exhibited violent behaviour towardsothers, 15 of these within the year preceding theiradmission. Also, four patients (12.1%) had a historyof sexual violence. Some patients also had a historyof self-injurious behaviour; nine (27.3%) hadattempted self-injury within the year before theiradmission, and an additional five (15.2%) had doneso more than 1 year prior. Of these 14 patients, four(12.1%) had engaged in these behaviours with theperceived attempt to kill themselves. In terms ofrecent life events, 13 of the 33 patients (39.4%) hadexperienced the death of a close family member orfriend (for 12 of these, this occurred more than 1
year prior to admission). Also of note is the propor-tion of patients who had been victims of physical(7; 21.2%), emotional (9; 27.3%) and sexual (10;
30.2%) assault or abuse in the past. Of the 16
patients with previous legal involvement, four wereadmitted under Ontario Review Board status, asthey were found unfit to stand trial or were notcriminally responsible because of their ID.
Measures
The following measures of clinical outcome wereused:
Global Assessment of Functioning Scales (AmericanPsychiatric Association, 1994)
This single rating scale evaluates overall function-ing, in terms of ‘psychological, social and occupa-tional functioning on a hypothetical continuum ofmental health-illness’, and ranges from 1 to 100.This scale correlates with other measures of symp-toms and social functioning, and has good inter-rater reliability and convergent validity. It has beenfound to be useful in measuring symptom changefollowing clinical intervention in some samples (i.e.Startup et al. 2002; Shedlack et al. 2005). It has alsobeen criticised in the ID population because of‘floor effects’ (Oliver et al. 2003; Shedlack et al.2005).
Reiss Screen for Maladaptive Behavior (Reiss 1986)
Comprising 38 items, this measure is used as ascreening tool for mental health problems in indi-viduals with mild, moderate or severe ID. Thisscreen is independently completed by two or moreraters, who rate each item on a 3-point scale (‘noproblem’, ‘a problem’ or ‘a major problem’). Thescale demonstrates good internal reliability, inter-rater reliability and validity (Reiss 1986; Prout1993). The scale provides a 26-item total score, andincludes eight sub-scales and six special items, eachwith clinical cut-offs that have been validated. Intheir study reviewed above, Tajuddin et al. (2004)cite the ‘usefulness of the Reiss scale in measuringthe outcome of psychiatric intervention’ in theirsample.
Aberrant Behavior Checklist (Aman & Singh 1986)
This scale was originally developed to assess treat-ment effects on behaviour, and includes 58 items,
37 inpatients
1 discharged due to court order
33 participants
2 discharged against clinical
recommendation
1 discharged due to medical
emergency
Figure 1 Inpatient flow.
63Journal of Intellectual Disability Research volume 54 part 1 january 2010
Y. Lunsky & A. M. Palucka • Outcomes of a specialised inpatient unit
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

categorised into five sub-scales: Irritability, Agitationand Crying (15 items); Lethargy and Social With-drawal (16 items); Stereotypic Behavior (7 items);Hyperactivity and Noncompliance (16 items) andInappropriate Speech (4 items). Possible ratings foreach item range from 0 (not a problem at all) to 3
(the problem is severe in degree). The ABC sub-scales have been found to have high internal consis-tency (mean alpha = 0.91) and test–retest reliability(mean r = 0.98), good inter-rater reliability (meanr = 0.63), and moderate correlations with measuresof adaptive behaviour (mean r = 0.60) (Aman et al.1985). Two prior studies (Carminati et al. 2005;
Shedlack et al. 2005) have examined ABC scoresprior to and following partial hospitalisation pro-grammes for adults with ID and psychiatric needs,and found reductions in scores following treatment.Shedlack et al. (2005) also reported that the ABCis more sensitive to change than standard GAFscores.
Procedure
Retrospective chart reviews for patients dischargedbetween January 2006 and December 2008 wereconducted. Charts were reviewed with respect to:
Table 1 Demographic characteristics (n = 33)
Mild Moderate/Severe Totaln (%) n (%) n (%)
Gender – male 6 (35.5) 8 (50.0) 14 (42.4)Age [mean (SD)] 36.06 (11.18) 33.38 (6.98) 35.19 (9.15)Ethnic group
White 14 (82.4) 14 (87.5) 28 (84.8)Non-white 3 (17.6) 2 (12.5) 5 (15.2)Black 2 (11.8) 1 (6.3) 3 (9.1)Mixed – 1 (6.3) 1 (3.0)Middle Eastern 1 (5.9) – 1 (3.0)
English as a second language for patient and/or parents 5 (29.4) 4 (25.0) 9 (27.3)Patient either visual minority or ESL 6 (35.3) 6 (37.5) 12 (36.3)Forensic involvement – past or current 11 (64.7) 5 (31.3) 16 (48.5)Primary reason for referral
Aggressive/challenging behaviour 5 (29.4) 8 (50.0) 13 (39.4)Clarification of Axis I/II diagnosis 5 (29.4) 3 (18.8) 8 (24.2)Threat/danger to self or others 1 (5.9) 3 (18.8) 4 (12.1)Support/crisis planning required – 2 (12.5) 2 (6.1)Involvement with legal system 2 (11.8) – 2 (6.1)Review of medication 2 (11.8) – 2 (6.1)Other reasons 2 (11.8) – 2 (6.1)
Medical diagnosesSeizure disorder 3 (17.6) 1 (6.3) 4 (12.1)Genetic syndromes 2 (11.8) 4 (25.0) 6 (18.2)Hearing/visual impairment 2 (11.8) 3 (18.8) 5 (15.2)Gastrointestinal condition 1 (5.9) 3 (18.8) 4 (12.1)Bone/joint condition 4 (23.5) – 4 (12.1)Any comorbid medical condition 9 (52.9) 7 (43.8) 16 (48.5)
Axis I diagnosis (discharge)Autism/PDD-NOS 4 (23.5) 7 (43.8) 11 (33.3)Psychotic disorder 8 (47.1) 1 (6.3) 9 (27.3)Mood disorder 3 (17.6) 2 (12.5) 5 (15.2)Anxiety disorder – – –No Axis I diagnosis 1 (5.9) 6 (37.5) 7 (21.2)
English as a second language, pervasive developmental disorder-Not otherwise specified.
64Journal of Intellectual Disability Research volume 54 part 1 january 2010
Y. Lunsky & A. M. Palucka • Outcomes of a specialised inpatient unit
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

age upon admission, gender, referral source, reasonsfor referral, place of residence, psychiatric diagnosesupon admission and discharge, level of ID, medicaldiagnoses, and admission and discharge scores onthe Reiss, ABC and GAF. Baseline data were col-lected by nursing staff within 2 weeks of each indi-vidual’s admission, and patients were re-assessedprior to discharge from the unit.
Data analysis
This study was approved by the Research EthicsBoard at the CAMH. All statistical analyses wereconducted using the Statistical Package for SocialSciences (SPSS) for Windows, version 15.0 (SPSS2007). For all analyses that examined relations toIQ, individuals with moderate and severe ID werecollapsed into one group, yielding two comparisongroups [Mild (n = 17) and Moderate/Severe(n = 16)].
Results
Demographics and behavioural history
Patients in the Mild ID group were more likely tobe diagnosed with psychotic disorder at discharge(P < 0.01), and to have previously engaged in self-injurious behaviour with the intent to kill them-selves (P < 0.05). There was a trend for a greater
likelihood of previous legal involvement (P = 0.055)and emotional abuse (P = 0.065) in the Mild IDgroup. The Moderate/Severe group was more likelyto have a history of violence towards others(P < 0.05). No other between-group differences indemographics or behavioural history were found.
Measures of outcome
Global Assessment of Functioning scores at bothadmission and discharge were available for 31 of the33 patients in our sample (one patient was admittedprior to the regular implementation of GAF scoresin our programme, and another was not assessedusing this scale at discharge). To assess GAF scorechange, a two-way repeated measures anova wascalculated, with GAF scores as the two-level within-subjects factor, and degree of ID (Mild, Moderate/Severe) as the two-level between-subjects factor.Results indicated a significant GAF ¥ IQ interac-tion, F(1, 29) = 5.37, P = 0.03, h2 = 0.16. Post hocanalyses of the interaction revealed a significantimprovement in GAF scores for patients with mildID (mean difference = 11.31, P < 0.001) andminimal improvement for individuals withmoderate/severe ID (mean difference = 2.13,P = 0.46). Individuals with mild ID tended to havehigher GAF scores than individuals with moderate/severe ID at admission (mean difference = 7.19,P = 0.07), and a greater difference at discharge(mean difference = 16.37, P < 0.001) (see Fig. 2). In
Figure 2 Change in GAF scores based on IQ. GAF, Global Assessment of Functioning.
65Journal of Intellectual Disability Research volume 54 part 1 january 2010
Y. Lunsky & A. M. Palucka • Outcomes of a specialised inpatient unit
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd
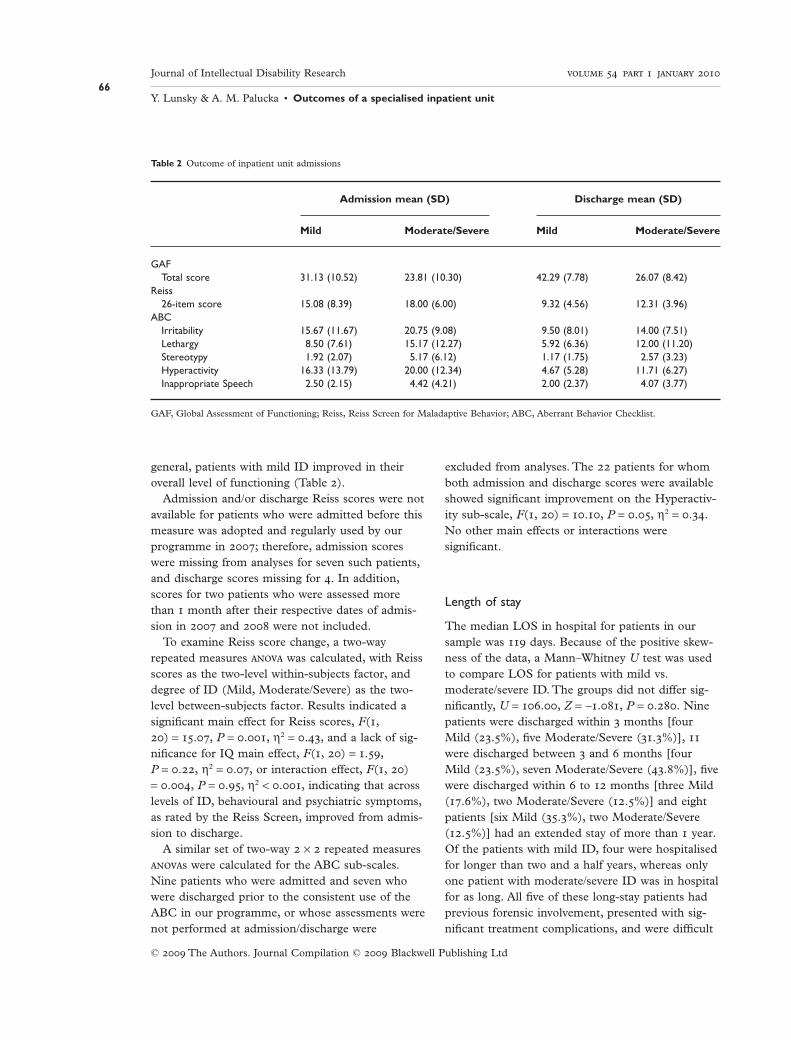
general, patients with mild ID improved in theiroverall level of functioning (Table 2).
Admission and/or discharge Reiss scores were notavailable for patients who were admitted before thismeasure was adopted and regularly used by ourprogramme in 2007; therefore, admission scoreswere missing from analyses for seven such patients,and discharge scores missing for 4. In addition,scores for two patients who were assessed morethan 1 month after their respective dates of admis-sion in 2007 and 2008 were not included.
To examine Reiss score change, a two-wayrepeated measures anova was calculated, with Reissscores as the two-level within-subjects factor, anddegree of ID (Mild, Moderate/Severe) as the two-level between-subjects factor. Results indicated asignificant main effect for Reiss scores, F(1,20) = 15.07, P = 0.001, h2 = 0.43, and a lack of sig-nificance for IQ main effect, F(1, 20) = 1.59,P = 0.22, h2 = 0.07, or interaction effect, F(1, 20)= 0.004, P = 0.95, h2 < 0.001, indicating that acrosslevels of ID, behavioural and psychiatric symptoms,as rated by the Reiss Screen, improved from admis-sion to discharge.
A similar set of two-way 2 ¥ 2 repeated measuresanovas were calculated for the ABC sub-scales.Nine patients who were admitted and seven whowere discharged prior to the consistent use of theABC in our programme, or whose assessments werenot performed at admission/discharge were
excluded from analyses. The 22 patients for whomboth admission and discharge scores were availableshowed significant improvement on the Hyperactiv-ity sub-scale, F(1, 20) = 10.10, P = 0.05, h2 = 0.34.No other main effects or interactions weresignificant.
Length of stay
The median LOS in hospital for patients in oursample was 119 days. Because of the positive skew-ness of the data, a Mann–Whitney U test was usedto compare LOS for patients with mild vs.moderate/severe ID. The groups did not differ sig-nificantly, U = 106.00, Z = -1.081, P = 0.280. Ninepatients were discharged within 3 months [fourMild (23.5%), five Moderate/Severe (31.3%)], 11
were discharged between 3 and 6 months [fourMild (23.5%), seven Moderate/Severe (43.8%)], fivewere discharged within 6 to 12 months [three Mild(17.6%), two Moderate/Severe (12.5%)] and eightpatients [six Mild (35.3%), two Moderate/Severe(12.5%)] had an extended stay of more than 1 year.Of the patients with mild ID, four were hospitalisedfor longer than two and a half years, whereas onlyone patient with moderate/severe ID was in hospitalfor as long. All five of these long-stay patients hadprevious forensic involvement, presented with sig-nificant treatment complications, and were difficult
Table 2 Outcome of inpatient unit admissions
Admission mean (SD) Discharge mean (SD)
Mild Moderate/Severe Mild Moderate/Severe
GAFTotal score 31.13 (10.52) 23.81 (10.30) 42.29 (7.78) 26.07 (8.42)
Reiss26-item score 15.08 (8.39) 18.00 (6.00) 9.32 (4.56) 12.31 (3.96)
ABCIrritability 15.67 (11.67) 20.75 (9.08) 9.50 (8.01) 14.00 (7.51)Lethargy 8.50 (7.61) 15.17 (12.27) 5.92 (6.36) 12.00 (11.20)Stereotypy 1.92 (2.07) 5.17 (6.12) 1.17 (1.75) 2.57 (3.23)Hyperactivity 16.33 (13.79) 20.00 (12.34) 4.67 (5.28) 11.71 (6.27)Inappropriate Speech 2.50 (2.15) 4.42 (4.21) 2.00 (2.37) 4.07 (3.77)
GAF, Global Assessment of Functioning; Reiss, Reiss Screen for Maladaptive Behavior; ABC, Aberrant Behavior Checklist.
66Journal of Intellectual Disability Research volume 54 part 1 january 2010
Y. Lunsky & A. M. Palucka • Outcomes of a specialised inpatient unit
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

to discharge to an environment willing and able tosupport them.
Other outcomes
Diagnostic change
Based on extensive case review by the inpatient psy-chologist, as well as comprehensive psychologicaltesting, seven patients (21.2%) received a change intheir ID diagnosis by discharge, four of whom(12.1%) were diagnosed with a less severe form ofID (moderate to mild) than was recorded in theirfile at admission. Further, three new cases (9.1%) ofAutistic Disorder/pervasive developmental disorder-not otherwise specified were diagnosed in patientspreviously diagnosed with mood and anxiety disor-ders (two Mild, one Moderate/Severe), and fivepatients (15.2%) admitted with a diagnosis of eitherschizophrenia or psychotic disorder NOS had thatdiagnosis removed at discharge (three Mild, twoModerate/Severe). In the latter case, these fivepatients had exhibited psychotic symptoms prior toadmission, as part of a transient reaction to situa-tions of extreme anxiety, grief or psychological dis-tress while in the community.
Changes in housing
For 11 individuals (six Mild, five Moderate/Severe),following inpatient admission, a new residentialsetting was sought. These patients were placed inmore supportive environments, moving from livingindependently or with family to group homes ortransitional treatment homes. One patient movedfrom a treatment home in the youth sector to theadult sector, and one patient moved from a nursinghome to a group home.
Re-admissions
Following discharge, seven individuals werere-admitted to the inpatient unit during the studyperiod (five Mild, two Moderate/Severe). Patientswere re-admitted within an average of 134 days(SD = 103.3) from the previous discharge. With theexception of one re-admitted patient who was stillon the unit at the time of this report, the medianlength of re-admission was 30 days. Of thesepatients, four were re-admitted because of aggres-sive behaviour towards others and/or property
destruction. Other reasons for re-admissionincluded self-injury and behaviours that created asignificant risk for self-harm, as well as increasedparanoia and general psychiatric deterioration. Forthese individuals, the re-admission allowed for staffto re-assess their mental status and make adjust-ments to the home setting as needed. The adjust-ments at home were particularly relevant to fourindividuals (three Mild, one Moderate/Severe), whowere re-admitted to hospital because supports inplace were inadequate. This was arguably due, ineach case, to the need for greater understanding ofclients’ behavioural and mental health challenges onthe part of caregiving staff in the community.
Discussion
This is one of the first studies to consider outcomesof higher and lower functioning individuals with IDin a specialised dual diagnosis inpatient unit. Thetwo groups differed in some respects at admission(psychiatric diagnosis, forensic involvement) butboth groups benefited from their inpatient stay. TheGAF was not sensitive enough to detect change inindividuals with more severe disability, but both theReiss Screen and the Hyperactivity sub-scale of theABC showed significant improvement for bothgroups from admission to discharge. Individuals inboth groups were equally likely to be re-admittedand to change residence from admission to dis-charge, and the groups did not differ in LOS.
This paper demonstrates that individuals withmild and more severe disability can be servedwithin the same programme. A larger proportion ofinpatients had more severe disability than what hasbeen reported in other studies, perhaps because it isa clear mandate of our programme to serve suchindividuals. Of course, there are complexities inserving both groups on the same unit, and somesafety concerns. Every admission is considered inlight of who is on the unit at the time, and howsuch an admission will impact the milieu. In addi-tion, a range of psychosocial interventions need tobe available on a daily basis, with the understandingthat certain interventions will be more utilised bysome patients than by others, depending on theirfunctioning level.
The GAF continues to be an important measureof functioning within the broader psychiatric
67Journal of Intellectual Disability Research volume 54 part 1 january 2010
Y. Lunsky & A. M. Palucka • Outcomes of a specialised inpatient unit
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

community and is a requirement within ourhospital, even though it was only sensitive enoughto detect changes in overall functioning for thosewith more mild disability. There was minimalimprovement in GAF scores for clients with moder-ate to severe ID in our sample, which is likelyreflective of the limitations of using the GAF withindividuals who present with very significant social,occupational and psychological impairmentsbecause of their ID (Oliver et al. 2003; Shedlacket al. 2005). The Reiss Screen, in contrast, coulddetect changes in both groups, suggesting that itmay be a more appropriate and detailed measure ofproblem areas for patients with ID. Shedlack et al.(2005) and Carminati et al. (2005) also reportedthat the ABC detected significant differences intheir day hospital clients with ID. Our study failedto detect these differences with the exception ofscores on the Hyperactivity sub-scale.
The median LOS for mild clients was 203 daysand, for moderate/severe clients, was 118 days.These numbers are higher than what was reportedin hospital programmes in the UK and Sweden[23.2 weeks (Xenitidis et al. 2004), 8 weeks (Hallet al. 2006), 2.91 months (Raitasuo et al. 1999),70.8 days (Tajuddin et al. 2004)]. This may be due,in part, to 39.4% of our sample staying in hospitalfor more than 6 months, and four individuals withmild ID being in hospital for an average of 1319
days. Rather than seeing shorter LOS in individualswith milder cognitive impairments as was reportedin the studies cited above, in our sample patientswith mild ID were as likely, if not more likely, tohave prolonged admissions. Individuals with ahistory of forensic involvement had the most diffi-cult time finding appropriate discharge placements,and more of those individuals had mild disability(11 Mild vs. five Moderate/Severe).
Discharges for patients in both groups are likelymore complicated in Canada than in other coun-tries like the UK, where there are local ‘communitylearning disability teams’, as well as health profes-sionals with specialised training in ID. Communitymental health services for people with ID inOntario are limited in comparison, and preparingcommunity teams to reintegrate inpatient clients isa more demanding enterprise. Our programmaticresponse to this shortage in appropriate service hasbeen to adopt a stronger continuity of care model
between our inpatient and outpatient services. Inthis way, our programme is better able to supportreintegration beyond the point of discharge, withthe option of re-admission. It would be importantfor us to evaluate LOS as well as re-hospitalisationrates of clients in the future, to see whether agreater emphasis on continuity of care is helping toreduce inpatient LOS.
There are a number of limitations in this studythat need to be taken into account. First, thesample size was relatively small, and statisticalanalyses lacked the power to reflect significantchanges in admission and discharge scores, or dif-ferences between patient groups. Second, becauseof the nature of research with a clinical population,data from some measures were not collected for allpatients. Future studies should include follow-updata on patients once discharged from the unit intothe community, to allow us to comment on longer-term outcomes of treatment, and to track, forexample, whether patients are later re-admitted toother hospitals for psychiatric reasons. Given thepotential difficulties with the GAF in this popula-tion, another measure of overall psychiatricimprovement, perhaps rated by a psychiatrist,should be incorporated. Finally, this study did notinclude a standardised assessment of the strengths,resources and quality of life of patients or caregiv-ers. It is important to know more about internaland external resources that patients and their fami-lies bring into hospital, or develop during the inpa-tient admission.
References
Aman M. G. & Singh N. N. (1986) Aberrant BehaviorChecklist: Manual. Slosson Educational Publications,East Aurora, NY.
Aman M. G., Singh N. N., Stewart A. W. & Field C. J.(1985) Psychometric characteristics of the AberrantBehavior Checklist. American Journal of Mental Defi-ciency 89, 492–502.
American Psychiatric Association (1994) Global Assess-ment of Functioning Scale. In: Diagnostic and StatisticalManual of Mental Disorders, 4th edn. (DSM-IV),p. 32. American Psychiatric Association, Washington,DC.
Ballinger B. R., Ballinger B., Reid A. H. & McQueen E.(1991) The psychiatric symptoms, diagnoses and careneeds of 100 mentally handicapped patients. BritishJournal of Psychiatry 158, 251–4.
68Journal of Intellectual Disability Research volume 54 part 1 january 2010
Y. Lunsky & A. M. Palucka • Outcomes of a specialised inpatient unit
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

Carminati G. G., Gerber F. & Constantin N. (2005) Aday hospital for adults with intellectual disabilities andpsychiatric disorders. Psychiatric Services 56, 609.
Chaplin R. (2006) General psychiatric services for adultswith intellectual disability and mental illness. Journal ofIntellectual Disability Research 48, 1–10.
Chaplin R. (2009) New research into general psychiatryservices for adults with intellectual disability and mentalillness. Journal of Intellectual Disability Research 53, 189–99.
Day K. (1985) Psychiatric disorder in the middle-aged andelderly mentally handicapped. British Journal of Psychia-try 147, 660–667.
Hall I., Parkes C., Samuels S. & Hassiotis A. (2006)Working across boundaries: clinical outcomes for anintegrated mental health service for people with intellec-tual disabilities. Journal of Intellectual Disability Research50, 598–607.
Hurst J., Nadarajah J. & Cumella S. (1994) In-patient carefor people with learning disability and mental illness.The first eight years of a specialist unit. Psychiatry Bulle-tin 18, 29–31.
van Minnen A., Hoogduin C. A. L. & Broekman T. G.(1997) Hospital vs. outreach treatment of patients withmental retardation and psychiatric disorders: a con-trolled study. Acta Psychiatrica Scandinavica 95, 515–22.
Morris S. (2005) Specialized inpatient mental health unitsin Ontario: their history and program characteristics.Mental Health Aspects of Developmental Disabilities 8,69–76.
Oliver P., Cooray S., Tyrer P. & Cicchetti D. (2003) Useof the Global Assessment of Function scale in learningdisability. British Journal of Psychiatry 182, 32–5.
Prout H. T. (1993) Assessing psychopathology in personswith mental retardation: a review of the Reiss scales.Journal of School Psychology 31, 535–40.
Raitasuo S., Taiminen T. & Salokangas R. K. R. (1999)Inpatient care and its outcome in a specialist psychiatricunit for people with intellectual disability: a prospectivestudy. Journal of Intellectual Disability Research 43, 119–27.
Reid A. H., Ballinger B. R., Heather B. B. & Melvin S. J.(1984) The natural history of behavioural symptomsamong severely and profoundly mentally retardedpatients. British Journal of Psychiatry 145, 289–93.
Reiss S. (1986) Reiss Screen for Maladaptive Behavior.International Diagnostic Systems, Inc, Orland Park, IL.
Shedlack K. J., Hennen J., Magee C. & Cheron D. M.(2005) A comparison of the Aberrant Behavior Check-list and the GAF among adults with mental retardationand mental illness. Psychiatric Servies 56, 484–6.
Sovner R., Beasley J. & Hurley A. D. (1995) How longshould a psychiatric inpatient stay be for a person withdevelopmental disabilities? The Habilitative MentalHealthcare Newsletter 14, 1–6.
Startup M., Jackson M. C. & Bendix S. (2002) The con-current validity of the global assessment of functioning(GAF). British Journal of Clinical Psychology 41, 417–22.
Statistical Package for Social Sciences (2007) SPSS Base15.0 forWindows. SPSS Inc, Chicago, IL.
Tajuddin M., Nadkarni S., Biswas A., Watson J. M. &Bhaumik S. (2004) A study of the use of an acute inpa-tient unit for adults with learning disability and mentalhealth problems in Leicestershire, UK. The BritishJournal of Developmental Disabilities 50, 59–68.
Xenitidis K., Gratsa A., Bouras N., Hammond R., Ditch-field H., Holt G. et al (2004) Psychiatric inpatient carefor adults with intellectual disabilities: generic or spe-cialist units? Journal of Intellectual Disability Research 48,11–8.
Accepted 4 August 2009
69Journal of Intellectual Disability Research volume 54 part 1 january 2010
Y. Lunsky & A. M. Palucka • Outcomes of a specialised inpatient unit
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd