-
Duke Robert J. Margolis, MD Center for Health Policy
Clinical Outcome Assessments: Establishing and Interpreting
Meaningful Within-Patient Change 4/4/17
-
CLINICAL OUTCOME ASSESSMENTS: INTERPRETING MEANINGFUL CHANGE
Duke Margolis Expert Workshop April 4, 2017
Elektra J. Papadopoulos, MD, MPH Clinical Outcome Assessments
Staff
Office of New Drugs
Center for Drug Evaluation and Research
U.S. Food and Drug Administration
www.fda.gov 1
http:www.fda.gov
-
Role of Patient Perspective
Dr. Janet Woodcock:
"It turns out that what is really bothering the patient and what
is really bothering the doctor can be radically different
things
-
Framing of FDA Drug Benefit-Risk Assessment
Decision Factor Evidence and Uncertainties I Conclusions and
Reasons & .... -=-- -- Sets the context for the weighing of
benefits and risks: l fiITTi n ffili1
________ ..... How serious is this indicated condition} and
why?
... -- - -~1i;;lllf;.f;U1-1T:lllli!' How wel l is the patient
populat ion}s medical! need be ing met by
current ly ava ilable therapies?
Characterize and assess the evidence of benefit:
Benefit How mean ingful is t he benefit} and for whom? How
compelling is the expected benefit in the post-market sett ing?
Characterize and assess the safety concerns:
Risk How serious are t he safety signa lls identified in the
submitted data? What potential risks could emerge in the
post-market setting?
Assess what risk management (e.g., labeling, REMS) may be Risk
Management necessary to address the identified safety concerns
Benefit-Risk Summary and Assessment
3
-
FD!s Patient-Focused Drug Development
(PFDD) Initiative
Patients are uniquely positioned to inform understanding of the
therapeutic context for drug development and evaluation There is a
need for more systematic ways of gathering patient
perspective on their condition and treatment options
Patient-Focused Drug Development (PFDD) is part of FDA
commitments under PDUFA V* FDA is convening 24 meetings on specific
disease areas in FY 2013-
17 Meetings can help advance a systematic approach to
gathering
input
*The fifth authorization of the Prescription Drug User Fee Act,
enacted in 2012
4 4
-
PFDD in Chronic Disease
PFDD meetings routinely ask for patients perspectives on what an
ideal treatment would look like and what clinical benefit would be
the most meaningful to them Concepts such as emotional impact of
disease,
ability to perform activities are often cited by patients as
important E;g;, in Parkinsons disease patients want to know
functional status over time Depending on the stage of disease
even small amounts
of deterioration can make the difference between being able to
perform basic activities (e.g., feeding oneself) independently or
not
5
-
PFDD Next Steps
Advance science of
patient input
Engage wider community to discuss methodologically sound
approaches that:
Bridge from initial PFDD meetings to more systematic collection
of patients input
Generate meaningful input on patients experiences and
perspectives to inform drug development and B-R assessment
!re fit for purpose in drug development and regulatory
context
Provide guidance
To: patient communities, researchers, and drug developers
On: pragmatic and methodologically sound strategies, pathways,
and methods to gather and use patient input
6 6
-
Interpretation of
Clinically Meaningful
Statistical significance alone is not sufficient
Clinical benefit: a positive clinically meaningful effect of an
intervention, i.e., a positive effect on how an individual feels,
functions, or survives.
To establish clinical benefit we consider two questions: 1) Does
the assessment measure or reflect something of
significance to patients? Relies on patient, caregiver and
expert input/engagement
2) Is the magnitude of change at the individual level
sufficiently large to affect how patients feel or function in daily
life? 7
-
Triangulation of Evidence
Multiple methods used to select a benchmark for meaningful
change
Often result in a range of values for what is a
clinically meaningful benchmark
Triangulation of evidence consists of examining these values to
converge on an appropriate value or range of values likely to
represent meaningful change in the outcome of interest
8
-
Guidance for Industry Patient-Reported Outcome Measures: Use in
Medical Product Development
to Support Labeling Claims
li.S. Depar1men1 of Healt h and Jiu.ma n Sfr.,.kes Food :md Drug
Adrninistm1 lon
Ct'nter for Drug E, :1l uatlon :md Resl".:t rd1 (CDER) Centf.'r
for Hiologics fi:, ,a luation and Res('a lTh (CHER) c ... nter for
IX',kes and Radiologka l Health (CDRJ [)
December 2009 Clinical/Medical
Good Measurement Principles
http://www.fda.gov/downlo ads/Drugs/GuidanceComplia
nceRegulatoryInformation/G uidances/UCM205269.pdf
FDA PRO Guidance defines good measurement principles to consider
for well-defined and reliable (21 CFR 314.126) PRO measures
All COAs can benefit from the good measurement principles
described within the guidance
But, judgment and flexibility are needed!
www.fda.gov 9
http:www.fda.govhttp://www.fda.gov/downlo
-
Final PRO Guidance (2009)
Clinically meaningful thresholds may vary by target population:
we will evaluate an instruments responder definition in the
context of each specific clinical trial.
Anchor-based methods emphasized: Empiric evidence for any
responder definition is derived using
anchor-based methods /explore the associations between the
targeted concept of
the PRO instrument and the concept measured by the anchors
Multiple anchors recommended
Distribution-based methods: /should be considered as supportive
and are not appropriate
as the sole basis for determining a responder definition 10
-
Final PRO Guidance (2009) Emphasizes the display of
individual
responses to treatment: /it is possible to present the entire
distribution
of responses for treatment and control group, avoiding the need
to pick a responder criterion. Whether the individual responses are
meaningful represents a judgment/
/cumulative distribution displays show a continuous plot of the
percent change from baseline on the X-axis and the percent of
patients experiencing that change on the Y-axis.
A variety of responder definitions can be identified along the
cumulative distribution of response curve. 11
-
ut
The presentation of all possible response level cut-off points
does not eliminate the need to identify the level of change that is
clinically important (or at least to state our uncertainty about
that level)
12
-
Cumulative Distribution Function (CDF) (DB4, pooled across
treatment arms)
100
-a, 90 .., ta 0:: i.. 80 a, -0 C: 0 C.
70 IA a,
60 0:: -a, 0J) so ta .., C: a,
40 u i.. a, Q.
30 a, -~ ni 20 :s E
10 :s u
0
-6
- Much Bett er (n=298)
- Somewhat Bet ter (n=288)
- Not Changed (n=185)
-5 -4 -3 -2 -1 0 1
Change from Baseline in Nocturia Episodes
Improvement
2
Source: Dr. Jia Guo; Bone, Reproductive and Urologic Drugs
13Advisory Committee 10/19/2016
-
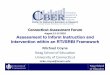
CDF Plot by Treatment Arms (D84) 100
90 - SER 120 1.5 mcg (n=260) 80
CJJ 70 +" - Placebo (n=260)
n, a: 60 ... CJJ
"'C so C: 0 40 Q. V)
CJJ 30 a: 36%
20
10
0
-6 -4 2
Change from Baseline in Nocturia Episodes
Improvement
Source: Dr. Jia Guo; Bone, Reproductive and Urologic Drugs
14Advisory Committee 10/19/2016
-
Establishing Meaningful Change:
Examples from FDA Guidance
!lzheimers Disease: Developing Drugs for the Treatment of Early
Stage Disease (2013) Co-primary endpoint of cognitive test and a
functional or global
assessment The intent of this dual measurement is to ensure the
clinical
meaningfulness of a cognitive benefit that may be observed
Irritable Bowel Syndrome: Clinical Evaluation of Drugs for
Treatment (2012) Patient global assessments
Example: How would you rate your IS signs or symptoms overall
over the past 7 days?
Analgesic Indications: Developing Drugs and Biological Products
(2014) Allows the use of a responder analysis (e.g., 30% reduction
in pain with
early discontinuation counted as failure) in addition to
differences in group means
Encourages use of cumulative distribution functions in the
package insert 15
-
A word about MID and MID
Minimum important difference (MID) was removed from the Final
PRO Guidance 2009 Confusion resulted from the term being used
interchangeably to indicate either group-level mean
differences as well as individual level change Use of the term
minimal is problematic: While a minimal amount of change may be
noticeable, it does not
necessarily imply the change is meaningful to patients
Minimal clinically important difference (MID)- i.e., the
smallest difference in score
-
Beyond Anchor-based and
Distribution-based methods:
Examples of Emerging Methods Bookmarking/Standard Setting
Patients and experts are presented with clinical vignettes of a
disease in
order to reach a consensus on thresholds for severity levels
Designed for measures that have been calibrated using an IRT
model
Scale judgment Panels of judges evaluate pairs of completed
tests to determine whether
the amount of change specified by the responses before and after
treatment is meaningful
Exit interviews Interviews of patients who recently completed a
clinical trial an be used to collect qualitative and quantitative
data about patients
experience of disease or treatment burden and changes during the
course of the clinical trial
Others 17
-
Todays Goals
Advance the discussion on methods to identify meaningful
within-patient change in COAs by discussing key issues and major
challenges, including: What are the advantages and disadvantages of
each of the
methods?
How might threshold determinations differ across the four types
of COAs?
What are special considerations for establishing meaningful
change in small and heterogeneous study populations?
How and when could these methods be most feasibly used in drug
development?
18
-
U.S. FOOD & DRUG
ADMINISTRATION
-
Duke Robert J. Margolis, MD Center for Health Policy
Clinical Outcome Assessments: Establishing and Interpreting
Meaningful Within-Patient Change 4/4/17
-
Exploring the Use of Emerging Methods to Derive and Interpret
Meaningful Within-Patient Change Using Idio
Scale-Judgment (Bookmarking/Standard-Setting)
Karon F. Cook
Department of Medical Social Sciences, Feinberg School of
Medicine, Northwestern University,
Chicago, IL
April 4, 2017
Washington, DC
-
\
Background H
ow
mu
ch w
e kn
ow
Building State of the Art Measures
How to Interpret Scores on State of the Art Measures
-
Meaningful Change
-
Methods for Defining Meaningful Score
Differences
Statistical
Global Ratings of Change
External Anchors
-
often
always
sometimes
How often are you too tired to
never
x
Pro
babili
ty o
f specifie
d r
esponse
0.0
1.0
x x
Fatigue
socialize with family?
-
11 I I I I I I I I
I I I I I I I I I
Never Rarely Sometimes
Never Rarely Sometimes Always
40 50 60 30 70
-
Item Response Samples T=40 never was too tired to do household
chores.
never needed to sleep during the day.
rarely had trouble finishing things because
she was too tired.
rarely was so tired that she needed to rest
during the day.
rarely felt that she had no energy.
FATIGUE
30 40 50 60 70
-
00000000 00000 0 0 0 0
I I I I I I I 11 I I I I I I 11 I I I I I I I I I I I I I I I 11
I I I I I I 1 11 I I I I I I I I I I I I I I I ii I I I I I 1 11 I
I I I I
Item Response Samples
sometimes was too tired to eat.
often had trouble finishing things because she was too
tired.
often was too tired to do her household chores.
often needed to sleep during the day.
T=62
always frustrated by being too tired to do the things she wanted
to do.
30 40 50 60 70
-
National Multiple Sclerosis Society
Grant #H00145 Deborah Miller, PI
10
-
36
Online panel of 500 participants with Multiple Sclerosis
Responded to NeuroQoL Fatigue Short Form
Developed 18, 5-item sample response sets, 2 pts apart.
Ms. Butler
e.g. Branched into 7 fatigue levels 48-51
Presented with 7 response samples
70
-
MY FATIGUE
OTHER PERSON'S FATIGUE
fCREEn /HOT/
In PART B, you will
Look at the fatigue reports of 7 people who have MS
Compare each persons fatigue to your own fatigue. For example,
your fatigue might be greater.
Or, you might decide your fatigue is the SAME or LESS than that
other persons.
-
Woul~ Maff er
/CREEn /HOT/
If you decide your fatigue is DIFFERENT from the other persons,
you will then
Consider what it would be like to have this persons fatigue,
and
Decide if the difference would matter to you in your daily
life.
13
-
/HOT/
Depending on your own fatigue, you may decide that none, some,
or all of these people have more, less, or
the same amount fatigue.
There are no right answers just your own thoughtful
judgments.
-
[T Score = 58]
This is what Ms. Anderson said about her fatigue over the last 7
days. She reported that she:
sometimes felt weak all over.
often had to limit social activity because she was tired.
sometimes had trouble starting things because she was too
tired.
often was too tired to take a short walk.
often had trouble finishing things because she was too
tired.
Compared to Ms. !ndersons , has YOUR FATIGUE been:
Greater than Ms. !ndersons
The same as Ms. !ndersons
Less than Ms. !ndersons
-
You said YOUR FATIGUE over the past week was Greater
If your fatigue IMPROVED to Ms. Andersons level, would it make a
difference in your daily life?
It wouldnt really make a difference in my daily life.
It would make a difference in my daily life (things I
do day-to-day would be easier).
Less
G
reat
er
MY FATIGUE
MS. ANDERSON'S FATIGUE
This is what Ms. Anderson said about his fatigue over the last 7
days. She reported that she:
sometimes felt weak all over.
often or always had to limit social activity because she was
tired.
sometimes had trouble starting things because she was too
tired.
often was too tired to take a short walk.
often had trouble finishing things because she was too
tired.
-
If your fatigue WORSENED to Ms. !ndersons level, You said YOUR
FATIGUE over the past week was would it make a difference in your
daily life? LESS than MS. !NDERSONS FATIGUE. It wouldnt really make
a difference in my daily
life.
It would make a difference in my daily life (many
Less
G
reat
er
MY FATIGUE
MS. !NDERSONS FATIGUE
of the things I do day-to-day would be harder).
This is what Ms. Anderson said about his fatigue over the last 7
days. She reported that she:
sometimes felt weak all over.
often or always had to limit social activity because she was
tired.
sometimes had trouble starting things because she was too
tired.
often was too tired to take a short walk.
often had trouble finishing things because she was too
tired.
-
1111 I 1111 I 1111 I 1111I111111111 I 1111 I 1111 I
1111I111111111I111111111 I 1 ~ t ~ t t ~ 1' L_JI IL_JI II IL_JI
I
5 2 5 4 5 6 5 8 6 0 6 2 6 4
Butler Richardson Woods Anderson Foster Allen Harris
T = 58.8 Score Group 56-60
7 points >
5 points >
3 points >
1 pt
5 points <
3 points <
1 pt*
*
*
*
-
ANALYSIS
Results
-
Analyses to Estimate Thresholds for
Interpreting Change
Calculate minimum distance endorsed by respondent as meaningful
improvement/decrement
Identify thresholds that would capture different percentages of
respondents minimums.
-
.0
14.0
13.0
12.0
11 .0
"ti 10.0
0 ~ Ill 9 .0 QI ... ~ 8.0 .... jij
7.0 ::::, "ti
> 6.0 :s C 5.0
4.0
3.0
2.0
1 .0
.0
Thresholds for Worsening Mean of Individual Thresholds @
0 0
0
90th Percentile 0 & 'C)" o ................. . 75 th
Percentile O O o ............................. Q .Q .. ~ 'O" G .
............... .
0 0 0 0 O O 0
-O E> 0 0 0 0
0 0
501h Percentile
0 0 0 0 0 0
0 0 0 0
0 0 0
20 30 40 50 60 70 80
Neuro-Qol Fatigue T-Score
Threshold locations for capturing 50, 75, and
95% of distances endorsed as important
worsening
-
0
-1 .0
-2.0
-3.0
-4.0
-5.0 -g
0 -6.0 .l: VI -7.0 QI ... .l: -8.0 .... ;; -9.0 ::::, -g
-10.0 > -g
-11 .0 C
-12.0
-13.0
-1 4.0
-15.0
-16.0
-17.0
0 0 0 0 0 0
0 0 O O 0 O O 0
0
0 0
0
50th Percentile= -3.3 0 o O O O 0 - - - - - - . - - - - - - - -
- - - - - - o- o-o 0 f)_ -cs - - - - -
0 0 O O 0 75th Percentile= -5.1 o O 0 - - - - - - - - - - - - -
- o- c- - - o- - - - - - - - -
0 0 O 0 0 0 0 0 0
90th Percentile= -7.3 o .. - - - ..... - - - .... - - - ... -~ -
- ... 0- . - o- .. ~- - -e5 ..... - - - .... - - - ..
20
Thresholds for Improvement Mean of Individual Thresholds ~
30 40 50 60
Neuro-Qol Fatigue T-Score
0
0
0
70 80
Threshold locations for capturing 50, 75, and
95% of distances endorsed as important
improvement
-
11111111111
1111 111111111 111111111 111il1111
111~11il111il1111l111il111il1
5 2 5 4 5 6 5 8 6 0 6 2 6 4
7 points >
5 points >
3 points >
1 pt
Richardson Woods Anderson Butler
*
*
*
*
8% Reversals92% Current Judgments Consistent with Prior
Judgment
-
1111 I 1111 I 1111 I 1111I111111111 I 1111 1111 I
1111I111111111I111111111 I 1
ALe
ss
G
reat
er
MY FATIGUE
MS. !NDERSONS F TIGUE
5 2 5 4 5 6 5 8 6 0 6 2 6 4
Anderson
Inconsistent Judgment
7.6% of all judgments were inconsistent with the one
prior (of 3000 opportunities)
344
94
51
11
0
50
100
150
200
250
300
350
400
0 1 2 3
FREQUENCY OF INCONSITENT JUDGMENTS
*
-
Qual Life Re (2017) 26:847 57 DOI 10. 1007/sl 11
6-016-1-114-
When global rating of change contradicts observed change:
Examining appraisal processes underlying paradoxical responses over
time
Carolyn E. Schwartz 1.2 Victoria E. Powell 1 Bruce D.
Rapkin3
Accepted: 1-1 September 2016/PublL,hcd onliae: October 20 16 lfl
prin e.- International Publlmin,, c, .. ' ~-' - ""'
CrossMarlc
Scores of N=525
Declined
Mental health component scores over time in MS
Unchanged
On GROC, 48.6% made a paradoxical judgment
reporting worse status when observed score was unchanged or
endorsing the same status when observed scores had declined.
-
'
:
We were able to estimate plausible responder thresholds for
consequential change.
Participants evaluated range of IRT-Vs close to their own
fatigue levels.
Participants reported high confidence that their judgments (3.3
between moderately and highly confident).
-
'
:
Judgments contextualized in a patient-relevant contextmake a
difference in daily life.
Design allowed large samples.
Judgment errors existed, but were within range of other
methods.
Judgement errors not strongly associated with demographics
(e.g., education)
-
How can we do better
Qualitative research to understand what is important to people
in assessing change.
Cognitive debriefing to understand what people are attending to.
Are they attending to different things. Could we selection of
concepts of the vignettes, should they be standardized.
Frame vignettes by what is important to people.
Try to understand the variation in levels of change that people
believe is important.
Can set a threshold that is most representative, but it will not
catch everyone.
Change study design so that everyone is getting same distances.
Branch on every score.
-
How can we do better?
-
I ? I
I ~ I
I.I ,
l.
-
An Alternative Model:
-
Duke Robert J. Margolis, MD Center for Health Policy
Clinical Outcome Assessments: Establishing and Interpreting
Meaningful Within-Patient Change 4/4/17
-
Some Remarks about
(Educational) Standard Setting, Characterizing Meaningful
Change, and the Scale-Judgment Method
David Thissen L.L.Thurstone Psychometric Laboratory
The University of North Carolina at Chapel Hill
-
Minimally Important Difference (MID) estimation is not like
answering the question
What is the ratio of the circumference of a circle
to its diameter?
-
Minimally Important Difference (MID) estimation is not like
answering the question
What is the ratio of the circumference of a circle
to its diameter?
-
Minimally Important Difference (MID) estimation is like
At least for regulatory purposes, MID is like a speed limit: A
policy decision informed by data
(And likely between 0.2 and 0.5 standard units)
-
Most authorities on standard setting (e.g., Green,Trimble, and
Lewis, 2003; Hambleton, 1980; Jaeger, 1989; Shepard, 1980; Zieky,
2001) suggest that, when setting cut scores, it is prudent to use
and compare results from different standard setting methods. (p.
155)
Green, D.R.,Trimble, C.S., and Lewis, D.M. (2003). Interpreting
the results of three different standard-setting procedures.
Educational Measurement: Issues and Practice, 22, 22-32. Hambleton,
R.K. (1980).Test score validity and standard setting methods. In
D.C. Berliner, (Ed.), Criterion-referenced measurement:The state of
the art (pp. 80-123). Baltimore, MD: Johns Hopkins University
Press. Jaeger, R.M. (1989). Certification of student competence. In
R.L. Linn (Ed.), Educational measurement (3rd ed., pp.
485-514).Washington DC:American Council on Education. Shepard, L.A.
(1980). Standard setting issues and methods. Applied Psychological
Measurement, 4, 447-467. Zieky, M.J. (2001). So much has changed:
How the setting of cutscores has evolved since the 1980s. In G.J.
Cizek (Ed.), Setting performance standards: Concepts, methods, and
perspectives. Mahwah, NJ: Lawrence Erlbaum.
-
Section II: Standard Setting Methods Chapter 4.The Nedelsky
Method Chapter 5.The Ebel Method Chapter 6.The Angoff Method
and Angoff Variations Chapter 7.The Direct Consensus Method
Chapter 8.The Contrasting Groups
and Borderline Group Methods Chapter 9.The Body of Work
and Other Holistic Methods The Body of Work Method The
Judgmental Policy Capturing Method The Dominant Profile Method The
Analytic Judgment Method
Chapter 10.The Bookmark Method Chapter 11.The
Item-Descriptor
Matching Method Chapter 12.The Hofstee and Beuk Methods
-
National Assessment of Educational Progress (NAEP) Achievement
Levels
Grade 4 Mathematics, 1996
Below Basic Basic Proficient Advanced
100 150 200 250 300 350 NAEP Scale Score
-
A Ranking Procedure to Find Score Ranges Associated with
Mild,Moderate, and Severe Conditions
(Cella et al., 2008, 2014)
Cella, D., Choi, S., Rosenbloom, S., Surges,Tatum, D., Garcia,
S., Lai, J.-S., George, J., & Gershon, R. (2008). A novel
IRT-Based
case-ranking approach to derive expert standards for symptom
severity (paper presentation), International Society for
Quality
of Life Research Annual Scientific Meeting. Montevideo, Uruguay.
Cella, D., Choi, S., Garcia, S., Cook, K. F., Rosenbloom, S., Lai,
J. S.,Tatum, D. S., & Gershon, R. (2014). Setting
standards for severity of common symptoms in oncology using the
PROMIS item banks and expert judgment. Quality of Life Research,
23, 2651-2661.
-
- -r ~
~ ~
- ---r "'1111 ~
~
- ---r "'1111 ~
~ -- ---,.. " ~ t
'-- ~ ~ ~ ~ ,~
Sample Fatigue VignetteT-score 40
Rating ______
FATIGUE PINK 1 How often did your fatigue make you
feel less alert? Never Rarely Some-
times Often Always
2 How often did you have trouble Never Rarely Some- Often Always
starting things because of your times fatigue?
3 How often did you feel run-down? Never Rarely Some-times
Often Always
4 How often were you energetic? Never Rarely Some-times
Often Always
5 How easily did you find yourself getting tired on average?
Not at all A little bit Some-what Quite a bit
Very much
Graphic from: Cella, D., Choi, S., Rosenbloom, S., Surges,Tatum,
D., Garcia, S., Lai, J.-S., George, J., & Gershon, R. (2008). A
novel IRT-Based case-ranking approach to derive expert standards
for symptom severity (paper presentation), International Society
for Quality of Life Research Annual Scientific Meeting. Montevideo,
Uruguay.
-
Sample Depression VignetteT-score 60
Rating ______
DEPRESSION - MINT 1 I felt that I had nothing to look
forward to Never Rarely Some-
times Often Always
2 I felt that I wanted to give up on everything
Never Rarely Some-times
Often Always
3 I felt disappointed in myself Never Rarely Some-times
Often Always
4 I felt lonely Never Rarely Some-times
Often Always
5 I felt I had no reason for living Never Rarely Some-times
Often Always
Graphic from: Cella, D., Choi, S., Rosenbloom, S., Surges,Tatum,
D., Garcia, S., Lai, J.-S., George, J., & Gershon, R. (2008). A
novel IRT-Based case-ranking approach to derive expert standards
for symptom severity (paper presentation), International Society
for Quality of Life Research Annual Scientific Meeting. Montevideo,
Uruguay.
-
I
I
ANXIETY - Case Examples Exercise
Step 1: Please rev ievv the ten different cards in the "Anxiety"
envelope. Each ca rd represents a patient \1vho fa I ls along a
different place on the anxiety continuum. Sort the cards in order
from least severe to most severe, giving each color a ranking ("1"
being least severe).
Please enter the card color (e.g. "Pink", "Blue", etc.) below
the number ranking that you have assigned it. You are encouraged to
give each card a unique ranking, but this is not required. If you
believe tvvo patients are tied, for example, at rank "6", then
vvrite both color names under the number "6. "
Least severe Most severe - -
1 2 3 4 5 6 7 8 9 10 -
COLOR:
COLOR: (if applicable)
COLOR: I (if applicable)
Step 2: Novv please d ra\1V three ve rtica I Ii nes bet\,veen
ran ks (e.g. betvveen \\3" and \\4"); one delineating each of the
follovving:
1. A separation between those cards (i.e. patients) that you
believe represent a normal level of anxiety and a mild level of
anxiety
2. A separation between those cards representing a n1ild level
of anxiety and a moderate level of anxiety 3. A separation between
those cards representing a moderate level of anxiety and a severe
level of anxiety
D
I
Expert Ranking Sheet:Anxiety, Step 1
Graphic from: Cella, D., Choi, S., Rosenbloom, S., Surges,Tatum,
D., Garcia, S., Lai, J.-S., George, J., & Gershon, R. (2008). A
novel IRT-Based case-ranking approach to derive expert standards
for symptom severity (paper presentation), International Society
for Quality of Life Research Annual Scientific Meeting. Montevideo,
Uruguay.
-
I I
I
ANXIETY - Case Examples Exercise
Step 1: Please review the ten different cards in the "Anxiety"
envelope. Each ca rd represents a patient who falls along a
different place on the anxiety continuum. Sort the cards in order
from least severe to most severe, giving each color a ranking ("1"
being least severe).
Please enter the card color (e.g. 'Pink", "Blue", etc.) below
the number ranking that you have assigned it. You are encouraged to
give each ca rd a unique ranking, but th is is not required. If you
believe tvvo patients are tied, for exam pie, at rank ' 6", th en
vvrite both color names under the number "6. "
Least severe ; Most severe - -
1
COLOR:
COLOR: (if applicable)
COLOR: I (if applicable)
2 - -
-..
.
-
t
3 4 - - - , - - 5 6 7 I 8 9 10 I - - _,, - - I I I I I I - I I "
, I
! I I I I I I
, I I I I
I I I I I I I I I -
Step 2: No\1V please d ra vv three ve rtica I Ii nes bet\,veen
ran ks (e.g. bet\,veen "3" and "4"); one delineating each of the
follo\1Ving:
1. A separation betvveen those cards (i.e. patients) that you
believe represent a normal level of anxiety and a mild level of
anxiety
2. A separation between those cards representing a mild level of
anxiety and a moderate level of anxiety 3. A separation between
those cards representing a moderate level of anxiety and a severe
level of anxiety
D
Expert Ranking Sheet:Anxiety, Step 2
Normal Mild Moderate Severe
Graphic from: Cella, D., Choi, S., Rosenbloom, S., Surges,Tatum,
D., Garcia, S., Lai, J.-S., George, J., & Gershon, R. (2008). A
novel IRT-Based case-ranking approach to derive expert standards
for symptom severity (paper presentation), International Society
for Quality of Life Research Annual Scientific Meeting. Montevideo,
Uruguay.
-
"U a "'C 0 ~ 0 ::::,
0 . 0 01
0 . 0 ~
0 . 0 w
0 . 0 I\.)
0 . 0 ....Ji.
52.5
Anxiety
62.5 0
.___----.-----------.----------------.......-------------____, .
0
30 40 50 60
T-Score
70 80
After a consensus-
building process
Normal Mild Moderate Severe
Graphic from: Cella, D., Choi, S., Rosenbloom, S., Surges,Tatum,
D., Garcia, S., Lai, J.-S., George, J., & Gershon, R. (2008). A
novel IRT-Based case-ranking approach to derive expert standards
for symptom severity (paper presentation), International Society
for Quality of Life Research Annual Scientific Meeting. Montevideo,
Uruguay.
-
A Bookmarked-Vignettes Procedure to Find Score Ranges Associated
with
Mild,Moderate, and Severe Conditions
(Cook et al., 2014; Morgan et al., 2017)
Cook, K. F.,Victorson, D. E., Cella, D., Schalet, B. D., &
Miller, C. (2014). Creating meaningful cut-scores for Neuro-QOL
measures of fatigue, physical functioning and sleep disturbance
using standard setting with patients and providers. Quality of Life
Research, 24, 575-589.
-
Judges do not know this vignette is for a T-score of 47.5
Ms. Millers Fatigue
In the last 7 days, Ms. Miller rarely felt weak all over and
rarely was so tired she couldnt take a short walk. However, she
sometimes felt tired, which got in the way of her doing her
household chores. Feeling too tired to do the things she wanted to
do was sometimes frustrating for her.
In summary, Ms. Miller reports being:
Rarely weak all over. Rarely too tired to take a short walk.
Sometimes tired. Sometimes too tired to do household chores.
Sometimes frustrated by being too tired to do the things she
wanted to do.
Cook, K. F.,Victorson, D. E., Cella, D., Schalet, B. D., &
Miller, C. (2014). Creating meaningful cut-scores for Neuro-QOL
measures of fatigue, physical functioning and sleep disturbance
using standard setting with patients and providers. Quality of Life
Research, 24, 575-589.
-
alertwhenhewokeupandreadytostarttheday.Inthelast7days,
hasneverhadtroublesleepingbecauseofbaddreamsandneverhada
hard9mecontrollinghisemo9onsbecauseofpoorsleep.
Insummary,Mr.Turner
Neverhavingtroublesleepingbecauseofbaddreams.
Neverhavingahard9mecontrollinghisemo9onsbecauseof
Rarelyfeeling9red. O,enfeelingalertwhenhewokeup.
O,enwakingupandfeelingreadytostarttheday.
Mr.Turnerhasrarelyfelt9red.O,en, hehasfelt
alertwhenhewokeupandreadytostarttheday.Inthelast7days,
hasneverhadtroublesleepingbecauseofbaddreamsandneverhada
hard9mecontrollinghisemo9onsbecauseofpoorsleep.
Insummary,Mr.Turner
Neverhavingtroublesleepingbecauseofbaddreams.
Neverhavingahard9mecontrollinghisemo9onsbecauseof
Rarelyfeeling9red. O,enfeelingalertwhenhewokeup.
O,enwakingupandfeelingreadytostarttheday.
Mr.Turnerhasrarelyfelt9red.O,en, hehasfelt
alertwhenhewokeupandreadytostarttheday.Inthelast7days,
hasneverhadtroublesleepingbecauseofbaddreamsandneverhada
hard9mecontrollinghisemo9onsbecauseofpoorsleep.
Insummary,Mr.Turner
Neverhavingtroublesleepingbecauseofbaddreams.
Neverhavingahard9mecontrollinghisemo9onsbecauseof
Rarelyfeeling9red. O,enfeelingalertwhenhewokeup.
O,enwakingupandfeelingreadytostarttheday.
Mr.Turnerhasrarelyfelt9red.O,en, hehasfelt
alertwhenhewokeupandreadytostarttheday.Inthelast7days,
hasneverhadtroublesleepingbecauseofbaddreamsandneverhada
hard9mecontrollinghisemo9onsbecauseofpoorsleep.
Insummary,Mr.Turner
Neverhavingtroublesleepingbecauseofbaddreams.
Neverhavingahard9mecontrollinghisemo9onsbecauseof
Rarelyfeeling9red. O,enfeelingalertwhenhewokeup.
O,enwakingupandfeelingreadytostarttheday.
Mr.Turnerhasrarelyfelt9red.O,en, hehasfelt
alertwhenhewokeupandreadytostarttheday.Inthelast7days,
hasneverhadtroublesleepingbecauseofbaddreamsandneverhada
hard9mecontrollinghisemo9onsbecauseofpoorsleep.
Insummary,Mr.Turner
Neverhavingtroublesleepingbecauseofbaddreams.
Neverhavingahard9mecontrollinghisemo9onsbecauseof
Rarelyfeeling9red. O,enfeelingalertwhenhewokeup.
O,enwakingupandfeelingreadytostarttheday.
Mr.Turnerhasrarelyfelt9red.O,en, hehasfelt
alertwhenhewokeupandreadytostarttheday.Inthelast7days,
hasneverhadtroublesleepingbecauseofbaddreamsandneverhada
hard9mecontrollinghisemo9onsbecauseofpoorsleep.
Insummary,Mr.Turner
Neverhavingtroublesleepingbecauseofbaddreams.
Neverhavingahard9mecontrollinghisemo9onsbecauseof
Rarelyfeeling9red. O,enfeelingalertwhenhewokeup.
O,enwakingupandfeelingreadytostarttheday.
Mr.Turnerhasrarelyfelt9red.O,en, hehasfelt
alertwhenhewokeupandreadytostarttheday.Inthelast7days,
hasneverhadtroublesleepingbecauseofbaddreamsandneverhada
hard9mecontrollinghisemo9onsbecauseofpoorsleep.
Insummary,Mr.Turner
Neverhavingtroublesleepingbecauseofbaddreams.
Neverhavingahard9mecontrollinghisemo9onsbecauseof
Rarelyfeeling9red. O,enfeelingalertwhenhewokeup.
O,enwakingupandfeelingreadytostarttheday.
Mr.Turnerhasrarelyfelt9red.O,en, hehasfelt
alertwhenhewokeupandreadytostarttheday.Inthelast7days,
hasneverhadtroublesleepingbecauseofbaddreamsandneverhada
hard9mecontrollinghisemo9onsbecauseofpoorsleep.
Insummary,Mr.Turner
Neverhavingtroublesleepingbecauseofbaddreams.
Neverhavingahard9mecontrollinghisemo9onsbecauseof
Rarelyfeeling9red. O,enfeelingalertwhenhewokeup.
O,enwakingupandfeelingreadytostarttheday.
t
I t
I
t
he
p.
he
p.
he
p.
he
p.
he
p.
he
p.
he
p.
he
p.
NoProblems MildProblems
AnnasPain
Inthelast7days, Mr.Turnerhasrarelyfelt9red.O,en, hehasfelt
JuliasPain
Inthelast7days, reported: AndreasPain
poor slee Inthelast7days,
MildProblems ModerateProblems
reported: JacobsPain
Inthelast7days,poor slee
reported: ChloesPain
Inthelast7days,poor slee reported: KristensPain
Inthelast7days,poor slee reported: MayasPain
Severe Problems ModerateProblems
Inthelast7days,poor slee reported: ClairesPain
Inthelast7days,poor slee reported: AddisonsPain
Inthelast7days, Addisonhasrarelyfelt9red.O,en, hehasfeltalert
poor slee whenhewokeupandreadytostarttheday.Inthelast7days, hehas
reported: neverhadtroublesleepingbecauseofbaddreamsandneverhada
hard9mecontrollinghisemo9onsbecauseofpoorsleep.
poor slee Insummary,Mr.Turner reported:
Neverhavingtroublesleepingbecauseofbaddreams.
Neverhavingahard9mecontrollinghisemo9onsbecauseof
poor sleep. Rarelyfeeling9red. O,enfeelingalertwhenhewokeup.
O,enwakingupandfeelingreadytostarttheday.
Graphic from: DeWitt, E.M. (2015, February 6). Establishing
clinical meaning and defining important differences for PROMIS
measures in Juvenile Idiopathic Arthritis. Presentation at UNC
PROMIS Pediatric Investigators Meeting, Chapel Hill, NC.
-
..D 0
5 7 8
Graphic from: Morgan, E.M., Mara, C.A., Huang, B., Barnett, K.,
Carle,A.C., Farrell, J.E., & Cook, K.F. (2017). Establishing
Clinical Meaning and Defining Important Differences for
Patient-Reported Outcomes Measurement Information System (PROMIS)
Measures in Juvenile Idiopathic Arthritis Using Standard Setting
with Patients, Parents, and Providers. Quality of Life Research,
26, 565-586.
-
The Scale-Judgment Method to Estimate the Minimally Important
Difference (MID)
between Scores
(Thissen et al., 2016)
Thissen, D., Liu,Y., Magnus, B., Quinn, H., Gipson D.S.,
Dampier, C., Huang, I-C., Hinds, P.S., Reeve, B.B., Gross, H.E.,
& DeWalt, D.A. (2016). Estimating minimally important
difference (MID) in PROMIS pediatric measures using the
scale-judgment method. Quality of Life Research, 25, 13-23.
-
A minimally important difference (MID) has been defined as the
smallest difference in score that patients perceive as important,
and which would lead the clinician to consider a change in the
patients management
Guyatt et al. (2002)
Existing methods:
Distribution-based indices (not an empirical method; merely
expresses change in standard units)
Anchor-based methods (contrasting groups in educational standard
setting)
Guyatt, G. H., Osoba, D.,Wu,A.W.,Wyrwich, K.W., & Norman, G.
R. (2002). Methods to explain the clinical significance of
health status measures. Mayo Clinic Proceedings, 77, 371-383.
Revicki, D., Hays, R. D., Cella, D., & Sloan, J. (2008).
Recommended methods for determining responsiveness and
minimally
important differences for patient-reported outcomes. Journal of
Clinical Epidemiology, 6, 102-109.
-
Earlier judgment-based methods Delphi Method, Delphi plus
anchor, physician survey, expert panels using visual analog scales
or changes to item responses Bellamy, N.,Anastassiades,T. P.,
Buchanan,W.W., Davis, P., Lee, P., McCain, G.A.,Wells, G.A., &
Campbell, J. (1991). Rheumatoid arthritis antirheumatic drug
trials. III. Setting the delta for clinical trials of antirheumatic
drugs--results of a
consensus development (Delphi) exercise. Journal of
Rheumatology, 18, 1908-1915. Bellamy, N., Buchanan,W.W., Esdaile,
J. M., Fam,A. G., Kean,W. F.,Thompson, J. M.,Wells, G.A., &
Campbell, J. (1991). Ankylosing spondylitis antirheumatic drug
trials. III. Setting the delta for clinical trials of antirheumatic
drugs--results of a
consensus development (Delphi) exercise. Journal of
Rheumatology, 18, 1716-1722. Bellamy, N., Carette, S., Ford, P. M.,
Kean,W. F., le Riche, N. G., Lussier,A.,Wells, G.A., &
Campbell, J. (1992). Osteoarthritis
antirheumatic drug trials. III. Setting the delta for clinical
trials--results of a consensus development (Delphi) exercise.
Journal of Rheumatology, 19, 451-457. Spiegel, B. M.,Younossi, Z.
M., Hays, R. D., Revicki, D., Robbins, S., & Kanwal, F. (2005).
Impact of hepatitis C on health
related quality of life: a systematic review and quantitative
assessment. Hepatology, 41, 790-800. Wyrwich, K.W., Metz, S. M.,
Kroenke, K.,Tierney,W. M., Babu,A. N., & Wolinsky, F. D.
(2007).Triangulating patient and
clinician perspectives on clinically important differences in
health-related quality of life among patients with heart disease.
Health Services Research, 42(6 Pt 1), 2257-2274; discussion
2294-2323. Wells, G., Li,T., Maxwell, L., MacLean, R., &
Tugwell, P. (2007). Determining the minimal clinically important
differences in
activity, fatigue, and sleep quality in patients with rheumatoid
arthritis. Journal of Rheumatology, 34, 280-289. Rai, S.
K.,Yazdany, J., Fortin, P. R., & Avina-Zubieta, J.A.
(2015).Approaches for estimating minimal clinically important
differences in systemic lupus erythematosus. Arthritis Research
and Therapy, 17, 143. van Walraven, C., Mahon, J. L., Moher, D.,
Bohm, C., & Laupacis,A. (1999). Surveying physicians to
determine the minimal
important difference: implications for sample-size calculation.
Journal of Clinical Epidemiology, 52, 717-723. Todd, K. H., &
Funk, J. P. (1996).The minimum clinically important difference in
physician-assigned visual analog pain scores. Academic Emergency
Medicine, 3, 142-146. Dempster, H., Porepa, M.,Young, N., &
Feldman, B. M. (2001).The clinical meaning of functional outcome
scores in children
with juvenile arthritis. Arthritis and Rheumatology, 44,
1768-1774. Gong, G.W.,Young, N. L., Dempster, H., Porepa, M., &
Feldman, B. M. (2007).The Quality of My Life questionnaire: the
minimal clinically important difference for pediatric
rheumatology patients. Journal of Rheumatology, 34, 581-587.
-
One month ago Today
I felt alone.
never almost never sometimes
I felt like I couldnt do anything right.
never almost never sometimes
I felt everything in my life went wrong.
never almost never
I felt sad.
never almost never
I thought that my life was bad.
never almost never
I could not stop feeling sad.
never almost never
I felt lonely.
never almost never
I felt unhappy.
never almost never
sometimes
sometimes
sometimes
sometimes
sometimes
sometimes
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
T-score 62.1
I felt alone.
never almost never sometimes
I felt like I couldnt do anything right.
never almost never sometimes
I felt everything in my life went wrong.
never almost never sometimes
I felt sad.
never almost never
I thought that my life was bad.
never almost never
sometimes
sometimes
I could not stop feeling sad.
never almost never sometimes
I felt lonely.
never almost never
I felt unhappy.
never almost never
sometimes
sometimes
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
T-score 58.9
The scale-judgment method presents judges with pairs of
questionnaires, artificially completed using IRT, with scores known
to the experimenter but not the judges Thissen, D., Liu,Y., Magnus,
B., Quinn, H., Gipson D.S., Dampier, C., Huang, I-C., Hinds, P.S.,
Reeve, B.B., Gross, H.E., & DeWalt, D.A. (2016). Estimating
minimally important difference (MID) in PROMIS pediatric measures
using the scale-judgment method. Quality of Life Research, 25,
13-23.
-
One month ago Today
I felt alone.
never almost never sometimes
I felt like I couldnt do anything right.
never almost never sometimes
I felt everything in my life went wrong.
never almost never
I felt sad.
never almost never
I thought that my life was bad.
never almost never
I could not stop feeling sad.
never almost never
I felt lonely.
never almost never
I felt unhappy.
never almost never
sometimes
sometimes
sometimes
sometimes
sometimes
sometimes
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
T-score 62.1
I felt alone.
never almost never sometimes
I felt like I couldnt do anything right.
never almost never sometimes
I felt everything in my life went wrong.
never almost never sometimes
I felt sad.
never almost never
I thought that my life was bad.
never almost never
sometimes
sometimes
I could not stop feeling sad.
never almost never sometimes
I felt lonely.
never almost never
I felt unhappy.
never almost never
sometimes
sometimes
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
often almost always
T-score 58.9
The judges (clinicians, adolescents, parents) judge for each
pair whether the (imaginary) respondent is doing or feeling better,
worse, or about the same. Thissen, D., Liu,Y., Magnus, B., Quinn,
H., Gipson D.S., Dampier, C., Huang, I-C., Hinds, P.S., Reeve,
B.B., Gross, H.E., & DeWalt, D.A. (2016). Estimating minimally
important difference (MID) in PROMIS pediatric measures using the
scale-judgment method. Quality of Life Research, 25, 13-23.
-
For the Depressive Symptoms example, this process yields data
with summary statistics like these
Scale Score Frequency Proportion 1 month No Wrong
Pair ago Today Difference Better difference Worse Direction
2 49.5 57.9 8.4 23 19 185 0.10
3 56.7 62.1 5.4 32 18 176 0.14
1 43.5 45.9 2.4 15 151 61 0.07
5 64.3 62.1 -2.2 133 66 27 0.12
4 62.1 58.9 -3.2 179 33 15 0.07
6 73.4 66.0 -7.4 189 21 17 0.07
There were more data for Fatigue, Mobility, and Pain. Thissen,
D., Liu,Y., Magnus, B., Quinn, H., Gipson D.S., Dampier, C., Huang,
I-C., Hinds, P.S., Reeve, B.B., Gross, H.E., & DeWalt, D.A.
(2016). Estimating minimally important difference (MID) in PROMIS
pediatric measures using the scale-judgment method. Quality of Life
Research, 25, 13-23.
-
If the judges were homogeneous, data analysis could be logistic
regression of the probability different on the scale score
difference, with the 50-50 point the MID:
0.0
0.5
1.0
P("different")
0 1 2 3 4 5 6 7 8 Scale Score Difference
But the judges were not homogeneous.
Thissen, D., Liu,Y., Magnus, B., Quinn, H., Gipson D.S.,
Dampier, C., Huang, I-C., Hinds, P.S., Reeve, B.B., Gross, H.E.,
& DeWalt, D.A. (2016). Estimating minimally important
difference (MID) in PROMIS pediatric measures using the
scale-judgment method. Quality of Life Research, 25, 13-23.
-
So we treated the pairs of questionnaires as items, the
same-different judgments as item responses, and fitted the data
with the 1PL IRT model:
0.0
0.5
1.0
P("different")
5.73.6 2.4 1.15.6 2.3
-3 -2 -1 0 1 2 3 (Propensity to respond "different")
Thissen, D., Liu,Y., Magnus, B., Quinn, H., Gipson D.S.,
Dampier, C., Huang, I-C., Hinds, P.S., Reeve, B.B., Gross, H.E.,
& DeWalt, D.A. (2016). Estimating minimally important
difference (MID) in PROMIS pediatric measures using the
scale-judgment method. Quality of Life Research, 25, 13-23.
-
Then we interpolated the scale-score difference for a
hypothetical item that would be judged different 50% of the time by
an average respondent:
0.0
0.5
1.0
P("different")
5.73.6 2.4 1.15.6 2.3
-3 -2 -1 0 1 2 3 (Propensity to respond "different")
Thissen, D., Liu,Y., Magnus, B., Quinn, H., Gipson D.S.,
Dampier, C., Huang, I-C., Hinds, P.S., Reeve, B.B., Gross, H.E.,
& DeWalt, D.A. (2016). Estimating minimally important
difference (MID) in PROMIS pediatric measures using the
scale-judgment method. Quality of Life Research, 25, 13-23.
-
XO XO xt:::,. X I:::,. 0 0 0 0
D,. D,.
+ + X X
x+ + +
+ X 0 I:::,.
I:::,. _____________ _Q_ ___ _ +o
X X
We used quadratic regression to interpolate the scale-score
difference associated with a pair of questionnaires that would have
a 1PL b of zero:
Wrong Direction Omitted Wrong Direction Reversed
2 4
6 8
Sca
le S
core
Diff
eren
ce
Dep. Symp. Fatigue Mobility Pain
-3 -2 -1 0 1
2 4
6 8
Sca
le S
core
Diff
eren
ce
Dep. Symp. Fatigue Mobility Pain
-3 -2 -1 0 1
b b
Thissen, D., Liu,Y., Magnus, B., Quinn, H., Gipson D.S.,
Dampier, C., Huang, I-C., Hinds, P.S., Reeve, B.B., Gross, H.E.,
& DeWalt, D.A. (2016). Estimating minimally important
difference (MID) in PROMIS pediatric measures using the
scale-judgment method. Quality of Life Research, 25, 13-23.
-
Wrong Direction Wrong Direction Omitted Omitted
MID s.e. MID s.e.
Clinicians 2.1 0.6 1.9 0.6
Adolescents 2.2 0.6 2.1 0.6
Parents 2.4 0.7 2.2 0.7
MID is about two points on the T-score scale for these health
outcomes measures, with no clear difference among the domains.
Thissen, D., Liu,Y., Magnus, B., Quinn, H., Gipson D.S.,
Dampier, C., Huang, I-C., Hinds, P.S., Reeve, B.B., Gross, H.E.,
& DeWalt, D.A. (2016). Estimating minimally important
difference (MID) in PROMIS pediatric measures using the
scale-judgment method. Quality of Life Research, 25, 13-23.
-
A Free-Response Method to Estimate the Minimally Important
Difference (MID)
between Scores
(Morgan et al., 2017)
Morgan, E.M., Mara, C.A., Huang, B., Barnett, K., Carle,A.C.,
Farrell, J.E., & Cook, K.F. (2017). Establishing Clinical
Meaning and Defining Important Differences for Patient-Reported
Outcomes Measurement Information System (PROMIS) Measures in
Juvenile Idiopathic Arthritis Using Standard Setting with Patients,
Parents, and Providers. Quality of Life Research, 26, 565-586.
-
DeWitt, Cook, and their colleagues also used something like the
scaled-judgment method, but with the judges filling out the
responses to the after protocol to make it minimally different from
the (given) pre protocol.
This can be conceptualized as a free response variant of the
scaled-judgment method.
Morgan, E.M., Mara, C.A., Huang, B., Barnett, K., Carle,A.C.,
Farrell, J.E., & Cook, K.F. (2017). Establishing Clinical
Meaning and Defining Important Differences for Patient-Reported
Outcomes Measurement Information System (PROMIS) Measures in
Juvenile Idiopathic Arthritis Using Standard Setting with Patients,
Parents, and Providers. Quality of Life Research, 26, 565-586.
-
Morgan, E.M., Mara, C.A., Huang, B., Barnett, K., Carle,A.C.,
Farrell, J.E., & Cook, K.F. (2017). Establishing Clinical
Meaning and Defining Important Differences for Patient-Reported
Outcomes Measurement Information System (PROMIS) Measures in
Juvenile Idiopathic Arthritis Using Standard Setting with Patients,
Parents, and Providers. Quality of Life Research, 26, 565-586.
-
Future Research
Do these different methods of data collection yield consistent
results? Or are there predictable differences?
How do results from these methods compare to results obtained
with anchor-based methods, when anchors are available?
Everyone finds differences between groups of judges...
adolescents, parents, clinicians; what is to be made of that?
-
THE UNIVERSITY
of NORTH CAROLINA at CHAPEL HILL
Acknowledgments
This work was funded by the National Institutes of Health
through the NIH Roadmap for Medical Research, Grant
1U01AR052181-01.
Thanks to Dave Cella, Karon Cook, and Esi Morgan for their
graphics used in this presentation, and my collaborators Yang Liu,
Brooke Magnus, Hally Quinn, Debbie S. Gipson, Carlton Dampier,
I-Chan Huang, Pamela S. Hinds, Bryce B. Reeve, Heather E. Gross,
and Darren A. DeWalt at UNC and across the rest of the PROMIS
pediatric multi-site project.
-
Duke Robert J. Margolis, MD Center for Health Policy
Clinical Outcome Assessments: Establishing and Interpreting
Meaningful Within-Patient Change 4/4/17
-
Clinical Trial Exit Interviews
Presented at the Clinical Outcome Assessments: Establishing and
Interpreting Meaningful Within-Patient Change Meeting
The Duke-Margolis Center for Health Policy, Washington, DC,
April 4, 2017
Dana DiBenedetti, PhD Executive Director, Patient-Centered
Outcomes Assessment
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Acknowledgments
T. Michelle Brown Carla (DeMuro) Romano Lynda Doward Claire
Ervin Sheri Fehnel Sandy Lewis Diane Whalley
2
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
What is an Exit Interview?
The collection of (mostly) qualitative data from clinical trial
participants Most commonly, interviews are conducted soon after
participants complete
the treatment period However, patients (and/or caregivers)
experiences and perspectives
regarding treatment benefit may not be fully captured with
traditional COAs.
Interviews with clinical trial participants provide the
opportunity to more fully explore the impacts of investigational
products Describe the meaningfulness of treatment-related changes
(positive and
negative) Identify unanticipated treatment benefits
Information regarding pre-study experiences, as well as
treatment-related expectations and unmet needs can also be
collected.
3
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Why Do Exit Interviews?
To identify Characteristics of (sometimes new or rare) patient
populations What symptoms/impacts are most important to
patients
Allows participants to articulate concepts that may be important
to them but that are not obtained (or fully obtained) in the trial,
thus
Enriching researchers and sponsors understanding of the patient
experience Aiding in interpretation of other clinical data
Full impact of treatment (meaningful changes) Unmet needs of
treatment Expectations for and experiences with disease and of
treatment Thematic information used to inform future COA strategies
and
clinical trial designs Potential treatment differentiators
4
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Exit Interviews
Supplement, support, and facilitate the interpretation of data
from traditional PRO, PerfO, ObsRO and/or clinical measures Provide
greater depth and rationale for data from traditional measures
Describe treatment effects Explore the relevance and clinical
meaningfulness of specific treatment
changes beyond clinical indices and side effects Explain
anomalous results
5
-
RTI (h)(s} Health Solutions
knowledge. understanding.
The power of The value of
Sample Interview Concepts
Patients (and Caregivers) Experiences With and Attitudes About
Treatment Symptoms/impact prior to study start Expectations of
changes/outcomes
Can compare pre-study expectations with clinical outcomes
Anticipated or unanticipated benefits, impact of those benefits
Impact of treatment on daily life/functioning Impact of
treatment on most important/bothersome symptoms Onset of
benefits/changes
Treatment experiences Convenience of visits, monitoring Managing
treatment schedule (e.g., regimen schedule, infusions, monitoring)
Most challenging aspect of study treatment Managing adverse
events
How well treatment addresses most important/bothersome symptoms
Impact of treatment on daily life/functioning, quality of life
Satisfaction levels with treatment
Reasons for satisfaction
6
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Potential Applications
When to conduct interviews
Both within and outside the context of a clinical trial
Implementing as part of a clinical trial is generally more
efficient and
maximizes participation as compared with a separate or
subsequent study
At various time points (not just at the end of a study)
Baseline, at key time point(s) during the study, at the end of a
randomized
treatment phase, at the end of open-label extension, etc.
With all participants or select samples of study participants
Participants can be selected by site, country, experience of a
particular side
effect, patient-reported data
7
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Approaches to Conducting Patient Interviews
Approach 1: Experienced, trained qualitative researchers conduct
interviews Interviews conducted via telephone or
in-person at designated time(s) Can be prospectively planned
into the
CT protocol or done as a substudy Interviews follow a
semi-structured guide Values of this approach
Richest source of data, robust methodologically
Level of granularity from experienced interviewers
Limits the variability in data quality (vs large number of
individuals with varying degrees of qualitative experience)
Qualitative analysis usually done byinterviewers themselves
Approach 2: Study coordinators (SCs) conduct interviews
Qualitative interviewers would develop
interview guide/related materials, and provide training to
SCs
Certify, demonstrate proficiency Use a more standardized and
heavily
scripted interview guide SCs provide field notes, audio
recording
etc. to qualitative researchers who analyze qualitative
results
Values of this approach Although data may be less in-depth
than Approach 1 Particularly effective in global trials in
which interview process needs to be scaled to allow for maximal
participation
Allows for interview to be conducted by a someone familiar to
patient
8
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Issues to Consider in Operationalizing
What questions are you trying to answer with the interviews?
Exploratory, looking for a signal vs providing data/support for
primary endpoint? Do you need patients from all countries to
answer your questions
or sample of participants?
Population Sample size Who is going to conduct interviews?
Method Timelines Budget Senior-management buy in
9
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Potential Methodological Considerations / Limitations How, if at
all, exit interview activities influence CT data Self-selection
bias of exit interview volunteers (site and patient
level) Sample
All patients, subsample(s), size
How data will be analyzed How interview data relate to CT
data
Potential for additional adverse event reporting
10
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Factors Contributing to a More Successful Interview Study
General rule of thumb: the more sites and patients, the easier
and
less expensive it is to recruit Include prospectively in
clinical trial (vs. relying on sites and
patients to volunteer their participation) Increases site and
patient willingness and compliance Increases patient sample size
Interview substudy can be included as a component of a clinical
trial for select
countries (does not have to be for the entire study) Additional
protocol amendments and IRB reviews would not be needed Does not
significantly add to site burden Training for interview substudy
adds ~ 30 minutes to site initiation visits
11
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Factors Contributing to a More Successful Interview Study
Adequate time to design interview substudy and materials Target an
adequate sample size (e.g., 30-50 interviewed patients)
More likely to identify themes/signals (vs. 10-15 patients)
Larger site and patient pool increases likelihood of success
Easier and more efficient to recruit More buy-in from sites and
patients
Include in phase 1B or phase 2 study Increases chances of early
identification of signals (e.g., treatment benefits,
impacts) Learn what is important to patients that may not be
included in protocols Early signals can help inform future study
design, PRO measurement
strategy, selection of other study endpoints, systematic
measurement of new endpoints
12
-
Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Exit Interview Study Examples
13
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Example 1: Exit Interviews with COPD and Asthma
Patients in Prospective, Real World Clinical Studies RTI-HS
designed and is implementing an exploratory study to capture
patient-centered information in the context of two real-world
studies being conducted in chronic obstructive pulmonary disease
(COPD) and asthma.
The study is investigating the impact and management of COPD and
asthma from the patients perspective and highlighting the
potentialrelationship between treatment and both behavioral and
psychologicalfactors on patients experiences. Goal is to identify
key risk factors for exacerbations and treatment adherence.
A mixed methods approach is being used: Quantitative data is
being collected through the administration of structured,
closed-ended questions administered to all patients via
telephone interviews. Qualitative data is also being collected
through semi-structured, open-ended
questions on key topic areas administered to a subset of
patients via face to face interviews.
14
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Example 2: Interviews with Patients with Diabetic Gastroparesis
Before and After Treatment RTI-HS recently collaborated with a
pharmaceutical client developing a new
treatment for diabetic gastroparesis (DG) Participation in
qualitative interviews at both the beginning (pre-treatment)
and
end (post-treatment) of a phase 2 study was offered to all
clinical trial participants Primary objective of the pre-treatment
interviews was to inform the development
of a new PRO measure or modification of an existing PRO measure
by: Identifying a comprehensive set of DG symptoms Learning how
patients describe the burden and natural variation in these
symptoms Understanding the relative bothersomeness of the symptoms
Describing expectations related to successful treatment
Primary objective of the post-treatment interviews was to gather
in-depth information about participants experience with the study
drug, including the magnitude and relative importance of both
positive and negative changes
A manuscript describing the methods and results of this study
have just been submitted for publication
15
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Example 3: Exit Interviews with Clinical Trial
Participants with Carcinoid Syndrome (CS) Task: Regulatory
requirement that client assess and document the relevance and
clinical meaningfulness of specific CS-related symptoms and
their impacts Designed and implemented a qualitative study to
explore perceptions and
experiences of patients following their participation in a
clinical trial. Conducted telephone exit interviews with 35
patients across 16 sites in 5 countries
enrolled in a phase 3 clinical trial investigating a new
treatment for carcinoid syndrome to assess:
Participants experiences (symptoms and impacts) with their
disease Perceived benefits of the study treatment The clinical
meaningfulness of specific symptom improvements and their
associated impact to the patients
Mixed methods (qualitative and quantitative data) Data
analyzed
Qualitative Quantitative Compared with selected clinical trial
data
16
-
RTI (h)(s J Health Solutions
Ti1e power of Th e va lu e o f
knowledge. understanding.
Example 3: Exit Interviews with Clinical Trial Participants with
Carcinoid Syndrome (CS): Results Supported the primary endpoint of
decrease in diarrhea The 3 most important symptoms to treat and the
most bothersome
symptoms were diarrhea, BM frequency, and urgency. BM frequency
was reported as being more important to treat than stool
form/consistency. Meaningfulness of changes with treatment 95%
of participants who reported reductions in BM frequency noted
that
this was meaningful to them, allowing them to better enjoy life,
leave the house, and participate in social and other
activities.
I definitely feel like I'm not a prisoner in my house, staying
10 feet to the nearest bathroom. I can go out to activities
But the biggest change is not having to run to the toilet
constantlyYou can't live going 20 times a day. I was able to go out
more often
Most participants reported that a BM frequency reduction of at
least 30%would be considered meaningful.
17
-
Duke Robert J. Margolis, MD Center for Health Policy
Clinical Outcome Assessments: Establishing and Interpreting
Meaningful Within-Patient Change 4/4/17
-
-
Exploring the Use of
Anchor-Based Methods
to Derive and Interpret
Meaningful Within-
Patient Change
April 4, 2017
Gwaltney Consulting Confidential
-
-
ANCHOR-BASED METHODS
The anchor-based approaches use an external indicator, either
clinical or patient-based, to assign subjects into several
groupings reflecting no change, small positive changes, large
positive changes, small negative changes, or large negative changes
in clinical or health status (Revicki 2008; p. 104)
[Anchor-based methods] anchor change scores on the COA to an
external criterion that identifies study subjects who have
experienced an important change in their condition (PRO Consortium
2015)
Meaningful within-person change = Change on the target COA
measure for patients who experience meaningful improvement or
worsening on the anchor
Gold standard for estimating meaningful within-person change
(FDA 2009)
Gwaltney Consulting Confidential
-
-
TYPES OF ANCHORS
Global Impression Change Patient, Caregiver, Clinician
Reported
Global Impression of Symptoms Patient Reported
Disease Severity Categories e.g., New York Heart Association
Classification among
heart failure patients
Occurrence of a Meaningful Event e.g., Hospitalization, disease
relapse
Experience of certain degree of change on a disease-related
variable
e.g., Loss of 5% body fat in obese patients (Crosby 2003)
Gwaltney Consulting Confidential
-
-
EXAMPLE: PGIC
Please choose the response below that best describes the
overall change in your
since you started taking the study medication.
Very much Better
Moderately Better
A Little Better
No Change
A Little Worse
Moderately Worse
Very much Worse
Gwaltney Consulting Confidential
-
-
Dist~ibu~on of Change Scores by PGIIC C.at,egory
6 -Q,J .5
4 "ffi rJJ m m .,
2 - .5 0 c.. 0 -0
C w iii -G) -2 ~
0 0 Cl)
-4 C m
CL C 6 Q) C) C: -8 ra
.c u
-1,0 ---"""'""l!"- --,------......-----------n=-=""~---'
ESTIMATING WITHIN-PATIENT MEANINGFUL CHANGE
Farrar 2001; Pain
Gwaltney Consulting Confidential
-
-
TYPES OF ANCHORS
Global Impression Change Patient, Caregiver, Clinician
Reported
Global Impression of Symptoms Patient Reported
Disease Severity Categories e.g., New York Heart Association
Classification among
heart failure patients
Occurrence of a Meaningful Event e.g., Hospitalization, disease
relapse
Experience of certain degree of change on a disease-related
variable
e.g., Loss of 5% body fat in obese patients (Crosby 2003)
Gwaltney Consulting Confidential
-
-
EXAMPLE: PGIS
Please choose the response below that best describes the
severity of your over the
past week.
None
Mild
Moderate
Severe
Very Severe
Gwaltney Consulting Confidential
-
-
TYPES OF ANCHORS
Global Impression Change Patient, Caregiver, Clinician
Reported
Global Impression of Symptoms Patient Reported
Disease Severity Categories e.g., New York Heart Association
Classification among
heart failure patients
Occurrence of a Meaningful Event e.g., Hospitalization, disease
relapse
Experience of certain degree of change on a disease-related
variable
e.g., Loss of 5% body fat in obese patients (Crosby 2003)
Gwaltney Consulting Confidential
-
-
CONSIDERATIONS WHEN SELECTING
ANCHORS
Anchors should be easier to interpret than the PRO measure
itself (FDA, 2009)
Correlation between anchor and target COA should be greater than
0.30-0.40 (Hays 2005; Revicki 2008)
Should anchor assess change in a specific symptom/function or a
more global assessment of
health?
Recall bias with impression of change items
Most appropriate anchor type for different types of COAs?
Recommended to use multiple independent anchors and to examine
and confirm responsiveness across
multiple samples (Revicki 2008)
Gwaltney Consulting Confidential
http:0.30-0.40
-
-
CONSIDERATIONS WHEN USING
ANCHOR-BASED METHODS
Type of analysis to determine meaningful change? Descriptive:
Average COA score at each level of PGIC
Formal: Regression analysis, ROC curve
What level of change should be considered as the marker for
meaningful change? Minimal?
Moderate? Large?
Only use estimate from group that has changed? Difference
between changed and stable groups?
Non-linear relationship between anchor and COA score
Gwaltney Consulting Confidential
-
-
Dist~ibu~on of Change Scores by PGIIC C.at,egory
6 -Q,J .5
4 "ffi rJJ m m .,
2 - .5 0 c.. 0 -0
C w iii -G) -2 ~
0 0 Cl)
-4 C m
CL C 6 Q) C) C: -8 ra
.c u
-1,0 ---"""'""l!"- --,------......-----------n=-=""~---'
NON-LINEAR RELATIONSHIP BETWEEN PGIC AND PRO
Farrar 2001; Pain
Gwaltney Consulting Confidential
-
-
Dist~ibu~on of Change Scores by PGIIC C.at,egory
6 -Q,J .5
4 "ffi rJJ m m .,
2 - .5 0 c.. 0 -0
C w iii -G) -2 ~
0 0 Cl)
-4 C m
CL C 6 Q) C) C: -8 ra
.c u
-1,0 ---"""'""l!"- --,------......-----------n=-=""~---'
NON-LINEAR RELATIONSHIP BETWEEN PGIC AND PRO
Farrar 2001; Pain
Gwaltney Consulting Confidential
-
-
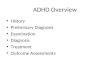
0 0 ....
0
=-'-~-1i--------+r 1: t,~ ~~ ...................... . I
' I
I 0 0
0
$ 0
0
g 0
0 0
0
v. much improved much improved mi1nlm. improved no change
mi1nim. worse much worse v. much worse answer to OG.I question
IG. 1. Boxplot: ofabsolute change from baseline to week 12 in
the number of moderate to _ever,e hot: flushe _ by answer to COi
question. COi,. Clinical loba Impression; v.} very; minim.~
minimally; ab_.} absolute.
NON-LINEAR RELATIONSHIP BETWEEN PGIC AND PRO
Gerlinger 2012; Menopause Gwaltney Consulting Confidential
-
-
CONSIDERATIONS WHEN USING
ANCHOR-BASED METHODS
Use of cross-sectional approaches? e.g., Difference between
disease severity categories at
single point in time
Effect of unblinding on PGIC rating?
False sense of precision Clinical trials are less likely to
acknowledge the error
associated with estimates
Different anchors can lead to substantially different findings
How integrate findings?
Gwaltney Consulting Confidential
-
-
REFERENCES
Crosby RD, Kolotkin RL, Williams GR. Defining clinically
meaningful change in health-related quality of life. J Clin
Epidemiol. 2003 May;56(5):395-407.
Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole RM.
Clinical importance of changes in chronic pain intensity measured
on an 11point numerical pain rating scale. Pain. 2001
Nov;94(2):149-58.
Gerlinger C, Gude K, Hiemeyer F, Schmelter T, Schfers M. An
empirically validated responder definition for the reduction of
moderate to severe hot flushes in postmenopausal women. Menopause.
2012 Jul;19(7):799-803
Hays RD, Farivar SS, Liu H. Approaches and recommendations for
estimating minimally important differences for health-related
quality of life measures. COPD. 2005 Mar;2(1):63-7.
PRO Consortium 2015. Interpreting Change in Scores on COA
Endpoint Measures
Revicki D, Hays RD, Cella D, Sloan J. Recommended methods for
determining responsiveness and minimally important differences for
patient-reported outcomes. J Clin Epidemiol. 2008
Feb;61(2):102-9.
Gwaltney Consulting Confidential
-
Duke Robert J. Margolis, MD Center for Health Policy
Clinical Outcome Assessments: Establishing and Interpreting
Meaningful Within-Patient Change 4/4/17
RTI-HS Exit interview overview slides_Duke-Margolis
conference_31MAR2017.pdfClinical Trial Exit Interviews
AcknowledgmentsWhat is an Exit Interview? Why Do Exit Interviews?
Exit InterviewsSample Interview ConceptsPotential
ApplicationsApproaches to Conducting Patient InterviewsIssues to
Consider in OperationalizingPotential Methodological Considerations
/ Limitations Factors Contributing to a More Successful Interview
StudyFactors Contributing to a More Successful Interview StudyExit
Interview Study ExamplesExample 1: Exit Interviews with COPD and
Asthma Patients in Prospective, Real World Clinical StudiesExample
2: Interviews with Patients with Diabetic Gastroparesis Before and
After TreatmentExample 3: Exit Interviews with Clinical Trial
Participants with Carcinoid Syndrome (CS)Example 3: Exit Interviews
with Clinical Trial Participants with Carcinoid Syndrome (CS):
Results