Embed Size (px)
Citation preview

The University of Leeds School of Medicine
2nd Year MB ChB 2015-16
CAMPUS TO CLINIC
CLINICAL EXAMINATION TEMPLATES

2
CONTENTS
3 Cardiovascular 7 Respiratory 11 Gastrointestinal 15 Cranial Nerves 23 Peripheral Nerve: Lower Limb 27 Peripheral Nerve: Upper Limb 31 Vascular Exam of Lower Limb 33 Clinical Exam of the Urological System 35 Clinical Exam of Lumbar Spine 37 Clinical Exam of the Cervical Spine 39 MSK Clinical Examination of the Elbow 41 MSK Clinical Examination of the Foot and Ankle 43 MSK Clinical Examination of the Hand and Wrist 47 MSK Clinical Examination of the Hip Joint 49 MSK Clinical Examination of the Knee 53 MSK Clinical Examination of the Shoulder 55 MSK Clinical Examination GALS (Gait, Arms, Legs, Spine)
59 Thyroid

3
Clinical Examination Template: Cardiovascular Examination Checklist
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
General observation
of patient (colour, conscious level, any pain or breathing difficulty, build)
of bedside ( oxygen or other bedside equipment, GTN spray/medication)
Hands and nails (clubbing, nicotine staining, splinter haemorrhages, tendon xanthoma, Janeway lesions, Osler’s nodes, pale palmar creases, palpate to ascertain capillary refill time which should be < 2 seconds.)
Pulse
palpate for 30 secs ( 60 secs if pulse irregular) report rate, rhythm & character Check for radio-radial delay and radio-femoral delay (aortic stenosis) Ensure your patient does not suffer with arm or shoulder pain before
examining for a collapsing pulse (present in aortic regurgitation)
Blood Pressure
should be measured manually using correct cuff size and placement, with arm supported at heart level pulse palpation during cuff inflation correct speed of deflation (2mmHg per second) correct recording

4
offer to take standing BP to assess postural hypotension
see clinical skills e-book for complete instructions and video demonstration on the following link www.clinicalskills.leeds.ac.uk/
Face: general colour, ? malar flush of mitral stenosis
Eyes, lips & tongue: look in the eyes for xanthelasma, a corneal arcus and for pallor of conjunctivae. Look at the lips for peripheral cyanosis and under the tongue for central cyanosis. Ascertain general dental hygiene. ? high-arched palate suggestive of Marfan's syndrome
Neck
carotid pulse: palpate and listen for bruits JVP – should be examined and measured with the patient rested at 45
degrees. (know how to demonstrate hepato-jugular reflux which may be useful in clinical practice but is not routinely performed in an OSCE)
Chest/Praecordium
Observation
look for scars (sternotomy, thoracotomy), a pacemaker, and for visible pulsations or heaves
Palpation
Locate the Apex Beat (should know expected site is 5th intercostal space, mid-clavicular line
Heaves – use the flat of the hand to feel for parasternal heaves indicative of LVH or RVH
Thrills – use the lateral border of the hand to palpate all 4 valve areas for palpable murmurs.
Auscultation
Auscultate all 4 valve areas (Aortic, Pulmonary, Tricuspid and Mitral) and carotid arteries with the diaphragm of the stethoscope– ascertain the heart sounds and for any added heart sounds or murmurs.

5
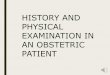
Used under creative commons license: http://www.sharinginhealth.ca/clinical_assessment/heart_sounds.html If an added sound is present try to ascertain if this is occurring in diastole or systole by timing with the carotid pulse.
If a murmur is present try to ascertain at which valve area it is heard and whether there is any radiation, for example into the carotids or into the apex.
Listen at the mitral area with the bell and the patient leaning onto their left hand side – this makes it easier to listen for the low pitched diastolic murmur of mitral stenosis.
Listen at the tricuspid area with the diaphragm of the stethoscope and your patient sat forward in held expiration which will intensify a murmur due to aortic regurgitation.
Auscultate the lungs, particularly looking for fluid at the bases which may be due to heart failure.
Peripheral Oedema: look for and palpate for sacral and ankle oedema which may indicate right sided heart failure. You should press into the area of oedema for 5 seconds to establish whether an indentation remains which indicates pitting oedema.

6
End Pieces (these are things you would routinely do to complete a thorough clinical examination, but would not be able to do in the OSCE)
Lying and standing BP
Abdomen
Observation – for scars, visible pulsations
Palpation
Organomegaly – hepatosplenomegaly can occur due to engorgement from right sided heart failure
Abdominal Aortic Aneurysm – expansile (aorta can be palpable in thin individuals and is pulsatile)
Palpate femoral pulses
Ausculation for renal and femoral bruits
Vascular Examination of the Lower Limbs (covered separately)
Fundoscopy: this is to check for hypertensive and diabetic retinopathy.
Finish the examination
Thank your patient Explain examination findings to your patient or to the examiner as instructed.

7
Clinical Examination Template: Respiratory Examination Checklist
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
General Observation
of patient (colour, SOB/respiratory distress, audible respiratory sounds, position of patient and whether this is to aid breathing, general habitus)
of bedside (oxygen, inhalers, nebuliser)
Always check whether the patient has any pain before proceeding further with the examination.
Inspection of hands and nails
Observe for clubbing, tar staining, peripheral cyanosis, and measure capillary refill time.
Know the three signs that constitute clubbing (increased nail curvature, loss of the hyponychial angle, fluctuance of the nail bed)
Know possible diagnoses this can indicate
Check for flap indicative of CO2 retention by asking patient to hold out their arms with wrists dorsi-flexed and fingers held in extension for 30 secs (know a similar flap can occur in liver failure).
Other signs suggestive of C02 retention include dilation of the veins and increased temperature of the hands.
Respiratory Rate – also consider breathing pattern and respiratory effort.

8
Pulse – rate and rhythm: the pulse can be bounding and tachycardic when there is CO2 retention.
Face, lips and tongue
Observe general colour, check conjunctivae for pallor, lips for peripheral cyanosis, check tongue for central cyanosis
JVP – should be examined and measured with the patient rested at 45 degrees.
Lymphadenopathy – palpate for occipital, post and pre-auricular, anterior and posterior cervical, submental, submandibular (including scalene) and supraclavicular lymph nodes.
Chest
Observation: scars (thoracotomy, sternotomy); chest wall deformities (kyphoscoliosis, Barrel chest)
Palpation
Locate trachea (which should be central) and apex beat (which should be 5th intercostal space mid-clavicular line).
Measure chest expansion (which should be >4cm with maximal inspiration) Check for tactile vocal resonance by palpating the lung fields with the lateral
border of your hand whilst your patient says ‘99’. Check for tactile vocal fremitus by palpating the lung fields whilst your
patient says ‘99’.
Auscultation
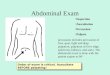
Auscultate using the diaphragm of the stethoscope whilst listening to the patient inhale and exhale through their mouth. (Listen in a J-shape as per diagram)

9
Reference: https://www.asep.org/asep/asep/Auscultation.html
Listen to all areas of the anterior, posterior and lateral lung fields, including the apices. Compare the breath sounds on each side.
Check for additional breath sounds such as stridor, wheeze, pleural rub.
Percussion – percuss all areas of the lung fields, as for auscultation, remembering to compare sides. Know the significance of tympanic, hyperresonant and dull percussion.
Examine sacrum and legs for oedema.
End Pieces
Remember to check PEFR : ask patient to stand, to hold the monitor horizontally and not to obscure measurement counter, to make a tight seal around the cardboard tube with their mouth, to take a deep breath in then blow out as hard and fast as they can. Take the best of 3 measurements as reading to record.
Measure temperature, BP, Sp02 and examine any sputum.
Finish the examination
Thank your patient Explain examination findings to your patient or to the examiner as instructed.

10

11
Clinical Examination Template: Gastrointestinal Examination Checklist
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
General Observation:
of patient conscious level, colour, comfortable or in pain, general habitus
of bedside catheter/IV fluids, ? Nil by mouth (NBM), PEG feed
Inspection of hands and nails: leuconychia, koilonychia, clubbing, palmar erythema, pale palmar creases, spider naevi, Dupytren’s contracture
Know the three signs that constitute clubbing (increased nail curvature, loss of the hyponychial angle, fluctuance of the nail bed) and the possible diagnoses this can indicate
Check for a hepatic flap indicative of liver failure by asking the patient to hold out their arms for approx 30 secs with the wrists dorsi-flexed and fingers held in extension.
pulse check
Inspection of face, lips and tongue
Pallor, jaundice, mouth ulcers, glossitis, candidiasis
Is there a distinctive odour suggestive of fetor hepatica, ketosis or uraemia?
Lymphadenopathy: Palpate for supraclavicular, axillary and inguinal lymphadenopathy.
Nb Virchow’s node in right supraclavicular fossa is suggestive of gastric malignancy.

12
Abdomen
Inspection
Look for scars, symmetry and shape, any obvious lumps or distension, peristalsis or pulsation, venous distension, discolouration or spider naevi.
Palpation
Ask your patient whether they have any pain before proceeding with palpation of their abdomen.
Warm your hands and pay attention to your patient’s face for any sign of discomfort during the examination.
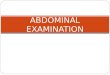
Systematically examine all nine regions of the abdomen starting with light palpation, moving clockwise away from the area of pain.

13
Used under creative commons license: http://www.rcemlearning.co.uk/modules/abdominal-pain-without-shock/clinical-assessment-and-pain-history/abdominal-examination-regions/
Then repeat with deep palpation, and note the site of any tenderness, checking for rebound tenderness
Palpate for organomegaly: liver, spleen, kidneys, bladder and aorta.
Remember a pulsatile aorta can often be palpated, but an expansile swelling may indicate an abdominal aortic aneurysm.
Percussion
To outline the liver, spleen and bladder. Test for shifting dullness and fluid thrill if ascites is suspected
Shifting dullness: Percuss from the centre of the patient’s abdomen laterally until dullness is apparent. Keeping your finger there, then ask the patient to roll onto the opposite side. Wait fot at least 30 seconds in this position, before starting top percuss. If the dullness initially detected was due to fluid, this area should now be resonant and dullness will become apparent as you continue to percuss down to the centre of the abdomen.
Fluid Thrill: Test for this by laying the flat of your left hand against the left side of the patient’s abdomen. Ask your patient to lay the flat of their hand longitudinally along the centre of their abdomen. Then tap your right hand on the right hand side of the patient’s abdomen and feel for a rippling of fluid against your left hand.
Auscultation
Bowel sounds should be present, but may be reduced, absent or increased.
Nb. You will need to listen for a minimum of 2 minutes, in more than one area of the abdomen, before being able to confirm the absence of bowel sounds.
Bruits – check for renal bruits, it is common to hear an aortic bruit which can be normal.
End Pieces (these are routinely done in clinical practice, but not for OSCE purposes)

14
Examine for inguinal herniae – this should be done with the patient standing. Observe for any swelling, ascertain whether there is a cough impulse, and if a hernia is present whether it is reducible.
Examine external genitalia
Rectal examination/PR
Measure temperature
Urinalysis (+ pregnancy test in female patients of child-bearing age) is another important element in the assessment of the GI tract.
Stool sample
Finish the examination
Thank your patient Explain examination findings to your patient or to the examiner as instructed.

15
Clinical Examination Template: Cranial Nerves
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
1: Olfactory
This is tested using a simple screening question, to check whether your patient has any problems with their sense of smell or whether they have noticed any change to this. If there is any doubt, testing can be done using strong-smelling food such as coffee or citrus fruit, or with a smelling kit.
2: Optic
Four different aspects require testing:
• Pupillary reflexes to light and accommodation • Visual acuity • Visual fields • Fundoscopy
Pupillary Light Reflexes
Firstly test for the direct and consensual pupillary reflexes.
First shine the light into the left pupil - in a normal examination the left pupil should constrict to light (The direct pupillary light reflex). Next shine the light into the right pupil looking for constriction on the left side. In a normal examination the left pupil should also constrict when light is shone into the right eye (the consensual light reflex). Then check the opposite side.

16
Secondly test for pupillary accommodation.
Hold your index finger approximately 1 metre away from the patient and gradually move it towards their nose.
In a normal examination both pupils should constrict as the eyes converge and accommodate to continue focusing on your finger.
Visual Acuity
This is tested using a Snellen Chart which has been specially designed to test Visual Acuity at a specific distance.
Please look at the following TedEd link produced by Central Manchester University Hospitals Undergraduate Medical Education which explains how to use a Snellen Chart and how to document your findings http://ed.ted.com/on/J6UoP73Q#watch
Remember your patient can wear their glasses/contact lenses to read the chart, and to test each eye separately.
Visual Fields
These are usually tested by checking the patient can detect finger movement in each of the four quadrants of the visual field – this is quite a crude way to detect gross defects.
Testing is done by ‘confrontation’ – which means testing with your patient sat opposite to you.
It is important to position yourself and the patient approximately an arms-length apart, with your eyes level, as you are testing the patient’s visual field in comparison to your own.
Fundoscopy
The next part of the examination is direct visualisation of the retina by fundoscopy.
Place your hand on their forehead, look for the red reflex, then use your right eye to visualise the back of the patient’s right eye. Start by locating a vessel, follow it to the optic disc, and repeat this until you have followed all 4 vessels.
Finish by asking your patient to look directly into the light to visualise the macula (nb this is extremely difficult in practice!)

17
Then repeat for the left eye.
Look at the following TedEd link produced by Central Manchester University Hospitals Undergraduate Medical Education which explains how to use an opthalmoscope and shows you what you should actually be able to see.
http://ed.ted.com/on/Rl943xSU
3, 4 and 6: Oculomotor, Trochlear and Abducens
These 3 cranial nerves are considered together as they work synergistically in normal eye movement.
Start the examination by looking for any asymmetry of eye position at rest, and checking for ptosis.
Move your finger along horizontal and vertical planes, then by making a letter H.
Ask the patient if they experience any double vision during the test. Note any nystagmus which is most likely to occur at extremes of gaze.
In a normal examination eyes will move smoothly and synchronously. Where a cranial nerve abnormality exists the eyes will not move synchronously and this will cause the patient to experience double vision.
5: Trigeminal Nerve
Trigeminal Nerve: Sensory Division
Test light touch sensation using cotton wool in each of the 3 divisions – ophthalmic, maxillary and mandibular divisions, comparing each side to the other.
The Corneal Reflex
Whilst you need to know how to perform this test it is not routinely tested unless a lesion is suspected as it is very uncomfortable for the patient.
Touch the cornea (not sclera) with cotton wool. In a normal examination both eyes should blink.
(nb The afferent pathway for this reflex is the Trigeminal Nerve and the efferent pathway for this reflex is the Facial Nerve).

18
Trigeminal Nerve: Motor Division
This involves testing of the muscles of mastication, namely temporalis, masseter and the pterygoids.
Ask the patient to clench their teeth while you palpate temporalis and masseter.
Then test the pterygoid muscles by asking the patient to open their jaw and keep it open against resistance.
Then ask the patient to move their jaw from side to side.
In a normal examination you should be able to feel contraction of temporalis and masseter, and should not be able to overcome the strength of the pterygoids. Jaw movement should be equal on both sides.
7. Facial Nerve
This involves testing of the muscles of facial expression, namely frontalis, orbicularis oculi, orbicularis oris and buccinators.
Firstly observe for any facial asymmetry.
Then ask your patient:
Please could you raise your eyebrows as high as you can – keep them there, don’t let me push them down
Now could you squeeze your eyes tight – hold them there, don’t let me open them
Now could you show me your teeth
And finally blow out your cheeks – keep them there
In a normal examination facial movement will be symmetrical.
8. Vestibulocochlear Nerve
This involves a simple screening test to identify hearing problems.
Clinical Hearing Test
Ask your patient if they have any hearing difficulty. Then explain you will whisper a number into each ear in turn and ask them to repeat it.

19
If any hearing difficulty is detected, further testing to distinguish between conductive and sensorineural deafness can be done using Rinne’s test and Weber’s test.
Rinne’s Test
This test uses a tuning fork to ascertain whether bone conduction is louder than air conduction.
Ask your patient if they can hear the vibrating tuning fork held at the entrance to the external auditory canal – this is sound 1
Then place the vibrating tuning fork on the bony prominence of the mastoid process) – this is sound 2
Then ask which sound your patient perceives as being the loudest.
In normal hearing Rinne’s test is positive, and this is when sound 1 (air conduction) is louder than sound 2 (bone conduction)
Rinne’s test is negative in sensorineural hearing impairment, making bone conduction louder than air conduction.
A negative Rinne’s test can actually be a false negative in patients with complete sensorineural deafness in one ear, so the Weber’s test is used to look for this.
Weber’s Test
This is designed in conjunction with Rinne’s test to further investigate unilateral hearing impairment.
Place the vibrating tuning fork in the centre of the patient’s forehead and ask whether they hear this equally on both sides, or whether they perceive the sound to be louder in one ear.
In normal hearing sound will be detected equally on both sides.
If the sound localizes to one ear it could mean that there is either an ipsilateral conductive hearing loss, or a contralateral sensorineural hearing loss.
9 & 10: Glossopharyngeal and Vagus
These nerves supply sensation and muscles controlling movement of the mouth and throat.
Ask your patient to give a cough, and then ask your patient to open their mouth whilst you look at the soft palate. Ask the patient to say ‘aaaah’.
In a normal examination the palate should rise equally on both sides.

20
The Gag Reflex
The Gag reflex can be tested when clinically indicated but is not routinely tested on a well patient.
This is tested by touching the posterior pharynx first to one side, and then the other with a wooden stick – this will cause the palate to rise and the patient to ‘gag’.
(Nb the afferent (sensory) pathway of this reflex is the Glossopharyngeal Nerve.
The efferent (motor) pathway of this nerve is the Vagus.)
11: The Accessory Nerve.
This nerve supplies the trapezius and sternocleidomastoid muscles.
Test by asking your patient to shrug their shoulders and keep them raised whilst you push down to test the strength of the trapezius.
The ask your patient to turn their head first to one side and then the other, again asking them to keep this position against resistance to test the strength of the sternocleidomastoid muscles.
In a normal examination movement and power of the muscles should be equal on both sides.
12: The Hypoglossal Nerve
This nerve supplies the tongue.
Ask your patient to stick out their tongue while you observe for any wasting or fascilculation.
Then ask your patient to move their tongue to one side, and then the other. Then ask them to move their tongue into one cheek and keep it there against resistance, then check the other side.
In a normal examination movement and power of the tongue should be equal on both sides.
In an abnormal examination the tongue will deviate towards the side of the lesion, because the inactive fibres will be overpowered by the functioning muscle fibres on the opposite side.

21
How to conclude the examination
Thank your patient Consider your findings and how to present them in a logical and fluent order. Then consider the possible clinical significance of these findings.

22

23
Peripheral Nerve Examination: Lower Limb
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
General Observation: look for any muscle-wasting, fasciculation, postural and movement abnormalities, involuntary movements e.g. tremors/tics/jerky choreiform movements/writhing athetoid movements). Observe gait, look for mobility aids/callipers.
Ask about any pain prior to starting examination as this involves active and passive movement of the limbs at all joints.
Tone
It is usual to examine your patient sat on a bed with their legs extended in a relaxed position in front of them.
Start by rolling each leg gently from side to side and observe foot movement to gauge whether there is any increase or reduction in muscle tone.
Then passively flex and extend the knee, then the ankle.
Understand the significance of any findings:
Increased tone.
In upper motor neurone disorders this causes spasticity, felt as ‘clasp-knife’ spasticity (Initial resistance, followed by sudden reduction in resistance to movement).

24
In disorder of the basal ganglia ‘lead-pipe’ rigidity is detected due to the sustained resistance throughout the range of movement.
‘Cog-wheel’ rigidity occurs in Parkinson’s disease because a tremor is superimposed on the underlying lead-pipe rigidity.
Decreased tone.
This is usually due to lower motor neurone or cerebellar lesions.
Power
Test each muscle group.
Firstly ask your patient to perform the movement, and then test power against resistance, comparing the sides. You should know which muscle groups you are testing with each movement.
Hip flexion, extension, abduction & adduction: ask your patient to raise their extended leg from the bed, ask them to keep their leg there whilst you resist the movement at the quadriceps. Then ask the patient to return their leg down onto the bed passively, then against resistance.
Knee flexion & extension: ask the patient to bend their knee (and hip). Stabilise their thigh with one hand and ask them to kick-out their leg, then pull their heel back in towards them. Then test the same movements against resistance.
Ankle dorsiflexion & plantarflexion: Ask the patient to bend their foot towards them and then back down to the bed. Then support their lower leg with one hand and test the same movements against resistance.
Big Toe flexion & extension: Stabilise the foot, then ask the patient to bend their big toe towards them, then back down towards the bed. Then test the same movements against resistance.
Coordination
Heel-shin test: ask your patient to place their left heel on their right knee, then run the left heel down towards the right ankle. Then ask them to lift their heel and replace it onto their right knee and repeat the movement several tims as quickly as possible. Compare with the other side.
Toe-tapping: ask your patient to repetitively tap their foot quickly against the floor as quickly as possible, then compare sides.

25
Reflexes: You should know which nerve roots are being tested with each reflex.
Patella (L3/4)
Ankle jerk (S1/2)
Plantar / ‘Babinski reflex’: support the ankle and ‘scratch’ the sole of the foot starting at the lateral side of the heel, moving up the lateral side of the foot, then underneath the toes.
Usually the big toe will flex, but if the big toe extends this indicates an upper motor neurone lesion.
Finally test for clonus: holding the lower leg with one hand, suddenly dorsiflex the ankle and hold it in this position. Clonus is when sustained and rhythmical contraction of the gastrocnemius muscle causes the foot to move backwards and forwards. This occurs if there is a upper motor neurone lesion.
Sensation
Test for light touch (using cotton wool) and sharp touch (using a neuro-tip) sensation in each dermatome, comparing sides.
You should know the dermatomes you are testing.
Joint position sense/Proprioception:
Test this at the DIP joint of the big toe. Stabilise the base of the big and ask your patient to close their eyes. Move the tip of the big toe up and down, explaining which movements you are performing to your patient as an example. Then move the tip of the big toe either up or down and ask your patient to sense the direction of that movement. Test 3 times. If your patient correctly detects the movement their joint position sense is intact. If they are not able to do this test a more proximal joint eg ankle joint, knee until joint position sense can be accurately detected.
Vibration sense:
Confirm that your patient can detect the vibration of a 128hz tuning fork on their sternum.
Then ask your patient to close their eyes and test whether they are able to detect the same vibration on the DIP joint of their big toe, and also when the vibration stops. If your patient correctly detects this their vibration sense is intact. If they are not able to

26
detect this test a more proximal joint e.g. ankle, knee, until vibration sense can be accurately detected.
End Pieces
Romberg: ask your patient to stand with their eyes open and feet apart. The ask the patient to bring their feet together, then close their eyes.
If they become unsteady they have a positive Romberg’s test. If they are unsteady with their eyes open this suggests a cerebellar lesion, if they become unsteady only when closing the eyes this suggests a sensory ataxia.
Gait
General observation of gait may indicate a broad-based ataxic gait suggestive of a cerebellar lesion, the spastic gait of hemiplegia, the shuffling gait of Parkinsonism, or the high-stepping gait which occurs with foot-drop.
Remember the gait may also be affected by pain or muscle-wasting.
How to conclude the examination
Thank your patient Consider your findings and how to present them in a logical and fluent order. Then consider the possible clinical significance of these findings.

27
Peripheral Nerve Examination: Upper Limb
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
General Observation: look for postural and movement abnormalities, involuntary movements e.g. tremors/tics/jerky choreiform movements/writhing athetoid movements). Look for mobility aids/callipers.
Ask about any pain prior to starting examination as this involves active and passive movement of the limbs at all joints.
Tone
Hold the patient’s hand, as if shaking their hand, and with the other hand support their arm at the elbow. Start by flexing and extending the wrist, then the elbow, pronate and supinate the forearm, and finally rotate the shoulder. Compare sides.
Understand the significance of any findings:
Increased tone.
In upper motor neurone disorders this causes spasticity, felt as ‘clasp-knife’ spasticity (Initial resistance, followed by sudden reduction in resistance to movement).
In disorder of the basal ganglia ‘lead-pipe’ rigidity is detected due to the sustained resistance throughout the range of movement.
‘Cog-wheel’ rigidity occurs in Parkinson’s disease because a tremor is superimposed on the underlying lead-pipe rigidity.
Decreased tone.

28
This is usually due to lower motor neurone or cerebellar lesions.
Power
Ascertain whether your patient is right or left-handed.
Pronator Drift: ask your patient to extend their arms, with their palms facing upwards. Ask them to close their eyes.
If there is an upper motor neurone lesion, the affected arm will pronate and fall. This is a positive pronator drift sign.
Test each muscle group.
Firstly ask your patient to perform the movement, and then test power against resistance, comparing the sides. You should know which muscle groups you are testing with each movement.
Shoulder abduction & adduction: ask your patient to flex their elbows, then abduct their arms against resistance applied to the upper arm. Then ask your patient to abduct and adduct an outstretched arm from the shoulder.
Elbow flexion & extension: ask your patient to flex their elbows to 90 degrees. Use one hand to support their upper arm, and the other to provide resistance to their forearm as you test flexion and extension.
Wrist flexion & extension: ask patient to hold out their arms and make a fist, then to flex and extend at the wrist.
Finger adduction, abduction, flexion & extension: ask your patient to squeeze your fingers, then open their fist against resistance. Ask them to spread their fingers wide, then to bring their fingers together.
Thumb adduction & abduction: ask your patient to lift their thumb away from a flat palm, and then bring it back towards a flat palm.

29
Coordination
Finger-nose test
Position yourself so you are facing your patient. Ask your patient to touch their nose with their index finger. Then ask them to reach out to touch your finger help in front of them. (You should hold your finger so that they have to fully extend the arm to reach it). Then ask them to repeat this movement backwards and forwards as between their nose and your finger as quickly as they can. Compare sides.
Look for past-pointing and intention tremor suggestive of cerebellar lesions, but note that coordination will also be affected by weakness or sensory disturbance.
Dysdiadokokinesis
Ask your patient to hold one hand out with the palm facing upwards. Then ask them to place the other hand, also palm upwards, into the other hand. Then ask them to turn the hand over so the back of their hand faces upwards and repeat as quickly as possible.
Dysdiadokokinesis is present when these movements are erratic in force and rhythm.
Rebound phenomena
Ask your patient to flex one arm at the elbow, then stand next to them placing your arm over their chest to protect them. Ask them to pull against your arm with theirs, and let go. Usually the antagonist muscles will stop the patient’s arm from pulling back towards them (and injuring themselves), but this protective mechanism will not be present in cerebellar disease. This is why it is important to protect the patient with your other arm.
Reflexes: You should know which nerve roots are being tested with each reflex.
Supinator (C5/C6)
Biceps (C5/C6)
Triceps (C6/C7)
Sensation

30
Test for light touch (using cotton wool) and sharp touch (using a neuro-tip) sensation in each dermatome, comparing sides.
You should know the dermatomes you are testing.
Joint position sense/Proprioception:
Test this at the DIP joint of the index finger. Hold the finger-tip at the sides of the finger distal to the DIP joint, whilst stabilising the joint below this. Ask your patient to close their eyes. Move the finger-tip up and down, explaining this to your patient as an example. Then move the finger-tip either up or down and ask your patient to sense the direction of that movement. Test 3 times. If your patient correctly detects the movement their joint position sense is intact. If they are not able to do this test a more proximal joint eg MCP joint, wrist, elbow until joint position sense can be accurately detected.
Vibration sense:
Confirm that your patient can detect the vibration of a 128hz tuning fork on their sternum.
Then ask your patient to close their eyes and test whether they are able to detect the same vibration on the DIP joint of their index finger, and also when the vibration stops. If your patient correctly detects this their vibration sense is intact. If they are not able to detect this test a more proximal joint e.g. MCP joint, wrist, elbow until vibration sense can be accurately detected.
How to conclude the examination
Thank your patient Consider your findings and how to present them in a logical and fluent order. Then consider the possible clinical significance of these findings.

31
Vascular Examination of Lower Limb
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
Inspection
This is to look for signs suggestive of venous or arterial insufficiency.
Compare the legs looking for discolouration, cyanosis, skin changes, varicosity, ulceration or hair loss.
Palpation
Ask whether the patient has any pain in their legs before proceeding with your examination.
First check the temperature of the legs using the back of your hand to compare sides.
Then test for capillary refill time in the toes which should be <2 seconds.
If capillary refill time is slow, Buerger’s Test can be used to demonstrate poor arterial blood flow to the lower legs. Raise your patient’s leg to 45 degrees and look for resulting pallor which will occur in the case of poor arterial blood supply suggestive of peripheral vascular disease.
This can be further assessed by ascertaining the APBI (see later).
Palpate the peripheral pulses:
Dorsalis Pedis: use two fingers placed lateral to the extensor hallucis longus tendon

32
Posterior Tibial: palpate behind the media malleolus Popliteal: this can be difficult to locate but is best palpated in the
popliteal fossa with the knee flexed. Femoral: palpate this in the mid-inguinal region.
Auscultation
Listen for bruits over the aorta, renal arteries & femoral arteries.
End Pieces
Trendelenberg Test
This test is used in the context of varicose veins to determine whether there is incompetence of the sapheno-femoral junction.
Ask your patient to lie down on the examination couch and raise their leg to 90 degrees which will allow the veins to empty. Then apply a tourniquet around the top of the thigh distal to the sapheno-femoral junction. Now ask your patient to stand. If the varicosity returns this indicates incompetence of the deep communicating veins. If no filling occurs on standing, remove the tourniquet. If this causes immediate refilling of the veins this suggests incompetence of the sapheno-femoral junction.
ABPI
Please see full instructions and video demonstration in the clinical skills e-book on the following link http://clinicalskills.leeds.ac.uk/cs_ebook
Finish the examination Thank your patient Explain your findings to your patient or to the examiner as instructed.

33
Clinical Examination of the Urological System
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
General inspection:
of patient: build, state of hydration, presence of oedema, pain, fever, sallow complexion due to uraemia, pallor suggestive of anaemia
of bedside: IV fluids, fistulae, catheter bags, dialysis
Pulse, BP and Respiratory Rate
This allows assessment of dehydration, hypertension and hyperventilation which can occur in metabolic acidosis.
Abdominal Examination
Inspection for masses, loin scars, presence of urostomy or catheter for peritoneal dialysis.
Palpation: ballot the kidneys and palpate the bladder
Percussion: if organomegaly or distended bladder
Auscultation: for renal bruits

34
End Pieces
Examination of external genetalia
Examination for inguinal herniae
Rectal examination
Temperature
Urinalysis ( see clinical skills e-book www.clinicalskills.leeds.ac.uk
for full instructions and video demonstration)
How to conclude the examination
Thank your patient Consider your findings and how to present them in a logical and fluent order. Then consider the possible clinical significance of these findings.

35
Clinical Examination of Lumbar Spine
Adapted from http://www.arthritisresearchuk.org/health-professionals-and-students/student-handbook/the-msk-examination-rems/
This site contains video demonstrations of clinical examination which will be useful to supplement your learning.
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
A good musculoskeletal examination relies on patient cooperation, in order for them to relax their muscles so that important clinical signs are not missed.
Check whether your patient is in pain before proceeding with the examination and consider this as you proceed with your examination.
Look
Observe the patient standing from behind looking for muscle wasting, asymmetry or scoliosis.
Then consider posture from the side to look for the normal thoracic kyphosis and lumbar lordosis.
Feel
Palpate the vertebrae and sacroiliac joints for alignment and tenderness.
The palpate the para-spinal muscles for tenderness.
Move
Assess the range of movement in the spine.

36
Lumbar flexion and extension: place three fingers over the lumbar spine then ask your patient to bend forward. Your fingers should move apart during flexion and together during extension.
Lumbar lateral flexion: ask the patient to run their left hand down their left leg bending to one side, then repeat for the right side.
Thoracic rotation: ask your patient to sit facing forwards with their arms crossed in front of them and ask them to twist their shoulders to one side then the other.
Straight Leg Raise (SLR): Ask your patient to lie as flat as possible on the examination couch, and then raise one leg (held straight in extension). Raising of the leg may trigger pain if nerve root irritation is present, and dorsiflexion of the foot will further exacerbate this.
Reflexes: patella and ankle jerk.
Dorsiflexion of the big toe: it is important to check this movement specifically as impairment of this movement, even in isolation, can indicate an L5 nerve root problem.
End Pieces
It may be necessary to perform a full Peripheral Nerve Examination of Lower Limb, including assessment of power, sensation and reflexes if indicated.
Also consider performing a full Peripheral Vascular Examination of the Lower Limb, again if clinically indicated.
How to conclude the examination
Thank your patient Consider your findings and how to present them in a logical and fluent order. Then consider the possible clinical significance of these findings.

37
Clinical Examination of the Cervical Spine
Adapted from http://www.arthritisresearchuk.org/health-professionals-and-students/student-handbook/the-msk-examination-rems/
This site contains video demonstrations of clinical examination which will be useful to supplement your learning.
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
A good musculoskeletal examination relies on patient cooperation, in order for them to relax their muscles so that important clinical signs are not missed.
Check whether your patient is experiencing any pain prior to proceeding with the examination and consider this as you proceed with your examination.
Look
Observe your patient sitting and standing to consider their posture and whether the normal cervical lordosis is present.
Feel
Palpate the cervical spine for alignment and tenderness.
Then palpate the para-spinal muscles, trapezius and upper back muscles for tenderness.
Move
Flexion: ask your patient to move their chin down towards their chest Extension: ask your patient to tilt their head backwards

38
Lateral flexion: then ask your patient to bring their ear towards their shoulder on each side.
Reflexes: check biceps, triceps and supinator reflexes in each arm.
End Pieces
It may be necessary to perform a full Peripheral Nerve Examination of the Upper and Lower Limb, including assessment of tone, power and sensation if clinically indicated.
How to conclude the examination
Thank your patient Consider your findings and how to present them in a logical and fluent order. Then consider the possible clinical significance of these findings.

39
MSK Clinical Examination of the Elbow
(adapted from http://www.arthritisresearchuk.org/health-professionals-and-students/student-handbook/the-msk-examination-rems)
This site contains video demonstrations of clinical examination which will be useful to complement your learning.
Introduction Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed with
the examination Clean your hands Ongoing communication to patient involves clear instructions and attention to your
patient’s comfort.
Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a logical
order. A good musculoskeletal examination relies on patient cooperation, in order for them to relax their muscles, if important clinical signs are not to be missed. Ask whether your patient has any pain before beginning your examination and consider this as you proceed. With their permission adequately expose the patient to expose the whole of both upper limbs. Examination should normally take place with the patient’s hands resting on a pillow as it can be painful for patients with elbow or shoulder problems to hold their hands up for long.
Look at your patient’s arm as they stand in the anatomical position from the front for carrying angle from the side for flexion deformity scars, rashes, muscle wasting, rheumatoid nodules, psoriatic plaques, swellings e.g.
olecranon bursitis
Feel skin temperature (using the back of your hand) across the joint and the forearm hold the forearm in one hand with the elbow flexed to 90°, palpate the elbow joint,
feeling the head of the radius and the joint line with your thumb. If swelling, is it fluctuant? (synovitis is usually felt as a fullness between the olecranon and the lateral epicondyle)
palpate the medial and lateral epicondyles (for golfer’s and tennis elbow respectively) and olecranon process for tenderness and evidence of bursitis
Move assess full range of elbow flexion and extension (assess both actively and passively
and compare one side with the other, feel for crepitus)

40
assess pronation and supination (assess both actively and passively and compare one side with the other, feel for crepitus)
Function can the patient reach their mouth with their hand? can they reach behind their head?
How to conclude the examination
Thank your patient Consider your findings and how to present them in a logical and fluent order. Then consider the possible clinical significance of these findings.

41
MSK Clinical Examination of the Foot and Ankle
Adapted from http://www.arthritisresearchuk.org/health-professionals-and-students/student-handbook/the-msk-examination-rems/
This site contains video demonstrations of clinical examination which will be useful to supplement your learning.
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed with
the examination Clean your hands Ongoing communication to patient involves clear instructions and attention to your
patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a logical
order. A good musculoskeletal examination relies on patient cooperation, in order for them to relax their muscles, if important clinical signs are not to be missed. Check whether your patient is experiencing any pain prior to proceeding with your examination and consider this as you proceed. With their permission adequately expose the patient to expose the whole of both lower limbs.
Look (with the patient sitting on the couch, their feet overhanging the end of it) Examine the forefoot for nail changes, skin rashes, alignment of the toes (?evidence of
hallux valgus or clawing of the toes) and for any joint swelling, then inspect the plantar surface for callus formation.
Look at the patient’s footwear: check for abnormal or asymmetrical wearing of the sole or upper, for evidence of poor fit or the presence of special insoles.
Look (with the patient weight-bearing)
Re-examine the forefoot for toe alignment (hallux valgus/clawing) midfoot for foot arch position (a dropped arch in a normal subject should resolve
when standing on tip toes).

42
Look (from behind)
hindfoot for Achilles tendon thickening or swelling. look for normal alignment of the hindfoot, as opposed to a varus or valgus
deformity of the subtalar joint.
Feel assess the temperature over the forefoot, midfoot and ankle (with back of hand). check peripheral pulses. gently squeeze across the MTP joints (ask permission first, watching the patient’s face
for signs of discomfort which may indicate inflammatory joint disease)
palpate the midfoot, the lateral and medial malleoli and subtalar joints for tenderness.
In the case of an acute ankle injury you must also palpate the lateral and medial malleolus, base of the 5th metatarsal and navicular for bony tenderness which may indicate a fracture as per the Ottowa Ankle Rule.
Move Assess movement actively and passively at the:
Subtalar joint (inversion/eversion) Dorsi-flexion and plantar-flexion of the big toe and ankle joint Passive rotation of the midtarsal joint: performed by fixing the heel with one hand
and, with the other hand, passively inverting and everting the forefoot. in the case of acute ankle injury you must also ascertain whether your patient can
fully weightbear
Function Observe your patient’s gait, watching for the normal cycle of heel strike, stance, and toe-
off.
How to conclude the examination
Thank your patient Consider your findings and how to present them in a logical and fluent order.
Then consider the possible clinical significance.

43
MSK Clinical Examination of the Hand and Wrist
Adapted from http://www.arthritisresearchuk.org/health-professionals-and-students/student-handbook/the-msk-examination-rems/
This site contains video demonstrations of clinical examination which will be useful to supplement your learning.
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed with
the examination Clean your hands Ongoing communication to patient involves clear instructions and attention to your
patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a logical
order.
A good musculoskeletal examination relies on patient cooperation, in order for them to relax their muscles, if important clinical signs are not to be missed. Check whether your patient has any pain before proceeding with your clinical examination. With their permission adequately expose the patient to expose the whole of both upper limbs. Examination should normally take place with the patient’s hands resting on a pillow as it can be painful for patients with elbow or shoulder problems to hold their hands up for long.
Look: hands palms down swelling, deformity(such as z-shaped deformity or ulnar deviation), muscle wasting,
scars, palmar erythema or Dupytren’s contracture. skin for thinning and bruising (signs of long-term steroid use) or rashes e.g. psoriasis nails for pitting or onycholysis (psoriatic changes), nailfold vasculitis, clubbing, splinter
haemorrhages.
Are the changes symmetrical or asymmetrical? Do they involve the small joints or the wrists?
Look: hands palms up
muscle wasting – if present, is it both the thenar and hypothenar eminences (if only thenar ? carpal tunnel syndrome)
Scar at wrist ? carpal tunnel release

44
Feel: hands palms up (ask about tenderness before starting palpation)
? muscle-wasting of thenar and hypothenar eminences median and ulnar nerve sensation (light touch over thenar and hypothenar eminences;
the index and little fingers respectively) ?normal and equal
Feel: hands palms down radial nerve sensation (light touch over the thumb and index finger web space) skin temperature at forearm, wrist, MCPs (use the back of your hand). ?any differences gently squeeze across the row of MCPs to assess for tenderness (watching the
patient’s face for signs of discomfort which can indicate inflammatory arthritis bimanually palpate any MCPs, PIPs or DIPs that appear swollen or painful.:
?evidence of active synovitis: warm, swollen, tender and may have a ‘rubbery’ feel or effusions ? hard, bony swellings ? squaring of the carpometacarpal (CMC) joint ?Heberden’s nodes on the DIPs.
(nb There may be evidence of previous synovitis i.e. thickened, rubbery but non-tender joints).
Bimanually palpate the patient’s wrists Check the radial pulse Finally run your hand up the patient’s arm along the ulnar border to the elbow (for
rheumatoid nodules or psoriatic plaques on the extensor surfaces) Move Finger movement: check flexion, extension, adduction and adduction. ask the patient to make a fist assess wrist flexion and extension actively (e.g. by making the ‘prayer’ sign see
picture below) and then passively. In patients where history or examination suggest carpal tunnel syndrome perform Phalen’s test (forced flexion of the wrists for 60 seconds). A positive test reproduces patient’s symptoms. (see picture below)

45
median and ulnar nerves for power: abduction of the thumb, and finger spread,
respectively. Function Ask the patient to grip your two fingers to assess grip strength. Ask the patient to pinch your finger to test their pincer grip. Ask the patient to pick a
small object such as a coin out of your hand or check their ability to undo buttons.
Finish the examination
Thank your patient Explain your findings to your patient or to the examiner as instructed.

46

47
MSK Clinical Examination of the Hip Joint
Adapted from http://www.arthritisresearchuk.org/health-professionals-and-students/student-handbook/the-msk-examination-rems/
This site contains video demonstrations of clinical examination which will be useful to supplement your learning.
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed with
the examination Clean your hands Ongoing communication to patient involves clear instructions and attention to your
patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a logical
order.
A good musculoskeletal examination relies on patient cooperation, in order for them to relax their muscles, if important clinical signs are not to be missed. Check whether your patient is experiencing pain prior to starting the examination and consider this as you proceed. With their permission adequately expose the patient to expose the whole of both lower limbs.
Look Ask your patient to stand and assess for muscle wasting (gluteal muscle bulk in
particular) Then ask your patient to lie supine on the examination couch and observe the legs,
?obvious flexion deformity of the hip (comparing one side with the other) Consider leg length disparity, assess true leg lengths using a tape measure
(measurements are taken from the anterior superior iliac crest to the medial malleolus of the ankle on the same side)
check for scars overlying the hip
Feel palpate over the greater trochanter for tenderness Move with knee flexed at 90º, assess full hip flexion (comparing one side with the other)

48
assess for fixed flexion deformity of the hip by performing Thomas’ test: keep one hand
under the patient’s back to ensure that normal lumbar lordosis is removed, fully flex one hip and observe the opposite leg. If it lifts off the couch then there is a fixed flexion deformity in that hip.
with the hip and knee flexed at 90º, assess internal and external rotation of both hips (often limited in hip disease)
assess the hip and proximal (gluteal) muscle strength by performing the Trendelenberg test: the patient alternately standing on each leg alone. In a negative test the pelvis remains level or even rises. In an abnormal test the pelvis will dip on the contralateral side.
Function assess gait ? antalgic (painful limp) or Trendelenberg gait (‘waddling’ often from
proximal muscle weakness)
Finish the examination
Thank your patient Explain your findings to your patient or to the examiner as instructed.

49
MSK Clinical Examination of the Knee
Adapted from http://www.arthritisresearchuk.org/health-professionals-and-students/student-handbook/the-msk-examination-rems/
This site contains video demonstrations of clinical examination which will be useful to supplement your learning.
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed with
the examination Clean your hands Ongoing communication to patient involves clear instructions and attention to your
patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a logical
order. A good musculoskeletal examination relies on patient cooperation, in order for them to relax their muscles, if important clinical signs are not to be missed. Check with your patient whether they are in pain prior to beginning the examination and consider this as you proceed. With their permission adequately expose the patient to expose the whole of both lower limbs.
Look from the end of the couch with the patient’s legs straight: look at the knees (comparing
one with the other) looking for symmetry and alignment. Looking for a valgus deformity (when the leg below the knee is deviated laterally (knock-kneed) or a varus deformity (when the leg below the knee is deviated medially (bow-legged).
check for a knee flexion deformity (distinguishing this from hip flexion deformity by examining hip movements as outlined in hip exam).
check for muscle wasting, scars, redness or swelling check for a rash suggesting psoriasis. NB: Popliteal swellings, varus and valgus deformities may be more apparent with the patient weight-bearing.
Feel skin temperature (with back of hand) starting with the mid-thigh and comparing it to the
temperature over the knee. Compare one knee to the other. palpate for tenderness of the patella.

50
with the knee flexed to 90º, palpate for tenderness and swelling along the joint line from the femoral condyles to the inferior pole of the patella, then down the inferior patella tendon to the tibial tuberosity.
feel behind the knee for a popliteal (Baker’s) cyst. assess for an effusion by performing a patellar tap Assess for a fluid bulge by cross fluctuation (if there is no patellar tap): Stroke the
medial side of the knee upwards (towards the suprapatellar pouch) to empty the medial compartment of fluid, then stroke the lateral side downwards (distally). The medial side may refill, and produce a bulge of fluid indicating an effusion.
Move ask the patient to flex the knee as far as possible (active movement) with patient fully relaxed, assess passive movement. Place one hand on the knee
(feeling for crepitus) and flexing the knee as far as possible, noting the range of movement
assess full flexion and extension of the knees (comparing one to the other) with the knee flexed to 90º, check the stability of the knee ligaments. Look initially
from the side of the knee, checking for a posterior sag or stepback of the tibia, suggesting posterior cruciate ligament damage.
perform an anterior draw test: place both hands round the upper tibia, with your thumbs over the tibial tuberosity and index fingers tucked under the hamstrings to make sure these are relaxed. Stabilize the lower tibia with your forearm and gently pull the upper tibia forward. In a relaxed, normal patient there is normally a small degree of movement. Excess movement suggests anterior cruciate ligament laxity.

51
assess medial and lateral collateral ligament stability by flexing the knee to 15º and
alternately stressing the joint line on each side. Place one hand on the opposite side of the joint line to that which you are testing, and apply force to the lower tibia. This may be done with the leg on the couch or with the lower tibia supported on the examiner’s pelvis.
Function ask the patient to stand and then walk a few steps, looking again for a varus or valgus
deformity
Finish the examination
Thank your patient Explain your findings to your patient or to the examiner as instructed.

52

53
MSK Clinical Examination of the Shoulder
Adapted from http://www.arthritisresearchuk.org/health-professionals-and-students/student-handbook/the-msk-examination-rems/
This site contains video demonstrations of clinical examination which will be useful to supplement your learning.
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed with
the examination Clean your hands Ongoing communication to patient involves clear instructions and attention to your
patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a logical
order. A good musculoskeletal examination relies on patient cooperation, in order for them to relax their muscles, if important clinical signs are not to be missed. Check whether your patient is experiencing pain before starting your examination and consider the implications of this as you proceed. With their permission adequately expose the patient to expose the whole of both upper limbs.
Look
inspect from the front, from the side and from behind, checking for symmetry, posture, muscle wasting and scars
Feel assess the temperature over the front of the shoulder
palpate the bony landmarks for tenderness, starting at the sternoclavicular joint, then
the clavicle, acromioclavicular joint, acromion process and around the scapula
palpate the joint line – anterior and posterior
palpate the muscle bulk of the supraspinatus, infraspinatus and deltoid muscles Move ask the patient to put their hands behind their head (external rotation) comparing one
side with the other

54
ask the patient to put their hands behind their back (internal rotation) comparing one side with the other. If there is a restriction in the latter movement, how far the patient can reach e.g. to the lumbar, lower thoracic or mid-thoracic level.
with the elbow flexed at 90º and tucked into the patient’s side, assess external rotation of the shoulder (loss of external rotation may indicate a frozen shoulder)
ask the patient to raise their arms behind them and to the front (extension and flexion) abduction: ask the patient to abduct the arm to assess for a painful arc (between 10º
and 120º). Can you passively take the arm further?
Be sure to assess abduction from behind the patient and observe scapular movement because restricted gleno-humeral movement can be compensated for by scapular/thoracic movements. Function Can the patient get the hands behind the head and back? This is important in washing, dressing and grooming.
Finish the examination
Thank your patient Explain your findings to your patient or to the examiner as instructed.

55
Clinical Examination: GALS (Gait, Arms, Legs, Spine)
Adapted from http://www.arthritisresearchuk.org/health-professionals-and-students/student-handbook/the-msk-examination-gals.aspx
This site contains a video demonstration of this clinical examination which will be useful to supplement your learning.
This is a routine screening examination which has been shown to be highly sensitive in detecting significant abnormalities of the musculoskeletal system.
You may be asked to perform this global assessment of the musculoskeletal system or a specific examination of a particular joint in an OSCE.
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
A good musculoskeletal examination relies on patient cooperation, in order for them to relax their muscles so that important clinical signs are not missed.
Check whether the patient has any pain prior to starting the examination and consider this when proceeding with the examination.
Inspection
Examine your patient standing in the anatomical position from behind, from the side and from the front looking for:
Muscle bulk, muscle wasting or asymmetry in the shoulder girdle, gluteal muscles, quadriceps and calf muscles.
Alignment of the spine: looking for scoliosis, kyphosis and lordosis which can be physiological or due to deformity.
Limb alignment Are the iliac crests level?

56
Can your patient fully extend their elbows and knees? Any popliteal swelling Foot abnormalities (high or flattened arches, hallux valgus)
Gait
Ask your patient to walk forwards, turn and walk back while you observe for the symmetry, stride length and smoothness of their gait, and whether they are able to turn quickly.
Arms
Ask your patient to put their hands behind their head and then onto their lower back.
This tests shoulder abduction and external rotation, which are important movements in performing activities of daily living.
Ask your patient to stretch out their hands, palms down with fingers outstretched, looking for deformity and joint swelling. Then inspect the palms for muscle bulk.
Gently squeeze the MCP joints looking for tenderness which may indicate inflammatory joint disease.
Then ask your patient to make a fist, squeeze your hand to test for grip strength, and ask them to perform pincer movements with fingers and thumb to test fine precision grip.
Legs
Ask your patient to lie supine on the examination couch. Inspect the legs for muscle bulk and obvious deformity.
Assess flexion and extension at the knees, feeling for crepitus, and perform the patellar tap test to check for any joint effusion.
Then test flexion and internal rotation at the hip joint.
Spine
Test movement of the cervical spine by asking your patient to tilt their ear towards their shoulder on each side (lateral flexion).
Finally ask your patient to stand, place three fingers on the vertebrae in the lumbar spine and ask your patient to bend forward to assess the degree of lumbar flexion.

57
This screening examination may need to be followed by more detailed examination of specific joints which are covered separately.
How to conclude the examination
Thank your patient Consider your findings and how to present them in a logical and fluent order. Then consider the possible clinical significance of these findings.

58

59
Clinical Examination Template: Thyroid Examination Checklist
Examination is of the thyroid gland itself and also to look for systemic evidence of the effect of an underactive/overactive thyroid.
Introduction
Greet your patient Introduce yourself and your role Explain what you are going to do and why, and gain consent to proceed
with the examination Clean your hands Ongoing communication to patient involves clear instructions and attention
to your patient’s comfort. Demonstrate a Professional manner throughout Examination method is structured and performed fluently and in a
logical order.
You should ask your patient to sit upright, and examine the neck from behind.
Start by examining for lymphadenopathy beneath the mandible, in the anterior and posterior triangles of the neck and the supraclavicular fossae.
Palpate for any anterior neck swelling. If swelling is present ask your patient to swallow. If you are palpating the thyroid gland this should elevate when your patient swallows.
If you suspect a thyroid swelling try to ascertain whether the swelling is soft or firm, and whether there are any palpable nodules, either single or multiple.
Auscultate for bruits (which can be present in Grave’s Disease).
Consider systemic signs of thyroid disease:
Tachycardia Tremor Eye signs- lid lag, exophthalmos, lid retraction Reflexes – brisk in hyperthyroidism
Finish the examination
Thank your patient
Explain examination findings to your patient or to the examiner as instructed.