Embed Size (px)
Citation preview
Clinical Efficacy of Flossing Versus Useof Antimicrobial RinsesStefan Zimmer,* Claudia Kolbe,* Gerrit Kaiser,* Tracy Krage,* Michelle Ommerborn,*and Claudia Barthel*
Background: Dental floss is only used by a small part of thepopulation on a daily basis. Therefore, an easy, applicablealternative is needed. This alternative could be a mouthrinsewith antimicrobial activity for daily use. The aim of the presentstudy was to evaluate the efficacy of two mouthrinses in reduc-ing interdental plaque and gingivitis compared to dental floss.
Methods: A total of 156 healthy volunteers were randomlyassigned to the following groups: 1) toothbrushing and rinsing(0.06% chlorhexidine and 0.025% fluoride); 2) toothbrushingand rinsing (0.1% cetylpyridiniumchloride and 0.025% fluo-ride); 3) toothbrushing and flossing; and 4) toothbrushingonly (N = 39 subjects in each group). At baseline, the modifiedproximal plaque index (MPPI) and papillary bleeding index(PBI) were recorded. Thereafter, subjects had to brush in theusual manner during 8 weeks. Additionally, test groups hadto rinse once a day (groups 1 and 2: 30 seconds) or to floss(group 3). Eight weeks after baseline, indices were recordedagain and improvements were calculated. Analysis of vari-ance (ANOVA) and the Bonferroni test served for statisticalanalysis.
Results: After 8 weeks, reductions for all indices were foundin all groups (P <0.05). With respect to the MPPI, mouthrinsegroups performed better than the control and floss groups:1) 0.73; 2) 0.82; 3) 0.40; and 4) 0.32 (P <0.05). The PBIshowed no statistically significant difference between groups:1) 0.46; 2); 0.50; 3); 0.42; and 4) 0.37.
Conclusion: The results suggest that, in combination withtoothbrushing, daily use of the tested mouthrinses may resultin a higher interproximal plaque reduction than daily flossing.J Periodontol 2006;77:1380-1385.
KEY WORDS
Controlled clinical trials; mouthwash; random allocation;single-blind method.
For subjects without attachmentloss, clinical data show that dentalfloss, if properly and frequently
used on a regular basis, can be effectivein reducing interproximal gingivitis1
and preventing caries on proximal toothsurfaces.2 However, representative sur-veys indicate that dental floss is usedby only a small part of the population.For example, Christensen et al.3 re-ported that 11% of the adult Danishpopulation was using dental floss on adaily basis. The respective value forGermany was 14.3% as reported byStaehle and Kerschbaum.4 It was shownrecently that a power toothbrush withsonic action was more effective in re-ducing interproximal plaque than amanual brush in combination with den-tal floss.5 Therefore, using a sonic brushmay be an alternative to using a com-bination of a manual brush and dentalfloss. However, there is no solution forsubjects who reject using an electricbrush.
Therefore, it was the aim of the presentstudy to evaluate the efficacy of twomouthrinses with antimicrobial activityin reducing interdental plaque and gingi-vitis compared to the use of dental flossand a negative control. A supplementalgoal was to evaluate the overall plaque-reducing effect of the products.
MATERIALS AND METHODS
SubjectsOut of blood donors who visited theblood bank of the University Hospital,
* Department of Operative and Preventive Dentistry and Endodontics,Heinrich-Heine-University of Duesseldorf, Dusseldorf, Germany.
doi: 10.1902/jop.2006.050362
Volume 77 • Number 8
1380

Duesseldorf, Germany, in July and August 2004, 156subjects were selected in a screening examinationusing the following inclusion criteria: a papillarybleeding index (PBI)6 per tooth ‡0.5 and a modifiedproximal plaque index (MPPI)7,8 per tooth ‡1.5. Thesecriteria ensured that no subjects with good oralhygiene under normal conditions were included inthe study.
Subjects were excluded from the study if they worefixed orthodontic appliances or had any form of severeperiodontitis, long-term use of drugs with anti-inflam-matory effects within 1 month prior and/or duringthe study, removable dentures, <20 natural teeth orregularly used dental floss or antimicrobial mouth-rinses during the past 3 months. According to Lindheet al.,9 severe periodontitis was defined as the presenceof clinical attachment loss ‡5 mm in a minimum ofthree teeth. Subjects with any furcation involvementor pathological tooth mobility were also excluded. Fur-thermore, dentists, dental hygienists, dental assistants,and dental students were not included in the study.Smoking habits of subjects were recorded.
Study ProtocolThe study was conducted by a blinded operator in aparallel design. All examinations were performed byone single examiner (GK). The screening examinationwas followed by calculus removal in the lower frontteeth. By using the stratification by gender and PBI(PBI per tooth ‡0.5, <1.0, and ‡1.0), the 156 partici-pants were randomly assigned to four groups with 39subjects in each group: 1) toothbrushing and rinsing(0.06% chlorhexidine [CHX] and 0.025% fluoride assodium fluoride†); 2) toothbrushing and rinsing(0.1% cetylpyridiniumchloride [CPC] and 0.025%F- as NaF‡); 3) toothbrushing and flossing;§ and 4)toothbrushing only (control group). The assignmentof subjects to groups was performed by a person notinvolved in the examination (CK). In a box containing156 envelopes in four strata (three strata with 40 andone with 36), each participant had to draw one enve-lope containing the number of the attributed product.
The data of the screening examination served asthe baseline; thus, the MPPI, the Quigley-Hein plaqueindex (QHI),10 and the PBI were already recorded atthe screening examination. Four and 8 weeks afterbaseline, the indices were recorded again. Third mo-lars were excluded from the analysis. Side effects suchas discomfort in taste, discomfort in sensibility, gingi-val damage, gingival bleeding, staining of teeth andtongue, mouth burning, and white plaque on thetongue immediately after use were registered at thefinal examination.
To achieve standardized conditions, each subjectused the same toothpastei and a fresh toothbrush.¶
The toothpaste was silica-based with 1,350 ppm fluo-
ride as NaF, a pH of 7.0, and relative dentine abrasion(RDA) values of 50 to 60. It did not contain any antimi-crobial ingredient. The toothbrush had a flat trim with43 tufts and end-rounded nylon bristles. Before startingthe study, the intraexaminer reliability was tested byrepeated measurements of MPPI, QHI, and PBI andanalyzed by Cohen’s k test. The results were as fol-lows: MPPI = 0.86; QHI = 0.82; and PBI = 0.88.
Participants received brief instructions for the pro-cedure they had to perform in addition to using thetoothbrush, dental floss, and oral rinsing. The dentalfloss instruction was demonstrated with a plastic toothmodel and did not exceed 2 minutes. The subjectswere advised to brush their teeth in the usual manner.No instructions concerning brushing technique andbrushing time were given. After using the brush, thesubjects of the dental floss group had to apply the flossonce a day in all interproximal spaces before going tobed. The subjects of the mouthrinse groups had torinse once a day for 30 seconds with the assignedrinse after toothbrushing and before going to bed.To control the rinsing time, each subject was providedwith a digital stopwatch.
During the study period, the use of other than theattributed oral hygiene tools was strictly prohibited.Only the intentional use of a toothpick to remove im-pacted food was allowed. The subjects were requestednot to brush their teeth for at least 1 hour prior to thedental appointment. At the intermediate and finalexamination, the subjects were interviewed to deter-mined if they had performed the oral hygiene mea-sures as requested.
The study was approved by the ethics committee ofthe Medical Faculty, Heinrich-Heine-University. Allsubjects signed an informed consent form.
Data AnalysisData analysis was performed using a statistical pro-gram.# Means and standard deviations were calcu-lated. Comparisons between groups were performedwith analysis of variance (ANOVA) and the Bonferronitest. Changes between baseline, intermediate, andfinal examination were analyzed as well as the valuesat the three examinations. Side effects occurring dur-ing the study period were recorded using a question-naire and by a clinical examination (GK).
RESULTS
A total of 156 subjects (78 males and 78 females) fin-ished the study. The mean age was 31.7 years (range:20.0 to 64.4 years). With respect to age, no statistically
† Experimental mouthrinse, GlaxoSmithKline, Buhl, Germany.‡ Experimental mouthrinse, GlaxoSmithKline, Brentford, U.K.§ Odol med 3 dental floss, GlaxoSmithKline, Buhl, Germany.i Dr. Best Multi Aktiv, GlaxoSmithKline.¶ Dr. Best flex plus medium, GlaxoSmithKline.# SPSS 12.0, SPSS, Chicago, IL.
J Periodontol • August 2006 Zimmer, Kolbe, Kaiser, Krage, Ommerborn, Barthel
1381
significant difference was detected between groups(ANOVA and Bonferroni; P <0.05). After 4 and 8weeks, all subjects stated that they had performed theiroral hygiene measures as requested. There were 123non-smokers and 33 smokers. Group 2 (CPC/NaF:12 smokers) and group 3 (floss: 11 smokers) con-tained more smokers compared to group 1 (CHX/NaF: four smokers) and group 4 (control: six smokers).However, this difference failed to reach statistical sig-nificance in the x2 test (P = 0.076).
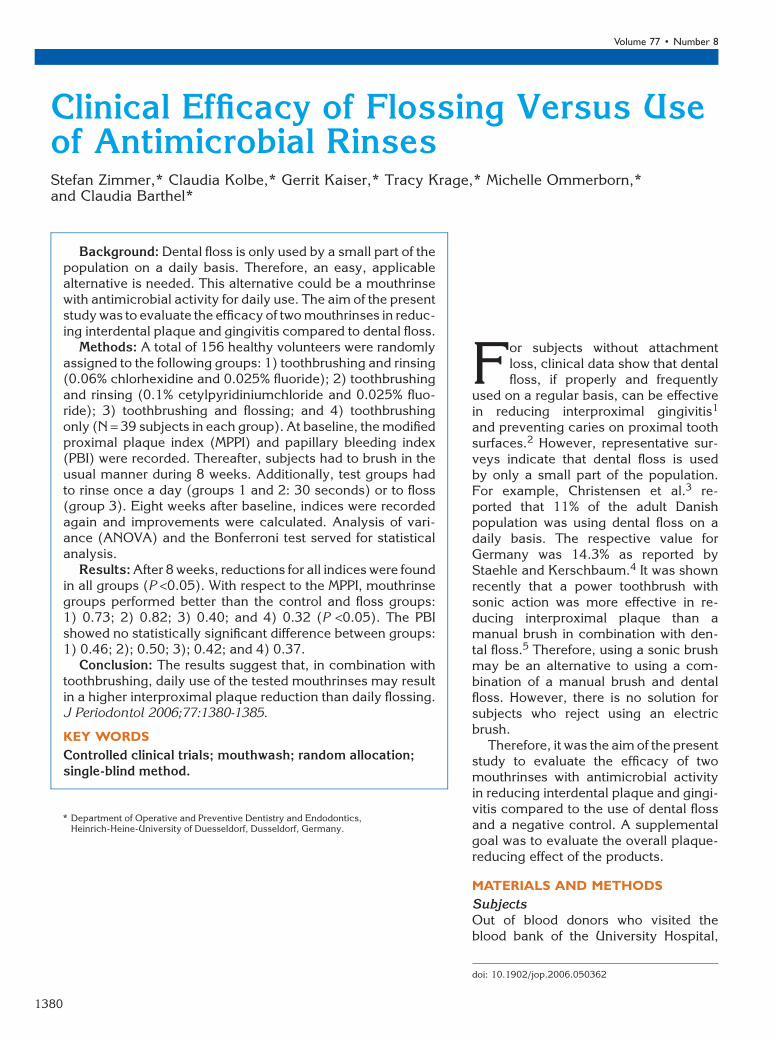
Figures 1 through 3 and Table 1 show the meanvalues of QHI, MPPI, and PBI at baseline and after 4and 8 weeks. After 8 weeks, reductions for all indiceswere found in all groups at P <0.05 (t test). Even if nostatistically significant differences could be found be-tween groups at baseline, the values were not exactlyidentical. Therefore, improvements between the threeappointments were calculated and compared betweengroups. Table 2 shows the improvements as percent-ages for QHI, MPPI, and PBI between baseline and 4weeks and between baseline and 8 weeks. After 8weeks, mouthrinse groups (1 and 2) performed better
than control and floss groups with respect to QHI andMPPI. The majority of the improvement was alreadyreached after 4 weeks. For PBI, no statistically signifi-cantdifferencewasfoundbetweengroupsafter8weeks.
To check the influence of smoking on the studyoutcome, statistical analysis was repeated for non-smokers alone. In comparison to the outcome for allparticipants, this analysis showed only very small dis-crepancies, e.g., PBI improvements for non-smokersafter 8 weeks were 0.59 (group 1), 0.47 (group 2),0.39 (group 3), and 0.37 (group 4) versus 0.56 (group1), 0.50 (group 2), 0.42 (group 3), and 0.37 (group4). According to these results, smoking status shouldnot have influenced the study outcome.
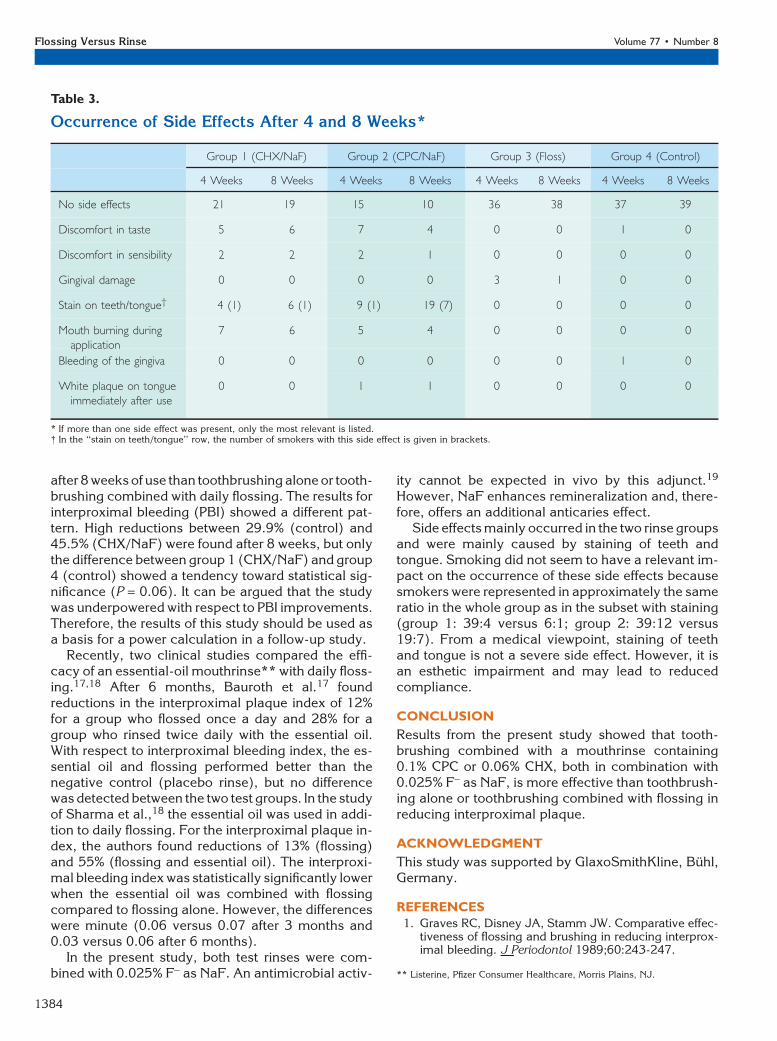
Side effects occurring after 4 and 8 weeks are pre-sented in Table 3. A few subjects showed more thanone side effect. In this case, the most relevant side ef-fect is reported. Compared to the other two groups,more statistically significant side effects were foundin the two mouthrinse groups after 4 and 8 weeks(x2; P <0.05). However, these side effects were onlymild and very limited in time. Staining could be re-moved by professional tooth cleaning. Statisticallysignificant differences between the two mouthrinsegroups were found after 8 weeks only. This wascaused by 19 cases of tooth and tongue staining inthe CPC/NaF-mouthrinse group (2).
Because clinically visible side effects (staining ofteeth and tongue) might have influenced examinerblinding, an additional statistical analysis was per-formed for subjects without visible side effects. Again,compared to all subjects, only small discrepancies ofthis subgroup and no changes in statistical signifi-cance were found. This finding indicates that clinicallyvisible side effects did not affect examiner accuracy.
DISCUSSION
In the present study, the efficacy of two mouthrinseswith antimicrobial activity in reducing interdental
Figure 1.Mean values of QHI at baseline and after 4 and 8 weeks.
Figure 2.Mean values of MPPI at baseline and after 4 and 8 weeks.
Figure 3.Mean values of PBI at baseline and after 4 and 8 weeks.
Flossing Versus Rinse Volume 77 • Number 8
1382
plaque and gingivitis was evaluated in comparison withthe use of dental floss and a negative control. This hadto be done under realistic circumstances. Therefore,no instruction in toothbrushing and no advice concern-ing the toothbrushing time was given. Because peopleusually do not use dental floss in a perfect way,11 theparticipants of our study did not get intensive training,except for a 2-minute instruction, in the use of dentalfloss. Inclusion criteria ensured that only subjects withsuboptimal oral hygiene were enrolled in the study.This was associated with the risk that the participantswould not comply with the study regimen in a perfectway. All participants were asked at each visit if theyhad used the attributed products as required. However,there was no objective measure to verify if dental flossor rinse was constantly used. On the other hand, thisreflected realistic conditions because recommenda-tions of dentists are not always followed.
No differences were found between the floss group(3) and the control group (4) with respect to all indices(Figures 1 through 3; Tables 1 and 2). This is in accor-
dance with results of Halla-Junior and Oppermann12
where the inclusion of flossing into an oral hygieneregimen did not show any improvement versus theuse of a toothbrush alone. In their 21-day crossoverstudy in 15-year-olds, interproximal bleeding was re-duced by 67.7% to 69.7% during the flossing phaseand 52.1% to 61.1% when no floss was used, showingno statistically significant differences. Similar resultswere found for proximal plaque. This supports theconclusion that the use of floss does not automaticallyimprove the quality of oral hygiene.
In contrast, when compared to groups 3 and 4, sub-jects of the rinse groups (1 and 2) showed statisticallysignificant higher plaque reductions after 8 weeks(Table 2). With respect to QHI, plaque reductionwas 26.2% for the CHX/NaF-mouthrinse group (1),and 27.4% for the CPC/NaF-formulation group (2).For MPPI, the respective values were 33.2% (group1) and 36.9% (group 2). This is in accordance withthe results of other clinical studies. In a 6-month clin-ical study, Allen et al.13 found a 28.2% reduction inQHI after rinsing twice a day with a 0.05% CPC mouth-rinse versus a placebo. Moran et al.14 showed a plaquereduction of 22.5% for a CPC rinse in a 4-day plaqueregrowth study with placebo control. In another 4-dayplaque regrowth study by Jenkins et al.,15 mouth-rinses with 0.1% CPC, 0.05% CPC, or 0.05% CHXshowed significant and similar reductions in plaqueand were superior to 0.05% triclosan. In these plaqueregrowth studies, rinsing was performed twice dailywithout an additional oral hygiene measure. In their6-month clinical study, Hoffmann et al.16 found thatsubjects using a 0.1% or 0.06% CHX solution showedsignificantly less plaque accumulation than those us-ing an amine fluoride/stannous fluoride mouthrinse.
The data of the present study clearly show that, inaddition to toothbrushing, rinsing with one of the twotested solutions is more effective in reducing plaque
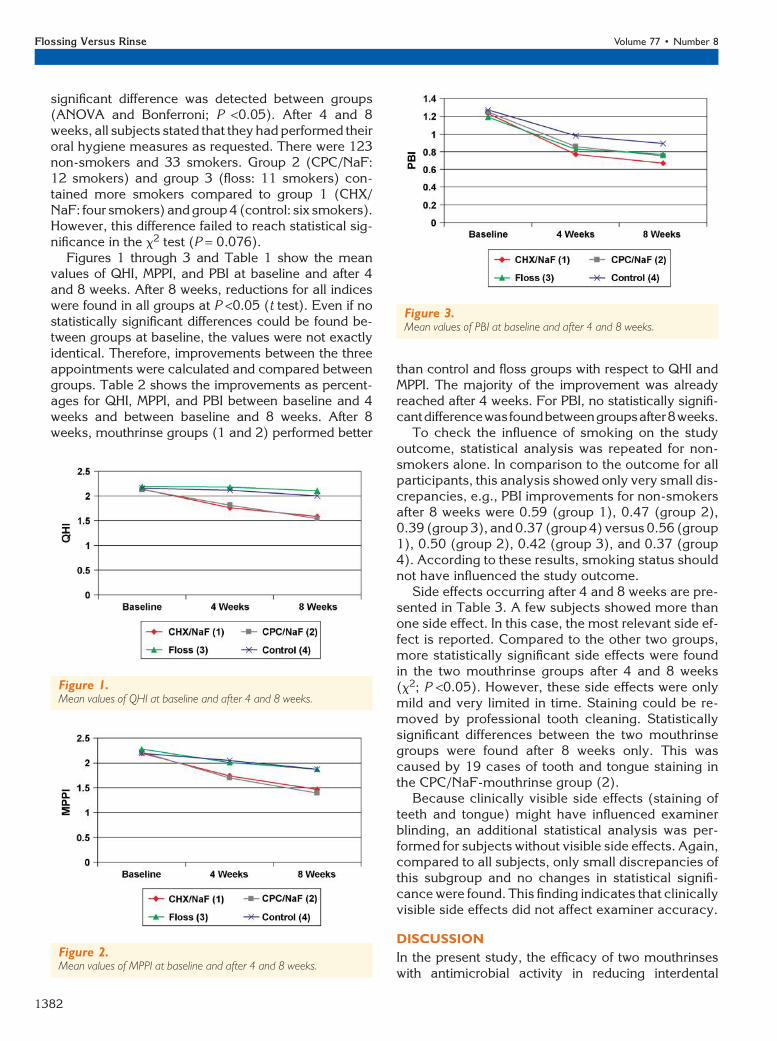
Table 1.
Mean (SD) Values of QHI, MPPI, and PBI at Baseline and After 4 and 8 Weeks
Group 1 (CHX/NaF) Group 2 (CPC/NaF) Group 3 (Floss) Group 4 (Control)
QHI Baseline 2.14 (0.45) 2.12 (0.34) 2.19 (0.39) 2.16 (0.41)
4 weeks 1.76 (0.38) a,b 1.81 (0.42) c,d 2.18 (0.46) a,c 2.11 (0.42) b,d
8 weeks 1.58 (0.44) a,b 1.54 (0.53) c,d 2.10 (0.49) a,c 2.00 (0.50) b,d
MPPI Baseline 2.20 (0.37) 2.22 (0.30) 2.28 (0.31) 2.20 (0.33)
4 weeks 1.74 (0.42) a 1.70 (0.49) b,c 2.01 (0.43) b 2.05 (0.45) a,c
8 weeks 1.47 (0.44) a,b 1.40 (0.49) c,d 1.88 (0.45) a,c 1.88 (0.50) b,d
PBI Baseline 1.23 (0.44) 1.25 (0.45) 1.19 (0.44) 1.27 (0.45)
4 weeks 0.77 (0.44) 0.86 (0.45) 0.83 (0.47) 0.98 (0.43)
8 weeks 0.67 (0.37) 0.75 (0.49) 0.77 (0.52) 0.89 (0.46)
Groups with the same letters are significantly different at P <0.05.
Table 2.
Mean Improvements (%) From Baseline ofQHI, MPPI, and PBI After 4 and 8 Weeks
Group 1
(CHX/NaF)
Group 2
(CPC/NaF)
Group 3
(Floss)
Group 4
(Control)
QHI Baseline-4 weeks 17.8 a,b 14.6 c,d 0.5 a,c 2.3 b,d
Baseline-8 weeks 26.2 a,b 27.4 c,d 4.1 a,c 7.4 b,d
MPPIBaseline-4 weeks 20.9 a 23.4 b,c 11.8 b 6.8 a,c
Baseline-8 weeks 33.2 a,b 36.9 c,d 17.5 a,c 14.5 b,d
PBI Baseline-4 weeks 37.4 a 31.2 30.3 22.8 a
Baseline-8 weeks 45.5 40.0 35.3 29.9
Groups with the same letters are significantly different at P <0.05.
J Periodontol • August 2006 Zimmer, Kolbe, Kaiser, Krage, Ommerborn, Barthel
1383
after 8 weeks of use than toothbrushing alone or tooth-brushing combined with daily flossing. The results forinterproximal bleeding (PBI) showed a different pat-tern. High reductions between 29.9% (control) and45.5% (CHX/NaF) were found after 8 weeks, but onlythe difference between group 1 (CHX/NaF) and group4 (control) showed a tendency toward statistical sig-nificance (P = 0.06). It can be argued that the studywas underpowered with respect to PBI improvements.Therefore, the results of this study should be used asa basis for a power calculation in a follow-up study.
Recently, two clinical studies compared the effi-cacy of an essential-oil mouthrinse** with daily floss-ing.17,18 After 6 months, Bauroth et al.17 foundreductions in the interproximal plaque index of 12%for a group who flossed once a day and 28% for agroup who rinsed twice daily with the essential oil.With respect to interproximal bleeding index, the es-sential oil and flossing performed better than thenegative control (placebo rinse), but no differencewas detected between the two test groups. In the studyof Sharma et al.,18 the essential oil was used in addi-tion to daily flossing. For the interproximal plaque in-dex, the authors found reductions of 13% (flossing)and 55% (flossing and essential oil). The interproxi-mal bleeding index was statistically significantly lowerwhen the essential oil was combined with flossingcompared to flossing alone. However, the differenceswere minute (0.06 versus 0.07 after 3 months and0.03 versus 0.06 after 6 months).
In the present study, both test rinses were com-bined with 0.025% F- as NaF. An antimicrobial activ-
ity cannot be expected in vivo by this adjunct.19
However, NaF enhances remineralization and, there-fore, offers an additional anticaries effect.
Side effects mainly occurred in the two rinse groupsand were mainly caused by staining of teeth andtongue. Smoking did not seem to have a relevant im-pact on the occurrence of these side effects becausesmokers were represented in approximately the sameratio in the whole group as in the subset with staining(group 1: 39:4 versus 6:1; group 2: 39:12 versus19:7). From a medical viewpoint, staining of teethand tongue is not a severe side effect. However, it isan esthetic impairment and may lead to reducedcompliance.
CONCLUSION
Results from the present study showed that tooth-brushing combined with a mouthrinse containing0.1% CPC or 0.06% CHX, both in combination with0.025% F- as NaF, is more effective than toothbrush-ing alone or toothbrushing combined with flossing inreducing interproximal plaque.
ACKNOWLEDGMENT
This study was supported by GlaxoSmithKline, Buhl,Germany.
REFERENCES1. Graves RC, Disney JA, Stamm JW. Comparative effec-
tiveness of flossing and brushing in reducing interprox-imal bleeding. J Periodontol 1989;60:243-247.
Table 3.
Occurrence of Side Effects After 4 and 8 Weeks*
Group 1 (CHX/NaF) Group 2 (CPC/NaF) Group 3 (Floss) Group 4 (Control)
4 Weeks 8 Weeks 4 Weeks 8 Weeks 4 Weeks 8 Weeks 4 Weeks 8 Weeks
No side effects 21 19 15 10 36 38 37 39
Discomfort in taste 5 6 7 4 0 0 1 0
Discomfort in sensibility 2 2 2 1 0 0 0 0
Gingival damage 0 0 0 0 3 1 0 0
Stain on teeth/tongue† 4 (1) 6 (1) 9 (1) 19 (7) 0 0 0 0
Mouth burning duringapplication
7 6 5 4 0 0 0 0
Bleeding of the gingiva 0 0 0 0 0 0 1 0
White plaque on tongueimmediately after use
0 0 1 1 0 0 0 0
* If more than one side effect was present, only the most relevant is listed.† In the ‘‘stain on teeth/tongue’’ row, the number of smokers with this side effect is given in brackets.
** Listerine, Pfizer Consumer Healthcare, Morris Plains, NJ.
Flossing Versus Rinse Volume 77 • Number 8
1384
2. Wright GZ, Banting DW, Feasby WH. Effect of inter-dental flossing on the incidence of proximal caries inchildren. J Dent Res 1977;56:574-578.
3. Christensen LB, Petersen PE, Krustrup U, Kjoller M.Self-reported oral hygiene practices among adults inDenmark. Community Dent Health 2003;20:229-235.
4. Staehle HJ, Kerschbaum T. Switzerland – The myth:Beliefs and facts about oral health in Switzerland com-pared to Germany. Dtsch Zahnarztl Z 2003;58:325-330.
5. Sjogren K, Lundberg AB, Birkhed D, Dudgeon DJ,Johnson MR. Interproximal plaque mass and fluorideretention after brushing and flossing-a comparativestudy of powered toothbrushing, manual toothbrush-ing and flossing. Oral Health Prev Dent 2004;2:119-124.
6. Saxer UP, Muhlemann HR. Motivation and education(in German) SSO Schweiz Monatsschr Zahnheilkd1975;85:905-919.
7. Lange DE, Plagmann HC, Eenboom A, PromesbergerA. Clinical methods for the objective evaluation of oralhygiene. Dtsch Zahnarztl Z 1977;32:44-47.
8. Zimmer S, Strauss J, Bizhang M, Krage T, Raab WH,Barthel C. Efficacy of the Cybersonic in comparisonwith the Braun 3D Excel and a manual toothbrush.J Clin Periodontol 2005;32:360-363.
9. Lindhe J, Ranney R, Lamster I, et al. Consensus report:Chronic periodontitis. Ann Periodontol 1999;4:38.
10. Quigley GA, Hein JW. Comparative cleansing effi-ciency of manual and power brushing. J Am DentAssoc 1962;65:26-29.
11. Segelnick SL. A survey of floss frequency, habit andtechnique in a hospital dental clinic & private peri-odontal practice. N Y State Dent J 2004;70:28-33.
12. Halla-Junior R, Oppermann RV. Evaluation of dentalflossing on a group of second grade students under-taking supervised tooth brushing. Oral Health PrevDent 2004;2:111-118.
13. Allen DR, Davies R, Bradshaw B, et al. Efficacy of amouthrinse containing 0.05% cetylpyridinium chloride
for the control of plaque and gingivitis: A 6-monthclinical study in adults. Compend Contin Educ Dent1998;19(Suppl. 2):20-26.
14. Moran J, Addy M, Jackson R, Newcombe RG. Com-parative effects of quaternary ammonium mouthrinseson 4-day plaque regrowth. J Clin Periodontol 2000;27:37-40.
15. Jenkins S, Addy M, Newcombe RG. A comparison ofcetylpyridinium chloride, triclosan and chlorhexidinemouthrinse formulations for effects on plaque re-growth. J Clin Periodontol 1994;21:441-444.
16. Hoffmann T, Bruhn G, Richter S, Netuschil L,Brecx M. Clinical controlled study on plaque andgingivitis reduction under long-term use of low-dose chlorhexidine solutions in a population exhibit-ing good oral hygiene. Clin Oral Investig 2001;5:89-95.
17. Bauroth K, Charles CH, Mankodi SM, Simmons K,Zhao Q, Kumar LD. The efficacy of an essential oilantiseptic mouthrinse vs. dental floss in controllinginterproximal gingivitis: A comparative study. J AmDent Assoc 2003;134:359-365.
18. Sharma N, Charles CH, Lynch MC, et al. Adjunctivebenefit of an essential oil-containing mouthrinse inreducing plaque and gingivitis in patients who brushand floss regularly: A six-month study. J Am DentAssoc 2004;135:496-504.
19. Van Loveren C. Antimicrobial activity of fluoride andits in vivo importance. Identification of research ques-tions. Caries Res 2001;35(Suppl. 1):65-70.
Correspondence: Dr. Stefan Zimmer, Department ofOperative and Preventive Dentistry and Endodontics,Heinrich-Heine-University of Dusseldorf, Building 1873,Moorenstr. 5, D-40225 Dusseldorf, Germany. Fax: 49-211-811 9244; e-mail: [email protected].
Accepted for publication February 24, 2006.
J Periodontol • August 2006 Zimmer, Kolbe, Kaiser, Krage, Ommerborn, Barthel
1385











![Flossing for the management of periodontal diseases and ...neuron.mefst.hr/docs/katedre/istrazivanja_bz/ibz m4/SR flossing.pdf · [Intervention Review] Flossing for the management](https://img.pdfslide.us/doc/110x75/5dd0b9c6d6be591ccb62647f/flossing-for-the-management-of-periodontal-diseases-and-m4sr-flossingpdf.jpg)