Embed Size (px)
Citation preview
Clinical Genetics
M. Kent Froberg, MD
2009
Purpose
• This lecture is designed to illustrate two examples of the use of molecular genetics in the clinical laboratory
• Learn the difference between oncogenic and physiological gene rearrangements and how they are demonstrated by PCR & Southern blot
• Learn how Factor V Leiden leads to thrombosis and how to detect the mutation
• Learn the major genetic and environmental causes of thrombosis
CLONALITY
• Clonality of B-cell neoplasms can be demonstrated by molecular techniques
• Can replace demonstration of specific pathological alteration
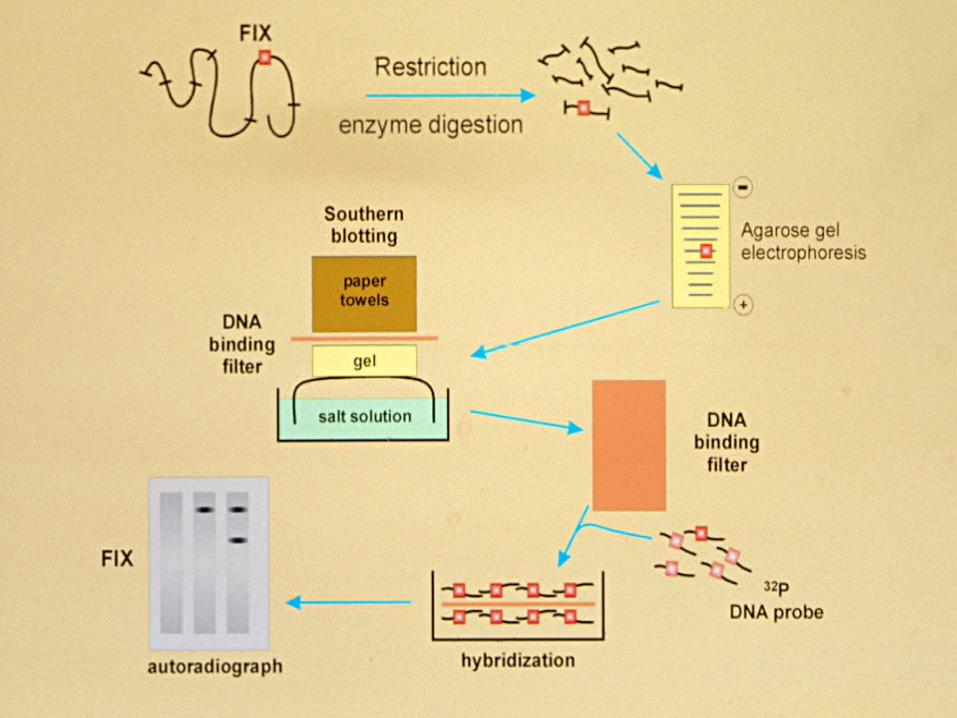
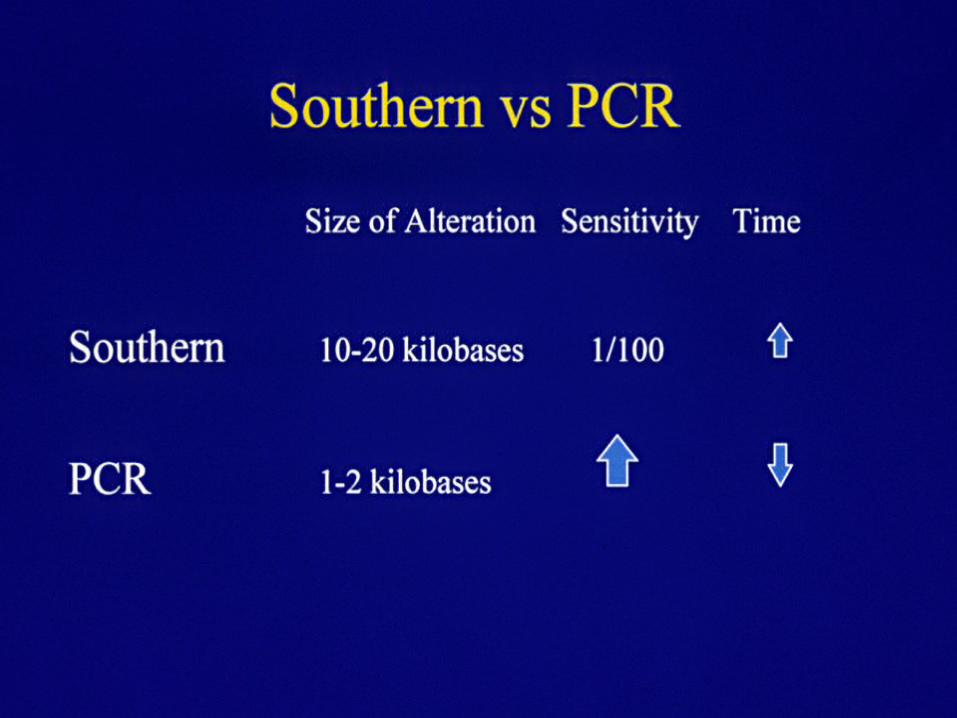
• PCR and Southern Blot
TYPES OF REARRANGEMENTS
• Pathological oncogenes
• Physiological antigen receptor genes
ONCOGENE REARRANGEMENTS
• Translocations
• Not present in all lymphoid neoplasms
• Often detected by cytogenetics or FISH
• Need prior knowledge of type of tumor and genes
rearranged
• Presently molecular probes not available for 2/3
of lymphomas
IG REARRANGEMENTS
• Physiological
• Since Ig rearrangement is normal for B lymphocytes, neoplasia of B-cell tumors show clonal Ig rearrangement
• Clonality = Malignancy (rare exceptions)
ANTIGEN RECEPTOR REARRANGEMENTS
• Immunoglobulin (Ig) and T-cell Receptor
• Ig rearrangements present in >90% of B-cell
neoplasms
• Detected by Southern Blot or PCR
• Used for Dx, establish lineage, identify minimal
residual disease, Rx
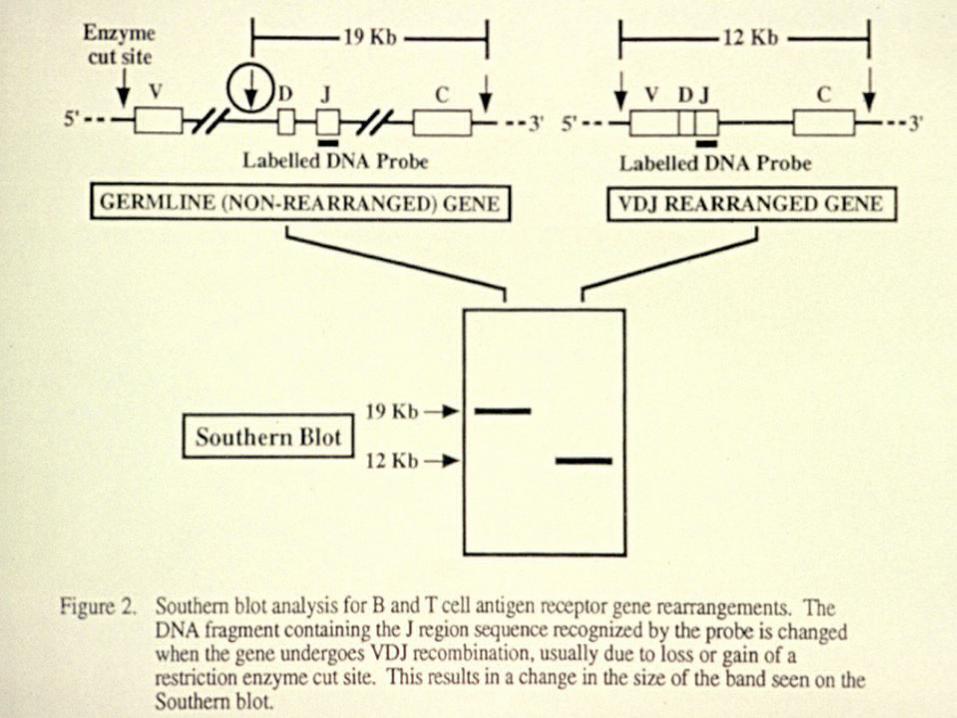
IG REARRANGEMENTS HIERARCHICAL
• Germline Ig specificity determined by somatic rearrangement of heavy & light chain genes
• Involve V (variable), D (diversity), and J (joining) gene segments
• D/J of heavy chain alleles, then V/DJ, followed by kappa light chain, then lambda
• Ig heavy chain selected first, so most commonly rearranged
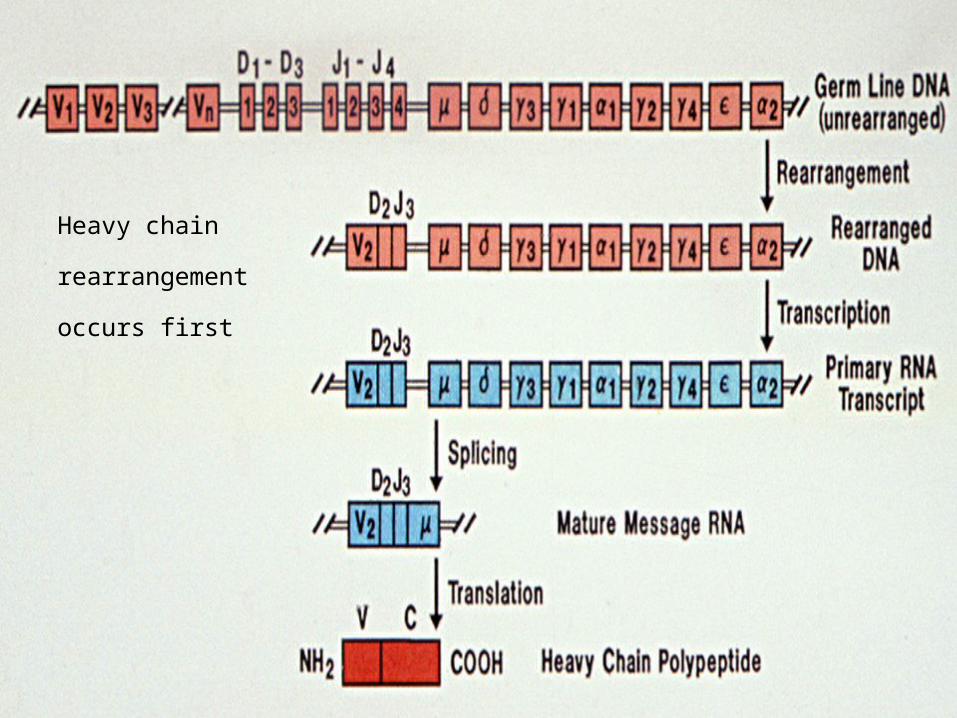
Heavy chain
rearrangement occurs
first
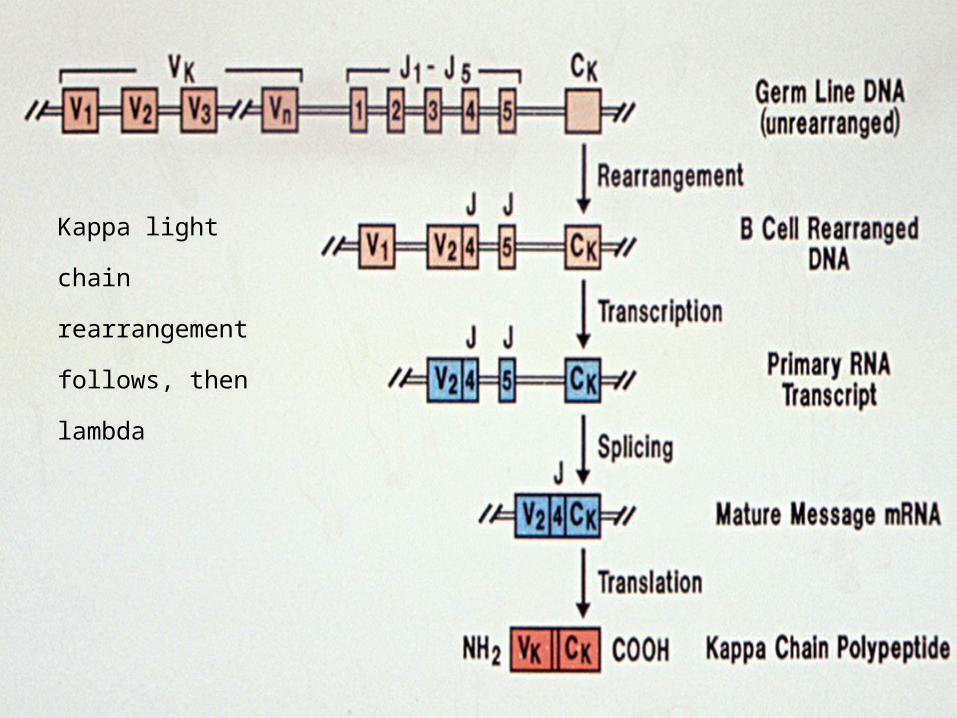
Kappa light chain
rearrangement
follows, then lambda
Clonality
• Tissue from Pt (biopsy of enlarged lymph node)
• Extract DNA
• Southern blot using probe for conserved region of IgM heavy chain
• If polyclonal smear (no discrete bands) besides germline
• If monoclonal see discrete bands (one germline & one clone)
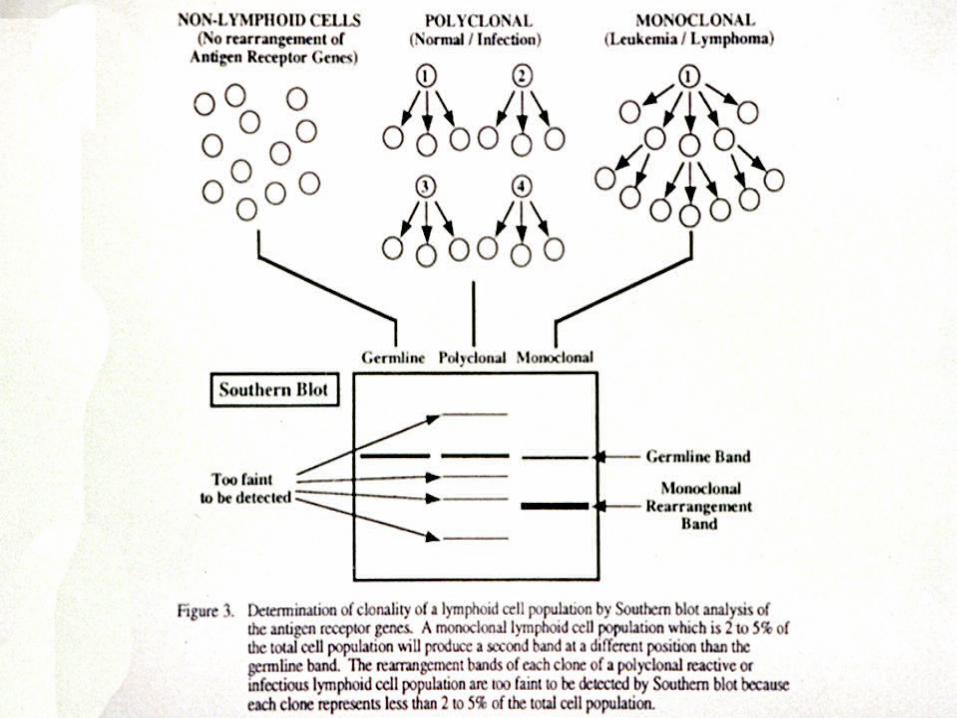
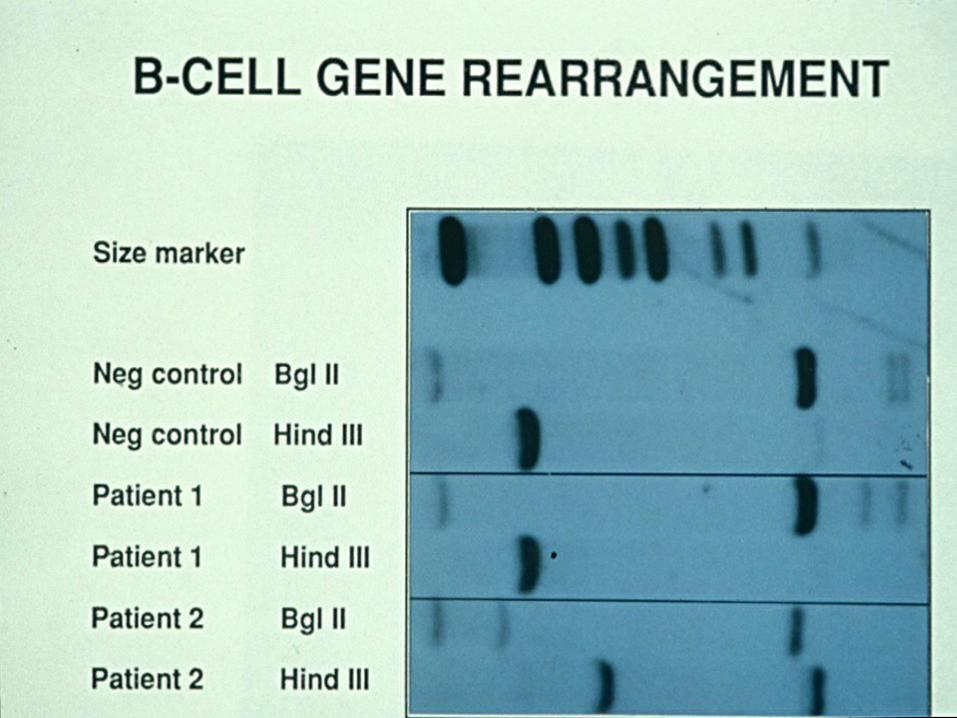
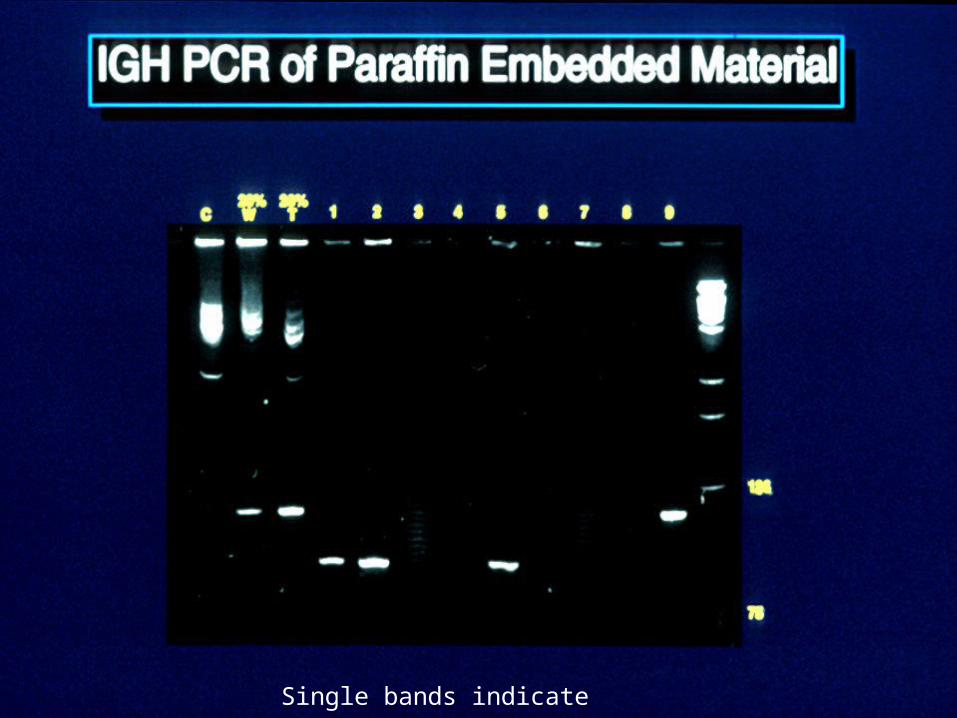
Single bands indicate clonality
CONCLUSIONS
• Demonstration of Ig Clonal Rearrangement of B-cell lesions by PCR is becoming the standard for many molecular labs in Dx and lineage establishment for B-cell neoplasms
• This method is faster, more economical and more sensitive than other molecular techniques or cytogenetics
HEREDITARY THROMBOPHILIA
• Most Hypercoagulable States are Acquired
– Deficiency of anticoagulant system or defective fibrinolysis
– Post-operative, immobility, pregnancy, trauma, oral contraceptives, SLE, neoplasia
– Need to eliminate acquired causes first
HEREDITARY THROMBOPHILIA
• Anticoagulant Deficiences
– heterozygotes have 35-65% reduction in protein
– have 3-7x risk for venous thrombosis
– deficiencies may be quantitative or qualitative
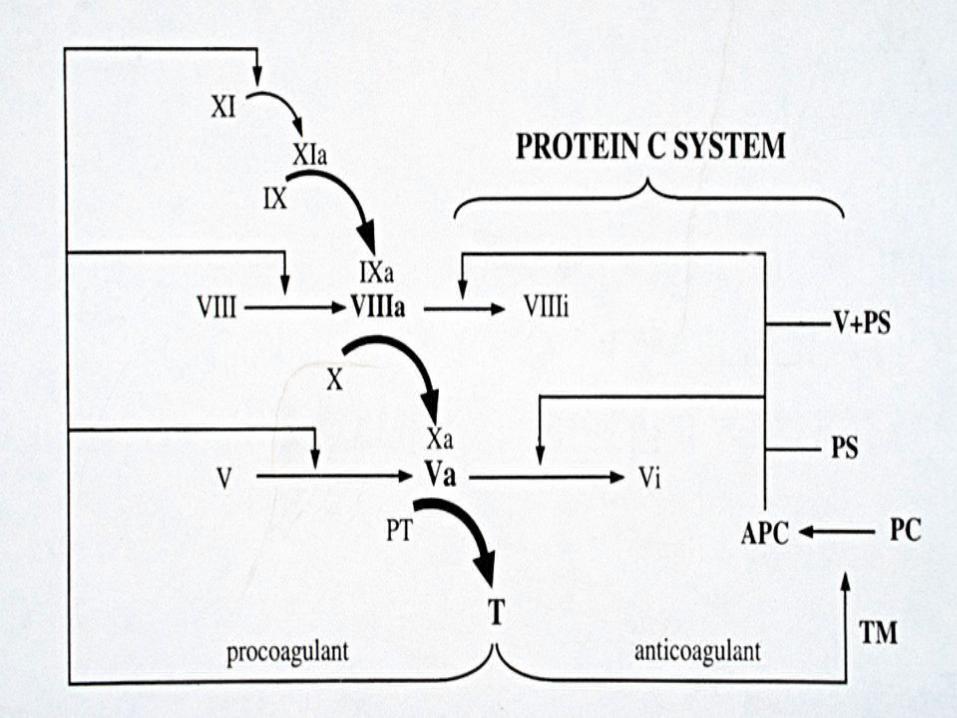
HEREDITARY THROMBOPHILIA ANTICOAGULANT DEFICIENCIES
• Protein C, Protein S and Anti-thrombin III account
for ~8% of hereditary thrombophilia
• 1st thrombotic event prior to 50
• Anti-thrombin def highest risk
• Need functional & antigenic assays
HEREDITARY THROMBOPHILIA PROTHROMBIN MUTATION
• Described 1996
• G A mutation at nucleotide 20210
• Heterozygotes found in 2.3% of NL population
• 6.2% of pts with venous thrombosis
• Hence, 2.8-fold risk
• Mechanism unknown
• Does serum thrombin levels
HEREDITARY THROMBOPHILIA HYPERHOMOCYSTEINEMIA
• Described 1994
• Acquired (def B12, B6, or folate)
• Hereditary: mutation in one of many enzymes
• Hereditary form accounts for ~20% of venous
thrombosis that is genetic
HEREDITARY THROMBOPHILIA HYPERHOMOCYSTEINEMIA
• Also have risk of atherosclerosis
• Mechanism:
– endothelial dysfunction
– interference with:
• antithrombin
• NO
• thrombomodulin
HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
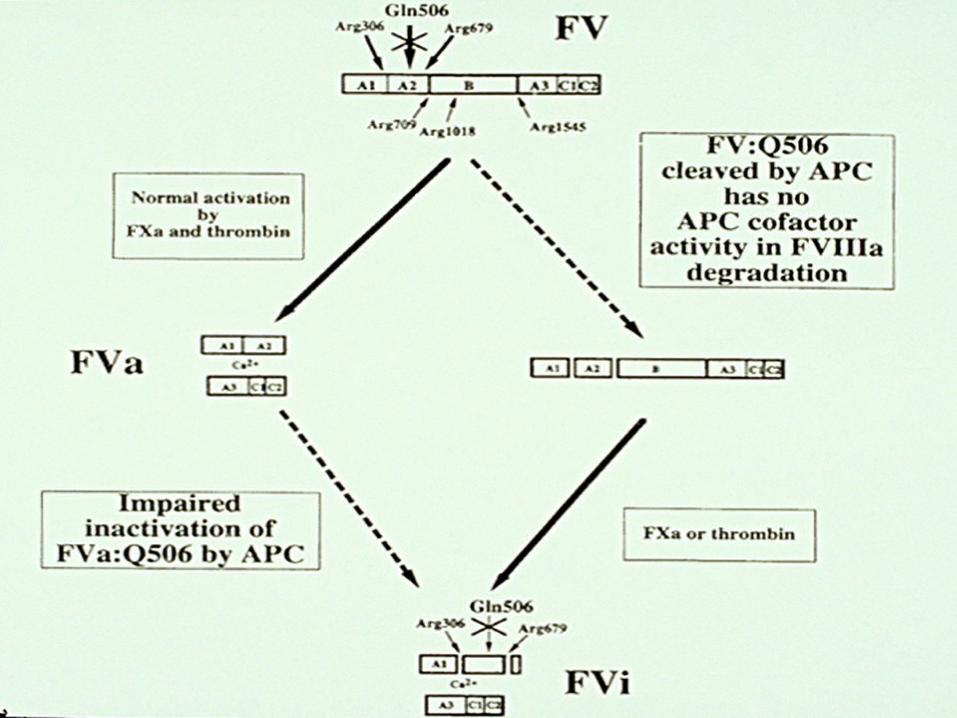
• Described 1993 as activated protein C resistance (APCR)
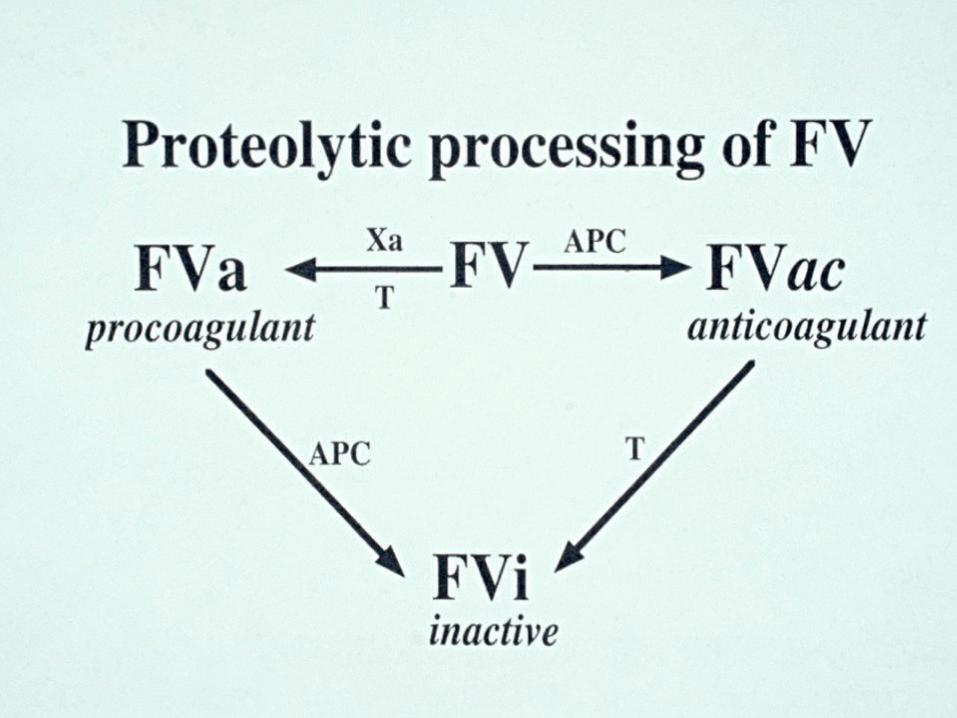
• Activated protein C cleaves factors V and VIII at specific arginine sites to inhibit coagulation
• Factor V Leiden is a point mutation at 506 in 95% of cases
HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
• FV:Q506 = arginine glutamine mutation
• Hence factor V resistant to proteolysis by activated
protein C
• Favors procoagulant state
• Carrier rate 5-7% of caucasians
• Accounts for >50% of hereditary venous thrombosis
(~20% of unselected pts)
HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
• Suspect when obvious etiologies of acquired thrombosis have been ruled out
• Pts with thrombosis < 50
• Recurrent thrombosis
• < 50 and > one family member with thrombosis
HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
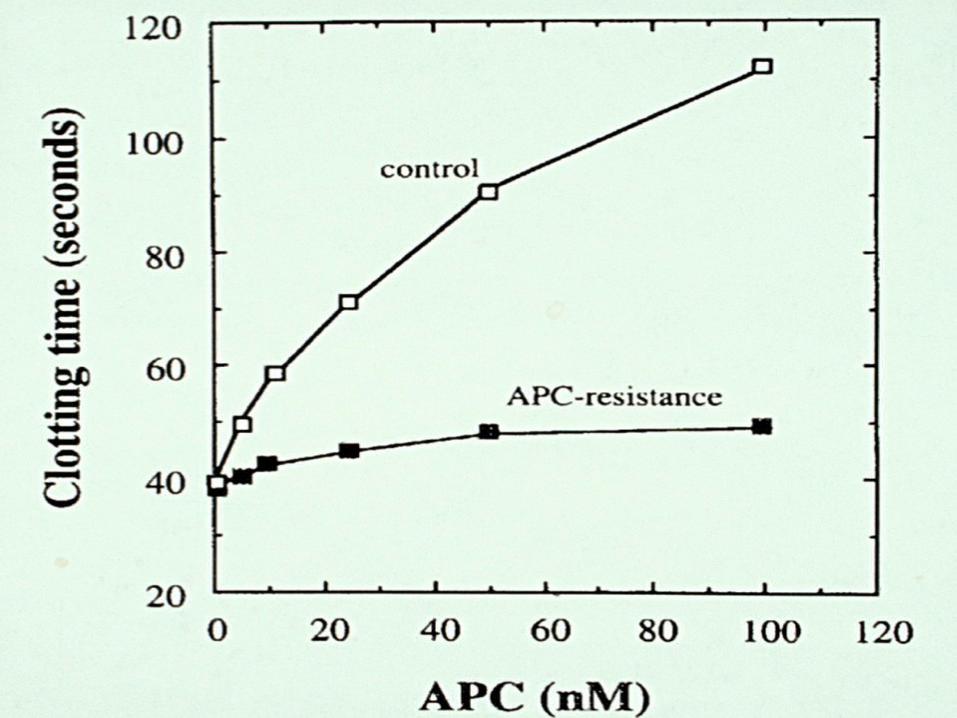
• Diagnosis: Assay for APCR (activated protein C
resistance)
• APCR: PTT performed + and - exogenous activated
protein C
• Plus APC = prolonged PTT
• Normal: ratio +APC/-APC=2.0
• APCR: ratio +APC/-APC<2.0
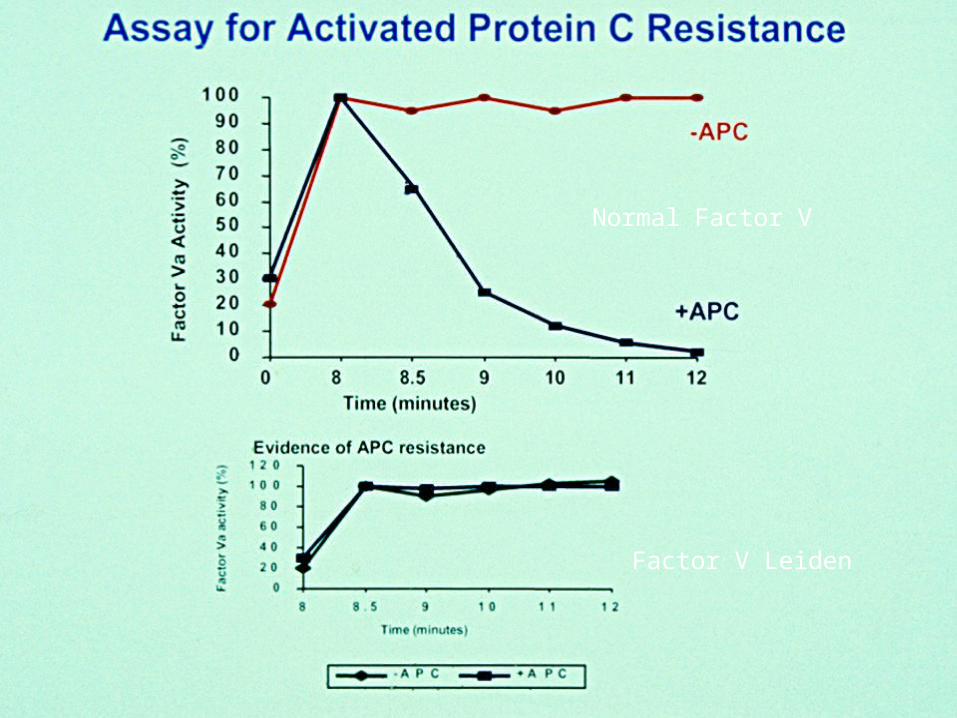
Normal Factor V
Factor V Leiden
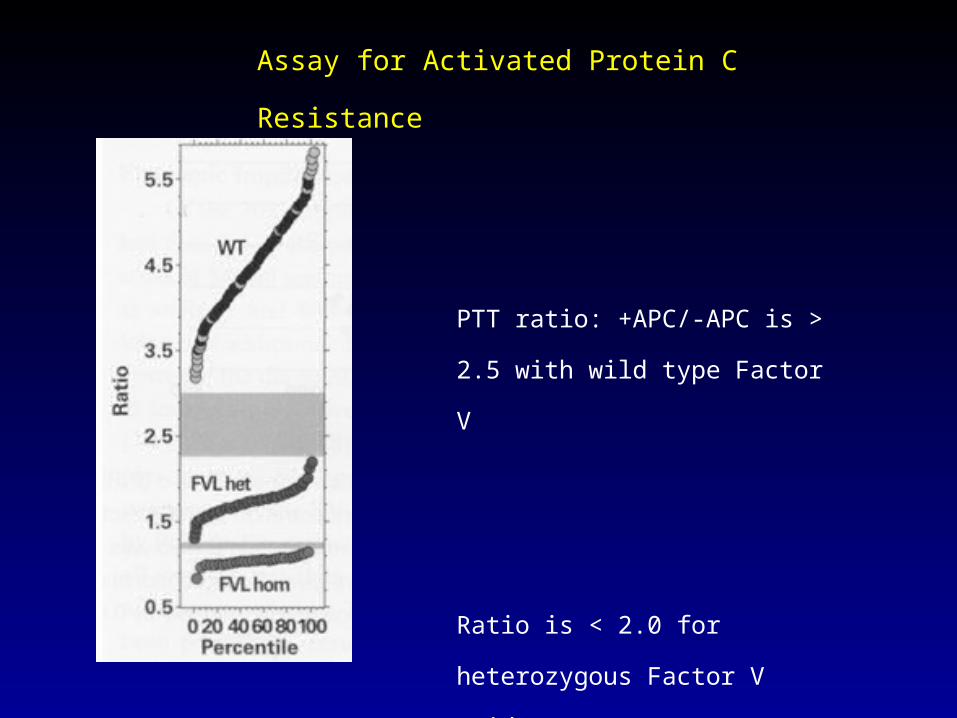
PTT ratio: +APC/-APC is > 2.5 with
wild type Factor V
Ratio is < 2.0 for heterozygous Factor
V Leiden
Ratio is lowest for homozygous
Factor V Leiden
Assay for Activated Protein C Resistance
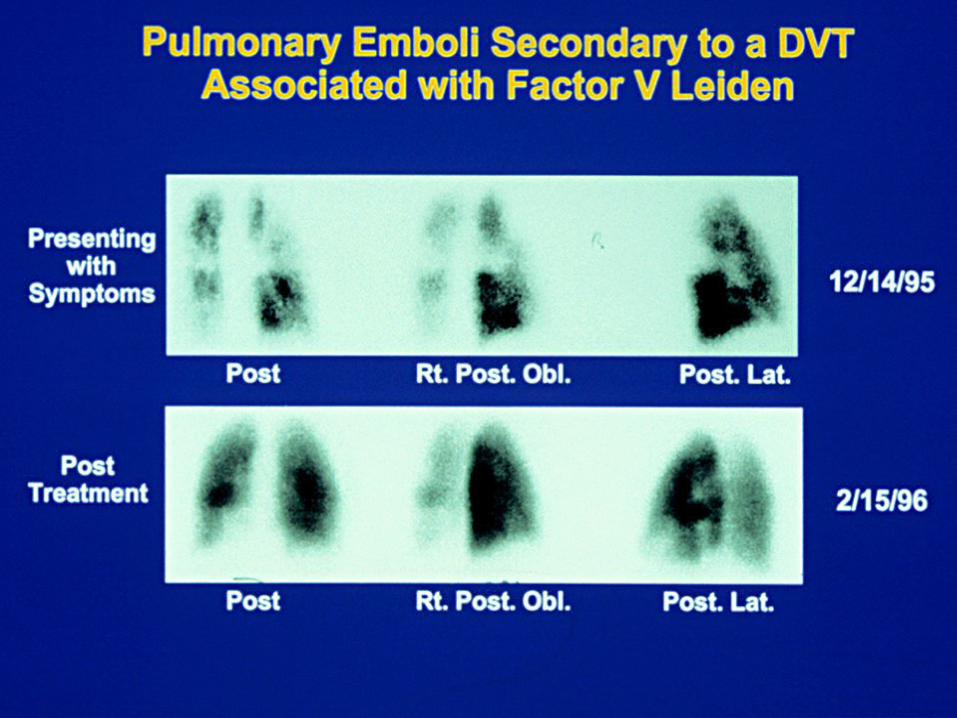
Case
• 51 year old physician with acute SOB on climbing stairs syncopal episode
• Taken to ED
• Perfusion Scan multiple pulmonary emboli
Followup
• Pt had APCR
• PCR for Factor V Leiden heterozygous
• 49 year old sister with Hx stroke 1 yr previously Factor V Leiden heterozygote
• Son of pt also Factor V Leiden +
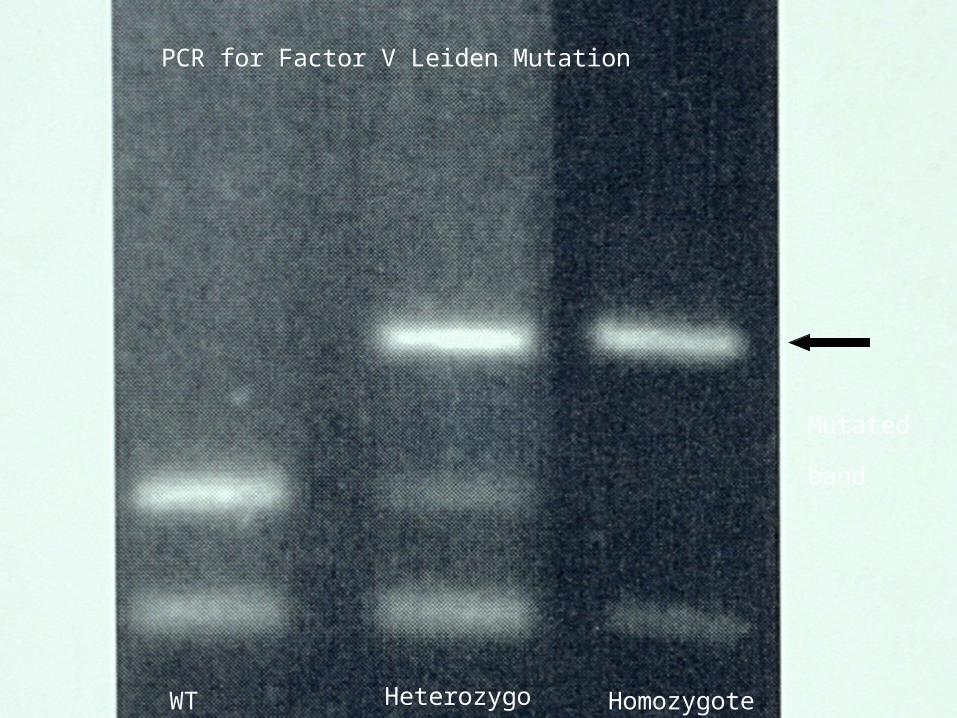
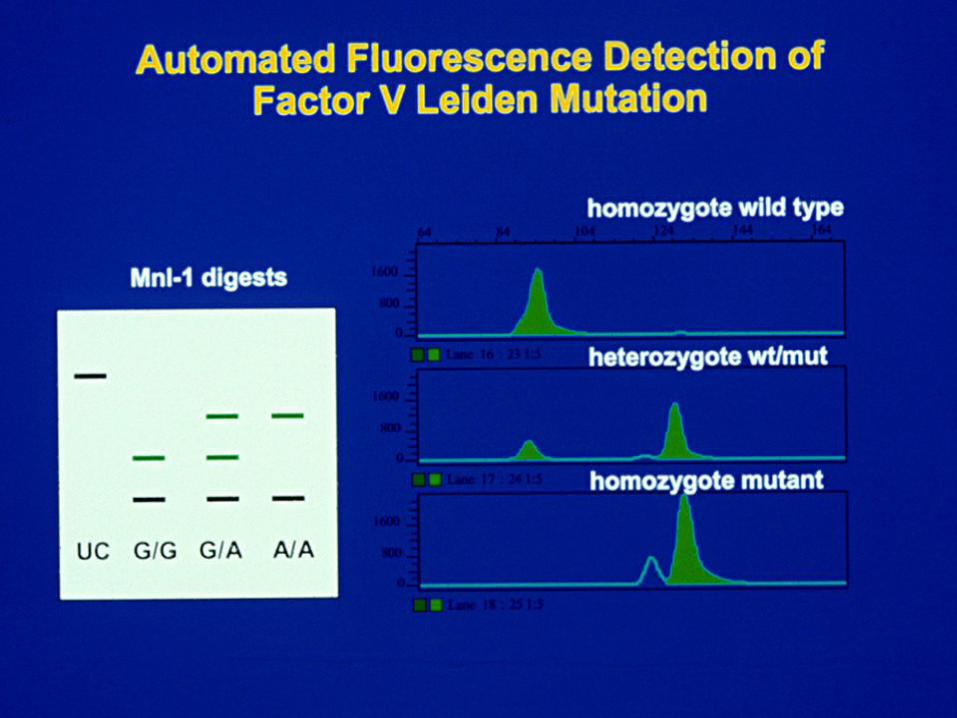
WT Heterozygote Homozygote
PCR for Factor V Leiden Mutation
Mutated band
HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
• Confirmation: DNA analysis by PCR
• Factor V mutation eliminates a Mnl I restriction site
• Blood sample, isolate DNA, amplify mutation site
by PCR, subject to Mnl I cleavage (cleaves at
arginine site)
• Factor V Leiden is resistant to digestion at 506
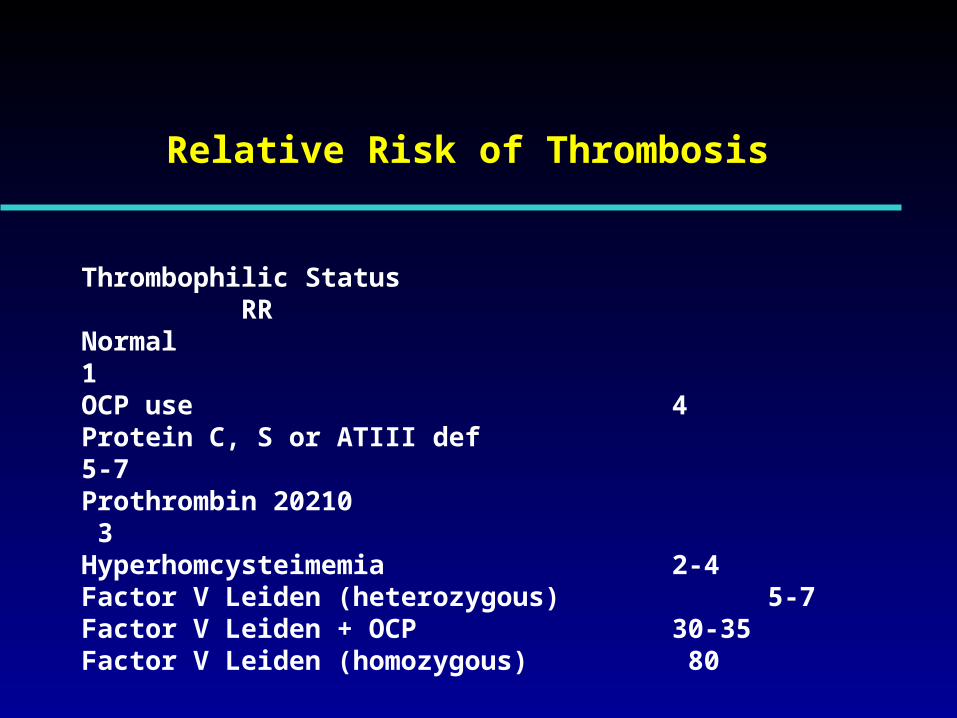
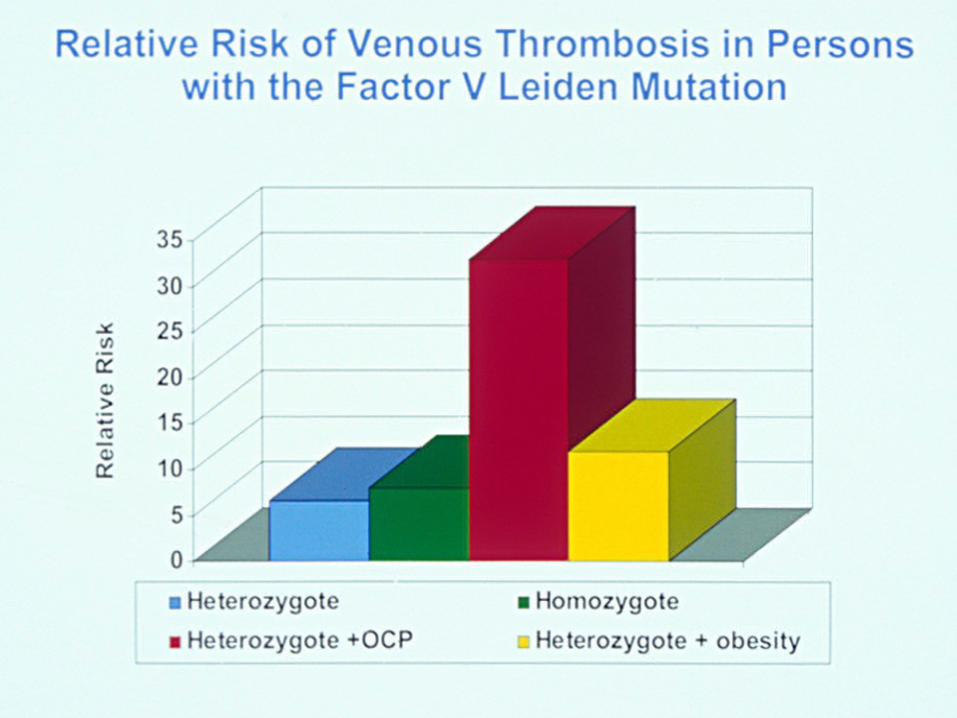
Relative Risk of Thrombosis
Thrombophilic Status RRNormal 1OCP use 4Protein C, S or ATIII def 5-7Prothrombin 20210 3Hyperhomcysteimemia 2-4Factor V Leiden (heterozygous) 5-7Factor V Leiden + OCP 30-35Factor V Leiden (homozygous) 80

Rx of Hereditary Thrombophilia
• Anticoagulant therapy (heparin, warfarin) • 3% risk of major hemorrhage/yr from Rx• 1/5 fatal• Avoid other risk factors (smoking, OCP)• Genetic counseling