Embed Size (px)
Citation preview

Normal aNd abNormal developmeNt
Clinical evaluation of child development from birth to five yearsajay Sharma
tony o’Sullivan
Gillian baird
AbstractChildren’s developmental progress is a dynamic and transactional
process that involves multiple influences. developmental delays and
disorders often coexist with behavioural problems, and any comprehen-
sive clinical process should include a method for their identification. this
article emphasizes the essential competencies for clinical evaluation of
children’s development. It introduces a basic conceptual framework for
understanding children’s typical development and some generic features
that suggest abnormalities of development. typical and ‘red flag’ ages
in the children’s developmental progress are described in each domain.
Some key principles for taking history and making observations are high-
lighted. an outline of the current understanding of the evidence-based
investigations is provided. Some practical considerations for making
a developmental diagnosis, seeking further opinion and management
planning are discussed.
Keywords assessment; children; delay; development; disorder;
investigations
A comprehensive clinical evaluation of children with behavioural concerns includes consideration of physical, developmental, emotional, behavioural, social and environmental aspects. The differential diagnosis of a child’s behavioural signs and symptoms includes the possibility of organic and developmental disorders. Behavioural and emotional disorders are much more common in children with developmental disorders. While physical disease may be identified by laboratory tests, developmental markers help to identify the developmental disorders. The clinician’s toolkit must include a working knowledge of typical developmental ages or milestones and ‘redflag alerts’ – ages that indicate significant delay. Competency is needed to elicit
Ajay Sharma FRCPCH is Consultant Paediatrician (Community Child
Health) at Southwark Primary Care Trust, London. Conflicts of interest:
none declared.
Tony O’Sullivan FRCPCH is Consultant Paediatrician (Community Child
Health) at Lewisham Primary Care Trust, London. Conflicts of interest:
none declared.
Gillian Baird FRCPCH is Consultant Paediatrician and Honorary Professor
in Paediatric Neurodisability at Guy’s and St Thomas’ NHS Trust,
London. Conflicts of interest: none declared.
pSYCHIatrY 7:6 23
relevant developmental history, make observations and assess a child’s development, undertake relevant physical examination and investigations and access local services for further assessment. A close working relationship is therefore essential between the child development team, the hospital paediatric services and the child and adolescent mental health services (CAMHS).
Child development
Child development is a dynamic process shaped by a complex interplay between genetic factors and environmental factors, such as antenatal maternal health (including fetal exposure to toxins), in utero conditions, the birth process, nutrition, the economic and social conditions facing the family, and family interpersonal behaviour. A developing child is transformed from a wholly dependent and reactive infant into a proactive and relatively independent child at school entry: mobile, dexterous, communicative, sociable and able to look after her/his basic needs. The sequences of development are similar in most children and the developmental milestones are useful markers to observe the rate of development. But there is enormous variation in both the rate and the pattern of normal development.
Warning signs of abnormal developmentA sound knowledge of typical child development makes it possible to recognize when development is going wrong. It is worth considering the common presentations, developmental red flags, and less common but important scenarios: • delayed rate of development beyond accepted normal range of
variation in one or more developmental domains (e.g. mouthing beyond the second year, and echolalia (repetitive imitation of speech) still present by 3 years)
• absolute failure to develop skills (e.g. no canonical babble (multisyllable babble with intonation) by 10 months)
• disordered developmental sequence (e.g. hyperlexia (advanced reading) coexisting with delayed language)
• motor asymmetry in hand use or walking • developmental regression – loss/plateauing of skills.
The developmental examination
History-takingObtaining a good history is the most useful aspect of developmental assessment in terms of establishing any diagnosis, causative and associated conditions. A history should cover the family history, social and family environment, and the pre, peri and postnatal history. A clinical session starts with enquiring into the parents’ or other caregivers’ concerns. This proactive eliciting of concerns, beginning with the broad areas of function, guides the clinician in focusing on areas for further elaboration through history and examination. Gathering of information from others who know the child (e.g. teachers, healthcare staff) is important in eliciting pervasiveness of concern.
Parents used to be perceived as not particularly good informants of their children’s development, but this was partly a result of asking too detailed questions about the age of acquisition of particular skills. Asking openended questions and then requesting examples elicits the most reliable history. All parents are very good at remembering whether or not they
5 © 2008 elsevier ltd. all rights reserved.

Normal aNd abNormal developmeNt
had concerns and, if so, what those concerns were. They are particularly good at observing current behaviour if the right questions are asked. Parents’ interpretation of what their child does may be incorrect (e.g. ‘he understands everything I say’) but their observations are usually accurate (e.g. ‘he will fetch his shoes only if they are visible’). Parents can be helped in remembering examples of developmental achievements by focusing the enquiry around transition points such as starting at the nursery or the school or other significant events such as birthdays and house moves.
The assessor should ask for the parents’ view of the cause of any developmental problem. If the child has a development disorder, reassuring the parents about unwarranted concerns that they may have been responsible (e.g. a belief that autism could be caused by the mother going out to work, or being depressed) can reduce or remove their guilt. It is particularly important that developmental problems are not wrongly attributed to causes that are plausible but improbable, such as MMR immunization or obstetric intervention. A traumatic event, such as the umbilical cord around the neck of the child at birth or a forceps delivery, alone is an unlikely aetiology of a neurodevelopmental disorder. Nevertheless, it is valuable to establish, from independent enquiry, the reason for obstetric intervention (e.g. fetal distress), the condition of the baby at birth (e.g. Apgar score<5 at 5 or 10 minutes), and any history suggestive of neonatal encephalopathy (e.g. neonatal fits). The child’s current general health and a history of serious illnesses may be relevant to understanding current abnormalities of behaviour or learning.
Developmental differencesDevelopmental differences exist between boys and girls (e.g. boys tend to lag behind girls in language). Boys are, on average, 1 month delayed in early language development compared to girls, but the difference accounts for less than 2% of the variation within the sexes and across ages. Gestational age should be considered when seeing a child under the age of 24 months, and correction should be made when assessing ageappropriate attainments, especially in the first postnatal year.
Observation and interactive assessment
The most meaningful and valid ascertainment of a child’s abilities is obtained by combining observations made in a freeplay and interactive session with information from a structured and relatively distractionfree session using developmental domainspecific material. Observations should also include the child’s social awareness, interests, attention, anxiety, their initiating and responding to interactions and any repetitive movements or behaviours. Any change in function and behaviour with increasing task complexity, such as changing from nonverbal to languagebased activity, and over time should be noted. The child’s inability to organize the environment and generate ideas on their own is a significant finding and may not be noticed if an adult is too helpful. One of the cardinal rules of developmental assessment is to look not only at what the child does, but also how he or she does it. The quality of response should therefore be monitored as well as the actual achievement. A range of standardized assessments is available to help gather detailed normative information for diagnostic or monitoring purposes. Some developmental assessment
pSYCHIatrY 7:6 23
schemes are practical, taking 15–20 minutes, and are easy to learn, although each has drawbacks as well as strengths.
A suitable selection of toys should be made available before meeting the family and interacting with the child. These should be appropriate for the age of the child and the domains of development to be assessed; for example: • copying behaviour (bell) and understanding of cause and
effect (popup animals toy) • definition by use (cup/spoon, doll/brush) and symbolic
understanding (doll/teddy/teaset) • fine motor/eye–hand (bricks, crayons/pencil/paper, soft ball,
form boards, puzzles) • language and play (books with single pictures and stories, range
of everyday toy objects, large and miniature world toys).
Developmental domains
Developmental milestones or norms are a way of describing development in a sequential manner. Delays in some developmental sequences may indicate an underlying neurological, visual or hearing problem that requires an early referral for further assessment. These are indicated below as ‘red flag’ ages. Children with moderate or severe developmental delay, plateauing or regression of development will also require further assessment and investigations.
Gross motorDelay in achievement of the gross motor milestones (Table 1) may be an indicator of neurological abnormalities and is sometimes associated with a global developmental delay. Although the correlation between gross motor skills and global developmental level is weak, there is usually an impact on skills that depend on an intact motor system for their expression. Developmental assessment involves establishing the child’s progress in the sequence of development, the style of learning, behaviours that interfere with learning (e.g. avoidance), any sensory sensitivities or impairments, and a qualitative description of the child’s motor competences. Clinical interpretation requires combining this information with the findings of physical examination.
Visual behaviour, eye–hand coordination and problem solvingProgressive coordination of maturing vision with head, body and fine motor movements and an increasing ability to comprehend and solve problems can be observed through creating a range of
Gross motor milestones
Developmental milestone Mean age
(months)
Limit age, red
flag (months)
Hands open most of the time
(not fisted)
3 4
Good head control when sitting:
no head lag when pulled to sit
4 6
Sits independently 7–8 10
Walks alone 11–13 18
Table 1
6 © 2008 elsevier ltd. all rights reserved.

Normal aNd abNormal developmeNt
test situations such as manipulation and use of pellet, rings, bell, cubes, crayon/pencil, form boards or puzzles. The use of many such interesting and nonthreatening test situations also helps to tease out the relative contributions of experience, emotional factors, and motor and cognitive abilities. Children’s achievements in this domain represent the precursor to later nonverbal problemsolving abilities, correlate well with overall intellectual ability and may provide early markers for learning, psychological and psychiatric disorders.
Coordinated eye movements and eye–head coordination: the earliest developmental sequence starts with fixing gaze on the mother’s face, then to following a face with eyes only, and then being able to coordinate eye–head movements to turn head to follow visually (Table 2). Any abnormality of early visual behaviour should prompt an early referral for ophthalmological assessment.
Eye–hand coordination: in this developmental sequence the infant shows visual awareness of hands and becomes increasingly refined in combining vision with hand movements for reaching, grasping, exploring and releasing objects (Table 3).
Object concepts and relationships: this developmental sequence reflects infants’ growing understanding of the nature of objects, their relatedness to each other and in space (visuospatial) combined with a refined grasp and release ability (Table 4).
Copying cube models: this sequence shows children’s desire and ability to copy from models (combining the processes of encoding, decoding and executing) – moving on from vertical alignment to horizontal alignment to making two and threedimensional models (Table 5).
Drawing: children initially start jabbing pencil on paper just as they relate any other two objects together. This is followed by their interest in making a mark on the paper and then making vigorous uncontrolled scribble. By the end of their second year they can do controlled circular scribble and soon imitate others’ hand movements to draw a line and later a circular shape before they are able to copy a predrawn circle or other shapes. Children gradually refine their grasp – 50% of children by the age of 3 years and 80% by 4 years have a good tripod grasp of a pencil (Table 6).
Language and communicationIdentification of language impairment needs to combine information from parents, and observations/assessment. Parents’ reporting of expressive language is improved by making lists of
Eye–head coordination milestones
Developmental milestone Limit age (months) Red flag
visually alert, orients to face 1 any delay
visually follows face 2 any delay
Coordinates eye movements
with head turning
3 any delay
Table 2
pSYCHIatrY 7:6 23
spoken words or phrases. As children have good understanding of daily family routines, their language comprehension is often overestimated by parents and healthcare professionals!
Infants show preference to the mother’s voice within the first few days of birth, make responsive ‘cooing’ sounds within the first few months and play ‘lap games’ by 6 months. At around 9 months the infant begins to combine vocalizations and gestures to convey wishes, feelings, purpose and experience to others. At this stage, some infants may imitate the sounds of certain oftenrepeated family words. This is followed by the development of speech and language understanding and expression with a considerable variation between children (Table 7).
Eye–hand coordination milestones
Developmental milestone Mean age
(months)
Holds objects briefly when placed in hands without
visual regard
3
visually examines own hand 4
reaches out with a two-handed scoop 5
reaches out and grasps objects on table surface
without a raking grasp
6
transfers from hand to hand 6
explores with index finger 6
picks up a pellet/raisin between thumb and finger 9
picks up a string between thumb and finger 10
Can release in a container 10
Has mature grasp 12
Has precise release – without pressing on surface 13
builds towers to 2 cubes 13
builds towers to three cubes 16
turns pages of a book one page at a time 24
Table 3
Object concepts and relationships milestones
Developmental milestone Mean age
(months)
permanence of object: looks for hidden object 8
‘Cast’: drops repeatedly – enjoys sound and attention 8
Cause and effect: presses or pushes to activate a toy 9
means–end relationship: pulls toy placed out of
reach with a string
9
relating two objects together 10
relating objects: enjoys putting things in and out of
container
10
Simple posting games: round shapes 12
matches simple shapes 16–18
matches three shapes with good ‘scanning’ 24
Table 4
7 © 2008 elsevier ltd. all rights reserved.

Normal aNd abNormal developmeNt
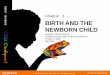
Play and social behaviourObservation of play offers a unique opportunity to look at a number of developmental sequences as they come together, including initiation of and response to social interaction and communication (using both verbal and nonverbal skills), imagination and the ability to generate varied ideas in play and to sustain these for a period of time while remaining alert to the social environment (Figure 1).
Development of attentionChildren pass through a number of different developmental stages as their attention, listening and selfregulatory skills improve. Below are the 6 main stages.
Stage 1 – children at this stage are very distractible. Their attention is held momentarily by whatever is the dominant stimulus (Year 1).
Stage 2 – at this stage children can concentrate on a task of their own choice. They have to ignore all other things in order to focus on this one task. Children are very resistant to interference by an adult (Year 2).
Stage 3 – by now, children are beginning to allow an adult to shift them from one task to another. Attention must still be fully gained before changing focus (Year 3: ‘singlechannel attention’).
Stage 4 – children now start to become able to control their own focus of attention. They move gradually towards needing
Cube model copying milestones
Developmental milestone Mean age (months)
Horizontal alignment of bricks 24
3-cube bridge 33
4-cube train with a chimney 39
3 steps with 6 cubes 48–54
4 steps with 10 cubes 60
Table 5
Drawing milestones
Developmental milestone Mean age (months)
Shape copying
makes a mark on paper 15
Scribble 18
Copies lines 24
Copies a circle 36 (90% by 24 months)
Copies a cross 42 (90% by 48 months)
Copies a square 48
Copies a triangle 60
Copies a diamond 66–72
Drawing a person
Figure with a head, other parts, no body 36 (80% by 45 months)
Figure with head, body, limbs 54
Table 6
pSYCHIatrY 7:6 23
to look at an adult only when the directions become difficult to understand (Year 4: early ‘integrated attention’).
Stage 5 – at this stage, children are usually entering school. They can now perform an activity while listening to the teacher giving directions (Year 5: mature integrated attention).
Stage 6 – this is a mature stage where attention skills are flexible and sustained for lengthy periods.
Cognitive developmentDevelopment of cognition, the progression from cause and effect and object permanence to increasingly conceptual and complex thinking is observed nonverbally, in the matching of shapes,
Language and communication milestones
Developmental milestone Mean age
(months)
Range
(months)
Comprehension/receptive language
Understands ‘no’/‘bye’ 7 6–9
recognizes own name 8 6–10
Understands familiar names 12 10–15
definition by use: using objects by 15
Giving objects on request by 15
points to body parts on self/carer 15 12–18
points to body parts on doll 18 15–21
Identifying objects on naming by 24
Follows a 2-step command 24 18–27
Functional understanding 30 21–33
Understands prepositions (in/on) 24 18–33
Understands prepositions (under) 30 24–39
Understands action words (e.g. eating,
sleeping)
by 36
Understands simple negatives 36 30–42
Understands comparatives 42 36–48
Follows 2 instructions (4 ideas) 42 36–48
Understands complex negatives 48 42–60
Follows 3 instructions (6 ideas) 54 48–66
Expressive language and non-verbal communication
Jargon 12 10–15
Syllabic and tuneful babble 8 6–9
pointing to demand 9 9–14
pointing to share interest 10 9–14
one word 12 10–18
2–6 words 15 12–21
7–20 words 21 18–24
50+ words 24 18–27
2 words joining 24 18–30
200+ words 30 24–36
3–4 words joining 30 25–36
Speech usually understandable 30 30–42
Question words 36 30–42
pronouns 42 36–48
Uses conjunctions (and, but) 48 36–54
Sentences of 5+ words 48 36–54
Complex explanations and sequences 54 48–66
Table 7
8 © 2008 elsevier ltd. all rights reserved.

Normal aNd abNormal developmeNt
Developmental sequences involved in play
Cognitive play sequence
Social play sequence
Object oriented
exploratory play
(maturing eye–hand
co-ordination and
object concepts)
18 months9 months
Functional use of real
objects on self and
others (e.g. spoon,
brush)
24–30 months
Symbolic use of toys
(e.g. toy, tea set, doll)
3–4 years
Pretend or imaginative
play
6–12 months
Social anticipation
Lap games
(e.g. peek-a-boo,
pat-a-cake)
4–5 weeks
Social smile
(90% by 6 weeks)
10–15 months
Joint attention
Points to show
3–3.5 years
Social imitative play
(e.g. role play)
Figure 1
patterns and pictures (deliberate rather than trial and error), and verbally and socially in the development of conceptual vocabulary – which toys go together for a particular attribute or attributes and in the number of ideas shown in play. Many children with significant global developmental delay or with severe delay or abnormality in one particular domain have longterm cognitive and functional impairments.
Significant developmental delayThe following is a guide to significant delay at varying ages. Moderate delay occurs approximately when the age equivalent for achieved milestones is between twothirds and half of chronological age (CA), and severe delay occurs when milestones are equivalent to 50% or less of CA (allowing for prematurity up to 2 years). These examples describe the ages commonly seen at referral for developmental concerns:
At 8 months: • moderate delay – developmentally 4–5 months (e.g. not sit
ting without support, not rolling, no singlesyllable babble) • severe delay – developmentally less than 4 months (e.g. not
lifting head).
At 2 years: • moderate delay – developmentally 12–18 months (e.g. less
than 10 words and not following simple commands) • severe delay – developmentally less than 12 months (e.g.
no single words, not walking, no functional play, no joint attention).
At 3 years and 6 months: • moderate delay – developmentally 21–28 months (e.g. just
linking words, less than 50 words, minimal concepts, cannot draw circle)
pSYCHIatrY 7:6 23
• severe delay – developmentally less than 21 months (e.g. single words or less, simple commands, but no concepts).
Physical examination
The physical examination is generally left to the end of the assessment, as the child may become upset and this would interfere with a subsequent developmental examination. The following key guidelines should be observed.
Motor function – determine whether the child has a motor disorder or if any delay is part of a global learning difficulty. Observe movement patterns and posture during the appointment and developmental examination, when the child is walking, speaking and handling material. This should give a good idea of the nature and extent of any motor problem. Formal examination of tone, reflexes and power is largely confirmatory.
Symmetry – compare the two sides of the body and determine the child’s hand preference. The motor skill, tone reflexes or limb size may be significantly asymmetrical, suggesting hemisphere dysfunction or other pathology.
Growth – measure the head circumference, height and weight and plot on a centile growth chart. Compare the consistency of the parameters and assess the growth rate. If concerned about the head size, it may be advisable to measure the parents’ head circumference (familial inheritance is the usual reason for an excessively large head, and there may be inherited reasons for microcephaly).
Sight – examination of the optic discs and fundi will usually not be possible, but it may be necessary to arrange this via the ophthalmologist or paediatrician (e.g. for septooptic dysplasia, raised intracranial pressure). All children with significant developmental disorders should be referred to ophthalmology.
Hearing would have been tested in the neonatal period but some sensorineural losses may be progressive and some children
9 © 2008 elsevier ltd. all rights reserved.

Normal aNd abNormal developmeNt
will have persistent middle ear problems. If there is any delay in language development and in all cases of significant learning or other developmental disorder, referral to audiology should be made.
Malformation – look for dysmorphic features and congenital malformations. They may suggest a particular syndrome or aetiology (e.g. fetal alcohol syndrome).
Skin – carefully examine the skin for pigmented and hypopigmented spots. Where there is significant developmental delay, and especially with epilepsy, a Wood’s ultraviolet light examination should be performed (for ashleaf skin patches in tuberous sclerosis) or arranged.
pSYCHIatrY 7:6 24
Planning investigations
The purpose of investigating the child with developmental disorder is to seek the cause of the disorder or to look for any associated or exacerbating conditions, such as hypothyroidism in Down’s syndrome or hearing loss coexisting with autism. When planning the investigations consider: • what is the likelihood of the condition under investigation
being present? • are there benefits from an early diagnosis: would it alter man
agement (e.g. by informing genetic advice), and what ‘bad outcomes’ could be prevented?
Investigation planning for developmental disorders
Context Recommended investigations Comments
Children with moderate or severe
global developmental delay
• Creatine kinase in boys aged less
than 3 years
• thyroid function tests irrespective
of neonatal screening
• Chromosomes for karyotype
• molecular analysis for fragile X
• mrI scan or Ct scan in more severe
mental retardation
• toxoplasma, rubella assay and Cmv
urine culture in children aged under
2 years
• Some consensus guidelines also recommend serum
lead, urate, U&e, ferritin and biotinidase
• Subtelomere FISH is receiving increasing support as
a routine investigation in children with generalized
learning difficulties/mental retardation (mr). Some
studies report such chromosome subtelomere
rearrangements occurring with a frequency of 7–10% in
children with mild-to-moderate mr and approximately
50% of cases are familial. positive results from this
investigation are 8 times more likely than fragile X in
some learning-difficulty populations
• plasma calcium and alkaline phosphatase
may help with diagnosis and management of
diGeorge syndrome, William’s syndrome, and
pseudohypoparathyroidism, and where motor delay is
due to vitamin d deficiency
associated abnormal head size
(micro- or macrocephaly), seizures,
focal neurological features, including
severe oromotor impairment and
speech abnormality
• mrI
• Karyotype and specific molecular
genetic tests (e.g. looking for 22q
deletion in oromotor and speech
dysfunction)
• Hb and FbC
• In some cases mrI studies can show a characteristic
signature for metabolic, neurocutaneous and
degenerative disorders and can even give enough
information to direct subsequent genetic testing
Specific history or examination
findings suggestive of poor nutrition
or neurometabolic disorders
• metabolic investigations – serum
amino acids, ammonia, vlCFa,
carnitine, homocysteine,
disialotransferrin
• Urine – organic acids, orotate,
GaGs, oligosaccharides
• Key pointers for metabolic disorders in the clinical
history include consanguinity, failure to thrive, and
episodic neurodevelopmental decompensations (often
during minor illnesses). examination findings may
include coarse facial features, or hepatosplenomegaly
Specific history or examination
findings suggestive of epilepsy or
specific behavioural phenotypes
(e.g. angelman syndrome)
• electroencephalography (eeG)
• referral to a paediatric neurologist/
consultation for planning further
appropriate investigations
• In angelman syndrome, characteristic eeG changes may
precede seizures. diagnosis is confirmed by deletion or
uniparental disomy on chromosome 15
• In many countries the human immunodeficiency
virus- linked infections are becoming an important
cause of regression with neurological and
neuropsychiatric manifestations usually presenting in
the first 3 years of life
regression with or without
associated features
Cmv, cytomegalovirus; FbC, full blood count; FISH, fluorescent in situ hybridization; GaGs, glycosaminoglycans; Hb, haemoglobin; U&e, urea and electrolytes; vlCFa, very long chain fatty acids.
Table 8
0 © 2008 elsevier ltd. all rights reserved.

Normal aNd abNormal developmeNt
• will the diagnosis give information of value to parents in their planning and coping?The answers to these questions may not always be clear but
their purpose is to focus investigation and to remain alert to the possibility of overinvestigating a child. However, there is also the danger of underinvestigating. If impairments are not detected early, other disabilities may result, which may be a source of resentment in parents when a late diagnosis is made (e.g. late diagnosis of hearing loss associated with failure to develop oral language adequately). Even more distressing is the scenario where a delay in genetic diagnosis may have led to the parents going ahead with a subsequent pregnancy, which they would have avoided had they known that their delayed child had an autosomal or Xlinked recessive condition. A balance needs to be struck between the two approaches – the conservative and the aggressive – when investigating the child with developmental delay. There is limited evidence basis for guidance and the suggested investigations depend on the type of developmental disorder and associated findings in history and examination. The diagnostic yield is highest for global developmental delay with associated history or physical abnormalities on examination and lowest for isolated developmental problems. For example, there are no routine investigations recommended for children with isolated language delay. However, specific enquiry should be made regarding concerns for hearing and vision, and in general there should be a low threshold for making hearing or vision checks. Table 8 shows an outline of the current evidencebased guidance for investigations.
Developmental diagnosis and management
• The outcome of the examination is a profile of the child’s developmental abilities and areas of difficulty, alongside the behavioural and mental health assessment. Consider how this profile reflects a child’s adaptation to the given biological and environmental constraints: repeated observations may be required for interpretation. A narrow focus on the child’s difficulties in one particular domain, without attention to other possible factors, may lead to a wrong conclusion such as diagnosing developmental delay in the presence of sensory impairment or poor social environment. An impulsive, anxious or a withdrawn child may underperform on certain developmental tasks, giving variability in results. The complexity and, at times, the uncertainty of the situation, must be acknowledged and shared with the carers. • The combined picture may point to a specific developmental delay or disorder (e.g. learning disability, autism). The clinician should be aware of the common behavioural phenotypes or seek appropriate advice.
pSYCHIatrY 7:6 24
• Functional difficulties may require referral for specialist assessments (e.g. speech and language therapy, occupational therapy, physiotherapy, or the community paediatrician) even where there is no specific diagnosis. • Teachers are often a good source of information for nursery/schoolage children, and should be informed regarding any concern or identified difficulties for the provision of additional educational help. Good interagency liaison is needed to address complex needs. • Concerns regarding a child’s protection or care may arise from combining multidisciplinary information from different settings. An early discussion with an experienced clinician and an interagency approach are essential for identification or prevention of potential risk to the child. • For many children, close links between CAMHS and the child development team help integrate the different aspects of their assessment and management, for example referral for language assessment. • Ongoing management may require shared care through partnership with one or more agencies. • A clear management plan should be included in the assessment report, incorporating referrals and further investigations; plan for who is to review the child and, where relevant, a named lead/key worker for the family. ◆
FuRTHER READInG
baron-Cohen S, Wheelwright S, Cox a, et al. the early identification
of autism: the checklist for autism in toddlers (CHat). J R Soc Med
2000; 93: 521–5.
bee H. the developing child. boston, USa: pearson, 2007.
Capute aJ, pasquale Ja. developmental disabilities in infancy and
childhood. baltimore, USa: paul H brooks, 1996.
egan dF. developmental examination of preschool children. oxford:
mac Keith press, 1990.
law J, ed. the early identification of language impairment in children.
london: Chapman Hall, 1992.
mcdonald l, rennie a, tolmie J, et al. Investigation of global
developmental delay. Arch Dis Child 2006; 91: 701–5.
Salt a, Gringras p, dorling J, Hartley l. developmental delay.
In: moyer va, elliott e, davis r, et al. eds. evidence based
paediatrics and child health. london: bmJ publishing Group, 2000.
Sheridan md. From birth to five years. (revised and updated by
Sharma a, Cockerill H). london: routledge, 2007.
Siegler r, deloache J, eisenberg N. How children develop. New York:
Worth, 2003.
1 © 2008 elsevier ltd. all rights reserved.