Embed Size (px)
Citation preview

Clinical Conference on Allergic Disease
Adrian Casillas, MD
Division of Clinical Immunology and Allergy
UCLA School of Medicine

ALLERGIC RHINITIS
• Affects 20-40 million Americans (15-20% of the
Population)
- Predominantly Older Adolescents and Young Adults
• 5th Most Common Chronic Illness
• Significant Impact on Quality of Life, Productivity,
Healthcare Costs
• Prevalence is Increasing

IMPACT OF ALLERGIC RHINITIS
• 28 Million Restricted Activity Days Each Year
• 6 Million Bedridden Days Each Year
• 2 Million Lost School Days Each Year
• 3.5 Million Lost Work Days Each Year
• Can Be a Factor in Other Illnesses
(Asthma, Chronic Sinusitis, Otitis Media with Effusion,
Nasal Polyposis, Upper Respiratory Infections)


Hypersensitivity States

The Allergic Response
• Susceptibility (approximately 25-30% of population)
• Allergen exposure
• IgE induction
• Effector cells of allergic inflammation: Mast cells, Basophils, and Eosinophils

Allergic Sensitization

Presentation ofAllergic Rhinitis: Clues
Reprinted from:Skoner et al. In: Zitelli et al. Atlas of Pediatric Physical Diagnosis. 1997. By permission of the publisher Mosby-Wolfe.
Nasal Nasal itchingitching
Mouth Mouth breathingbreathing
Repeated Repeated nose nose rubbing rubbing (“allergic (“allergic salute”)salute”)
AllergicAllergicshinersshiners

Classification of Rhinitis
• Allergic rhinitis– Seasonal– Perennial– Both
• Nonallergic rhinitis– Perennial nonallergic rhinitis
(idiopathic/vasomotor)– Infectious– Rhinitis medicamentosa– Hormonal– Anatomical
American Academy of Allergy, Asthma and Immunology. The Allergy Report. http://www.aaaai.org/. Accessed: April 13, 2000.

Prevalence of Allergic Rhinitisby Age Group

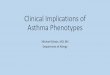
In Chronic Rhinitis, Nonallergic Rhinitis Is a Major Causative Factor
Pure Nonallergic RhinitisPure Nonallergic Rhinitis23%23%
Pure Allergic RhinitisPure Allergic Rhinitis43%43%
Mixture of Both Allergic andMixture of Both Allergic andNonallergic RhinitisNonallergic Rhinitis
34%34%
Settipane et al. In: Kaliner, ed. Current Review of Allergic Diseases. 2000.
National Rhinitis Classification Task Force Survey ResultsNational Rhinitis Classification Task Force Survey Results



Mast Cells and Basophils
Characteristic Mast Cells BasophilsOrigin CD34+
progenitorsCD34+progenitors
Maturation Connective tissue Bone MarrowCirculation No Yes
MajorDevelopmental.Factor
Stem Cell Factor IL3
Life Span Weeks to months Days
FcRI High High

EosinophilsCharacteristic Eosinophils
Origin CD34+ progentor
Maturation Bone marrow
Circulation Yes
MajorDevelopmentalFactor
IL5
Life span Days to weeks
FcRI Low levels

IgE-Dependent Mast Cell Activation
Ca++
Phosphodiesterase
Ca++
cAMP
AA
LTs PGs
Preformed MediatorsAg


Direct Activation of Mast Cells and Basophils (not dependent on
IgE)• Complement:C3a, C5a
• Neuropeptides
• Opiates:Morphine, codeine
• Radiocontrast dyes (ionic)
• Muscle relaxants
• Physical stimuli: vibration, light, temperature changes.


Major Biological Effects of Leukotrienes
LTC4, LTD4 and LTE4
• contraction of smooth muscle,bronchioles and coronary arteries• vasoconstriction with leakage from postcapillary venules and edema
formation• phospholipase A2 stimulation with subsequent prostaglandin and
thromboxane release• secretion of mucus in the respiratory tract
• potent chemotactic mediator that regulates leukocyte function• increases vascular permeability with exudation of plasma• induces lymphocyte transformation into suppressor or cytotoxic T cells
LTB4
Larsen,JS;Acosta,EP. Ann PharmacolJuly/Aug 1993


Mediators Eosinophils
Preformed Major basic protein, ECP,neurotoxin, EPO,lysophospholipase
Lipid mediators (newlyformed)
LTC4
Cytokines IL1a, IL2, IL3, IL4, IL5,IL6, IL8, IL10, GMCSF,TNFa, RANTES, MIP1a,etc

Allergic Mechanisms in Health and Disease
• Immediate hypersensitivity
• Late phase reactions-follows immediate reaction by about 4 to 8 hours and is characterized by swelling and leukocyte infiltration
• Parasitic diseases-Trichinella spiralis and Strongyloides ratti infections are longer in mast cell deficient mice. Resolution of ectoparasite (i.e. ticks) infections also depend on basophil/mast cell activation

Induction of Allergic Sensitization
APC
APC
Allergen
IL-12, IFN-
Tnaive
IL4, IL10
T-1
T-2
B
IFN-
Mast
Mediators of allergic response
IgE
IL-4 IL-4
EosIL-5
IL-4

Role of IgE in Atopic Disease
AsthmaAdapted from Cochrane GM, Jackson WF, Rees PJ.
IgE PRODUCTION
Allergen
Second allergen
encounter
IgE
GranulesB-cell
Mast cellFirst exposure to antigen
MAST CELL SENSITIZATION
DEGRANULATION REACTION
Chemical mediators induce hay fever, eczema, asthma


Diagnosis of Allergic Rhinitis: History
Family history of atopy
Personal history of other allergenic conditions
– Asthma
– Atopic dermatitis
– Food hypersensitivity
Personal history of
– Long-lasting or recurrent colds
– Chronic sinusitis
– Frequent ear infections
– Chest symptoms (e.g., pain or wheezing)

Allergic Rhinitis: Physical Examination
Allergic facies (e.g., shiners, transnasal crease)
Pale, edematous nasal mucous membranes; clear, watery nasal discharge
Watery, swollen, red eyes
Wheezing, noticeable cough
Middle ear fluid, eustachian tube dysfunction
Tenderness over the sinuses
Eczema

Environment and Genetics in Allergic Disease

Genetic Factors
• Monozygous twins show a 70% concordance rate for an IgE response to any common allergen.
•Statistically significant genetic linkages identified for a number of genes, for example:
• IL-4 gene cluster (chr. 5) polymorphism related to high IgE production and asthma
•Variants of the high affinity IgE receptor (chr. 11) on mast cells and basophils

Why the increased prevalence?
Evidence for environmental effects on atopic disease

• Increase in levels of indoor allergen loads--”tighter” homes
• Dietary changes--too much controversy to accept
• Microbial exposure
Relationship between atopic state and
1. Lack of immunity to HAV
2. Vaccination to measles
3. Negative DTH reaction to TB
(these are all intracellular diseases which would stimulate a Th1 response and downregulate a Th2 (favoring atopy) response)
Other theories for increase in atopic disease prevalence

Diagnostic Tests for Allergic Disease

Allergic Rhinitis: Diagnostic Testing
Skin tests for specific IgE antibodies
– Confirm allergens suspected by history
Serum-specific IgE tests
– Correlate well with skin tests
– Not as sensitive as skin tests
Nasal cytology
– Eosinophils, basophils imply allergy or
NARES syndrome*
– Neutrophils suggest bacterial infection
*Nonallergenic rhinitis with eosinophilia syndrome.

•Rast Testing--detects the presence of preformed IgE in a patient’s serum
•Less sensitive than skin tests
•May take several days to get results
RAST or ELISA Tests

Rast Testing
• Use when it is not possible to skin test
Immobilized Ag + Patient’s
serum
+
Tagged anti-human IgE
Colorimetric assay

- RAST HONEY BEE VENOM IGE 144 count 0-500 - RAST PAPER WASP VENOM IGE ALL @ 808 count 0-500 - RAST WHITE-FACE HORNET VENOM 220 count 0-500 - RAST YELLOW HORNET VENOM IGE 212 count 0-500 - RAST YELLOW JACKET VENOM IGE @ 2739 count 0-500 - Allergen Interpretation Range - IgE counts Score Interpretation - 0-500 0 No antibodies detected - 501-750 0-1 Low equivocal - 751-1600 1 Equivocal - 1601-3600 2 - 3601-8000 3 Scores 2-6 indicate - 8001-18000 4 increasing levels - 18000-40000 5 of antibody - 40000+ 6

Skin testing• Quicker and cheaper that RAST
• A physiological test that detects the presence of sensitized mast cells within in a patient’s dermis
• Refer to experienced allergist
• Prick vs Intradermal--start with prick although less sensitive, it is safer since intradermal introduces 103 to 104 more antigen to the patient

Skin Testing
Photographs courtesy of Dr. Ed Philpot.



Treatment
I. Avoidance
II. Pharmacotherapy
III. Immunotherapy
IV. Psychotherapy

I. AVOIDANCE

Environmental Control Measures
• Keep windows/doors closed during the allergy season
• Reduce outdoor activity during high pollen days
• Maintain a dust/allergen-free environment• Keep pets outdoors• Avoid smoke and strong odors• Use air conditioning and/or air filters
Druce. In: Middleton et al, eds. Allergy Principles & Practice. 1998.

Potentially Avoidable Environmental Allergens
– Molds
– Cockroaches
– Dust mites
– Pet dander

Dust Mites

Dust mites• Dust mite covers
• Wash sheets/covers in HOT water
• Diminish humidity
• Vacuum with HEPA filter
• Move to Taos, NM

Cats
•Keep out of bedroom
•Wash frequently
•Wash once (permanently)

Cat allergen--Fel D1saliva and skin, not hair

Compliance With Environmental Control Measures
•Response %
Dust my house frequently 34.1
Do not have pets inside my house 20.8
Avoid outdoor activities 18.7
Wash bedding in hot water 15.0
Wrap mattresses in plastic cover 6.0
Do not have carpeting (or rugs) in my house 2.1
No measures 25.4
Note: Respondents (481 patients with self-reported allergic rhinitis) were asked to check all items that apply.

II. PHARMACOTHERAPY

Allergic Rhinitis: Pharmacotherapy
OTC treatments• Intranasal cromolyn sodium• Intranasal decongestants• Intranasal saline• Oral antihistamines• Oral decongestants
Rx treatments• Antihistamines
– Intranasal– Systemic
• Decongestants– Systemic
• Corticosteroids– Intranasal– Systemic
• Anticholinergics– Intranasal
• LT receptor antagonists
This table lists the various classes of pharmacotherapy This table lists the various classes of pharmacotherapy available to treat allergic rhinitis.available to treat allergic rhinitis.
American Academy of Allergy, Asthma and Immunology. The Allergy Report. http://www.aaaai.org/. Accessed: April 13, 2000.

First-generation Antihistamines
H1 Sedative Anticholinergic GI Blockade Effects Effects Effects
Ethylenediamines +++ ++ ++ ++(tripelennamine)
Ethanolamines +++ +++ +++ +(diphenhydramine)
Alkylamines +++ + ++ + (chlorpheniramine)
Piperazines +++ ++ ++ +(hydroxyzine)
Piperidines +++ ++ ++ +(azatadine)
++++ Strongly positive effects

Second-generation Antihistamines
H1 Sedative Anticholinergic GI Blockade Effects Effects Effects
Fexofenadine +++ – – – (60 mg bid)
Astemizole ++++ – – – (10 mg qd)
Loratadine +++ – – – (10 mg qd)
Cetirizine +++ + – – (10 mg qd)
– Negative effect
++++ Strongly positive effect

Advantages of Second-generation Nonsedating Antihistamines
• Bind strongly to histamine (H1) receptors
• negligible affinity for nonhistamine receptors
• no anticholinergic effects
• Do not cross the blood-brain barrier• do not affect cognitive functions
or psychomotor performance
• do not potentiate impairment caused by alcohol or benzodiazepines
• do not impair driving skills

Decongestants
• Actions– Constrict mucous membranes: shrinkage promotes drainage,
improves ventilation, relieves nasal stuffiness
• Routes of administration– Systemic, topical
• Indications– Allergic rhinitis, vasomotor rhinitis, sinusitis, eustachian tube
congestion
• Side effects– Systemic: stimulation (CNS, cardiovascular)– Topical: rhinitis medicamentosa, CNS stimulation, local irritation

Primary CarePrimary Care(including Internal Medicine)(including Internal Medicine)
ENTENT
AllergistAllergist
PediatricianPediatrician
All OthersAll Others
PrescriptionPrescriptionAntihistaminesAntihistamines
72.2%72.2%
50.7%50.7%
63.5%63.5%
72.4%72.4%
73.9%73.9%
IntranasalIntranasalCorticosteroidsCorticosteroids
27.8%27.8%
49.3%49.3%
36.5%36.5%
27.6%27.6%
26.1%26.1%
IntranasalIntranasalCorticosteroidsCorticosteroids
10.8%10.8%
4.2%4.2%
4.9%4.9%
14.3%14.3%
9.8%9.8%
Source: SourceTM Prescription Audit (SPA). MAT August 2000. Scott-Levin, Inc.
% of Use% of Use
Intranasal Corticosteroid Use Is Increasing
% incr vs% incr vs previous yrprevious yr

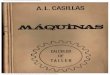
Absence of red-Absence of red-stained cells is stained cells is evidence of a evidence of a reduction in reduction in mast-cell mast-cell infiltration after infiltration after 1 year of therapy 1 year of therapy with fluticasone.with fluticasone.
Before TreatmentBefore TreatmentAfter 52 weeks After 52 weeks
of Treatmentof Treatment
The direct relationship of these findings to long-term symptom relief is unknown.The direct relationship of these findings to long-term symptom relief is unknown.
[Magnification: x100][Magnification: x100]
Reduction in the Infiltration of Mast Cells

The Fate of Intranasal Steroids
Adapted from: Allen. J Allergy Clin Immunol. 2000.

Allen. J Allergy Clin Immunol. 2000.
Fate of Intranasal Steroids• Majority of nasal steroid administered is
swallowed• Systemic bioavailability is determined primarily
by the amount of swallowed drug — not inactivated by first-pass hepatic inactivation — that subsequently reaches the circulation
• Factors such as lipophilicity affect the amount of drug that is absorbed across the nasal mucosa– Drugs with higher lipophilicity have lower absorption

The esterified The esterified carbothioate carbothioate
moleculemoleculefluticasone fluticasone propionatepropionate
The major metabolite of fluticasone propionate, 17ß-carboxylic acid, wich is devoid of glucocorticoid activity because of the loss of ester at C17ß.
Fluticasone propionate undergoes first-pass metabolism in the liver, being rapidly hydrolysed to the corresponding 17ß-carboxylic acid (GR36264).

III. IMMUNOTHERAPY

HISTORY OF ALLERGEN IMMUNOTHERAPY
1819: Bostock described his personal experience of having hayfever.
1889: Seventy years later, Wyman identified pollen as a cause of fall hayfever.
1890: Blackley identified grass pollen as the cause of his seasonal rhinitis.
1900: Curtis reported beneficial effects from the injection of aqueous pollen extracts for rhinitis and asthma.
1911: Freeman published data suggesting decreased symptoms in patients with allergic rhinitis treated with grass extract--“desensitization.”


Immunological Changes in Allergen Immunotherapytherapy • Diminished leukocyte histamine release
sensitivity with allergen challenge
• Diminished lymphoproliferative response to allergen
• Stimulation of Allergen specific CD8+ lymphocytes
• Decreased tissue CD4+ lymphocytes

Immunological Changes (cont)
• Blunted IL2 production to antigen
• Increased IFN g production
• Down regulation of the low affinity IgE receptor
• Decreased recruitment and activation of tissue eosinophils

DISEASES IN WHICHIMMUNOTHERAPY IS EFFECTIVE
1. Allergic Rhino-Conjunctivitis
2. Allergic Asthma
3. Hymenoptera Hypersensitivity

Some patients have unrealistic expectations from treatment.
IV. PSYCHOTHERAPY

Key Points
• Allergic (atopic) disease is one type of hypersensitivity state that depends on IgE production
• AR and asthma are characterized by early and late phase reactions due to rapidly released medators and newly formed AA metabolites.
• Th cell differentiation along a Th2 pathway favors allergic disease development

Key Points(cont.)
• Diagnostic tests for atopic deseases can be physiologic or simply measure preformed IgE
• IT is effective in part due to alterations in allergen specific antibody formation

*P < 0.01 for prednisone vs placebo, FP ANS 200 mcg QD, and FP ANS 400 mcg QD
Vargas et al. J Allergy Clin Immunol. 1998.
Pre-Infusion 2 4 6 Post-Infusion
0
10
20
30
40
Placebo Fluticasone 200 mcg QD
Fluticasone 400 mcg BID
Prednisone 7.5 mg QD
Prednisone 15 mg QD
Cosyntropin Infusion Time (hr)
Mea
n P
lasm
a C
ort
iso
l (m
cg/d
l)Stimulation Challenge
After 4 Weeks of Therapy
*
****
**
Cortisol Levels Comparable to Vehicle Placebo After Treatment With Futicasone