Embed Size (px)
Citation preview
Barney S. Graham, MD, PhDAugust 8, 2014
Clinical Evaluation the HIV-1 CD4 Binding Site-Specific Monoclonal
Antibody VRC01
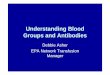
Structure-basedVaccine Design
Passive Transfer- Direct IgG- Gene vector (AAV)
An Integrated Approach to HIV Vaccine Development
CD4bs
VRC01
Immune pathways ofantibody evolution
10e8
MPER
PG9
V1V2 glycan Trimer11
PGT 128
V3 glycan
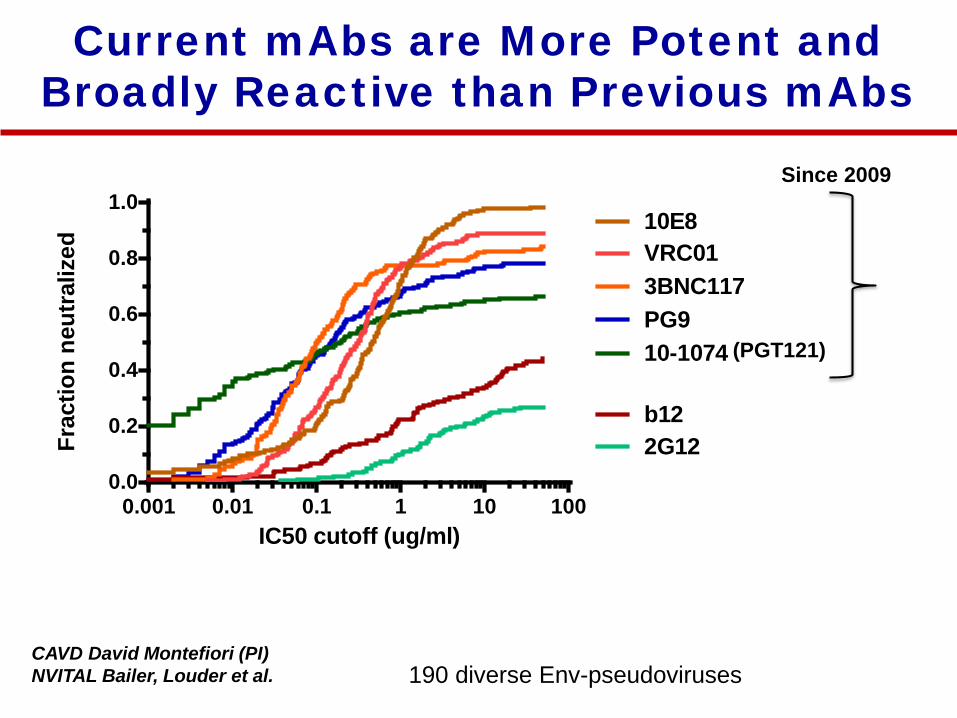
Current mAbs are More Potent andBroadly Reactive than Previous mAbs
CAVD David Montefiori (PI)NVITAL Bailer, Louder et al.
0.001 0.01 0.1 1 10 1000.0
0.2
0.4
0.6
0.8
1.0
IC50 cutoff (ug/ml)
Frac
tion
neut
raliz
ed
b12
VRC013BNC117
10E8
2G12
10-1074PG9
190 diverse Env-pseudoviruses
(PGT121)
Since 2009
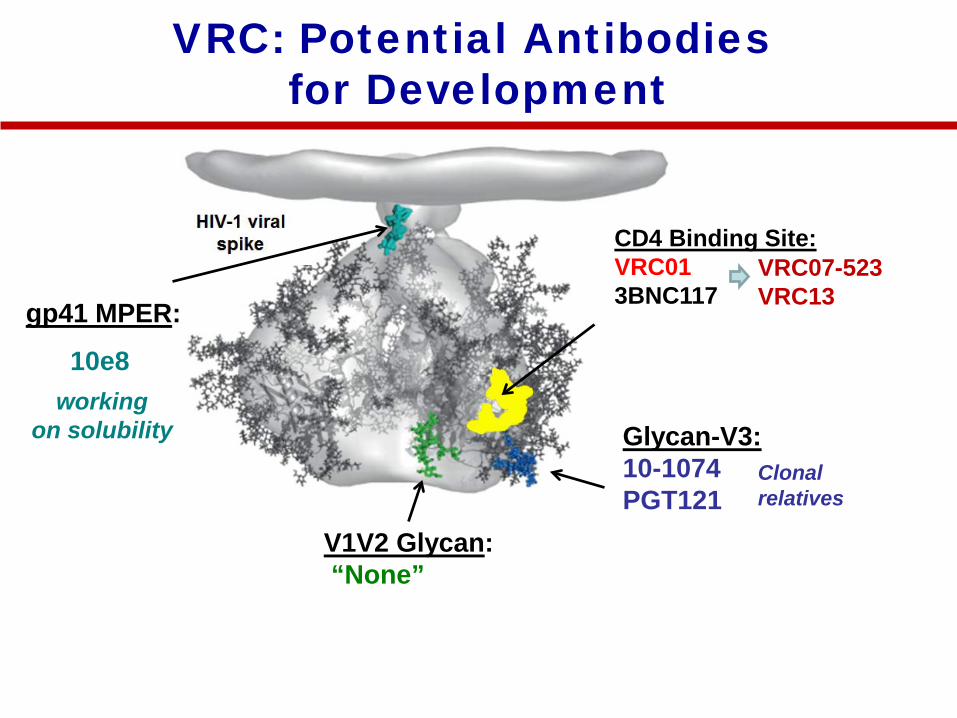
VRC: Potential Antibodies for Development
gp41 MPER:
10e8
V1V2 Glycan:“None”
CD4 Binding Site:VRC013BNC117
Glycan-V3:10-1074PGT121
VRC07-523VRC13
Clonalrelatives
working on solubility
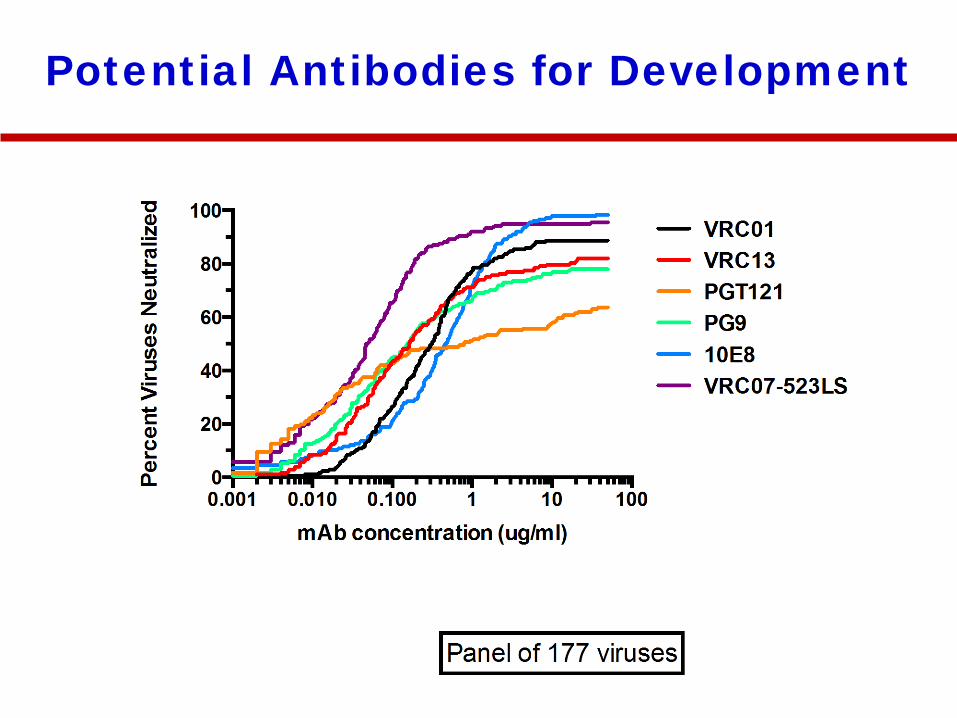
Potential Antibodies for Development
Clinical Use of HIV Antibodies
• Breastfeeding Infants • High risk young adults• Discordant couples• High risk MSM
• Acute affect on viremia• Treatment interruption/sparing• Impact on viral reservoir• Combined with ARV (functional cure)
Prevention Treatment
Maximize Coverage (breadth)Potent enough to work
Maximize potency Avoid escape
6
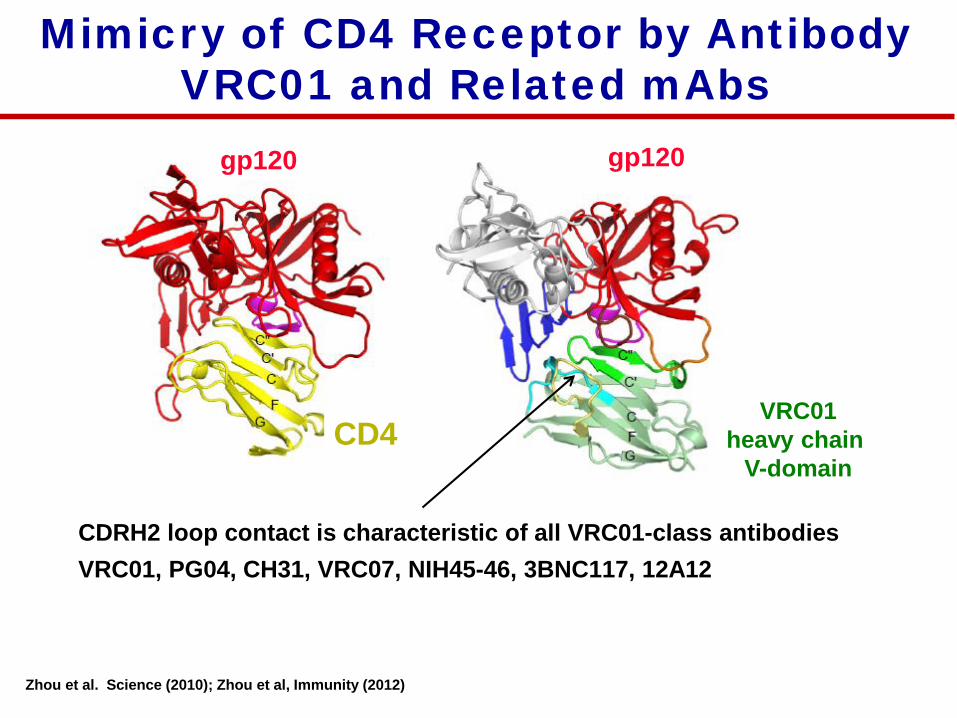
Mimicry of CD4 Receptor by Antibody VRC01 and Related mAbs
gp120
CD4VRC01
heavy chain V-domain
Zhou et al. Science (2010); Zhou et al, Immunity (2012)
gp120
CDRH2 loop contact is characteristic of all VRC01-class antibodiesVRC01, PG04, CH31, VRC07, NIH45-46, 3BNC117, 12A12
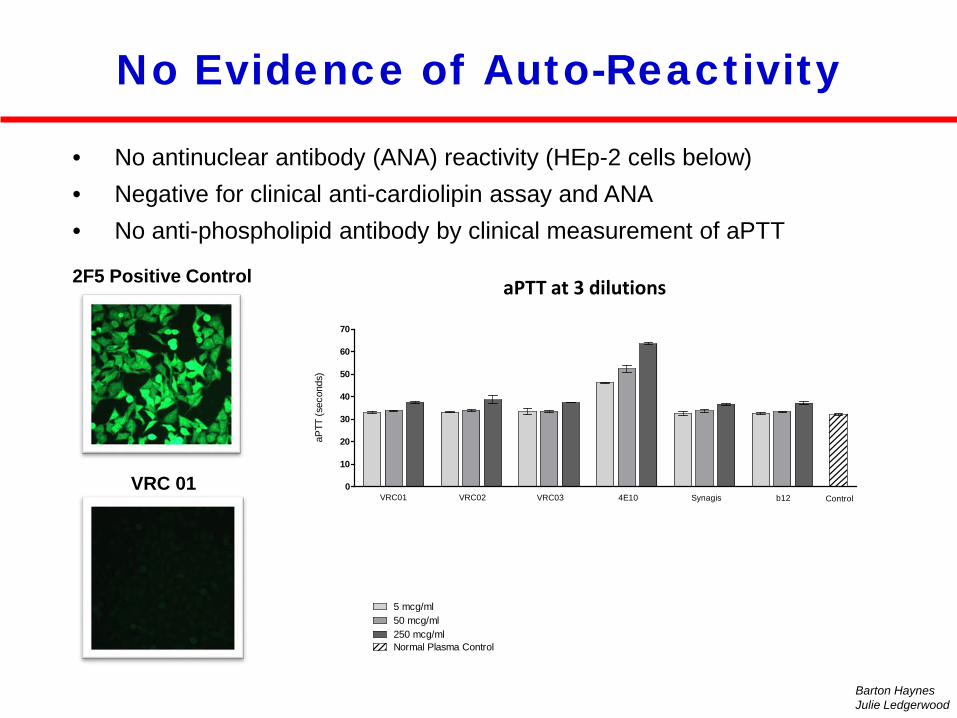
2F5 Positive Control
VRC 01
No Evidence of Auto-Reactivity
• No antinuclear antibody (ANA) reactivity (HEp-2 cells below)• Negative for clinical anti-cardiolipin assay and ANA• No anti-phospholipid antibody by clinical measurement of aPTT
Barton HaynesJulie Ledgerwood
Immediate aPTT
0
10
20
30
40
50
60
70
Normal Plasma Control
5 mcg/ml50 mcg/ml
VRC02 VRC03 4E10 Synagis b12 ControlVRC01
250 mcg/ml
aPTT
(sec
onds
)
aPTT at 3 dilutions
Number of Viruses Tested
A B C CRF01_AE CRF02_AG CRF07_BC D Other Total25 39 53 16 16 7 8 13 177
Other: AC = 4, ACD = 2, AD = 3 , CD = 3, G = 1
10E8
VRC01
3BNC11
7PG9
10-10
74
PGT121
0
20
40
60
80
100
Perc
ent V
iruse
s N
eutr
aliz
ed
ABCCRF01_AECRF02_AGCRF07_BCDOther
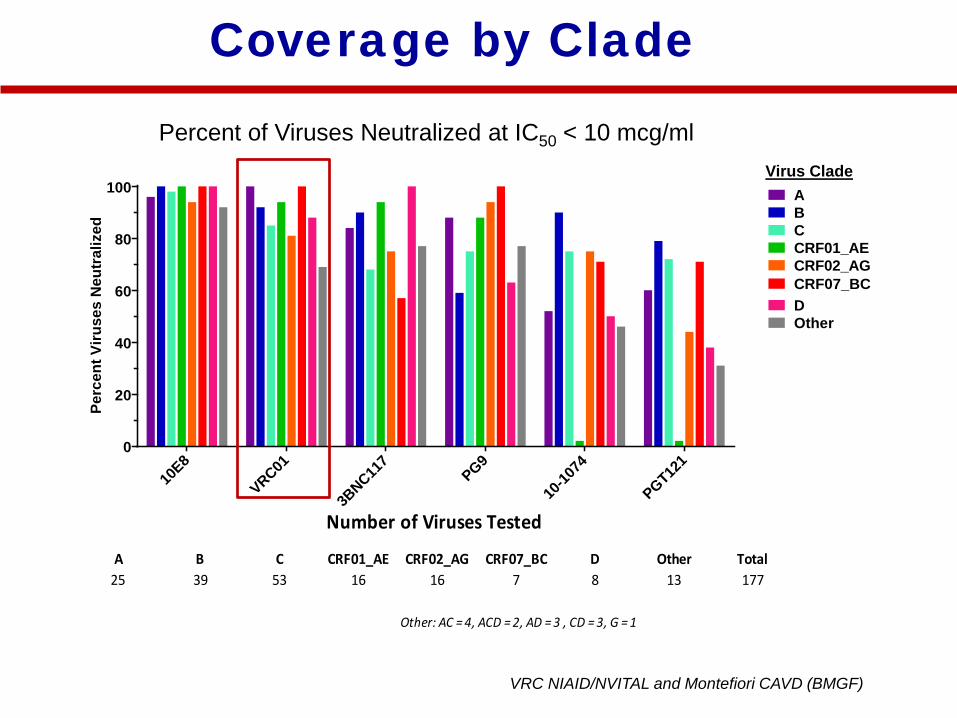
Coverage by Clade
VRC NIAID/NVITAL and Montefiori CAVD (BMGF)
Virus Clade
Percent of Viruses Neutralized at IC50 < 10 mcg/ml
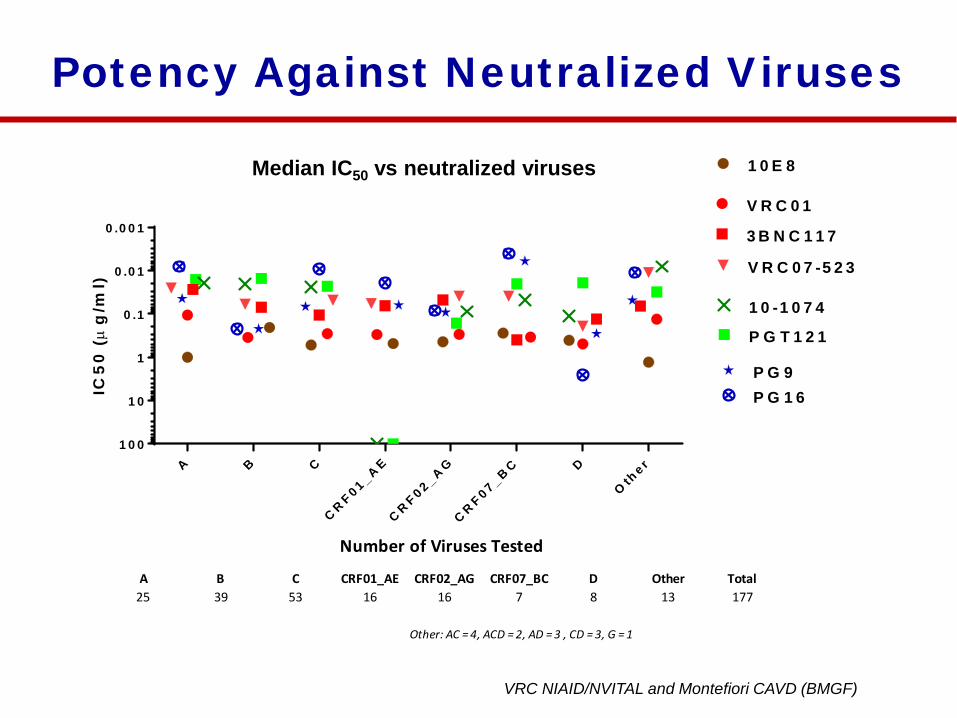
Number of Viruses Tested
A B C CRF01_AE CRF02_AG CRF07_BC D Other Total25 39 53 16 16 7 8 13 177
Other: AC = 4, ACD = 2, AD = 3 , CD = 3, G = 1
A B C
C R F 0 1 _A E
C R F 0 2 _A G
C R F 0 7 _B C D
Oth
e r
0 .0 0 1
0 .0 1
0 .1
1
1 0
1 0 0
IC5
0 (µ
g/m
l)
1 0 E 8
V R C 0 7 -5 2 3
V R C 0 1
3 B N C 1 1 7
1 0 -1 0 7 4
P G T 1 2 1
P G 9P G 1 6
Potency Against Neutralized Viruses
Median IC50 vs neutralized viruses
VRC NIAID/NVITAL and Montefiori CAVD (BMGF)
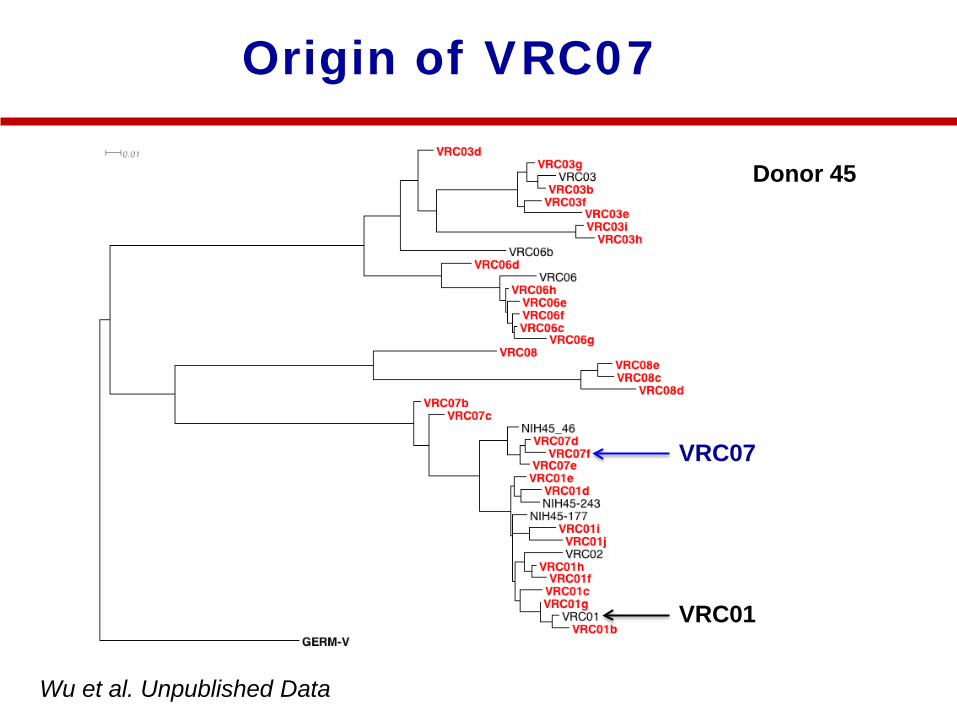
Origin of VRC07
Donor 45
VRC07
VRC01
Wu et al. Unpublished Data
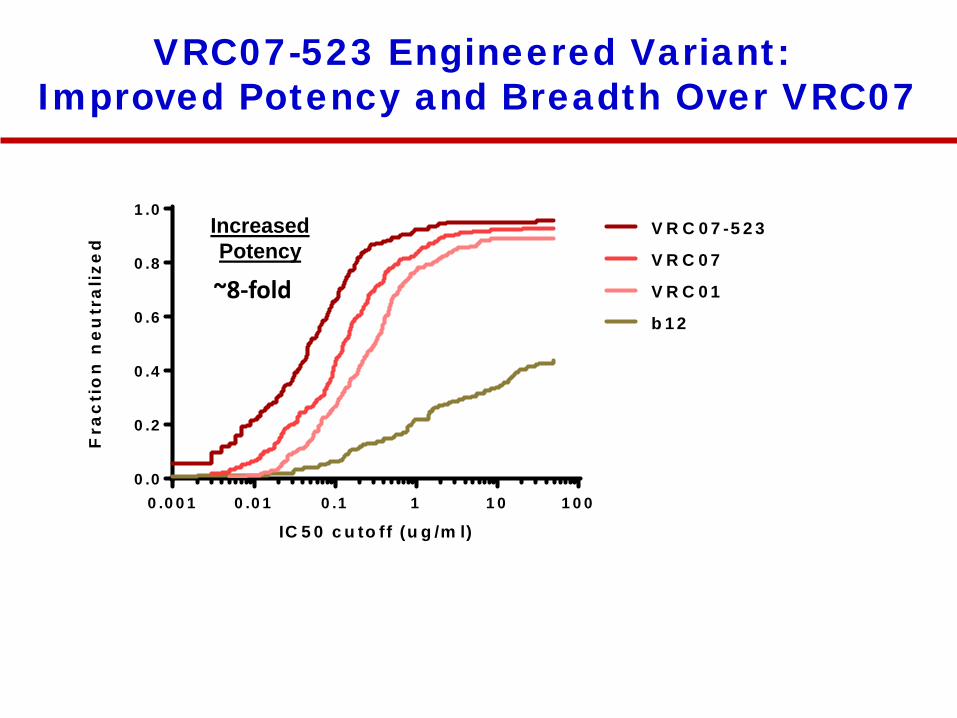
VRC07-523 Engineered Variant: Improved Potency and Breadth Over VRC07
0 .0 0 1 0 .0 1 0 .1 1 1 0 1 0 00 .0
0 .2
0 .4
0 .6
0 .8
1 .0
IC 5 0 c u to ff (u g /m l)
Fra
cti
on
ne
utr
ali
zed
b 1 2
V R C 0 1
V R C 0 7
V R C 0 7 -5 2 3
~8-fold
IncreasedPotency
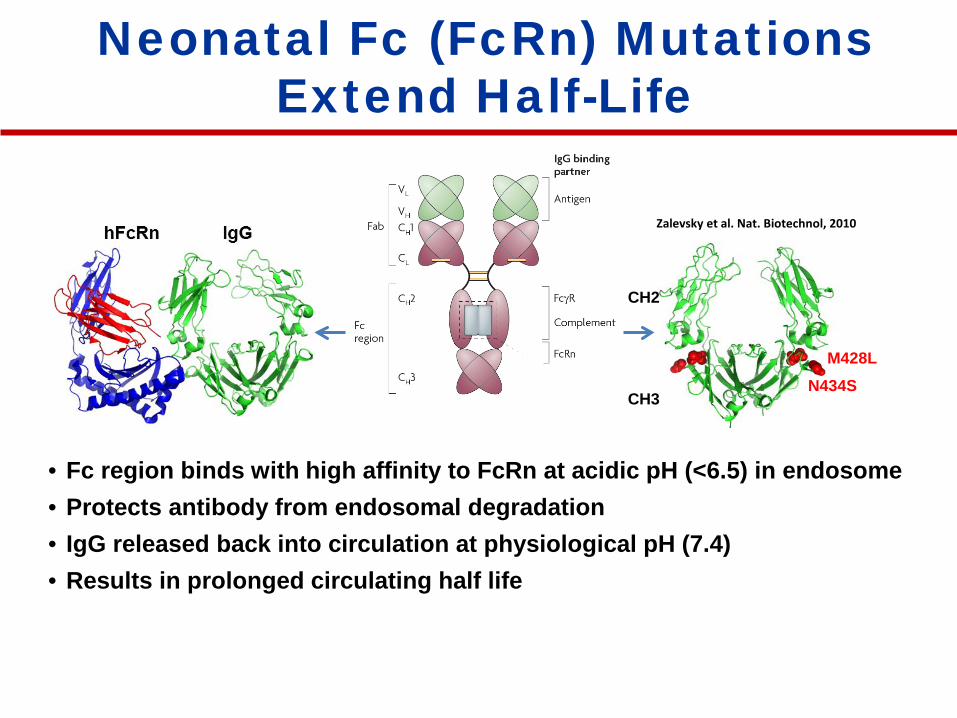
M428LN434S
CH2
CH3
• Fc region binds with high affinity to FcRn at acidic pH (<6.5) in endosome• Protects antibody from endosomal degradation • IgG released back into circulation at physiological pH (7.4)• Results in prolonged circulating half life
Neonatal Fc (FcRn) MutationsExtend Half-Life
Zalevsky et al. Nat. Biotechnol, 2010
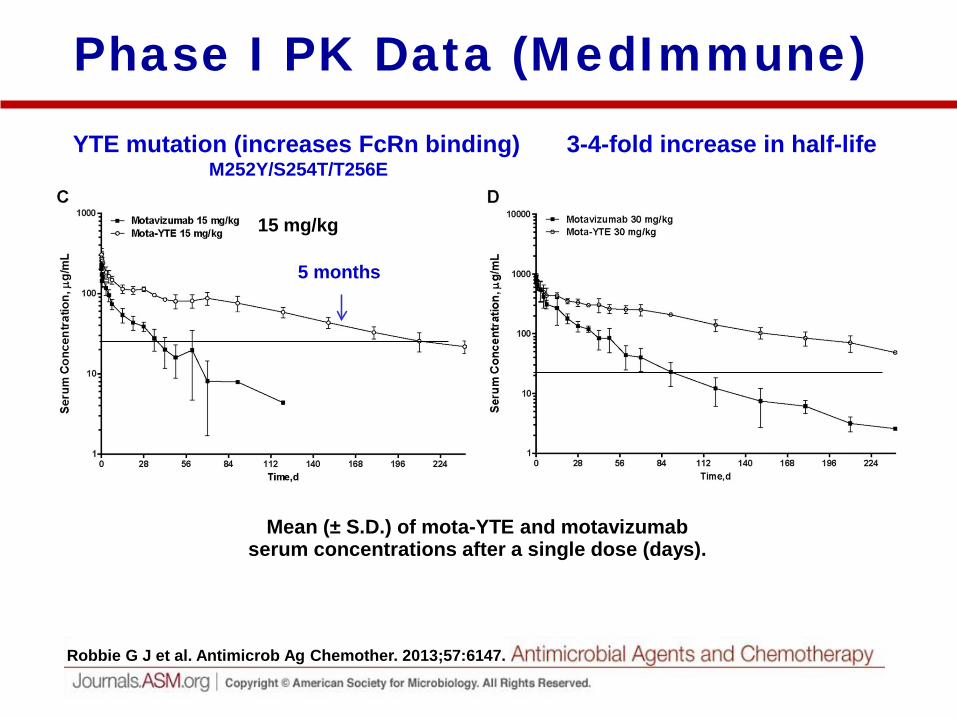
Mean (± S.D.) of mota-YTE and motavizumab serum concentrations after a single dose (days).
Robbie G J et al. Antimicrob Ag Chemother. 2013;57:6147.
Phase I PK Data (MedImmune) YTE mutation (increases FcRn binding)
M252Y/S254T/T256E3-4-fold increase in half-life
5 months
15 mg/kg
M428LN434S
CH2
CH3
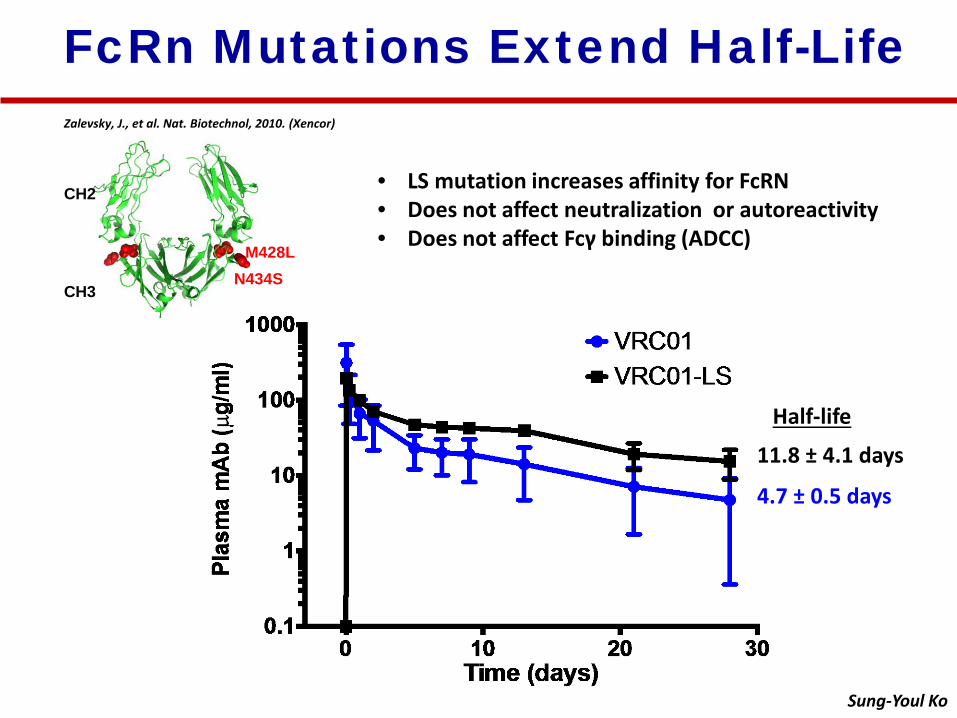
Zalevsky, J., et al. Nat. Biotechnol, 2010. (Xencor)
FcRn Mutations Extend Half-Life
• LS mutation increases affinity for FcRN• Does not affect neutralization or autoreactivity• Does not affect Fcγ binding (ADCC)
Sung-Youl Ko
Half-life
4.7 ± 0.5 days
11.8 ± 4.1 days
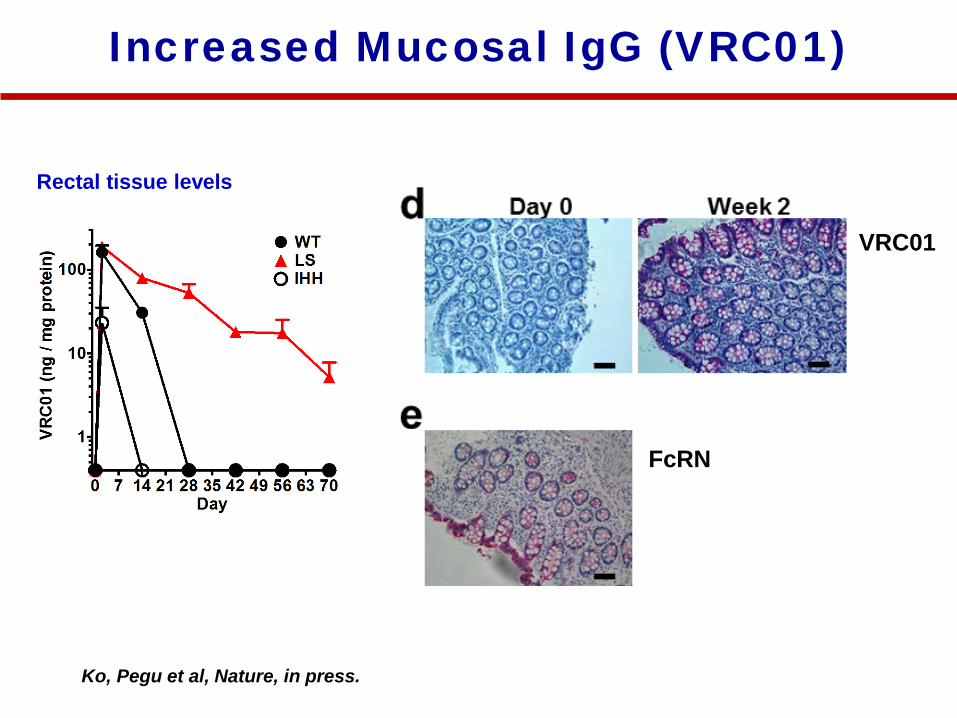
Increased Mucosal IgG (VRC01)
Rectal tissue levels
Ko, Pegu et al, Nature, in press.
FcRN
FcRNVRC01
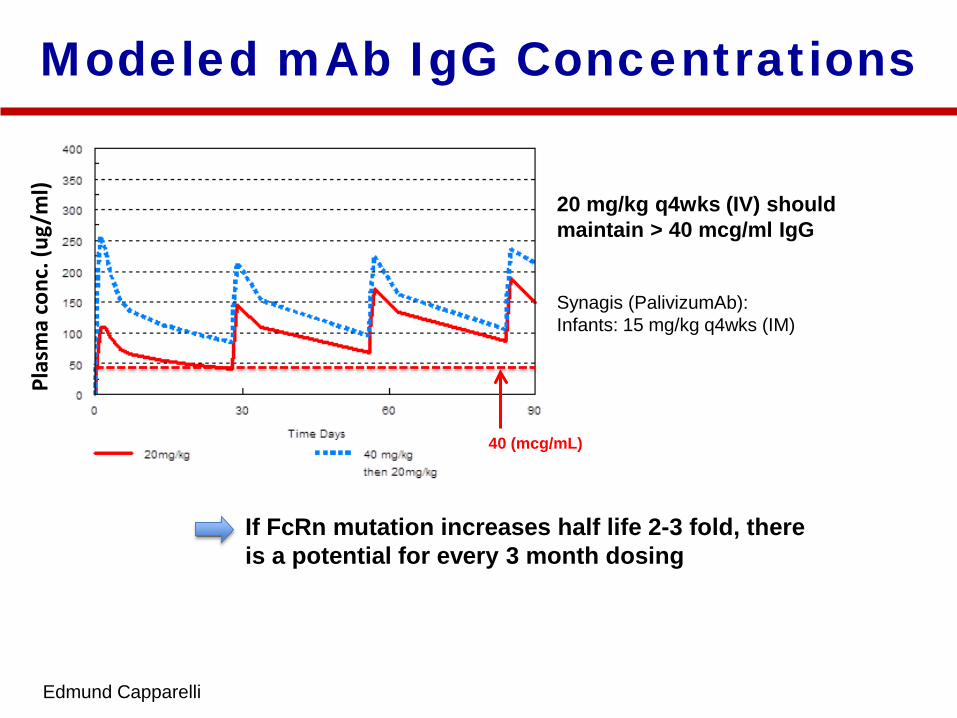
Modeled mAb IgG ConcentrationsPl
asm
a co
nc. (
ug/m
l)
Edmund Capparelli
20 mg/kg q4wks (IV) should maintain > 40 mcg/ml IgG
40 (mcg/mL)
Synagis (PalivizumAb): Infants: 15 mg/kg q4wks (IM)
If FcRn mutation increases half life 2-3 fold, there is a potential for every 3 month dosing
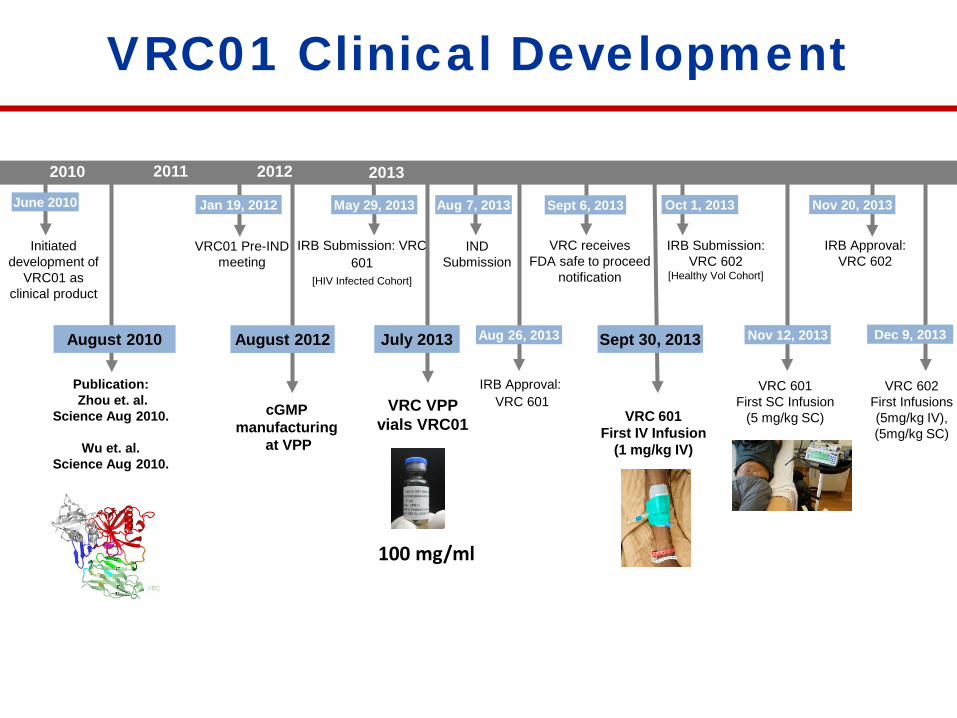
VRC01 Clinical Development
August 2010
IRB Approval: VRC 601
Aug 26, 2013
Jan 19, 2012 May 29, 2013 Aug 7, 2013
2011
VRC01 Pre-IND meeting
IRB Submission: VRC 601
[HIV Infected Cohort]
IND Submission
Publication:Zhou et. al.
Science Aug 2010.
Wu et. al. Science Aug 2010.
Sept 6, 2013
2012 20132010
VRC receives FDA safe to proceed
notification
Sept 30, 2013
VRC 601 First IV Infusion
(1 mg/kg IV)
Nov 12, 2013
VRC 601 First SC Infusion
(5 mg/kg SC)
Oct 1, 2013
IRB Submission:VRC 602
[Healthy Vol Cohort]
Nov 20, 2013
IRB Approval: VRC 602
August 2012
cGMPmanufacturing
at VPP
July 2013
VRC VPP vials VRC01
June 2010
Initiated development of
VRC01 as clinical product
Dec 9, 2013
VRC 602 First Infusions(5mg/kg IV), (5mg/kg SC)
100 mg/ml
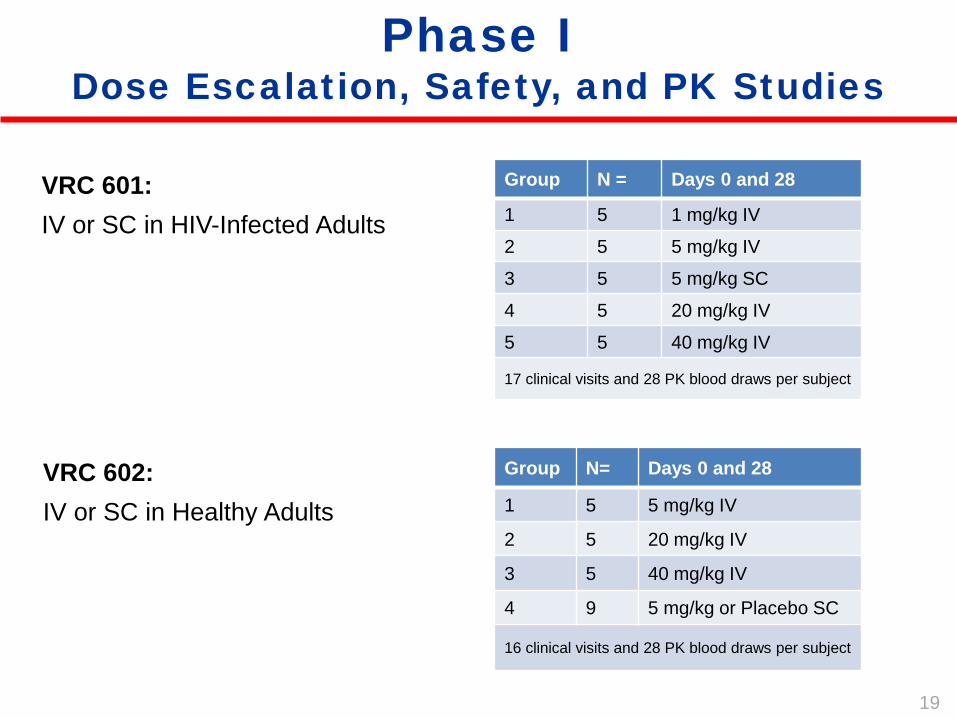
Phase IDose Escalation, Safety, and PK Studies
VRC 601: IV or SC in HIV-Infected Adults
Group N = Days 0 and 28
1 5 1 mg/kg IV
2 5 5 mg/kg IV
3 5 5 mg/kg SC
4 5 20 mg/kg IV
5 5 40 mg/kg IV
17 clinical visits and 28 PK blood draws per subject
Group N= Days 0 and 28
1 5 5 mg/kg IV
2 5 20 mg/kg IV
3 5 40 mg/kg IV
4 9 5 mg/kg or Placebo SC
16 clinical visits and 28 PK blood draws per subject
VRC 602: IV or SC in Healthy Adults
19
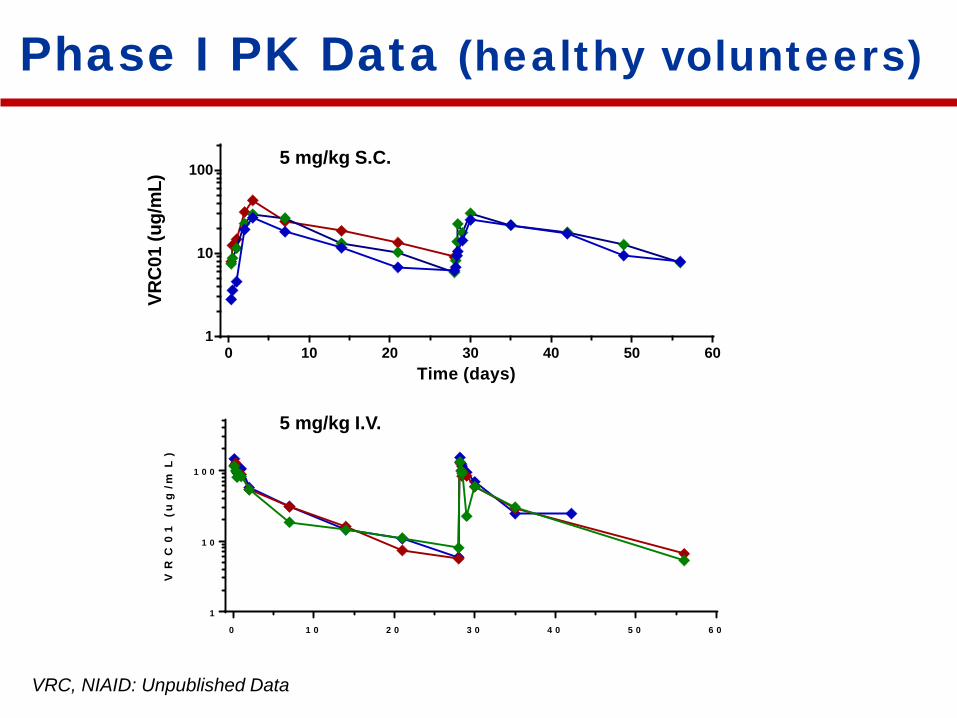
Phase I PK Data (healthy volunteers)
VRC, NIAID: Unpublished Data
0 1 0 2 0 3 0 4 0 5 0 6 0
1
1 0
1 0 0
VR
C0
1 (
ug
/mL
)
0 10 20 30 40 50 601
10
100
Time (days)
VRC0
1 (u
g/m
L)
5 mg/kg I.V.
5 mg/kg S.C.
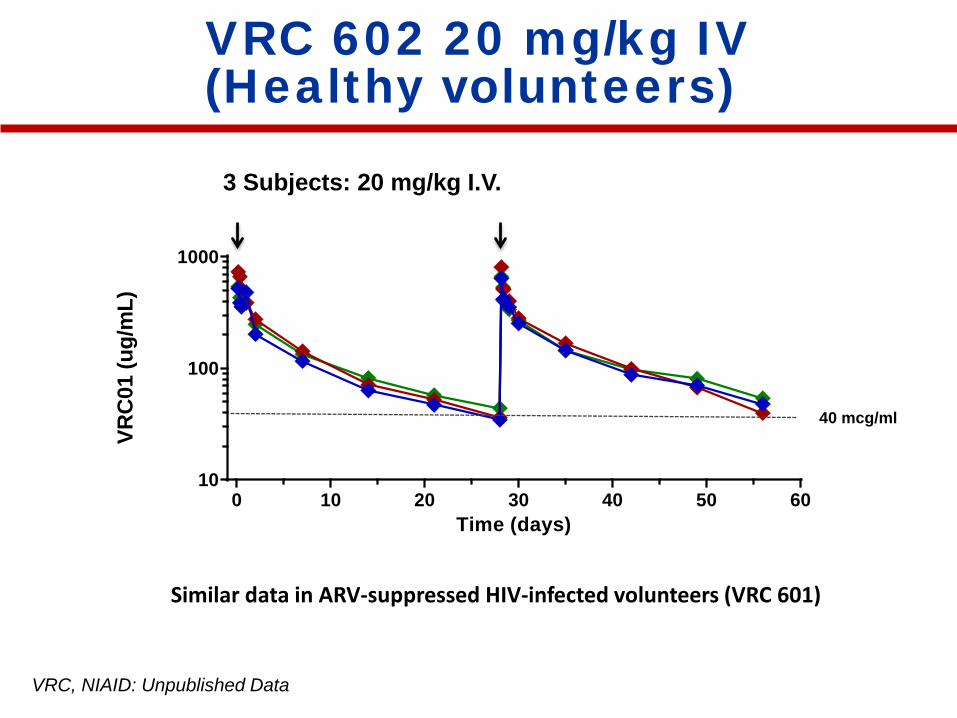
VRC 602 20 mg/kg IV(Healthy volunteers)
VRC, NIAID: Unpublished Data
0 10 20 30 40 50 6010
100
1000
Time (days)
VRC0
1 (u
g/m
L)
3 Subjects: 20 mg/kg I.V.
40 mcg/ml
Similar data in ARV-suppressed HIV-infected volunteers (VRC 601)
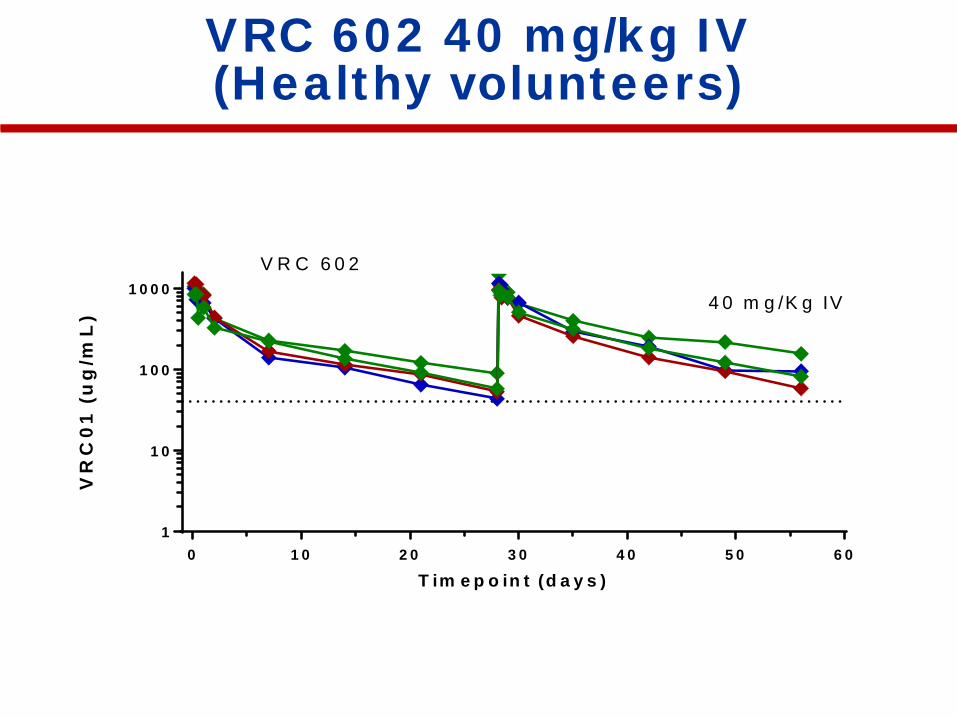
VRC 602 40 mg/kg IV(Healthy volunteers)
0 1 0 2 0 3 0 4 0 5 0 6 01
1 0
1 0 0
1 0 0 0
T im e p o in t (d a y s )
VR
C0
1 (
ug
/mL
) 4 0 m g /K g IV
V R C 6 0 2
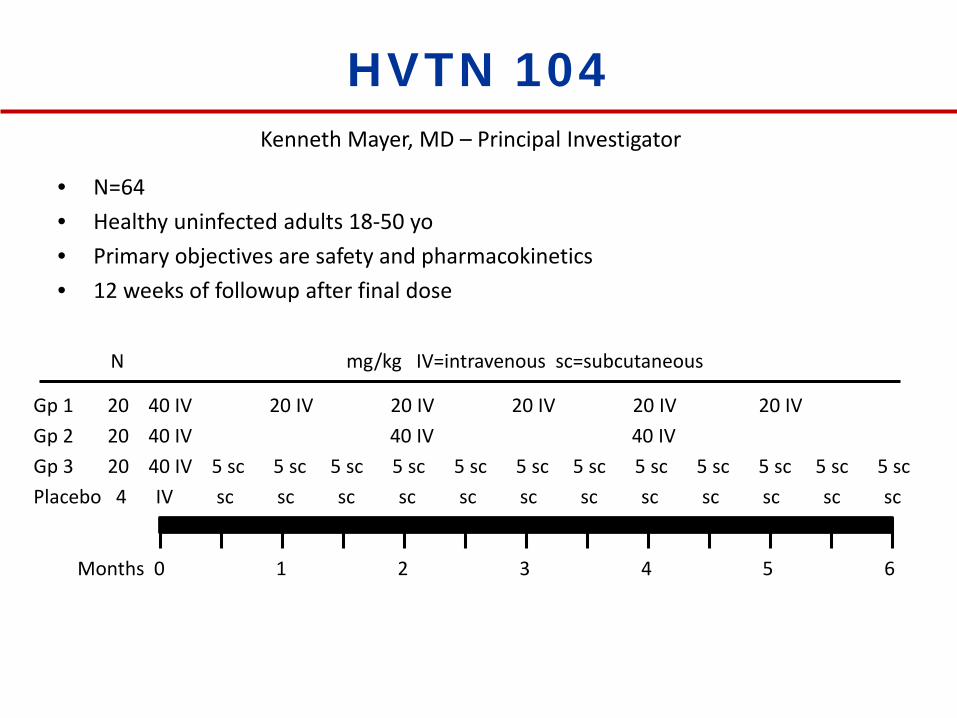
HVTN 104
• N=64• Healthy uninfected adults 18-50 yo• Primary objectives are safety and pharmacokinetics• 12 weeks of followup after final dose
Kenneth Mayer, MD – Principal Investigator
Gp 3 20 40 IV 5 sc 5 sc 5 sc 5 sc 5 sc 5 sc 5 sc 5 sc 5 sc 5 sc 5 sc 5 sc
Months 0 1 2 3 4 5 6
N mg/kg IV=intravenous sc=subcutaneous
Placebo 4 IV sc sc sc sc sc sc sc sc sc sc sc sc
Gp 2 20 40 IV 40 IV 40 IV Gp 1 20 40 IV 20 IV 20 IV 20 IV 20 IV 20 IV
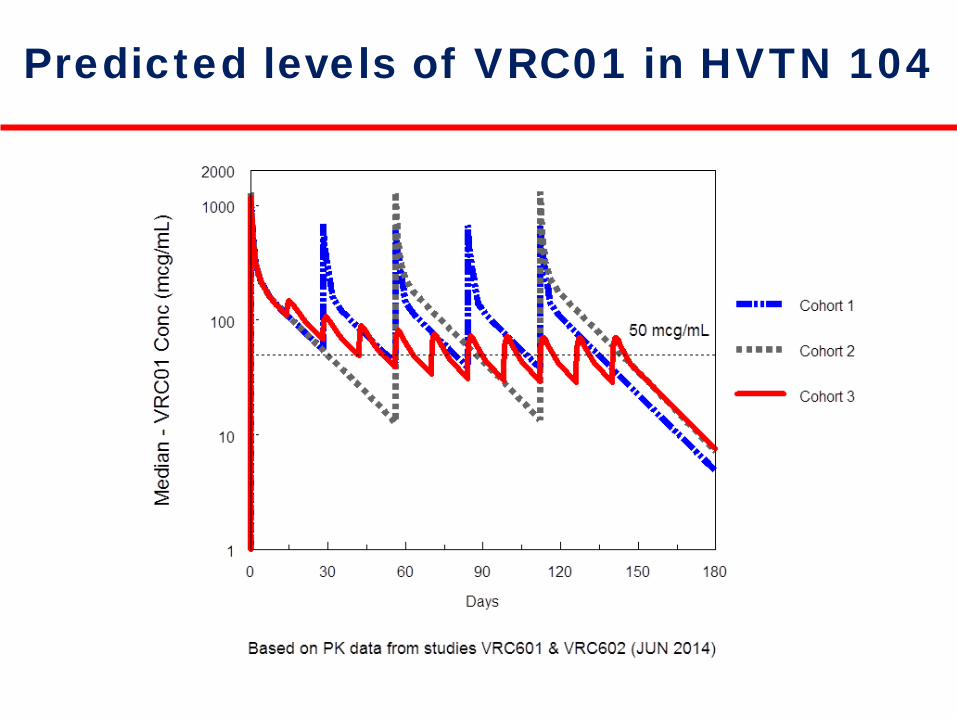
Predicted levels of VRC01 in HVTN 104
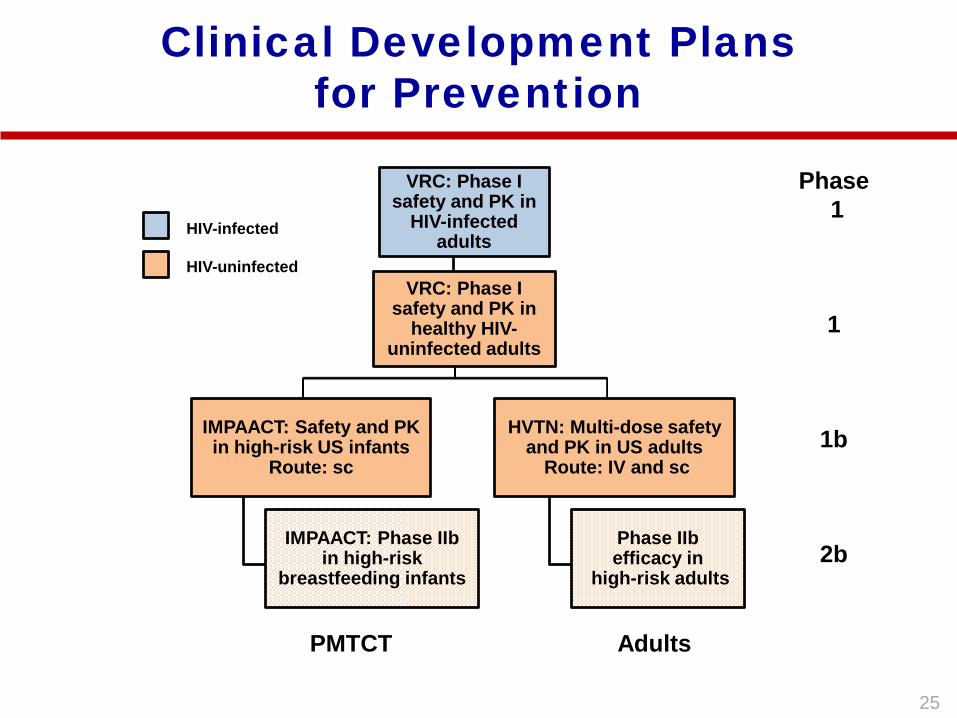
Clinical Development Plans for Prevention
VRC: Phase I safety and PK in
HIV-infected adults
VRC: Phase I safety and PK in
healthy HIV-uninfected adults
IMPAACT: Safety and PK in high-risk US infants
Route: sc
IMPAACT: Phase IIbin high-risk
breastfeeding infants
HVTN: Multi-dose safety and PK in US adults
Route: IV and sc
Phase IIbefficacy in
high-risk adults
HIV-uninfected
HIV-infected
AdultsPMTCT
Phase1
1
1b
2b
25
Proj
ecte
d Ph
ase
I and
II V
RC
01 C
linic
al T
rials
Year
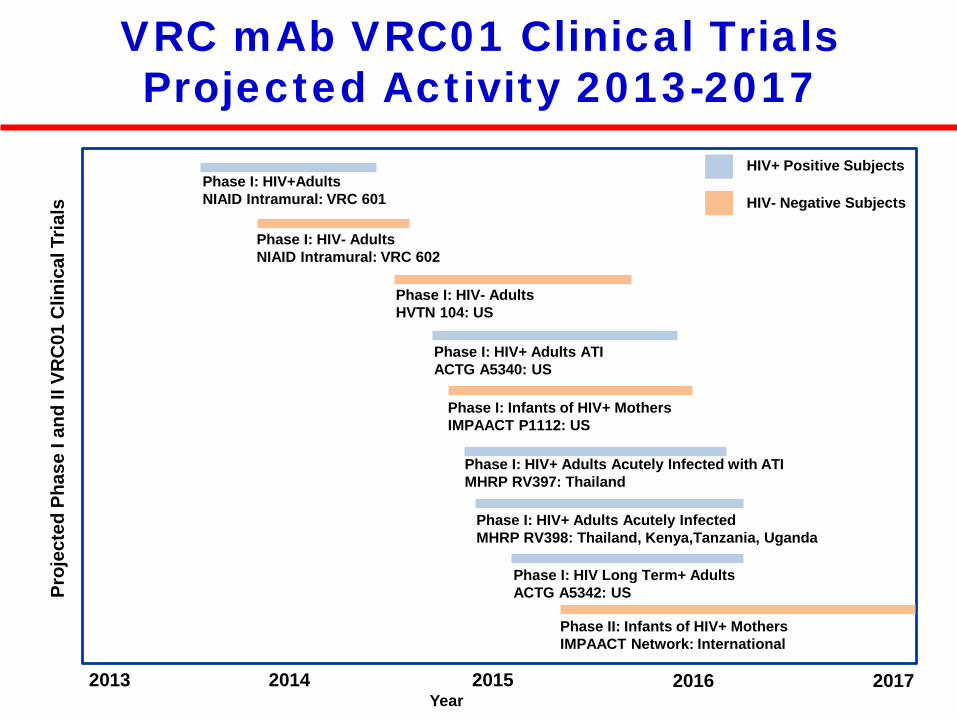
VRC mAb VRC01 Clinical TrialsProjected Activity 2013-2017
2013 2014
Phase I: HIV- AdultsHVTN 104: US
2015
Phase I: HIV+AdultsNIAID Intramural: VRC 601
Phase I: Infants of HIV+ Mothers IMPAACT P1112: US
Phase I: HIV- AdultsNIAID Intramural: VRC 602
Phase I: HIV+ Adults Acutely Infected with ATIMHRP RV397: Thailand
2016 2017
HIV- Negative Subjects
HIV+ Positive Subjects
Phase II: Infants of HIV+ MothersIMPAACT Network: International
Phase I: HIV+ Adults Acutely Infected MHRP RV398: Thailand, Kenya,Tanzania, Uganda
Phase I: HIV+ Adults ATIACTG A5340: US
Phase I: HIV Long Term+ AdultsACTG A5342: US
AcknowledgementsJulie LedgerwoodMary Enama Ingelise GordonEleanor WilsonLasonji HolmanSarah PlummerCynthia Starr HendelLaura NovikPamela CostnerKathy ZephirFloreliz MendozaJamie SaundersSandra SitarBrenda LarkinGalina YamshchikovOlga VasilenkoIris PittmanNina BerkowitzBrandon WilsonPernell WilliamsAlisha KabadiCarmencita Artis
Clinical Trials Program
27

AcknowledgmentsMascola labNicole Doria-RoseXueling WuCharlene WangRebecca LynchLillian TramSijy O’DellStephen SchmidtNancy LongoMark LouderKrisha McKee
CHAVI Mattia BonsignoriGeorgia TomarasTony MoodyDavid MontefioriJohn A CrumpSaidi H. KapigaSam E. Noel Myron CohenBart Haynes
Wyatt lab (Scripps)Yuxing LiFeng YuBimal Chakrabarti
(former) Nabel labZhi-yong YangLing XuLan WuXuejun ChenAmar PeguRebecca RudicellKevin SaundersSung-Youl KoWei ShiJeffrey Boyington
CTPJulie LedgerwoodMary EnamaIngelise GordonLaura Novik
Univ of WashingtonBill Schief
Koup labBob BailerLaurie Lamoreaux
IAVI and NACMelisa SimekPat FastLaura WalkerSanjay PhogatWayne KoffDennis Burton
Kwong labTongqing ZhouJiang ZhuLarry ShapiroBaoshan ZhangIvelin GeorgievYoung Do KwonGilad OfekYongping Yang
NISCHolly ColemanBrian SchmidtMorgan ParkJim Mullikin
HVTN & SCHARPScott Hammer (Columbia)Larry CoreyJulie McElrathSteve SelfPeter GilbertKen Mayer (Harvard)
Roederer labSteve PerfettoRichard NguyenDavid AmbrozakKathryn FouldsMitzi Donaldson
Rao LabJohn-Paul ToddAlida AultSaran BaoAlyse Zajac
DAIDSCarl DiffenbachAlan Fix
LIR, NIAIDMark ConnorsJinghe Huang
28