Embed Size (px)
Citation preview
CLINICAL DIAGNOSTIC TB LABORATORY
Alexander Sloutsky, Director
University of Massachusetts Supranational Reference TB Laboratory
Boston, MA

ASSESSMENT OF THE TB LABORATORY SERVICES
• Currently used methods and new methods implementation
• Turn-around time (TAT) and CDC guidelines
• Quality Control/Quality Assurance
Functions of Large TB Diagnostic Lab
Ope
ratio
nal
rese
arch
International
projects
Diagnostics
QA/QC
USERS: Who Needs TB Laboratory Services?
• Clinical Community (hospitals, individual doctors);• Public Health practitioners;• Social Institutions (penitentiary system, shelters,
nursing homes and assisted living facilities, refugee health, and other w/congregated living);
• Research and Development teams from pharmaceutical companies, other research institutions;
• Non-profit organizations launching international TB-related projects in low-income countries.

METHODS
• Detection of acid-fast bacilli (AFB) primarily in respiratory specimens; also in other body fluids or tissues.
• Smear preparation and microscopy• Processing specimens• Detection of AFB growth in liquid and solid cultures• Molecular detection (PCR, MTD and other methods)
• Identification to species • Conventional (biochemical) methods• Molecular probes • HPLC• DNA-sequencing of highly polymorphic regions, amplified by PCR
• Drug Susceptibility testing (DST)• Conventional (Agar Plate Proportion)• Rapid ( BACTEC) • Molecular methods
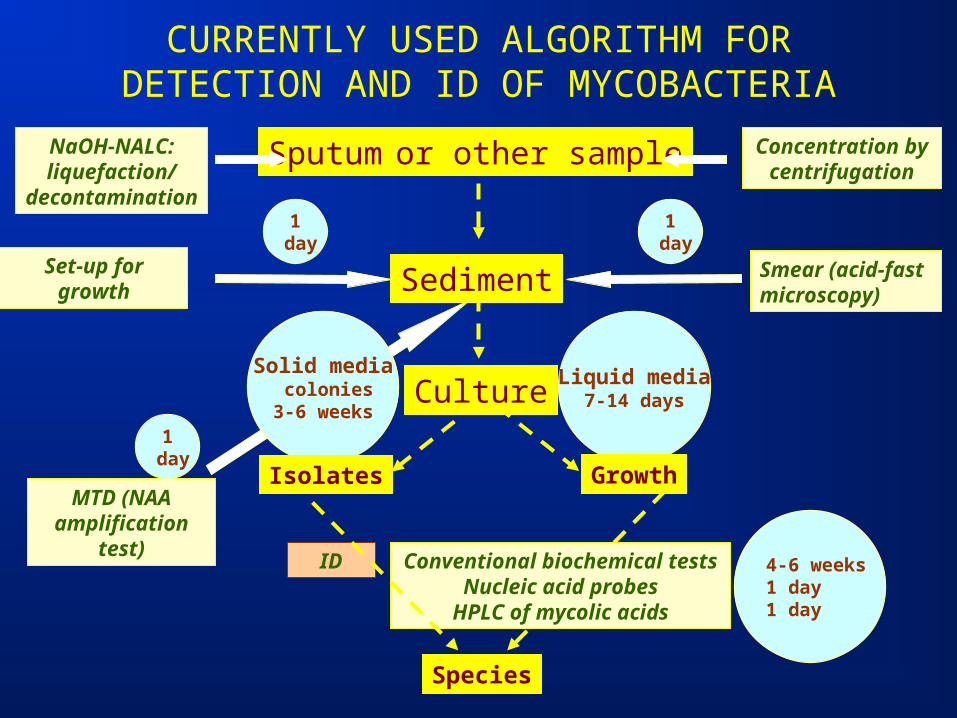
CURRENTLY USED ALGORITHM FOR DETECTION AND ID OF MYCOBACTERIA
Sputum or other sampleNaOH-NALC:liquefaction/
decontamination
Concentration by centrifugation
Smear (acid-fast microscopy)Sediment
Culture
Species
Conventional biochemical testsNucleic acid probes
HPLC of mycolic acids
ID
1 day
Solid media colonies3-6 weeks
Set-up for growth
1 day
Liquid media7-14 days
4-6 weeks1 day1 day
MTD (NAA amplification
test)
1 day
Isolates Growth
New Methods in TB Diagnostics
Q.: What drives people’s desire to develop and implement new methods for TB diagnostics?
A.: Reduction of the TAT and its impact on patient management.
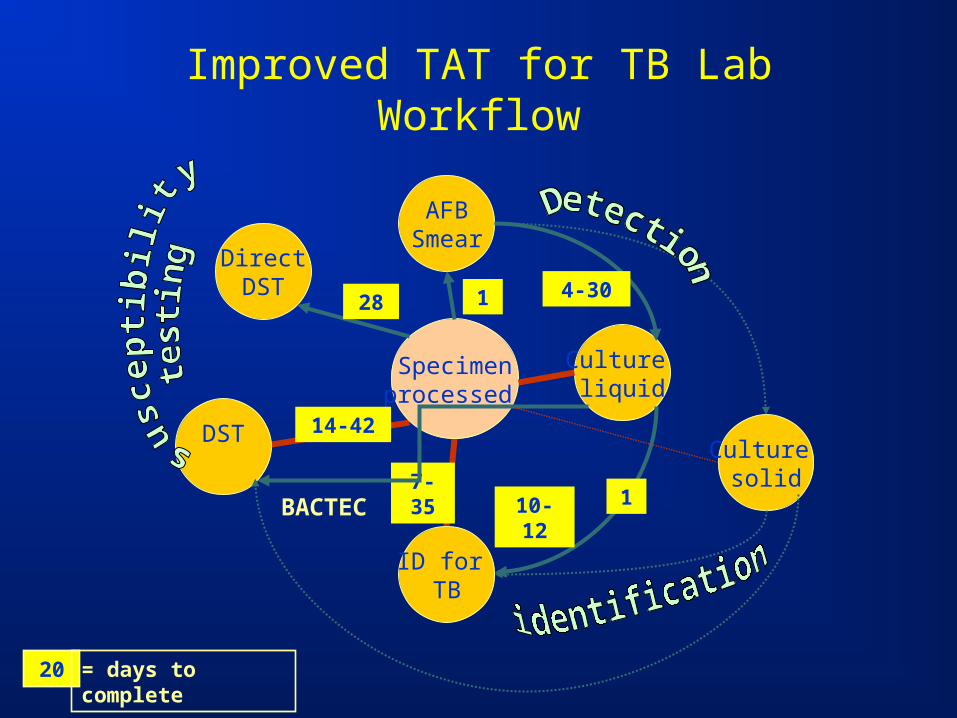
Improved TAT for TB Lab Workflow
Specimenprocessed
AFBSmear
Culture solid
ID for TB
DST
1
14-42
20 = days to complete
7-35
Culture liquid
4-30
1
DirectDST
28
BACTEC 10-12

TAT After Implementation of New Methods
Procedure Required TAT (days)
Real TAT (days)
Improved TAT
Smear 1 1 1
Detection of growth
14 20-60 5-30
Identification 21 35-90 7-35
DST 28 50-90 14-42
30 (dir)

Rapid detection of DR TB: gains
• Urban populations with significant prevalence of MDR TB and HIV co-infection, where data on the resistance genotype may result in better patients management
• Congregate living facilities where a quick action has to be taken
• Culture is not available but the answer is very important– Exposure of a large group of cancer patients to a
TB case
Rapid detection of DR TB: pains
• All molecular techniques are based on NAA (PCR) which will gladly amplify any DNAs including contaminating ones…
• Each case falsely diagnosed with DR TB will receive unnecessary treatment with second line drugs
• Cost for molecular testing is high. Difficult to include into lab algorithm (batching vs. TAT)
• Except Rifampin, testing for R to all other TB drugs have complications
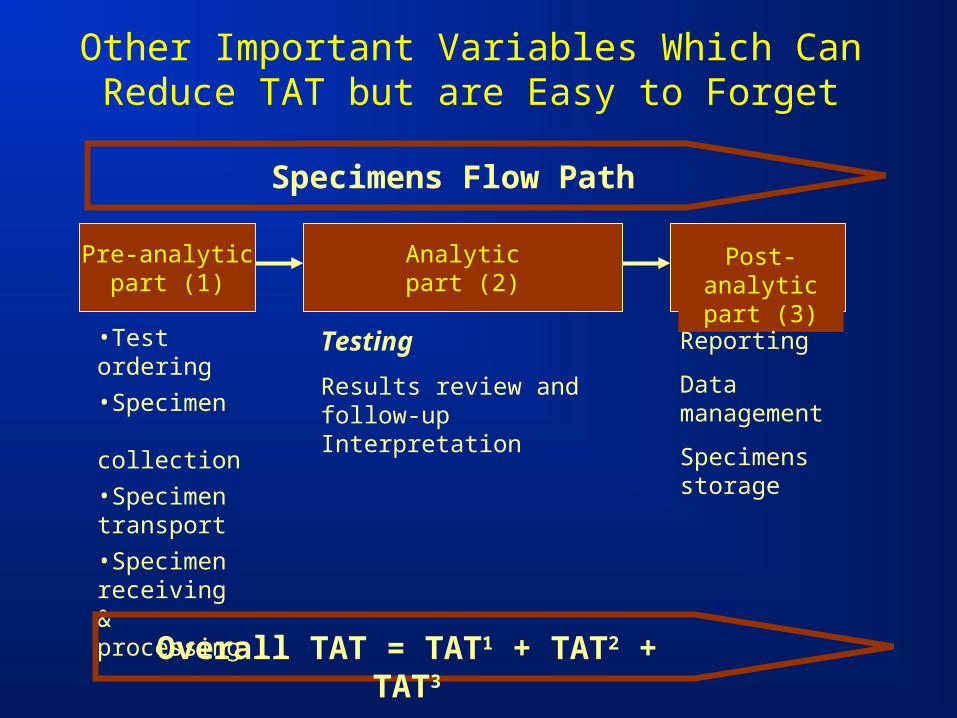
Other Important Variables Which Can Reduce TAT but are Easy to Forget
Post-analytic part (3)
Pre-analyticpart (1)
Analyticpart (2)
•Test ordering
•Specimen collection
•Specimen transport
•Specimen receiving & processing
Testing
Results review and follow-up Interpretation
Reporting
Data management
Specimens storage
Overall TAT = TAT1 + TAT2 + TAT3
Specimens Flow Path
QUALITY CONTROL (QC)
Quality Control (QC)
• Process of effective and systematic control for all laboratory activities which helps to eliminaterestrictions for quality testing
• Good QC program provides warranty for accuracy,reliability and comparability of laboratory results.
• Mechanism which helps to verify proficiency of TB diagnostic Services.
• QC is responsibility of all Lab staff and management
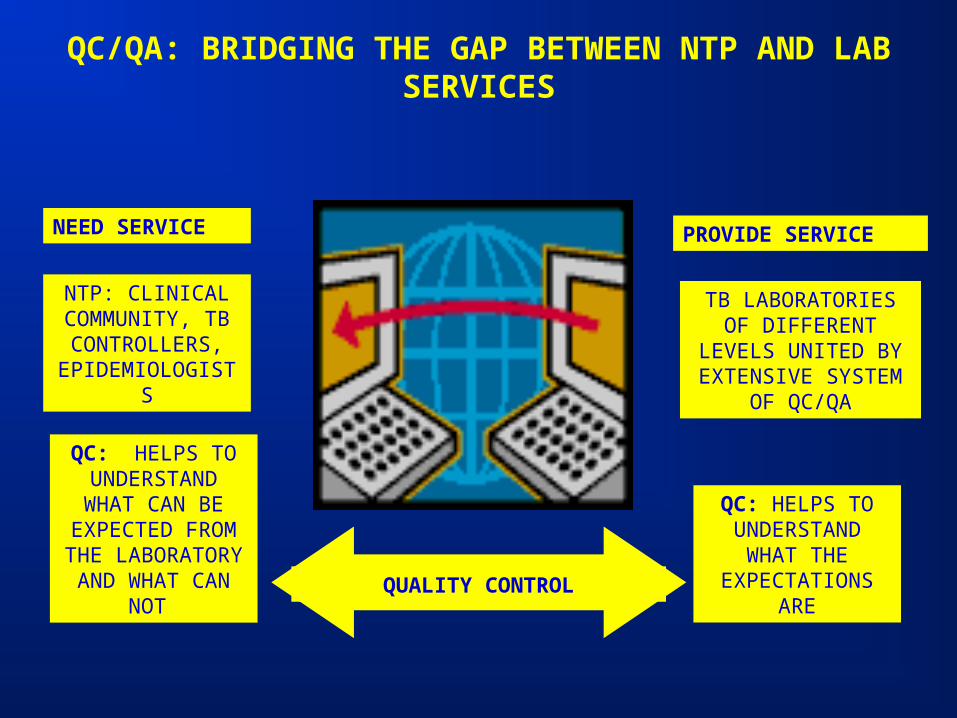
QC/QA: BRIDGING THE GAP BETWEEN NTP AND LAB SERVICES
NTP: CLINICAL COMMUNITY, TB CONTROLLERS,
EPIDEMIOLOGISTS
TB LABORATORIES OF DIFFERENT
LEVELS UNITED BY EXTENSIVE SYSTEM
OF QC/QA
NEED SERVICE PROVIDE SERVICE
QC: HELPS TO UNDERSTAND WHAT CAN BE
EXPECTED FROM THE
LABORATORY AND WHAT CAN
NOT
QC: HELPS TO UNDERSTAND
WHAT THE EXPECTATIONS
AREQUALITY CONTROL
OPERATIONAL RESEARCH IMPROVING ROUTINE DIAGNOSTICS
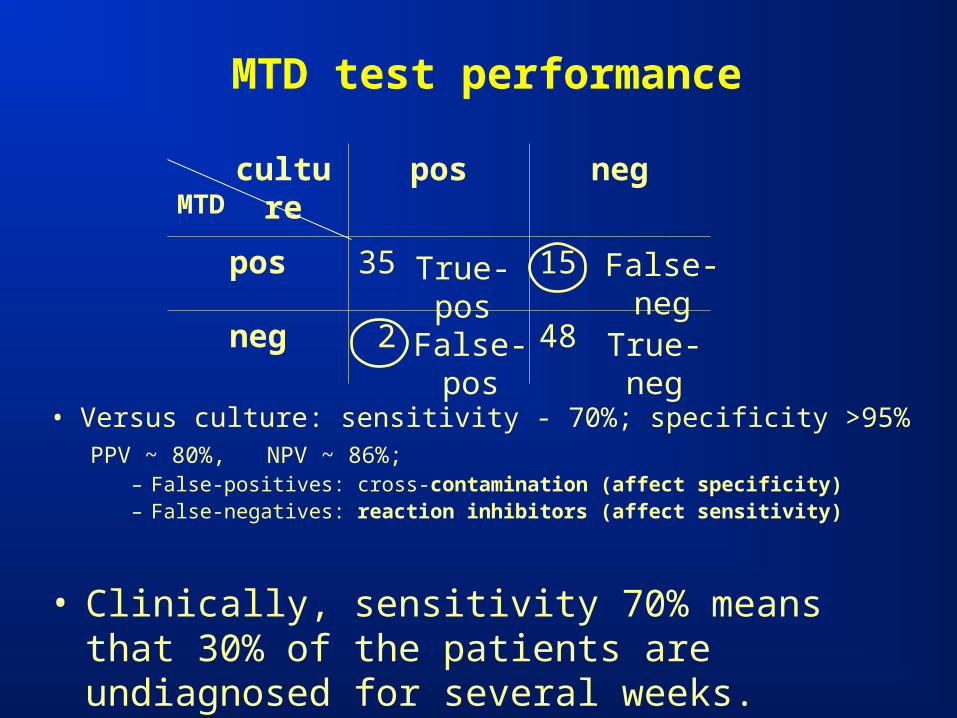
MTD test performance
• Versus culture: sensitivity - 70%; specificity >95%PPV ~ 80%, NPV ~ 86%;
– False-positives: cross-contamination (affect specificity)– False-negatives: reaction inhibitors (affect sensitivity)
• Clinically, sensitivity 70% means that 30% of the patients are undiagnosed for several weeks.
MTDpos neg
pos 35 15
neg 2 48
culture
False-neg
False-pos True-neg
True-pos
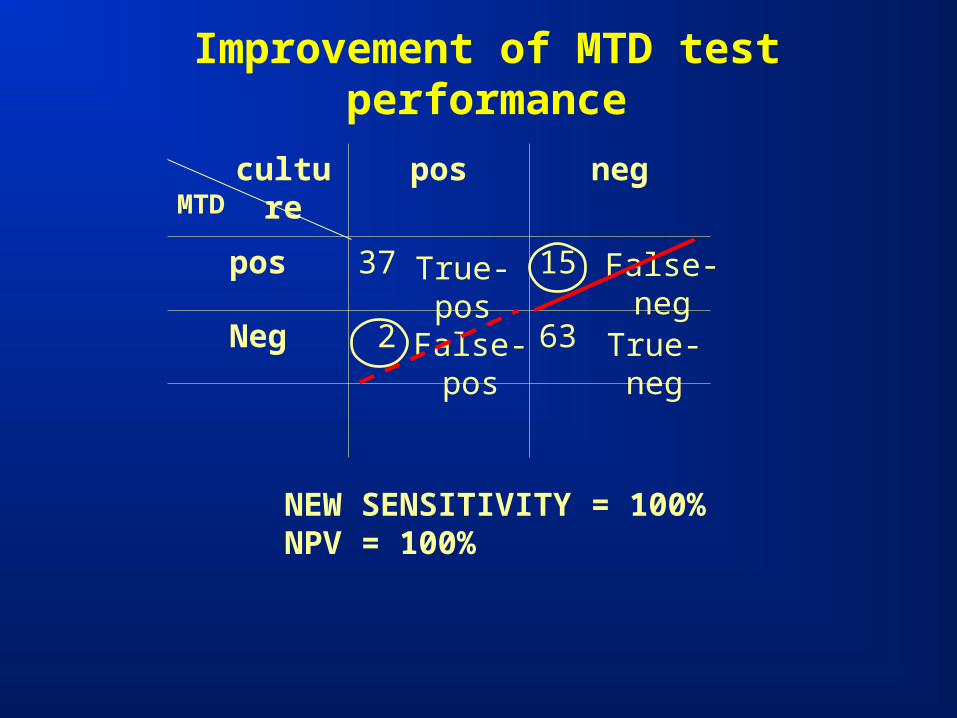
Improvement of MTD test performance
MTDpos neg
pos 37 15
Neg 2 63
culture
False-neg
False-pos True-neg
True-pos
NEW SENSITIVITY = 100%NPV = 100%
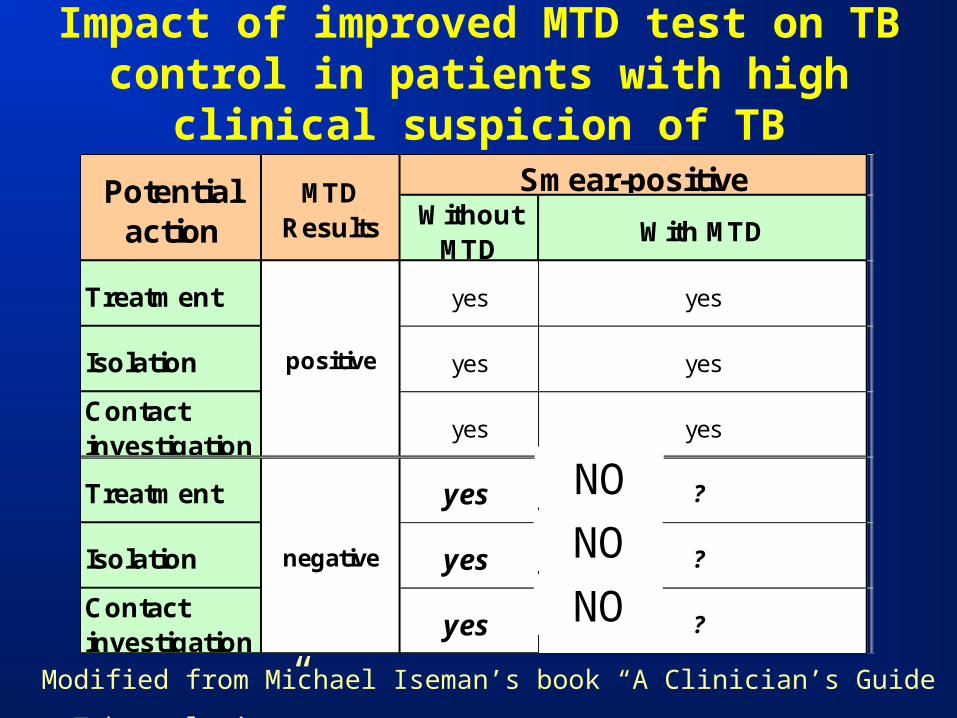
Without MTD
With MTD
Treatment yes yes
Isolation yes yes
Contact investigation
yes yes
Treatment yes ?
Isolation yes ?
Contact investigation
yes ?
Potential action
positive
negative
Smear-positiveMTD Results
Impact of improved MTD test on TB control in patients with high clinical suspicion of TB
Modified from Michael Iseman’s book “A Clinician’s Guide toTuberculosis”
NO
NO
NO
Examples of research projects in TB Lab• Evaluation, validation and implementation of
molecular diagnostics by broad spectrum PCR and a follow-up DNA-sequencing in:– liquid media, when there is not enough growth to use
Molecular Probes
– paraffin-embedded tissue specimens– Primary specimens Also, PCR and DNA-sequencing of specific mutation conferring
resistance to INH, ETH, Rif, PZA, FQs (in lieu of DST)
• Development of an original method for assessment of quality of sputum specimens.
• RFLP typing for detection of cross-contamination.• Development of new medium improving recovery of
Mycobacteria from sputum specimens.• Study of cross-resistance between aminoglycosides as well
as between INH and Ethionamide