Embed Size (px)
Citation preview
Clinical concepts for regenerativetherapy in intrabony defectsPIERPAOLO CORTELLINI & MAURIZIO S. TONETTI
Periodontal-regenerative technologies are applied toimprove the short- and long-term clinical outcomesof periodontally compromised teeth presenting withdeep pockets and reduced periodontal support. Thepersistence of deep pockets following active peri-odontal therapy has been associated with anincreased probability of tooth loss in patients attend-ing supportive periodontal-care programs (81). Teethwith deep pockets associated with deep intrabonydefects are considered a clinical challenge. Mostauthors have classified such teeth as having either aquestionable or a hopeless prognosis. Key elementsto support these opinions are the complex interplayof a reduced residual periodontal attachment, deeppocketing, functional demands and frequently thedegree of residual tooth mobility (70, 72, 84, 85). It istherefore clear that the possibility of changing theprognosis of a tooth from ‘questionable’ or ‘hopeless’into ‘fair’ or ‘favorable’ would greatly help cliniciansand patients in the difficult job of maintaining teethover time, and the possibility of gaining periodontalsupport would help patients improve their comfortand function.
The aims of periodontal regeneration are to obtain:(i) an increase in the periodontal attachment andbone of a severely compromised tooth; (ii) a decreasein pocket depth; and (iii) no, or a minimal, increase ingingival recession. Periodontal regeneration has beenshown to be effective in the treatment of one-, two-and three-wall intrabony defects, or combinationsthereof, from very deep to very shallow, and fromvery wide to very narrow (43, 44, 90, 91). However, theapproaches used currently are technique sensitiveand are burdened by a significant amount of clinicalfailures or incomplete success. At present, we knowthat most failures of regenerative therapy have anexplanation in terms of negative patient factors,suboptimal use of surgical approaches and materi-als, and insufficient clinical skill and experience of
the surgeon (26). Clinical success requires applica-tion of meticulous diagnostic and treatment strate-gies (26, 31). The aims of this narrative review wereas follows: first, to review the current scientific lit-erature highlighting the strengths and weaknessesof periodontal-regenerative approaches in intrabonydefects; second, to discuss the patient, defect andsurgery-associated factors that have an impact onclinical outcomes; and, third, to propose a step-by-step clinical approach in order to build up a scien-tifically sound strategy to optimize the clinical out-comes in different patients and in different defectanatomies.
Evidence for clinical efficacy andeffectiveness
Questions of efficacy relate to the added benefit of atreatment modality under ideal experimental condi-tions (such as those of a highly controlled research-center environment). Effectiveness, on the otherhand, relates to the benefit that can be achieved, inrelation to morbidity and adverse events, in a regularclinical setting where the procedure is likely to be per-formed. Besides efficiency considerations, evidencefor both efficacy and effectiveness need to be avail-able in order to provide support for the adoption oftreatment approaches in clinical practice.
The clinical efficacy of periodontal-regenerativeprocedures has been extensively evaluated in ran-domized controlled clinical trials that have comparedregenerative procedures with a standard access flapapproach. To limit sample size and study duration,these trials have utilized surrogate outcomes – clinicalattachment-level changes, decrease in pocket depths,furcation closure or radiographic measurements –
rather than changes in tooth survival. However, thesesurrogate outcomes are considered to be adequate
282
Periodontology 2000, Vol. 68, 2015, 282–307 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Printed in Singapore. All rights reserved PERIODONTOLOGY 2000

proxies of the true outcome represented by tooth sur-vival: the persistence of deep pockets or furcationinvolvement are associated with a higher risk of peri-odontal breakdown and tooth extraction.
The majority of reported clinical trials have beensmall, single-center studies, with only a few beinglarger multicenter clinical trials. The evidence fromthese studies has recently been summarized inmeta-analyses performed on data retrieved by sys-tematic reviews of the published literature. In 2002,2003 and 2008, the European Workshop on Peri-odontology (held by the European Federation ofPeriodontology) and the Workshop on EmergingTechnologies in Periodontics (held by the AmericanAcademy of Periodontology) provided much of thesystematic assessment of the evidence for currentlyavailable technologies. These include the use of bar-rier membranes (guided tissue regeneration), the useof bone-replacement graft materials, the use of bio-logically active regenerative materials and the use ofcombinations of the aforementioned materials/agents.
Evidence for clinical efficacy of barrier membranesin intrabony defects was assessed in the systematicreviews and meta-analyses performed by Murphy &Gunsolley (90) and Needleman et al. (91). The latterreported a significant added benefit of the use of bar-riers on top of open flap debridement alone in termsof clinical attachment level gain (16 studies) andprobing pocket-depth reduction (11 studies). Theresults of large prospective multicenter studies in pri-vate practice settings (28, 134) conclusively supportthe additional benefit of membranes in reducingpocket depth and improving clinical attachment lev-els and bone levels in intrabony defects and thus theirefficacy and effectiveness.
The efficacy of bone-replacement graft materialshas been assessed in two systematic reviews per-formed by Trombelli et al. (141) and Reynolds et al.(106). As these two systematic reviews used signifi-cantly different criteria for study inclusion, the resultsdid not show complete agreement. Trombelli et al.(141), who included only controlled studies thatreported changes in clinical attachment level as theprimary outcome, concluded that there was insuffi-cient evidence to support the clinical use of bone-replacement graft materials in intrabony defectsbecause there was significant heterogeneity amongincluded studies, the size of the adjunctive effect wassmall and not statistically significant and there weredifferences that did not allow pooling of resultsobtained with different materials. In the othersystematic review for intrabony defects, 27 controlled
trials with 797 intrabony defects were included(106). The clinical efficacy of allografts in terms ofbone fill and clinical attachment level gains wassupported by a meta-analysis indicating that anadditional bone fill of 1 mm and additional clinicalattachment level gains of 0.4 mm were achievedcompared with an access flap control (106). How-ever, the total number of defects contributing tothis meta-analysis was relatively small (136 for clini-cal attachment level gain and 154 for bone fill).Furthermore, no large-scale multicenter trial onallografts has ever been performed and hence theapplicability of these results to clinical practicesettings remains to be established.
The evidence of clinical efficacy of biologicallyactive regenerative materials in intrabony defects hasbeen summarized, through the years, in meta-analy-ses only for enamel matrix derivative (43, 44, 47,141). The outcomes of eight studies, including 444defects, have indicated that enamel matrix derivativeprovides significant additional benefits in terms ofpocket-depth reduction, clinical attachment levelgain and radiographic bone level. These data are inaccordance with those of a large practice-based mul-ticenter trial that demonstrated both efficacy andeffectiveness of enamel matrix derivative in intra-bony defects (135).
Combination therapy has been explored in tworecent meta-analyses. Trombelli & Farina (142) evalu-ated the clinical effects of the use of bioactive agentswhen used in addition to open flap debridement,either alone or in association with grafts and/or bar-rier membranes. The authors concluded the follow-ing: there was evidence to support the use ofamelogenins, either alone or in combination withgrafts, to treat intra-osseous defects effectively andthe additional use of a graft seemed to enhance theclinical outcome of amelogenins; the combined useof recombinant human platelet derived growth fac-tor-BB and peptide P-15 with a graft biomaterialshowed beneficial effects in intra-osseous defects;and contrasting results were reported for platelet-richplasma and graft combinations.
Tu et al. (145) explored the additional treatmenteffect of barriers or bone grafts compared with ame-logenins alone in 28 studies. Amelogenins plus bonegrafts and amelogenins plus membranes attained0.24 and 0.07 mm more probing pocket-depth reduc-tion, respectively, compared with amelogenins alone,and amelogenins plus bone grafts and amelogeninsplus membranes attained 0.46 and 0.15 mm, respec-tively, of clinical attachment level gain. When differ-ent types of bone grafts and barrier membranes were
Clinical concepts for regenerative therapy in intrabony defects
283

treated separately, amelogenins with bovine bonegrafts showed greater treatment effects. The authorsconcluded that there was little evidence to supportthe additional benefits of amelogenins in conjunctionwith other regenerative materials.
Support for the clinical use of growth factors comesfrom two multicenter studies on recombinant humanplatelet-derived growth factor-BB and two on fibro-blast growth factor-2. In one multicenter trial (92),180 defects (comprising both intrabony and furcationdefects) were treated with either one of two concen-trations of human platelet-derived growth factor-BB(0.3 and 1.0 mg/ml) combined with the beta-trical-cium phosphate delivery device or with tricalciumphosphate alone. Clinical attachment level gains at6 months failed to demonstrate a significant benefitof either concentration of platelet-derived growth fac-tor compared with the bone replacement graft alone.However, with regard to radiographic assessments,the lower concentration of platelet-derived growthfactor resulted in significantly higher percentages ofradiographic bone fill of the defect (57% vs. 18%) andlinear radiographic bone growth (2.6 vs. 0.9 mm). Inthe other multicenter trial on recombinant humanplatelet-derived growth factor-BB, Jayakumar et al.(71) studied 54 patients who were treated with humanplatelet-derived growth factor-BB1b combined withthe beta-tricalcium phosphate delivery device or tri-calcium phosphate alone. Clinical attachment levelgain, bone growth and percentage bone fill at6 months were significantly greater in the test groupcompared with the tricalcium phosphate controlgroup.
A study on 74 patients (68) compared three differ-ent concentrations of fibroblast growth factor-2 vehi-cle with 3% hydroxypropylcellulose and withhydroxypropylcellulose alone. No difference wasreported in terms of clinical attachment level gainbetween test and control groups. A significant differ-ence in terms of bone gain was reported in favor ofthe 0.3% concentration of fibroblast growth factor-2compared with hydroxypropylcellulose alone. Noadvantage, in terms of bone gain, was observed withthe other two concentrations of fibroblast growth fac-tor-2 (0.03% and 0.1%). A second randomized, dou-ble-blind, placebo-controlled clinical trial on 253adult patients was performed, in which 0.2, 0.3 or0.4% fibroblast growth factor-2 was compared withvehicle alone in two- or three-walled vertical bonedefects (69). Each concentration of fibroblast growthfactor-2 showed significant superiority over vehiclealone (P < 0.01) for the percentage bone fill 36 weeksafter administration. No significant differences
among groups were observed for clinical attachmentgain. No clinical safety problems were reported in anyof the four cited studies. Drawing conclusions fromthe four studies, it is apparent that both of the growthfactors tested resulted in a measurable added benefitcompared with controls in terms of bone gain,whereas three out of four did not induce a significantdifference in terms of clinical attachment level gain.Both efficacy and effectiveness of human platelet-derived growth factor-BB1b and fibroblast growthfactor-2 have to be further explored before clinicalapplication.
A recent controlled study evaluated, clinically andhistologically, wound healing/regeneration followingsurgical implantation of recombinant human growth/differentiation factor-5 adsorbed onto a particulatebeta-tricalcium phosphate carrier into periodontaldefects in 28 patients (128). Control defects were trea-ted with open flap debridement alone. The authorsreported greater probing pocket-depth reduction andclinical attachment level gain, and greater alveolarbone regeneration and periodontal regeneration atsites that received recombinant human growth/dif-ferentiation factor-5/beta-tricalcium phosphate com-pared with control sites. However, these differenceswere not statistically significant.
Block biopsies of the defect sites were collected6 months postsurgery. Histologically, bone regenera-tion height was almost threefold greater for therecombinant human growth/differentiation factor-5/beta-tricalcium phosphate treatment compared withopen flap debridement alone (2.19 � 1.59 vs.0.81 � 1.02 mm, respectively; P = 0.08). Similarly, anincrease of almost twofold was observed for peri-odontal ligament (2.16 � 1.43 vs. 1.23 � 1.07 mm,respectively; P = 0.26), cementum (2.16 � 1.43 vs.1.23 � 1.07 mm, respectively; P = 0.26) and boneregeneration area (0.74 � 0.69 vs. 0.32 � 0.47 mm2,respectively; P = 0.14). Root resorption/ankylosis wasnot observed. Future studies with larger sample sizeswill have to be conducted to verify these findings.
Comparative studies between different regenera-tive approaches have been analyzed in a systematicreview by Esposito et al. (44). The authors did notfind any difference when comparing amelogeninswith barriers, in terms of clinical attachment levelgain and probing pocket-depth reduction, in the sixstudies examined. These data are supported by twolarge practice-based multicenter trials (110, 123).However, Sanz et al. (110) reported a significantlyhigher prevalence of complications in the barrier-treated group compared with the amelogenin-treatedgroup.
Cortellini & Tonetti
284
Clinical periodontal regeneration
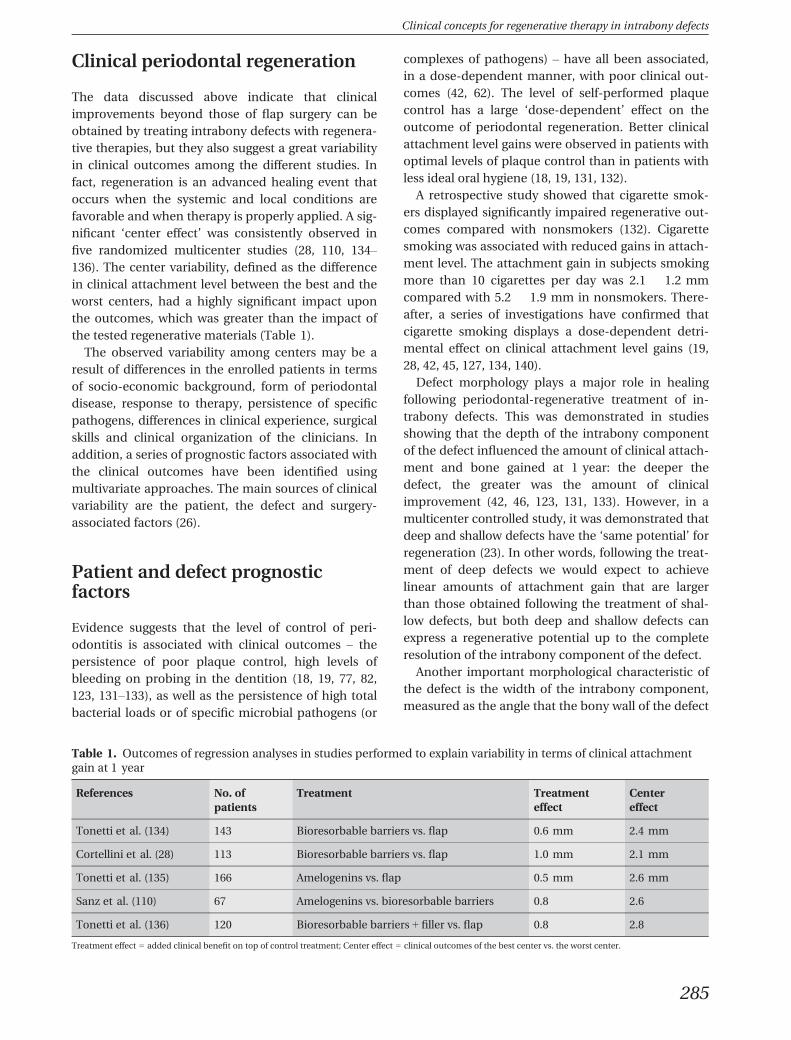
The data discussed above indicate that clinicalimprovements beyond those of flap surgery can beobtained by treating intrabony defects with regenera-tive therapies, but they also suggest a great variabilityin clinical outcomes among the different studies. Infact, regeneration is an advanced healing event thatoccurs when the systemic and local conditions arefavorable and when therapy is properly applied. A sig-nificant ‘center effect’ was consistently observed infive randomized multicenter studies (28, 110, 134–136). The center variability, defined as the differencein clinical attachment level between the best and theworst centers, had a highly significant impact uponthe outcomes, which was greater than the impact ofthe tested regenerative materials (Table 1).
The observed variability among centers may be aresult of differences in the enrolled patients in termsof socio-economic background, form of periodontaldisease, response to therapy, persistence of specificpathogens, differences in clinical experience, surgicalskills and clinical organization of the clinicians. Inaddition, a series of prognostic factors associated withthe clinical outcomes have been identified usingmultivariate approaches. The main sources of clinicalvariability are the patient, the defect and surgery-associated factors (26).
Patient and defect prognosticfactors
Evidence suggests that the level of control of peri-odontitis is associated with clinical outcomes – thepersistence of poor plaque control, high levels ofbleeding on probing in the dentition (18, 19, 77, 82,123, 131–133), as well as the persistence of high totalbacterial loads or of specific microbial pathogens (or
complexes of pathogens) – have all been associated,in a dose-dependent manner, with poor clinical out-comes (42, 62). The level of self-performed plaquecontrol has a large ‘dose-dependent’ effect on theoutcome of periodontal regeneration. Better clinicalattachment level gains were observed in patients withoptimal levels of plaque control than in patients withless ideal oral hygiene (18, 19, 131, 132).
A retrospective study showed that cigarette smok-ers displayed significantly impaired regenerative out-comes compared with nonsmokers (132). Cigarettesmoking was associated with reduced gains in attach-ment level. The attachment gain in subjects smokingmore than 10 cigarettes per day was 2.1 � 1.2 mmcompared with 5.2 � 1.9 mm in nonsmokers. There-after, a series of investigations have confirmed thatcigarette smoking displays a dose-dependent detri-mental effect on clinical attachment level gains (19,28, 42, 45, 127, 134, 140).
Defect morphology plays a major role in healingfollowing periodontal-regenerative treatment of in-trabony defects. This was demonstrated in studiesshowing that the depth of the intrabony componentof the defect influenced the amount of clinical attach-ment and bone gained at 1 year: the deeper thedefect, the greater was the amount of clinicalimprovement (42, 46, 123, 131, 133). However, in amulticenter controlled study, it was demonstrated thatdeep and shallow defects have the ‘same potential’ forregeneration (23). In other words, following the treat-ment of deep defects we would expect to achievelinear amounts of attachment gain that are largerthan those obtained following the treatment of shal-low defects, but both deep and shallow defects canexpress a regenerative potential up to the completeresolution of the intrabony component of the defect.
Another important morphological characteristic ofthe defect is the width of the intrabony component,measured as the angle that the bony wall of the defect
Table 1. Outcomes of regression analyses in studies performed to explain variability in terms of clinical attachmentgain at 1 year
References No. ofpatients
Treatment Treatmenteffect
Centereffect
Tonetti et al. (134) 143 Bioresorbable barriers vs. flap 0.6 mm 2.4 mm
Cortellini et al. (28) 113 Bioresorbable barriers vs. flap 1.0 mm 2.1 mm
Tonetti et al. (135) 166 Amelogenins vs. flap 0.5 mm 2.6 mm
Sanz et al. (110) 67 Amelogenins vs. bioresorbable barriers 0.8 2.6
Tonetti et al. (136) 120 Bioresorbable barriers + filler vs. flap 0.8 2.8
Treatment effect = added clinical benefit on top of control treatment; Center effect = clinical outcomes of the best center vs. the worst center.
Clinical concepts for regenerative therapy in intrabony defects
285

forms with the long axis of the tooth (129). Widerdefects have been associated with reduced amountsof clinical attachment level and bone gain at 1 year(46, 131, 133). In a study on 242 intrabony defectstreated with membranes, Cortellini & Tonetti (24)demonstrated that defects with a radiographic angleof ≤ 25° gained consistently more attachment(1.6 mm on average) than did defects of ≥ 37°. A fol-low-up study addressed the significance of the base-line radiographic angle of the intrabony defectfollowing the use of enamel matrix derivative (144).The analysis revealed a negative association betweenthe radiographic angle of the defect and the clinicalattachment level gains observed at 1 year. Anothersecondary analysis of a multicenter study on a combi-nation of bone replacement graft with a barrier mem-brane, in contrast, has indicated a reduced effect ofthe radiographic angle on clinical attachment gain at1 year (74). Similarly, an earlier secondary analysis ofa controlled clinical trial using titanium-reinforcedexpanded-polytetrafluoroethylene membranes (133)indicated that the negative impact of an unfavorabledefect morphology may be reduced with the use ofsupported membranes. In particular, the width of thedefects was not correlated with the clinical outcomes.
It has also been shown that the number of residualbony walls is correlated with the outcomes of variousregenerative approaches (48, 112). This point, asrelated to regenerative therapy, was addressed in afew investigations with nonresorbable barriers. Inone study, clinical attachment level gain was report-edly related to the number of bony walls (120),whereas, in another study with the same barriers,gains in attachment were not related to the defectconfiguration in terms of one-, two- and three-wallsubcomponents (131). Although the number of wallsdid not result in a significant difference when tita-nium barriers (133) or combination therapy (136, 137)were used, when bioresorbable barriers (45, 123) andamelogenins were used, significant differences werereported (123, 135). In particular, a secondary analysisof a multicenter trial showed that, in intrabonydefects, the added benefit of amelogenins was greaterin three-walled defects than in one-walled defects(135). These data have questioned the suitability ofthe gel formulation of amelogenins for the treatmentof defects with a nonsupporting anatomy (i.e. widedefects with missing bony walls). However, morerecently, two studies demonstrated a reduced impactof the number of residual bony walls and of defectwidth on the outcomes obtained with amelogeninsunder a minimally invasive surgical technique (34,35). This clearly differs from the evidence, discussed
above, of a strong impact of the defect anatomy interms of residual bony walls and defect width on theclinical outcomes when amelogenins were usedunder conventional large, and intrinsically less stable,papilla preservation flaps (135, 136).
The endodontic status of the tooth has been sug-gested as a potentially relevant factor in periodontaltherapy. Cortellini & Tonetti (27), in a clinical studyon 208 consecutive patients who had one intrabonydefect each, demonstrated that when performedproperly, root canal treatment does not negativelyaffect the healing response and the long-term stabilityof results of deep intrabony defects treated with bar-rier membranes.
Tooth mobility has long been considered an impor-tant factor for periodontal regeneration (111). A mul-tivariate analysis of a multicenter controlled clinicaltrial demonstrated that increased tooth mobility isnegatively and dose-dependently associated with theclinical outcomes of regeneration (28). Although sig-nificant, the size of the effect was small within therange of physiologic mobility. The study concludedthat Miller grade III mobility (88) negatively affectsperiodontal regeneration. Another recent secondaryanalysis of three previously reported trials assessedthe regenerative outcomes of mobile teeth (139). Thisreport indicated that teeth with baseline mobilityamounting to < 1 mm horizontally could be success-fully treated by periodontal regeneration.
Based on these results, it can be concluded thatdeep and narrow intrabony defects at either vital orendodontically succesfully treated teeth are those inwhich the most significant and predictable outcomescan be achieved by guided tissue-regeneration treat-ment. The number of walls and the width of thedefect are influential when nonsupportive biomateri-als are used. The influence of defect anatomy appearsto be reduced, to some extent, when a more stabledesign of the flap is applied. Severe, uncontrolledtooth mobility (Miller grade II or higher) (88) mayimpair the regenerative outcomes. Significant clinicalimprovements can be expected only in patients withoptimal plaque control and with reduced levels ofperiodontal contamination, and in nonsmokers.
Surgery-associated factors
Basic and clinical research indicate that the absoluterequirements for successful regeneration include thepresence of space for the formation of the blood clotat the interface between the flap and the root surface(18, 19, 55, 67, 121, 133, 151), the stability of the bloodclot to maintain continuity with the root surface,
Cortellini & Tonetti
286

avoiding formation of a long junctional epithelium(55, 64, 75, 150) and the soft-tissue protection of thetreated area to avoid bacterial contamination (39, 40,94, 95, 110, 119). Development of periodontal-regen-erative medicine in the last 25 years has followed twodistinctive, yet totally intertwined, paths. The interestof researchers has so far focused on regenerativematerials or products on the one hand and on novelsurgical approaches on the other.
Materials for regenerative surgery
In the area of materials and products, three differentregenerative concepts have been explored – barriermembranes, grafts and wound-healing modifiers –
plus many combinations of those. Historically, barriermembranes have been used to mechanically selectthe cells able to repopulate the blood clot (104). Inaddition, barrier membranes also possess the capa-city to provide space and to increase blood-clot sta-bility (104). In the first attempts of guided tissueregeneration, a bacterial filter produced from cellu-lose acetate (Millipore�) was used as an occlusivemembrane (49, 79, 97). Although this type of mem-brane served its purpose, it was not ideal for clinicalapplication. Later studies utilized nonresorbablemembranes of expanded-polytetrafluoroethylenethat were specially designed for periodontal regenera-tion (Gore-Tex Periodontal Material�). This type ofmembrane must be removed in a second operation.Membranes of expanded-polytetrafluoroethylenehave been used successfully in animal experimentsand in several clinical studies (90, 91).
Natural or synthetic bioabsorbable barrier materi-als for guided tissue regeneration were introduced inorder to avoid a second surgery for membraneremoval. Barrier materials of collagen from differentspecies and from different anatomic sites have beentested in animals and in humans (3, 4, 11, 100, 103,130, 149). Barrier materials of polylactic acid or co-polymers of polylactic acid and polyglycolic acid havebeen evaluated in animal and human studies and arecommonly used (9, 12, 22, 28, 50, 52, 66, 73, 80, 114,125, 134).
The biologic principles supporting the use of autol-ogous and heterologous grafts include osteoconduc-tivity and osteo-inductivity, and also their capacityfor space provision and blood-clot stabilization (109,142). Bone-replacement grafts comprise a heteroge-neous group of materials of human, animal or syn-thetic origin. Some consist of bone or exoskeletalmineral, whereas others contain mainly bone matrix.Few materials present evidence of periodontal rege-neration. A randomized controlled clinical trial
provided histological support that the healing out-come following application of demineralized freeze-dried bone allograft in intrabony defects had a regen-erative component in the apical to middle portion ofthe depth of the defect (6–8).
The adoption of biologic products/compounds isbased on their ability to induce or accelerate the pro-cesses of matrix formation and cell differentiation (5).These products enforce the healing process but lackthe mechanical properties to help in the provision ofspace and blood-clot stabilization. Accordingly, someof these products are loaded onto solid, bioresorbablecarriers to provide some mechanical properties (98,142). Currently, two preparations consisting of growthand/or differentiation factors are available for use inperiodontal regeneration: enamel matrix derivative ina gel form; and platelet-derived growth factor mixedin a beta-tricalcium phosphate bone-replacement graft.
Significant pre-clinical evidence supports the posi-tive effect of recombinant human platelet-derivedgrowth factor-BB associated with recombinanthuman insulin-like growth factor-1 on periodontalwound healing and regeneration (65). Support for theclinical use of growth factors comes from two multi-center studies on recombinant human-derivedgrowth factor (71, 92) and two on fibroblast growthfactor-2 (68, 69). Drawing conclusions from the fourstudies, it is apparent that both the tested growth fac-tors resulted in a measurable added benefit com-pared with controls in terms of bone gain, but inthree of the four studies a significant difference interms of clinical attachment level gain was notachieved.
The benefit of the use of amelogenin (enamelmatrix derivative) gel in the treatment of intrabonydefects is supported by human histologic evidence,case report studies, meta-analyses of randomizedcontrolled clinical trials and large multicenter trials(43, 44, 47, 59–61, 63, 86, 115, 122, 123, 135). Clinically,the rate of wound healing following application ofamelogenins seems to be enhanced. A study investi-gating soft-tissue density in the surgical site usingunderexposed radiographs (137) reported that therate of increase in soft-tissue density following theapplication of amelogenins may be faster than in theaccess flap control. Such modulation has been inter-preted as the outcome of the local release of growthand differentiation factors by the cells involved in thelocal wound-healing process (5).
The biologic principles supporting combinationtherapy relate to the possibility of obtaining anadditive effect from one regenerative principle whenused in combination with another one, such as
Clinical concepts for regenerative therapy in intrabony defects
287

osteoconductivity and osteo-inductivity, the capacityfor space provision and blood-clot stabilization, andthe ability to induce or accelerate the processes ofmatrix formation and cell differentiation that areinherent in barriers, grafts and bioactive substances.Various modalities of combination therapy based onthe use of barrier membranes plus grafting materialshave been proposed. Pre-clinical (i.e. animal) studiespresenting histologic support for periodontal regene-ration using the combination of barrier membranesand grafting materials have been recently reviewed(118). The 10 papers completely fulfilling the inclu-sion criteria demonstrated superior histologic healingfollowing use of the combination of barrier mem-branes and grafting materials than following openflap debridement. Histologically superior healing fol-lowing use of the combination of barrier membranesand grafting materials compared with use of barriermembranes alone or grafting materials alone wereonly obtained in noncontained two-wall intrabonyand supra-alveolar defects. The cited analysis indi-cates that the combination of barrier membranes andgrafting materials may result in histologic evidence ofperiodontal regeneration, predominantly bone repair.
From a clinical standpoint, Schallhorn & McClain(113) reported on improved clinical results in intra-bony defects and degree II furcations, following acombination therapy that included barrier mem-branes plus demineralized freeze-dried bone allograftand citric acid root conditioning. In three controlledclinical trials, the treatment of a total of 45 pairs of in-trabony defects with demineralized freeze-dried boneallograft grafting and guided tissue regeneration werecompared with guided tissue regeneration alone. Thedifferences between the two treatments did not reachstatistical significance, thus indicating no addedeffect of combining demineralized freeze-dried boneallograft with barrier materials in the treatment ofintrabony defects. Guillemin et al. (53) compared theeffect of demineralized freeze-dried bone allograftalone with a combination of barrier materials plusdemineralized freeze-dried bone allograft in 15 pairsof intrabony defects. Both treatments resulted in sig-nificant amounts of clinical attachment level gainsand bone fill at 6 months, but no difference wasfound between the treatments. The same outcomeswere reported by Trejo et al. (138) in a randomizedclinical trial that compared polylactic acid barriersplus demineralized freeze-dried bone allograft withpolylactic acid barriers alone.
Promising clinical results with a clinical attachmentlevel gain ranging from 1.0 to 5.5 mm were obtainedin human case reports, in which the combination of
barrier membranes and Bio-Oss� was used for thetreatment of intrabony periodontal defects (76, 87,99). The combined Bio-Oss� and guided tissue-regen-eration treatment resulted in greater pocket-depthreduction, clinical attachment level gain and defectfill compared with the implantation of Bio-Oss� alonein a case series (11) and flap surgery alone in a split-mouth study (10). Three randomized controlled clini-cal studies (116, 126, 136) confirmed that clinicalimprovements in defects treated with barrier mem-branes in combination with Bio-Oss� grafting weresignificantly better than those obtained with flap sur-gery alone. In a controlled study (101), similar clinicalimprovements were obtained when Bio-Oss� com-bined with guided tissue regeneration was comparedwith biomodification of the root surface with enamelmatrix protein.
Combination therapy, including the use of amelo-genins plus barrier membranes and/or grafting mate-rials, has been tested. A systematic review (142)concluded that there is evidence to support the use ofamelogenins, either alone or in combination withgrafts, to treat intra-osseous defects effectively. Theadditional use of a graft seems to enhance the clinicaloutcome of amelogenins; the combined use ofhuman platelet-derived growth factor-BB and P-15with a graft biomaterial has shown beneficial effectsin intra-osseous defects; contrasting results werereported for platelet-rich plasma and graft combina-tions. The systematic review of Tu et al. (145) con-cluded that there was little evidence to support theadditional benefits of amelogenins in conjunctionwith other regenerative materials when comparedwith amelogenins alone. When different types of bonegrafts and barrier membranes were treated sepa-rately, amelogenins with bovine bone grafts showedgreater treatment effects.
The surgical approach
Application of all the aforementioned regenerativestrategies, including combinations, requires stableprotection by soft tissues to avoid bacterial contami-nation. Membrane exposure with consequent bacte-rial contamination during healing represented themajor complication of periodontal-regenerative pro-cedures previously, with prevalence in the range of50–100% (1, 2, 14–16, 39, 40, 45, 82, 89, 119, 140). Cor-tellini et al. (19, 20) reported that the prevalence ofmembrane exposure could be greatly reduced withthe use of access flaps, specifically designed to pre-serve the interdental tissues (i.e. the modified papillapreservation technique). Many studies have shownthat exposed membranes are contaminated with
Cortellini & Tonetti
288

bacteria (39, 40, 77, 94, 95) and contamination ofexposed nonbioabsorbable as well as bioabsorbablemembranes is associated with lower probing attach-ment-level gains in intrabony defects.
Another important issue associated with clinicalresults is the coverage of the regenerated tissue afterremoval of a nonbioabsorbable membrane. Manyauthors have reported that the frequent occurrenceof a gingival dehiscence over barrier membranes islikely to result in insufficient protection of the inter-dental regenerated tissue (1, 2, 15, 16, 119, 131). Expo-sure of the regenerated tissue to the oral environmentenhances the risks of mechanical and infectiousinsults that may, in turn, prevent complete matura-tion of the regenerated tissue into a new connectivetissue attachment. In fact, incomplete coverage of theregenerated tissue was associated with reducedattachment and bone gain at 1 year (131). The posi-tioning of a saddle-shaped free gingival graft over theregenerated interdental tissue was suggested to offerbetter coverage and protection than a dehiscent gin-gival flap (18).
In general, the development of new procedures wasaimed at complete preservation of the marginal tissuein order to achieve and maintain primary closure ontop of the applied regenerative material/substanceduring the critical stages of healing. Specifically, flapdesigns attempted to achieve passive primary closureof the flap combined with optimal wound stability.
Papilla preservation flaps. The modified papilla pres-ervation technique was developed in order to achieveand maintain primary closure of the flap and toincrease the ability to create space for regeneration inthe interdental area, (20). This approach is based onthe elevation of ample full-thickness buccal and lin-gual flaps, followed by a buccal periosteal incision toincrease buccal flap mobility. Vertical releasing inci-sions are traced when needed. Flaps are generallycoronally positioned on top of barriers and/or graftsor combinations and are sutured with a double-layersuturing technique to provide stable interdental clo-sure. The double-layer suturing approach is manda-tory. The deep internal crossed mattress suture isaimed at coronally advancing the buccal flap and thesecond suture is aimed at sealing the papilla in theabsence of tension. The application of this techniquereduced wound failure and subsequent bacterial con-tamination to about 30% of the treated sites (Fig. 1A–J).The modified papilla preservation technique allowedstable primary closure of the flap in the interdentalspace in 70% of the sites, providing protection ofthe regenerative materials and the underlying
regenerating tissues from the oral environment. In arandomized controlled clinical study on 45 patients(19), significantly greater amounts of attachmentgain were obtained with the modified papilla preser-vation technique and titanium-reinforced barriers(5.3 � 2.2 mm) in comparison with either conven-tional guided tissue regeneration (4.1 � 1.9 mm) orflap surgery (2.5 � 0.8 mm). The sites treated withthe modified papilla preservation technique alsodeveloped less gingival recession compared with con-trol therapies. This controlled clinical study demon-strated that a papilla preservation flap can result inimproved clinical outcomes compared with regenera-tion performed using conventional flap approacheswithout interdental soft-tissue preservation.
A meta-analysis (90) showed a trend of increasedclinical outcomes in studies using flap designs andsuturing techniques considered conducive to theachievement and maintenance of primary closure ofthe flap. The modified papilla preservation techniquecan be successfully applied in sites in which the inter-dental space width is at least 2 mm at the most coro-nal portion of the papilla and in conjunction with avariety of regenerative materials, including barriers,biologically active materials such as amelogenins(135) or growth factors and bone replacement grafts(31, 136).
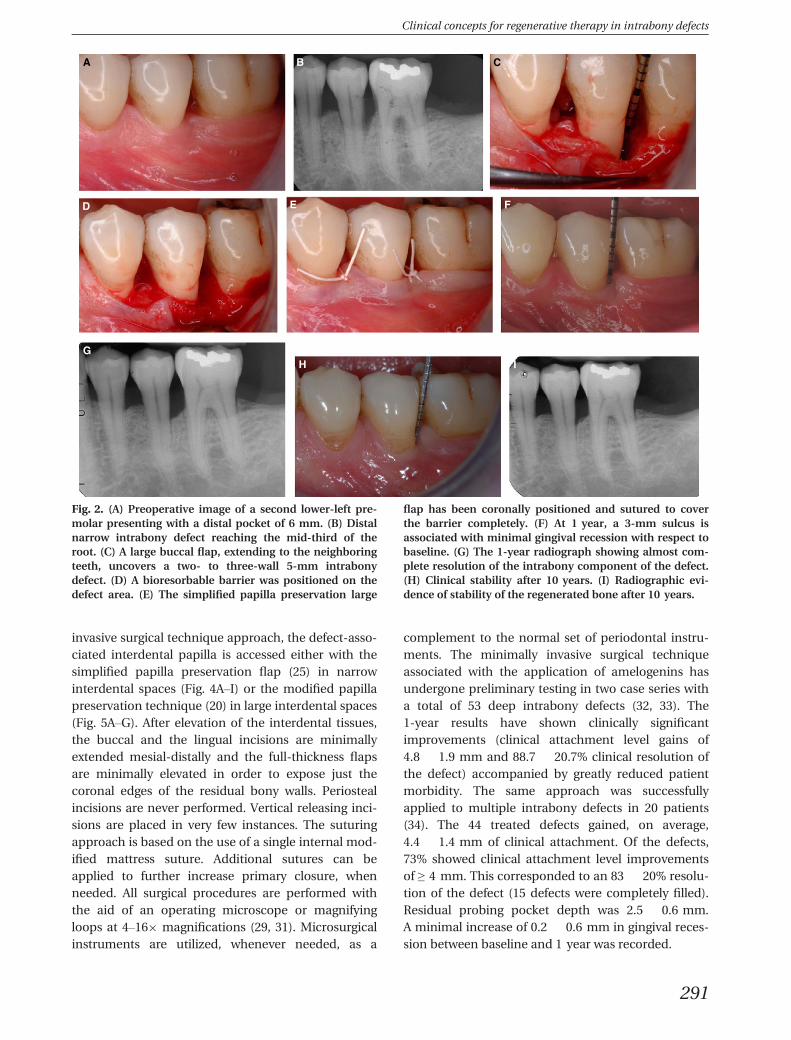
When interdental sites are narrower, a differentpapilla preservation procedure has been proposed,the simplified papilla preservation flap (25). In thecited study, 100% of the narrow interdental papillacould be closed on top of bioresorbable barriers, and67% maintained primary closure over time, resultingin gains of clinical attachment level of 4.9 � 1.8 mm(Fig. 2A–I). This approach has been successfullyapplied in several multicenter randomized clinical tri-als designed to test the generalizability of the addedbenefits of using barrier membranes in deep intra-bony defects (28, 134) and in conjunction with a vari-ety of regenerative materials, including biologicallyactive materials such as amelogenins (135) and bone-replacement grafts (31, 136).
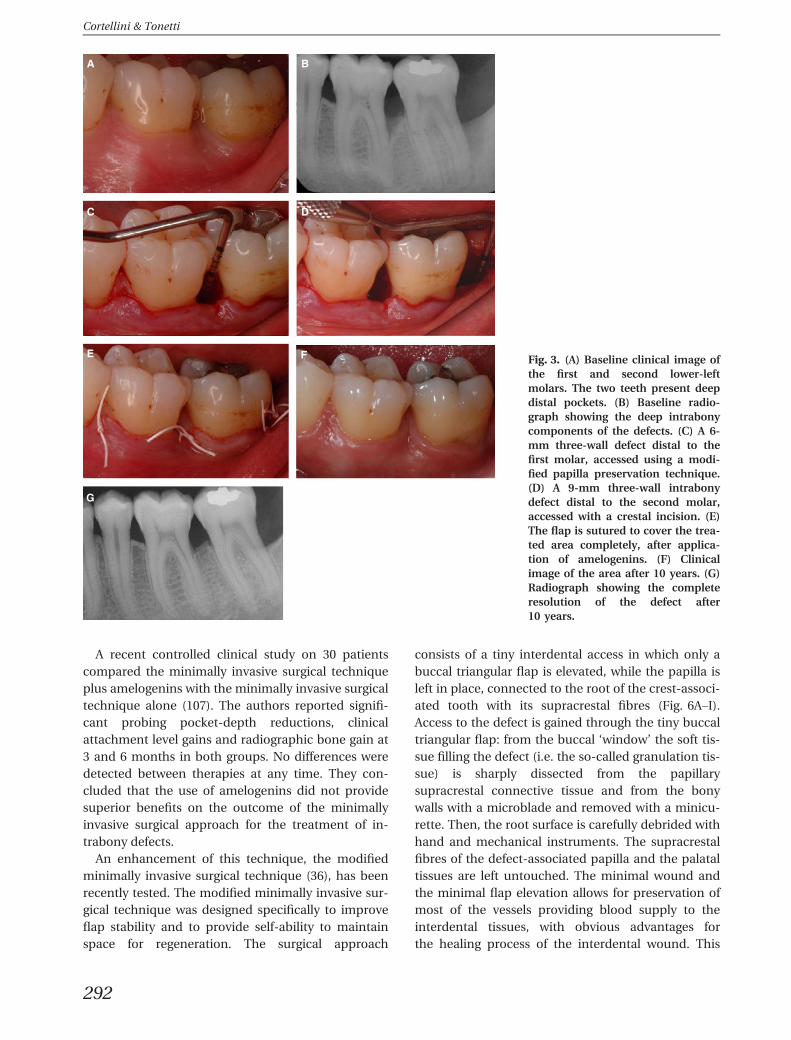
Following the path of surgical refinements, thepotential of soft-tissue manipulation to obtain stableprotection of the regeneration site has been furtherexplored, applying a microsurgical approach in theregenerative therapy of deep intrabony defects. Cor-tellini & Tonetti (29, 31) and Wachtel et al. (148)tested the use of operative microscopes and micro-surgical instruments to increase visual acuity and sur-gical accuracy in the application of papillapreservation flaps in periodontal regeneration(Fig. 3A–G). Microsurgery reduced wound failure to a
Clinical concepts for regenerative therapy in intrabony defects
289

mere 6% of the treated sites when applying the modi-fied papilla preservation technique and the simplifiedpapilla preservation flap (29, 31). In a patient cohortstudy on 26 patients with 26 intrabony defects treatedwith papilla preservation techniques, primary closureon the barrier was obtained in 100% of the defectsand maintained over time in 92.3% of the sites (29).Treatment resulted in large amounts of clinicalattachment level gains (5.4 � 1.2 mm) and minimalgingival recession (0.4 � 0.7 mm).
Minimally invasive surgical technique
In the last decade, a growing interest for morepatient-friendly and patient-oriented surgery has
urged clinical investigators to focus their interest inthe development of less-invasive approaches. Harrel& Rees (56) proposed the minimally invasive surgicaltechnique with the aim to produce minimal wounds,minimal flap reflection and gentle handling of the softand hard tissues (57, 58). In order to provide evengreater wound stability and protection, and to limitpatient morbidity further, Cortellini & Tonetti pro-posed a papilla preservation flap in the context of aminimally invasive, high-power, magnification-assisted surgical technique (32). The minimally inva-sive approach is particularly suited for treatment inconjunction with biologically active agents, such asamelogenins or growth factors, which are eventuallyassociated with grafting materials. In the minimally
A
D E
G H
I J
F
B C
Fig. 1. (A) Preoperative image of a right central incisorpresenting with a pocket depth of 16 and 2 mm of gingivalrecession. (B) Baseline radiograph showing an intrabonydefect reaching the apex of the tooth. (C) A large buccalflap has been raised to obtain proper access to the severedefect. After debridement, a two-wall, wide, 14-mm-deepintrabony defect associated with a buccal bone dehiscenceis evident on the central incisor. The lateral incisor showsloss of bone on the buccal and mesial root surfaces. (D)The severe bone defect also involves the lingual root sur-face. The lingual flap is extended to the neighboring teeth.
(E) A titanium-reinforced expanded-polytetrafluoroethyl-ene barrier has been positioned. (F) Postoperativeradiograph showing the ‘space’ provided by the titanium-reinforced barrier. (G) The modified papilla preservationlarge flap has been coronally advanced and sutured with adouble-layer suturing technique. (H) One-year radiographshowing the consistent bone fill of the defect. (I) Clinicalimage after 15 years. An interdental free gingival graft waspositioned 2 years after regeneration, partly to solve thebaseline gingival recession. (J) Radiograph after 15 years,showing complete mineralization of the defect area.
Cortellini & Tonetti
290
invasive surgical technique approach, the defect-asso-ciated interdental papilla is accessed either with thesimplified papilla preservation flap (25) in narrowinterdental spaces (Fig. 4A–I) or the modified papillapreservation technique (20) in large interdental spaces(Fig. 5A–G). After elevation of the interdental tissues,the buccal and the lingual incisions are minimallyextended mesial-distally and the full-thickness flapsare minimally elevated in order to expose just thecoronal edges of the residual bony walls. Periostealincisions are never performed. Vertical releasing inci-sions are placed in very few instances. The suturingapproach is based on the use of a single internal mod-ified mattress suture. Additional sutures can beapplied to further increase primary closure, whenneeded. All surgical procedures are performed withthe aid of an operating microscope or magnifyingloops at 4–169 magnifications (29, 31). Microsurgicalinstruments are utilized, whenever needed, as a
complement to the normal set of periodontal instru-ments. The minimally invasive surgical techniqueassociated with the application of amelogenins hasundergone preliminary testing in two case series witha total of 53 deep intrabony defects (32, 33). The1-year results have shown clinically significantimprovements (clinical attachment level gains of4.8 � 1.9 mm and 88.7 � 20.7% clinical resolution ofthe defect) accompanied by greatly reduced patientmorbidity. The same approach was successfullyapplied to multiple intrabony defects in 20 patients(34). The 44 treated defects gained, on average,4.4 � 1.4 mm of clinical attachment. Of the defects,73% showed clinical attachment level improvementsof ≥ 4 mm. This corresponded to an 83 � 20% resolu-tion of the defect (15 defects were completely filled).Residual probing pocket depth was 2.5 � 0.6 mm.A minimal increase of 0.2 � 0.6 mm in gingival reces-sion between baseline and 1 year was recorded.
A B C
D E
G
F
H I
Fig. 2. (A) Preoperative image of a second lower-left pre-molar presenting with a distal pocket of 6 mm. (B) Distalnarrow intrabony defect reaching the mid-third of theroot. (C) A large buccal flap, extending to the neighboringteeth, uncovers a two- to three-wall 5-mm intrabonydefect. (D) A bioresorbable barrier was positioned on thedefect area. (E) The simplified papilla preservation large
flap has been coronally positioned and sutured to coverthe barrier completely. (F) At 1 year, a 3-mm sulcus isassociated with minimal gingival recession with respect tobaseline. (G) The 1-year radiograph showing almost com-plete resolution of the intrabony component of the defect.(H) Clinical stability after 10 years. (I) Radiographic evi-dence of stability of the regenerated bone after 10 years.
Clinical concepts for regenerative therapy in intrabony defects
291
A recent controlled clinical study on 30 patientscompared the minimally invasive surgical techniqueplus amelogenins with the minimally invasive surgicaltechnique alone (107). The authors reported signifi-cant probing pocket-depth reductions, clinicalattachment level gains and radiographic bone gain at3 and 6 months in both groups. No differences weredetected between therapies at any time. They con-cluded that the use of amelogenins did not providesuperior benefits on the outcome of the minimallyinvasive surgical approach for the treatment of in-trabony defects.
An enhancement of this technique, the modifiedminimally invasive surgical technique (36), has beenrecently tested. The modified minimally invasive sur-gical technique was designed specifically to improveflap stability and to provide self-ability to maintainspace for regeneration. The surgical approach
consists of a tiny interdental access in which only abuccal triangular flap is elevated, while the papilla isleft in place, connected to the root of the crest-associ-ated tooth with its supracrestal fibres (Fig. 6A–I).Access to the defect is gained through the tiny buccaltriangular flap: from the buccal ‘window’ the soft tis-sue filling the defect (i.e. the so-called granulation tis-sue) is sharply dissected from the papillarysupracrestal connective tissue and from the bonywalls with a microblade and removed with a minicu-rette. Then, the root surface is carefully debrided withhand and mechanical instruments. The supracrestalfibres of the defect-associated papilla and the palataltissues are left untouched. The minimal wound andthe minimal flap elevation allows for preservation ofmost of the vessels providing blood supply to theinterdental tissues, with obvious advantages forthe healing process of the interdental wound. This
A B
C D
F
G
E Fig. 3. (A) Baseline clinical image ofthe first and second lower-leftmolars. The two teeth present deepdistal pockets. (B) Baseline radio-graph showing the deep intrabonycomponents of the defects. (C) A 6-mm three-wall defect distal to thefirst molar, accessed using a modi-fied papilla preservation technique.(D) A 9-mm three-wall intrabonydefect distal to the second molar,accessed with a crestal incision. (E)The flap is sutured to cover the trea-ted area completely, after applica-tion of amelogenins. (F) Clinicalimage of the area after 10 years. (G)Radiograph showing the completeresolution of the defect after10 years.
Cortellini & Tonetti
292
A B
D E
F G
H I
C
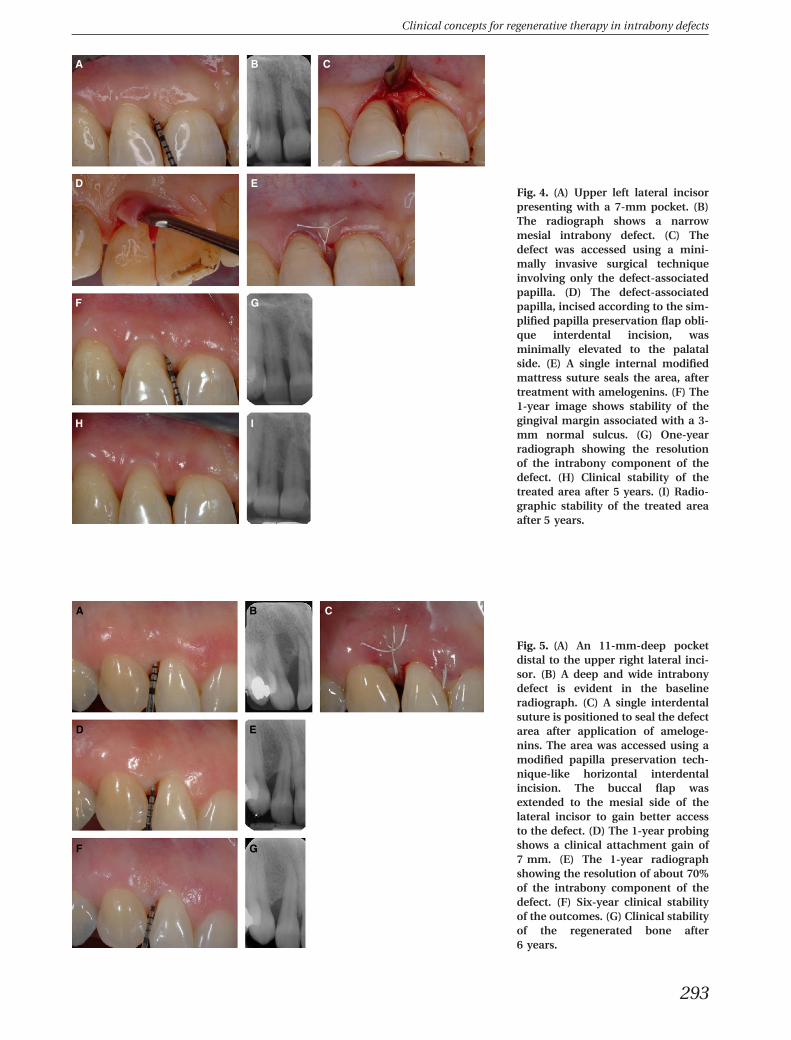
Fig. 4. (A) Upper left lateral incisorpresenting with a 7-mm pocket. (B)The radiograph shows a narrowmesial intrabony defect. (C) Thedefect was accessed using a mini-mally invasive surgical techniqueinvolving only the defect-associatedpapilla. (D) The defect-associatedpapilla, incised according to the sim-plified papilla preservation flap obli-que interdental incision, wasminimally elevated to the palatalside. (E) A single internal modifiedmattress suture seals the area, aftertreatment with amelogenins. (F) The1-year image shows stability of thegingival margin associated with a 3-mm normal sulcus. (G) One-yearradiograph showing the resolutionof the intrabony component of thedefect. (H) Clinical stability of thetreated area after 5 years. (I) Radio-graphic stability of the treated areaafter 5 years.
A B
D E
F G
C
Fig. 5. (A) An 11-mm-deep pocketdistal to the upper right lateral inci-sor. (B) A deep and wide intrabonydefect is evident in the baselineradiograph. (C) A single interdentalsuture is positioned to seal the defectarea after application of ameloge-nins. The area was accessed using amodified papilla preservation tech-nique-like horizontal interdentalincision. The buccal flap wasextended to the mesial side of thelateral incisor to gain better accessto the defect. (D) The 1-year probingshows a clinical attachment gain of7 mm. (E) The 1-year radiographshowing the resolution of about 70%of the intrabony component of thedefect. (F) Six-year clinical stabilityof the outcomes. (G) Clinical stabilityof the regenerated bone after6 years.
Clinical concepts for regenerative therapy in intrabony defects
293
surgical approach, with its particular design, ensuresself-support to the interdental soft tissues throughthe ‘hanging’ papilla, thereby enhancing space provi-sion. The flap is extremely stable because most of thesoft tissues around the bony defect are not incised orelevated, thereby enhancing blood-clot stability. Min-imal flap trauma, integrity of the blood supply andabsolute passivity in the suturing technique ensuresprimary closure of the interdental wound in themajority of cases, thereby preventing bacterial con-tamination. The suturing approach is based on theuse of a single internal modified mattress suture.Additional sutures can be applied, when needed, toensure primary closure. However, the reduced buccalaccess means that this approach is not applicable tovery deep defects that involve the lingual side of atooth in which the diseased root surface cannot bereached easily for instrumentation from the smallbuccal window (36).
Recently, a three-armed randomized controlledclinical trial was designed to compare the clinical
efficacy of the modified minimally invasive surgicaltechnique alone with the modified minimally invasivesurgical technique plus amelogenins (enamel matrixderivative) and with the modified minimally invasivesurgical technique plus amelogenins plus bone min-eral-derived xenograph, in the treatment of isolated,interdental intrabony defects (37). The study was per-formed on 45 deep, isolated, intrabony defectsaccessed using the modified minimally invasive surgi-cal technique and randomly assigned to three experi-mental groups: 15 to the modified minimally invasivesurgical technique alone; 15 to the modified mini-mally invasive surgical technique + enamel matrixderivative; and 15 to the modified minimally invasivesurgical technique + enamel matrix derivative + bonemineral-derived xenograph. Differences betweenbaseline and 1 year were statistically significant in thethree groups in terms of probing pocket-depth reduc-tion (P < 0.0001, Student’s t-test) and clinical attach-ment level gain (P < 0.0001). Comparisons among thethree groups showed no statistically significant
A
D E F
G H I
B C
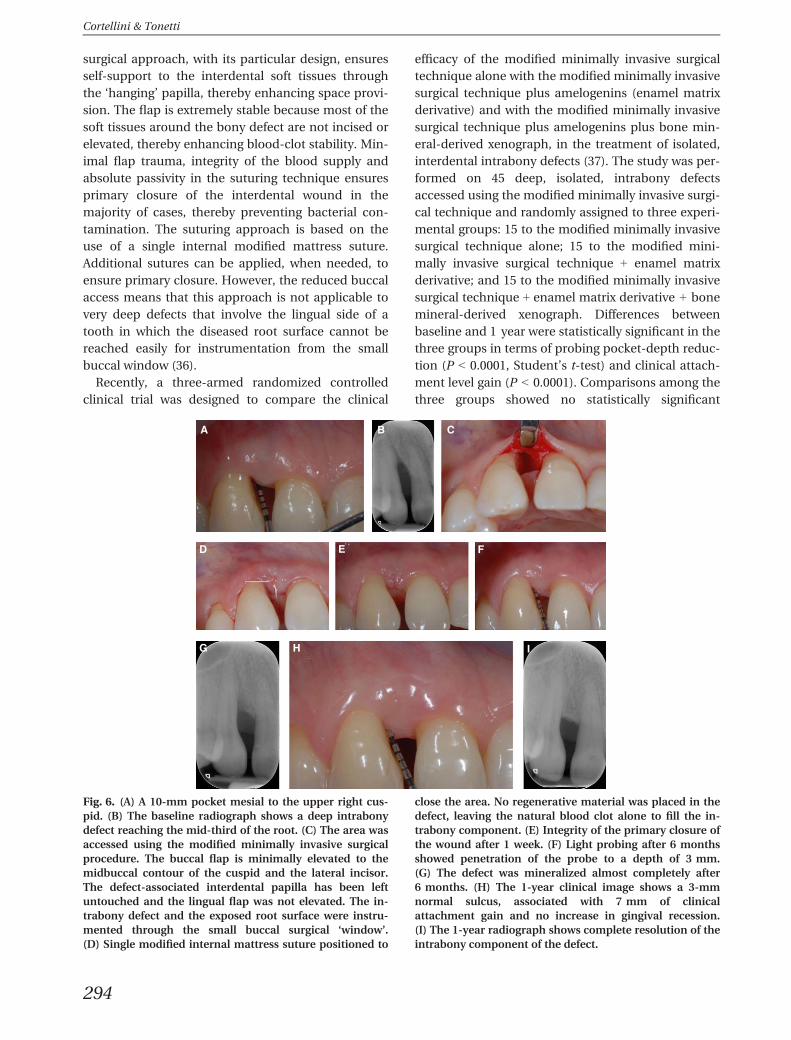
Fig. 6. (A) A 10-mm pocket mesial to the upper right cus-pid. (B) The baseline radiograph shows a deep intrabonydefect reaching the mid-third of the root. (C) The area wasaccessed using the modified minimally invasive surgicalprocedure. The buccal flap is minimally elevated to themidbuccal contour of the cuspid and the lateral incisor.The defect-associated interdental papilla has been leftuntouched and the lingual flap was not elevated. The in-trabony defect and the exposed root surface were instru-mented through the small buccal surgical ‘window’.(D) Single modified internal mattress suture positioned to
close the area. No regenerative material was placed in thedefect, leaving the natural blood clot alone to fill the in-trabony component. (E) Integrity of the primary closure ofthe wound after 1 week. (F) Light probing after 6 monthsshowed penetration of the probe to a depth of 3 mm.(G) The defect was mineralized almost completely after6 months. (H) The 1-year clinical image shows a 3-mmnormal sulcus, associated with 7 mm of clinicalattachment gain and no increase in gingival recession.(I) The 1-year radiograph shows complete resolution of theintrabony component of the defect.
Cortellini & Tonetti
294

difference in any of the measured clinical outcomes.In particular, clinical attachment level gains were4.1 � 1.4 mm in the modified minimally invasive sur-gical technique control group, 4.1 � 1.2 mm in theenamel matrix derivative group and 3.7 � 1.3 mm inthe enamel matrix derivative + bone mineral-derivedxenograph group. The radiographic bone fill of the in-trabony component was 77 � 19% in the modifiedminimally invasive surgical technique control group,71 � 18% in the enamel matrix derivative group and78 � 27% in the enamel matrix derivative + bonemineral-derived xenograph group. This initial con-trolled study had the power to detect a true differenceof 0.96 mm in clinical attachment levels among treat-ment groups. However, the fact that the outcomesamong the three groups could not be discriminatedraises a series of hypotheses that focus on the intrin-sic healing potential of a wound when ideal condi-tions are provided with the surgical approach. Inother words, the outcomes of this study challenge cli-nicians with the possibility to obtain substantial clini-cal improvements without the use of products ormaterials. An independent study (143) reported simi-lar outcomes, with no difference between a single flapapproach only and a single flap approach plus a bior-esorbable barrier and hydroxyapatite. However, lar-ger studies are needed to confirm the reportedoutcomes.
Surgical and postsurgical events
Clinicians are interested in information about thesurgical and postsurgical period, such as chair-timerequired for the surgical procedure, postsurgical com-plications, and pain and painkiller consumption afterthe procedure. From the very beginning of the‘guided tissue regeneration era’ the frequent occur-rence of complications was apparent, in particularexposure of barriers. It arose in almost 100% of casesin the pre-papilla preservation techniques period (1,2, 14–16, 39, 40, 45, 82, 89, 119, 140) and was report-edly reduced to a small number of cases (6–50%)when papilla preservation flaps were adopted (19, 20,22, 25, 26, 28, 29, 78, 90, 134–136). A consistentdecrease in complications was observed when barri-ers were not incorporated into the surgical procedure.In particular, the adoption of amelogenins largelyreduced the prevalence of complications (44, 134).A comparative study between barriers and ameloge-nins clearly demonstrated such a striking difference,reporting a complication rate of 100% in the barrier-treated sites compared with 6% in the amelogenin-treated sites (110).
Table 2 documents some surgical and postsurgicalparameters from three studies. Two studies were per-formed applying the traditional papilla preservationflaps with bioresorbable barriers (28) and ameloge-nins (135). The third study was performed using theminimally invasive surgical technique in combinationwith amelogenins (33). A historical comparisonhighlights clear differences in some parametersamong the three studies. Surgical chair-time was thelongest when large papilla preservation flaps and bar-riers were applied, shorter when large papilla preser-vation flaps were combined with amelogenins and byfar the shortest when the minimally invasive surgicaltechnique and amelogenins were used. The numberof subjects reporting postoperative pain was similarin the two papilla preservation flap studies and muchreduced in the minimally invasive surgical techniquestudy, as was pain intensity and consumption ofpainkillers (Table 2). The reported outcomes indicatethat use of different materials (barriers or ameloge-nins) applied in combination with a similar surgicalapproach results in similar postoperative pain,whereas a more user-friendly, shorter chair-time,minimally invasive surgery is associated with lesspostoperative pain. In other words, postoperativepain apparently is not influenced by the type ofregenerative material but by the type of surgicalapproach. The minimal amount of complications andpostoperative problems associated with applicationof minimally invasive surgical technique and amelo-genins was recently confirmed by the same group inanother study on multiple defects (34) and by anindependent controlled study (108). These conside-rations suggest that clinicians should adopt tissue-friendly approaches whenever possible.
Clinical potential and limits forregeneration
From the very beginning of modern periodontalregeneration therapy it was apparent that periodontaltissues could express a surprising regenerative poten-tial under particular circumstances. Sparse case reportsdemonstrated that very deep defects, reaching theapical third of the root, could be substantially filledwith new bone and new clinical attachment (1, 14,102). Larger studies suggested that in deeper defects agreater amount of clinical improvements is generallyobtained (46, 124, 131). These observations raisedquestions about the ‘potential’ for regeneration: is thepotential greater in deeper defects? A multicenterrandomized controlled study demonstrated that deepand shallow defects have the ‘same potential’ for
Clinical concepts for regenerative therapy in intrabony defects
295
regeneration (23). The cited study reported similaramounts of attachment gain in defects presentingwith an intrabony component of ≤ 3 mm (76% defectresolution) and defects of ≥ 4 mm (77% defect resolu-tion), indicating that the potential for regeneration issimilar in either shallow or deep intrabony compo-nents. The conclusions of this study are indirectlysupported by the results of large controlled clinicaltrials performed with the application of different suc-cessful regenerative approaches (19, 22, 28, 134–136).Unpublished subanalyses of these experimental pop-ulations, in which the treated defects have been clus-tered according to defect depth, show that clinicalattachment gain is obtained in all defects from shal-low to deep, but deeper defects gain more attach-ment (in millimetres) than do shallow defects. Inother words, regeneration seems to express its poten-tial as much as the ‘container’ allows it to do so andirrespective of the ‘regenerative approach’ chosen,within the panel of the regenerative approachestested. A recent controlled study has challenged thelimits of the periodontium to repair or regenerate(38). The aim of this randomized, long-term clinicaltrial was to compare clinical and patient-based out-comes following periodontal regeneration or extrac-tion and replacement of ‘hopeless’ teeth withattachment loss to or beyond the apex. Twenty-fivehopeless teeth were treated with the application of aregenerative strategy. Most of the treated teeth had aperiodontal lesion exceeding the apex of the toothand involving three to four sides of the root (Figs. 7A–Fand 8A–G). Twenty-three of the 25 regenerated teethexperienced extensive clinical improvements. Theaverage clinical attachment level gain was 7.7 �2.8 mm, the radiographic bone gain was 8.5 �3.1 mm and the probing pocket-depth reduction was
8.8 � 3.0 mm. Most of the regenerated teeth showeda decrease in tooth mobility. Only two teeth showedunsatisfactory outcomes and these were extracted at1 year. The 23 (92%) successfully regenerated teethwere in good health and function at the 5-year exami-nation visit and 84% did not develop biologic compli-cations during the recall period. The authorsconcluded that regenerative therapy can be success-fully applied, even at hopeless teeth, and has thepotential to change their prognosis. It should beclearly shared that the reported outcomes wereobtained in a carefully selected patient population,after applying ‘state of the art’ regenerative therapyby very experienced clinicians, within a high-qualityprogram of periodontal and dental therapy and astrict periodontal supportive-care program. In otherwords, it is apparent from the cited studies that tosucceed in extreme conditions a sound strategy hasto be adopted.
Clinical strategies
Scientific background
In summary, periodontal regeneration in intrabonydefects has been successfully attempted with a varietyof different regenerative materials and surgicalapproaches. As discussed, meta-analyses of random-ized controlled clinical trials, as well as human andanimal histologic findings, support the potential ofbarrier membranes (50, 97), demineralized freeze-dried bone allograft (6–8), combinations of barriermembranes and grafts (11, 87) and the use of enamelmatrix derivative (86, 147) or growth factors (65) toinduce periodontal regeneration. Controlled clini-cal trials report that the above-mentionedapproaches provide added benefits, in terms of
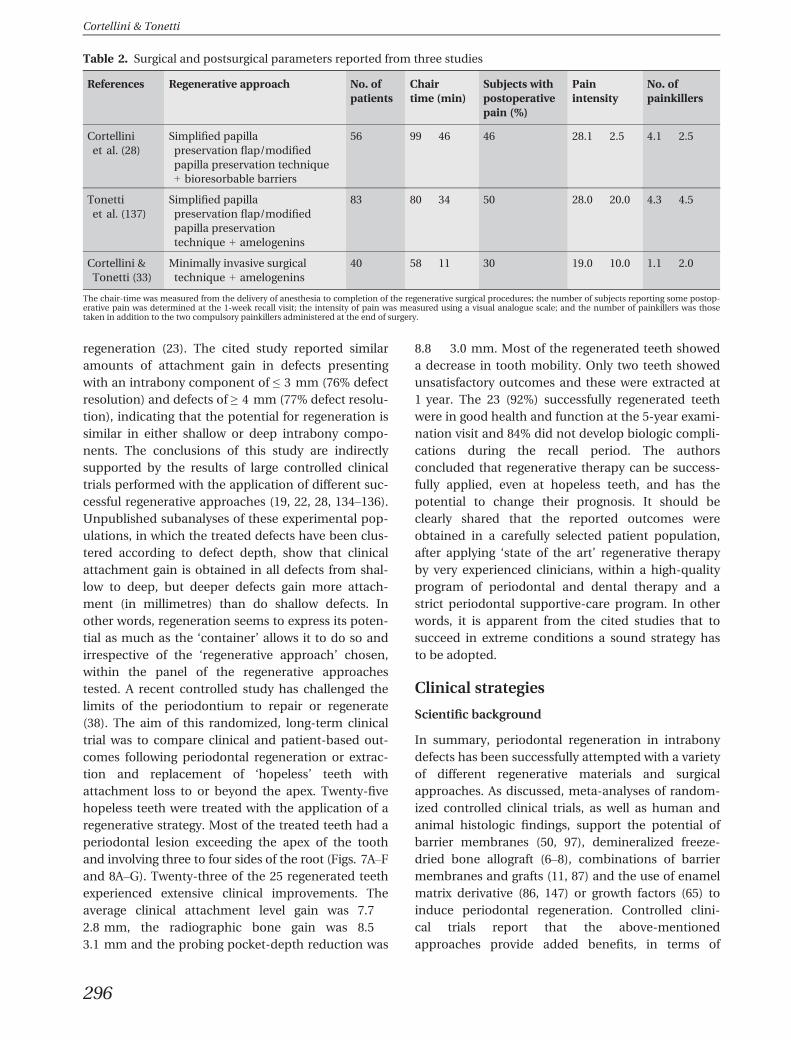
Table 2. Surgical and postsurgical parameters reported from three studies
References Regenerative approach No. ofpatients
Chairtime (min)
Subjects withpostoperativepain (%)
Painintensity
No. ofpainkillers
Cortelliniet al. (28)
Simplified papillapreservation flap/modifiedpapilla preservation technique+ bioresorbable barriers
56 99 � 46 46 28.1 � 2.5 4.1 � 2.5
Tonettiet al. (137)
Simplified papillapreservation flap/modifiedpapilla preservationtechnique + amelogenins
83 80 � 34 50 28.0 � 20.0 4.3 � 4.5
Cortellini &Tonetti (33)
Minimally invasive surgicaltechnique + amelogenins
40 58 � 11 30 19.0 � 10.0 1.1 � 2.0
The chair-time was measured from the delivery of anesthesia to completion of the regenerative surgical procedures; the number of subjects reporting some postop-erative pain was determined at the 1-week recall visit; the intensity of pain was measured using a visual analogue scale; and the number of painkillers was thosetaken in addition to the two compulsory painkillers administered at the end of surgery.
Cortellini & Tonetti
296

clinical attachment level gain, compared with openflap debridement alone [Trombelli et al. (141), Mur-phy & Gunsolley (90), Giannobile & Somerman (47),Esposito et al. (43, 44), Needleman et al. (91)]. Com-parisons among some of the cited regenerativeapproaches failed to demonstrate clear superiority ofone of the tested materials (44, 47, 90, 106, 142, 145).Therefore, the existing evidence does not support thechoice of a single approach among the differentregenerative possibilities. In addition, all the citedstudies have shown a substantial degree of variability,in terms of clinical attachment level gains, reportingfailures or unsatisfactory outcomes in part of the trea-ted population. This trend is not unexpected becauseeach patient randomly entered in each study presentswith unique individual characteristics and eachdefect presents with very different and unique anato-mies. The outcomes of each randomized study clearlydemonstrate that none of the regenerativeapproaches can resolve all the different patient anddefect presentations. It is therefore essential to buildup a clinical decision tree that allows clinicians toapply the appropriate regenerative strategy to eachindividual case.
The body of evidence discussed above has alreadybeen utilized in recent years to develop an evidence-based regenerative strategy to guide cliniciansthrough a decision-making process aimed at optimiz-ing the clinical outcomes of periodontal regenerationin intrabony defects (26, 31). The performance of thisclinical strategy has been assessed in a 40-patientconsecutive case series treated with the papilla pre-servation techniques (31). Based on defect anatomy,nonresorbable titanium-reinforced expanded-poly-tetrafluoroethylene barrier membranes or bioresorb-able membranes supported with a bone-replacementgraft were used in 23 one- to two-wall-wide intrabonydefects, bioresorbable barriers alone were used inseven narrow two-wall defects and amelogenins wereapplied to 10 defects with a prevalent three-wall com-ponent. Flap primary closure was obtained in 100% ofthe patients at completion of surgery and wasmaintained in 93% of the sites during the entire earlyhealing phase. The 1-year clinical attachment gainwas 6 � 1.8 mm. No sites gained < 4 mm of clini-cal attachment; 77.5% gained ≥ 5 mm and 40%gained > 6 mm. Residual probing depths were2.7 � 0.6 mm, and the increase in gingival recession
A B
C D
E F
Fig. 7. (A) Baseline image of a 16-mm pocket mesial to the first lower-left molar. (B) The baseline radio-graph shows evidence of a very deepintrabony defect extending beyondthe apex of the mesial root. Thetooth was vital and the furcation wasnot involved. (C) The vital tooth wasendodontically treated 3 monthsbefore regeneration. The reason forthe endodontic treatment of thisvital tooth was the need to instru-ment the apex of the mesial rootinvolved by the severe periodontaldefect. (D) The mesial root isinvolved by an all-around periodon-tal defect and appears to be hangingin the space of a complex intrabonydefect associated with a completebuccal bone dehiscence. The defectwas treated with amelogenins. (E)The 1-year radiograph shows almostcomplete resolution of the defectassociated with the mesial root. (F)Stability of the radiological out-comes after 5 years.
Clinical concepts for regenerative therapy in intrabony defects
297
was minimal between baseline and 1 year(0.1 � 0.7 mm). The four approaches resulted in 88–95% resolution of the original depth of the intrabonycomponent of the defect (31). The outcomes of thereported study clearly demonstrate that the applica-tion of a sound strategy can help clinicians to opti-mize the clinical outcomes in each single case.
A novel, more comprehensive, clinical strategy hasbeen developed to improve the clinical capacity fur-ther, to ensure optimal therapy for each given patientand defect site. This approach takes into account therelevance of the patient characteristics, as previouslyreported in this review, and bases its foundations onthe need to satisfy the three major contributors toperiodontal regeneration: (i) the need for space forthe formation of the blood clot at the interfacebetween the flap and the root surface (19, 20, 55, 67,121, 133, 151); (ii) the need for stability of the bloodclot to maintain continuity with the root surface,avoiding formation of a long junctional epithelium(55, 64, 75, 150); and (iii) the need for soft-tissue pro-tection of the treated area to avoid bacterial contami-nation (39, 40, 94, 95, 104, 110, 119).
Space and blood-clot stability are self-provided inthe so-called ‘containing defects’, the narrow
three-wall defects in particular (24, 48, 74, 112, 120,144). The ‘noncontaining defects’ – the large one- ortwo-wall defects – require an intervention to supple-ment the deficient anatomy (45, 131, 132, 135–137).The intervention can be based on the use of biomate-rials, such as exoskeleton-like barriers or endoskele-ton-like grafts, which are able to support the softtissues and to stabilize the blood clot, or a combina-tion of both approaches. In other words, the ana-tomic deficiencies of the defects have to besupplemented by the additional use of biomaterials.The same goal may also be achieved by adopting par-ticular surgical strategies in which tissues are mini-mally elevated to increase their stability (theminimally invasive surgical technique and the modi-fied minimally invasive surgical techniqueapproaches) (32–37). Blood-clot stability is alsoclearly influenced by tooth mobility: splinting teethwith Miller grade II or grade III mobility is essential toavoid the disruption of the blood clot in the earlyhealing phase (28, 138).
Protection of the regenerating area should be pro-vided through the adoption of specifically designedsurgical approaches. The different surgicalapproaches developed over time incorporate clear
A B
D
F G
E
C
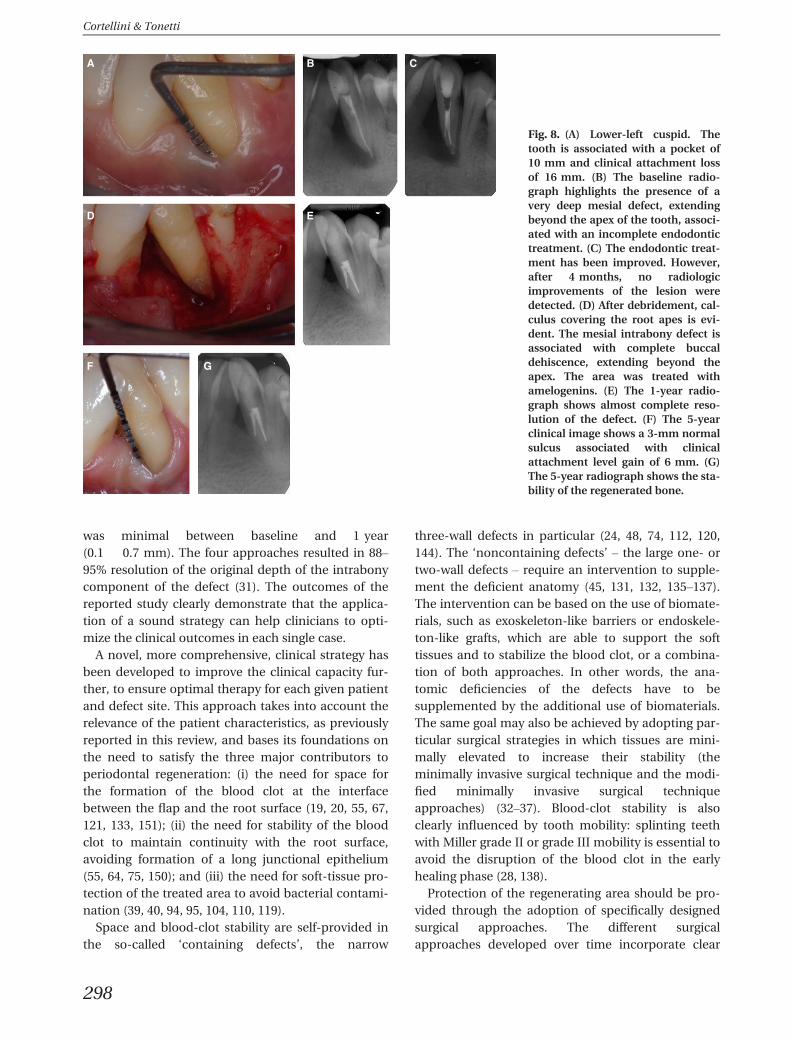
Fig. 8. (A) Lower-left cuspid. Thetooth is associated with a pocket of10 mm and clinical attachment lossof 16 mm. (B) The baseline radio-graph highlights the presence of avery deep mesial defect, extendingbeyond the apex of the tooth, associ-ated with an incomplete endodontictreatment. (C) The endodontic treat-ment has been improved. However,after 4 months, no radiologicimprovements of the lesion weredetected. (D) After debridement, cal-culus covering the root apes is evi-dent. The mesial intrabony defect isassociated with complete buccaldehiscence, extending beyond theapex. The area was treated withamelogenins. (E) The 1-year radio-graph shows almost complete reso-lution of the defect. (F) The 5-yearclinical image shows a 3-mm normalsulcus associated with clinicalattachment level gain of 6 mm. (G)The 5-year radiograph shows the sta-bility of the regenerated bone.
Cortellini & Tonetti
298
differences in terms of flap design and suturing tech-nique. In addition to their ability to provide protec-tion to the regenerating area, they may makedifferent contributions to improve one or more of themany processes potentially relevant to overall woundhealing. The traditional papilla-preservation flaps (20,25) were designed as wide and very mobile flaps inorder to allow perfect visibility of the defect area, easyapplication of biomaterials and for the coronal posi-tioning of the buccal flap to cover barriers and bio-materials. In other words, the papilla preservationflaps did not incorporate the mechanical characteris-tics to improve wound stability and the independentcapacity to create space for regeneration. In contrast,the minimally invasive surgical technique (32, 33) wasdesigned to reduce flap extension and mobility asmuch as possible, and to increase the ability for pri-mary wound closure and blood-clot stability. Thispotential was partly highlighted in two studies thatdemonstrated a reduced impact of the number ofresidual bony walls and of the defect width on theoutcomes obtained with amelogenins under a mini-mally invasive surgical technique (34, 35) and wasrecently confirmed in a comparative study demon-strating similar outcomes between the minimallyinvasive surgical technique alone and the minimallyinvasive surgical technique plus amelogenins (107).
A further development of this surgical approachended in the modified minimally invasive surgicaltechnique approach (36, 37). This advanced flapdesign further enhances the potential of the flap toprovide space and stability for regeneration by lea-ving the interdental papillary soft tissues attached tothe root surface of the crest-associated tooth and byavoiding any palatal flap elevation. The interdentalsoft tissues are the stable ‘roof’ of a room where theblood fills in and forms a clot. In addition, the hang-ing papilla prevents the collapse of the soft tissues,maintaining space for regeneration: the anatomicbone deficiencies are potentially supplemented bythe specific flap design that provides additional ‘soft-tissue walls’ to the missing bony walls, thus improv-ing stability: the walls of the ‘room’ are the residualbony walls, the root surface and the buccal/lingualsoft tissues. The minimal flap extension and elevationalso greatly reduces the damage to the vascular sys-tem. It is clear that such a flap is not designed to allowfor the positioning of a barrier, but easily allows forthe use of biologicals or grafts. The clinical flow chartspresented here (Fig. 9–14) were developed also takinginto account the scientific contributions on surgicaland postsurgical events, such as chair-time, sideeffects and postoperative pain.
Clinical flow charts
The step-by-step clinical approach to the treatmentof intrabony defects includes two presurgical flowcharts dealing with patient and local factors (Flowcharts 1 and 2) and four surgical flow charts (surgicalnodes) (Flow charts 3–6). The build-up of the surgicalnodes was driven by the willingness to treat a givendefect using the procedure judged as fastest, easiest,less burdened by side effects and best tolerated bypatients. Lastly, suggestions for postoperative careare discussed.
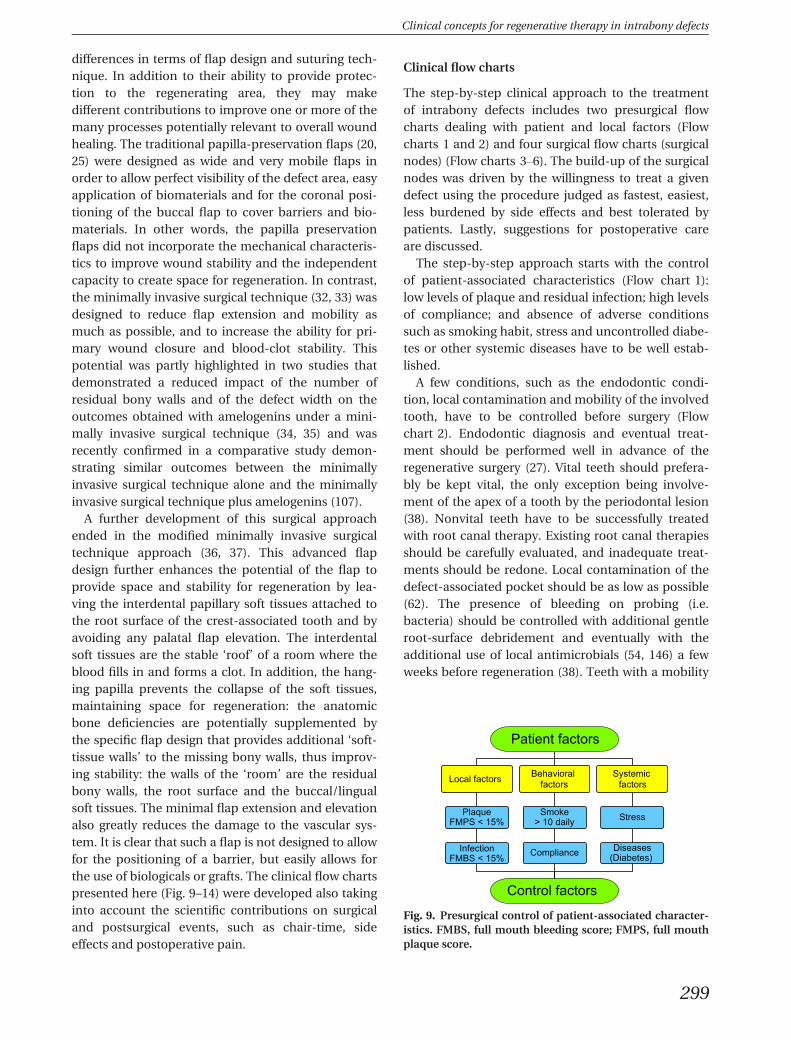
The step-by-step approach starts with the controlof patient-associated characteristics (Flow chart 1):low levels of plaque and residual infection; high levelsof compliance; and absence of adverse conditionssuch as smoking habit, stress and uncontrolled diabe-tes or other systemic diseases have to be well estab-lished.
A few conditions, such as the endodontic condi-tion, local contamination and mobility of the involvedtooth, have to be controlled before surgery (Flowchart 2). Endodontic diagnosis and eventual treat-ment should be performed well in advance of theregenerative surgery (27). Vital teeth should prefera-bly be kept vital, the only exception being involve-ment of the apex of a tooth by the periodontal lesion(38). Nonvital teeth have to be successfully treatedwith root canal therapy. Existing root canal therapiesshould be carefully evaluated, and inadequate treat-ments should be redone. Local contamination of thedefect-associated pocket should be as low as possible(62). The presence of bleeding on probing (i.e.bacteria) should be controlled with additional gentleroot-surface debridement and eventually with theadditional use of local antimicrobials (54, 146) a fewweeks before regeneration (38). Teeth with a mobility
Patient factors
Local factors Behavioral factors
Systemic factors
Smoke> 10 daily
Compliance
PlaqueFMPS < 15%
InfectionFMBS < 15%
Stress
Diseases(Diabetes)
Control factors
Fig. 9. Presurgical control of patient-associated character-istics. FMBS, full mouth bleeding score; FMPS, full mouthplaque score.
Clinical concepts for regenerative therapy in intrabony defects
299
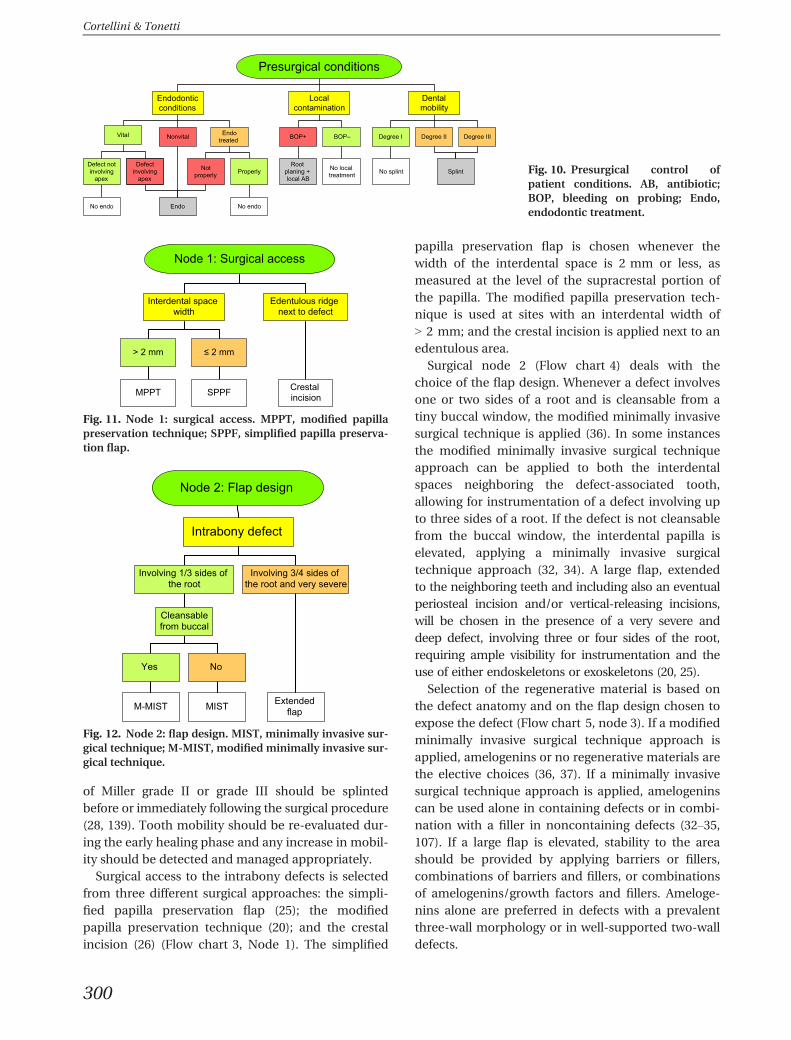
of Miller grade II or grade III should be splintedbefore or immediately following the surgical procedure(28, 139). Tooth mobility should be re-evaluated dur-ing the early healing phase and any increase in mobil-ity should be detected and managed appropriately.
Surgical access to the intrabony defects is selectedfrom three different surgical approaches: the simpli-fied papilla preservation flap (25); the modifiedpapilla preservation technique (20); and the crestalincision (26) (Flow chart 3, Node 1). The simplified
papilla preservation flap is chosen whenever thewidth of the interdental space is 2 mm or less, asmeasured at the level of the supracrestal portion ofthe papilla. The modified papilla preservation tech-nique is used at sites with an interdental width of> 2 mm; and the crestal incision is applied next to anedentulous area.
Surgical node 2 (Flow chart 4) deals with thechoice of the flap design. Whenever a defect involvesone or two sides of a root and is cleansable from atiny buccal window, the modified minimally invasivesurgical technique is applied (36). In some instancesthe modified minimally invasive surgical techniqueapproach can be applied to both the interdentalspaces neighboring the defect-associated tooth,allowing for instrumentation of a defect involving upto three sides of a root. If the defect is not cleansablefrom the buccal window, the interdental papilla iselevated, applying a minimally invasive surgicaltechnique approach (32, 34). A large flap, extendedto the neighboring teeth and including also an eventualperiosteal incision and/or vertical-releasing incisions,will be chosen in the presence of a very severe anddeep defect, involving three or four sides of the root,requiring ample visibility for instrumentation and theuse of either endoskeletons or exoskeletons (20, 25).
Selection of the regenerative material is based onthe defect anatomy and on the flap design chosen toexpose the defect (Flow chart 5, node 3). If a modifiedminimally invasive surgical technique approach isapplied, amelogenins or no regenerative materials arethe elective choices (36, 37). If a minimally invasivesurgical technique approach is applied, amelogeninscan be used alone in containing defects or in combi-nation with a filler in noncontaining defects (32–35,107). If a large flap is elevated, stability to the areashould be provided by applying barriers or fillers,combinations of barriers and fillers, or combinationsof amelogenins/growth factors and fillers. Ameloge-nins alone are preferred in defects with a prevalentthree-wall morphology or in well-supported two-walldefects.
Presurgical conditions
Endodontic conditions
Localcontamination
Dentalmobility
Degree I Degree II Degree IIIBOP+ BOP–Vital Nonvital Endo treated
Defect not involving
apex
Defect involving
apex
Not properly Properly
Root planing + local AB
No local treatment No splint Splint
EndoNo endo No endo
Fig. 10. Presurgical control ofpatient conditions. AB, antibiotic;BOP, bleeding on probing; Endo,endodontic treatment.
Node 1: Surgical access
Edentulous ridge next to defect
Interdental space width
> 2 mm ≤ 2 mm
Crestal incisionMPPT SPPF
Fig. 11. Node 1: surgical access. MPPT, modified papillapreservation technique; SPPF, simplified papilla preserva-tion flap.
Node 2: Flap design
Intrabony defect
Involving 1/3 sides of the root
Involving 3/4 sides of the root and very severe
Cleansablefrom buccal
Extendedflap
Yes No
MISTM-MIST
Fig. 12. Node 2: flap design. MIST, minimally invasive sur-gical technique; M-MIST, modified minimally invasive sur-gical technique.
Cortellini & Tonetti
300
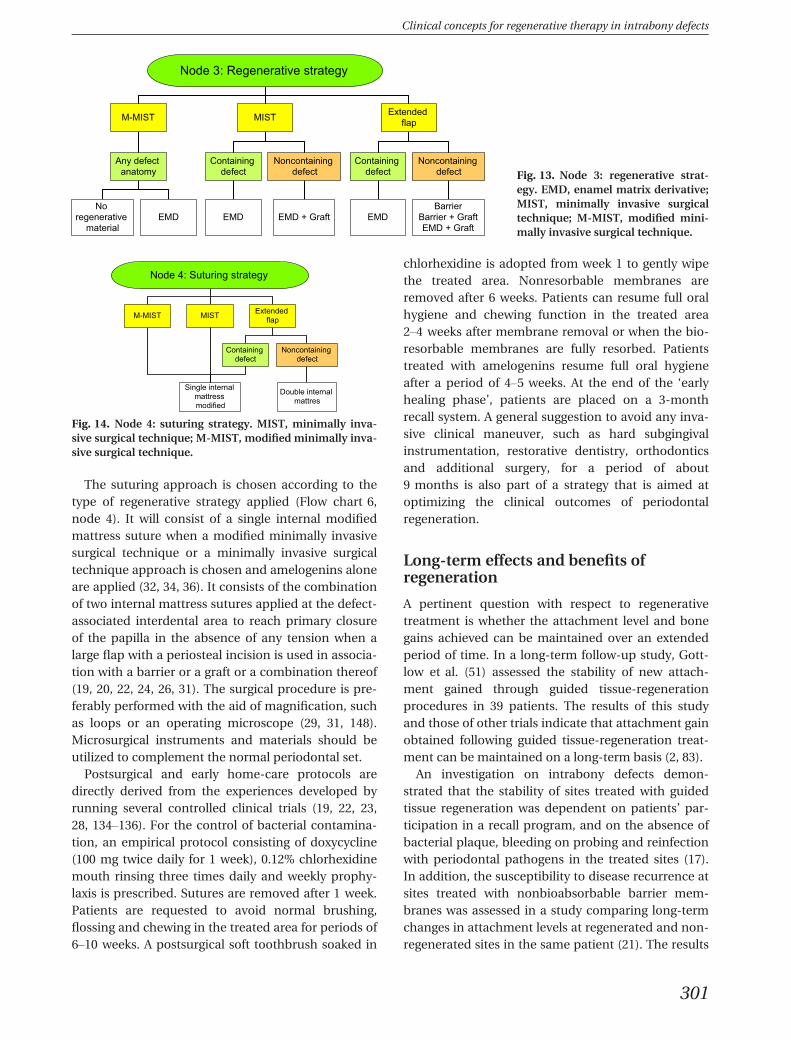
The suturing approach is chosen according to thetype of regenerative strategy applied (Flow chart 6,node 4). It will consist of a single internal modifiedmattress suture when a modified minimally invasivesurgical technique or a minimally invasive surgicaltechnique approach is chosen and amelogenins aloneare applied (32, 34, 36). It consists of the combinationof two internal mattress sutures applied at the defect-associated interdental area to reach primary closureof the papilla in the absence of any tension when alarge flap with a periosteal incision is used in associa-tion with a barrier or a graft or a combination thereof(19, 20, 22, 24, 26, 31). The surgical procedure is pre-ferably performed with the aid of magnification, suchas loops or an operating microscope (29, 31, 148).Microsurgical instruments and materials should beutilized to complement the normal periodontal set.
Postsurgical and early home-care protocols aredirectly derived from the experiences developed byrunning several controlled clinical trials (19, 22, 23,28, 134–136). For the control of bacterial contamina-tion, an empirical protocol consisting of doxycycline(100 mg twice daily for 1 week), 0.12% chlorhexidinemouth rinsing three times daily and weekly prophy-laxis is prescribed. Sutures are removed after 1 week.Patients are requested to avoid normal brushing,flossing and chewing in the treated area for periods of6–10 weeks. A postsurgical soft toothbrush soaked in
chlorhexidine is adopted from week 1 to gently wipethe treated area. Nonresorbable membranes areremoved after 6 weeks. Patients can resume full oralhygiene and chewing function in the treated area2–4 weeks after membrane removal or when the bio-resorbable membranes are fully resorbed. Patientstreated with amelogenins resume full oral hygieneafter a period of 4–5 weeks. At the end of the ‘earlyhealing phase’, patients are placed on a 3-monthrecall system. A general suggestion to avoid any inva-sive clinical maneuver, such as hard subgingivalinstrumentation, restorative dentistry, orthodonticsand additional surgery, for a period of about9 months is also part of a strategy that is aimed atoptimizing the clinical outcomes of periodontalregeneration.
Long-term effects and benefits ofregeneration
A pertinent question with respect to regenerativetreatment is whether the attachment level and bonegains achieved can be maintained over an extendedperiod of time. In a long-term follow-up study, Gott-low et al. (51) assessed the stability of new attach-ment gained through guided tissue-regenerationprocedures in 39 patients. The results of this studyand those of other trials indicate that attachment gainobtained following guided tissue-regeneration treat-ment can be maintained on a long-term basis (2, 83).
An investigation on intrabony defects demon-strated that the stability of sites treated with guidedtissue regeneration was dependent on patients’ par-ticipation in a recall program, and on the absence ofbacterial plaque, bleeding on probing and reinfectionwith periodontal pathogens in the treated sites (17).In addition, the susceptibility to disease recurrence atsites treated with nonbioabsorbable barrier mem-branes was assessed in a study comparing long-termchanges in attachment levels at regenerated and non-regenerated sites in the same patient (21). The results
Node 3: Regenerative strategy
M-MIST MIST Extended flap
Containing defect
Noncontaining defect
Any defect anatomy
Containing defect
Noncontaining defect
BarrierBarrier + GraftEMD + Graft
EMDEMD + GraftEMDNo
regenerative material
EMD
Fig. 13. Node 3: regenerative strat-egy. EMD, enamel matrix derivative;MIST, minimally invasive surgicaltechnique; M-MIST, modified mini-mally invasive surgical technique.
Node 4: Suturing strategy
M-MIST MIST Extended flap
Containing defect
Noncontaining defect
Single internal mattress modified
Double internal mattres
Fig. 14. Node 4: suturing strategy. MIST, minimally inva-sive surgical technique; M-MIST, modified minimally inva-sive surgical technique.
Clinical concepts for regenerative therapy in intrabony defects
301

indicated a high degree of concordance in the clinicaloutcomes (stability compared with recurrence ofattachment loss) within the same patient, suggestingthat patient factors, rather than site factors, are asso-ciated with disease recurrence. Among patient fac-tors, compliance with oral hygiene, smoking habitsand susceptibility to disease progression, rather thanthe treatment modality employed, were the majordeterminants of stability of the treated sites. Otherlong-term studies show that if the patient participatesin a professionally delivered supportive periodontalcare program and maintains good oral hygiene, theregenerated attachment can be maintained long-term(13, 41, 93, 96, 105, 117, 124).
One investigation has looked at the long-termeffects of periodontal regeneration on tooth survival.Cortellini & Tonetti (30) performed a Kaplan–Meieranalysis of tooth survival following periodontal-regenerative treatment in a sample of 175 patientsfollowed up for 2–16 years (average 8 � 3.4 years) ina specialist environment. In this study, 96% of teethtreated by periodontal regeneration survived. Ofinterest was the observation that tooth loss wasobserved only among the 32% of the population thatwas smoking (tooth survival was 89% among smokersand 100% among nonsmokers). Clinical attachmentlevels were located at the same level or coronal to thepretreatment levels in 92% of patients up to 15 yearsafter treatment.
Conclusions
Periodontal regeneration with many different regen-erative materials, including barrier membranes,grafts, active biological compounds and combina-tions of those, demonstrated significant clinicalimprovements in intrabony defects, far beyond thoseachieved with debridement only. Different surgicalapproaches have been proposed and tested in combi-nation with the various regenerative materials, butnone has demonstrated clear superiority over the oth-ers. Although all proposed regenerative approachesshowed a high degree of clinical variability in terms ofclinical attachment level gain, none demonstratedthe capacity to solve all the different and uniquepatient/defect presentations. It is therefore necessaryto choose a regenerative strategy out of a panel ofoptions to treat a given defect. The adoption of a clin-ical strategy for optimal application of materials andsurgical approach could increase the efficacy of peri-odontal regeneration and provide improved clinicaloutcomes. The potential for periodontal regeneration
can be expressed in defects from very shallow to verydeep, up to extreme conditions in which the applica-tion of regenerative therapy can change the prognosisof a hopeless tooth into a maintainable unit. Clinicaloutcomes obtained with periodontal regenerationcan be stably maintained on a long-term basis, pro-vided that good oral hygiene and infection controlwithin a stringent recall program are enforced. Cur-rent data indicate that, in patients participating in asupportive periodontal-care program, 96% of teethwith severe intrabony defects and treated with a peri-odontal-regenerative procedure could be retained fora period of up to 15 years.
References
1. Becker W, Becker BE, Berg L, Pritchard J, Caffesse R,Rosenberg E. New attachment after treatment with rootisolation procedures: report for treated class III and classII furcations and vertical osseous defects. Int J PeriodonticsRestorative Dent 1988: 8: 2–16.
2. Becker W, Becker B. Treatment of mandibular three-wallintrabony defects by flap debridement and expandedpolytetrafluoroethylene barrier membranes. Long termevaluation of 32 treated patients. J Periodontol 1993: 64:1138–1144.
3. Blumenthal NM. The use of collagen membranes to guideregeneration of new connective tissue attachment in dogs.J Periodontol 1988: 59: 830–836.
4. Blumenthal MN. A clinical comparison of collagen mem-branes with e-PTFE membranes in the treatment ofhuman mandibular buccal class II furcation defects. J Peri-odontol 1993: 64: 925–933.
5. Bosshardt DD. Biological mediators and periodontalregeneration: a review of enamel matrix proteins at thecellular and molecular levels. J Clin Periodontol 2008: 35(Suppl. 8): 87–105.
6. Bowers GM, Chadroff B, Carnevale R, Mellonig J, Corio R,Emerson J, Stevens M, Romberg E. Histologic evaluationof new attachment apparatus formation in humans. Part I.J Periodontol 1989: 60: 664–674.
7. Bowers GM, Chadroff B, Carnevale R, Mellonig J, Corio R,Emerson J, Stevens M, Romberg E. Histologic evaluationof new human attachment apparatus formation inhumans. Part II. J Periodontol 1989: 60: 675–682.
8. Bowers GM, Chadroff B, Carnevale R, Mellonig J, Corio R,Emerson J, Stevens M, Romberg E. Histologic evaluationof a new attachment apparatus formation in humans. PartIII. J Periodontol 1989: 60: 683–693.
9. Caffesse RG, Nasjleti CE, Morrison EC, Sanchez R.Guided tissue regeneration: comparison of bioabsorb-able and non-bioabsorbable membranes. Histologicand histometric study in dogs. J Periodontol 1994: 65:583–591.
10. Camargo PM, Lekovic V, Weinlander M, Nedic M, VasilicN, Wolinsky LE, Kenney EB. A controlled re-entry study onthe effectiveness of bovine porous bone mineral used incombination with a collagen membrane of porcine origin
Cortellini & Tonetti
302
in the treatment of intrabony defects in humans. J Clin Pe-riodontol 2000: 27: 889–896.
11. Camelo M, Nevins ML, Schenk RK, Simion M, Rasperini G,Lynch SE, Nevins M. Clinical radiographic, and histologicevaluation of human periodontal defects treated with Bio-Oss� and Bio-Gide. Int J Periodontics Restorative Dent1998: 18: 321–331.
12. Caton J, Greenstein G, Zappa U. Synthetic bioabsorbablebarrier for regeneration in human periodontal defects.J Periodontol 1994: 65: 1037–1045.
13. Christgau M, Schamlz G, Wenzel A, Hiller KA. Periodontalregeneration of intrabony defects with resorbable andnon-resorbable membranes: 30 month results. J Clin Peri-odontol 1997: 24: 17–27.
14. Cortellini P, Pini-Prato G, Baldi C, Clauser C. Guided tissueregeneration with different materials. Int J PeriodonticsRestorative Dent 1990: 10: 136–151.
15. Cortellini P, Pini-Prato G, Tonetti M. Periodontal regenera-tion of human infrabony defects. I. Clinical measures.J Periodontol 1993: 64: 254–260.
16. Cortellini P, Pini-Prato G, Tonetti M. Periodontal regenera-tion of human infrabony defects. II. Reentry proceduresand bone measures. J Periodontol 1993: 64: 261–268.
17. Cortellini P, Pini-Prato G, Tonetti M. Periodontalregeneration of human infrabony defects. V. Effect of oralhygiene on long term stability. J Clin Periodontol 1994: 21:606–610.
18. Cortellini P, Pini-Prato G, Tonetti M. Interproximal freegingival grafts after membrane removal in GTR treat-ment of infrabony defects. A controlled clinical trialindicating improved outcomes. J Periodontol 1995: 66:488–493.
19. Cortellini P, Pini-Prato G, Tonetti M. Periodontal regenera-tion of human infrabony defects with titanium reinforcedmembranes. A controlled clinical trial. J Periodontol 1995:66: 797–803.
20. Cortellini P, Pini-Prato G, Tonetti M. The modified papillapreservation technique. A new surgical approach for inter-proximal regenerative procedures. J Periodontol 1995: 66:261–266.
21. Cortellini P, Pini-Prato G, Tonetti M. Long term stability ofclinical attachment following guided tissue regenerationand conventional therapy. J Clin Periodontol 1996: 23:106–111.
22. Cortellini P, Pini-Prato G, Tonetti M. Periodontal regenera-tion of human intrabony defects with bioresorbable mem-branes. A controlled clinical trial. J Periodontol 1996: 67:217–223.
23. Cortellini P, Carnevale G, Sanz M, Tonetti MS. Treatmentof deep and shallow intrabony defects. A multicenter ran-domized controlled clinical trial. J Clin Periodontol 1998:25: 981–987.
24. Cortellini P, Tonetti M. Radiographic defect angle influ-ences the outcome of GTR therapy in intrabony defects.J Dent Res 1999: 78: 381 (abstract).
25. Cortellini P, Pini-Prato G, Tonetti M. The simplified papillapreservation flap. A novel surgical approach for the man-agement of soft tissues in regenerative procedures. IntJ Periodontics Restorative Dent 1999: 19: 589–599.
26. Cortellini P, Tonetti MS. Focus on intrabony defects:guided tissue regeneration (GTR). Periodontol 2000 2000:22: 104–132.
27. Cortellini P, Tonetti M. Evaluation of the effect of toothvitality on regenerative outcomes in intrabony defects.J Clin Periodontol 2000: 28: 672–679.
28. Cortellini P, Tonetti MS, Lang NP, Suvan JE, Zucchelli G,Vangsted T, Silvestri M, Rossi R, McClain P, Fonzar A, Du-bravec D, Adriaens P. The simplified papilla preservationflap in the regenerative treatment of deep intrabonydefects: clinical outcomes and postoperative morbidity.J Periodontol 2001: 72: 1701–1712.
29. Cortellini P, Tonetti MS. Microsurgical approach to peri-odontal regeneration. Initial evaluation in a case cohort.J Periodontol 2001: 72: 559–569.
30. Cortellini P, Tonetti MS. Long-term tooth survival follow-ing regenerative treatment of intrabony defects. J Period-ontol 2004: 75: 672–678.
31. Cortellini P, Tonetti MS. Clinical performance of aregenerative strategy for intrabony defects: scientificevidence and clinical experience. J Periodontol 2005: 76:341–350.
32. Cortellini P, Tonetti MS. A minimally invasive surgicaltechnique (MIST) with enamel matrix derivate in theregenerative treatment of intrabony defects: a novelapproach to limit morbidity. J Clin Periodontol 2007: 34:87–93.
33. Cortellini P, Tonetti MS. Minimally invasive surgical tech-nique (M.I.S.T.) and enamel matrix derivative (EMD) in in-trabony defects. (I) Clinical outcomes and intra-operativeand post-operative morbidity. J Clin Periodontol 2007: 34:1082–1088.
34. Cortellini P, Nieri M, Pini Prato GP, Tonetti MS. Singleminimally invasive surgical technique (MIST) with enamelmatrix derivative (EMD) to treat multiple adjacent intrab-ony defects. Clinical outcomes and patient morbidity. JClin Periodontol 2008: 35: 605–613.
35. Cortellini P, Tonetti MS. Minimally invasive surgical tech-nique and enamel matrix derivative (EMD) in intrabonydefects: 2. Factors associated with healing outcomes. Int JPeriodontics Restorative Dent 2009: 29: 256–265.
36. Cortellini P, Tonetti MS. Improved wound stability with amodified minimally invasive surgical technique in theregenerative treatment of isolated interdental intrabonydefects. J Clin Periodontol 2009: 36: 157–163.
37. Cortellini P, Tonetti MS. Clinical and radiographic out-comes of the modified minimally invasive surgical tech-nique with and without regenerative materials: arandomized- controlled trial in intra-bony defects. J ClinPeridontol 2011: 38: 365–373.
38. Cortellini P, Stalpers G, Mollo A, Tonetti MS. Periodontalregeneration versus extraction and prosthetic replacementof teeth severely compromised by attachment loss to theapex: 5-year results of an ongoing randomized clinicaltrial. J Clin Periodontol 2011: 38: 915–924.
39. DeSanctis M, Clauser C, Zucchelli G. Bacterial colonizationof barrier material and periodontal regeneration. J Clin Pe-riodontol 1996: 23: 1039–1046.
40. DeSanctis M, Zucchelli G, Clauser C. Bacterial colonizationof bioabsorbable barrier material and periodontal regener-ation. J Periodontol 1996: 67: 1193–1200.
41. Eickholz P, Krigar DM, Kim TS, Reitmeir P, Rawlinson A.Stability of clinical and radiographic results after guidedtissue regeneration in infrabony defects. J Periodontol2007: 78: 37–46.
Clinical concepts for regenerative therapy in intrabony defects
303
42. Ehmke B, Rudiger SG, Hommens A, Karch H, Flemmig FD.Guided tissue regeneration using a polylactic acid barrier.Part II: predictors influencing treatment outcome. J ClinPeriodontol 2003: 30: 368–374.
43. Esposito M, Grusovin MG, Coulthard P, Worthington HV.Enamel matrix derivative (Emdogain) for periodontal tis-sue regeneration in intrabony defects. Cochrane DatabaseSyst Rev 2005: 19: CD003875.
44. Esposito M, Grusovin MG, Papanikolaou N, Coulthard P,Worthington HV. Enamel matrix derivative (Emdogain) forperiodontal tissue regeneration in intrabony defects.A Cochrane Systematic Review. Eur J Oral Implantol 2009:2: 247–266.
45. Falk H, Laurell L, Ravald N, Teiwik A, Persson R. Guidedtissue regeneration therapy of 203 consecutively treatedintrabony defects using a bioabsorbable matrix barrier.Clinical and radiographic findings. J Periodontol 1997: 68:571–581.
46. Garrett S, Loos B, Chamberlain D, Egelberg J. Treatment ofintraosseous periodontal defects with a combined therapyof citric acid conditioning, bone grafting and placement ofcollagenous membranes. J Clin Periodontol 1988: 15:383–389.
47. Giannobile WV, Somerman MJ. Growth and amelogenin-like factors in periodontal wound healing. A systematicreview. Ann Periodontol 2003: 8: 193–204.
48. Goldman H, Cohen DW. The infrabony pocket:classification and treatment. J Periodontol 1958: 29:272–291.
49. Gottlow J, Nyman S, Karring T, Lindhe J. New attachmentformation as the result of controlled tissue regeneration.J Clin Periodontol 1984: 11: 494–503.
50. Gottlow J, Nyman S, Lindhe J, Karring T, Wennstr€om J.New attachment formation in the human periodontiumby guided tissue regeneration. J Clin Periodontol 1986: 13:604–616.
51. Gottlow J, Nyman S, Karring T. Maintenance of newattachment gained through guided tissue regeneration.J Clin Periodontol 1992: 19: 315–317.
52. Gottlow J, Laurell L, Lundgren D, Mathiesen T, Nyman S,Rylander H, Bogentoft C. Periodontal tissue response to anew bioresorbable guided tissue regeneration device.A longitudinal study in monkeys. Int J Periodontics Restor-ative Dent 1994: 14: 437–449.
53. Guillemin M, Mellonig J, Brunswold M. Healing in peri-odontal defects treated by decalcified freeze-dried bone al-lografts in combination with e-PTFE membranes. (I)Clinical and scanning electron microscope analysis. J ClinPeriodontol 1993: 20: 528–536.
54. Hanes PJ, Purvis JP. Local anti-infective therapy: pharma-cological agents. A systematic review. Ann Periodontol2003: 8: 79–98.
55. Haney JM, Nilveus RE, McMillan PJ, Wikesjo UME.Periodontal repair in dogs: expanded polytetrafluorethyl-ene barrier membranes support wound stabilisation andenhance bone regeneration. J Periodontol 1993: 64: 883–890.
56. Harrel SK, Rees TD. Granulation tissue removal in routineand minimally invasive surgical procedures. CompendContin Educ Dent 1995: 16: 960–967.
57. Harrel TK, Nunn ME. Longitudinal comparison of the peri-odontal status of patients with moderate to severe
periodontal disease receiving no treatment, non-surgicaltreatment, and surgical treatment utilizing individual sitesfor analysis. J Periodontol 2001: 72: 1509–1519.
58. Harrel SK, Wilson TG Jr, Nunn ME. Prospective assessmentof the use of enamel matrix proteins with minimally inva-sive surgery. J Periodontol 2005: 76: 380–384.
59. Heden G, Wennstr€om J, Lindhe J. Periodontal tissue altera-tions following Emdogain treatment of periodontal siteswith angular bone defects. A series of case reports. J ClinPeriodontol 1999: 26: 855–860.
60. Heden G. A case report study of 72 consecutive Emdogain-treated intrabony periodontal defects: clinical and radio-graphic findings after 1 year. Int J Periodontics RestorativeDent 2000: 20: 127–139.
61. Heden G, Wennstrom JL. Five-year follow-up of regenera-tive periodontal therapy with enamel matrix derivative atsites with angular bone defects. J Periodontol 2006: 77:295–301.
62. Heitz-Mayfield L, Tonetti MS, Cortellini P, Lang NP, Euro-pean Research Group on Periodontology (ERGOPERIO).Microbial colonization patterns predict the outcomes ofsurgical treatment of intrabony defects. J Clin Periodontol2006: 33: 62–68.
63. Heijl L, Heden G, Sv€ardstr€om C, Ostgren A. Enamel matrixderivate (EMDOGAIN�) in the treatment of intrabonyperiodontal defects. J Clin Periodontol 1997: 24: 705–714.
64. Hiatt WH, Stallard RE, Butler ED, Badget B. Repair follow-ing mucoperiosteal flap surgery with full gingival reten-tion. J Periodontol 1968: 39: 11–16.
65. Howell TH, Fiorellini JP, Paquette DW, Offenbacher S, Gi-annobile WV, Lynch S. A phase I/II clinical trial to evaluatea combination of recombinant human platelet-derivedgrowth factor-BB and recombinant human insulin-likegrowth factor-I in patients with periodontal disease. J Peri-odontol 1997: 68: 1186–1193.
66. H€urzeler MB, Quinones CR, Caffesse RG, Schupback P,Morrison EC. Guided periodontal tissue regeneration ininterproximal intrabony defects following treatment with asynthetic bioabsorbable barrier. J Periodontol 1997: 68:489–497.
67. Kim CS, Choi SH, Chai JK, Cho KS, Moon IS, Wikesjo UME,Kim CK. Periodontal repair in surgically created intrabonydefects in dogs. Influence of the number on bone walls onhealing response. J Periodontol 2004: 75: 229–235.
68. Kitamura M, Nakashima K, Kowashi Y, Fujii T, ShimauchiH, Sasano T, Furuuchi T, Fukuda M, Noguchi T, ShibutaniT, Iwayama Y, Takashiba S, Kurihara H, Ninomiya M, KidoJ, Nagata T, Hamachi T, Maeda K, Hara Y, Izumi Y, HirofujiT, Imai E, Omae M, Watanuki M, Murakami S. Periodontaltissue regeneration using fibroblast growth factor-2: ran-domized controlled phase II clinical trial. PLoS ONE 2008:3: e2611.
69. Kitamura M, Akamatsu M, Machigashira M, Hara Y, Saka-gami R, Hirofuji T, Hamachi T, Maeda K, Yokota M, Kido J,Nagata T, Kurihara H, Takashiba S, Sibutani T, Fukuda M,Noguchi T, Yamazaki K, Yoshie H, Ioroi K, Arai T, Nakaga-wa T, Ito K, Oda S, Izumi Y, Ogata Y, Yamada S, ShimauchiH, Kunimatsu K, Kawanami M, Fujii T, Furuichi Y, Furuu-chi T, Sasano T, Imai E, Omae M, Yamada S, Watanuki M,Murakami S. FGF-2 stimulates periodontal regeneration:results of a multi-center randomized clinical trial. J DentRes 2011: 90: 35–40.
Cortellini & Tonetti
304

70. Kwok V, Caton J. Prognosis revisited: a system for assign-ing periodontal prognosis. J Periodontol 2007: 78: 2063–2071.
71. Jayakumar A, Rajababu P, Rohini S, Butchibabu K, NaveenA, Krishnajaneya Reddy P, Vidyasagar S, Satyanarayana D,Pavan Kumar S. Multi-centre, randomized clinical trial onefficacy and safety of recombinant human platelet-derivedgrowth factor with b-tricalcium phosphate in humanintra-osseous periodontal defects. J Clin Periodontol 2011:38: 163–172.
72. Lang NP, Tonetti MS. Periodontal diagnosis in treatedperiodontitis. Why, when and how to use clinical parame-ters. J Clin Periodontol 1996: 23: 240–250.
73. Laurell L, Falk H, Fornell J, Johard G, Gottlow J. Clinicaluse of a bioresorbable matrix barrier in guided tissueregeneration therapy. Case series. J Periodontol 1994: 65:967–975.
74. Linares A, Cortellini P, Lang NP, Suvan J, Tonetti MS, Euro-pean Research Group on Periodontology (ErgoPerio).Guided tissue regeneration/deproteinized bovine bonemineral or papilla preservation flaps alone for treatmentof intrabony defects. II: radiographic predictors and out-comes. J Clin Periodontol 2006: 33: 351–358.
75. Linghorne WJ, O’Connel DC. Studies in the regenerationand reattachment of supporting structures of teeth. I. Softtissue reattachment. J Dental Res 1950: 29: 419–428.
76. Lundgren D, Slotte C. Reconstruction of anatomicallycomplicated periodontal defects using a bioresorbableGTR barrier supported by bone mineral. A 6-monthfollow-up study of 6 cases. J Clin Periodontol 1999: 26:56–62.
77. Machtei E, Cho M, Dunford R, Norderyd J, Zambon J, Gen-co R. Clinical, microbiological, and histological factorswhich influence the success of regenerative periodontaltherapy. J Periodontol 1994: 65: 154–161.
78. Machtei E. The effect of membrane exposure on the out-come of regenerative procedures in humans: a meta-analysis. J Periodontol 2001: 72: 512–516.
79. Magnusson I, Nyman S, Karring T, Egelberg J. Connectivetissue attachment formation following exclusion of con-nective tissue and epithelium during healing. J PeriodontRes 1985: 20: 201–208.
80. Magnusson I, Batich C, Collins BR. New attachment for-mation following controlled tissue regeneration using bio-degradable membranes. J Periodontol 1988: 59: 1–6.
81. Matuliene G, Pjetursson BE, Salvi GE, Schmidlin K, Br€aggerU, Zwahlen M, Lang NP. Influence of residual pockets onprogression of periodontitis and tooth loss: results after11 years of maintenance. J Clin Periodontol 2008: 35: 685–695.
82. Mayfield L, S€oderholm G, Hallstr€om H, Kullendorff B, Ed-wardsson S, Bratthall G, Br€agger U, Attstr€om R. Guided tis-sue regeneration for the treatment of intraosseous defectsusing a bioabsorbable membrane. A controlled clinicalstudy. J Clin Periodontol 1998: 25: 585–595.
83. McClain P, Schallhorn RG. Long term assessment of com-bined osseous composite grafting, root conditioning andguided tissue regeneration. Int J Periodontics RestorativeDent 1993: 13: 9–27.
84. McGuire MK, Nunn ME. Prognosis versus actual outcome.II. The effectiveness of clinical parameters in developingan accurate prognosis. J Periodontol 1996: 67: 658–665.
85. McGuire MK, Nunn ME. Prognosis versus actual out-come. III. The effectiveness of clinical parameters inaccurately predicting tooth survival. J Periodontol 1996:67: 658–665.
86. Mellonig JT. Enamel matrix derivate for periodontal recon-structive surgery: Technique and clinical and histologiccase report. Int J Periodontics Restorative Dent 1999: 19:9–19.
87. Mellonig JT. Human histologic evaluation of a bovine-derived bone xenograft in the treatment of periodontalosseous defects. Int J Periodontics Restorative Dent 2000:20: 18–29.
88. Miller SC. Textbook of periodontia (Oral Medicine), 2ndedn. Philadelphia: The Blakiston Co., 1943: 103.
89. Murphy K. Post-operative healing complications associ-ated with Gore-tex periodontal material. Part 1. Incidenceand characterization. Int J Periodontics Restorative Dent1995: 15: 363–375.
90. Murphy KG, Gunsolley JC. Guided tissue regeneration forthe treatment of periodontal intrabony and furcationdefects. A systematic review. Ann Periodontol 2003: 8: 266–302.
91. Needleman IG, Worthington HV, Giedrys-Leeper E, TuckerRJ. Guided tissue regeneration for periodontal infra-bonydefects. Cochrane Database Syst Rev 2006: 19: CD001724.
92. Nevins M, Giannobile WV, McGuire MK, Kao RT, MellonigJT, Hinrichs JE, McAllister BS, Murphy KS, McClain PK,Nevins ML, Paquette DW, Ham TJ, Reddy MS, Lavin PT,Genco RJ, Lynch SE. Platelet-derived growth factor stimu-lates bone fill and rate of attachment level gain: results ofa large multicenter randomised controlled trial. J Period-ontol 2005: 76: 2205–2215.
93. Nickles K, Ratka-Kruger P, Neukranz E, Raetzke P, EickholzP. Open flap debridement and guided tissue regenerationafter 10 years in infrabony defects. J Clin Periodontol 2009:36: 976–983.
94. Nowzari H, Slots J. Microorganisms in polytetrafluoroeth-ylene barrier membranes for guided tissue regeneration.J Clin Periodontol 1994: 21: 203–210.
95. Nowzari H, Matian F, Slots J. Periodontal pathogens onpolytetrafluoroethylene membrane for guided tissueregeneration inhibit healing. J Clin Periodontol 1995: 22:469–474.
96. Nygaard-Østby P, Bakke V, Nesdal O, Susin C, Wikesj€oUME. Periodontal healing following reconstructive sur-gery: effect of guided tissue regeneration using a biore-sorbable barrier device when combined with autogenousbone grafting. A randomized controlled trial 10-year fol-low-up. J Clin Periodontol 2010: 37: 366–373.
97. Nyman S, Lindhe J, Karring T, Rylander H. New attach-ment following surgical treatment of human periodontaldisease. J Clin Periodontol 1982: 9: 290–296.
98. Palmer RM, Cortellini P, Group B of European Workshopon Periodontology. Periodontal tissue engineering andregeneration: consensus Report of the Sixth EuropeanWorkshop on Periodontology. J Clin Periodontol 2008: 35(Suppl. 8): 83–86.
99. Paolantonio M, Scarano A, Di Placido G, Tumini V, D’Ar-chivio D, Piattelli A. Periodontal healing in humans usinganorganic bovine bone and bovine peritoneum-derivedcollagen membrane: a clinical and histologic case report.Int J Periodontics Restorative Dent 2001: 21: 505–515.
Clinical concepts for regenerative therapy in intrabony defects
305
100. Paul BF, Mellonig JT, Towle HJ III, Gray JL. Use of collagenbarrier to enhance healing in human periodontal furcationdefects. Int J Periodontics Restorative Dent 1992: 12:123–131.
101. Pietruska MD. A comparative study on the use of Bio-Ossand enamel matrix derivative (Emdogain) in the treatmentof periodontal bone defects. Eur J Oral Sci 2001: 109: 178–181.
102. Pini Prato GP, Cortellini P, Clauser C. Fibrin and fibronec-tin sealing system in a guided tissue regeneration proce-dure. A case report. J Periodontol 1988: 59: 679–683.
103. Pitaru S, Tal H, Soldinger M, Grosskopf A, Noff M. Partialregeneration of periodontal tissues using collagen barriers.Initial observations in the canine. J Periodontol 1988: 59:380–386.
104. Polimeni G, Xiropaidis VX, Wikesjo UME. Biology andprinciples of periodontal wound healing/regeneration. Pe-riodontol 2000 2006: 41: 30–47.
105. Pretzl B, Kim TS, Steinbrenner H, Dorfer C, Himmer K,Eickholz P. Guided tissue regeneration with bioabsorbablebarriers III 10-year results in infrabony defects. J Clin Peri-odontol 2009: 36: 349–356.
106. Reynolds MA, Aichelmann-Reidy ME, Branch-Mays GL,Gunsolley JC. The efficacy of bone replacement grafts inthe treatment of periodontal osseous defects. A systematicreview. Ann Periodontol 2003: 8: 227–265.
107. Ribeiro FV, Casarin RC, Palma MA, J�unior FH, Sallum EA,Casati MZ. The role of enamel matrix derivative protein inminimally invasive surgery in treating intrabony defects insingle rooted teeth: a randomized clinical trial. J Periodon-tol 2011: 82: 522–532.
108. Ribeiro FV, Casarin RC, Palma MA, J�unior FH, Sallum EA,Casati MZ. Clinical and patient-centered outcomes afterminimally invasive non-surgical or surgical approaches forthe treatment of intrabony defects: a randomized clinicaltrial. J Periodontol 2011: 82: 1256–1266.
109. Rosen PS, Reynolds MA, Bowers GM. The treatment of in-trabony defects with bone grafts. Periodontol 2000 2000:22: 88–103.
110. Sanz M, Tonetti MS, Zabalegui I, Sicilia A, Blanco J, RebeloH, Rasperini G, Merli M, Cortellini P, Suvan JE. Treatmentof intrabony defects with enamel matrix proteins or bar-rier membranes: results from a multicenter practice-basedclinical trial. J Clin Periodontol 2005: 75: 726–733.
111. Sanders JJ, Sepe WW, Bowers GM, Koch RW, Williams JE,Lekas JS, Mellonig JT, Pelleu GB Jr, Gambill V. Clinicalevaluation of freeze-dried bone allografts in periodontalosseous defects. Part III. Composite freeze-dried bone al-lografts with and without autogenous bone grafts. J Peri-odontol 1983: 54: 1–8.
112. Schallhorn RG, Hiatt WH, Boyce W. Iliac transplants inperiodontal therapy. J Periodontol 1970: 41: 566–580.
113. Schallhorn RG, McClain PK. Combined osseous compositegrafting, root conditioning, and guided tissue regenera-tion. Int J Periodontics Restorative Dent 1988: 4: 9–31.
114. Sculean A, Donos N, Chiantella GC, Windisch P, ReichE, Brecx M. GTR with bioresorbable membranes in thetreatment of intrabony defects: a clinical and histologicstudy. Int J Periodontics Restorative Dent 1999: 19: 501–509.
115. Sculean A, Donos N, Windisch P, Brecx M, Gera I, Reich E,Karring T. Healing of human intrabony defects following
treatment with enamel matrix proteins or guided tissueregeneration. J Periodontal Res 1999: 34: 310–322.
116. Sculean A, Berakdar M, Chiantella GC, Donos N, ArweilerNB, Brecx M. Healing of intrabony defects following treat-ment with a bovine-derived xenograft and collagen mem-brane. A controlled clinical study. J Clin Periodontol 2003:30: 73–80.
117. Sculean A, Schwarz F, Miliauskaite A, Kiss A, Arweiler N,Becker J, Brecx M. Treatment of infrabony defects with anenamel matrix protein derivative or bioresorbable mem-brane: an 8-year follow-up split-mouth study. J Periodon-tol 2006: 77: 1879–1886.
118. Sculean A, Kiss A, Miliauskaite A, Schwarz F, Arweiler NB,Hannig M. Ten-year results following treatment of intra-bony defects with enamel matrix proteins and guidedtissue regeneration. J Clin Periodontol 2008: 35: 817–824.
119. Selvig K, Kersten B, Chamberlain A, Wikesjo UME, NilveusR. Regenerative surgery of intrabony periodontal defectsusing e-PTFE barrier membranes. Scanning electronmicroscopic evaluation of retrieved membranes vs. clinicalhealing. J Periodontol 1992: 63: 974–978.
120. Selvig K, Kersten B, Wikesj€o UME. Surgical treatment of in-trabony periodontal defects using expanded polytetraflu-oroethylene barrier membranes: influence of defectconfiguration on healing response. J Periodontol 1993: 64:730–733.
121. Sigurdsson TJ, Hardwick R, Bogle GC, Wikesjo UME. Peri-odontal repair in dogs: space provision by reinforced ePT-FE membranes enhances bone and cementumregeneration in large supraalveolar defects. J Periodontol1994: 65: 350–356.
122. Silvestri M, Ricci G, Rasperini G, Sartori S, Cattaneo V.Comparison of treatments of infrabony defects withenamel matrix derivate, guided tissue regeneration with anonresorbable membrane and Widman modified flap. Apilot study. J Clin Periodontol 2000: 27: 603–610.
123. Silvestri M, Sartori S, Rasperini G, Ricci G, Rota C, Catta-neo V. Comparison of infrabony defects treated withenamel matrix derivative versus guided tissue regenera-tion with a nonresorbable membrane. A multicenter con-trolled clinical trial. J Clin Periodontol 2003: 30: 386–393.
124. Slotte C, Asklow B, Lundgren D. Surgical guided tissueregeneration treatment of advanced periodontal defects: a5-year follow-up study. J Clin Periodontol 2007: 34: 977–984.
125. Smith MacDonald E, Nowzari H, Contreras A, Flynn J,Morrison J, Slots J. Clinical evaluation of a bioabsorbableand a nonresorbable membrane in the treatment ofperiodontal intraosseous lesions. J Periodontol 1998: 69:445–453.
126. Stavropoulos A, Karring ES, Kostopoulos L, Karring T. De-proteinized bovine bone and gentamicin as an adjunct toGTR in the treatment of intrabony defects: a randomizedcontrolled clinical study. J Clin Periodontol 2003: 30:486–495.
127. Stavropoulos A, Mardas N, Herrero F, Karring T. Smokingaffects the outcome of guided tissue regeneration with bi-oresorbable membranes: a retrospective analysis of intrab-ony defects. J Clin Periodontol 2004: 31: 945–950.
128. Stavropoulos A, Windisch P, Gera I, Capsius B, Sculean A,Wikesjo UME. A phase IIa randomized controlled clinicaland histological pilot study evaluating rhGDF-5/b-TCP for
Cortellini & Tonetti
306
periodontal regeneration. J Clin Periodontol 2011: 38:1044–1054.
129. Steffensen B, Weber HP. Relationship between the radio-logic periodontal defect angle and healing after treatment.J Periodontol 1989: 60: 248–254.
130. Tanner MG, Solt CW, Vuddhakanok S. An evaluation ofnew attachment formation using a microfibrillar collagenbarrier. J Periodontol 1988: 59: 524–530.
131. Tonetti M, Pini-Prato G, Cortellini P. Periodontal regenera-tion of human infrabony defects. IV. Determinants of thehealing response. J Periodontol 1993: 64: 934–940.
132. Tonetti M, Pini-Prato G, Cortellini P. Effect of cigarettesmoking on periodontal healing following GTR in infrab-ony defects. A preliminary retrospective study. J Clin Peri-odontol 1995: 22: 229–234.
133. Tonetti M, Pini-Prato G, Cortellini P. Factors affecting thehealing response of intrabony defects following guided tis-sue regeneration and access flap surgery. J Clin Periodon-tol 1996: 23: 548–556.
134. Tonetti M, Cortellini P, Suvan JE, Adriaens P, Baldi C, Du-bravec D, Fonzar A, Fourmosis I, Magnani C, Muller-Cam-panile V, Patroni S, Sanz M, Vangsted T, Zabalegui I, PiniPrato G, Lang NP. Generalizability of the added benefits ofguided tissue regeneration in the treatment of deepintrabony defects. Evaluation in a multi-center random-ized controlled clinical trial. J Periodontol 1998: 69: 1183–1192.
135. Tonetti MS, Lang NP, Cortellini P, Suvan JE, Adriaens P,Dubravec D, Fonzar A, Fourmousis I, Mayfield L, Rossi R,Silvestri M, Tiedemann C, Topoll H, Vangsted T, Wall-kamm B. Enamel matrix proteins in the regenerative ther-apy of deep intrabony defects. A multicenter randomizedcontrolled clinical trial. J Clin Periodontol 2002: 29: 317–325.
136. Tonetti MS, Cortellini P, Lang NP, Suvan JE, Adriaens P,Dubravec D, Fonzar A, Fourmousis I, Rasperini G, Rossi R,Silvestri M, Topoll H, Wallkamm B, Zybutz M. Clinical out-comes following treatment of human intrabony defectswith GTR/bone replacement material or access flap alone.A multicenter randomized controlled clinical trial. J ClinPeriodontol 2004: 31: 770–776.
137. Tonetti MS, Fourmousis I, Suvan J, Cortellini P, Bragger U,Lang NP, European Research Group on Periodontology(ERGOPERIO). Healing, post-operative morbidity andpatient perception of outcomes following regenerativetherapy of deep intrabony defects. J Clin Periodontol 2004:31: 1092–1098.
138. Trejo PM, Weltman R, Caffesse R. Treatment of intraos-seous defects with bioabsorbable barrier alone or incombination with decalcified freeze-dried bone allograft: arandomized clinical trial. J Periodontol 2000: 71: 1852–1861.
139. Trejo PM, Weltman RL. Favourable periodontalregenerative outcomes from teeth with presurgical
mobility: a retrospective study. J Clin Periodontol 2004: 75:1532–1538.
140. Trombelli L, Kim CK, Zimmerman GJ, Wikesj€o UME. Ret-rospective analysis of factors related to clinical outcome ofguided tissue regeneration procedures in intrabonydefects. J Clin Periodontol 1997: 24: 366–371.
141. Trombelli L, Heitz-Mayfield LJ, Needleman I, Moles D,Scabbia A. A systematic review of graft materials and bio-logical agents for periodontal intraosseous defects. J ClinPeriodontol 2002: 29(Suppl. 3): 117–135.
142. Trombelli L, Farina R. Clinical outcomes with bioactiveagents alone or in combination with grafting or guidedtissue regeneration. J Clin Periodontol 2008: 35(Suppl.):117–135.
143. Trombelli L, Simonelli A, Pramstraller M, Wikesjo UME,Farina R. Single flap approach with and without guidedtissue regeneration and a hydroxyapatite biomaterial inthe management of intraosseous periodontal defects. J Pe-riodontol 2010: 81: 1256–1263.
144. Tsitoura E, Tucker R, Suvan J, Laurell L, Cortellini P, To-netti M. Baseline radiographic defect angle of the intrab-ony defect as a prognostic indicator in regenerativeperiodontal surgery with enamel matrix derivative. J ClinPeriodontol 2004: 31: 643–647.
145. Tu Y-K, Woolston A, Faggion CM Jr. Do bone grafts or bar-rier membranes provide additional treatment effects forinfrabony lesions treated with enamel matrix derivatives?A network meta-analysis of randomized-controlled trials.J Clin Periodontol 2010: 37: 59–79.
146. Tunkel J, Heinecke A, Flemmig TF. A systematic review ofefficacy of machine-driven and manual subgingivaldebridement in the treatment of chronic periodontitis.J Clin Periodontol 2002: 29(Suppl. 3): 72–81.
147. Yukna R, Mellonig JT. Histologic evaluation of periodontalhealing in humans following regenerative therapy withenamel matrix derivative. A 10-case series. J Periodontol2000: 71: 752–759.
148. Wachtel H, Schenk G, Bohm S, Weng D, Zuhr O, HurzelerMB. Microsurgical access flap and enamel matrix deriva-tive for the treatment of periodontal intrabony defects: acontrolled clinical study. J Clin Periodontol 2003: 30: 496–504.
149. Wang HL, O’Neal RB, Thomas CL, Shyr Y, Macneil RL.Evaluation of an absorbable collagen membrane intreating class II furcation defects. J Periodontol 1994: 65:1029–1036.
150. Wikesjo UME, Nilveus R. Periodontal repair in dogs: effectof wound stabilisation on healing. J Periodontol 1990: 61:719–724.
151. Wikesjo UME, Lim WH, Thomson RC, Cook AD, HardwickWR. Periodontal repair in dogs: gingival tissue occlusion, acritical require- ment for guided tissue regeneration. J ClinPeriodontol 2003: 30: 655–664.
Clinical concepts for regenerative therapy in intrabony defects
307





























