Embed Size (px)
Citation preview

A
Clinical cases with Coversyl 10 mg
For upgraded beneFits in hypertension

This brochure, “Clinical cases with Coversyl 10 mg
for upgraded benefits in hypertension,” illustrates
a variety of hypertensive patients you may encounter
and shows how effective Coversyl 10 mg is at reducing
blood pressure and cardiovascular complications in
these types of patient.
Throughout this issue, you will discover why Coversyl
up to 10 mg holds a privileged position among
antihypertensive drugs, both as a monotherapy and
as an alternative to other therapies.
This brochure presents reports on 5 patients from
real-life clinical practice and explains the most
appropriate therapeutic strategies according to
evidence-based medicine.
We hope you will appreciate this brochure, which
will not only provide you with valuable scientific
information, but also with advice and practical
guidance for improving the management of
hypertension with Coversyl 10 mg.
Editorial
1 A newly diagnosed patient p 2
2 A hypertensive patient p 4
uncontrolled on ARBs
3 A hypertensive patient p 6
uncontrolled on an ACE inhibitor
4 A hypertensive patient p 8
with dyslipidemia
5 A hypertensive patient p 10
with coronary artery disease
Contents
Note: This brochure presents results expressed with Coversyl arginine (5 or 10 mg/day), which is bioequivalent to Coversyl 4 or 8 mg/day (perindopril tert-butylamine).
1
newly diagnosed patient
soMMaiRe
uncontRolled on aRBs
uncontRolled on aRBs
with dyslipideMia
with coRonaRy aRteRy disease

2
1. A newly diagnosed hypertensive patient
The CONFIDENCE Study: “This study is the first demonstration of the antihypertensive benefits of uptitration to perindopril 10 mg/day* in hypertensive patients without CAD. Therefore, uptitration to the full dose of perindopril may be considered as an effective approach for improving the management of hypertensive patients.”Tsoukas G et al. Am J Cardiovasc Drugs. 2011; 11 (1): 45-55.
case report• Man • 53 years old • Relatively marked obesity: weight 105 kg,
height 185 cm (body mass index 30 kg/m2)• Smoker (one cigar every evening)• Little physical activity
At a recent visit to the doctor for episodes of insomnia, the general practitioner noted a high blood pressure of 160/102 mm Hg. The rest of the examination was normal.
A complete examination was ordered because of these BP values, his obesity, and his moderate smoking. The examination was intended to confirm the existence of high blood pressure, determine other risk factors, and assess possible consequences of the high blood pressure, whose precise duration was not known.
the examination• Laboratory tests Cholesterol was within the normal range, but
blood sugar was 1.15 g/L (6.38 mmol/L).
• Electrocardiogram Sinus rhythm of 66 beats/min PR interval = 0.16 sec QRS axis =+ 70° Normal ventricular repolarization
comments This patient has systolic-diastolic high blood pressure and two risk factors, obesity and moderate smoking. In addition, his blood sugar is considered to be at the limit of normal. Antihypertensive treatment involves proposing a therapeutic class to this patient that offers BP-lowering efficacy and protection of target organs. It was recommended that the patient lose weight, take regular physical exercise (1 hour of walking a day), and stop smoking. Quarterly surveillance with measurement of blood pressure and a plasma glucose assay was also advised.
therapeutic objective:• Choose an appropriate first-line therapy • Choose the right dose• Control BP with SBP <140 mm Hg and DBP
< 90 mm Hg• Reduce risk of cardiovascular events and
mortality
Why Coversyl 10 mg ?
1. ace inhibitors: a first-choice option in young hypertensive patients
The joint BHS/NICE guidelines for the treatment of hypertension were updated and now recommend that in newly diagnosed patients under 55 years of age, an ACE inhibitor be used as the first-line treatment (Figure 1).1
Figure 1. ace inhibitors are recommended as the first-choice treatment in young hypertensive patients. NCGC/NICE 2011 guidelines in clinical management of primary hypertension in adults (NCGC: National Clinical Guidelines Center, NICE: National Institute for Health and Clinical Excellence).
ncgc/nice 2011 hypertension guidelines
consider 4th-line drug• a-blocker• further diuretic therapy • β-blocker • consider seeking specialist advice
< 55 yrs ≥ 55 yrs or any age if black
a = ace inhibitoror low cost ARB (*consider ARB if ACE inhibitor intolerant)C = calcium channel blockerD = thiazide-like diuretic (e.g. indapamide or chlorthalidone, instead of hydrochlorothiazide)
a* c
a* + c + d
a* + c
*Results expressed with Coversyl arginine 10 mg/day, which is bioequivalent to Coversyl tert-butylamine 8 mg/day used in the CONFIDENCE study.
Single agent at low dose
Two- to three-drug combination at full doses
Full-dose monotherapy
Mild BP elevation Low/moderate CV risk Conventional BP target
previous agent at full dose
Switch to different agent at low dose
3
2. objective: full-dose monotherapy with 10 mg
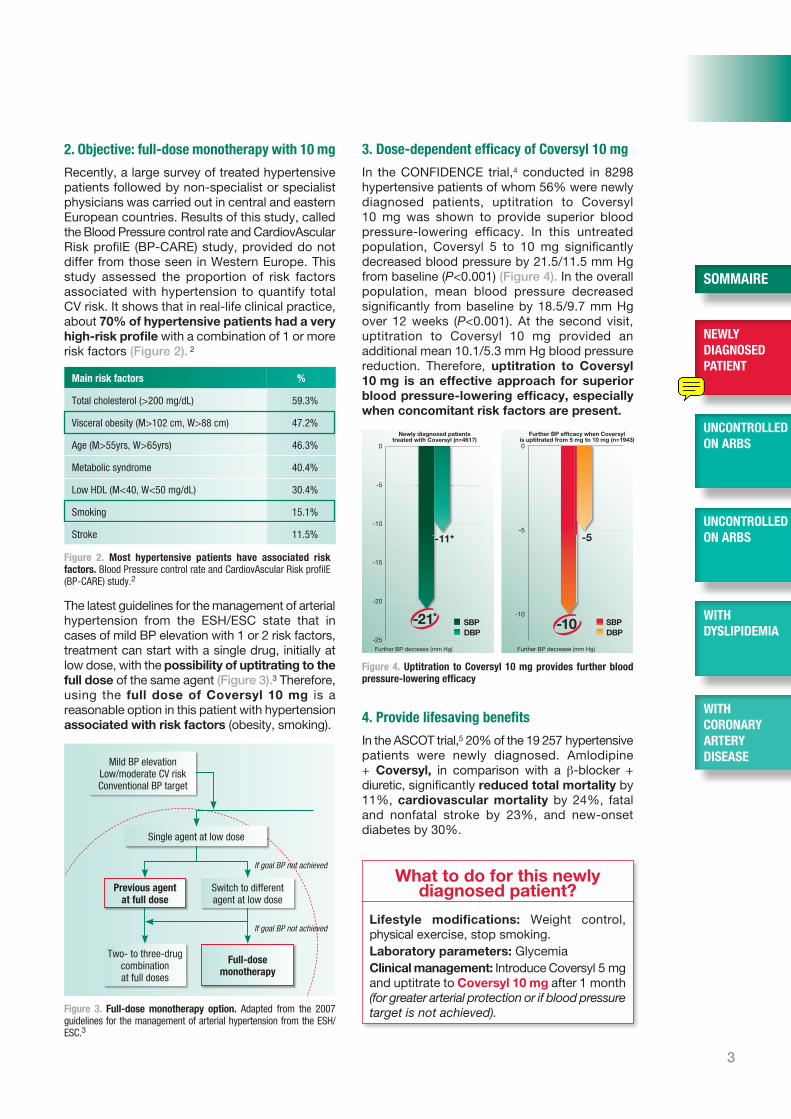
Recently, a large survey of treated hypertensive patients followed by non-specialist or specialist physicians was carried out in central and eastern European countries. Results of this study, called the Blood Pressure control rate and CardiovAscular Risk profilE (BP-CARE) study, provided do not differ from those seen in Western Europe. This study assessed the proportion of risk factors associated with hypertension to quantify total CV risk. It shows that in real-life clinical practice, about 70% of hypertensive patients had a very high-risk profile with a combination of 1 or more risk factors (Figure 2). 2
The latest guidelines for the management of arterial hypertension from the ESH/ESC state that in cases of mild BP elevation with 1 or 2 risk factors, treatment can start with a single drug, initially at low dose, with the possibility of uptitrating to the full dose of the same agent (Figure 3).3 Therefore, using the full dose of Coversyl 10 mg is a reasonable option in this patient with hypertension associated with risk factors (ob esity, smoking).
3. dose-dependent efficacy of coversyl 10 mg
In the CONFIDENCE trial,4 conducted in 8298 hypertensive patients of whom 56% were newly diagnosed patients, uptitration to Coversyl 10 mg was shown to provide superior blood pressure-lowering efficacy. In this untreated population, Coversyl 5 to 10 mg significantly decreased blood pressure by 21.5/11.5 mm Hg from baseline (P<0.001) (Figure 4). In the overall population, mean blood pressure decreased significantly from baseline by 18.5/9.7 mm Hg over 12 weeks (P<0.001). At the second visit, uptitration to Coversyl 10 mg provided an additional mean 10.1/5.3 mm Hg blood pressure reduction. Therefore, uptitration to Coversyl 10 mg is an effective approach for superior blood pressure-lowering efficacy, especially when concomitant risk factors are present.
4. provide lifesaving benefits
In the ASCOT trial,5 20% of the 19 257 hypertensive patients were newly diagnosed. Amlodipine + Coversyl, in comparison with a β-blocker + diuretic, significantly reduced total mortality by 11%, cardiovascular mortality by 24%, fatal and nonfatal stroke by 23%, and new-onset diabetes by 30%.
What to do for this newly diagnosed patient?
Lifestyle modifications: Weight control, physical exercise, stop smoking. Laboratory parameters: Glycemia Clinical management: Introduce Coversyl 5 mg and uptitrate to Coversyl 10 mg after 1 month (for greater arterial protection or if blood pressure target is not achieved).
0
-5
-10
-15
-20
-25Further BP decrease (mm Hg)
Newly diagnosed patientstreated with Coversyl (n=4617)
SBPDBP
-11*
-21*
0
-5
-10
Further BP decrease (mm Hg)
Further BP efficacy when Coversylis uptitrated from 5 mg to 10 mg (n=1943)
SBPDBP
-5
-10
Figure 2. Most hypertensive patients have associated risk factors. Blood Pressure control rate and CardiovAscular Risk profilE (BP-CARE) study.2
Figure 4. uptitration to coversyl 10 mg provides further blood pressure-lowering efficacy
Figure 3. Full-dose monotherapy option. Adapted from the 2007 guidelines for the management of arterial hypertension from the ESH/ESC.3
Main risk factors %
Total cholesterol (>200 mg/dL) 59.3%
Visceral obesity (M>102 cm, W>88 cm) 47.2%
Age (M>55yrs, W>65yrs) 46.3%
Metabolic syndrome 40.4%
Low HDL (M<40, W<50 mg/dL) 30.4%
Smoking 15.1%
Stroke 11.5%
If goal BP not achieved
If goal BP not achieved
newly diagnosed patient
soMMaiRe
uncontRolled on aRBs
uncontRolled on aRBs
with dyslipideMia
with coRonaRy aRteRy disease
4
2. A hypertensive patient uncontrolled on ARBs
“Perindopril-based regimens were associated with a statistically significant reduction in all-cause mortality (HR, 0.87; 95% CI, 0.81 to 0.94; P<0.0001), whereas the remaining ACE inhibitors were not.” “No significant reduction in all-cause mortality could be demonstrated with ARBs.” Meta-analysis on all-cause mortality in hypertension trials: Bertrand ME et al. Eur Heart J. 2011;Vol.32(Abstract Supplement):13.
case report• Man • 54 years old • No particular cardiovascular history, either
personal or family • Travels a lot in Europe• Treated with losartan 50 mg/day in the morning
for 2 years.
He has experienced recent episodes of asthenia, for which he has been seeing a doctor. He has no suggestive symptoms or signs. Blood pressure values 1 month apart revealed high systolic blood pressure with diastolic pressure at the upper normal limit (158/85 mm Hg). The rest of the clinical examination was normal.
the examination• Laboratory tests Total cholesterol: 156 mg/dL (4.02 mmol/L) HDL cholesterol: 37 mg/dL (0.95 mmol/L) LDL cholesterol: 107 mg/dL (2.74 mmol/L) Plasma glucose: 91 mg/dL (5.05 mmol/L)
• Electrocardiogram Sinus rhythm of 80 beats/min PR interval = 0.14 sec QRS axis = - 10° Normal repolarization
commentsThis patient continues to have high blood pressure in spite of treatment with losartan, which suggests that his medical treatment should be reconsidered and that regular physical exercise and a healthy diet be recommended.
therapeutic objective:• Provide further BP-lowering efficacy • Control BP with SBP <140 mm Hg and DBP
<90 mm Hg• Ensure 24-hour BP control • Provide cardiovascular protection (evidence-
based medicine) and lifesaving benefits
Why Coversyl 10 mg ?
1. switch to the right dose of coversyl
In patients uncontrolled on ARBs, it is usual to add a thiazide diuretic and then prescribe a fixed-dose ARB/hydrochlorothiazide combination. This is easy to do, but are optimal efficacy and cardiovascular protection actually provided? Recent data showed that the use of a diuretic such as hydrochlorothiazide (HCTZ) could increase the risk of new-onset diabetes1 or lead to a higher risk of events.2,3
In this particular clinical case, the renin-angiotensin system has been inhibited by the ARB losartan, but the BP of this patient is not controlled by this agent anymore. One of the options from the latest guidelines for the management of arterial hypertension from the ESH/ESC states that it is reasonable to switch to another agent, at the full monotherapy dose of this agent, if the BP goal is not achieved.4 Unlike ARBs, by simultaneously inhibiting the interaction of angiotensin II with its different receptors (AT1, AT2, AT4) and by increasing levels of circulating bradykinin, Coversyl provides a more complete mode of action to inhibit the renin-angiotensin system. This increased level of circulating bradykinin may explain Coversyl’s additional benefits in terms of cardiovascular protection. Therefore, losartan treatment could be switched to Coversyl (up to 10 mg) for further blood pressure-lowering efficacy and proven cardiovascular benefits (the dose of Coversyl should be individualized according to the patient profile and blood pressure response).
2. Further Bp-lowering efficacy
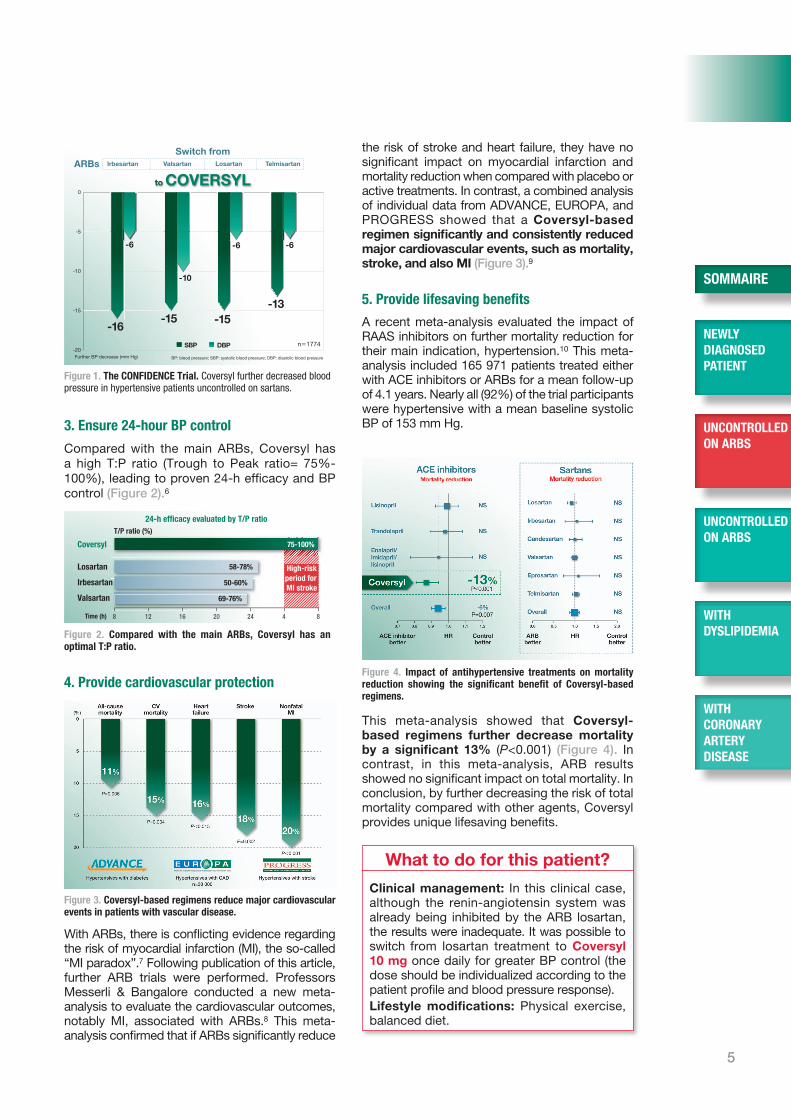
In the CONFIDENCE trial, hypertensive patients uncontrolled on other ACE inhibitors or sartans were switched to Coversyl, and uptitrated to 10 mg if necessary.5 In this everyday hypertensive population, Coversyl provided a further 16/8 mm Hg BP decrease in uncontrolled patients after switching from a sartan (Figure 1). Therefore, Coversyl, up to a dose of 10 mg, is an excellent choice for patients uncontrolled on sartans.
5
3. ensure 24-hour Bp control
Compared with the main ARBs, Coversyl has a high T:P ratio (Trough to Peak ratio= 75%-100%), leading to proven 24-h efficacy and BP control (Figure 2).6
4. provide cardiovascular protection
With ARBs, there is conflicting evidence regarding the risk of myocardial infarction (MI), the so-called “MI paradox”.7 Following publication of this article, further ARB trials were performed. Professors Messerli & Bangalore conducted a new meta-analysis to evaluate the cardiovascular outcomes, notably MI, associated with ARBs.8 This meta-analysis confirmed that if ARBs significantly reduce
This meta-analysis showed that Coversyl-based regimens further decrease mortality by a significant 13% (P<0.001) (Figure 4). In contrast, in this meta-analysis, ARB results showed no significant impact on total mortality. In conclusion, by further decreasing the risk of total mortality compared with other agents, Coversyl provides unique lifesaving benefits.
What to do for this patient?
Clinical management: In this clinical case, although the renin-angiotensin system was already being inhibited by the ARB losartan, the results were inadequate. It was possible to switch from losartan treatment to Coversyl 10 mg once daily for greater BP control (the dose should be individualized according to the patient profile and blood pressure response). Lifestyle modifications: Physical exercise, balanced diet.
Figure 4. impact of antihypertensive treatments on mortality reduction showing the significant benefit of coversyl-based regimens.
Figure 3. coversyl-based regimens reduce major cardiovascular events in patients with vascular disease.
Switch from
to COVERSYL0
-5
-10
-15
-20Further BP decrease (mm Hg) BP: blood pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure
-10
-6-6
-13
n�1774
Losartan Valsartan Telmisartan Irbesartan
-15
-6
-16
ARBs
-15
SBP DBP
Figure 1. the conFidence trial. Coversyl further decreased blood pressure in hypertensive patients uncontrolled on sartans.
Figure 2. compared with the main aRBs, coversyl has an optimal t:p ratio.
the risk of stroke and heart failure, they have no significant impact on myocardial infarction and mortality reduction when compared with placebo or active treatments. In contrast, a combined analysis of individual data from ADVANCE, EUROPA, and PROGRESS showed that a Coversyl-based regimen significantly and consistently reduced major cardiovascular events, such as mortality, stroke, and also MI (Figure 3).9
5. provide lifesaving benefits
A recent meta-analysis evaluated the impact of RAAS inhibitors on further mortality reduction for their main indication, hypertension.10 This meta-analysis included 165 971 patients treated either with ACE inhibitors or ARBs for a mean follow-up of 4.1 years. Nearly all (92%) of the trial participants were hypertensive with a mean baseline systolic BP of 153 mm Hg.
T/P ratio (%)
Time (h)
High-riskperiod for MI stroke
75-100%
24-h efficacy evaluated by T/P ratio
8 12 16 20 24 4 8
Coversyl
Losartan
Irbesartan
Valsartan
58-78%
50-60%
69-76%
newly diagnosed patient
soMMaiRe
uncontRolled on aRBs
uncontRolled on aRBs
with dyslipideMia
with coRonaRy aRteRy disease

6
3. A hypertensive patient uncontrolled on an ACE inhibitor
The PREFER Study: “Perindopril 5–10 mg/day lowers blood pressure and pulse pressure and improves blood pressure control among hypertensive patients who were previously unresponsive to other ACE inhibitor-based regimens”. Ionescu DD et al. Clin Drug Investig. 2009; 29 (12): 767-776.
Choosing “correct dosages to ensure effective and homogeneous 24-hour BP reduction.” The Correct Administration of Antihypertensive Drugs. Taddei S et al. Am J Cardiovasc Drugs. 2011; 11 (1): 13-20.
case report• Woman• 53 years old • Still active, but sometimes she experienced
considerable fatigue with a sensation of tachycardia, but no suspicious chest pain
• Mild-to-moderate high blood pressure• No other coronary risk factors• Treated with ramipril 10 mg/day• No other treatment.
Cardiac auscultation revealed a very discreet systolic murmur from a mitral insufficiency diagnosed some time ago. In spite of treatment with ramipril, her blood pressure values remained high at 156/88 mm Hg.
the examination• Electrocardiogram sinus rhythm of 75 beats/min, PR interval = 0.20 sec QRS axis = +25° Normal repolarization
• Ultrasonography Heart volume: normal with a conserved
ejection fraction Grade I mitral insufficiency in the left atrium
within normal limits. No pulmonary hypertension. This ultrasonography was identical to one conducted 2 years before.
comments The symptomatology of this patient is unrelated to her mitral insufficiency, which does not involve the heart or lungs. Her symptoms might result from increased pressure values that can be managed by changing the angiotensin-converting enzyme inhibitor and possibly adding a calcium channel blocker or a diuretic if possible.
In the PREFER study,2 the antihypertensive efficacy of Coversyl 5 and 10 mg was evaluated in 824 hypertensive patients inadequately controlled on previous treatment with ACE inhibitors. They were receiving an ACE inhibitor as monotherapy (21.5%) or in combination (78.5%) with β-blockers, diuretics, or CCBs. At 3 months, the switch
therapeutic objective:• Provide further BP-lowering efficacy • Control BP with SBP <140 mm Hg and DBP
<90 mm Hg• Ensure 24-hour BP control • Provide cardiovascular protection (evidence-
based medicine) and lifesaving benefits
Why Coversyl 10 mg ?
1. change to another ace inhibitor
In young hypertensive patients under 55 years old, guidelines recommend ACE inhibitors as a first-line option.1 This patient is uncontrolled on ramipril, therefore it would be useful to change from this to another ACE inhibitor that simultaneously provides further blood pressure-lowering efficacy, 24-h blood pressure control, and cardiovascular protection.
Figure 1. the pReFeR trial. Coversyl further decreased blood pressure in hypertensive patients uncontrolled on other ACE inhibitors.
7
to Coversyl (up to 10 mg in 57% of patients) provided an additional reduction in blood pressure of -26/-13 mm Hg, whatever the ACE inhibitor initially prescribed at usual dosage (Figure 1). Therefore, the PREFER trial shows that choosing Coversyl, at a dose up to 10 mg, is a valuable option in uncontrolled patients on other ACE inhibitors.
2. ensure 24-hour Bp control and optimal ace inhibition
There is no class effect among ACE inhibitors. They are commonly believed to be similar, as they all belong to the same class of drugs. However, although all ACE inhibitors inhibit the angiotensin-converting enzyme and decrease blood pressure, they also present many pharmacokinetic and pharmacodynamic differences Coversyl has very high and long-lasting tissue ACE affinity, a very high bradykinin/angiotensin ratio, as well as the best 24-hour BP control (Figure 2).3-7
In addition, Coversyl has an excellent tolerability profile, with a very low rate of cough that is not dose-dependent.8 A recent meta-analysis involving 200 000 patients from 125 ACE inhibitor trials reported the lowest incidence of cough for Coversyl of the 9 main ACE inhibitors (including ramipril, benazepril, enalapril, etc.) observed.9
3. provide lifesaving benefits in hypertension
A recent meta-analysis evaluated the impact of RAAS inhibitors on further mortality reduction for their main indication, hypertension.10 This meta-analysis included 165 971 patients treated with either ACE inhibitors or ARBs for a mean follow-up period of 4.1 years. Nearly all (92%) of the trial participants were hypertensive (inclusion criteria: >66% of patients had hypertension), with a mean baseline systolic BP of 153 mm Hg.
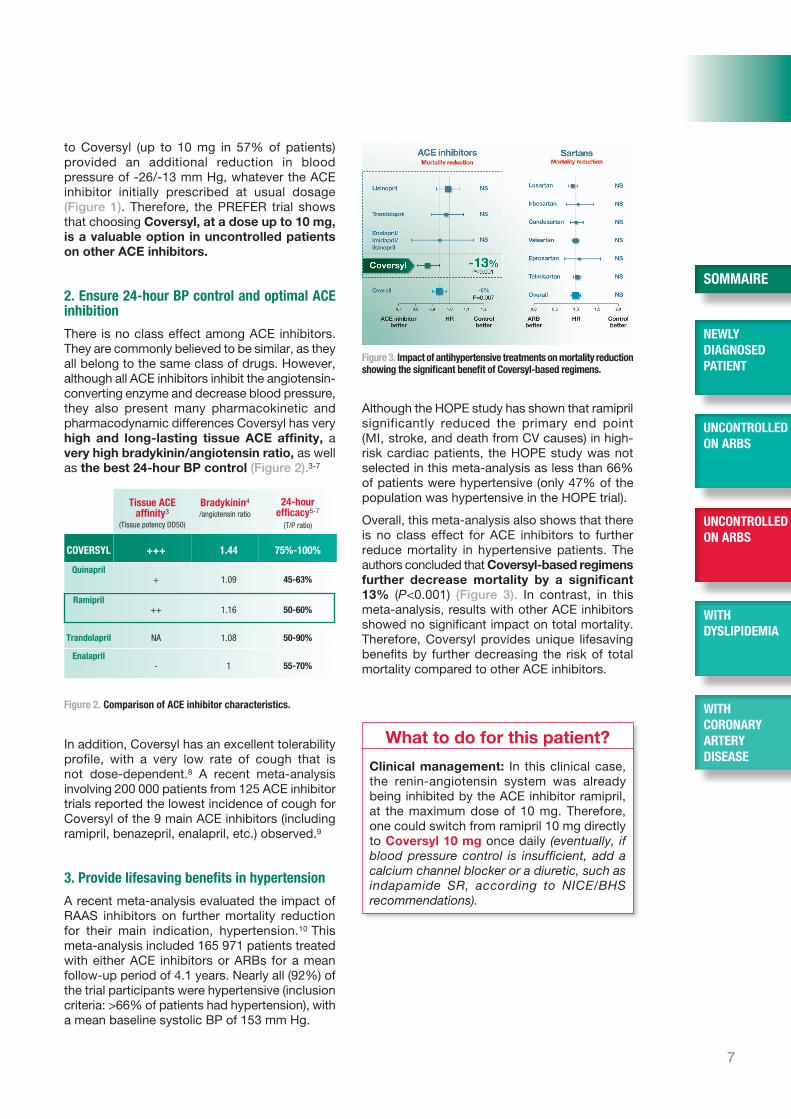
Although the HOPE study has shown that ramipril significantly reduced the primary end point (MI, stroke, and death from CV causes) in high-risk cardiac patients, the HOPE study was not selected in this meta-analysis as less than 66% of patients were hypertensive (only 47% of the population was hypertensive in the HOPE trial).
Overall, this meta-analysis also shows that there is no class effect for ACE inhibitors to further reduce mortality in hypertensive patients. The authors concluded that Coversyl-based regimens further decrease mortality by a significant 13% (P<0.001) (Figure 3). In contrast, in this meta-analysis, results with other ACE inhibitors showed no significant impact on total mortality. Therefore, Coversyl provides unique lifesaving benefits by further decreasing the risk of total mortality compared to other ACE inhibitors.
What to do for this patient?
Clinical management: In this clinical case, the renin-angiotensin system was already being inhibited by the ACE inhibitor ramipril, at the maximum dose of 10 mg. Therefore, one could switch from ramipril 10 mg directly to Coversyl 10 mg once daily (eventually, if blood pressure control is insufficient, add a calcium channel blocker or a diuretic, such as indapamide SR, according to NICE/BHS recommendations).
Figure 3. impact of antihypertensive treatments on mortality reduction showing the significant benefit of coversyl-based regimens.
Figure 2. comparison of ace inhibitor characteristics.
tissue ace affinity3
(Tissue potency DD50)
Bradykinin4
/angiotensin ratio 24-hour
efficacy5-7
(T/P ratio)
coveRsyl +++ 1.44 75%-100%
Quinapril+ 1.09 45-63%
Ramipril++ 1.16 50-60%
trandolapril NA 1.08 50-90%
enalapril- 1 55-70%
newly diagnosed patient
soMMaiRe
uncontRolled on aRBs
uncontRolled on aRBs
with dyslipideMia
with coRonaRy aRteRy disease

NCGC/NICE 2011 hypertension guidelines
Consider 4th-line drug• a-blocker•furtherdiuretictherapy• β-blocker•considerseekingspecialistadvice
<55yrs ≥55yrsoranyageifblack
A = ACE inhibitororlowcostARB(*considerARBifACEinhibitorintolerant)C=calciumchannelblockerD=thiazide-likediuretic(e.g.indapamideorchlorthalidone,insteadofhydrochlorothiazide)
A* C
A* + C + D
A* + C





























