-
Clinical HIV-1 eradication studies
Mathias Lichterfeld, M. D., Ph. D. Massachusetts General
Hospital
Harvard Medical School
No disclosures
-
HIV
RN
A (c
ps/m
L)
50
Years on cART 0 1
1
Slide courtesy of Javier Martinez-Picado/Sharon Lewin
Plasma single copy assay
Cell associated HIV DNA
Infectious virus (IUPM)
Blood Tissue Cell associated HIV DNA
Cell associated HIV RNA
HIV-1 persistence despite HAART
>10 years
-
Eckstein, Immunity 2001; Swiggard, J Virol 2005; Saleh, Blood
2007; Marini, J Immunol 2008; Bosque, Blood 2009; Cameron, PNAS
2010; Lassen, PLoS One 2012
Activated CD4+ T cell
Resting CD4+ T cell
cART
Survival (long-half life)
Homeostatic proliferation
Latent and replicative HIV-1 infection in CD4 T cells
Slide courtesy of Javier Martinez-Picado/Sharon Lewin
-
Clinical HIV-1 eradication strategies
•Ex-vivo gene editing/gene therapy to reduce viral
co-receptor
expression, followed by adoptive immunotherapy of HIV-1
resistant cells
• Bone marrow/HSC transplantation with CCR5-negative grafts
• Combination of latency reversing agents with immune
mediated
interventions (“kick and kill”)
-
HMTi EZH2 inhibitors
PKC activators Prostratin
DNA methylation Inhibitors
Didier Trono et, al. Science 2010
Pharmacological latency-reversing agents “Shock” component
HDACi Panobinostat Romidepsin Vorinostat
-
• Vaccines designed to induce effector T cell responses •
Broadly-neutralizing antibodies, possibly labeled with
Immunotoxins etc.
• Activators of innate immunity • Immunoregulatory interventions
(i. e. PD-1 inhibitors etc)
Immune-mediated interventions “kill” component
-
TF
OFF
Bolden, Nat Rev Drug Disc 2006; Prince. Clin Canc Res 2009;
Contreras, J Biol Chem 2009; Archin AIDS Res Hum Retrovir 2009;
Reuse, PLoS One 2009; Burnett , J Virol 2010
HDACi
DNA nucleosomes
HDACi turn HIV-1 transcription “on”
Slide courtesy of Javier Martinez-Picado/Sharon Lewin
-
Clinical studies with HDACi
Vorinostat (Merck) Romidepsin (Celgene/Gilead)
Panobinostat (Novartis)
Ex-vivo HIV-1 reactivation
weaker strong strong
Dose, dosing schedule and formulation
400mg p. o. •Single-dose (Archin et al, Nature 2012)
•three consecutive doses per week for eight weeks (Archin et al,
JID 2014)
•daily for 14 days (Elliott et al, CROI 2013)
• 5mg/m2 i. v. single-dose infusion (Aarhus)
• 0.5/2/5mg/m2 (ACTG)
20mg p. o. TIW (M, W, F) QOW •Rasmussen et al, Lancet HIV
2014
Pilot clinical trials in HAART-treated
HIV patients
completed (UNC, Melbourne)
in process (ACTG, Aarhus)
completed (Aarhus)
-
Archin et al, Nature 2012 and JID 2014
Elliott/Lewin, CROI 2013
• Single dose vorinostat led to a 4.8-fold increase in
cell-associated HIV RNA.
• No significant increases in HIV-1 RNA during repetitive
dosing
• No change in HIV-1 DNA
• Multiple dose vorinostat led to a mean 2.5-fold increase in
cell-associated HIV RNA in total CD4+ T cells.
• No effect on CD4 T cell-associated HIV-1 DNA or plasma HIV-1
RNA
Clinical studies with Vorinostat (Saha)
-
• Licensed in US for treatment of PTCL and CTCL
• Can reactive HIV-1 in ex-vivo assays (Wei et al, Plos Path
2014)
• Currently being tested in RCT (ACTG5315) (single dose at
0.5mg/m2, 2mg/m2, 5mg/m2)
• In vivo evaluation in a non-randomized trial in six patients
(Sogaard et al, IAS 2014)
– Romidepsin (5 mg/m2) iv on day 0, 7, and 14 – Endpoints:
Safety, cell-associated HIV RNA, plasma HIV RNA
– Self-reported AEs: Total of 40, 36 related to RMD. Most
common:
• Nausea, vomiting, diarrhea, abdominal pain • Fatigue • All
self-resolving, none with > grade 2
Romidepsin
http://en.wikipedia.org/wiki/File:Romidepsin_structure_(2).svg
-
Cell-associated HIV-1 RNA during treatment with Romidepsin
Sogaard et al, IAS 2014
-
Viral load: COBAS® TaqMan® HIV-1 Test, v2.0 TMA: Qualitative NAT
screening system (PROCLEIX ULTRIO Plus, Genprobe)
Plasma HIV-1 RNA during treatment with Romidepsin
Sogaard et al, IAS 2014
-
Cell-associated HIV-1 DNA during treatment with Romidepsin
Sogaard et al, IAS 2014
-
Panobinostat (LBH589)
• A hydroxamic acid pan-HDAC inhibitor • Developed by Novartis
for the treatment
of multiple myeloma (approval expected in 2014)
• Dosed 30-60 mg TIW or TIW QOW • Inhibitory activity in the
lower nM range
against HDACs 1, 2 and 3 which appear important to maintaining
HIV latency
Huber et al 2011. J Biol Chem Keedy et al 2009. Journal of
Virology Archin et al 2009. AIDS
• Panobinostat induced HIV production in latently infected cell
lines and primary T cells with high potency
Rasmussen et al 2013, HVI
-
Overall study design
• Blood draws – Twice at baseline – Twice every treatment cycle
and once every pause week (13 times during panobinostat
treatment) – 12 and 32 weeks after panobinostat initiation
• Lumbar puncture and sigmoid biopsies before and during the
last treatment cycle
-
Safety – adverse events
• A total of 16 AEs presumed related to panobinostat (all CTCAE
grade 1) • 10/15 patients experienced AEs presumed related to
panobinostat • Fatigue the most frequent AE (experienced by 7/15
patients) • All completed full panobinostat dosing and
follow-up
Rasmussen et al, Lancet HIV 2014
-
• A highly statistically significant increase over time
(repeated measurement ANOVA; P
-
HIV-1 plasma viremia during treatment with panobinostat
Transcription mediated amplification (TMA)-based detection of
HIV RNA:
50% analytic sensitivity to detect 3.8 copies/ml
95% analytic sensitivity to detect 12 copies/ml
• Only 1/15 remained undetectable at all time points during
panobinostat treatment • 4/15 patients positive at all time points
(make up 8/9 positive baseline values) • 9/15 negative at both
baseline samples and became positive during panobinostat
treatment
Rasmussen et al, Lancet HIV 2014
-
Total cell-associated HIV-1 DNA during treatment with
panobinostat
• Decrease from baseline to day 14 (end of first treatment
cycle) • Overall no decline in total HIV DNA from baseline to week
12 (4 weeks post treatment)
Measured per 106 CD4+ T cells using ddPCR
Rasmussen et al, Lancet HIV 2014
-
• 4/15 patients displayed sustained reductions in total HIV DNA
• No difference in nadir CD4, baseline CD4 or baseline HIV DNA
Total cell-associated HIV-1 DNA during treatment with
panobinostat
-
Total HIV DNA during panobinostat treatment – post-hoc
analysis
-
Change in HIV-1 DNA during treatment with panobinostat
correlates with kinetics
of viral rebound during ATI
• 9/15 patients agreed to participate in ATI, including three
“responder patients”
• No association between baseline characteristics and viral
rebound during ATI
Rasmussen et al, Lancet HIV 2014
0 20 40 60 80101
102
103
104
105
106
107
time after treatment interruption (days)
plas
ma
viral
load
(cop
ies/
ml)
0 20 40 60 80101
102
103
104
105
106
107
time after treatment interruption (days)
plas
ma
viral
load
(cop
ies/
ml)
-
Expansion of HIV-1-specific CTL during Panobinostat
treatment
0
500
1000
1500
2000
tota
l mag
nitu
de o
fH
IV-1
-spe
cific
CTL
(SFC
/mill
ion
PBM
C)
p=0.007
Magnitude Breadth
0
2
4
6
8
tota
l bre
adth
of
HIV
-1-s
peci
fic C
TL(n
o of
res
pons
es)
p=0.01
before treatment
before treatment
after treatment
after treatment
• Screening for CTL with library of optimal CTL epitopic
peptides (IFN-γ Elispot)
-
HIV-1-specific CTL are not associated with HIV-1 DNA changes
during
panobinostat treatment
Interferon-γ TNF-α
FC HIV-1 DNA (log10) FC HIV-1 DNA (log10) FC H
IV-1
-spe
cific
effe
ctor
CTL
FC H
IV-1
-spe
cific
effe
ctor
CTL
• no associations between CTL magnitude or breadth and HIV-1 DNA
levels • also no associations between protective HLA class I
alleles and HIV-1 DNA levels
-
Expression patterns of Interferon-stimulated genes correlate
with HIV-1 DNA decrease during treatment
with panobinostat
-
HIV-1 DNA decrease during panobinostat treatment occurs
preferentially in carriers of IL28B “CC”
carriers
CC CT0.1
1
10Fo
ldc h
ange
into
talH
I V-1
DN
A p=0.04
CC CT0.1
1
10Fo
ldc h
ange
into
talH
IV- 1
DN
A p=0.04
IL-28B
-
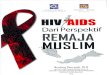
Changes in HIV-1 DNA during panobinostat treatment are
correlated to changes in NK cells
0.1 1 100
1
2
3
FC in HIV-1 DNA (log10)
FC in
CD
69+
NK
cel
ls
0.1 1 100.0
0.5
1.0
1.5
2.0
2.5
FC in HIV-1 DNA (log10)
FC in
CD
69+
NK
cel
ls
0.25 1 4 160
1
2
3
FC in HIV-1 DNA (log10)
FC in
CD
69+
NK
cel
ls
rho:-0.64, p=0.02rho:-0.66; p=0.02 rho:-0.56; p=0.05
Week 2 Week 6 Week 8(end of study)
0.1 1 100
1
2
3
FC in HIV-1 DNA (log10)
FC in
CD
69+
NK
cel
ls
0.1 1 100.0
0.5
1.0
1.5
2.0
2.5
FC in HIV-1 DNA (log10)
FC in
CD
69+
NK
cel
ls
0.25 1 4 160
1
2
3
FC in HIV-1 DNA (log10)
FC in
CD
69+
NK
cel
ls
rho:-0.64, p=0.02rho:-0.66; p=0.02 rho:-0.56; p=0.05
Week 2 Week 6 Week 8(end of study)
-
Changes in HIV-1 DNA during panobinostat treatment are
correlated with changes in NK cells
-
pre-IFN post-IFN100
101
102
103
104
105HI
V-1
DNA
copi
es/1
06 C
D4+
T c
ells
p=0.0003
Changes in HIV-1 DNA during treatment with IFN-a/RBV in HIV/HCV
co-infected patients
-
Conclusions
• HDACi can increase HIV-1 transcription in CD4 T cells from
ART-treated
patients
• Viral reactivation with RMD and PBT leads to transient
increases of plasma RNA
• All HDACi have an acceptable safety profile in ART-treated
patients
• No significant changes in HIV-1 DNA during HDACi treatment on
population
level
• Some patients during treatment with PBT and RMA have
substantial decline of
HIV-1 DNA
• Patients with reduction of HIV-1 DNA during PBT treatment
differ in • IL-28B “CC” GT
• ISG expression patterns
• Innate effector cell activity
• Kinetics of viral rebound during ATI
-
Department of Infectious Diseases, Aarhus University Hospital
•Thomas Rasmussen, MD •Ole Schmeltz Søgaard, MD, PhD •Martin
Tolstrup, MSc, PhD •Lars Østergaard, Professor/Head, MD, DMSc, PhD
•Christel Rothe Brinkmann, MSc, PhD •Rikke Olesen, MD, PhD •Anni
Winckelmann and Ann-Sofie Kjer •Lene Svinth Jøhnke and Erik Hagen
Nielsen
Department of Infectious Diseases, Alfred Hospital, Melbourne
•Sharon Lewin, Professor/Head, PhD •Ajantha Solomon, BSc
Massachusetts General Hospital, Ragon Institute, Boston •Maria
Buzon, MSc, PhD •Selena Vigano, PhD
Westmead Millennium Institute for Medical Research, Sydney
•Sarah Palmer, PhD
University of Colorado, School of Medicine •Charles A.
Dinarello, Professor of Medicine and Immunology
Acknowledgments
Clinical HIV-1 eradication �studies��Mathias Lichterfeld, M. D.,
Ph. D.�Massachusetts General Hospital�Harvard Medical School��
�Dianummer 2Dianummer 3Clinical HIV-1 eradication
strategiesPharmacological latency-reversing agents�“Shock”
componentImmune-mediated interventions�“kill” componentDianummer
7Clinical studies with HDACiClinical studies with Vorinostat
(Saha)Dianummer 10Dianummer 11Dianummer 12Dianummer 13Panobinostat
(LBH589)Overall study designSafety – adverse eventsCell-associated
unspliced HIV RNA (CA US HIV-RNA)HIV-1 plasma viremia during
treatment with panobinostatTotal cell-associated HIV-1 DNA during
�treatment with panobinostatTotal cell-associated HIV-1 DNA during
�treatment with panobinostatTotal HIV DNA during panobinostat
treatment – post-hoc analysisChange in HIV-1 DNA during treatment
with panobinostat correlates with kinetics �of viral rebound during
ATIExpansion of HIV-1-specific CTL �during Panobinostat
treatmentHIV-1-specific CTL �are not associated with HIV-1 DNA
changes during �panobinostat treatmentExpression patterns of
Interferon-stimulated genes�correlate with HIV-1 DNA decrease
during treatment with panobinostatHIV-1 DNA decrease during
panobinostat treatment occurs preferentially in carriers of IL28B
“CC” carriersDianummer 27Dianummer 28Dianummer
29ConclusionsDianummer 31