Embed Size (px)
Citation preview
Clinical Cases: Difficult Sleep Cases in Women
Katherine M. Sharkey, MD, PhDDepartments of Medicine and Psychiatry & Human Behavior
Alpert Medical School Brown University Rhode Island Hospital
Conflict of Interest Disclosure
Type of Potential Conflict Details of Potential Conflict
Grant/Research SupportHarmony Biosciences research support
Consultant Verily
Speakers’ Bureaus
Financial support
Other Up-to-Date Royalties
X
X
1.2.
Case 1• 37 yo woman with narcolepsy dx age 19• Sx started in high school: falling sleep in
class, daily napping, cataplexy, hypnogichallucinations
• Presented as new patient 11 weeks into her first pregnancy
• Medications: sodium oxybate 9 grams, armodafinil 250 mg and escitalopram 10 mg
• Previous physician took her out of work
What do you do next?• Stop all medications• Decrease all medications• Continue all medications• Discontinue armodafinil and escitalopram,
continue sodium oxybate• Discontinue armodafinil, continue
escitalopram and sodium oxybate• Something else
What do you do next?• Stop all medications• Decrease all medications• Continue all medications• Discontinue armodafinil and escitalopram,
continue sodium oxybate• Discontinue armodafinil, continue
escitalopram and sodium oxybate• Discuss risks/benefits/side
effects/alternatives with patient, seek to understand patient’s preferences/concerns
Drug Treatment for Narcolepsy
• Excessive Daytime Sleepiness stimulants
• REM-associated phenomena SSRIs or Tricyclics
• Excessive daytime sleepiness and Cataplexy Sodium oxybate (Xyrem)
Issues discussed at first visit:
• Will you go back to work during pregnancy?• Do you want to breast feed? For how long?• Is there a possibility of a night nurse? • Family leave for dads - can your husband
take it?• No medication at all during pregnancy?• Meds when baby comes?
Issues discussed at first visit:• Options for medications:
– Sertraline: SSRI to help with cataplexy– Ritalin - low dose, short acting has the most
data - and in many instances the benefits to you and fetus will outweigh risks to fetus (DideriksenD, et al., 2013; Pottegård A, et al., 2014)
– Xyrem - short term exposure may allow you to have a vaginal delivery and benefits may outweigh risk.
Sleep Disorders in Pregnancy: Narcolepsy
• Multinational cohort study, 2013• Pregnant narcolepsy patients:
– Older – Anemia– BMI – Impaired glucose tolerance– C-section rate – weight gain
• 3/249 had cataplexy during delivery• 40% reported worsening narcolepsy sx
Maurovich-Horvat et al, J Sleep Res, 2013
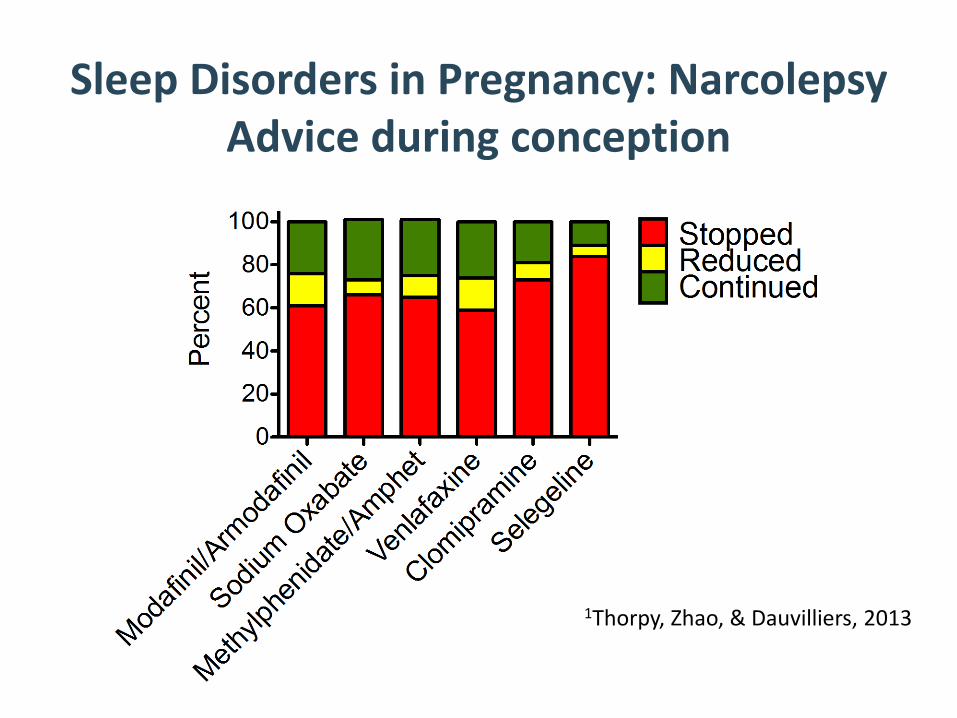
Sleep Disorders in Pregnancy: NarcolepsyAdvice during conception
1Thorpy, Zhao, & Dauvilliers, 2013
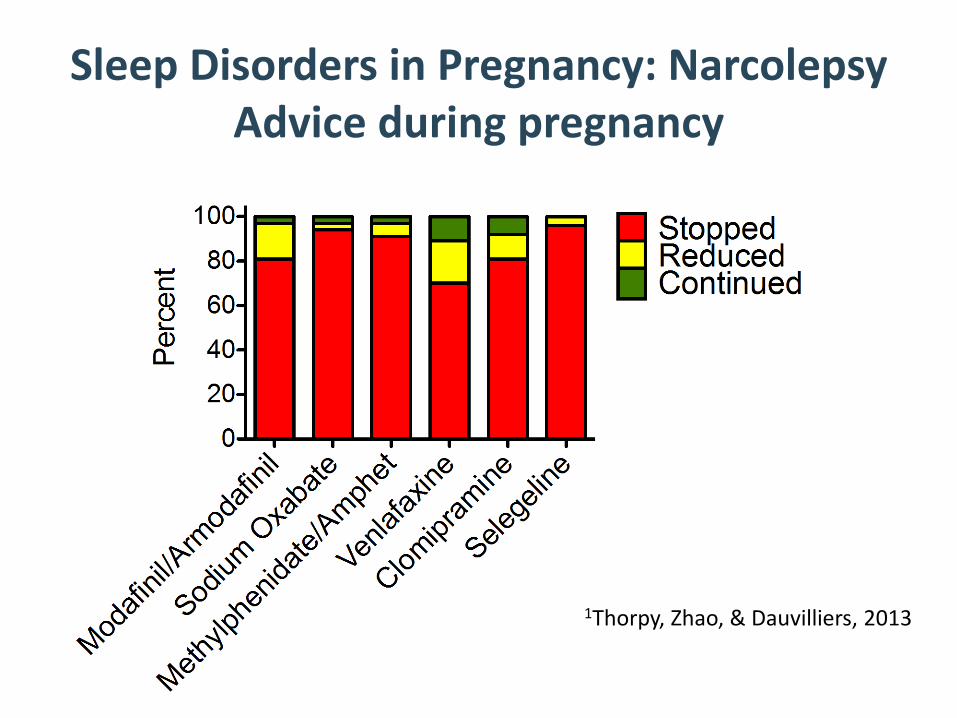
Sleep Disorders in Pregnancy: NarcolepsyAdvice during pregnancy
1Thorpy, Zhao, & Dauvilliers, 2013
Case 1• 15 weeks
– Came with husband– Having more cataplexy– Obtained OB Medicine Consult– Scheduled level 2 ultrasound– Some anxiety/loneliness
• 20 weeks– started sertraline 25 mg– Napping more– Worried about work
Case 1• 27 weeks
– Having more cataplexy– Sleep irregular– Increased sertraline to 50 mg
• 31 weeks– Looking into measuring sodium oxybate in
breast milk• 35 weeks
– Has gained 50 lbs– Cataplexy and anxiety better on zoloft
Case 1• 39 weeks
– sertraline to 50 mg– doing great
• Postpartum week 5– Vaginal delivery of healthy infant– Exclusively breastfeeding– Interested in restarting Xyrem
What do you do next?• Restart sodium oxybate, encourage patient
to continue breast feeding• Restart sodium oxybate, encourage patient
to switch to formula• Continue to hold sodium oxybate,
encourage patient to continue breast feeding
• Something else
What do you do next?• Restart sodium oxybate, encourage patient
to continue breast feeding• Restart sodium oxybate, encourage patient
to switch to formula• Continue to hold sodium oxybate,
encourage patient to continue breast feeding
• Postpartum Month 5– Collected breast milk for GHB levels
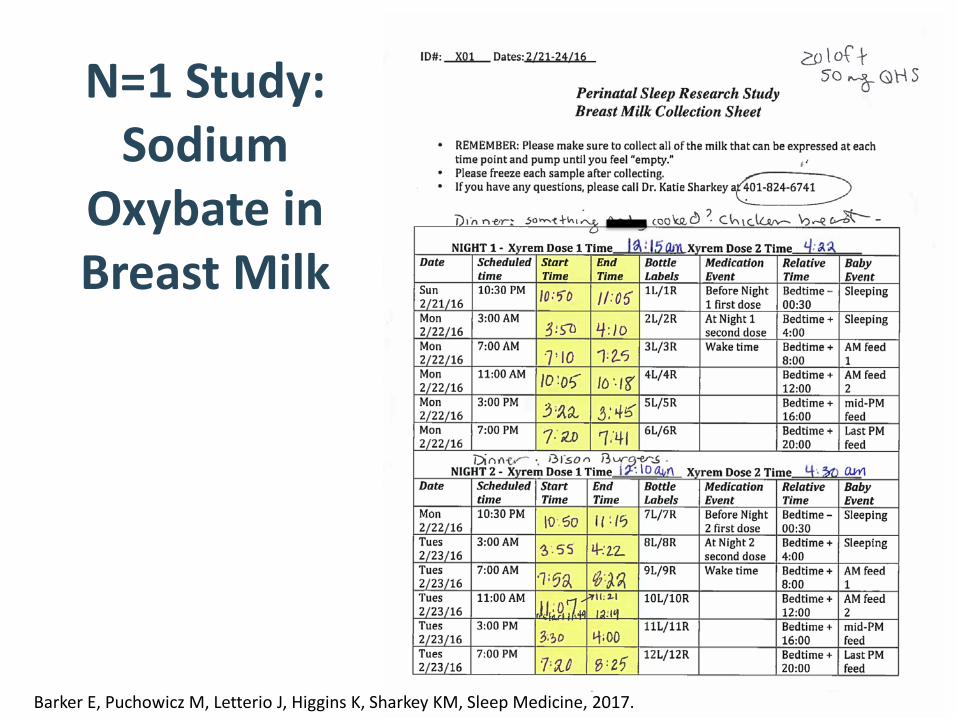
N=1 Study: Sodium
Oxybate in Breast Milk
Barker E, Puchowicz M, Letterio J, Higgins K, Sharkey KM, Sleep Medicine, 2017.
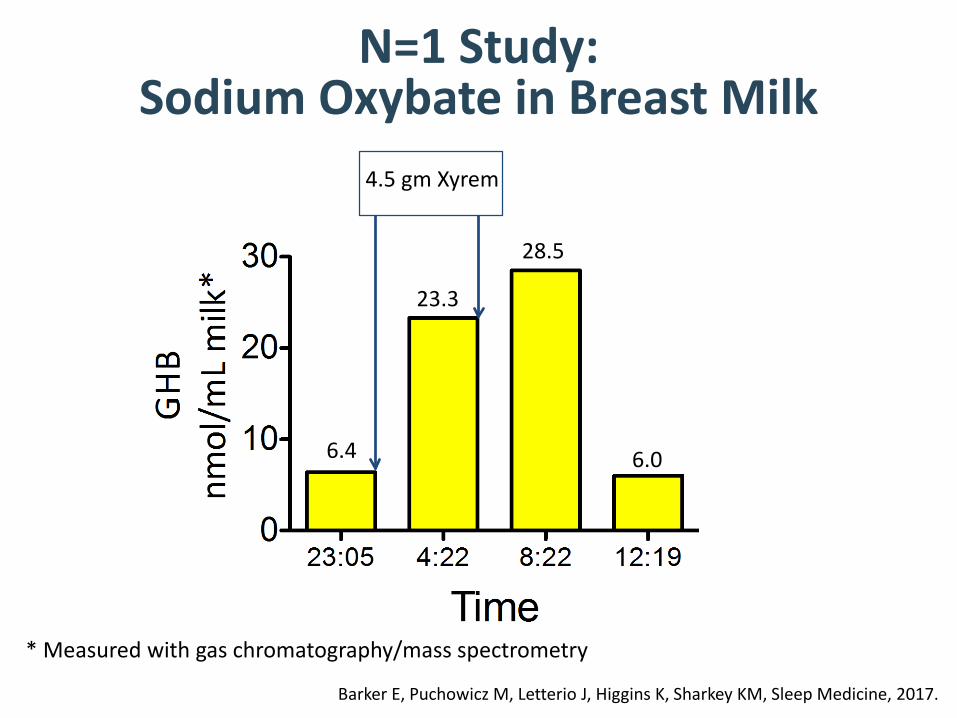
N=1 Study: Sodium Oxybate in Breast Milk
6.4
23.3
28.5
6.0
* Measured with gas chromatography/mass spectrometry
4.5 gm Xyrem
Barker E, Puchowicz M, Letterio J, Higgins K, Sharkey KM, Sleep Medicine, 2017.
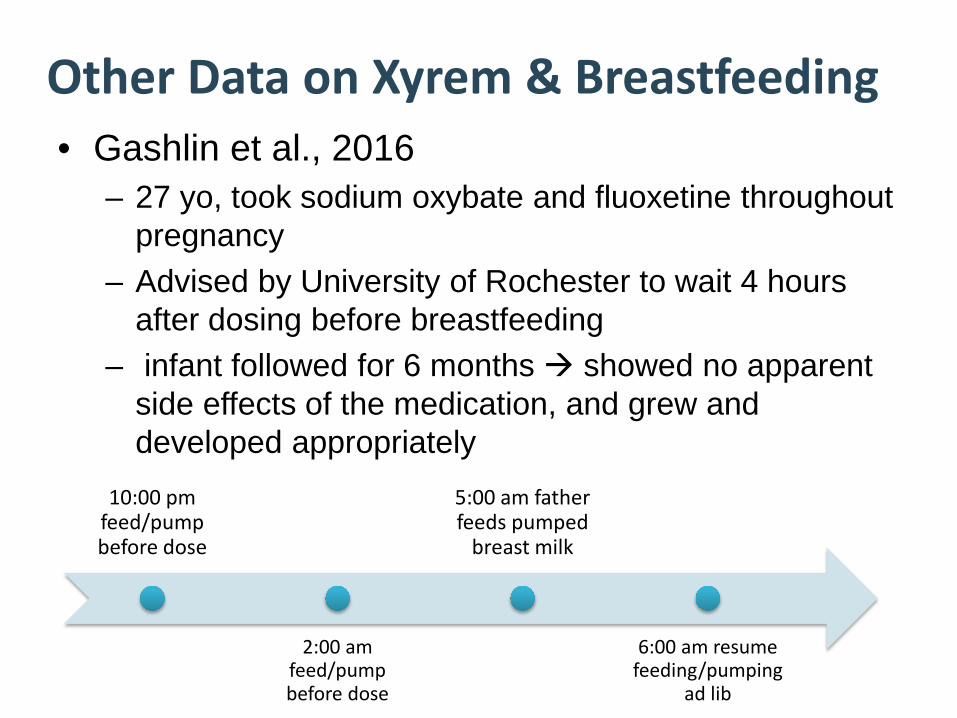
Other Data on Xyrem & Breastfeeding• Gashlin et al., 2016
– 27 yo, took sodium oxybate and fluoxetine throughout pregnancy
– Advised by University of Rochester to wait 4 hours after dosing before breastfeeding
– infant followed for 6 months showed no apparent side effects of the medication, and grew and developed appropriately
10:00 pm feed/pump before dose
2:00 am feed/pump before dose
5:00 am father feeds pumped
breast milk
6:00 am resume feeding/pumping
ad lib
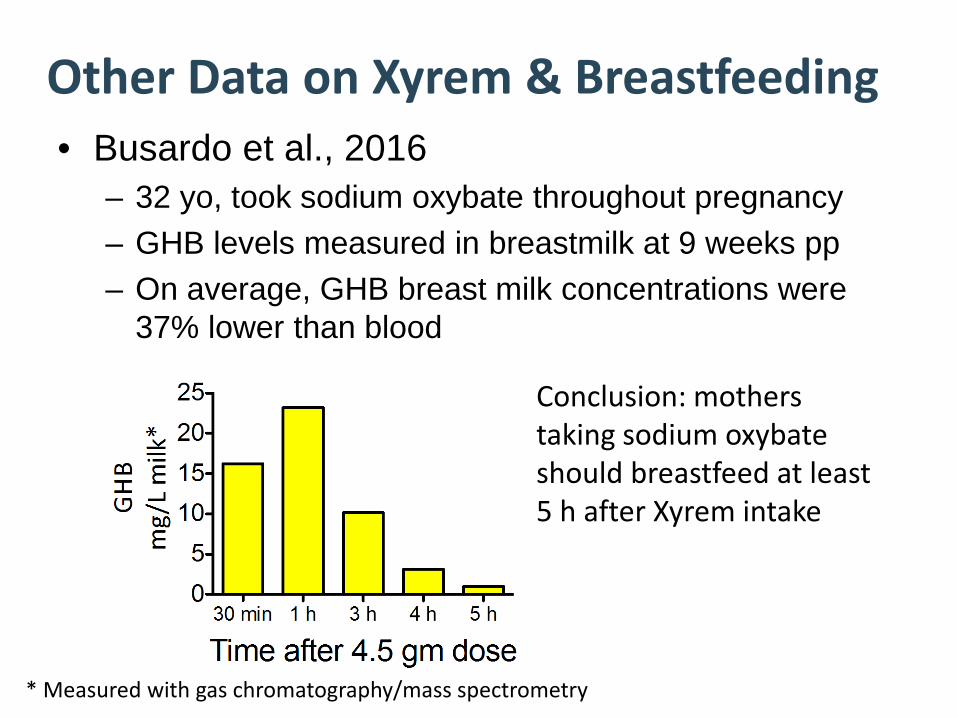
Other Data on Xyrem & Breastfeeding• Busardo et al., 2016
– 32 yo, took sodium oxybate throughout pregnancy– GHB levels measured in breastmilk at 9 weeks pp– On average, GHB breast milk concentrations were
37% lower than blood
* Measured with gas chromatography/mass spectrometry
Conclusion: mothers taking sodium oxybateshould breastfeed at least 5 h after Xyrem intake
Sleep Disorders in Pregnancy: Narcolepsy
• No standard treatment guidelines• Most physicians d/c meds1
• Perceived risks overestimated1
• Most women have vaginal delivery• EDS, cataplexy, and sleepiness are pervasive
postpartum
1Thorpy, Zhao, & Dauvilliers, 2013; Oyeingo, Louis, Hott, & Bourjeily, 2014
Sleep Disorders in Pregnancy: NarcolepsyPractical Aspects
• Manage work schedule• Work with obstetric team• Good pain control• Avoid sleep loss • Deliver during the day• Enlist help with infant care to minimize
maternal sleep deprivation1Thorpy, Zhao, & Dauvilliers, 2013; Oyeingo, Louis, Hott, & Bourjeily, 2014

Case 2• 82 yo woman with hypothyroidism and
dementia referred for insomnia and hallucinations
• Memory difficulties for 3 years• Daytime symptoms: daytime sleepiness,
hallucinations, confusion• Nocturnal behaviors: waking from sleep
and getting OOB to perform activities that did not make sense
Case 2• Bedtime: 10 pm falls asleep without
difficulty• Nocturnal awakenings: 2-4x per night • Snoring• Sleep fragmentation• Wakes with hallucinations and confusion• No RLS or leg kicks
Case 2• Wake time: 7 am husband wakes her to
give thyroid medication– She is frequently already awake at this time
• Stays in bed until 8:00-8:30 am– Breakfast
Case 2• Best time of day pt says early pm• Husband says lots of daytime dozing• Daytime hallucinations seem to emanate
from naps:– E.g., she will be asleep and then when she
wakes she reports seeing a family member in the room
Case 2 - Exam• BMI = 32.4 kg/m2
• Mallampati class 4 airway, crowded posterior oropharynx
• Neurologic exam – no tremor or cogwheel rigidity
• MMSE = 23/30 abnormal
Case 2 - Differential• Obstructive sleep apnea• REM Behavior Disorder (RBD)• Irregular sleep-wake rhythm disorder
Case 2 – Initial Plan• Home sleep testing
• Laboratory polysomnography
• Actigraphy
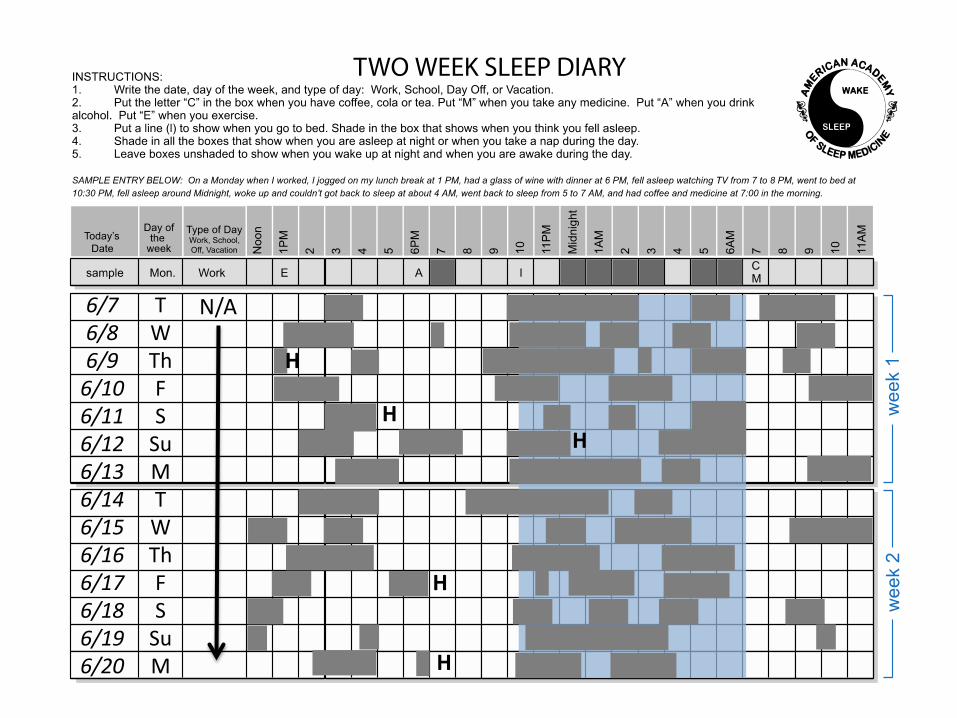
• Sleep Diaries
• Something Else
Case 2 – Initial Plan• Home sleep testing
• Laboratory polysomnography
• Actigraphy
• Sleep Diaries
• Something Else
Case 2 – Lab PSG• Sleep latency: 22 minutes• Sleep efficiency: 71%• Arousal index: 22.1 events/hr• No REM• Respiratory events: 9 apneas, 7 hypopneas,
4% AHI < 5 events/hr• O2 Sat min = 89% but 98.3% of recording
showed O2 Sat > 90%• No PLMS
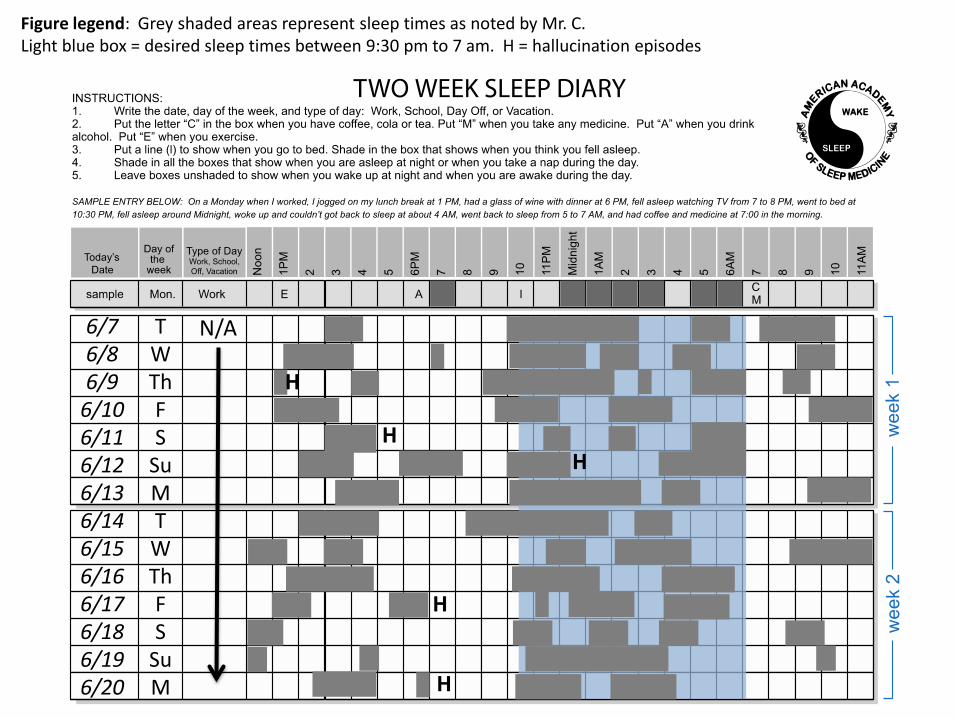
N/ATWThFS
SuMTWThFS
SuM
6/76/86/9
6/106/116/126/136/146/156/166/176/186/196/20
HH
H
H
H
Figure legend: Grey shaded areas represent sleep times as noted by Mr. C. Light blue box = desired sleep times between 9:30 pm to 7 am. H = hallucination episodes
What do you think she has?
• Obstructive sleep apnea• REM Behavior Disorder (RBD)• Irregular sleep-wake rhythm disorder
What do you think she has?
• Obstructive sleep apnea• REM Behavior Disorder (RBD)• Irregular sleep-wake rhythm disorder
What do you do next?• Repeat PSG• 2 weeks of actigraphy• CBT-I• Start modafinil• Start morning light therapy• Start melatonin
What do you do next?• Repeat PSG• 2 weeks of actigraphy• CBT-I• Start modafinil• Start morning light therapy• Start melatonin
Irregular Sleep-Wake Phase Disorder
• Lack of circadian pattern of sleep-wake behavior
• Periods of wakefulness during sleep hours • Excessive sleepiness and daytime napping• Fragmented and insufficient sleep• More common among patients with
neurodevelopmental/neurodegenerative disorders– Can pose challenges for caregivers
FeaturesIrregular Sleep-Wake Rhythm Disorder
DiagnosisIrregular Sleep-Wake Rhythm Disorder
• Diaries• Actigraphy• Minimum duration 7 days
N/ATWThFS
SuMTWThFS
SuM
6/76/86/9
6/106/116/126/136/146/156/166/176/186/196/20
HH
H
H
H
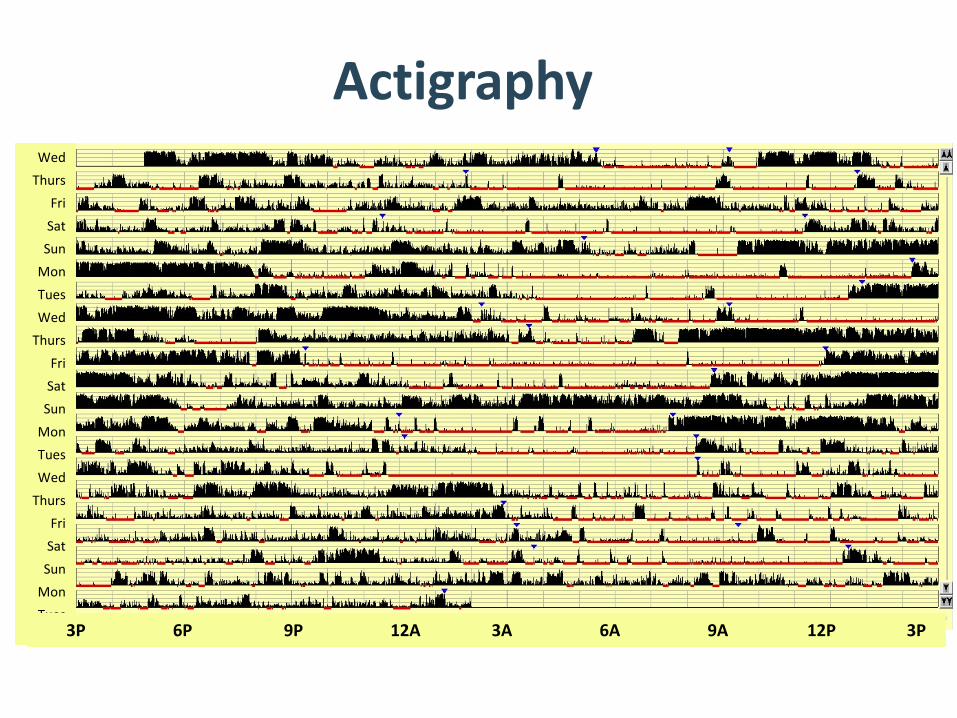
WedThurs
FriSat
SunMonTuesWed
ThursFri
SatSun
MonTuesWed
ThursFri
SatSun
MonTues
3P 6P 9P 12A 3A 6A 9A 12P 3P
Actigraphy
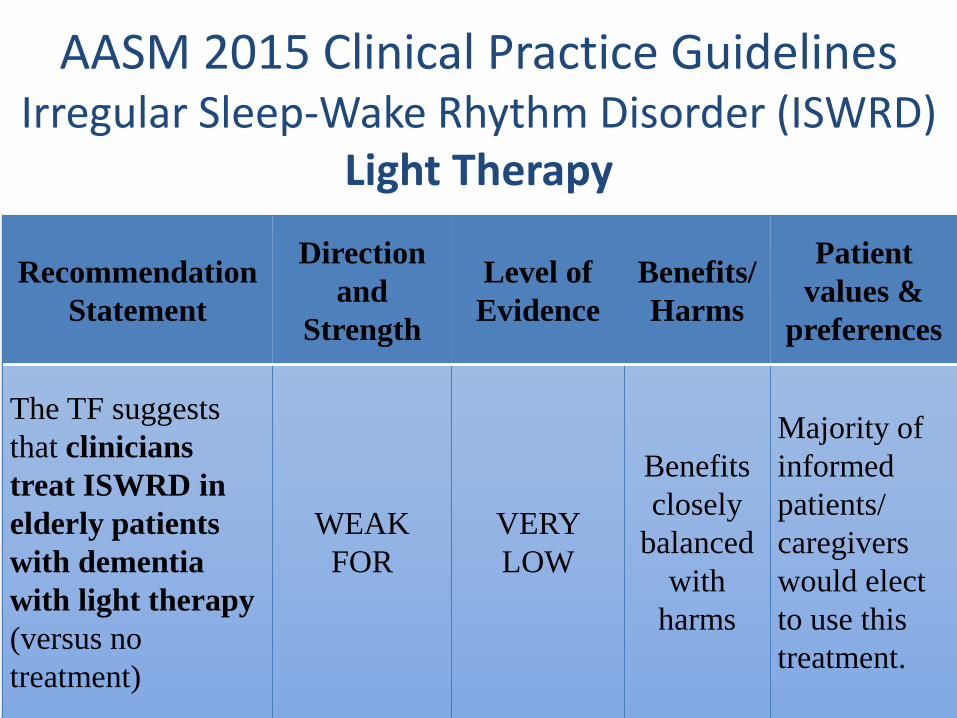
AASM 2015 Clinical Practice GuidelinesIrregular Sleep-Wake Rhythm Disorder (ISWRD)
Light Therapy
Recommendation Statement
Direction and
Strength
Level of Evidence
Benefits/Harms
Patient values &
preferences
The TF suggests that clinicians treat ISWRD in elderly patients with dementia with light therapy (versus no treatment)
WEAK FOR
VERY LOW
Benefits closely
balanced with
harms
Majority of informed patients/ caregivers would elect to use this treatment.
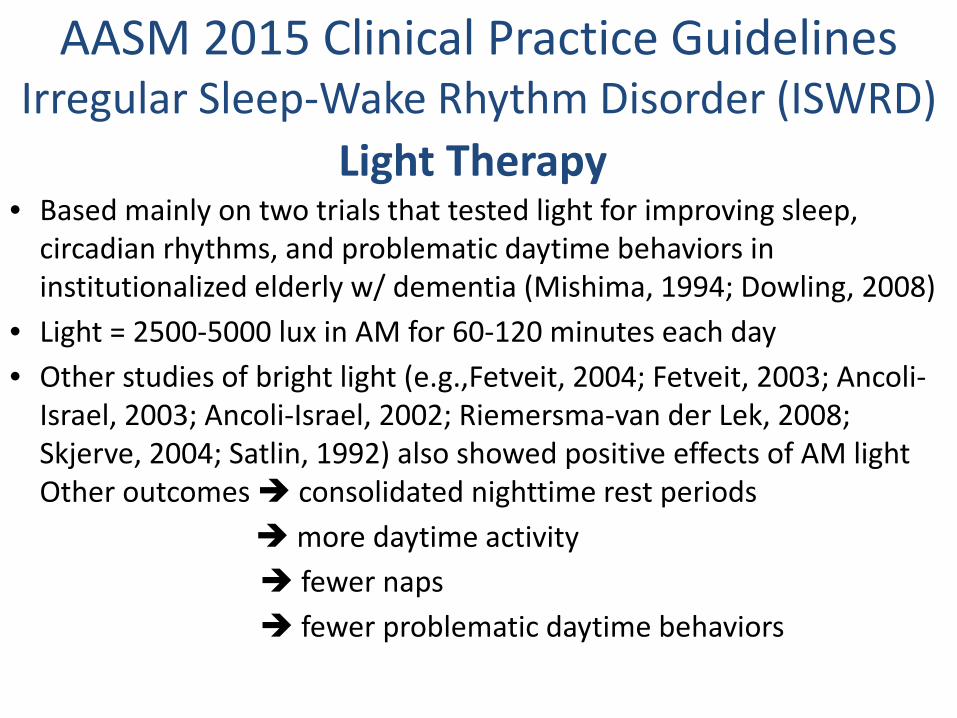
AASM 2015 Clinical Practice GuidelinesIrregular Sleep-Wake Rhythm Disorder (ISWRD)
Light Therapy• Based mainly on two trials that tested light for improving sleep,
circadian rhythms, and problematic daytime behaviors in institutionalized elderly w/ dementia (Mishima, 1994; Dowling, 2008)
• Light = 2500-5000 lux in AM for 60-120 minutes each day • Other studies of bright light (e.g.,Fetveit, 2004; Fetveit, 2003; Ancoli-
Israel, 2003; Ancoli-Israel, 2002; Riemersma-van der Lek, 2008; Skjerve, 2004; Satlin, 1992) also showed positive effects of AM light Other outcomes consolidated nighttime rest periods
more daytime activity fewer naps fewer problematic daytime behaviors
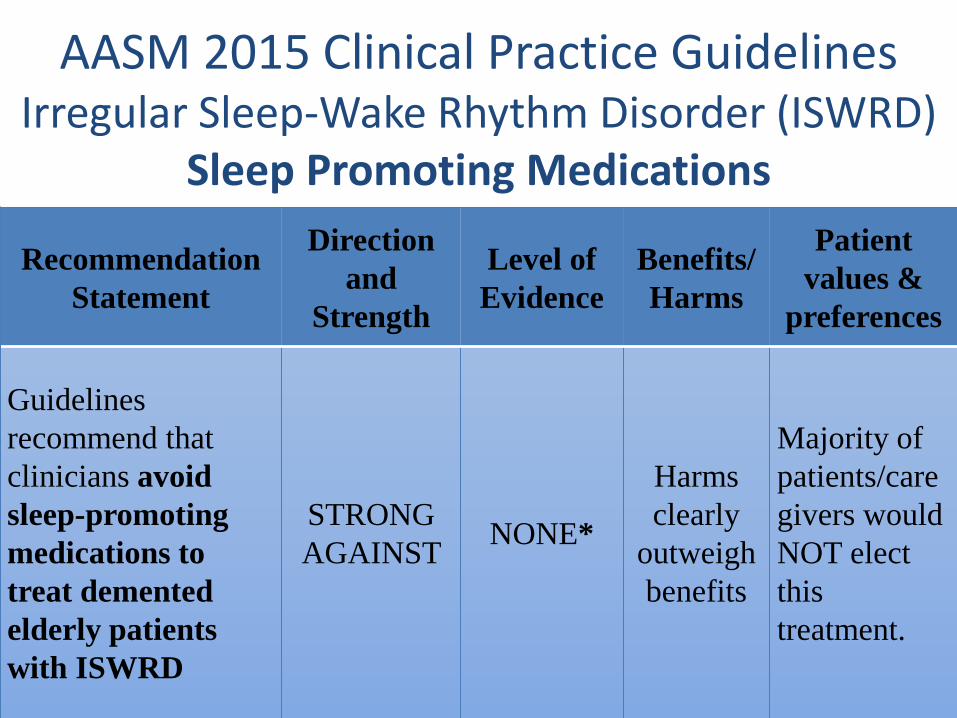
AASM 2015 Clinical Practice GuidelinesIrregular Sleep-Wake Rhythm Disorder (ISWRD)
Sleep Promoting Medications
Recommendation Statement
Direction and
Strength
Level of Evidence
Benefits/Harms
Patient values &
preferences
Guidelines recommend that clinicians avoidsleep-promoting medications to treat demented elderly patients with ISWRD
STRONG AGAINST NONE*
Harms clearly
outweigh benefits
Majority of patients/caregivers would NOT elect this treatment.
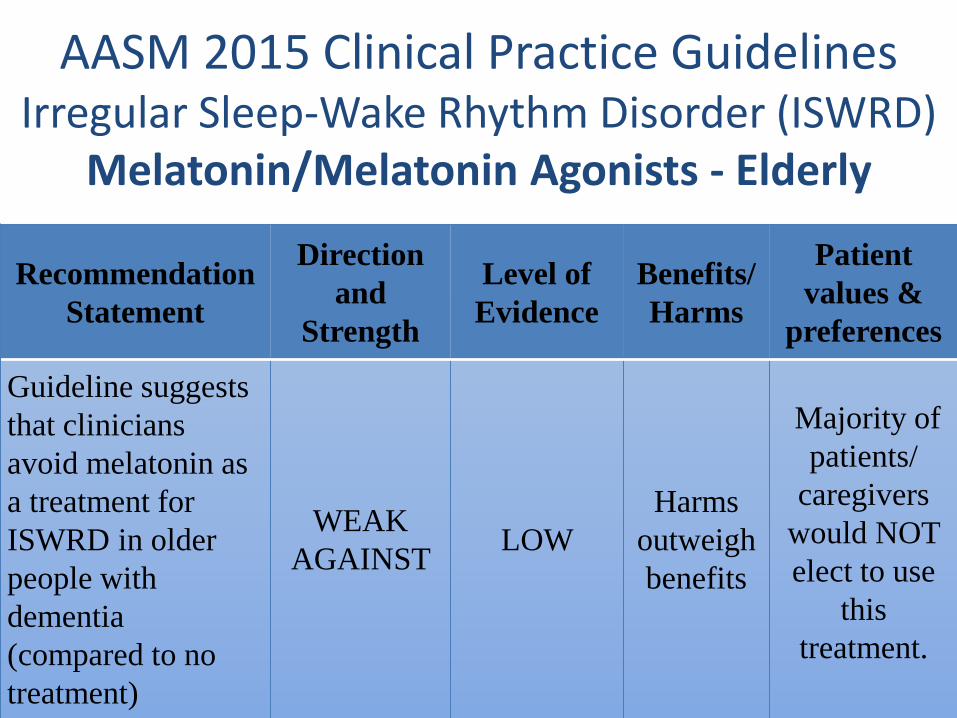
AASM 2015 Clinical Practice GuidelinesIrregular Sleep-Wake Rhythm Disorder (ISWRD)
Melatonin/Melatonin Agonists - Elderly
Recommendation Statement
Direction and
Strength
Level of Evidence
Benefits/Harms
Patient values &
preferences
Guideline suggests that clinicians avoid melatonin as a treatment for ISWRD in older people with dementia (compared to no treatment)
WEAK AGAINST LOW
Harms outweigh benefits
Majority of patients/
caregivers would NOT elect to use
this treatment.
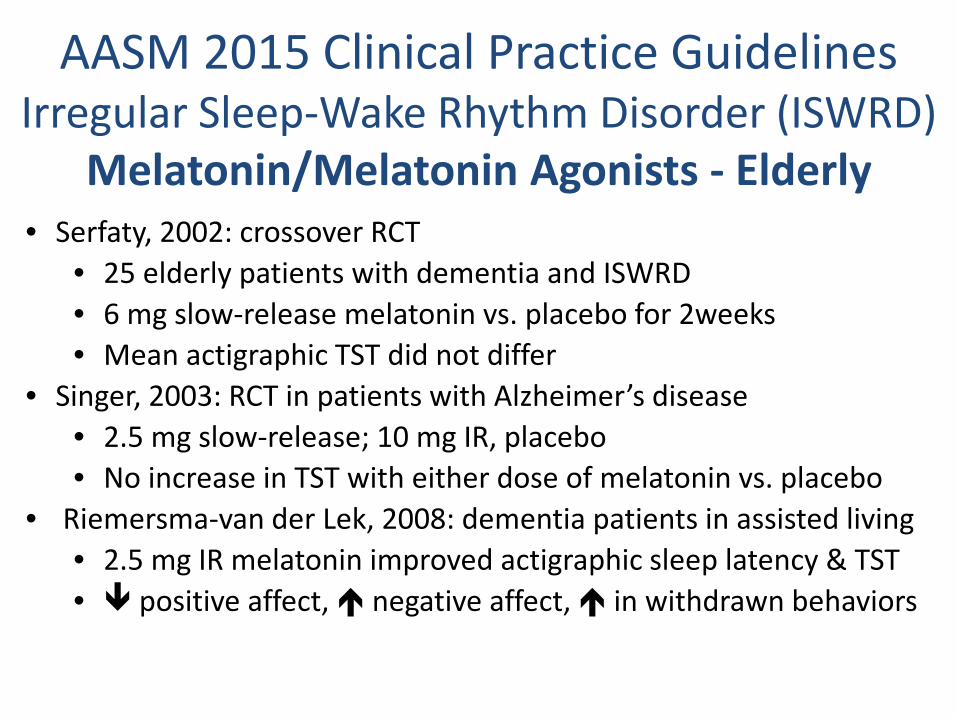
AASM 2015 Clinical Practice GuidelinesIrregular Sleep-Wake Rhythm Disorder (ISWRD)
Melatonin/Melatonin Agonists - Elderly• Serfaty, 2002: crossover RCT
• 25 elderly patients with dementia and ISWRD • 6 mg slow-release melatonin vs. placebo for 2weeks• Mean actigraphic TST did not differ
• Singer, 2003: RCT in patients with Alzheimer’s disease• 2.5 mg slow-release; 10 mg IR, placebo• No increase in TST with either dose of melatonin vs. placebo
• Riemersma-van der Lek, 2008: dementia patients in assisted living • 2.5 mg IR melatonin improved actigraphic sleep latency & TST• positive affect, negative affect, in withdrawn behaviors
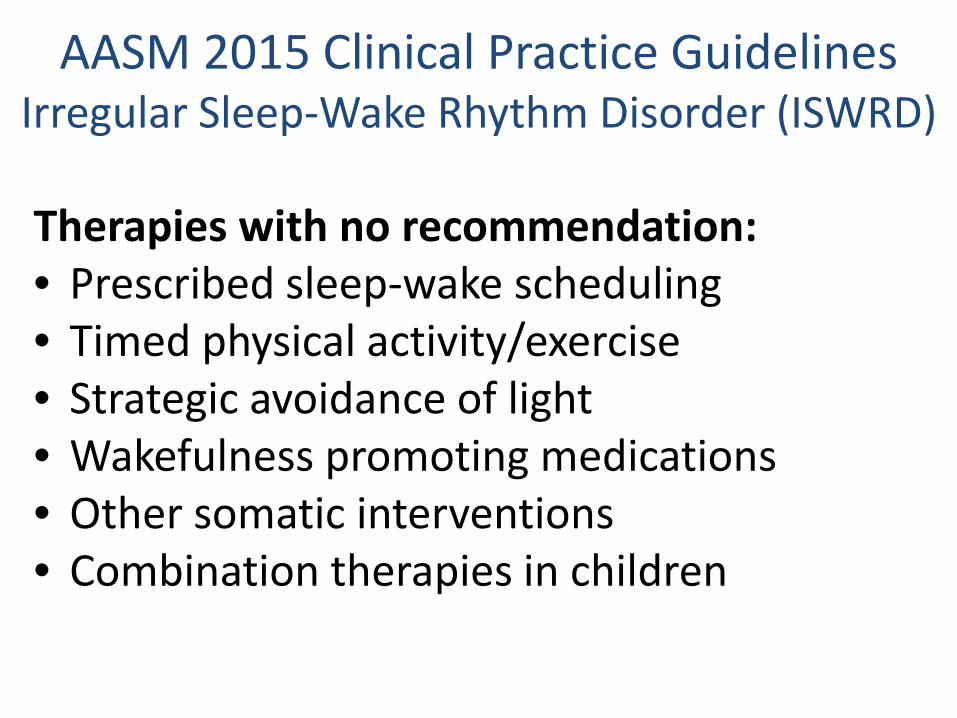
AASM 2015 Clinical Practice GuidelinesIrregular Sleep-Wake Rhythm Disorder (ISWRD)
Therapies with no recommendation:• Prescribed sleep-wake scheduling• Timed physical activity/exercise• Strategic avoidance of light• Wakefulness promoting medications• Other somatic interventions• Combination therapies in children
• Bright light therapy recommended for all patients– AM light has most data supporting use
• Strategically-timed melatonin recommended for developmentally-delayed children/adolescents– Usually administered at bedtime
• Melatonin is not recommended for elderly patients Lack of documented efficacy Increased risk of depressive mood
Treatment Summary
Irregular Sleep-Wake Rhythm Disorder
Case 2 – Treatment initiation• Discussed positive effects of AM bright light
– more consolidated rest periods at night – more daytime activity and fewer naps– Fewer problematic behaviors during the day
• Recommended morning bright light• Reluctant to get a bright light box
– noted that the room where pt sits in the morningis well lit and has south-facing windows
Case 2 – Treatment initiation• Discussed risks/benefits/side
effects/alternatives to melatonin• Pt and husband elected to try melatonin
3mg immediate release at bedtime in combination with natural bright light
• Discussed need to monitor for depressive symptoms
…but, wait...
• Obstructive sleep apnea• REM Behavior Disorder (RBD)
– CANNOT EXCLUDE RBD BUT DECISION WAS MADE TO HOLD OFF ON REPEAT SLEEP STUDY OR TRIAL OF CLONAZEPAM DUE TO RISK OF FALLS AND POTENTIAL BENEFIT OF MELATONIN IN RBD
• Irregular sleep-wake rhythm disorder
Case 2 – Follow up• Melatonin at night and increased effort to keep
drapes open in the AM• Pt reports sleep is better and “the various
aches and pains in my body are not as bad and I don’t have as much trouble settling down at night.”
• Husband says sleep is better at night, fewer hallucinations
• Initially had daytime sedation cut melatonin dose to 1.5 mg
• No worsening in depressive symptoms (sadness, crying, emotional lability, decreased interaction with others or suicidal ideation)