Embed Size (px)
Citation preview

10/7/12
1
Clinical Insights in Hereditary Antithrombin Deficiency in Pregnancy
and the Role of Thrombate III® (Antithrombin III [Human])
Thrombate III is a registered trademark of Grifols Inc.; 2012. TH12-0312
In Our Discussion Today…
• Discuss the prevalence, clinical relevance, and risks associated with venous thromboembolism (VTE) and hereditary antithrombin (AT) deficiency in pregnancy
• Review the role of endogenous AT in coagulation and heparin therapy
• Discuss the data supporting the use of Thrombate III® (antithrombin III [human]) in patients with hereditary AT deficiency in high-risk situations, such as childbirth
• Review safety profile, dosing, and administration of Thrombate III
• Address commonly asked questions

10/7/12
2
Is Stephanie Your Next Patient?
• Stephanie’s history – 28-year-old female – Two first-trimester spontaneous abortions in past year – Diagnosed with hereditary AT deficiency – Family history
• Father: peripheral artery disease and fatal massive PE at age 55 • Sister: nonfatal DVT after long flight; 3 miscarriages
with no full-term pregnancies preceding DVT episode
• Current status – Uncomplicated pregnancy; took enoxaparin 40 mg BID and
wore compression stockings – Admitted for induction of labor at 39 weeks’ gestation – AT level at admission: 57%
BID, twice daily; DVT, deep vein thrombosis; PE, pulmonary embolism. Hypothetical case profile is not intended to convey clinical diagnostic or therapeutic recommendations.
What Is Hereditary AT Deficiency? Who Should Be Tested and When Should Those Patients Be Tested?

10/7/12
3
Overview of Hereditary AT Deficiency
• Rare but serious autosomal dominant disorder1
• >150 known AT mutations; various phenotypes1
• Defined as 40%-60% reduction in AT activity2
– Activated procoagulant proteins circulate longer3
– Increased risk of venous thromboembolism (VTE) and pulmonary embolism (PE)2,4
• No specific ethnic group or gender is affected more than others3,4
1. Maclean PS, Tait RC. Drugs. 2007;67:1429-1440. 2. Schwartz RS et al. Am J Med. 1989;87(suppl 3B):53S-60S. 3. Rajan A et al. eMedicine from WebMD. http://www.emedicine.com/med/topic150.htm. Accessed April 2, 2010. 4. Franchini M et al. Crit Rev Clin Lab Sci. 2006;43:249-290.
Prevalence
• Overall prevalence: 1 in every 500 to 5000 individuals1-3
– Approximately 60,000 to 600,000 people in the US are affected4
• >250,000 patients are hospitalized for VTE each year in the US5
– Up to 7500 (3%) may have hereditary AT deficiency6
• Up to 70% of pregnant women with hereditary AT deficiency who do not receive prophylactic therapy may experience thromboembolic complications7
1. Patnaik MM, Moll S. Haemophilia. 2008;14:1229-1239. 2. Thrombate III® (antithrombin III [human]) Prescribing Information. Research Triangle Park, NC: Grifols; 2009. 3. Wells PS et al. Am J Hematol. 1994;45:321-324. 4. US Census Bureau, Population Division. US and World Population Clocks—POPClocks. http://www.census.gov/main/www/popclock.html. Revised December 21, 2010. Accessed May 24, 2011. 5. Lloyd-Jones D et al. Circulation. 2010;121:e46-e215. 6. Franchini M et al. Crit Rev Clin Lab Sci. 2006;43:249-290. 7. Hellgren M et al. Gynecol Obstet Invest.1982;14:127-141.

10/7/12
4
Hereditary AT Deficiency: Defect May Be Quantitative or Qualitative
• Type I1
– Quantitative defect – Approximately 50% reduction in AT activity and
antigen levels – More common among symptomatic patients2
• Type II1,2
– Qualitative defect – More common among the general population2
– Reduction in AT activity but antigen levels may be normal • Subtype IIa: defect in the reactive site; high risk of thrombosis • Subtype IIb: defect in the heparin-binding site;
low risk of thrombosis • Subtype IIc: defects in both sites; high risk of thrombosis
1. Maclean PS, Tait RC. Drugs. 2007;67:1429-1440. 2. Patnaik MM, Moll S. Haemophilia. 2008;14:1229-1239.
1. Gutt CN et al. Am J Surg. 2005;189:14-22. 2. Tengborn L, Bergqvist D. Acta Chir Scan. 1988;154:179-183. 3. Kaaja RJ, Greer IA. JAMA. 2005;294:2751-2757. 4. Schwartz RS et al. Am J Med. 1989;87(suppl 3B):53S-60S. 5. Pabinger I, Schneider B. Arterioscler Thromb Vasc Biol. 1996;16:742-748.
When Is the Risk Highest in Hereditary AT Deficiency?
• Pregnancy – VTE risk3:
• Increases 7- to 10-fold during pregnancy • Is greatest after delivery
– Pregnancy-related VTE incidence: up to 70% in women with hereditary AT deficiency4
• Surgery – Orthopedic, oncologic, general, neurosurgery, and
gynecologic surgeries1
– Thrombotic complications in 17%-22% of surgical patients who did not receive AT concentrate2
• Thromboembolism – VTE: up to 85% of patients by age 505
– Recurrent thromboses: approximately 60% of patients5

10/7/12
5
Patient and Family History May Raise Suspicion of Hereditary Thrombophilia
• Patient History – Unexplained VTE at a younger age (<50 years) – Recurrent spontaneous VTE or unusually extensive
spontaneous VTE – Unexplained arterial thromboembolism in a younger patient – Unexplained VTE at an unusual site – Recurrence of VTE while adequately anticoagulated
• Family History – Family history of spontaneous VTE – Asymptomatic individual with family history of known
thrombophilia
• History of Pregnancy Loss – ≥3 unexplained pregnancy losses before 10 weeks’ gestation
or ≥1 loss after week 10
Foy P, Moll S. Curr Treat Options Cardiovasc Med. 2009;11:114–128.
Functional and Antigenic Assays Are Used in Making the Diagnosis
• Functional AT assays – Based on factor inhibition – Initial testing – High specificity
and sensitivity • Positive predictive
value of 96%
Kottke-Marchant K, Duncan A. Arch Pathol Lab Med. 2002;126:1326–1336.
• Antigenic AT assays – May differentiate type I
from type II – High specificity; limited
sensitivity
Functional assays measuring thrombin or factor Xa inhibition are the most
commonly used assays

10/7/12
6
Diagnostic Algorithm for Hereditary AT Deficiency
Repeat functional AT assay + Consider antigenic assay
• Functional assay result: LOW • Antigenic assay result: LOW
Possible type I hereditary AT deficiency
• Functional assay result: LOW • Antigenic assay result: NORMAL
Possible type II hereditary AT deficiency
Kottke-Marchant K, Duncan A. Arch Pathol Lab Med. 2002;126:1326–1336.
Results of functional AT assay: LOW
When Are Pregnant Patients at Greatest Risk of VTE?

10/7/12
7
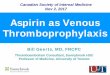
Hereditary AT Deficiency Increases Thrombotic Risk 20-Fold
Thrombotic risk may be lower depending on type of defect. Thrombate III® (antithrombin III [human]) is not indicated for the treatment of thrombophilias other than hereditary antithrombin deficiency. Adapted from Franchini M et al. Crit Rev Clin Lab Sci. 2006;43:249-290.
3
5
10
10
20
Prothrombin gene mutation
Factor V Leiden
Protein S deficiency
Protein C deficiency
Hereditary AT deficiency
Number of Times Relative to General Population 0 5 10 15 20 25
Hereditary AT deficiency increases thrombotic risk 20-fold.
Risk is greater than that of Factor V Leiden
Pregnant Women Are 4 Times More Likely to Suffer From VTE1
Virchow’s Triad Hypercoagulability Venous stasis
Vascular damage
1. James AH. Am J Med. 2007;120(10 suppl 2):S26-S34. 2. Andres RL, Miles A. Obstet Gynecol Clin North Am. 2001;28:613-630.
“During pregnancy and the postpartum period, women are 4 times more likely to suffer from VTE than when they are
not pregnant”1 because of Virchow’s triad.
Each component of Virchow’s triad is present in the pregnant woman2

10/7/12
8
Changes That Occur During Pregnancy
• Venous distention begins in 1st trimester1
• Venous flow to lower extremities is reduced by half by 3rd trimester1
• Increase in clotting factors I, II, VII, IX, X, XII and fibrinogen1-3
• Decrease in factors XI and XIII3
1. Hamersley SL. In: Shirato K, ed. Venous Thromboembolism: Prevention and Treatment. Tokyo: Springer-Verlag; 2005:143-150. 2. Andres RL, Miles A. Obstet Gynecol Clin North Am. 2001;28:613-630. 3. Bremme KA. Best Pract Res Clin Haematol. 2003;16:153-168.
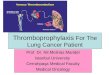
Risk of VTE Increases 25-Fold Immediately After Delivery
Heit JA et al. Ann Intern Med. 2005;143:697-706.
* Census estimates of the female population of Olmsted County were used to estimate person-years at risk. First trimester data not captured. Trim, trimester; PP, postpartum.
Number of VTEs (DVT or PE) during pregnancy and the postpartum period in the general population
Incidence of VTE increases 25-fold in the first week after delivery
Inci
denc
e pe
r 100
,000
wom
an-y
ears
*
0
500
1000
1500
2000
2500
3000
3500
4000
2nd Trim 3rd Trim Wk 1 PP Wk 2 PP Wk 3 PP Wk 4 PP Wk 5 PP Wk 6 PP

10/7/12
9
What Is the Role of Antithrombin in Achieving Anticoagulation?
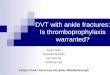
AT Provides 80% of the Natural Anticoagulant Effect Against Thrombin1
• 58 kDa glycoprotein produced in the liver1
• Half-life ~ 2-3 days1
• Binds irreversibly to thrombin and factor Xa, preventing the conversion of fibrinogen into fibrin2,3
• AT is necessary for the anticoagulation effects of heparin3
1. Maclean PS, Tait RC. Drugs. 2007;67:1429-1440. 2. Kottke-Marchant K, Duncan A. Arch Pathol Lab Med. 2002;126:1326-1336. 3. Li W et al. Nat Struct Mol Biol. 2004;11:857-862. 4. Patnaik MM, Moll S. Haemophilia.2008;14:1229-1239. With permission from John Wiley and Sons.
(a) Antithrombin (red) bound to factor Xa (orange) and a pentasaccharide (yellow);
(b) Antithrombin bound to thrombin (green) and heparin (yellow).4

10/7/12
10
Norris LA. Best Pract Res Clin Obstet Gynaecol. 2003;17:369-383.
Antithrombin Inactivates Several Clotting Factors
HMWK, high-molecular-weight kininogen; PK, prekallikrein; TF, tissue factor.
TF
FIIa (thrombin) FII
FXa
FVa
FXIa
FXI
FIX
FXIIa
FXII
Intrinsic Pathway
HMWK
PK
Kallikrein Tissue Factor Pathway
FVIIIa
FXa
FX
FIXa FVIIa
Fibrinogen
Fibrin CLOT
AT AT
Common Pathway
Antithrombin Inactivates Several Clotting Factors
Ca++
PL
PK HK
HK
Ca++
TF XII
XI
IX
VIIa VII
VIIa/TF
VIIIa
X
PT
VIII
V Va
Ca++
PL
Fibrinogen Fibrin monomer
Fibrin polymer X-linked fibrin
XIIa
XIa
IXa
Xa
Th ATIII
Hamersley SL. In: Shirato K, ed. Venous Thromboembolism: Prevention and Treatment. Tokyo: Springer-Verlag; 2005:143-150. With permission of Springer Science+Business Media.

10/7/12
11
AT Irreversibly Binds to and Inhibits Factor Xa and Thrombin
AT provides 80% of the natural anticoagulant effect against thrombin
Adapted from Turpie AG et al. N Engl J Med. 2001;344:619-625. Maclean PS, Tait RC. Drugs. 2007;67:1429-1440.
What Is the Role of AT Replacement in Patients With Hereditary AT Deficiency During Pregnancy,
Labor, and Childbirth?

10/7/12
12
How Do We Approach the Management of Stephanie’s Case?
• Patient assessment – Last dose of enoxaparin administered 24 hours before
arrival at hospital – Normal blood pressure, pulse, temperature – Normal fetal status per fetal monitoring – Ultrasound and examination to assess for signs
of DVT were unremarkable – Patient height: 5′4″ – Patient weight: 154 lbs (70 kg) – AT activity level of 57%
• Call to action: Schedule intermittent measurements of patient’s AT activity level in anticipation of delivery
Hypothetical case profile is not intended to convey clinical diagnostic or therapeutic recommendations.
Goal of Guidelines: Minimize Bleeds and Return AT Levels to Normal
According to Consensus Report and Recommendations for Prevention and Treatment of Venous Thromboembolism and Adverse Pregnancy Outcomes: • AT deficient patients are “hypercoagulable”
during the ante-, intra-, and postpartum periods • Patients who develop or are at increased risk to
develop acute thrombosis should receive – AT concentrate – Adjusted-dose anticoagulation
• AT levels should be returned to normal and maintained at the normal level for 2-8 days in obstetric patients receiving AT concentrate
Duhl AJ et al. Am J Obstet Gynecol. 2007;197:457.e1-457.e21.

10/7/12
13
Thromboprophylaxis in Pregnancy
According to the ACOG Practice Bulletin: • Recommended thromboprophylaxis for pregnancies
complicated by inherited thrombophilias:1,2
• Women with AT deficiency may be candidates for AT concentrates in the peripartum period1,2
High Risk* (no previous VTE)
High Risk* (single previous VTE, not on long-term anticoagulation therapy)
Antepartum Management
Prophylactic LMWH or UFH
Prophylactic, intermediate-dose, or adjusted-dose LMWH/UFH regimen
Postpartum Management
Anticoagulation therapy
Anticoagulation therapy, intermediate- or adjusted-dose LMWH/UFH x 6 weeks†
* Including AT deficiency. † Therapy level should be at least as high as antepartum treatment.
1. James A. Obstet Gynecol. 2011;118:718-729. 2. Lockwood C, Wendel G. Obstet Gynecol. 2011;118:730-740.
ACOG, American College of Obstetricians and Gynecologists.
AT Replacement Can Be Used During the Critical Window
• The time period before initiating regional anesthesia is a critical window during which hereditary AT deficiency patients are at high risk for VTE1,2
• AT replacement can be used during this critical window3
Pregnant patient with hereditary AT deficiency
Delivery
1. Duhl AJ et al. Am J Obstet Gynecol. 2007;197:457.e1-457.e21. 2. Horlocker TT et al. Reg Anesth Pain Med. 2003;28:172-197. 3. Sabadell J et al. Eur J Obstet Gynecol Reprod Biol. 2010;149:47-51.
LMWH and/or UFH is withheld due to bleeding concerns
and administration of regional anesthesia

10/7/12
14
AT Concentrate: Proven Safety and Effectiveness
• The effect of heparin and AT concentrate* during pregnancy was evaluated in 8 women with hereditary AT deficiency during 9 pregnancies
• AT concentrate was administered during delivery or abortion and the AT level was maintained at ≥80%
• The anticoagulant effect of heparin was enhanced with the increase in AT activity level
• No bleeding complications, allergic reactions, thrombocytopenia, or liver insufficiencies occurred
• No thrombotic events occurred during the time period in which AT concentrate was administered
Hellgren M et al. Gynecol Obstet Invest.1982;14:127-141. * The AT concentrate used in this study was not Thrombate III® (antithrombin III [human]).
Event
Diagnosed and Treated
(n/N)
Not Diagnosed and Not Treated†
(n/N)
VTE 0/11 (0%) 3/7 (43%)
AT Concentrate in the Peripartum Period Helps Prevent VTE Without Complications
• Retrospective study of 18 pregnancies among 9 patients with hereditary AT deficiency. Treatment defined as LMWH during pregnancy and AT concentrate* during the peripartum period
n = number of pregnancies with the listed event; N = total number of pregnancies in the analysis group. * The AT concentrate used in this study was not Thrombate III® (antithrombin III [human]). † Thromboprophylaxis was given in all pregnancies in which hereditary AT deficiency was diagnosed at the time. ‡ All patients received neuraxial anesthesia.
Sabadell J et al. Eur J Obstet Gynecol Reprod Biol. 2010;149:47-51.
Potential Complication
Incidence of Complication With AT
Concentrate Treatment
Complications following neuraxial anesthesia‡ 0%
Heavy bleeding 0%

10/7/12
15
A Treatment Plan for Stephanie
• Treatment goals – Overall treatment goal: deliver full-term infant while
preventing VTE due to hereditary AT deficiency – Increase AT activity level via administration of
Thrombate III®
• Increase level from 57% of normal to between 80% and 120% during delivery and postpartum
• Birth plan – Induce labor – Deliver vaginally with epidural anesthesia – Administer Thrombate III before initiating regional
anesthesia and postpartum for up to 1 week
Hypothetical case profile is not intended to convey clinical diagnostic or therapeutic recommendations.
FDA-approved for patients with hereditary AT deficiency in connection with surgery
or obstetrical procedures or when they suffer from thromboembolism
Please see Important Safety Information about Thrombate III® on slides 45 and 46 and refer to complete Prescribing Information for complete prescribing details.

10/7/12
16
Thrombate III®: Mimics the Mechanism of Action of Endogenous AT
• Thrombate III is a preparation of antithrombin concentrate purified from human plasma
• Replaces antithrombin that is normally present in the body
• Restores body’s natural ability to inhibit clot formation
• Half-life (3.8 days) similar to endogenous antithrombin
Thrombate III® (antithrombin III [human]) [prescribing information]. Research Triangle Park, NC: Grifols; 2009.
Thrombate III®: Pivotal Efficacy
Objective1
• Patients with hereditary AT deficiency were treated with Thrombate III if they
– Required prophylaxis for a condition associated with increased risk of thromboembolism (surgery or pregnancy)
– Required short-term treatment for thrombosis or pulmonary embolism
• Treatment with Thrombate III – Dosed to maintain plasma AT levels in the range of 75%-120%*
of normal1
– Continued until clinical condition resolved, patient was treated with oral anticoagulants, no further benefit was expected, or patient experienced side effects that led to withdrawal2
1. Data on file, Grifols. 2. Schwartz RS et al. Am J Med. 1989;87(suppl 3B):53S-60S.
* This is per the study protocol.

10/7/12
17
No Cases of Thrombotic Complications During Surgical and Obstetrical Procedures1,2
Clinical situation No. of cases Therapeutic outcome
Prophylaxis Childbirth 5* No thrombosis or pulmonary
embolism Surgery 11* No thrombosis or pulmonary
embolism Treatment
Thromboembolism 8† No further thromboembolic episodes‡
* Data included 13 patients treated on 16 separate occasions (1 patient was treated for both surgery and childbirth). Average baseline antithrombin level was 53% (range, 22%-71%). Heparin was administered in 3 of the 11 surgical procedures and all 5 deliveries.
† All patients received heparin. ‡ One patient died of nontreatment-related causes.
1. Thrombate III® (antithrombin III [human]) [prescribing information]. Research Triangle Park, NC: Grifols; 2009. 2. Data on file, Grifols.
One Dosing Formula for Thrombate III®
• Dosing recommendations – As a general recommendation, increase AT activity to 120%
of normal levels – Plasma levels between 80% and 120% may be maintained
with maintenance doses of 60% of the initial loading dose, given every 24 hours for 2-8 days
– Adjustments in the maintenance dose and/or interval between doses should be made based on the actual plasma AT levels achieved
Calculation of initial loading dose of AT
Units required (IU) = [desired – baseline AT level*] x weight (kg)
1.4 * Expressed as percent of normal level based on functional AT assay.
The anticoagulant effect of heparin is enhanced by concurrent treatment with Thrombate III in patients with hereditary antithrombin deficiency. Thus, in order to avoid bleeding, reduced dosage of heparin is recommended during treatment with Thrombate III. Thrombate III® (antithrombin III [human]) [prescribing information]. Research Triangle Park, NC: Grifols; 2009.

10/7/12
18
• Digital dosing calculator – Allows you to quickly calculate the loading and maintenance doses – Available for the iPhone®, iPad®, and DROID® mobile digital devices – Easy and free: go to app store and search for “Thrombate”
Easy Dosing Calculations: Use the App for Thrombate III®
iPod and iPad are registered trademarks of Apple Inc. DROID is a registered trademark of Lucasfilm Ltd. and its related companies.
Thrombate III® Provides Concentrated Antithrombin Replacement for Patients With Hereditary AT Deficiency
Thrombate III*1 FFP2,3
How supplied 500-IU vials 250-mL bags AT concentration 50 IU/mL ~1 IU/mL Volume in a 3500-IU loading dose† 70 mL‡ (bolus infusion) 3500 mL (14 bags)
Other considerations
• Convenient to store, reconstitute, and administer
• Requires thawing time • Requires blood testing and coordination with blood bank
1. Thrombate III® (antithrombin III [human]) [prescribing information]. Research Triangle Park, NC: Grifols; 2009. 2. American Association of Blood Banks, America’s Blood Centers, American Red Cross. Circular of information for the use of human blood and blood components. July 2002. 3. Bharadwaj J et al. Lab Hematol. 2003;9:125-131.
FFP, fresh frozen plasma. * Head-to-head clinical trials comparing Thrombate III and FFP in patients with hereditary AT
deficiency have not been conducted. † Loading dose example based on a 70-kg patient with 50% AT activity. ‡ Based on calculation of 7 vials and 10 mL of diluent per vial.

10/7/12
19
Easy Administration and Convenient Storage
• Bolus intravenous infusion • Infusion rate is adapted to patient response
– Total infusion time of 10-20 minutes is generally well tolerated
• Administer within 3 hours following reconstitution
• Room temperature storage (not to exceed 25°C [77°F])
• Convenient vial size to minimize waste – Approximately 500 IU reconstituted to 10 mL
Thrombate III® (antithrombin III [human]) [prescribing information]. Research Triangle Park, NC: Grifols; 2009.
Approach to Dosing for Stephanie
• Initial Thrombate III® dose of 3150 IU administered without complication
Units required (IU) = [120 – 57] x 70 (kg) 1.4
• Low-volume bolus: 63 mL • Epidural catheter placed when Stephanie’s cervix
was dilated to 4 cm; placement uneventful • AT activity assay 5 hours after epidural placement
was 105% • No complications of delivery; healthy infant delivered
Hypothetical case profile is not intended to convey clinical diagnostic or therapeutic recommendations.

10/7/12
20
Postpartum Approach for Stephanie
• Individualized maintenance dose of Thrombate III®
– 60% of total loading dose administered every 24 hours
– Goal: maintain AT activity levels in the normal range (80% to 120%) until discharge
– Adjustments in maintenance dose and/or interval between doses should be based on actual plasma AT levels achieved
Hypothetical case profile is not intended to convey clinical diagnostic or therapeutic recommendations.
Safety Profile for Thrombate III®
Commitment to Safety • No known contraindications1 • Pregnancy category B1
• Pasteurized to inactivate viruses, with no confirmed cases of virus transmission
– Thrombate III is made from human plasma. Products made from human plasma may contain infectious agents, such as viruses, and, theoretically, the Creutzfeldt-Jakob agent that can cause disease
Tolerability • In clinical studies with Thrombate III, the most common side effects
were dizziness (2%), chest tightness (0.9%), nausea (0.9%), and foul taste in the mouth (0.9%)1
Experience • Used for the treatment of hereditary antithrombin deficiency for
>20 years2
The anticoagulant effect of heparin is enhanced by concurrent treatment with Thrombate III in patients with hereditary antithrombin III deficiency. Thus, in order to avoid bleeding, reduced dosage of heparin is recommended during treatment with Thrombate III. 1. Thrombate III® (antithrombin III [human]) [prescribing information]. Research Triangle Park, NC: Grifols; 2009. 2. Scott GR et al. FDA Drug and Device Product Approvals; 1991;14(2):333.

10/7/12
21
Thrombate III®: Proven Effective in Pregnant Women With Hereditary AT Deficiency
• Risk of VTE is highest in the first week after delivery1
• Up to 70% of pregnant women with hereditary AT deficiency who do not receive prophylactic therapy may experience thromboembolic complications2
• Patient and family history may indicate a need for AT deficiency testing3
• In clinical studies of Thrombate III, no cases of thrombotic complications during surgical and obstetrical procedures were reported4
• Thrombate III® replaces antithrombin that is normally present in the body
1. Heit JA, et al. Ann Intern Med. 2005;143:697-706. 2. Hellgren M et al. Gynecol Obstet Invest. 1982;14:127-141. 3. Foy P, Moll S. Curr Treat Options Cardiovasc Med. 2009;11:114–128. 4. Thrombate III® (antithrombin III [human]) [prescribing information]. Research Triangle Park, NC: Grifols; 2009.
Thrombate III is made from human plasma. Products made from human plasma may contain infectious agents, such as viruses, and, theoretically, the Creutzfeldt-Jakob disease (CJD) agent that can cause disease. There is also the possibility that unknown infectious agents may be present in such products.
Case Study: Denise
Thrombate III® in the Peripartum Period

10/7/12
22
Denise: 25-Year-Old Patient in the 36th Week of Pregnancy
• History – After an episode of mesenteric vein thrombosis at
age 17 years, Denise was diagnosed with hereditary AT deficiency and placed on lifelong anticoagulation with warfarin
– Denise has a history of one missed abortion
• Current Status – Denise is being admitted for induction of labor due
to oligohydramnios – Warfarin was changed to enoxaparin at a dose of
60 mg BID when she was found to be pregnant – Her AT level on warfarin was 47%
Data on file, Grifols.
BID, twice daily.
Denise’s Postpartum Course
0255075
100125150
0 1 2 3 4 5 6
Day
Func
tiona
l AT
(%)
• Weight was 152 pounds on admission; antithrombin level was 45%. She received antithrombin concentrate targeting 100% as the desired level on Day 0, Day 2, and Day 4 of hospitalization.
• Delivery was late on Day 1, with last enoxaparin dose prior to that on the day of admission. The newborn had an uneventful recovery.
• Enoxaparin 30 mg BID was started immediately after delivery (Day 2) and continued until discharge • Warfarin was also started on Day 2, and she was discharged home on a dose of 5 mg/day, with
instructions to watch for bleeding and have regular PT/INR checks. No complications were noted.
AT (IU) 2.60
1280 2710 1380 2.67 2.45 0.99 0.97 INR
Warfarin dose (mg) 7.5 5.0 0.5 5.0 5.0
delivery discharge
INR, international normalized ratio; PT, prothrombin time. Data on file, Grifols.

10/7/12
23
Important Safety Information
• Thrombate III is indicated for the treatment of patients with hereditary antithrombin deficiency in connection with surgical or obstetrical procedures or when they suffer from thromboembolism.
• In clinical studies with Thrombate III, the most common side effects were dizziness, chest tightness, nausea, and foul taste in the mouth.
• The anticoagulant effect of heparin is enhanced by concurrent treatment with Thrombate III in patients with hereditary antithrombin III deficiency. Thus, in order to avoid bleeding, reduced dosage of heparin is recommended during treatment with Thrombate III.
Please see accompanying Thrombate III full Prescribing Information for complete prescribing details.
CORE
Important Safety Information
• Thrombate III is made from human plasma. Products made from human plasma may contain infectious agents, such as viruses, and, theoretically, the Creutzfeldt-Jakob disease (CJD) agent that can cause disease. There is also the possibility that unknown infectious agents may be present in such products.
• Individuals who receive infusions of blood or blood plasma may develop signs and/or symptoms of some viral infections, particularly hepatitis C.
Please see accompanying Thrombate III full Prescribing Information for complete prescribing details.
CORE

10/7/12
24