Embed Size (px)
Citation preview

CORRESPONDING AUTHOR:Wenjuan Zhou, Division of Oraland Maxillofacial Surgery, UConnSchool of Dental Medicine, 263Farmington Avenue, Farmington,CT 06030, USA.E-mail: [email protected]
KEYWORDSDental implants, Computer-assisted,Guided surgery, Surgical guides,Accuracy
Conflict of Interest: The authors haveno actual or potential conflicts ofinterest.
Received 26 June 2017; accepted17 July 2017
J Evid Base Dent Pract 2018: [28-40]
1532-3382/$36.00
ª 2017 Elsevier Inc. Allrights reserved.doi: http://dx.doi.org/10.1016/j.jebdp.2017.07.007
Volume 18, Number 128
The Journal of EVIDENCE-BASED DENTAL PRACTICE
ORIGINAL ARTICLE
CLINICAL FACTORS AFFECTING THEACCURACY OF GUIDED IMPLANT SURGERY—A SYSTEMATIC REVIEW AND META-ANALYSIS
WENJUAN ZHOU, DDS, PhDa,b,c, ZHONGHAO LIU, DDS, PhDa,LIANSHENG SONG, DDS, MSb, CHIA-LING KUO, PhDd, AND DAVID M. SHAFER, DMDb
aDepartment of Implant Dentistry, Yantai Stomatological Hospital, Binzhou Medical University, Yantai, ChinabDivision of Oral and Maxillofacial Surgery, UConn School of Dental Medicine, Farmington, CT, USAcDivision of Conservative Dentistry and Periodontology, Competent Center of Periodontal Research, University Clinic of Dentistry, Medical University of Vienna,Vienna, AustriadCT Institute for Clinical and Translational Science, UConn Health, Farmington, CT, USA
ABSTRACT
ObjectivesTo systematically review the current dental literature regarding clinical accuracy ofguided implant surgery and to analyze the involved clinical factors.
Material and MethodsPubMed and Cochrane Central Register of Controlled Trials were searched. Meta-analysis and meta-regression analysis were performed. Clinical studies with thefollowing outcome measurements were included: (1) angle deviation, (2) devia-tion at the entry point, and (3) deviation at the apex. The involved clinical factorswere further evaluated.
ResultsFourteen clinical studies from 1951 articles initially identified met the inclusioncriteria. Meta-regression analysis revealed a mean deviation at the entry point of1.25 mm (95% confidence interval [CI]: 1.22-1.29), 1.57 mm (95% CI: 1.53-1.62) atthe apex, and 4.1� in angle (95% CI: 3.97-4.23). A statistically significant differ-ence (P , .001) was observed in angular deviations between the maxilla andmandible. Partially guided surgery showed a statistically significant greater de-viation in angle (P , .001), at the entry point (P , .001), and at the apex (P , .001)compared with totally guided surgery. The outcome of guided surgery withflapless approach indicated significantly more accuracy in angle (P , .001), at theentry point (P , .001), and at apex (P , .001). Significant differences wereobserved in angular deviation based on the use of fixation screw (P , .001).
ConclusionsThe position of guide, guide fixation, type of guide, and flap approach couldinfluence the accuracy of computer-aided implant surgery. A totally guided sys-tem using fixation screws with a flapless protocol demonstrated the greatestaccuracy. Future clinical research should use a standardized measurement tech-nique for improved accuracy.
INTRODUCTION
Digital technology has been playing a more and more important role indentistry for number of years, one of the most common used digitalized

The Journal of EVIDENCE-BASED DENTAL PRACTICE
dental technique is digital radiography, which providesdental professionals potentially a better way of diagnosisand treatment for dental desease.1-3 In the past severalyears, with the introduction of computed tomography (CT)and 3-dimensional (3D) printing into the field of implantdentistry, computer-aided design and computer-aidedmanufacturing (CAD/CAM) technology brought a greatevolution of novel treatment concepts to dental implanttreatment.4 CT and 3D implant planning software can notonly provide clinicians with 3D information of patient’sanatomic structures, but also data regarding the patient’sfinal prosthesis, these digital data can be combined withthe CAD/CAM technology and further lead to a digitalworkflow ending with the production of stereolithographic(STL) template via a prototyping system.5,6 The STLtemplate can then be used to guide the position anddirection of certain implants during surgery. By which, thewhole surgical procedure is so called “guided dentalimplant surgery.”
According to the consensus statement published in 2009,7
the term “computer-guided surgery” is defined as the useof a static surgical guide that reproduces the virtualimplant position directly from CT data and does not allowfor intraoperative modification of the implant position. Ithas been demonstrated to be an established treatment,6
which reduces the probability of damage to the adjacentcritical structures such as bones, nerves, adjacent toothroots, and sinus cavities. The main advantage of guidedsurgery is the ability to plan and optimize the implantposition in a restoration-driven placement manner. More-over, computer-guided technique can help to decreasepostoperative discomfort and allows for immediate func-tion, as they enable implant placement with minimal surgicaltrauma. In addition, this technique offers an alternative tobone augmentation in situation of severely resorbed alve-olar ridges, as they facilitate optimal position of implants inavailable bones.8-10 However, with the generalization of thistechnique, many doubts have risen on its usefulness andespecially the accuracy.11-15
Accuracy in guided implant surgery is defined as matchingthe planned position of the implant in the software with theactual position of the implant in the patient’s mouth.13 Itreflects the accumulation of all deviations from imagingover the transformation of data into a guide, to theimproper positioning of the latter during surgery,14 andthe different types of errors include error during imageacquisition and data processing, error during surgicaltemplate production, error during template positioningand movement of the template during drilling, andmechanical error caused by tolerance of surgicalinstruments. All errors, although seldom occurring, can becumulative.
In recent years, several studies have been performed ondifferent factors affecting the accuracy of guided sur-gery,16,17 and systematic reviews6,18-20 have evaluated thesestudies very well, focusing on the accuracy, clinical advan-tages, survival rates, complications of computer-guidedsurgery, and the influence of using different types ofguide. However, only limited and incomplete data wereprovided in clinical trials regarding the accuracy and influ-ence of relevant clinical factors except for tissue of sup-port.18 There are still no concerted standard parameters forthe evaluation of deviation, which leads to diversity inresults and, therefore, can hardly provide an effectiveindication for the clinical application of guided surgery.
In the present study, we tried to review the current dentalliterature, focusing on the clinical accuracy of guided dentalimplant surgery, to analyze the involved clinical factorsaffecting the accuracy, and tried to find the most appro-priate method for the evaluation of accuracy.
MATERIALS AND METHODS
Protocol and RegistrationThis review was registered at the International ProspectiveRegister of Systematic Reviews (https://www.crd.york.ac.uk/PROSPERO, registration number 42016050127). It wasconducted in accordance with the guidelines of “PreferredReporting Items for Systematic Review and Meta-analysisProtocols 2015 Statement.”21
Search Strategy for Identification of StudiesTwo Internet sources of MEDLINE-PubMed and CochraneCentral Register of Controlled Trials (CENTRAL) were usedto search for eligible articles (published and online preview)in English, and this was complemented by a manual searchof the references of all selected full-text articles. Publica-tions from January 1, 1990, to October 31, 2016,were searched using the following search strategy:PubMed: ((((((((((((“Dental Implantation”[Mesh]) OR“Dental Implants”[Mesh]) AND “Surgery, Computer-Assis-ted”[Mesh]) OR “Computer-Aided Design”[Mesh]) ORdental implant navigation) OR digital dentistry) OR guideddental implant surgery) OR image-guided dental implantsurgery) OR computer-guided dental implant surgery) ORdental stereo lithography) AND “Dimensional MeasurementAccuracy”[Mesh]) OR dental implant deviation) OR dentalimplant precision) OR dental implant accuracy); CochraneCentral Register of Controlled Trials: dental implantation ORdental implant and dental navigation OR computer aideddental implant OR three-dimensional (3D) dental planningOR 3D dental planning OR computer-assisted dentalimplant OR dental stereo lithography OR guided dentalimplant placement OR dental surgical template OR dentalguided surgery OR dental surgical guide AND dimensional
March 2018 29

Figure 1. Flow diagram of articles retrieved fromdatabases.
u
The Journal of EVIDENCE-BASED DENTAL PRACTICE
30
measurement accuracy OR dental implant deviation ORdental implant precision OR dental implant accuracy.
Studies Selection and Data ExtractionFor inclusion in this study, the articles were selected ac-cording to the following criteria: (1) articles published inEnglish; (2) clinical cohort studies; (3) the article title isrelated to the question, that is, studies reporting on theaccuracy of static guided implant surgery performed in thepartially or complete edentulous jaw; (4) studies in whichquantitative results are provided (only studies providingexact information on the amount and direction of implant orosteotomy deviations were included); and (5) studies with aminimum sample size of 10. To evaluate the deviation, atleast the following parameters should have been observed:deviation at the entry point, deviation at the apex, anddeviation of the axis.
Articles were additionally rejected after full-text analysis inthe following situations: (1) expert opinions or literature re-views; (2) reports of techniques; (3) case series; (4) implantsinstalled in areas of bone augmentation; (5) studies withzygomatic implants, pterygoid implants, or mini-implants fororthodontic purposes; and (6) studies using CT for implantplanning without applying CAD/CAM surgical guide duringsurgery (mental navigation).
Two reviewers retrieved the data independently and dis-cussed with a third reviewer for the final selection ofincluded studies. Except for the deviation of guided sur-gery; age, radiology method (CT or cone beam CT (CBCT)),position of guide (maxilla or mandible), fixation of guide(with or without fixation screw), type of guide (totally/fullyguided or partially guided), and flap method (open flap orflapless) were further considered to be factors that wouldinfluence the accuracy of the outcome.
For the assessment of bias risk in included studies, theadapted Newcastle-Ottawa Scale was used according to 2previous systematic reviews.18,22 In brief, a maximum of 13stars could be assigned for each included study; studies with10-12 points indicated high methodological quality, 7-9points indicated medium-level methodological quality, andothers were considered as studies with low methodologicalquality.
Statistical AnalysisThe results of different studies were combined by meta-analysis assuming a random-effects model. Subgroupcomparisons, for example, age groups and radiationmethods, were performed in the framework of mixed-effectsmeta-regression. An omnibus test was used to test if there ismean difference between groups. If the result was signifi-cant, all possible pairwise comparisons were conducted withmultiple testing adjustment by Tukey’s method. A P value
Volume 18, Number 1
less than 5% was deemed statistically significant. All themeta-regression analyses were performed using R 3.3.1. Forthe comparison of other involved clinical factors, meta-analysis was conducted using Review Manager, version 5.0(The Nordic Cochrane Center, Denmark). Heterogeneitybetween studies was assessed with the I2 statistics ($50%)and Cochran’s Q test (P, .001/95% confidence interval [CI]).P values and 95% CIs were calculated for each variable ofinterest. The level of significance was set at P # .05.
RESULTSThe initial search yielded 1743 titles from PubMed and 208from the Cochrane Central Register of Controlled Trials.After reviewing the abstract, 1906 were excluded and 45were considered for further full-text screening. Finally, 14articles (6 retrospective studies and 8 prospective studies)were included in this systematic review (Figure 1). Thecharacteristics of the included articles are presented inTable 1; the review did not include studies with smokersand patients with periodontal disease or other systemicdiseases to avoid selection bias. The risk of biasassessment showed that most observational studiesincluded in this systematic review received 8-10 stars,which indicates a medium-level methodological quality,

Table 1. Characteristics of studies included for qualitative analysis.
Study Design RxPatients/no.of implants
Meanage(y)
Edentulism(no. of
implants)Jaw (no.
of implants)Guidesystem
Type ofguide(no. of
implants)
Type offlap
(no. ofimplants)
Fix screw(no. of
implants)
Angledeviation(degree)
Globaldeviationcoronal(mm)
Globaldeviationapical(mm)
Lateraldeviationcoronal(mm)
Lateraldeviationapical(mm)
Depthdeviationcoronal(mm)
Depthdeviationapical(mm)
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
Ozanet al., 2009
Retrospective CT 30/110 47 Fully; partially Max. (58);Mand. (52)
StentCAD
Total Flapless (60);flap(50)
N (110) 4.10 2.30 1.11 0.70 1.41 0.90 – – – – – – – –
Cassettaet al., 2011
Retrospective CT 10/111 54 Fully (94);partially (17)
Max. (68);Mand. (43)
SimPlant Total Flapless (93);flap(18)
Y (67); N (44) 4.68 2.98 1.52 0.61 1.97 0.86 1.20 0.63 – –
Cassettaet al., 2013
Retrospective CT 12/129 55 Fully (112);partially (17)
Max. (78);Mand. (51)
SimPlant Total Flapless (111);flap (18)
Y (75);N (54)
4.78 2.89 1.57 0.63 2.06 0.88 1.23 0.60 – –
Vieiraet al., 2013
Retrospective CBCT 14/62 – Fully (62) Max.; Mand. DentalSlice
Total Flapless (62) Y (62) 1.89 0.46 1.79 0.81 2.21 1.50 – – – – – – – –
Farley etal., 2013
Prospective CBCT 10/Oct 42 Single (10) Max. (3);Mand. (7)
iDent Total Flapless (10) – 3.68 2.19 1.45 0.60 1.82 0.60 0.63 0.37 1.11 0.71 21.20 0.70 21.24 0.68
Cassettaet al., 2013a
Retrospective CT 20/227 55 Fully (182);partially (45)
Max. (135);Mand. (92)
SimPlant Total (111);partial(116)
Flapless (187);flap (40)
Y (111);N (116)
4.82 3.14 1.50 0.63 1.92 0.91 1.35 0.68 – – – –
Arisanet al., 2013
Prospective CT/CBCT 11/102 – Fully (102) Max. (64);Mand. (44)
SimPlant Total Flapless (102) Y (102) 3.38 1.11 0.78 0.32 0.83 0.33 – – – – – – – –
Leeet al., 2013
Retrospective CT 48/102 52.9 Fully (17);partially (85)
Max. (62);Mand. (40)
OnDemand 3D Total (102) Flap (102) Y (102) 3.80 3.24 1.09 1.10 1.56 1.48 0.72 0.75 1.23 1.25 0.66 0.95 0.69 1.03
Ersoyet al., 2008
Prospective CT 21/94 43 Fully (65); partially(20); single (9)
Max. (48);Mand. (46)
Stent CAD Total (94) Flapless (41);flap (53)
– 4.90 2.36 1.22 0.85 1.51 1.00 – – – – – – – –
Arisanet al., 2010
Prospective CBCT 54/279 48.4 Fully;partially
– Stent CADSimPlant
Total (29);partial (30)
Flapless; flap – 3.96 1.05 1.22 0.39 1.44 0.43 – – – – – – – –
Di Giacomoet al., 2011
Prospective CBCT 12/60 60.3 Fully (60) Max. (22);Mand. (38)
NTT Partial (60) Flapless (60) Y (60) 6.53 4.31 1.35 0.65 1.79 1.01 – – – – – – – –
Stubingeret al., 2014
Prospective CT 10/44 62.5 Fully (44) – Astra Tech AB Total (44) Flap (44) Y (44) 2.39 0.97 0.71 0.399 0.77 0.382 0.43 0.297 0.52 0.273 – –
Vasaket al., 2011
Prospective CT 16/79 58 Fully;partially
Max.; Mand. Nobel Biocare Total (79) Y (79) 3.53 1.77 0.46 0.35 0.70 0.49 – – – – 0.53 0.38 0.52 0.42
Verhammeet al., 2015
Prospective CBCT 30/104 – Fully (104) Max. (104) Nobel Biocare Total (104) Flapless (104) Y (64);N (40)
2.819 – 1.368 – 1.587 – 0.60 – 0.751 – – – 0.843 –
CAD, computer-aided design; CT, computer tomography; CBCT, cone beam computer tomography; Max., maxilla; Mand., mandible; SD, standard deviation.
TheJo
urnalofEVID
ENCE-BASED
DEN
TALPRA
CTIC
E
March
2018
31

The Journal of EVIDENCE-BASED DENTAL PRACTICE
32
and 4 studies had high-level methodological quality(Figure 2).
Meta-regression analysis revealed an overall (14 studies, n 5
1513 implants) mean deviation at the entry point of 1.25 mm(95% CI: 1.22-1.29), 1.57 mm (95% CI: 1.53-1.62) at the apex,and the mean angular deviation is 4.1� (95% CI: 3.97-4.23).Seven studies (n 5 727 implants) reported a mean lateralerror at the entry point of 1.05 mm (95% CI: 1.00-1.09),whereas the mean apical lateral deviation (4 studies, n 5 260implants) was 0.91 mm (95% CI: 0.81-1.02). The mean depthdeviation was 0.64 mm (95% CI: 0.53-0.74) at the entry point(3 studies, n 5 191 implants) and 1.24 mm (95% CI: 1.16-1.32) at the apex (4 studies, n 5 295).
Effect of Age on the Accuracy of Guided SurgeryData on patients’ age were retrieved from 11 studies. Threeage groups were created: 40-50 years (4 studies, n 5 493implants); 50-60 years (5 studies, n 5 648 implants); and 60years or older (2 studies, n 5 104 implants).
The mean angular deviation was 4.15� (95% CI: 3.62-4.67)for the 40- to 50-year group, 4.32� (95% CI: 3.78-4.87) forthe 50- to 60-year group, and 4.43� (95% CI: 0.37-8.48) forthe 60 years or older group. The mean deviation at the entrypoint for the 3 age groups was 1.21 mm (95% CI: 1.15-1.26),1.23 mm (95% CI: 0.81-1.64), and 1.03 mm (95% CI: 0.40-1.65), respectively, and their corresponding mean apical
Figure 2. Risk of bias of included studies. Stars were assigneindicated a medium-level methodological quality, and 4 studiquality.
Volume 18, Number 1
errors were 1.47 mm (95% CI: 1.40-1.53), 1.64 mm (95% CI:1.14-2.14), and 1.27 mm (95% CI: 0.27-2.27).
P values from the omnibus test associated with age forangular deviation, deviation at the entry point, and devia-tion at the apex were 0.975, 0.789, and 0.658, respectively.None of the P values are statistically significant, which im-plies that there is no significant difference between agegroups for the 3 deviations.
Effect of Radiology Methods on the Accuracy ofGuided SurgeryFor the influence of radiology techniques, 9 studies (n5 946implants) used CT for the guided surgery, whereas 6 studies(n 5 567 implants) used CBCT. The mean angular deviationwas 4.02� (95% CI: 3.45-4.59) for the CT group and 3.86�
(95% CI: 2.41-5.30) for the CBCT group. For deviation at theentry point, the CT group revealed a mean error of 1.10 mm(95% CI: 0.84-1.36), whereas the CBCT group presented amean error of 1.31 mm (95% CI: 0.99-1.63). The mean de-viation at the apex was 1.59 mm (95% CI: 1.52-1.66) and1.54 mm (95% CI: 1.48-1.60), respectively, for CT and CBCTgroups.
The study of Arisan et al.23 had both CT and CBCT data. Weconducted sensitivity analysis by including both data andexcluding the CT data. The omnibus test P values forangular deviation, deviation at the entry point, and apical
d to respective study, 10 studies received 8-10 stars thates with more than 10 stars had high-level methodological
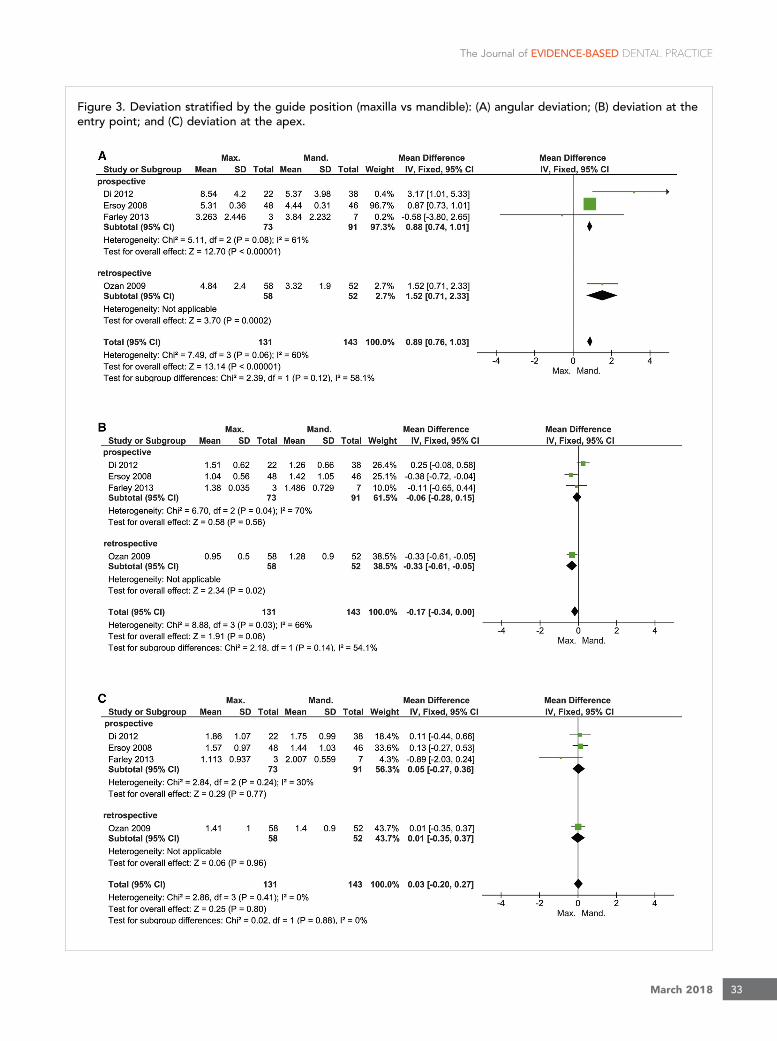
Figure 3. Deviation stratified by the guide position (maxilla vs mandible): (A) angular deviation; (B) deviation at theentry point; and (C) deviation at the apex.
The Journal of EVIDENCE-BASED DENTAL PRACTICE
March 2018 33

The Journal of EVIDENCE-BASED DENTAL PRACTICE
34
deviation were 0.738, 0.336, and 0.508 when including bothdata and were 0.654, 0.460, and 0.689 when excluding theCT data. Both gave consistent results and suggested thatthere is no significant difference in the accuracy betweenCT and CBCT.
Effect of the Guide PositionFour studies (3 prospective studies and 1 retrospective study;n5 274 implants) were reviewed for comparing the accuracyof guided surgery performed on the maxillary or mandiblejaw. Statistically significant differences (P , .001) were foundin the mean angular deviation between maxillary andmandible positions (MD: 0.89 [95%CI: 0.76-1.03]; Figure 3A).The global meta-analysis showed no statistical significance(P5.06) in coronal accuracy when comparing the maxilla andmandible positions (MD: 20.17 [95% CI: 20.34 to 0.00];Figure 3B), whereas differences in apical error betweenmaxillae and mandibles were also not statistically significant(P 5 .8) (MD: 0.03 [95% CI: 20.20 to 0.27]; Figure 3C).
Influence of Guide Type (Totally Guide vs. PartiallyGuide)Only 2 studies (1 prospective and 1 retrospective study; n 5
215 implants) reported data comparison of totally andpartially guided surgery protocols. The results of the pro-spective study showed that the angular deviation wassignificantly greater (P, .001) in the partially guided surgerygroup, whereas the retrospective study showed no statisticaldifference (P 5 .35) in angular deviation when comparingthe partially guided with totally guided surgery. Globalmeta-analysis indicated statistically greater accuracy(P , .001) in angle in the totally guided surgery group thanthe partially guided surgery group (MD: 21.16 [95%CI: 21.40 to 20.92]; Figure 4A). As for the deviation at theentry point and apex, the results showed significant greatererror (P , .001) in the partially guided surgery group(MD: 20.53 [95% CI: 20.61 to 20.45] and MD: 20.65[95% CI: 20.75 to 20.56], respectively) (Figure 4B-C).
Effect of Flap ApproachThree studies (2 prospective studies and 1 retrospectivestudy, n 5 190 implants) compared the effect of open-flapor flapless approach on the accuracy of guided surgery.A statistically significant greater reduction (P, .001) in angledeviation (MD: 1.20 [95% CI: 0.90-1.50]) (Figure 5A) andcoronal deviation (MD: 0.55 [95% CI: 0.45-0.65])(Figure 5B) was reported in the guided surgery group witha flapless approach. For deviation at the apex, theoutcome of the subgroup with retrospective study showedno statistical difference between flap and flapless groups(P 5 .07); however, the global analysis showed that theflapless group had significantly more accuracy (P , .001)than the open-flap group (MD: 0.66 [95% CI: 0.54-0.79])(Figure 5C).
Volume 18, Number 1
Influence of the Guide FixationTo evaluate the influence of fixation on accuracy, only 2retrospective studies (n 5 132 implants) were included.Significant differences (P , .001) were observed in the de-viation of angle based on the use of fixation screw(MD: 21.30 [95% CI: 21.94 to 20.66]) (Figure 6A). Nostatistically differences were seen between fixed andunfixed guides in coronal deviation (P 5 .88) and apicaldeviation (P 5 .93) (Figure 6B-C).
DISCUSSIONIn this systematic review of the literature, the accuracy ofguided implant surgery and the involved clinical factorswere evaluated. At the time of this review, 4 other publica-tions6,18-20 had reviewed literature regarding the accuracy;however, only limited and incomplete data were provided onclinical trials. In this meta-analysis, in addition to evaluation ofthe overall deviation of guided surgery, a comprehensivecomparison of involved clinical factors was also performed tosee whether these factors could influence the accuracy of theposition of implants inserted with STL guides. The involvedfactors included age, radiology method, the position ofguide (maxilla or mandible),24-27 type of guide (totally orpartially guided),28,29 flap approach (open flap or flap-less),25,27,28 and guide fixation (use of fixation screw ornot).29,30 The effect of the type of tissue support has beenwell evaluated in another review,18 so we did not repeat thesame work on the type of tissue support.
In addition, during study selection, we found that the pa-rameters used in clinical studies for evaluating deviationwerediverse. Some of the studies reported 2D deviations with orwithout lateral and depth parameters, whereas other studiesused 3D measurement. Some studies evaluated lateral anddepth errors both coronally and apically, whereas othersincluded data only at the entry point or at the apex. More-over, calculation of these parameters was different. To stan-dardize the measurement, only studies with data of at leastglobal angular, coronal, and apical deviations were included;lateral and depth deviations at the entry point and the apexwas reviewed separately. According to some plausible andstraightforward measurement of deviation,20,31 global devi-ation was defined as the distance between the coronal/apicalcenters of the planned and placed implants, and angulardeviation was calculated as the 3D angle between the lon-gitudinal axes of both. Depth deviation was the coronal/apical vertical distance between the planned and placedimplants, and lateral deviation was the coronal/apical hori-zontal distance between the planned and placed implants.These should be taken into account as consensus parametersin further studies to standardize the research work.
The results in this meta-analysis showed a mean deviation atthe entry point of 1.25 mm, at the apex of 1.57 mm, and

Figure 4. Deviation stratified by the guide type (totally guided vs partially guided): (A) angular deviation; (B) deviationat the entry point; and (C) deviation at the apex. CI, confidence interval; Max., maxilla; Mand., mandible; SD, standarddeviation.
The Journal of EVIDENCE-BASED DENTAL PRACTICE
angle of 4.1�. Meanwhile, the lateral coronal deviationretrieved from 7 studies26,29,30,32-35 was 1.05 mm, andlateral apical deviation retrieved from 4 studies26,33-35 was
0.91 mm. Coronal/apical depth deviation26,33,35,36 was0.64 mm/1.24 mm. These results agree with previous reviewstudies, which indicated that although guided implant
March 2018 35

Figure 5. Deviation stratified by the flap approach (flap vs flapless): (A) angular deviation; (B) deviation at the entrypoint; and (C) deviation at the apex. CI, confidence interval; Max., maxilla; Mand., mandible; SD, standard deviation.
The Journal of EVIDENCE-BASED DENTAL PRACTICE
Volume 18, Number 136

Figure 6. Deviation stratified by the fixation method (fixed vs unfixed): (A) angular deviation; (B) deviation at the entrypoint; and (C) deviation at the apex. CI, confidence interval; Max., maxilla; Mand., mandible; SD, standard deviation.
The Journal of EVIDENCE-BASED DENTAL PRACTICE
surgery has many advantages, the possible deviation errorswith this technique that might cause damage to adjacentanatomic structures or lead to restoration misfit are notnegligible.
As we mentioned earlier, the deviation errors accumulatefrom every step of the procedure, so the involved clinicalfactors must be considered. Some authors17 reportedsmoking as an influencing factor, and others37 reportedsurgeon experience as an influencing factor.Factors such as CT scan method, guide position, type ofguide, and so on were also reported in theliterature.12,16,27,38,39 In this systematic review, wesummarized these clinical factors, and several importantfindings were observed.
First, guided surgery performed on the mandible has a moreangular accuracy than on the maxilla. Based on our dailypractice, the possible explanation might be the boneanatomy and bone density; the structure of the mandible isstraight with an arcuate shape, whereas the shape of maxillais a circular curve, which restrains the angulation control. Inaddition, the mandible bone is denser. Another importantfinding was that the totally guided procedure was moreprecise than the partially guided procedure, which isbecause with the partially guided procedure, implants wereinserted manually, thus leading to a greater error than im-plants inserted with a guide. Comparing the accuracy ofguided surgery between the flapless and open-flap ap-proaches, the results indicated that a flapless approach ismore accurate than an open-flap approach. This can be
March 2018 37

The Journal of EVIDENCE-BASED DENTAL PRACTICE
38
explained by the fact that guided surgery required a moreextensive flap than conventional surgery did18;repositioning of the guide during surgery is more difficultbecause of the possible interference of the reflectedtissue.40,41 Finally, a guide with fixation screws showedgreater reduction in angular deviation than a guidewithout fixation screws. The stability of STL template couldbe the explanation; a fixed surgical guide is more accuratethan manual pressure or freehand placement to positionthe surgical guide.42
Regarding the effects of age and the radiology method,the meta-regressive analysis observed that age has nosignificant influence on accuracy. This result rejected ourprevious hypothesis that guided surgery performed onyounger patients has greater accuracy because of highbone quality; dense bone cannot affect the angular devi-ation, regardless of the implant placement method.39 Apossible explanation is that the subjects included in thisstudy were at their middle age or older, in which stageindividuals achieve peak bone mass, and after that, boneloss became more rapid than bone formation.Comparison of CT and CBCT revealed no significantdifference for the influence on accuracy, which coincidedwith the results of the only study reporting on deviationcomparison between CT- and CBCT-derived STLguides.23 Other factors such as smoking habit, thesurgeon’s experience, surgery site in arch, guide system,and implant length were not analyzed in this review; thereason is that not enough eligible studies focusing onthese factors were available. This fact reminds us ofincluding these factors in further studies.
As to the quality of included studies and potential bias, onlyprospective and retrospective clinical studies were includedin this meta-analysis considering our daily clinical practice.Each study was analyzed using the Newcastle-Ottawa Scaleto evaluate methodological quality, which showed moder-ate to high quality. To avoid or minimize possible selectionbias, a standard protocol was employed, and exact inclusionand exclusion criteria were defined. In addition, the datafrom prospective and retrospective studies were analyzedseparately in subgroups. Significant heterogeneity wasobserved when comparing some of the involved clinicalfactors. Possible explanations are as follows: the study de-signs were different, the included patients were diverse, andthere were clinical variations. After sensibility analysis, onestudy26 including only 10 subjects with single missing toothwas recognized, but with low sensitive to the overall results.One obvious limitation of this review is the limited numberof included studies, which impacts the results of this meta-analysis. These limitations remind us that additional clinicalstudies on accuracy are still needed to provide guideline forclinical work.
Volume 18, Number 1
CONCLUSIONIt can be concluded that the position of guide (maxilla ormandible), guide fixation (use of fixation screw or not), typeof guide (totally or partially guided), and flap approach(open flap or flapless) influence the accuracy of computer-aided implant surgery. Totally guided systems using fixedscrews with a flapless approach had greater accuracy. Tominimize the cumulative errors, clinicians can make a totallyguided system with fixed screws as the first choice in dailypractice, which can be made better with a flaplessapproach. Future clinical research work should be directedto use a standardized measurement for accuracy and tocontrol all involved factors to improve the accuracy ofguided implant surgery.
REFERENCES1. BouSerhal C, Jacobs R, Quirynen M, Steenberghe D. Imaging
technique selection for the preoperative planning of oral im-plants: a review of the literature. Clin Implant Dentistry RelatRes 2002;4:156-72.
2. Lofthag-Hansen S, Grondahl K, Ekestubbe A. Cone-beam CTfor preoperative implant planning in the posterior mandible:visibility of anatomic landmarks. Clin Implant Dent Relat Res2009;11:246-55.
3. Weber HP, Cano J, Bonino F. Digital implant surgery. Clin ApplDigital Dental Technology-Wiley-Blackwell; 2015:155-6.
4. Orentlicher G, Abboud M. Guided surgery for implant therapy.Oral Maxillofac Surg Clin North Am 2011;23:239-56. v-vi.
5. Chen X, Yuan J, Wang C, Huang Y, Kang L. Modular preoper-ative planning software for computer-aided oral implantologyand the application of a novel stereolithographic template: apilot study. Clin Implant Dent Relat Res 2010;12:181-93.
6. Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computertechnology applications in surgical implant dentistry: a sys-tematic review. Int J Oral Maxillofac Implants 2014;29(Suppl):25-42.
7. Hämmerle C, Stone P, Jung R, Kapos T, Brodala N. Consensusstatements and recommended clinical procedures regardingcomputer-assisted implant dentistry. Int J Oral MaxillofacialImplants 2009;24:126-30.
8. Hultin M, Svensson KG, Trulsson M. Clinical advantages ofcomputer-guided implant placement: a systematic review. ClinOral Implants Res 2012;23(suppl 6):124-35.
9. Kang SH, Lee JW, Lim SH, Kim YH, Kim MK. Verification of theusability of a navigation method in dental implant surgery:in vitro comparison with the stereolithographic surgical guidetemplate method. J Craniomaxillofac Surg 2014;42:1530-5.
10. Ramasamy M, Giri, Raja R, Subramonian, Karthik,Narendrakumar R. Implant surgical guides: from the past to thepresent. J Pharm Bioallied Sci 2013;5:S98-102.

The Journal of EVIDENCE-BASED DENTAL PRACTICE
11. Platzer S, Bertha G, Heschl A, Wegscheider WA, Lorenzoni M.Three-dimensional accuracy of guided implant placement: in-direct assessment of clinical outcomes. Clin Implant Dent RelatRes 2013;15:724-34.
12. Van Assche N, van Steenberghe D, Quirynen M, Jacobs R.Accuracy assessment of computer-assisted flapless implantplacement in partial edentulism. J Clin Periodontol 2010;37:398-403.
13. Vercruyssen M, Hultin M, Assche N, Svensson K, Naert I,Quirynen M. Guided surgery: accuracy and efficacy. Perio-dontol 2000 2014;66:228-46.
14. Vercruyssen M, Cox C, Coucke W, Naert I, Jacobs R,Quirynen M. A randomized clinical trial comparing guidedimplant surgery (bone- or mucosa-supported) with mentalnavigation or the use of a pilot-drill template. J Clin Periodontol2014a;41:717-23.
15. Vercruyssen M, Laleman I, Jacobs R, Quirynen M. Computer-supported implant planning and guided surgery: a narrativereview. Clin Oral Implants Res 2015;26(suppl 11):69-76.
16. Behneke A, Burwinkel M, Behneke N. Factors influencingtransfer accuracy of cone beam CT-derived template-basedimplant placement. Clin Oral Implants Res 2012;23:416-23.
17. D’Haese J, De Bruyn H. Effect of smoking habits on accuracy ofimplant placement using mucosally supported stereolitho-graphic surgical guides. Clin Implant Dent Relat Res 2013;15:402-11.
18. Raico Gallardo YN, da Silva-Olivio IR, Mukai E, Morimoto S,Sesma N, Cordaro L. Accuracy comparison of guided surgeryfor dental implants according to the tissue of support: a sys-tematic review and meta-analysis. Clin Oral Implants Res2017;28(5):602-12.
19. Schneider D, Marquardt P, Zwahlen M, Jung RE. A systematicreview on the accuracy and the clinical outcome of computer-guided template-based implant dentistry. Clin Oral ImplantsRes 2009;20(suppl 4):73-86.
20. Van Assche N, Vercruyssen M, Coucke W, Teughels W,Jacobs R, Quirynen M. Accuracy of computer-aided implantplacement. Clin Oral Implants Res 2012;23(suppl 6):112-23.
21. Moher D, Shamseer L, ClarkeM, et al. Preferred Reporting Itemsfor Systematic Review and Meta-analysis Protocols (PRISMA-p);2015. statement, http://wwwsystematicreviewsjournalcom/content/4/1/1 2015.
22. Chambrone L, Shibli JA, Mercurio CE, Cardoso B,Preshaw PM. Efficacy of standard (SLA) and modified sand-blasted and acid-etched (SLActive) dental implants in pro-moting immediate and/or early occlusal loading protocols: asystematic review of prospective studies. Clin Oral ImplantsRes 2015;26:359-70.
23. Arisan V, Karabuda ZC, Piskin B, Ozdemir T. Conventional multi-slice computed tomography (CT) and cone-beam CT (CBCT) forcomputer-aided implant placement. Part II: reliability of
mucosa-supported stereolithographic guides. Clin ImplantDent Relat Res 2013;15:907-17.
24. Di Giacomo GA, da Silva JV, da Silva AM, Paschoal GH,Cury PR, Szarf G. Accuracy and complications of computer-designed selective laser sintering surgical guides for flaplessdental implant placement and immediate definitive prosthesisinstallation. J Periodontol 2012;83:410-9.
25. Ersoy AE, Turkyilmaz I, Ozan O, McGlumphy EA. Reliability ofimplant placement with stereolithographic surgical guidesgenerated from computed tomography: clinical data from 94implants. J Periodontol 2008;79:1339-45.
26. Farley NE, Kennedy K, McGlumphy EA, Clelland NL. Split-mouth comparison of the accuracy of computer-generated andconventional surgical guides. Int J Oral Maxillofac Implants2013;28:563-72.
27. Ozan O, Turkyilmaz I, Ersoy AE, McGlumphy EA, Rosenstiel SF.Clinical accuracy of 3 different types of computed tomography-derived stereolithographic surgical guides in implant place-ment. J Oral Maxillofac Surg 2009;67:394-401.
28. Arisan V, Karabuda ZC, Ozdemir T. Accuracy of two stereo-lithographic guide systems for computer-aided implant place-ment: a computed tomography-based clinical comparativestudy. J Periodontol 2010;81:43-51.
29. Cassetta M, Di Mambro A, Giansanti M, Stefanelli LV,Cavallini C. The intrinsic error of a stereolithographic surgicaltemplate in implant guided surgery. Int J Oral Maxillofac Surg2013;42:264-75.
30. Cassetta M, Giansanti M, Di Mambro A, Calasso S, Barbato E.Accuracy of two stereolithographic surgical templates: a retro-spective study. Clin Implant Dent Relat Res 2013a;15:448-59.
31. Valente F, Schiroli G, Sbrenna A. Accuracy of computer-aidedoral implant surgery, a clinical and radiographic study. Int JOral Maxillofacial Implants 2009;24:234-42.
32. Cassetta M, Stefanelli LV, Giansanti M, Di Mambro A, Calasso S.Depth deviation and occurrence of early surgical complicationsor unexpected events using a single stereolithographic surgi-guide. Int J Oral Maxillofac Surg 2011;40:1377-87.
33. Lee JH, Park JM, Kim SM, Kim MJ, Lee JH, Kim MJ. Anassessment of template-guided implant surgery in terms ofaccuracy and related factors. J Adv Prosthodont 2013;5:440-7.
34. Stubinger S, Buitrago-Tellez C, Cantelmi G. Deviations be-tween placed and planned implant positions: an accuracy pilotstudy of skeletally supported stereolithographic surgical tem-plates. Clin Implant Dent Relat Res 2014;16:540-51.
35. Verhamme LM, Meijer GJ, Boumans T, de Haan AF, Berge SJ,Maal TJ. A clinically relevant accuracy study of computer-planned implant placement in the edentulous maxilla usingmucosa-supported surgical templates. Clin Implant Dent RelatRes 2015;17:343-52.
36. Vasak C, Watzak G, Gahleitner A, Strbac G, Schemper M,Zechner W. Computed tomography-based evaluation of
March 2018 39

The Journal of EVIDENCE-BASED DENTAL PRACTICE
40
template (NobelGuide)-guided implant positions: a prospectiveradiological study. Clin Oral Implants Res 2011;22:1157-63.
37. Cushen SE, Turkyilmaz I. Impact of operator experience on theaccuracy of implant placement with stereolithographic surgicaltemplates: an in vitro study. J Prosthetic Dentistry 2013;109:248-54.
38. Cassetta M, Di Mambro A, Di Giorgio G, Stefanelli LV,Barbato E. The influence of the tolerance between mechanicalComponents on the accuracy of implants inserted with a ster-eolithographic surgical guide: a retrospective clinical study. ClinImplant Dent Relat Res 2015;17:580-8.
39. Ozan O, Orhan K, Turkyilmaz I. Correlation between bonedensity and angular deviation of implants placed using
Volume 18, Number 1
CT-generated surgical guides. J Craniofac Surg 2011;22:1755-61.
40. Lal K, White GS, Morea DN, Wright RF. Use of stereolithographictemplates for surgical and prosthodontic implant planning andplacement. Part I. The concept. J Prosthodont 2006;15:51-8.
41. Vieira DM, Sotto-Maior BS, Barros CA, Reis ES,Francischone CE. Clinical accuracy of flapless computer-guidedsurgery for implant placement in edentulous arches. Int J OralMaxillofac Implants 2013;28:1347-51.
42. Arisan V, Karabuda CZ, Ozdemir T. Implant surgery using bone-and mucosa-supported stereolithographic guides in totallyedentulous jaws: surgical and post-operative outcomes ofcomputer-aided vs. standard techniques. Clin Oral Implants Res2010;21:980-8.

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具