Embed Size (px)
Citation preview

British Journal of Ophthalmology, 1989, 73, 639-644
Clinical criteria for the assessment of disease activity inGraves' ophthalmopathy: a novel approachM PH MOURITS,' L KOORNNEEF,' W M WIERSINGA,' M F PRUMMEL,'A BERGHOUT,' AND R V D GAAG'
From the 'Orbital Centre and the 2Department of Endocrinology of the University ofAmsterdam, and the'Department ofImmunology of the Netherlands Ophthalmic Research Institute, The Netherlands
SUMMARY Patients with serious inflammatory Graves' ophthalmopathy should be treated withanti-inflammatory drugs or radiotherapy to prevent complications like fibrosis, while those withnon-inflammatory ophthalmopathy may be treated by surgery immediately. It is often difficult,however, to distinguish inflammatory from non-inflammatory Graves' disease. We thereforepresent a simple clinical classification here to differentiate between these two conditions. Thisclassification is based on the classical signs of inflammation-pain, redness, swelling, and impairedfunction. After two consecutive clinical examinations an 'activity score' can be determined,ranging from 0 to 10 points. In a retrospective study testing the efficacy of this classification wefound that patients with an activity score of 3 or more at the beginning of therapy responded well toanti-inflammatory drugs, while those with a lower activity score mostly did not. Comparing thepretreatment activity score with the degree of enlargement of the extraocular muscles on the CTscan, we found a significant correlation between these two parameters: the higher the activityscore, the more the enlargement of the muscles. We conclude that this classification facilitates theproper selection of patients for treatment.
Graves' ophthalmopathy appears to be an organ-specific autoimmune disorder.' A still unidentifiedpathogenic process induces swelling, lymphocyticinfiltration, and later fibrosis and contractures thatrestrict *the normal function of the extraocularmuscles.' Two stages in the development of thedisease are generally distinguished: the stage ofactive inflammation in which the eyes are red andpainful, and the quiescent stage in which the eyes arewhite and unchanging with a painless motility deficit.'Treatment of serious Graves' ophthalmopathy
may be either non-surgical or surgical. Of the non-surgical treatments orally administered steroids orradiotherapy or a combination of both are usuallyfavoured. No agreement on the results of thesetreatments can be found. Brain4 reported immediatebeneficial effects on the inflammatory componentsof the ophthalmopathy after short high doses ofcorticosteroids. Day and Caroll' noted dramaticimprovement of optic neuropathy by this therapy.
Correspondence to M Ph Mourits, MD, Orbita Centrum,Academisch Medisch Centrum, A-2 116. Meibergdreef 9. 1105 AZAmsterdam, The Netherlands.
639
McCohaney' stated that extraocular muscle dysfunc-tion at the stage of fibrosis and proptosis does notgenerally respond well to corticosteroids. However,Wiersinga et al.' found a positive response in 66% ofall patients treated with prednisone alone. Hurbli etal.' found better results with radiation therapy inpatients having a short history of Graves' ophthalmo-pathy than in patients with long-term ocular changes.Apart from basic differences in the definitions ofsuccessful treatment among authors these unequalsuccess rates can be explained by the heterogeneity ofthe patients-patients with inflammatory progressiveGraves' ophthalmopathy and those with the non-inflammatory stationary stage of the disease.The indication for treatment has always been the
severity of symptoms (according to the NOSPECSclassification*) instead of the rate of progression ofthe disease. During the initial stage immunosuppres-*An abridged classification of eye changes in Graves' ophthalmo-pathy'' : class (0): no physical signs or symptoms; (1) only signs, nosymptoms (signs limited to upper lid retraction, stare, and lid lag);(2) soft-tissue involvement (symptoms and signs); (3) proptosis;(4) extraocular muscle movement: (5) corneal involvement; (6) sightloss (optic nerve insolvement).
on 7 June 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.8.639 on 1 August 1989. D
ownloaded from

M Ph Mourits, L Koornneef, WM Wiersitiga, M F Prummel., A Berg/out, antd R v (I Gaag
sive treatment or radiotherapy is logical and inhibitsthe inflammatory process. Once fibrosis has takenplace, this kind of treatment is useless. Surgery candeal with the residual sequelae successfully. It istherefore imperative to know whether a patient hasactive or quiescent Graves' ophthalmopathy.To match appropriate therapy to the patients we
propose a clinical classification to discriminate easilybetween the active and quiescent stages of thedisease. This system is based on the well known signsof acute inflammation: pain (Latin: dolor), redness(rubor), swelling (tumor), and impaired function(functio laesa), defined by Celsus and Galencenturies ago.
Clinical classification for disease activity
Patients with Graves' ophthalmopathy complain ofpain, a burning sensation, excessive lacrimation,photophobia, swelling of the eyelids, proptosis,double vision, and visual impairment. Thesesymptoms and signs are related to the classical signsof inflammation (Table 1).
In Graves' ophthalmopathy several kinds of paincan be distinguished. One kind of pain arises from thestretching of the inflamed muscle(s), especially onattempted upgaze." Another sort of pain is caused bythe rise in intraorbital pressure, when the orbitaltissues expand through fluid accumulation andcellular infiltration. This is felt as a painful, oppres-sive feeling on or behind the globes. When asked,most patients can discriminate well between thesetwo kinds of pain. The 'stretching pain' cannot beprovoked by digital pressing on the eyeball, as wouldbe expected if it were a manifestation of the raisedintraorbital pressure. Both kinds of pain are the first
Table 1 Proposed classification system to assess diseaseactivity in Graves' oplthalmopathy
painful, oppressive feeling on or behind the globe.pain on attempted up, side, or down gaze
Rednessredness of the eyelid(s),diffuse redness of the conjunctiva
SivellingChemosis,swollen carunculeoedema of the eyelid(s)increase of proptosis of 2 mm or more during a period between Iand 3 months
Impairedfunctiondecrease in s isual acuity of I or more lines on the Snellen chart
(using a pinhole) during a period between I and 3 monthsdecrease of eye movements in any direction equal to or more than
5 degrees during a period of time between I and 3 months
For each of the signs present one point is given. The sum of thesepoints defines the active its score.
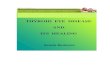
Fig. I Patient wit/i inflammatory Graves op/lit/almop)at/iy,showing redness of the eyelids andi diffuse redness of theconjunctiva. Oedema of the eyelids is also clear/v visible.
symptoms to disappear after anti-inflammatory treat-ment. We therefore consider these kinds of pain to bedirectly related to the inflammation in the orbit andthus useful in assessing inflammatory activity. Theydiffer from pain caused by corneal defects, pain dueto a spasm of the orbicularis muscle secondary tophotophobia, or pain in the context of asthenopiabecause of a changed refraction. We consider theselast symptoms to be epiphenomena and therefore notuseful in assessing the disease activity.
Redness as an expression of inflammation is causedby vasodilatation. In Graves' ophthalmopathy this isseen as redness of the eyelids and over the conjunc-tiva (Fig. 1). These signs must be differentiated fromthe redness accompanying exposure keratitis and thegrossly dilated vessels over the insertions of theextraocular muscles. The latter condition is seen bothin active and in quiescent Graves' ophthalmopathy.
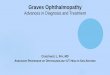
Swelling in Graves' ophthalmopathy is seen aschemosis (oedema of the conjunctiva) and a swollencaruncule (Fig. 2). Both are signs of activity. Swollen
r Ad~~~~~~~~~~~~~~~~~~~~~~~~~...-...l.....
Fig. 2 Patient with inflammatory Graves' ophthalmopathy,showing grossly enlarged caruncles and oedema oftheeyelids.
640
on 7 June 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.8.639 on 1 August 1989. D
ownloaded from

Clinical criteria ofdisease acdtivitv in Graves' ophthalmopathy
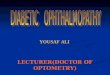
Fig. 3 Patient wit/i burnt out Graves' ophthalmopathy.The swelling of the eyelids is not caused by oedema.
eyelids can be caused by oedema, fat prolapsethrough the orbital septum, or fibrotic degeneration(Fig. 3). Here only eyelid oedema should be con-
sidered a sign of inflammation. To differentiateoedema from other causes of eyelid swelling palpa-tion and illumination of the eyelids with a torch are
mandatory.In Graves' ophthalmopathy inflammation causes
fluid accumulation and cellular infiltration in theorbit, later to be followed by fibrotic tissue. Proptosisand swelling of the eyelids are the result of the entireprocess. Therefore proptosis and eyelid swelling are
not in themselves signs of acute inflammation.However, increasing proptosis in this context is a
proof of it. A test-retest error of 2 mm is usually citedas the limit of exophthalmometer accuracy."' Wetherefore consider an increase in proptosis of 2 ormore millimetres to be a positive sign of diseaseactivity.
Visual impairment in Graves' ophthalmopathy,resulting from dysfunction of the optic nerve, iscaused by raised intraorbital pressure due to theinflammatory process.'2 Therefore a decrease ofvisual acuity as a result of optic compression is a signof disease activity. However, a decrease of visualacuity due to corneal defects cannot be considered an
early sign of active Graves' disease. Corneal defectsare most probably caused by increased width of thepalpebral fissure, which accelerates tear filmevaporation, thus increasing tear film osmolarity,with resulting ocular damage. '3That is why we
consider corneal involvement to be an epipheno-menon. A decrease in eye movements implies thatthe extraocular muscle function is progressivelyimpaired. It can therefore be regarded as a sign ofdisease activity.To detect an increase in proptosis or a decrease in
eye movements or visual acuity over a span of time atleast two different consecutive examinations are
necessary. In view of the natural history of Graves'ophthalmopathy we consider that the intervalbetween these examinations should be at least oneand not more than three months.
Pilot study to test efficacy of classification
The patients' records from an ongoing prospective,randomised, clinical trial to compare the efficacy,safety, and tolerability of cyclosporin and oralprednisone in severe Graves' ophthalmopathy'4 wereused for this purpose. In this study 26 consecutivepatients with serious Graves' ophthalmopathy,defined as falling into NOSPECS categories 2c, 3b,3c, 4b, 4c, 5a, 5b, 5c, or 6a, were treated with oralprednisone or cyclosporin for a period of 12 weeks.These patients were euthyroid for more than twomonths when they started the trial. They had had noprevious eye treatment other than local measures.Eighteen were female and eight male. Their agesranged from 23 to 70 years.The treatment consisted of 60 mg prednisone/day
during the first two weeks, 40 mg during the next twoweeks, 30 mg during the next four weeks, and 20 mgduring the last four weeks, then tapering off, orcyclosporin 7-5 mg/kg bodyweight/day for 12 weeks.When the therapeutic outcome after 12 weeks wasconsidered unsuccessful, the patients were treatedfor another 12 weeks with a combination of both oralprednisone (20 mg/day) and cyclosporin (in the samedosage as mentioned above). After 24 weeks the finaloutcome was evaluated. The success or failure oftreatment was defined as shown in Table 2. Patientswere examined before and at the beginning oftherapy and after 1, 3, 4, and 6 months. Apart fromclassifying each patient in the NOSPECS system ineach category, the visual acuity, proptosis, and eyemovements were measured and eyelid oedema andchemosis recorded. At each visit photographs of theface were taken and the patients were asked abouttheir complaints. Coronal CT scans of the orbits werecarried out at the beginning of treatment.The definitions of pain, as given in our scoring
classification, could not be applied, as we were using
Table 2 Definitions ofsuccess and failure of treatment inGraves' oplithalmopathy
SuccessA decrease (compared to baseline) in NOSPECS class or. if thisdid not occur, a decrease in grade within a class
FailureAn increase (compared to baseline) in NOSPECS class or. if thisdid not occur in grade within a class, or no change in NOSPECSclass or grade
If both decreases and increases occurred in different classes, thechange in the highest class was evaluated for therapeutic outcome.
641
on 7 June 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.8.639 on 1 August 1989. D
ownloaded from

Ph Mounts, L Koortuneef, WM Wiersinga, M F Pruminmel, A Berghout, atnd R dI (aag
7
6 -'
V)
z
F
0
z
2
I
u
0 1 2 3 4 5 6 7
ACTIVITY SCORE
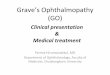
retrospective data, in which this item had not beenplanned for. However, all other signs of clinicalactivity could be assessed from the data.The results of this study are shown in Fig. 4 and
Table 3. After 24 weeks of therapy 19 out of 26patients with serious Graves' ophthalmopathy hadimproved according to our predefined parametersand described standards. One patient (No. 24)underwent orbital decompression before the finalevaluation of medical treatment was done, becauseof increasing visual impairment due to optic neuro-pathy (and was therefore not incorporated in Fig. 4).Three patients showed a worsening of their ophthal-mopathy during treatment. They had an activityscore of 1 or 2 points. The condition of the remaining
three patients, all of them with an activity score ofzero, did not change.The degree of extraocular muscle enlargement on
the orbital coronal CT scan was assessed in a ratingsystem of 5 points (0: no enlarged muscles; 5: grosslyenlarged muscles) by an ophthalmologist who was
not informed about the activity score. By linearcorrelation and regression analysis a significantcorrelation was found between the extraocularmuscle size and our activity score (r=(052, volume=1-9+0n31xactivity score, p=0007). The relation-ships between muscle size and the activity score willbe studied in more detail in future prospectivestudies.
Fig. 4 suggests that the clinical activity score is
Table 3 Sex, age, relative incidence of disease activity signs, actii'it' score, thlerap v', 11(1 results of i/wraps' in 26 patientstreated for serious Graves' oplithalhnopathy
Paienet number 1 2 3 4 6 7 8 9 10 11 12 1 14 15 16 17 18 1( 20( 21 22 23 24 25 26
Sex F F F M F F F M F F F M F F M F F F M F M M F F F MAge 67 '5 39 68 7 54 '2 70 54 54 44 40 23 '2 62 '8 46 36 47 37 54 60 44 43 40 64Pain + + + + + + + + + + + + + + + +Redness of evelids + + + + + + + + + + + + + + + + + +Redness of conjunctisa + + + + + + + + + + +Chemosis + + + + + + + + +Swollen caruncula + + + +Eyelid oedema + + + + + + + + + + + + + + + +Increase proptosis +Decrease in VA + + + + + +Decrease in motility +Activity score 3 2 6 6 3 1 2 5 1 3 2 0 3 4 2 6 4 4 * 2 8 3 2
Therapy D D C A C A B D D C A D A C I) D A D I) A ) A I) C B BResults of therapy S S S S S S S S F S S F S F S F S F S S S S F S S
*Patient No. 24 underwent orhital decompression before the final evaliiiation of medical treatment "nas maide.F=female. M=male.A=prednisone. B=cyclosporin. C=prednisone first, then cyclosporin added. D=cyclosporin first, then prednisone added.S= treatment success. F= treatment failure.
642
Fig. 4 Relation s/zip betweenactivity score and number ofpatients treatedfor serious Grates'oplit/alnmiopat/ v.
= treatment success
=3 treatment failure
8 9 1o
I
I*-11 V11" VZ1,t ;z<|v 141/ I
on 7 June 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.8.639 on 1 August 1989. D
ownloaded from

Clinical criteria ofdisease activity in Graves' ophthalmopathy
helpful in predicting the therapeutic outcome ofimmunosuppressive treatment in Graves' ophthal-mopathy. In patients with an activity score of zero nochange of the ocular condition could be demon-strated. Patients with a pretreatment activity score ofless than 2 points showed no improvement, whereaspatients with 3 or more points did improve onimmunosuppressive treatment. In patients with anactivity score of 2 points the result of this treatmentcould not be predicted.
Discussion
We propose a classification system for disease activityof Graves' ophthalmopathy which is easily manage-able and entirely clinical, making it applicable with-out the use of special instruments. For this reason,the item 'heat' (Latin: calor), also one of the classicalsigns of acute inflammation, has been omitted, as theexaminer would have difficulty diagnosing it withoutsophisticated instruments.
In the past patients have been treated with steroidsand radiotherapy because of serious but not neces-sarily active Graves' ophthalmopathy. Our studysuggests a positive correlation between our clinicalactivity score and a final favourable therapeuticoutcome. This implies that patients with an activityscore of 3 or more can expect beneficial effects frommedical treatment. Those with a zero activity scoreshould be spared from radiotherapy or steroids,of which the substantial side effects must not beforgotten.'4 They should be treated surgically. It isgenerally accepted that a period of at least six monthshas to elapse before surgical procedures can beapplied, provided that no change in the NOSPECSclassification has been observed. With our classifica-tion system this period may be considerably reduced.After two clinical examinations a few months apartdisease activity can be assessed.
Support for the need of the above mentionedclassification system can be derived from the litera-ture. In 1969 Werner,'5 as chairman of the AmericanThyroid Association ad hoc committee on eyedisease, introduced the NOSPECS classificationsystem for Graves' ophthalmopathy to summarisethe most important symptoms once the diagnosis hadbeen made. This system was modified in 1977.6IAlthough Werner's classification has been demon-strated to be of value for studying series of patientswith comparable Graves' ophthalmopathy and fordefining 'success and failure' in the treatment of thedisease, it does not provide a means of distinguishinginflammatory progressive from non-inflammatorystationary Graves' ophthalmopathy. It is therefore ofno help in deciding how and when to treat a patient.This is substantially illustrated by Figs. 1 and 3. Both
patients had the same NOSPECS classification(namely, 2/2, 3/1, 4/2, 5/0, 6/0). The first patient (Fig.1) clearly had active Graves' disease, the second hadnot.Van Dijk,5 questioning the fact that the modified
NOSPECS classification system no longer alloweddisease activity to be specified, has proposed a secondmodification of the original classification, including arestoration of the listing of soft tissue signs. For class2 he introduced the mnemonic RELIEF, trying toinclude designators of activity of the orbital processin the NOSPECS classification system. Although weagree that some of his designators clearly describeactivity (for example, oedema of the caruncule,conjunctiva, and eyelid, and redness of the con-junctiva), other important symptoms and signs areomitted (for example, pain, redness of the eyelid,increase in proptosis, and impaired function), whilefinally two signs of questionable usefulness arementioned (namely, resistance to retrodisplacementof the eye and lacrimal gland enlargement). We donot contest that these signs actually may occur inGraves' ophthalmopathy, but why should theyindicate disease activity? Besides, according to Fruehet al. ' digital estimation of the resistance to retropul-sion does not reliably suggest the measured forces.We believe that only eyelid swelling caused byoedema can be considered as a sign of activity, whilefullness caused by a fat prolapse or infiltrationcannot.
Kahaly et al. determined an activity score fromthe patient's history, clinical findings, and results oflaboratory and imaging techniques. In this systemsigns and epiphenomena, such as eyelid closure andphotosensitivity, are confused. while unchangingdouble vision and proptosis are included as signs ofactivity.
Sergott et al.," attempting to devise a diseaseactivity index for Graves' ophthalmopathy tocorrelate with immunological parameters, found fiveclinical signs the best indicators of active, progressiveophthalmopathy. We have objections against two ofthese indicators. The sign of resistance to retrodis-placement has been discussed above. From ourclinical experience we conclude that dilated bloodvessels over the insertions of the horizontal extra-ocular muscles are a sign of both progressive andquiescent Graves' ophthalmopathy.
In our classification of disease activity we did notmention loss of colour vision because we considerthat testing patients with Ishihara pseudoisochro-matic colour plates gives less reproducible results anddoes not provide more information than alreadygathered by testing the visual acuity.
Although we are aware of the limitations of ourpilot study, the results encouraged us to start a
643
on 7 June 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.8.639 on 1 August 1989. D
ownloaded from

M Ph Mourits, L Koornneef, WM Wiersinga, M F Prummel, A Berghout, and R v d Gaag
prospective study to show that our classificationsystem is easily managed and increases the successrate of anti-inflammatory treatment in active.Graves'ophthalmopathy.
We thank Mr P Y Moriarty, ophthalmic surgeon, for carefullyreading and commenting on the manuscript.
References
1 Jacobson DH, Gorman CA. Endocrine ophthalmopathy:current ideas concerning etiology, pathogenesis and treatment.Endocr Rev 1984: 5: 200-20.
2 Gorman CA. Ophthalmopathy of Graves' disease. (Editorial.)N Engl J Med 1983; 308: 453-5.
3 van Dijk HJL. Orbital Graves' disease. A modification of the'NOSPECS'-classification. Ophthalmology 1981; 88: 479-84.
4 Brian R. Cortisone in exophthalmos: report on a therapeutictrial of cortisone and corticotrophin (ACTH)) in exophthalmosand exophthalmic ophthalmoplegia by a panel appointed by theMedical Research Council. Lancet 1955; i: 6-9.
5 Day RM, Caroll FD. Corticosteroids in the treatment of opticnerve involvement associated with thyroid dysfunction. TransAm Ophthalmol Soc 1967; 65: 41-51.
6 McCohany WH. The eye and orbit in thyroid disease. New York:Raven Press, 1984: 317-23.
7 Wiersinga WM, Smit T, Schuster-Uitterhoeve AJL, van derGaag R, Koornneef L. Therapeutic outcome of prednisone andof orbital irradiation in patients with severe Graves' ophthalmo-pathy. Ophthalmologica 1988X;197: 75-84.
8 Hurbli T, Char DH, Harris J, Weaver R, Greenspan F, ShelineG. Radiation therapy for thyroid eye disease. Am J Ophthalmol1985; 99: 633-7.
9 Sergott RC, Felberg NT, Savino PJ, Blizzard JJ, Schatz NJ.Graves' ophthalmopathy-immunologic parameters related tocorticosteroid therapy. Invest Ophthalmnol Vis Sci 1981; 20: 173-83.
It) DeSanto LW. Transantral orbital decompression. In: GormannCA, Wailer RR, Dyer JA, eds. The eye and orbit in thyroiddisease. New York: Raven Press, 1984: 236.
11 Char DH. Eye signs and diagnosis of thyroid ophthalmopathy.In: Gardner J, Vaughn V, Powell L, eds. Thyroid eye disease.Baltimore: Williams and Wilkins, 1985: 37.
12 Koornneef L. Eyelid and orbital fascial attachments and theirclinical significance. Eye 1988: 2: 13(04.
13 Gilbard JP, Linsy Farrir R. Ocular surface drying and tear filmosmolarity in thyroid eye disease. Acta Ophthalmol (Kb/h) 1983:61: 108-16.
14 Prummel MF, Mourits MPh, Wiersinga WM, et al.. Cyclo-sporine versus prednisone in the treatment of severe Graves'ophthalmopathy. Preliminary results. (Abstr.) In: University ofTexas Health Science Center, ed. The second internationalcongress on cyclosporine. Washington DC, 1987: 92.
15 Werner SC. Classification of the eye changes of Graves' disease.J Clin Endocrinol Metab 1969; 29: 782-4.
16 Werner SC. Modification o)f the classification-of the eye changesof Graves' disease. Am J Ophthalmol 1977: 83: 725-7.
17 Frueh BR, Musch DC, Grill R, Garber F, Hamby S. Orbitalcompliance in Graves' eye disease. Ophthalmology 1985; 92:657-65.
18 Kahaly G, Schrezenmeir J, Krause U, et al. Cyclosporine andprednisone.v. prednisone in treatment of Graves' ophthalmo-pathy, a controlled randomized and prospective study. Eur J ofClin Invest 1986; 16: 415-22.
Accepted for publication 24 November 1988.
644
on 7 June 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.8.639 on 1 August 1989. D
ownloaded from


![Ophthalmopathy of Graves' Disease: Computerized Volume ... · Graves' disease may occur in patients without hyperthyroidism (euthyroid ophthalmic Graves' disease [EOGO]) as well as](https://img.pdfslide.us/doc/110x75/5cd55f0188c993f06f8c3abe/ophthalmopathy-of-graves-disease-computerized-volume-graves-disease-may.jpg)