Clinical
39 | December 12 | 2003 OT
Clinical management of aniseikoniaAn overview
Clinical management of aniseikonia has long been neglected by
alarge part of the optometric community. One of the mainreasons is
the lack of simple and accurate instrumentation fordiagnosing and
measuring aniseikonia. With the knowledge that thenumber of
aniseikonia patients is significant, and that aniseikoniarules of
thumb often do not predict the actual situation well, newproducts
have recently emerged on the market to manageaniseikonia
clinically.
Gerard C. de Wit PhD and Arnulf Remole BFA, OD, MS, PhD
Aniseikonia is a binocular condition inwhich left and right
images differ in size orshape. There are two types of aniseikonia
static and dynamic aniseikonia1. The firsttype is the classical
aniseikonia, denoting aperceived image size difference with afixed
gaze direction. The second type ofaniseikonia is also called
inducedanisophoria2 and denotes a perceivedimage size difference
due to unequal prismeffects when looking through differentparts of
the two (anisometropic) spectaclelenses. For clinical purposes, the
two typesof aniseikonia are often related. The staticaniseikonia is
typically (but not always)two thirds of the dynamic
aniseikonia1.
SymptomsTable 1 classifies the symptoms ofaniseikonia. Because
most of these arerather general, it is sometimes difficult forthe
optometrist to recognise the condition.However, recognising and
treating thesymptomatic aniseikonia will usuallyresult in very
grateful patients and mayalso be financially rewarding for
theoptometrist.
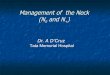
Alternatively, the aniseikonia can also besimulated by
presenting images ofdifferent size to the two eyes. This isshown in
Figure 1, where binocularseparation should be achieved by
usingred-green anaglyph glasses (see later).
IncidenceThe incidence of aniseikonia is oftenunderestimated.
The most well knownpatient group at risk is theanisometropes. The
prevalence ofanisometropia (>1D difference) above theage of 20
is 5-10%4. A second large groupof patients at risk for aniseikonia
is thepeople who have had cataract orrefractive surgery. For
example, Kramer etal5 found that 40% of all pseudophakeshad
ophthalmic complaints referable toaniseikonia. In England alone,
there areapproximately 250,000 cataractoperations annually6.
Because thesenumbers are significant and becauseaniseikonia rules
of thumb have beenproven unreliable7,8, testing for, andmanaging,
aniseikonia is important.
ManagementThe three basic steps of aniseikoniamanagement are:
Objectively measuring the aniseikonia Subjectively verifying that
the patient
would be helped by prescribingiseikonic lenses
Determining a new spectacleprescription to correct for
theaniseikonia
Measurement (objective eikonometry)There are two methods of
measuringaniseikonia: space perception eikonometryand direct
comparison eikonometry. Theobjective in a space
perceptioneikonometric measurement is to neutralisespace
distortions induced by theaniseikonia. Although this method can
bequite accurate in a laboratory setting, it isless suited for
clinical use. To ourknowledge, there are also no
commerciallyavailable instruments based on thismethod.
Regarding direct comparisoneikonometric tests, there are at
least twotests commercially available. One is theNAT (New
Aniseikonia Test, Handaya,Tokyo, Japan). The other is the
aniseikoniatest of the aniseikonia managementsoftware called the
Aniseikonia Inspector(Optical Diagnostics, Culemborg,
theNetherlands).
The principle of direct comparisoneikonometry is that a
different size target ispresented to each eye and that those
twosize targets have to be made equal in size
SSyymmppttoomm PPeerrcceennttaaggee ooff ppaattiieennttss
Headaches 67%Astenopia (fatigue, burning, tearing, ache, pain,
pulling, etc) 67%
Photophobia 27%
Reading difficulty 23%
Nausea 15%
Motility (diplopia) 11%
Nervousness 11%
Vertigo and dizziness 7%
General fatigue 7%
Distorted space perception 6%
For someone to experience thediscomfort of aniseikonia, he/she
couldput an afocal size lens in front of one eye.This type of lens
induces a magnification,but does not have an optical power.
Table 1Characteristic symptoms reported by 500patients referred
for aniseikonia examination3
Figure 1When using red-green anaglyph spectacles, this image
shows the discomfort produced by3% of aniseikonia (assuming the
viewer does not have inherent aniseikonia)
Clinical Gerard C. de Wit PhD and Arnulf Remole BFA, OD, MS,
PhD
40 | December 12 | 2003 OT
by either holding size lenses in front ofone eye, or by
physically changing the sizeof one of the size targets.
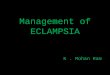
Figure 2 shows the half-circle sizetargets of the Aniseikonia
Inspector test.The layout of the test, in particular,
the(in)visibility of binocularly fuseableobjects around the size
targets, isimportant in comparison witheikonometry9. Due to
binocularly visibleobjects around the size targets, the NATtest
seems to underestimate aniseikonia10,while the Aniseikonia
Inspector testmeasures aniseikonia more correctly10,11.
Verification (subjective eikonometry)The second step in
aniseikoniamanagement is often to verify if thepatient would be
helped by iseikoniclenses. The reason is that the sensitivity
toaniseikonia can vary a lot from patient topatient. Some patients
are very grateful if1% of aniseikonia is corrected, whileothers
might not be bothered by as muchas 3% of aniseikonia.
Subjectiveeikonometry can be done by simulation,as shown in Figure
3, but a better way maybe to use size lenses.
CorrectionEquivalent to a sphere and cylinderrefractive error,
there is an overall and ameridional aniseikonia. For
clinicalpurposes, correcting the overallaniseikonia is usually most
important andsufficient1. That is, overall aniseikonia givesrise to
headache and asthenopia.Meridional aniseikonia, on the otherhand,
gives rise to distorted spaceperception.
The most effective way to reduce oreliminate aniseikonia is to
provide aniseikonic prescription. One cannot changethe effective
power at the cornea, becausethis would reduce the patients
visualacuity. However, one can change theaccompanying spectacle
magnifications ofthe corrective lenses by manipulating the
base curve, centre thickness, index ofrefraction, and back
vertex distance.
Besides the lack of instrumentation,determining an iseikonic
prescription wastoo big a hurdle for some optometrists toactually
manage aniseikonia. However,with the advent of
computers,determining such a prescription hasbecome much easier
(Figure 3).
ConclusionClinical management of aniseikonia usedto be done only
by a few specialists. Themain reasons for this lack of skill
andknowledge among optometrists arebelieved to be outdated and
insufficientinstruction, the lack of simple andaccurate
instrumentation, and therelatively complicated or
time-consumingdetermination of iseikonic spectacles. Onthe other
hand, the number ofaniseikonia patients is substantial andgrowing,
due to the ageing populationand the increase in cataract and
refractivesurgery operations.
Another reason, heard sometimes, fornot managing aniseikonia, is
thatiseikonic prescription spectacles can becosmetically
unattractive. Of course, thisdepends a lot on the amount
ofaniseikonia to be corrected and the framesize. There might also
be a trade-off toundercorrect aniseikonia to keep thespectacles
attractive. The trade-off betweenappearance and correction will
depend alot on the patient and on the severity ofthe symptoms. Many
aniseikonia patientswould prefer to trade a reduction in
goodappearance for more visual comfort. Also,the patient might
purchase two pair ofspectacles one for optimum visualcomfort for
daily routine and one foroptimum appearance during social
events.
A product like the AniseikoniaInspector now gives the
optometrist theopportunity to manage aniseikonia.Potential rewards
will be some verygrateful patients, a larger patient base, anda
possible increase in revenue.
About the authorsDr Gerard C. de Wit is involved withresearch at
Optical Diagnostics in theNetherlands. Dr Arnulf Remole is on
thefaculty of the School of Optometry at theUniversity of Waterloo
in Canada.
Special offerFor viewing Figure 1, Dr de Wit is offeringto send
a simple pair of red-greenspectacles to the first OT readers to
emailhim at [email protected].
References1. Remole A, Robertson KM (1996)
Aniseikonia and Anisophoria: CurrentConcepts and Clinical
Applications.Runestone Publishing, Waterloo, Ontario,Canada.
2. Friedenwald JS (1936) Diagnosis andtreatment of anisophoria.
Arch.Ophthalmol. 15: 283-307.
3. Bannon RE, Triller W (1944) Aniseikonia a clinical report
covering a ten-yearperiod. Am. J. Optom. 21: 171-182.
4. Weale RA (2002) On the age-relatedprevalence of
anisometropia. OphthalmicResearch 34: 389-392.
5. Kramer PW, Lubkin V, Pavlica M, Covin R(1999) Symptomatic
aniseikonia inunilateral and bilateral pseudophakia. A projection
space eikonometer study.Binoc. Vis. Strabis. Q. 14: 183-190.
6. NHS Executive (2000) Action on Cataracts:Good practice
guidance. Department ofHealth,
London(www.doh.gov.uk/cataracts).
7. Lubkin V, Shippman S, Bennett G. et al(1999) Aniseikonia
quantification: errorrate of rule of thumb estimation.Binoc. Vis.
Strabis. Q. 14: 191-196.
8. Kramer P, Shippman S, Bennett G et al(1999) A study of
aniseikonia and KnappsLaw using a projection space
eikonometer.Binoc. Vis. Strabis. Q. 14: 197-201.
9. Ogle KN (1950) Researches in BinocularVision. WB Saunders,
Philadelphia, USA.
10. McCormack G, Peli E, Stone P (1992)Differences in tests of
aniseikonia. Invest.Ophthalmol. Vis. Sci. 33: 2063-2067.
10. De Wit GC (2003) Evaluation of a newdirect-comparison
aniseikonia test. Binoc. Vis. Strabis. Q. 18: 87-94.
Figure 3Determining an aniseikonia corrected prescription with
the AniseikoniaInspector software is fast and easy
Figure 2Layout of the aniseikonia test of the Aniseikonia
Inspector. The patientuses red-green spectacles to separate the two
half-circle size targetsbinocularly. The objective of the test is
to make the two half-circlesvisually equal in size